
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol., 16 June 2021
Sec. Vaccines and Molecular Therapeutics
Volume 12 - 2021 | https://doi.org/10.3389/fimmu.2021.704773
 Emanuel Zitt1,2,3*
Emanuel Zitt1,2,3* Tamara Davidovic1Judith Schimpf1Armin Abbassi-Nik1Beatrix Mutschlechner4Hanno Ulmer5Magdalena A. Benda6Hannelore Sprenger-Mähr1Thomas Winder6Karl Lhotta1,2
Tamara Davidovic1Judith Schimpf1Armin Abbassi-Nik1Beatrix Mutschlechner4Hanno Ulmer5Magdalena A. Benda6Hannelore Sprenger-Mähr1Thomas Winder6Karl Lhotta1,2Background: Hemodialysis patients are at high risk for severe COVID-19. SARS-CoV-2 vaccination related safety and immunogenicity data in these patients are rare.
Methods: In this observational study SARS-CoV-2-seronegative hemodialysis patients were vaccinated with two doses of the Pfizer/BioNTech mRNA-BNT162b2 vaccine (COMIRNATY® 30 µg) and followed for 90 days. Local and systemic side effects were assessed at every dialysis session during the first post-vaccination week after the first and second vaccine dose. Immunogenicity was determined four weeks after vaccination by quantifying anti-SARS-CoV-2 spike protein IgG antibodies (LIAISON® SARS-CoV-2-TrimericS IgG chemiluminescent immunoassay) expressed in binding activity units per milliliter (BAU/mL) adapted to the WHO International standard.
Results: Fifty patients (32% women, 68% men) with a mean (SD) age of 67.6 (14.8) years were included. Mild local reactions occurred in 38% after the first injection, and in 29.2% with mild, in 2.1% with moderate and in 2.1% with severe degree after the second injection. Systemic reactive events occurred less often, with diarrhea (4% mild, 4% moderate) and fatigue (8% mild) being the most frequent ones. After the first injection 42% of the patients developed a positive response using the assay specific cut-off value of 33.8 binding activity units per milliliter (BAU/mL) with a median (Q1, Q3) anti-SARS-CoV-2 spike IgG concentration of 20.0 (11.7, 51.0) BAU/mL. After the second injection the percentage of seropositive patients increased to 97.9% with an anti-SARS-CoV-2 spike IgG concentration of 1075 (290.8, 1735) BAU/mL. Higher age and immunosuppression were associated with lower, calcitriol treatment and prior seroconversion to hepatitis B vaccination with significantly higher antibody concentration.
Conclusions: The mRNA-BNT162b2 SARS-CoV-2 vaccine appears to be safe and well-tolerated and shows a high immunogenicity in hemodialysis patients.
Patients with chronic kidney disease, and particularly hemodialysis patients carry a high burden of coronavirus disease 2019 (COVID-19) and are at highest risk for a severe course and death (1–3). The vast majority of these vulnerable patients are treated with in-center hemodialysis. This translates into an unpreventably increased risk of exposure to COVID-19 due to the frequent contacts with potentially infected patients, health care professionals or transport personnel. Several SARS-CoV-2 vaccines have proven to be highly effective to prevent COVID-19 in the general population (4–6). Hemodialysis patients were not included in the pivotal trials but have shown a similar seroconversion rate after SARS-CoV-2 infection as compared to the general population (7). Therefore, it seems plausible to assume an adequate seroconversion after vaccination. On the other hand, vaccination hypo-responsiveness has been shown in dialysis patients. As an example, the seroconversion rate after active hepatitis B vaccination is only 40-70% compared to >95% in healthy controls despite the use of a high-dose vaccine (8–11). Different host factors contribute to this impaired vaccination response, including age, presence of diabetes, an altered innate and adaptive immune response, nutritional status and vaccine characteristics such as formulation, dosage and administration route (12, 13).
The Austrian government and the Austrian National vaccination committee prioritized hemodialysis patients in the national vaccination strategy. We therefore were able to assess the safety and immunogenicity after a complete vaccination course using the mRNA-BNT162b2 SARS-CoV-2 vaccine in chronic hemodialysis patients.
All chronic in-center hemodialysis patients treated at Feldkirch Academic Teaching Hospital, Austria, were invited to receive the SARS-CoV-2 vaccination following the prioritization by the National Vaccination Committee (14). Only patients with a negative anti SARS-CoV-2-serology were included in accordance with the National Vaccination Recommendation. After written informed consent all patients were vaccinated with the Pfizer/BioNTech mRNA-BNT162b2 SARS-CoV-2 vaccine (COMIRNATY®) with a dosing interval of 25 to 26 days between the first and second injection. The first doses were given on January 9th and 11th, the second doses on February 4th and 5th 2021. Out of 87 hemodialysis patients, 50 received the first dose, and 48 completed the vaccination course with a second dose. A detailed patient flow chart is presented in Figure 1. Every patient received 30 µg of the vaccine delivered in the deltoid muscle of the non-fistula carrying arm using a 22 gauge (0.7 x 30 mm) needle (BD Eclipse™ Needle) approximately 30 minutes before the end of the dialysis session and was carefully monitored thereafter. Dialysis settings remained unchanged during the sessions the patients were vaccinated. No changes were made to anticoagulation. Low-molecular weight heparin was used as usual without dose adjustments, and patients on oral anticoagulation were not asked to reduce or pause oral anticoagulation therapy on the vaccination day. Baseline laboratory parameters were collected during the week prior to each vaccination as routinely recorded at the beginning of the month. Single-pool Kt/V was calculated using the Daugirdas formula (15) and averaged for one week.
