 Marta Crespo1,2*†
Marta Crespo1,2*† Laura Llinàs-Mallol1,2†Dolores Redondo-Pachón1,2Carrie Butler3,4Javier Gimeno2,5
Laura Llinàs-Mallol1,2†Dolores Redondo-Pachón1,2Carrie Butler3,4Javier Gimeno2,5 María José Pérez-Sáez1,2Carla Burballa1,2Anna Buxeda1,2Carlos Arias-Cabrales1,2Montserrat Folgueiras1,2
María José Pérez-Sáez1,2Carla Burballa1,2Anna Buxeda1,2Carlos Arias-Cabrales1,2Montserrat Folgueiras1,2 Sara Sanz-Ureña1,2
Sara Sanz-Ureña1,2 Nicole M. Valenzuela3,4
Nicole M. Valenzuela3,4 Elaine F. Reed3,4‡
Elaine F. Reed3,4‡ Julio Pascual1,2‡
Julio Pascual1,2‡- 1Department of Nephrology, Hospital del Mar, Barcelona, Spain
- 2Hospital del Mar Medical Research Institute (IMIM), Barcelona, Spain
- 3UCLA Immunogenetics Center, University of California Los Angeles, Los Angeles, CA, United States
- 4Department of Pathology and Laboratory Medicine, David Geffen School of Medicine, University of California Los Angeles, Los Angeles, CA, United States
- 5Department of Pathology, Hospital del Mar, Barcelona, Spain
Background: Correlation between antibody-mediated rejection (ABMR) and circulating HLA donor-specific antibodies (HLA-DSA) is strong but imperfect in kidney transplant (KT) recipients, raising the possibility of undetected HLA-DSA or non-HLA antibodies contributing to ABMR. Detailed evaluation of the degree of HLA matching together with the identification of non-HLA antibodies in KT may help to decipher the antibody involved.
Methods: We retrospectively assessed patients with transplant biopsies scored following Banff’15 classification. Pre- and post-transplant serum samples were checked for HLA and non-HLA antibodies [MICA-Ab, angiotensin-II type-1-receptor (AT1R)-Ab, endothelin-1 type-A-receptor (ETAR)-Ab and crossmatches with primary aortic endothelial cells (EC-XM)]. We also analyzed HLA epitope mismatches (HLA-EM) between donors and recipients to explore their role in ABMR histology (ABMRh) with and without HLA-DSA.
Results: One-hundred eighteen patients with normal histology (n = 19), ABMRh (n = 52) or IFTA (n = 47) were studied. ABMRh patients were HLA-DSApos (n = 38, 73%) or HLA-DSAneg (n = 14, 27%). Pre-transplant HLA-DSA and AT1R-Ab were more frequent in ABMRh compared with IFTA and normal histology cases (p = 0.006 and 0.003), without differences in other non-HLA antibodies. Only three ABMRhDSAneg cases showed non-HLA antibodies. ABMRhDSAneg and ABMRhDSApos cases showed similar biopsy changes and graft-survival. Both total class II and DRB1 HLA-EM were associated with ABMRhDSApos but not with ABMRhDSAneg. Multivariate analysis showed that pre-transplant HLA-DSA (OR: 3.69 [1.31–10.37], p = 0.013) and AT1R-Ab (OR: 5.47 [1.78–16.76], p = 0.003) were independent predictors of ABMRhDSApos.
Conclusions: In conclusion, pre-transplant AT1R-Ab is frequently found in ABMRhDSApos patients. However, AT1R-Ab, MICA-Ab, ETAR-Ab or EC-XM+ are rarely found among ABMRhDSAneg patients. Pre-transplant AT1R-Ab may act synergistically with preformed or de novo HLA-DSA to produce ABMRhDSApos but not ABMRhDSAneg. HLA epitope mismatch associates with ABMRhDSApos compared with ABMRhDSAneg, suggesting factors other than HLA are responsible for the damage.
Introduction
Correlation between the detection of HLA donor-specific antibodies (HLA-DSA) and antibody-mediated rejection (ABMR) is strong but imperfect in kidney transplant (KT) recipients (1–7). Not all patients with pre- or post-transplant HLA-DSA have ABMR damage in their biopsies (8). Different groups have tried to identify characteristics of HLA-DSA that may predict ABMR (9–12). There is also an active search for other invasive or non-invasive biomarkers for ABMR diagnosis (13–15). In the other hand, some patients have biopsies with histological findings suggestive of ABMR (ABMRh) without circulating HLA-DSA (16), generating the concept of the existence of ABMRhDSApos and ABMRhDSAneg cases. There is still limited literature describing the incidence of this type of ABMR without HLA-DSA, evaluating if these cases collectively show different clinical or histological characteristics or if non-HLA antibodies may explain the damage. Besides, controversial results in outcomes comparing ABMRhDSApos and ABMRhDSAneg cases have been reported (17, 18).
Based on the hypothesis that other antibodies may play a lead role in the case of ABMR histological damage with or without HLA-DSA, some groups have evaluated non-HLA antibodies in KT recipients (19, 20). Although first reports connecting non-HLA antibodies and graft outcomes were published in 2005 (19, 21), evidence is still weak and debated. Antibodies against specific alloantigens such as MICA (MICA-Ab) or MICB, or against autoantigens like angiotensin II type 1 receptor (AT1R-Ab), endothelin-1 type A receptor (ETAR-Ab), perlecan, agrin or vimentin, among others, have been reviewed recently (22). Some groups focused into the analysis of pathogenic antibodies directed against endothelial cells—which express some of those but also other antigens—with endothelial cell crossmatches (23–25). The increased evidence that the prevalence of non-HLA antibodies in KT recipients is high (26), together with the heterogeneous post-KT clinical course of patients included in these studies (25) hamper the correct identification of deleterious non-HLA antibodies. On the other hand, HLA epitope mismatch (HLA-EM) assessment has gained interest as an added immune monitoring tool to provide a more precise evaluation of HLA matching (27–29). HLA-EM has been previously associated with the development of de novo HLA-DSA (30) and ABMR (31). The clinical relevance of HLA-EM analysis remains under discussion and its application is not generalized yet.
Here, we systematically explored pre- and post-KT serum samples for HLA and different types of non-HLA antibodies: MICA-Ab, AT1R-Ab and ETAR-Ab, and other non-HLA antibodies performing crossmatches with primary aortic endothelial cells (EC-XM). Additionally, we evaluated pre-KT HLA-EM load. We focused on KT patients with biopsies with Banff category 2 diagnosis and compared them with two other Banff diagnosis: category 1 or no abnormalities (normal), as a usual control group, and category 5 or interstitial fibrosis and tubular atrophy (IFTA), damage with not clear pathogenicity to evaluate the potential role of non-HLA antibodies in this case (32).
Materials and Methods
Study Population and Design
Prospective observational study performed in KT patients active at our transplant program in Hospital del Mar. A total of 234 consecutive clinical and surveillance renal biopsies were performed in ABO compatible KT after a negative CDC crossmatch (February 2011–June 2015). Ninety-two biopsies fulfilling Banff 2015 categories 3, 4 and 6 were excluded and 142 biopsies achieving categories 1, 2 or 5 were selected. From these 142 biopsies, we selected only one biopsy per patient according to these criteria: the first biopsy obtained after 3 months post-transplantation, unless a biopsy with category 2 diagnosis was available. Five biopsies were excluded due to unsuitable serum samples. Finally, 118 biopsies corresponding to 118 patients were included in the study (Supplementary Figure 1). Demographical and clinical data were collected as previously described (33), and follow-up was done until graft-loss, death, 96 months post biopsy or July/2020. The study was approved by the Parc de Salut Mar Ethical Research Board (2010/3904/I) and all patients signed informed consents. All clinical and research activities reported are consistent with the Declarations of Istanbul and Helsinki.
Histological Scoring and Classification of the Biopsies
Biopsies were performed for indication or follow-up (including HLA-DSA detection without graft dysfunction). Processing was undertaken as previously described (33). All biopsies were scored by a pathologist following Banff 2015 classification and assigned to any of the six Banff categories (33). Category 2 included biopsies that met the first two Banff 2015–2019 criteria for ABMR histology, fulfilling the suspicious or full diagnosis of ABMR in Banff 2015 classification.
Sera Collection and Detection of HLA and Non-HLA Antibodies
One-hundred one available pre-KT and 118 post-KT serum samples collected contemporaneously to biopsies were retrospectively analyzed. HLA antibody testing (HLA-A, B, C, DRB and DQB) was performed as previously described (34) using Luminex HLA Single Antigen Bead assays (LABScreen, One Lambda, Canoga Park, CA). Antibodies against MICA antigens (*001, *002, *004, *007, *009, *012, *017, *018, *019, *027) were determined using LABScreen assay by Luminex Technology, according to the manufacturer’s specifications (One Lambda, CA). MICA-Ab were considered positive if mean fluorescence intensity >1,000. MICA typing for donors and recipients was not available. AT1R-Ab and ETAR-Ab were measured using enzyme-linked immunosorbent-based assays (35) (One Lambda, CA), diluted 1:100, tested in duplicate and read on an Epoch Microplate Spectrophotometer (Bio-Tek, Winooski, VT). Samples with AT1R-Ab or ETAR ≥10 U/ml were considered positive based on previous studies and our receiver operating curve analysis.
Endothelial Cell Crossmatches
Primary human aortic endothelial cells (ECs) were isolated from aortic rings of explanted donor hearts (36). EC were cultured in M199 medium supplemented with 20% (vol/vol) FBS, penicillin–streptomycin (100 U/ml and 100 ug/ml; Invitrogen Life Technologies), sodium pyruvate (1 mM), heparin (90 ug/ml; Sigma-Aldrich) and EC growth supplement (20 mcg/ml; Fisher Scientific). ECs from passages 7–8 were frozen and used in the EC-XM. Two different ECs (phenotyped as follows, donor CAR: HLA A2, A68, B60, B65; and donor Y126: HLA A1, A11, B35, B37) were employed avoiding for each KT recipient any HLA class I match with the kidney graft which could yield a reaction towards donor-specific HLA antigens. A total of 2 ×105 ECs were incubated 30 min with 100 ul patient serum on ice. ECs were washed three times and incubated with 50 mc of 1:400 diluted FITC-AffiniPure F(ab’)2 Fragment Goat Anti-Human IgG Fc fragment (Jackson ImmunoResearch Laboratories) for 30 min on ice. After three washes, cell fluorescence was analyzed on a FACSCalibur flow cytometer using CellQuest software (BD Biosciences). Gates for forward and side scatter measurements were set on EC, and a minimum of 10,000 events was acquired. Positive EC-XM threshold was set at two standard deviations (50 Median Channel Shift) above the mean of negative control serum tests. EC-XM were only performed in 83 pre and 103 post-KT cases due to insufficient sample.
HLA Epitope Mismatch Characterization
HLAMatchmaker software according to the July 2020 update (ABC and DRDQDP Eplet Matching Program V3.1, http://www.epitopes.net) was used to define potential HLA-EM between donors and recipients (37). High-resolution typing for all donors and recipients was performed or inferred using the HaploStats tool (www.haplostats.org) selecting the most likely high-resolution typing for HLA-A, B, C, DR and DQ according to three-five highest haplotype frequencies in the population of each one (Caucasian, African American, Asian or Hispanic).
Statistics
Data are presented as mean ( ± standard deviation), median, interquartile range, or number (percentage) based on data distribution. Comparisons between clinical variables were carried out using Student’s T test for parametric continuous variables and U Mann–Whitney or Kruskal–Wallis test for non-parametric data. Chi-squared or Fisher’s exact tests were used to test categorical variables. Survival analyses were performed using the Kaplan–Meier method using the log-rank test. Logistic regression analysis was used to estimate the odds ratio (OR) for ABMRhDSApos development. All variables with a p-value <0.10 in the univariate analysis were included in the multivariate analysis. Statistical analysis was performed using SPSS v.27.0 (IBM Corp., Armonk, NY, USA) and p-values <0.05 were considered statistically significant.
Results
Clinical Characteristics and Graft Survival
The selected 118 patients were grouped according to Banff diagnostic categories: category 1 or normal biopsy (n = 19), category 2 or ABMR histology (ABMRh, n = 52) and category 5 or IFTA (n = 47). Thirty patients (25.4%) lost their grafts and 13 died with a functioning graft (11%) during the study period. Death-censored graft survival 68 months after the biopsy [IQR 48–80] was worse in ABMRh cases than in those with IFTA or normal biopsies (Supplementary Figure 2). Baseline characteristics showed that normal histology patients were more frequently males, whereas ABMRh patients received grafts from younger donors and were more frequently retransplanted. ABMRh biopsies were less frequently surveillance biopsies and were performed later post-KT. At biopsy time, ABMRh patients had worse glomerular filtration rate (GFR) and higher proteinuria. Finally, IFTA patients were more frequently receiving calcineurin inhibitors and less on mTOR inhibitors (Table 1).
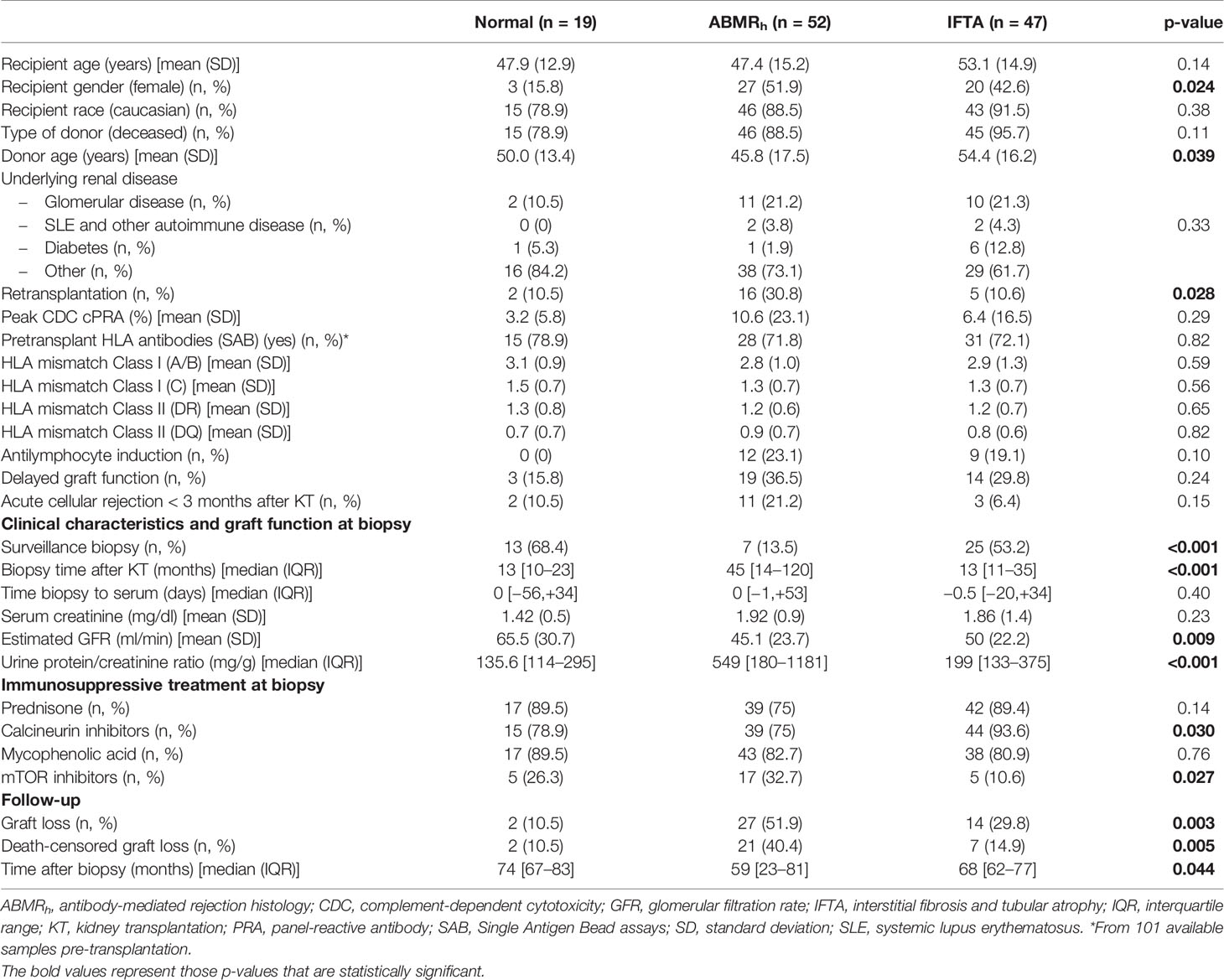
Table 1 Demographics and clinical characteristics of all included patients.