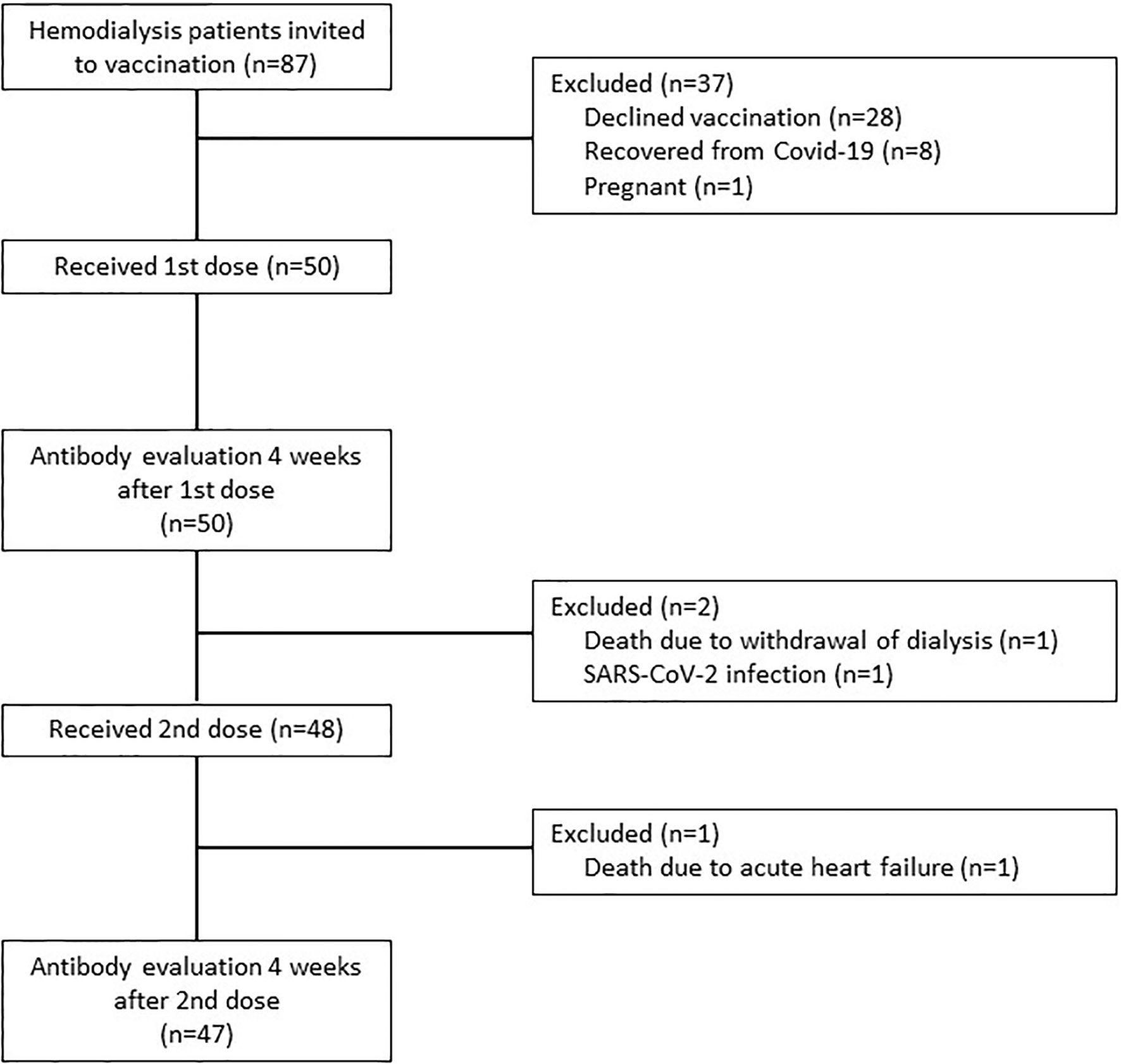
Figure 1 Patient flow diagram.
All vaccinated patients were asked in personal interviews at each hemodialysis session during the first post-vaccination week for the occurrence of local and systemic side effects and reactions after the first and second vaccine dose. Body temperature was measured at the beginning of each session. Side effects and reactions were evaluated in accordance with the pivotal study of Polack et al. (5)
Immunogenicity was determined after the first injection on the day of the second injection and four weeks after the second vaccine dose by quantifying IgG antibodies from the patients´ serum. We used the LIAISON® SARS-CoV-2-TrimericS IgG chemiluminescent immunoassay (Diasorin S.p.A., Saluggia, Italy). The assay detects IgG antibodies against the trimeric spike glycoprotein including the receptor-binding domain (RBD) and the N-terminal domain (NTD) sites from the S1 subunit. The assay has a clinical sensitivity of 98.7%, a specificity of 99.5% (95% confidence interval [95% CI] 99.0% - 99.7%), and has a very good correlation with the microneutralization test with a positive predictive agreement of 100% (95% CI 97.8% - 100%) and a negative predictive agreement of 96.9% (95% CI 92.9% - 98.7%). Test results were adapted to the WHO International standard for anti-SARS-CoV-2 immunoglobulin binding activity and presented in binding activity units per milliliter (BAU/mL) following the conversion equation “AU/mL*2.6 = BAU/mL” according to the manufacturer. A value of ≥33.8 BAU/mL was considered as evidence of a positive vaccination antibody response with seroconversion. The assay range according to the manufacturer is 4.81 - 2080 BAU/ml. For the detection of SARS-CoV-2- infection a commercially available RT-PCR (Seegene Allplex™ SARS-CoV-2 assay, Seegene Inc., Seoul, South Korea) targeting the three viral genes E-, RdRP- and N-gene on a nasopharyngeal swab was used.
This observational cohort study was conducted in compliance with the Helsinki Declaration of 1975, as revised in 2013, and Good Clinical Practice. The study protocol was approved by the institutional review board and the ethics committees of the Innsbruck Medical University (EK Nr: 1088/2021). STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) guidelines were followed for the preparation of this article (16).
Categorical data are presented as absolute and relative number of patients. For continuous data mean and standard deviation (SD) or median with interquartile range (1st quartile, 3rd quartile) was used, depending on its distribution. Categorical parameters were compared using exact Chi-squared tests, normally distributed continuous parameters were analysed with Student’s T test and not normally distributed parameters with Mann-Whitney U test. A multiple linear regression analysis including the explanatory variables age, gender, dialysis vintage, diabetes mellitus, immunosuppression and calcitriol treatment was used to determine significant predictors of the antibody concentration four weeks after the second vaccine dose. The selection of explanatory variables for the multiple linear regression model was based on clinical importance and published literature, and restricted due to the patient number. The R² for the overall model was 0.314 (adjusted R² = 0.214), indicative for a high goodness-of-fit. A two-sided P value <0.05 was deemed to indicate statistical significance. All statistical analyses were performed with IBM SPSS Statistics 26 (IBM, Armonk (NY), USA).
Out of our total in-center hemodialysis cohort of 87 patients, 50 patients (32% women, 68% men) with a mean (SD) age of 67.6 (14.8) years received the first vaccine dose. As shown in Figure 1, 28 patients declined vaccination due to personal reasons, eight patients had recovered from prior COVID-19 with detectable antibodies and were therefore not prioritized for early vaccination, and one patient was pregnant and therefore excluded from vaccination. Forty-eight patients received the second dose, and 47 patients were available for the assessment of antibody response four weeks after the complete vaccination course. Safety data could be collected from 50 patients after the first injection and from 48 patients after the second dose. The baseline characteristics of all vaccinated patients are presented in Table 1.
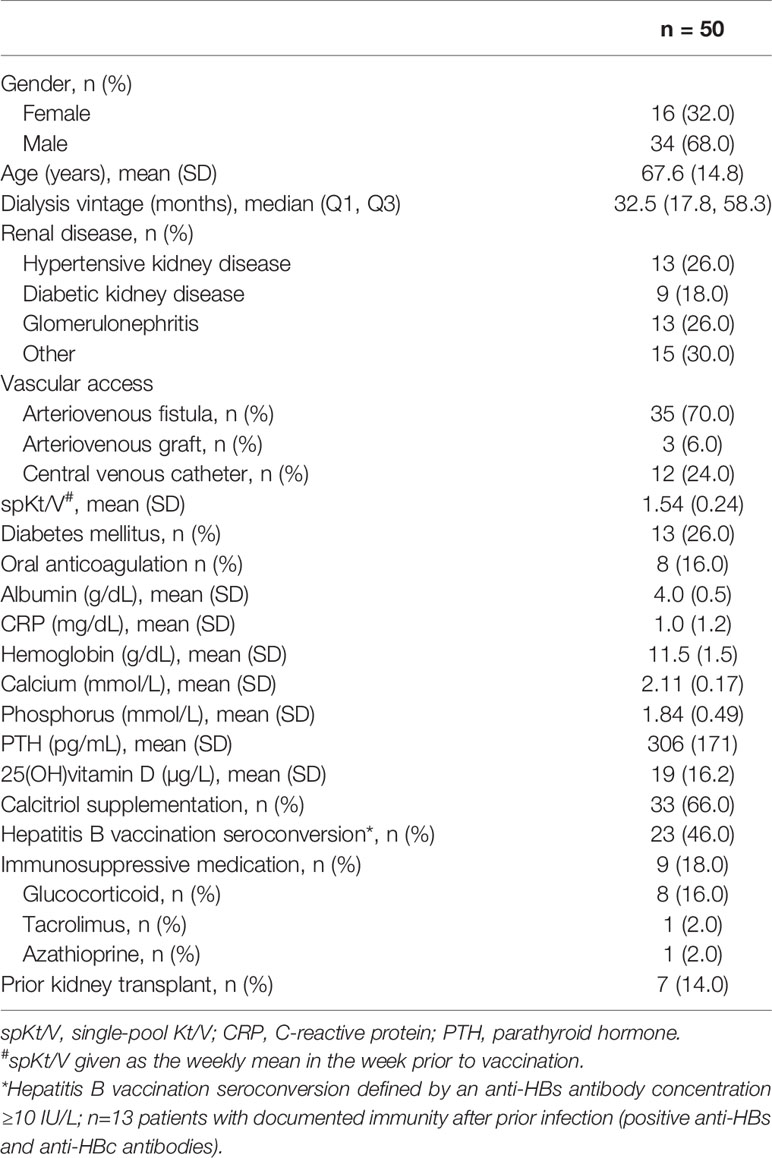
Table 1 Baseline characteristics of the study population.
Overall, the mRNA-BNT162b2 SARS-CoV-2 vaccine was well tolerated. Pain at the injection site within seven days after the injection was the most commonly reported local reaction, occurring in 38% of the patients of mild degree after the first injection. After the second injection, 29.2% of the patients reported mild, 2.1% moderate and 2.1% severe local pain. Despite regular blood circuit anticoagulation with low-molecular weight heparin and continuation of oral anticoagulation no hematoma occurred at the injection site, neither after the first nor the second vaccination.
Systemic reactive events occurred less often, with diarrhea (4% mild, 4% moderate) and fatigue (8% mild) being the most frequent ones after the first injection. The occurrence of chills, muscle and joint pain slightly increased after the second injection, affecting 4.2% of the patients. None of the patients reported fever. In none of the patients a body temperature >38°C was measured before the start of dialysis at the three dialysis sessions during the first week after the injections. An overview of all local and systemic reactions within seven days after the vaccination is given in Figure 2. Two patients died during the study period. One patient deceased five weeks after the first injection because hemodialysis was discontinued and replaced by palliative care. Therefore, this patient did not receive the second vaccine dose. The second patient died from acute on chronic heart failure five days after the second injection. Both deaths were not considered to be related to vaccination.
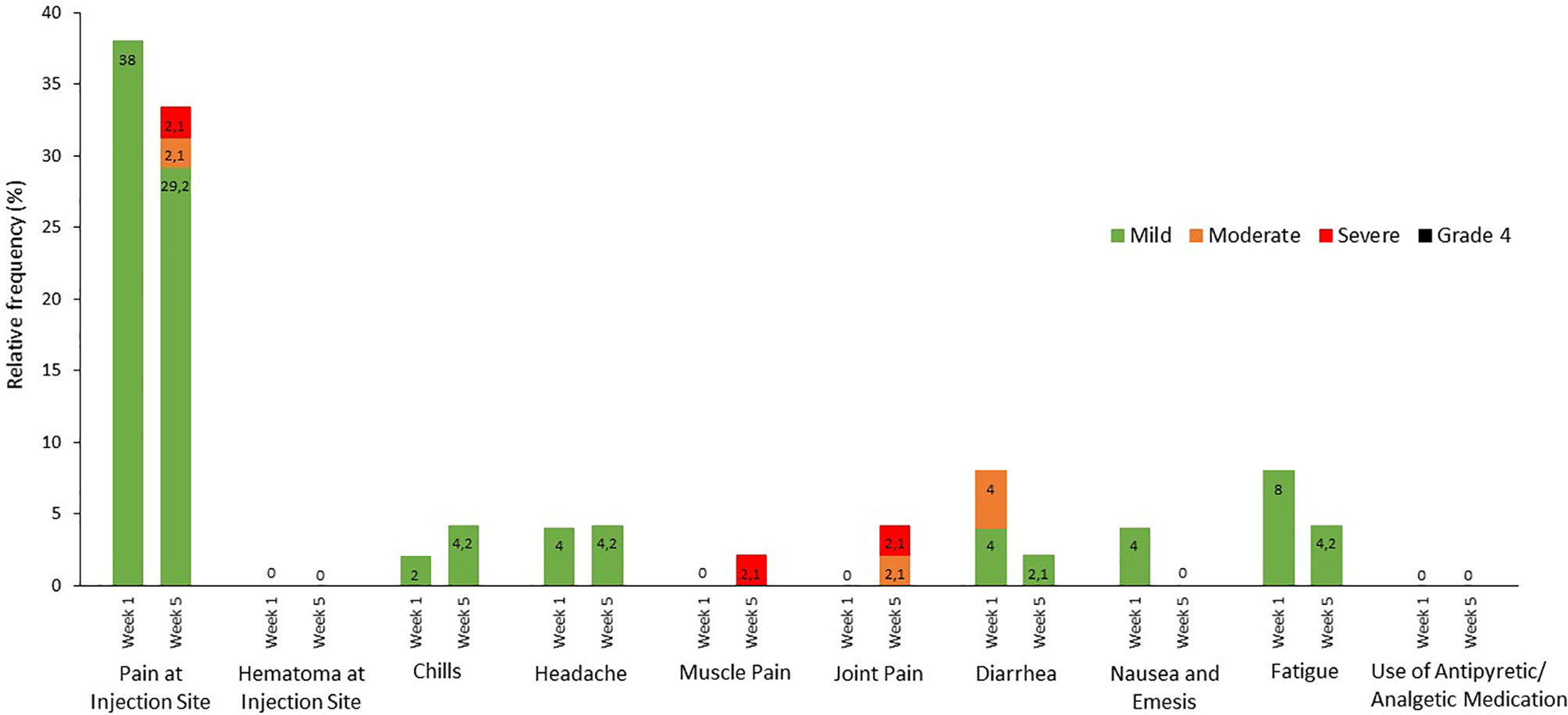
Figure 2 Local and systemic reactions occurring within seven days after vaccination. Data on local and systemic reactions and the use of antipyretic/analgetic medication were collected during each of the three hemodialysis sessions in the first week following vaccination. Pain and hematoma at the injection site was assessed according to the following scale: mild, does not interfere with daily activity; moderate, interferes with daily activity; severe, prevents daily activity; and grade 4, emergency department visit or hospitalization. The systemic reactions were graded according to the following scale: chills, headache, muscle pain, joint pain, fatigue: mild, does not interfere with daily activity; moderate, some interference with daily activity; severe, prevents daily activity; diarrhea: mild, 2 to 3 loose stools in 24 hours; moderate, 4 to 5 loose stools in 24 hours; severe, 6 or more loose stools in 24 hours, nausea & emesis: mild, vomiting 1 to 2 times in 24 hours; moderate, >2 times in 24 hours; severe, requires intravenous hydration; and grade 4 for all events indicated an emergency department visit or hospitalization. Medication use was not graded. Numbers in the bars are the percentage of participants who reported the specified reaction.