Pretransplant HLA-DSA and Non-HLA Antibodies
Pre-Transplant HLA-DSA
Pre-transplant serum samples were available for 101 patients (19 normal histology, 39 ABMRh and 43 IFTA). We found pre-transplant HLA-DSA in 18 ABMRh (46.2%), 9 IFTA (20.9%) and in two normal histology cases (10.5%) (p = 0.006) (Figure 1A). In ABMRh pre-transplant HLA-DSA were more frequently class I&II combined (38.9%, p = 0.087) and less isolated class I (27.8%).

Figure 1 Pre-transplant HLA and non-HLA antibodies. (A) HLA, AT1R-Ab, ETAR-Ab, MICA-Ab and EC-XM before transplantation in the three groups of study. (B) Pre-transplant AT1R-Ab positive and negative patients with preformed persistent HLA-DSA, preformed cleared HLA-DSA, de novo HLA-DSA or without HLA-DSA at any time. (C) Detection of pre-transplant HLA-DSA and/or AT1R-Ab in the three study groups. (D) Post-transplant HLA and non-HLA antibodies. HLA, AT1R-Ab, ETAR-Ab, MICA-Ab and EC-XM after transplantation in the three groups of study. ABMRh, antibody-mediated rejection histology; AT1R-Ab, antibodies against angiotensin II type 1 receptor; EC-XM, crossmatch with primary aortic endothelial cells; ETAR-Ab, antibodies against endothelin-1 type A receptor; IFTA, interstitial fibrosis and tubular atrophy; KT, kidney transplantation; MICA-Ab, antibodies against major histocompatibility complex class I related chain A. ns, non-significant.
Pre-Transplant AT1R-Ab
Pre-transplant AT1R-Ab strongly associated with ABMRh diagnosis (16/39 ABMRh (41%) vs. 2/19 normal histology (10.5%) and 5/43 IFTA (11.6%), p = 0.003) (Figure 1A). All 16 ABMRh patients with pre-transplant AT1R-Ab developed ABMRhDSApos, whereas no ABMRhDSAneg patient showed pre-transplant AT1R-Ab (p = 0.029). Detection of pre-transplant AT1R-Ab correlated with both persistent preformed HLA-DSA (12/23, 52%) and de novo HLA-DSA detection (8/18, 44%), but not with preformed HLA-DSA which cleared after transplant (1/6, 17%) or no HLA-DSA (2/54, 4%, p <0.001) (Figure 1B). The median MFI of preformed HLA-DSA coexistent with AT1R-Ab was not significantly different than preformed HLA-DSA without AT1R-Ab (8898 vs 2874, p = 0.083).
Other Non-HLA Antibodies
Neither pre-transplant ETAR-Ab nor MICA-Ab associated with ABMRh. Pre-transplant ETAR-Ab and MICA-Ab were present similarly in normal histology, ABMRh and IFTA cases (31.6, 25.6 and 18.6%, p = 0.51; 10.5, 7.7 and 9.3%, p = 1.00). Of 83 KT recipients tested with EC-XM, only 3/29 ABMRh (10.3%) and 3/39 IF/TA cases (7.7%) had a pre-transplant positive EC-XM (Figure 1A).
Pre-Transplant Combination of HLA-DSA and Non-HLA Antibodies
Detection of pre-transplant HLA-DSA and/or AT1R-Ab were highly associated with ABMRh compared with IFTA and normal biopsies (66.7 vs. 25.6 vs. 21%, p <0.001, Figure 1C). Nine ABMRh cases presented with simultaneous HLA-DSA and AT1R-Ab (23.1%), 17 with either HLA-DSA or AT1R-Ab (43.6%) and the remaining 13 did not present any of these antibodies (33.3%).
Post-Transplant HLA-DSA and Non-HLA Antibodies
Post-Transplant HLA-DSA
At the time of biopsy, HLA-DSA was detectable in 38/52 ABMRh patients [73.1%, 17 preformed (44.7%) and 21 de novo (55.3%)]. Among them, 7.7% were class I, 53.8% class II and 11.5% combined class I&II. HLA-DSA were also detected in 17% IFTA and 15.8% normal histology cases (Figure 1D).
Post-Transplant AT1R-Ab
Post-transplant AT1R-Ab showed no association with ABMRh (23.1% in ABMRh vs. 26.3% in normal histology and 27.7% in IFTA cases, p = 0.85, Figure 1D). Detection of post-transplant AT1R-Ab did not correlate with the detection of HLA-DSA [15/49 HLA-DSApos cases had AT1R-Ab at biopsy (30.6%) vs. 15/69 HLA-DSAneg cases (21.7%), p = 0.28].
Other Non-HLA Antibodies
Neither post-transplant ETAR-Ab nor MICA-Ab was related with ABMRh. Post-transplant ETAR-Ab were found in 3/19 normal histology (15.8%), 7/52 ABMRh (13.5%) and 9/47 IFTA cases (19.1%, p = 0.80). MICA-Ab were detectable in 1/19 normal histology (5.3%), 8/52 ABMRh (15.4%) and 6/47 IFTA cases (12.8%, p = 0.62). Two normal histology (11.1%), four ABMRh (9.3%) and two IFTA cases (4.8%) had a positive EC-XM (p = 0.70, Figure 1D).
Patients With ABMRh With and Without HLA-DSA
From 52 patients with ABMRh 14 (26.9%) had no peri-biopsy HLA-DSA. ABMRhDSApos cases were more frequently HLA sensitized, less well DR-matched with their donors and received more frequently a graft from a deceased donor than those ABMRhDSAneg. No differences were found in graft function or immunosuppression at biopsy (Table 2). Patients showed similar microvascular inflammation, but diffuse C4d was more frequent in ABMRhDSApos cases (27% vs 0%, p = 0.07, Table 2). Graft survival was similar between both groups (Figure 2). We assessed pre- and post-transplant non-HLA antibodies in ABMRhDSAneg cases. Of 7 cases with pre-transplant sample, two had EC-XM+ but none showed MICA-Ab, AT1R-Ab or ETAR-Ab (Table 3A). After KT, one had coexistent MICA-Ab, AT1R-Ab and ETAR-Ab; one had MICA-Ab and a third one AT1R-Ab (Supplementary Table 1A). In 9/14 ABMRhDSAneg patients (64.3%) we could not identify any of the non-HLA antibodies studied.