Prior to vaccination, all patients were tested to be seronegative for anti-SARS-CoV-2 spike protein IgG antibodies. Four weeks after the first injection 42% of the patients developed a positive antibody response according to the assay specific cut-off value of 33.8 BAU/mL. The median (Q1, Q3) anti-SARS-CoV-2 spike IgG concentration was 20.0 (11.7, 51.0) BAU/mL. Four weeks after the second injection the percentage of seropositive patients increased to 97.9% with a median (Q1, Q3) anti-SARS-CoV-2 spike IgG concentration of 1075 (290.8, 1735) BAU/mL (Figure 3). Only one patient suffering from membranoproliferative glomerulonephritis type I with long-term corticosteroid therapy (ongoing low-dose regimen during the vaccination course) did not respond to vaccination (anti-SARS-CoV-2 spike IgG concentration 4.81 BAU/mL after the first and second injection). Patients with seroconversion after the first vaccine dose were significantly younger than those without (62.7 vs 71.2 years, p=0.043). Patient age was the only baseline characteristic that significantly differed between these two groups (Table 2). Patients with seroconversion after the first vaccine dose (56.7 [48.9, 101.7] BAU/mL) had a significantly higher median [Q1, Q3] anti-SARS-CoV-2 spike IgG concentration after the second dose than those without seroconversion after the first injection (1565.0 [1022.5, 2080.0] BAU/mL vs 635.5 [118.3, 1352.5] BAU/mL; p=0.001).
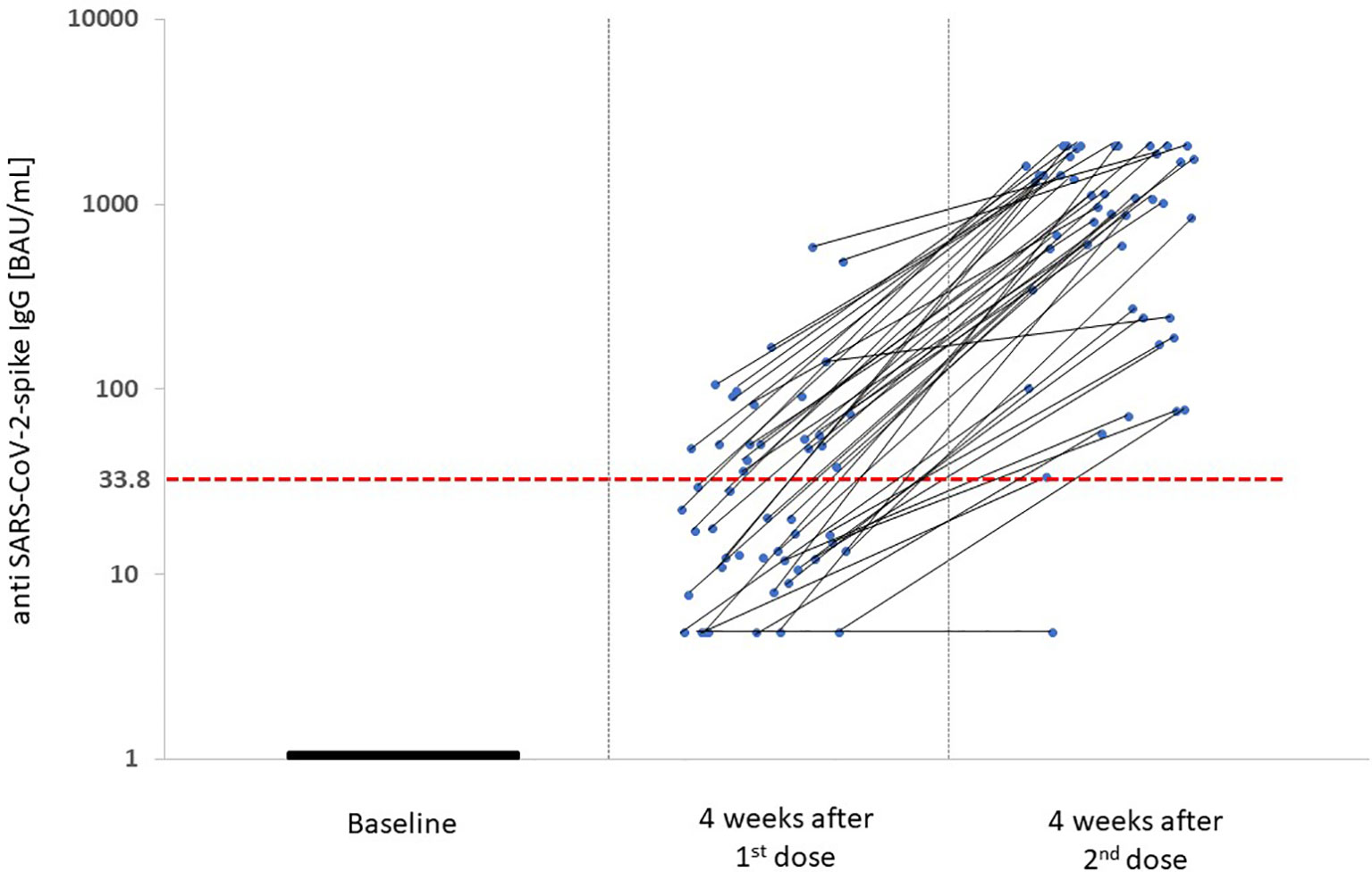
Figure 3 Anti-SARS-CoV-2-spike IgG concentration four weeks after both vaccine doses. Individual antibody kinetics after both vaccine doses are shown. Median (Q1, Q3) anti-SARS-CoV-2-spike IgG concentration four weeks after the 1st vaccine dose was 20.0 (11.7, 51.0) BAU/mL, four weeks after the 2nd vaccine dose 1075 (290.8, 1735.0) BAU/mL. The anti-SARS-CoV-2-spike IgG concentration is given in binding antibody units (BAU)/mL of the WHO International standard in log scale on the y-axis. The red dashed line presents the cut-off value for seropositivity in the Liaison® SARS-CoV-2-TrimericS IgG assay of 33.8 BAU/mL.

Table 2 Characteristics of patients with and without seroconversion after the 1st vaccine dose.
Patients who reported a local reaction after injection showed a numerically higher median (Q1, Q3) anti-SARS-CoV-2 spike IgG concentration after the complete vaccination course [1210 (751.3, 1817.5) vs 763 (201.5, 1705) BAU/mL], but this difference was not statistically significant (p=0.245). The antibody concentration four weeks after the second vaccine injection was significantly higher in patients with documented hepatitis B seroconversion at baseline and detectable anti-HBs antibodies after earlier active hepatitis B vaccination (1440 [961, 2080] BAU/mL, n=23) compared with hepatitis B vaccination non-responders (308.5 [176.8, 1622.5] BAU/mL, n=12; p=0.035). Hemodialysis patients with documented immunity after hepatitis B infection (positive anti-HBc antibodies) were excluded from this analysis. Immunosuppressed patients (n=9) developed lower antibody concentration (592 [64.1, 1210.0] BAU/mL] compared to patients without additional immunosuppression (n=39; 1130 [576.0, 1800.0] BAU/mL; p=0.046). In a multiple linear regression analysis (Table 3) higher age (β: -14.1, 95% CI: -28.0, -0.2; p=0.046) and immunosuppression (β: -560.4, 95% CI: -1100.2, -20.7; p=0.042) were associated with a lower antibody concentration after the second vaccine dose, whereas calcitriol treatment was associated with an increased immune response (β: 488.1, 95% CI: 885.0, 91.2; p=0.017).