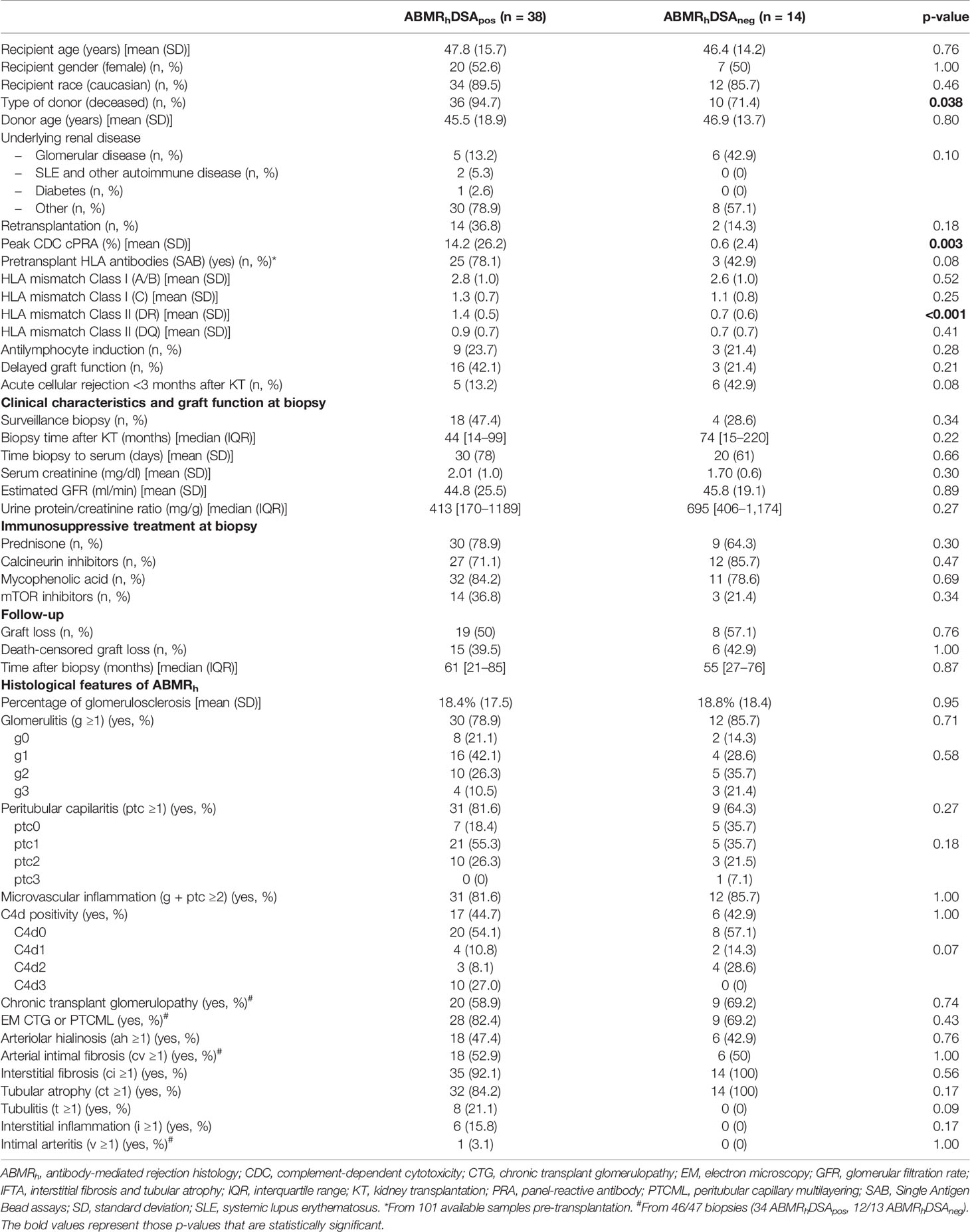
Table 2 Characteristics of patients with and without HLA-DSA.
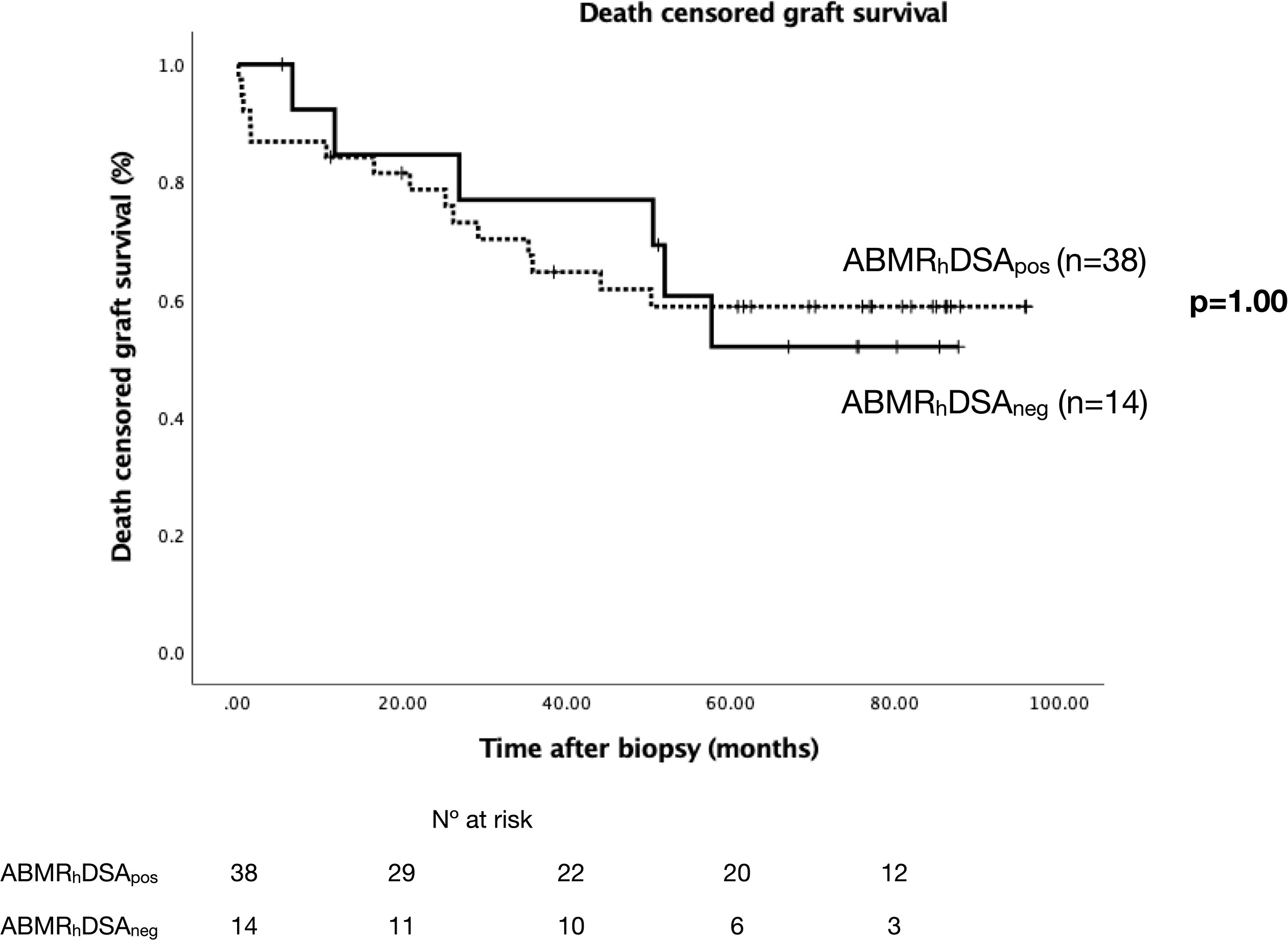
Figure 2 Death censored graft survival in ABMRh patients with and without HLA-DSA. Kaplan–Meier survival curves representing death censored graft survival. ABMRh, antibody-mediated rejection histology; DSA, donor-specific antibodies.

Table 3A Comparison of pre-transplant non-HLA antibodies between ABMRhDSApos and ABMRhDSAneg cases.
HLA Epitope Mismatch Characterization
The median number of class I and class II HLA-EM in our cohort were 16 (0–36) and 18 (0–46) respectively. Among them, 10 class I and 7 class II HLA-EM were antibody-verified (HLA-EMver). We observed similar class I and class II HLA-EMver in all three groups of study (data not shown). We compared the load of HLA-EMver between ABMRhDSApos and ABMRhDSAneg patients, finding similar class I but significantly higher class II and DRB HLA-EMver in ABMRhDSApos cases (8 vs 4.5, p = 0.046; 5 vs. 0.5, p = 0.044, Figure 3). We compared HLA-EM and HLA antigen mismatch (HLA-AM) for de novo DSA (dnDSA) development prediction. Neither class I HLA-EMver nor HLA-AM were useful tools for class I dnDSA prediction. Class II HLA-EMver were significantly associated with class II dnDSA (8 vs. 7, p = 0.031), but not class II HLA-AM (p = 0.26). The extent of DRB HLA-EMver associated with DRB dnDSA (6 vs. 4, p = 0.024), and the rate of DQB HLA-EMver showed a weak association with DQB dnDSA (4 vs. 2, p = 0.077). Neither DRB nor DQB HLA-AM predicted DRB or DQB dnDSA (p = 0.27, p = 0.21).
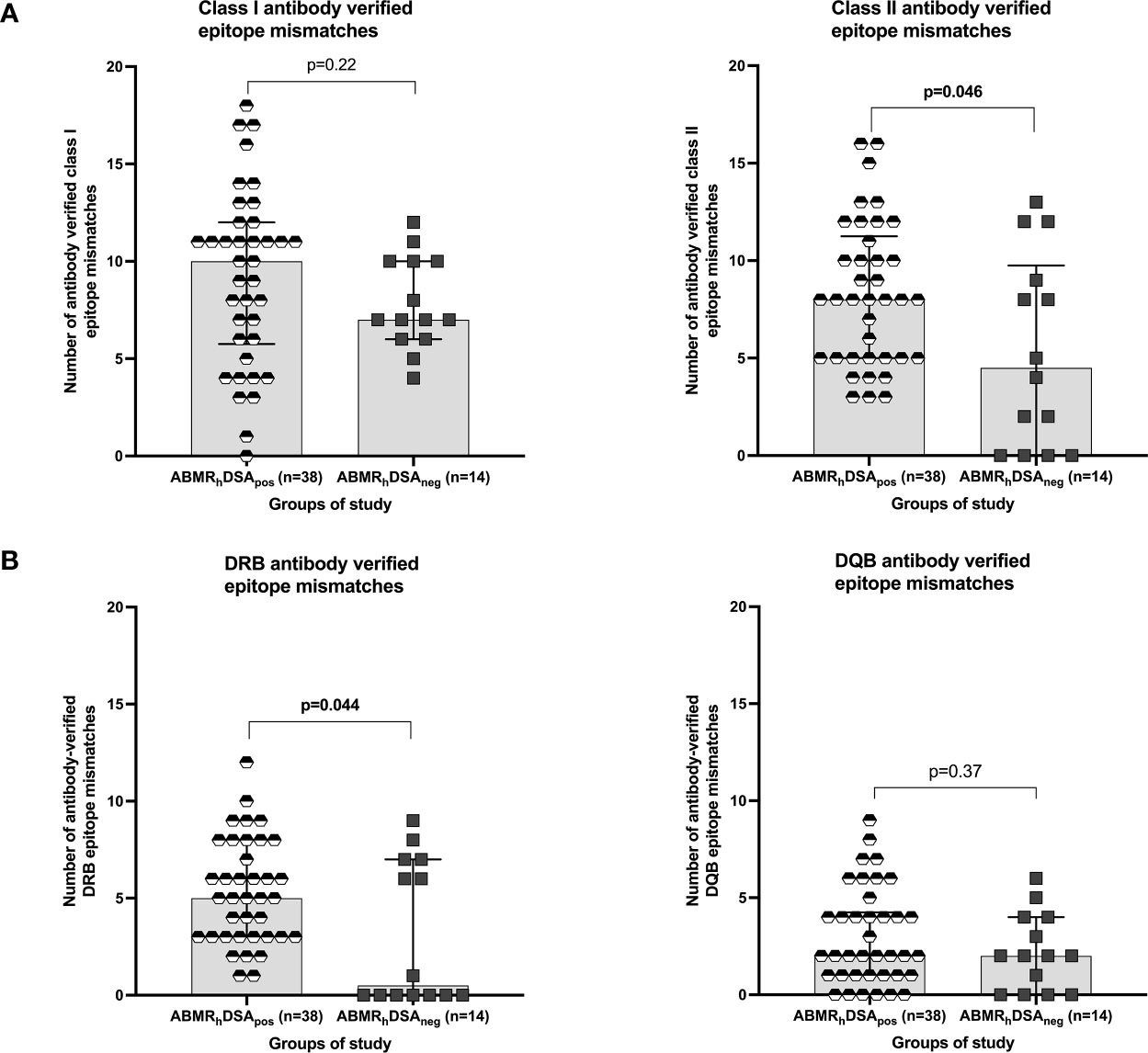
Figure 3 HLA epitope mismatch analysis in ABMRhDSApos and ABMRhDSAneg cases. (A) Number of antibody-verified class I and class II epitope mismatches and (B) Number of antibody-verified DRB and DQB epitope mismatches in ABMRhDSApos (black and white hexagons) and ABMRhDSAneg (black squares) cases. All plots show median and interquartile range (IQR).
Risk Factors for Post-Transplant ABMRhDSApos Development
ABMRhDSApos patients showed higher rates of pre-transplant HLA-DSA and AT1R-Ab (p <0.001, Table 3B), but regarding post-transplant antibodies, only HLA-DSA was associated with ABMRhDSApos (p <0.001, Supplementary Table 1B). In order to assess the role of each factor, we adjusted a multivariate model which showed that both pre-transplant HLA-DSA (OR: 3.69 [1.31–10.37], p = 0.013) and AT1R-Ab (OR: 5.47 [1.78–16.76], p = 0.003) were independent ABMRhDSApos predictors. DRB HLA-EMver also showed a weak association with ABMRhDSApos (p = 0.071, Table 4).

Table 3B Pre-transplant HLA and non-HLA antibodies: comparison between ABMRhDSApos and non-ABMRhDSApos cases (normal histology, IFTA and ABMRhDSAneg cases).
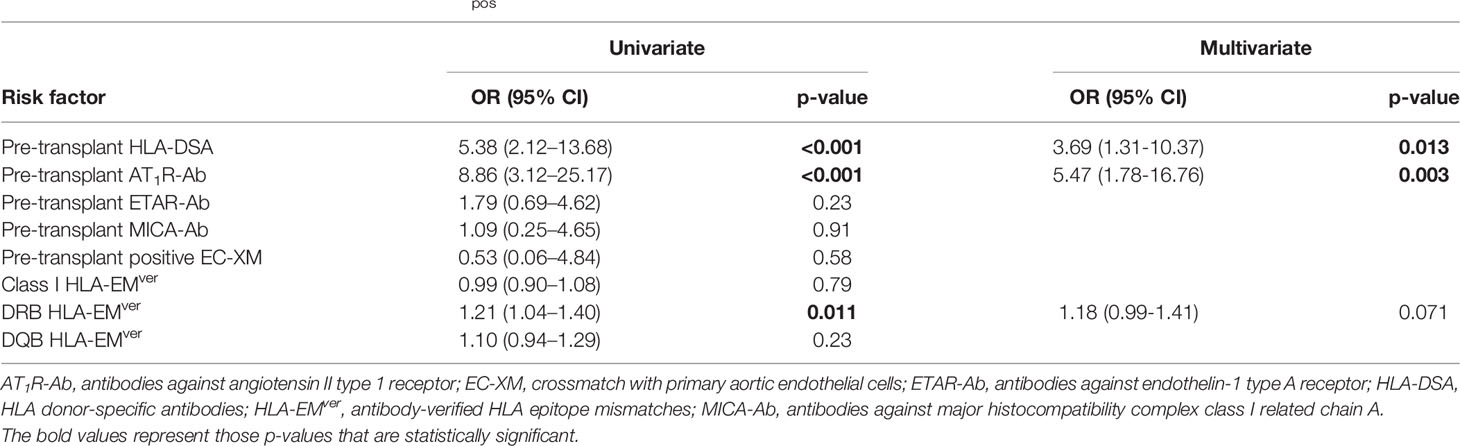
Table 4 Logistic regression analysis of ABMRhDSApos risk factors.
Discussion
We report here that ABMR damage in KT recipients occurs in a significant proportion of cases without the detection of HLA-DSA at biopsy. We have evaluated the role of non-HLA antibodies, such as AT1R-Ab, ETAR-Ab, MICA-Ab or anti-EC antibodies detected with crossmatches and found they could not explain ABMRhDSAneg. Our results suggest a synergistic interaction between pre-transplant AT1R-Ab and HLA-DSA to produce ABMRhDSApos or facilitate de novo appearance of HLA-DSA, but not to induce ABMRhDSAneg. Interestingly, it appears more strongly associated with ABMRh than incompatibility evaluated through HLA-EM analysis.