Table 3 Baseline predictors of the antibody concentration four weeks after the 2nd vaccine dose.
During a follow-up of 90 days after the first vaccine dose only one patient was diagnosed with symptomatic SARS-CoV-2 infection. A 48-year-old woman was tested SARS-CoV-2 positive (PCR cycle threshold value 15.6) on the day of the second vaccination. She suffered from mild flu-like symptoms. At that time, she had already developed seroconversion after the first vaccine dose with an anti-SARS-CoV-2 spike IgG concentration of 49.7 BAU/mL. She did not receive the second vaccine dose and remained almost asymptomatic. One week later she had a PCR cycle threshold of 33.4. Four weeks after the diagnosis her anti-SARS-CoV-2 spike IgG concentration had increased to 2080 BAU/mL.
In our study, we present detailed data on the safety and immunogenicity of the mRNA-BNT162b2 SARS-CoV-2 vaccine in chronic hemodialysis patients. We found a good safety profile with a low rate of local and systemic side reactions and a high seroconversion rate of 97.9% in this cohort with a substantial antibody response after the complete vaccination course.
To our knowledge, no safety data of SARS-CoV-2 vaccines in hemodialysis patients have been published so far. Compared to the general population, a lower percentage of hemodialysis patients suffered from local reactions after the vaccine injections. In the pivotal trial with the same vaccine by Polack et al. (5), 70% to 80% of individuals reported local pain at the injection site, whereas approximately half as many patients in our study complained about this side effect. The participants´ age difference with an on average 15 years older cohort in our study may explain this finding, because an age-dependence with fewer local reactions in people aged >55 years compared with younger study participants has already been described in the general population (5). Importantly, no significant local hematoma occurred despite intramuscular injection during the hemodialysis session with full low-molecular weight heparin anticoagulation. Therefore, intramuscular vaccination in hemodialysis patients can be performed safely during the last 30 minutes of the hemodialysis treatment session. This enables sufficient observation after vaccination with adequate monitoring of vital signs, and no change in patients´ logistics and hemodialysis prescription is required. This approach is in accordance with the CDC general best practice guidelines for immunization in patients with bleeding disorders or taking warfarin in the general population (17).
Similarly, systemic reactions during the first week after the injection were found in only eight percent of the patients in our study, which is also less frequent than in the general population (5). Only 2.1% of patients reported severe muscle or joint pain, which were the only reactions that had numerically increased after the second injection compared to the first one. No patient reported a grade 4 local or systemic reaction requiring hospitalization. The incidence of local or systemic reactions in our study was also lower when compared to the second available mRNA vaccine mRNA-1273 (4).