The relationship between ABMRh and HLA-DSA has been described in KT recipients for over 20 years (1, 2). However, there is increased evidence that ABMR compatible histological lesions may be present in the graft without detectable circulating HLA-DSA (18, 38). Up to 27% of our ABMRh patients did not show circulating HLA-DSA at the time of biopsy. This could be attributed to the inability of current techniques to detect these HLA antibodies or due to the participation of a different set of antibodies in graft damage. ABMRhDSAneg patients presented significantly lower class II and DRB HLA-EM compared with ABMRhDSApos cases. This finding strengthens the hypothesis of the participation of other mechanisms of damage in these cases rather than non-detected HLA-DSA. However, neither AT1R-Ab, ETAR-Ab, MICA-Ab nor antibodies identified with EC-XM before or after KT were able to explain the ABMRhDSAneg cases in our study. We describe here that ABMRh patients without HLA-DSA showed similar graft function, immunosuppressive treatment, histological features at biopsy and graft survival at the end of follow-up compared with ABMRhDSApos cases. Like us, Sablik et al. (17) reported a similar histological phenotype in ABMRhDSApos and ABMRhDSAneg patients, but a larger study by Senev et al. (18) found that ABMRhDSApos biopsies were more frequently C4d positive compared with ABMRhDSAneg cases, as the unique histological difference between the groups. In our series, although C4d positivity was similar between both groups, C4d intensity was higher in the ABMRhDSApos group. In our cohort, graft survival was similar between both groups, in agreement with results reported by Sablik et al. (17) but in contrast with the study from Senev et al. (18), which included mostly active ABMR cases without chronicity, unlike our cohort.
KT recipients may produce immune responses through indirect recognition against foreign proteins or even against own proteins expressed by the donor graft acting as autoantigens due to different factors that induce graft damage during the transplant process. These antibodies may then react against polymorphic alloantigens, like HLA related MICA or MICB, or against autoantigens like AT1R, ETAR, agrin, vimentin, perlecan, K-tubulin, etc. (39–41) which may be prevalent in KT recipients. Some of these autoantibodies and new ones recently validated (42) have not been evaluated in our cohort yet. They might explain some ABMRhDSAneg cases. Some groups have evaluated the relationship between antibodies directed against ECs—the barrier between donor and recipient—and graft survival (43), and exploratory studies have employed array techniques in limited series with antibodies against ECs validating potential target proteins with ELISA (44, 45). Jackson and col. were able to identify four antigenic targets expressed on ECs in nine patients with ABMRhDSAneg (44). They found that antibodies against these proteins in pre-transplant sera predicted ABMRhDSApos. In our cohort, of seven ABMRhDSAneg cases with pre-transplant samples, two had a positive EC-XM+, but none showed MICA-Ab, AT1R-Ab or ETAR-Ab. In line with our results, a recent report from Delville et al. (23) found that only 26% of patients with early acute ABMRhDSAneg had pre-transplant AT1R-Ab using our same threshold of 10 UI/ml. Moreover, MICA-Ab were only detected in two of these ABMRhDSAneg cases. However, these cases had preformed IgG antibodies against constitutively expressed antigens of microvascular glomerular cells (23). Of note, our two cases with pre-transplant EC-XM+ developed ABMRh within the first 12 months of KT, while the other twelve developed ABMRh later on. Unlike Lefaucheur et al. (46), despite employing the same threshold for AT1R antibodies, the presence of these antibodies in our ABMRhDSAneg cohort is negligible. Nevertheless, our overall prevalence of 25% in post-transplant AT1R-Ab is not different from theirs. Unfortunately, these authors do not analyze the relation between pre-transplant AT1R-Ab and ABMR.
We report here a strong and independent association between pre-transplant AT1R-Ab and ABMRhDSApos development. AT1R can be found in several cell types such as vascular endothelial cells and binds to angiotensin II (39, 47). First report linking AT1R-Ab and kidney allograft rejection suggested a potential relationship between AT1R agonistic antibodies and vascular injury (19, 39). Subsequently, pre- or post-transplant AT1R-Ab detection have been linked to both rejection and allograft failure (19, 48). Philogene et al. (24) described higher post-transplant AT1R-Ab levels in patients with ABMR compared with patients with cellular rejection or those without rejection, however, they provided no data regarding pre-transplant AT1R-Ab. In another report (49), pre- and post-transplant AT1R-Ab were strongly associated with biopsy-proven rejection, not specifically ABMR. Some reports suggest that non-HLA and HLA-DSA antibodies may function in synergy (24, 49). Taniguchi et al. (49) reported lower graft survival mainly in the presence of de novo AT1R-Ab and HLA-DSA at biopsy with lesions compared with those cases with HLA-DSA alone. Here we show a strong association of pre-transplant AT1R-Ab with post-transplant HLA-DSA, either persistent preformed or de novo, and with ABMRhDSApos development. This association may be of utmost importance for KT outcomes. We previously reported the strong association among persistent preformed HLA-DSA and lower ABMR free survival, only surpassed by the development of de novo HLA-DSA (34). Moreover, here we show that all 16 ABMRh patients with pre-transplant AT1R-Ab had HLA-DSA at biopsy, nine of them maintained the preformed HLA-DSA and seven developed de novo HLA-DSA. We found no association between pre-transplant AT1R-Ab and graft survival, in line with other reports (26, 49). In our multivariate analysis, pre-transplant HLA-DSA and AT1R-Ab were independent predictors for ABMRh. Our study may not be powered enough to assess the relationship between AT1R-Ab and graft loss. Given the strong and already known association between ABMR and increased risk of kidney allograft loss (34, 50–52), our data supports that pre-transplant AT1R-Ab assessment should be carefully considered in KT candidates.
In the last years, HLA-EM analysis has been proposed as a better strategy to prevent HLA-DSA development than antigen matching (29). Here we confirm that class II and DRB dnDSA development may be predicted with HLA-EM, as previously reported (30), however, only a weak association was observed with DQB dnDSA, probably due to the limited number of cases included. Interestingly, neither class II, DRB or DQB HLA-AM were able to predict dnDSA. As mentioned, the detection of lower number of class II and DRB HLA-EM in ABMRhDSAneg cases may contradict the idea of undetected HLA-DSA responsible for the damage. Class II and DRB HLA-EM associated with ABMRhDSApos, although the existence of preformed HLA-DSA or AT1R-Ab are more potent predictors of ABMRhDSApos in our experience. In our study, ABMRhDSAneg could not be explained by higher HLA-EM or by the non-HLA antibodies evaluated. Interestingly, an alternative mechanism to produce ABMRh termed “the missing-self hypothesis” has been proposed. According to it, the inability of graft EC to provide HLA I-mediated inhibitory signals to recipient circulating NK cells may trigger NK cell activation, resulting in endothelial damage and chronic vascular rejection (53).
The main limitation of our study is the restricted number of ABMRhDSAneg cases in the whole cohort. In order to further increase its number and the significance of the study, a multicenter trial is advisable. Besides, it is based on a mix of indication and surveillance biopsies which introduces heterogeneity in the timing and clinical picture of patients. Of note, EC-XM were performed with aortic cells which may not express the same proteins as a renal EC. Last, another limitation may be the use of inferred four-digit HLA typing for HLA-EM analysis. Despite careful estimation of second field HLA typing, we cannot rule out the possibility that some rare HLA genotypes are not correctly assigned, as recently suggested (54). However, ours is a large well characterized cohort of KT recipients, reflecting clinical practice, with thorough analysis of biopsies, including electron microscopy, crucial to detect some cases of ABMRh and with systematical study of HLA-DSA and a known set of non-HLA antibodies.