Although the clinically meaningful antibody concentration cut-off value for definite seroprotection is unknown at present, the high seroconversion rate in our hemodialysis cohort is somehow surprising when compared to the response to other vaccines. After hepatitis B vaccination a seroconversion rate from 40% to 70% was detected in hemodialysis patients (8–11). Vaccination against the seasonal influenza and the 2009 pandemic influenza A virus H1N1 in hemodialysis patients resulted in seroconversion rates varying from 25% to 57% (18–22) with higher response rates using adjuvanted versus non-adjuvanted vaccines (23). In comparison to these findings, the strong immunogenicity with the mRNA-BNT162b2 SARS-CoV-2 vaccine found in our study is encouraging and hopefully translates into the prevention of clinically important outcomes such as severe COVID-19, hospitalization and death. Our results confirm the recently published high antibody response rates from 90% to 96% in three dialysis cohorts from Israel (24–26), and show a better vaccine response compared to 56 French SARS-CoV-2 infection-naïve hemodialysis patients (82%) (27). Vaccine safety data were reported in none of these studies. Nevertheless, the weak seroconversion rate of only 42% after the first vaccine dose in our study emphasizes that most of these vulnerable and high-risk patients are not protected after the first vaccine dose. Safety precautions and personal protective measures must be maintained at least until the second vaccine dose has been administered. Due to this delayed antibody response hemodialysis patients should be prioritized for rapid vaccination strategies, and the interval between first and second dose should not be extended.
The high rates of side reactions and good antibody responses with mRNA-based vaccines points to the possibility that they are more immunogenic compared to conventional vaccines. The mRNA vaccines have been shown to stimulate the production of neutralizing antibodies targeting the same epitopes in a manner similar to natural infection (28). In an attempt to explore a possible relationship between local reaction at the injection site and antibody response after the complete vaccination course, we determined the antibody concentration in patients with and without local reaction. Although patients who reported local pain had numerically higher concentrations than patients without, this difference did not reach statistical significance. Interestingly, patients with a documented seroconversion after prior active hepatitis vaccination with a second-generation recombinant hepatitis B vaccine had a significantly higher antibody response after the SARS-CoV-2 vaccination compared to non-responders. This finding supports the hypothesis that the vaccination response allows an integrated interpretation of the patients´ general immune competence. The fact that all but one hepatitis B vaccination non-responders seroconverted upon the mRNA-BNT162b2 SARS-CoV-2 vaccine points to a higher immunogenicity and efficacy of mRNA platform-based vaccines. Future mRNA-based hepatitis B vaccines may possibly lead to higher seroconversion rates in dialysis patients.
Age is a well-known key driver of vaccination response in hemodialysis patients with higher age being associated with a weaker antibody concentration as shown in the studies by Grupper at al (25). and Agur et al. (24), and substantiated in our study. Patients with seroconversion after the first vaccine dose were significantly younger than those without, and higher age was significantly associated with a lower antibody concentration four weeks after the complete vaccination course.
Active calcitriol treatment during vaccination was associated with a higher antibody concentration after the complete vaccination course. Most immune cells express vitamin D receptors (29). Additionally, dendritic cells, macrophages and monocytes convert the precursor 25(OH) vitamin D to active calcitriol using their own 1α-hydroxylase (30). Upon toll-like receptor-mediated activation and induced by increased calcitriol dendritic cells can migrate from the vaccination site to non-draining lymphoid organs, where they can stimulate antigen-specific T and B lymphocytes to produce a significant antibody response after vaccination (31, 32). Calcitriol stimulates the production of the Th2-like cytokines IL-4, IL-5, IL-10 and IL-13 supporting the humoral immune response (33–35).
Immunosuppressed patients had significantly lower anti-SARS-CoV-2 spike antibody concentrations, but still nearly all these patients (8/9) showed a seroconversion. Six out of these patients were treated with 5 mg prednisolone daily during the vaccination course, one patient with 5 mg prednisolone and 2 mg tacrolimus daily, one patient with 5 mg prednisolone and 150 mg azathioprine daily, and one patient had been treated with dexamethasone, bortezomib and thalidomide followed by autologous hematopoietic cell transplantation four months prior to vaccination and lenalidomide maintenance therapy during vaccination. The good response rate observed in immunosuppressed hemodialysis patients raises hope to a protective seroconversion with the mRNA-BNT162b2 SARS-CoV-2 vaccine in other patient groups with immunosuppression, although the response rate in patients with more profound immunosuppressive therapy, especially kidney transplant recipients has to be evaluated.
Certain limitations of our study must be acknowledged. The small cohort size is a limitation, but we included all patients consenting to vaccination in our centre without any selection criteria. Due to the uniform ethnic nature of our Caucasian hemodialysis cohort, we cannot generalize our findings to other ethnicities. Our results are limited to SARS-CoV-2 infection-naïve seronegative patients and the mRNA-BNT162b2 vaccine. Although neutralizing capacity cannot be directly derived from positive anti-SARS-CoV-2 spike IgG antibodies, the assay used in our study has a very good correlation with the microneutralization test. Furthermore, Speer et al. recently found positive anti-S1 IgG antibodies in 18% of 22 German hemodialysis patients (4/22) three weeks after the first vaccination, and in 82% (14/17) three weeks after the second vaccination using the mRNA BNT162b2 vaccine (36). The same number of patients had SARS-CoV-2 neutralizing antibodies (18% after 1st vaccination, 82% after 2nd vaccination), a finding which is in line with the assumption that IgG antibodies directed against the S1 spike protein and RBD correspond to virus neutralizing antibodies. We were unable to determine the cellular immune response to vaccination (37, 38). Furthermore, we did not perform regular PCR-based screening of asymptomatic patients during the four weeks between first and second vaccination. Therefore, we cannot exclude the possibility of a positive antibody response or amplification of the vaccination response caused by an asymptomatic SARS-CoV-2 infection. However, whenever a patient presented with equivocal symptoms, antigen- and PCR-based testing was applied. In the case of a positive test result, all fellow patients of the same dialysis shift were tested at each session for one week.
As a strength of our work, all patients were serologically proven SARS-CoV-2 negative prior to vaccination. Therefore, we can exclude a booster effect of vaccination after undetected asymptomatic infection. Moreover, we assessed the safety profile of the mRNA-BNT162b2 SARS-CoV-2 vaccine in detail in chronic hemodialysis patients. So far, vaccine safety data have been missing in this patient group. Our approach, similar to the one used in the pivotal trial by Polack et al. (5) to evaluate side effects enables the comparison to general population data.
Some open questions remain: How long do hemodialysis patients maintain a significant vaccine-induced antibody concentration? Keeping in mind the rapid antibody waning after hepatitis B or influenza vaccination, a booster dose, possibly virus variant-specific, may be necessary. Is there a seroprotective cut-off value and what is the vaccine efficacy concerning the most important clinical outcomes of prevention of (severe) COVID-19, COVID-19-related hospitalization and intensive care treatment and COVID-19-related mortality? Do SARS-CoV-2-variants escape the vaccine-induced immune response in hemodialysis patients?