In summary, although the majority of patients with HLA-DSA at the time of biopsy show ABMRh, almost 30% of ABMRh patients did not show evidence of circulating HLA-DSA. These patients were more frequently HLA unsensitized pretransplant and less HLA matched but did not show other specific characteristics at transplantation or at biopsy. Neither AT1R-Ab, ETAR-Ab, MICA-Ab nor antibodies identified with EC-XM before or after KT were able to explain ABMRhDSAneg cases. Importantly AT1R-Ab with or without HLA-DSA before KT clearly increased the risk of ABMRhDSApos, suggesting it should be included in the pre-transplant immune assessment together with HLA-DSA.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by the Parc de Salut Mar Ethical Research Board. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
MC designed the study, coordinated logistics, analyzed the results, and drafted the manuscript. LL-M analyzed the results and drafted the manuscript. DR-P analyzed the results and revised the manuscript. CBut coordinated lab procedures and revised the manuscript. JG contributed with the assessment of the graft biopsies. MP-S, CBur, AB, CA-C, and SS-U revised the manuscript. MF coordinated sample drawing and storage. NV supervised HLA and non-HLA antibody interpretation. ER and JP evaluated the design of the study and revised the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This study was performed with funding from projects PI13/00598, PI16/00617, and PI20/00090 (Spanish Ministry of Health ISCIII FIS-FEDER); RD16/0009/0013 (ISCIII FEDER REDinREN) and 201822-10 (Fundació la Marató de TV3). MC received grants of the Sociedad Española de Nefrología and Parc de Salut Mar for a research stay at UCLA Immunogenetics Center (Los Angeles, USA). ER is supported by National Institute of Allergy and Infectious Diseases Grants RO1 AI135201. One Lambda provided reagents but had no role in the design of the study or the analyses and writing of the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We are indebted to Anna Faura, Rosa Causadias and Anna Bach for their assistance with patients. We thank Duska Dragun for her personal encouragement to perform the study the way it is. We also extend our gratitude to the staff of the UCLA Immunogenetics Center for technical assistance with non-HLA antibody tests and EC-XM. Finally, the authors hereby express their thanks to the organ donors and their families for giving the gift of life and, together with the recipients, the gift of knowledge. LL-M did this study as part of her doctoral thesis program at the Department of Medicine from the Universitat Autonoma of Barcelona (UAB).
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2021.703457/full#supplementary-material
Abbreviations
ABMR, antibody-mediated rejection; ABMRh, antibody-mediated rejection histology; ABMRhDSApos, antibody-mediated rejection histology with HLA-DSA; ABMRhDSAneg, antibody-mediated rejection histology without HLA-DSA; AT1R-Ab, antibodies against angiotensin II type 1 receptor; CDC, complement-dependent cytotoxicity; CTG, chronic transplant glomerulopathy; ECs, primary human aortic endothelial cells; EC-XM, crossmatch with primary human aortic endothelial cells; EM, electron microscopy; ETAR-Ab, antibodies against endothelin-1 type A receptor; GFR, glomerular filtration rate; HLA-DSA, HLA donor-specific antibodies; HLA-AM, HLA antigen mismatches; HLA-EM, HLA epitope mismatches; IFTA, interstitial fibrosis and tubular atrophy; IQR, interquartile range; KT, kidney transplant; MICA-Ab, antibodies against major histocompatibility complex class I related chain A; PRA, panel-reactive antibody; PTCML, peritubular capillary multilayering; SAB, Single Antigen Bead assays; SD, standard deviation.
References
1. Crespo M, Pascual M, Tolkoff-Rubin N, Mauiyyedi S, Bernard Collins A, Fitzpatrick D, et al. Acute Humoral Rejection in Renal Allograft Recipients: I. Incidence, Serology and Clinical Characteristics. Transplantation (2001) 71(5):652–8. doi: 10.1097/00007890-200103150-00013
2. Terasaki PI, Ozawa M. Predicting Kidney Graft Failure by HLA Antibodies: A Prospective Trial. Am J Transplant (2004) 4:438–43. doi: 10.1111/j.1600-6143.2004.00360.x
3. Djamali A, Kaufman DB, Ellis TM, Zhong W, Matas A, Samaniego M. Diagnosis and Management of Antibody-Mediated Rejection: Current Status and Novel Approaches. Am J Transplant (2014) 14:255–71. doi: 10.1111/ajt.12589
4. Lefaucheur C, Viglietti D, Mangiola M, Loupy A, Zeevi A. From Humoral Theory to Performant Risk Stratification in Kidney Transplantation. J Immunol Res (2017) 2017:10–8. doi: 10.1155/2017/5201098
5. Viglietti D, Loupy A, Vernerey D, Bentlejewski C, Gosset C, Aubert O, et al. Value of Donor-Specific Anti-HLA Antibody Monitoring and Characterization for Risk Stratification of Kidney Allograft Loss. J Am Soc Nephrol (2017) 28:702–15. doi: 10.1681/ASN.2016030368
6. Wiebe C, Gibson IW, Blydt-Hansen TD, Karpinski M, Ho J, Storsley LJ, et al. Evolution and Clinical Pathologic Correlations of De Novo Donor-Specific HLA Antibody Post Kidney Transplant. Am J Transplant (2012) 12:1157–67. doi: 10.1111/j.1600-6143.2012.04013.x
7. Eskandary F, Bond G, Kozakowski N, Regele H, Marinova L, Wahrmann M, et al. Diagnostic Contribution of Donor-Specific Antibody Characteristics to Uncover Late Silent Antibody-Mediated Rejection-Results of a Cross-Sectional Screening Study. Transplantation (2017) 101(3):631–41. doi: 10.1097/TP.0000000000001195
8. Schinstock CA, Cosio F, Cheungpasitporn W, Dadhania DM, Everly MJ, Samaniego-Picota MD, et al. The Value of Protocol Biopsies to Identify Patients With De Novo Donor-Specific Antibody at High Risk for Allograft Loss. Am J Transplant (2017) 17(6):1574–84. doi: 10.1111/ajt.14161
9. Crespo M, Torio A, Mas V, Redondo D, Perez-Saez MJ, Mir M, et al. Clinical Relevance of Pretransplant Anti-HLA Donor-Specific Antibodies: Does C1q-Fixation Matter? Transpl Immunol (2013) 29:28–33. doi: 10.1016/j.trim.2013.07.002
10. Loupy A, Lefaucheur C, Vernerey D, Prugger C, Duong van Huyen JP, Mooney N, et al. Complement-Binding Anti-HLA Antibodies and Kidney-Allograft Survival. N Engl J Med (2013) 369(13):1215–26. doi: 10.1056/NEJMoa1302506
11. Sicard A, Ducreux S, Rabeyrin M, Couzi L, McGregor B, Badet L, et al. Detection of C3d-Binding Donor-Specific Anti-HLA Antibodies at Diagnosis of Humoral Rejection Predicts Renal Graft Loss. J Am Soc Nephrol (2015) 26:457–67. doi: 10.1681/ASN.2013101144
12. Lefaucheur C, Viglietti D, Bentlejewski C, Duong van Huyen JP, Vernerey D, Aubert O, et al. IgG Donor-Specific Anti-Human HLA Antibody Subclasses and Kidney Allograft Antibody-Mediated Injury. J Am Soc Nephrol (2016) 27:293–304. doi: 10.1681/ASN.2014111120