In conclusion, the mRNA-BNT162b2 SARS-CoV-2 vaccine appears to be safe and well-tolerated in hemodialysis patients and shows a high immunogenicity in these patients. These data support the prioritization and rapid vaccination of this highly vulnerable patient cohort.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Ethics committee of the Innsbruck Medical University. The patients/participants provided their written informed consent to participate in this study.
BM, MB, HU, TW, and KL designed the study and revised the article. TD, JS, AA-N and HS-M collected and interpreted data and revised the article. EZ designed the study, analyzed and interpreted data, drafted and revised the article. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Hilbrands LB, Duivenvoorden R, Vart P, Franssen CFM, Hemmelder MH, Jager KJ, et al. COVID-19-Related Mortality in Kidney Transplant and Dialysis Patients: Results of the ERACODA Collaboration. Nephrol Dial Transplant (2020) 35(11):1973–83. doi: 10.1093/ndt/gfaa261
2. Jager KJ, Kramer A, Chesnaye NC, Couchoud C, Sanchez-Alvarez JE, Garneata L, et al. Results From the ERA-EDTA Registry Indicate a High Mortality Due to COVID-19 in Dialysis Patients and Kidney Transplant Recipients Across Europe. Kidney Int (2020) 98(6):1540–8. doi: 10.1016/j.kint.2020.09.006
3. Williamson EJ, Walker AJ, Bhaskaran K, Bacon S, Bates C, Morton CE, et al. Factors Associated With COVID-19-Related Death Using Opensafely. Nature (2020) 584(7821):430–6. doi: 10.1038/s41586-020-2521-4
4. Baden LR, El Sahly HM, Essink B, Kotloff K, Frey S, Novak R, et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N Engl J Med (2021) 384(5):403–16. doi: 10.1056/NEJMoa2035389
5. Polack FP, Thomas SJ, Kitchin N, Absalon J, Gurtman A, Lockhart S, et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N Engl J Med (2020) 383(27):2603–15. doi: 10.1056/NEJMoa2034577
6. Voysey M, Clemens SAC, Madhi SA, Weckx LY, Folegatti PM, Aley PK, et al. Safety and Efficacy of the ChAdOx1 nCoV-19 Vaccine (AZD1222) Against SARS-CoV-2: An Interim Analysis of Four Randomised Controlled Trials in Brazil, South Africa, and the UK. Lancet (2021) 397(10269):99–111. doi: 10.1016/S0140-6736(20)32661-1
7. Forbes S, Davari M, Gnanasampanthan S, Roth N, Young G, Rajakariar R, et al. Persistence of Antibody Response to SARS-CoV-2 in a Cohort of Haemodialysis Patients With COVID-19. Nephrol Dial Transplant (2021) gfab066. doi: 10.1093/ndt/gfab066
8. Buti M, Viladomiu L, Jardi R, Olmos A, Rodriguez JA, Bartolome J, et al. Long-Term Immunogenicity and Efficacy of Hepatitis B Vaccine in Hemodialysis Patients. Am J Nephrol (1992) 12(3):144–7. doi: 10.1159/000168436
9. Ghadiani MH, Besharati S, Mousavinasab N, Jalalzadeh M. Response Rates to HB Vaccine in CKD Stages 3-4 and Hemodialysis Patients. J Res Med Sci (2012) 17(6):527–33.
10. Stevens CE, Alter HJ, Taylor PE, Zang EA, Harley EJ, Szmuness W. Hepatitis B Vaccine in Patients Receiving Hemodialysis. Immunogenicity and Efficacy. N Engl J Med (1984) 311(8):496–501. doi: 10.1056/NEJM198408233110803
11. Zitt E, Sprenger-Mahr H, Knoll F, Neyer U, Lhotta K. Vitamin D Deficiency is Associated With Poor Response to Active Hepatitis B Immunisation in Patients With Chronic Kidney Disease. Vaccine (2012) 30(5):931–5. doi: 10.1016/j.vaccine.2011.11.086
12. Krueger KM, Ison MG, Ghossein C. Practical Guide to Vaccination in All Stages of CKD, Including Patients Treated by Dialysis or Kidney Transplantation. Am J Kidney Dis (2020) 75(3):417–25. doi: 10.1053/j.ajkd.2019.06.014
13. Saco TV, Strauss AT, Ledford DK. Hepatitis B Vaccine Nonresponders: Possible Mechanisms and Solutions. Ann Allergy Asthma Immunol (2018) 121(3):320–7. doi: 10.1016/j.anai.2018.03.017
14. Available at: https://www.sozialministerium.at/dam/jcr:d127a743-1047-46e8-8183-ae3ed06623e5/COVID-19_Priorisierung_Nationalen_Impfgremiums_Version_4.0_(Stand:31.03.2021)_Anlage_2.pdf (Accessed 31.03.2021).
15. Daugirdas JT. Second Generation Logarithmic Estimates of Single-Pool Variable Volume Kt/V: An Analysis of Error. J Am Soc Nephrol (1993) 4(5):1205–13. doi: 10.1681/ASN.V451205
16. von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Lancet (2007) 370(9596):1453–7. doi: 10.1016/S0140-6736(07)61602-X
17. Advisory Committee on Immunization Practices. General Best Practice Guidelines for Immunization: Best Practices Guidance of the Advisory Committee on Immunization Practices (ACIP) (2019). Available at: https://www.cdc.gov/vaccines/hcp/acip-recs/general-recs/special-situations.html (Accessed March 31, 2021).
18. Broeders NE, Hombrouck A, Lemy A, Wissing KM, Racape J, Gastaldello K, et al. Influenza A/H1N1 Vaccine in Patients Treated by Kidney Transplant or Dialysis: A Cohort Study. Clin J Am Soc Nephrol (2011) 6(11):2573–8. doi: 10.2215/CJN.04670511
19. Chang YT, Guo CY, Tsai MS, Cheng YY, Lin MT, Chen CH, et al. Poor Immune Response to a Standard Single Dose Non-Adjuvanted Vaccination Against 2009 Pandemic H1N1 Influenza Virus A in the Adult and Elder Hemodialysis Patients. Vaccine (2012) 30(33):5009–18. doi: 10.1016/j.vaccine.2012.05.016
20. Chang YT, Wang JR, Lin MT, Wu CJ, Tsai MS, Wen-Chi CL, et al. Changes of Immunogenic Profiles Between a Single Dose and One Booster Influenza Vaccination in Hemodialysis Patients - An 18-Week, Open-Label Trial. Sci Rep (2016) 6:20725. doi: 10.1038/srep20725
21. Crespo M, Collado S, Mir M, Cao H, Barbosa F, Serra C, et al. Efficacy of Influenza A H1N1/2009 Vaccine in Hemodialysis and Kidney Transplant Patients. Clin J Am Soc Nephrol (2011) 6(9):2208–14. doi: 10.2215/CJN.02160311
22. Lertdumrongluk P, Changsirikulchai S, Limkunakul C, Prachukthum P, Punpiput P, Buppanharun R, et al. Safety and Immunogenicity of a 2009 Influenza A (H1N1) Vaccine in Hemodialysis Patients. Vaccine (2012) 30(6):1108–14. doi: 10.1016/j.vaccine.2011.12.023
23. Noh JY, Song JY, Choi WS, Lee J, Seo YB, Kwon YJ, et al. Immunogenicity of Trivalent Influenza Vaccines in Patients With Chronic Kidney Disease Undergoing Hemodialysis: MF59-Adjuvanted Versus Non-Adjuvanted Vaccines. Hum Vaccin Immunother (2016) 12(11):2902–8. doi: 10.1080/21645515.2016.1191717
24. Agur T, Ben-Dor N, Goldman S, Lichtenberg S, Herman-Edelstein M, Yahav D, et al. Antibody Response to Mrna SARS-CoV-2 Vaccine Among Dialysis Patients - a Prospectivecohort Study. Nephrol Dial Transplant (2021) gfab155. doi: 10.1093/ndt/gfab155
25. Grupper A, Sharon N, Finn T, Cohen R, Israel M, Agbaria A, et al. Humoral Response to the Pfizer BNT162b2 Vaccine in Patients Undergoing Maintenance Hemodialysis. Clin J Am Soc Nephrol (2021) CJN.03500321. doi: 10.2215/CJN.03500321
26. Yanay NB, Freiman S, Shapira M, Wishahi S, Hamze M, Elhaj M, et al. Experience With SARS-COV-2 Bnt162b2 mRNA Vaccine in Dialysis Patients. Kidney Int (2021) 99(6):1496–8. doi: 10.1016/j.kint.2021.04.006
27. Attias P, Sakhi H, Rieu P, Soorkia A, Assayag D, Bouhroum S, et al. Antibody Response to BNT162b2 Vaccine in Maintenance Hemodialysis Patients. Kidney Int (2021) 99(6):1490–2. doi: 10.1016/j.kint.2021.04.009
28. Wang Z, Schmidt F, Weisblum Y, Muecksch F, Barnes CO, Finkin S, et al. mRNA Vaccine-Elicited Antibodies to SARS-CoV-2 and Circulating Variants. Nature (2021) 592(7855):616–22. doi: 10.1038/s41586-021-03324-6
29. Veldman CM, Cantorna MT, DeLuca HF. Expression of 1,25-Dihydroxyvitamin D(3) Receptor in the Immune System. Arch Biochem Biophys (2000) 374(2):334–8. doi: 10.1006/abbi.1999.1605
30. Liu PT, Stenger S, Li H, Wenzel L, Tan BH, Krutzik SR, et al. Toll-Like Receptor Triggering of a Vitamin D-Mediated Human Antimicrobial Response. Science (2006) 311(5768):1770–3. doi: 10.1126/science.1123933
31. Enioutina EY, Bareyan D, Daynes RA. TLR Ligands That Stimulate the Metabolism of Vitamin D3 in Activated Murine Dendritic Cells can Function as Effective Mucosal Adjuvants to Subcutaneously Administered Vaccines. Vaccine (2008) 26(5):601–13. doi: 10.1016/j.vaccine.2007
32. Enioutina EY, Bareyan D, Daynes RA. TLR-Induced Local Metabolism of Vitamin D3 Plays an Important Role in the Diversification of Adaptive Immune Responses. J Immunol (2009) 182(7):4296–305. doi: 10.4049/jimmunol.0804344
33. Boonstra A, Barrat FJ, Crain C, Heath VL, Savelkoul HF, O’Garra A. 1alpha,25-Dihydroxyvitamin D3 Has a Direct Effect on Naive CD4(+) T Cells to Enhance the Development of Th2 Cells. J Immunol (2001) 167(9):4974–80. doi: 10.4049/jimmunol.167.9.4974
34. Cippitelli M, Fionda C, Di Bona D, Di Rosa F, Lupo A, Piccoli M, et al. Negative Regulation of CD95 Ligand Gene Expression by Vitamin D3 in T Lymphocytes. J Immunol (2002) 168(3):1154–66. doi: 10.4049/jimmunol.168.3.1154
35. Romagnani S. T-Cell Subsets (Th1 Versus Th2). Ann Allergy Asthma Immunol (2000) 85(1):9–18. doi: 10.1016/S1081-1206(10)62426-X
36. Speer C, Goth D, Benning L, Buylaert M, Schaier M, Grenz J, et al. Early Humoral Responses of Hemodialysis Patients After COVID-19 Vaccination With BNT162b2. Clin J Am Soc Nephrol (2021) CJN.03700321. doi: 10.2215/CJN.03700321
37. Jeyanathan M, Afkhami S, Smaill F, Miller MS, Lichty BD, Xing Z. Immunological Considerations for COVID-19 Vaccine Strategies. Nat Rev Immunol (2020) 20(10):615–32. doi: 10.1038/s41577-020-00434-6
Keywords: BNT162b2, COVID-19, hemodialysis, mRNA vaccine, SARS-CoV-2
Citation: Zitt E, Davidovic T, Schimpf J, Abbassi-Nik A, Mutschlechner B, Ulmer H, Benda MA, Sprenger-Mähr H, Winder T and Lhotta K (2021) The Safety and Immunogenicity of the mRNA-BNT162b2 SARS-CoV-2 Vaccine in Hemodialysis Patients. Front. Immunol. 12:704773. doi: 10.3389/fimmu.2021.704773
Received: 03 May 2021; Accepted: 02 June 2021;
Published: 16 June 2021.
Edited by:
Anke Huckriede, University Medical Center Groningen, NetherlandsReviewed by:
David Hains, Riley Hospital for Children, United StatesCopyright © 2021 Zitt, Davidovic, Schimpf, Abbassi-Nik, Mutschlechner, Ulmer, Benda, Sprenger-Mähr, Winder and Lhotta. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Emanuel Zitt, ZW1hbnVlbC56aXR0QGxraGYuYXQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.