13. Crespo M, Yelamos J, Redondo D, Muntasell A, Perez-Saez MJ, Lopez-Montanes M, et al. Circulating NK-Cell Subsets in Renal Allograft Recipients With Anti-HLA Donor-Specific Antibodies. Am J Transplant (2015) 15:806–14. doi: 10.1111/ajt.13010
14. Hidalgo LG, Sis B, Sellares J, Campbell PM, Mengel M, Einecke G, et al. NK Cell Transcripts and NK Cells in Kidney Biopsies From Patients With Donor-Specific Antibodies: Evidence for NK Cell Involvement in Antibody-Mediated Rejection. Am J Transplant (2010) 10:1812–22. doi: 10.1111/j.1600-6143.2010.03201.x
15. Gupta A, Broin PO, Bao Y, Pullman J, Kamal L, Ajaimy M, et al. Clinical and Molecular Significance of Microvascular Inflammation in Transplant Kidney Biopsies. Kidney Int (2016) 89:217–25. doi: 10.1038/ki.2015.276
16. Haas M, Sis B, Racusen LC, Solez K, Glotz D, Colvin RB, et al. Banff 2013 Meeting Report: Inclusion of C4d-Negative Antibody-Mediated Rejection and Antibody-Associated Arterial Lesions. Am J Transplant (2014) 14:272–83. doi: 10.1111/ajt.12590
17. Sablik KA, Clahsen-van Groningen MC, Looman CWN, Damman J, Roelen DL, van Agteren M, et al. Chronic-Active Antibody-Mediated Rejection With or Without Donor-Specific Antibodies has Similar Histomorphology and Clinical Outcome - A Retrospective Study. Transpl Int (2018) 31:900–8. doi: 10.1111/tri.13154
18. Senev A, Coemans M, Lerut E, Van Sandt V, Daniels L, Kuypers D, et al. Histological Picture of Antibody-Mediated Rejection Without Donor-Specific Anti-HLA Antibodies: Clinical Presentation and Implications for Outcome. Am J Transplant (2019) 19:763–80. doi: 10.1111/ajt.15074
19. Dragun D, Müller DN, Bräsen JH, Fritsche L, Nieminen-Kelhä M, Dechend R, et al. Angiotensin II Type 1-Receptor Activating Antibodies in Renal-Allograft Rejection. N Engl J Med (2005) 352(6):558–69. doi: 10.1056/NEJMoa035717
20. Reinsmoen NL, Lai CH, Heidecke H, Haas M, Cao K, Ong G, et al. Anti-Angiotensin Type 1 Receptor Antibodies Associated With Antibody Mediated Rejection in Donor HLA Antibody Negative Patients. Transplantation (2010) 90(12):1473–7. doi: 10.1097/TP.0b013e3181fd97f1
21. Opelz G. Non-HLA Transplantation Immunity Revealed by Lymphocytotoxic Antibodies. Lancet (2005) 365:1570–6. doi: 10.1016/S0140-6736(05)66458-6
22. Delville M, Charreau B, Rabant M, Legendre C, Anglicheau D. Pathogenesis of Non-HLA Antibodies in Solid Organ Transplantation: Where Do We Stand? Hum Immunol (2016) 77:1055–62. doi: 10.1016/j.humimm.2016.05.021
23. Delville M, Lamarthee B, Pagie S, See SB, Rabant M, Burger C, et al. Early Acute Microvascular Kidney Transplant Rejection in the Absence of Anti-HLA Antibodies Is Associated With Preformed IgG Antibodies Against Diverse Glomerular Endothelial Cell Antigen. J Am Soc Nephrol (2019) 30:692–709. doi: 10.1681/ASN.2018080868
24. Philogene MC, Bagnasco S, Kraus ES, Montgomery RA, Dragun D, Leffell MS, et al. Anti-Angiotensin II Type 1 Receptor and Anti-Endothelial Cell Antibodies: A Cross-Sectional Analysis of Pathological Findings in Allograft Biopsie. Transplantation (2017) 101(3):608–15. doi: 10.1097/TP.0000000000001231
25. Zitzner JR, Shah S, Jie C, Wegner W, Tambur AR, Friedewald JJ. A Prospective Study Evaluating the Role of Donor-Specific Anti-Endothelial Crossmatch (XM-ONE Assay) in Predicting Living Donor Kidney Transplant Outcome. Hum Immunol (2013) 74:1431–6. doi: 10.1016/j.humimm.2013.06.007
26. Gareau AJ, Wiebe C, Pochinco D, Gibson IW, Ho J, Rush DN, et al. Pre-Transplant AT1R Antibodies Correlate With Early Allograft Rejection. Transpl Immunol (2018) 46:29–35. doi: 10.1016/j.trim.2017.12.001
27. Lim WH, Wong G, Heidt S, Claas FHJ. Novel Aspects of Epitope Matching and Practical Application in Kidney Transplantation. Kidney Int (2018) 93(2):314–24. doi: 10.1016/j.kint.2017.08.008
28. Duquesnoy RJ, Kamoun M, Baxter-Lowe LA, Woodle ES, Bray RA, Claas FH, et al. Should HLA Mismatch Acceptability for Sensitized Transplant Candidates be Determined at the High-Resolution Rather Than the Antigen Level? Am J Transplant (2015) 15(4):923–30. doi: 10.1111/ajt.13167
29. Wiebe C, Pochinco D, Blydt-Hansen TD, Ho J, Birk PE, Karpinski M, et al. Class II HLA Epitope Matching - A Strategy to Minimize De Novo Donor-Specific Antibody Development and Improve Outcomes. Am J Transplant (2013) 13:3114–22. doi: 10.1111/ajt.12478
30. Wiebe C, Rush DN, Nevins TE, Birk PE, Blydt-Hansen T, Gibson IW, et al. Class II Eplet Mismatch Modulates Tacrolimus Trough Levels Required to Prevent Donor-Specific Antibody Developmen. J Am Soc Nephrol (2017) 28:3353–62. doi: 10.1681/ASN.2017030287
31. Tafulo S, Malheiro J, Santos S, Dias L, Almeida M, Martins S, et al. Degree of HLA Class II Eplet Mismatch Load Improves Prediction of Antibody-Mediated Rejection in Living Donor Kidney Transplantation. Hum Immunol (2019) 80(12):966–75. doi: 10.1016/j.humimm.2019.09.010
32. Besarani D, Cerundolo L, Smith JD, Procter J, Barnardo MC, Roberts IS, et al. Role of Anti-Vimentin Antibodies in Renal Transplantation. Transplantation (2014) 98(1):72–8. doi: 10.1097/01.TP.0000443224.66960.37
33. Gimeno J, Redondo D, Perez-Saez MJ, Naranjo-Hans D, Pascual J, Crespo M. Impact of the Banff 2013 Classification on the Diagnosis of Suspicious Versus Conclusive Late Antibody-Mediated Rejection in Allografts Without Acute Dysfunction. Nephrol Dial Transplant (2016) 31:1938–46. doi: 10.1093/ndt/gfw223
34. Redondo-Pachon D, Perez-Saez MJ, Mir M, Gimeno J, Llinas L, Garcia C, et al. Impact of Persistent and Cleared Preformed HLA DSA on Kidney Transplant Outcomes. Hum Immunol (2018) 79:424–31. doi: 10.1016/j.humimm.2018.02.014
35. Reinsmoen NL, Mirocha J, Ensor CR, Marrari M, Chaux G, Levine DJ, et al. A 3-Center Study Reveals New Insights Into the Impact of Non-HLA Antibodies on Lung Transplantation Outcom. Transplantation (2017) 101(6):1215–21. doi: 10.1097/TP.0000000000001389
36. Zhang Q, Cecka JM, Gjertson DW, Ge P, Rose ML, Patel JK, et al. HLA and MICA: Targets of Antibody-Mediated Rejection in Heart Transplantation. Transplantation (2011) 91(10):1153–8. doi: 10.1097/TP.0b013e3182157d60
37. Duquesnoy RJ. A Structurally Based Approach to Determine HLA Compatibility at the Humoral Immune Level. Hum Immunol (2006) 67:847–62. doi: 10.1016/j.humimm.2006.08.001
38. Luque S, Lucia M, Melilli E, Lefaucheur C, Crespo M, Loupy A, et al. Value of Monitoring Circulating Donor-Reactive Memory B Cells to Characterize Antibody-Mediated Rejection After Kidney Transplantation. Am J Transplant (2019) 19:368–80. doi: 10.1111/ajt.15055
39. Zhang Q, Reed EF. The Importance of Non-HLA Antibodies in Transplantation. Nat Rev Nephrol (2016) 12:484–95. doi: 10.1038/nrneph.2016.88
40. Sanchez-Zapardiel E, Castro-Panete MJ, Mancebo E, Morales P, Laguna-Goya R, Morales JM, et al. Early Renal Graft Function Deterioration in Recipients With Preformed Anti-MICA Antibodies: Partial Contribution of Complement-Dependent Cytotoxicity. Nephrol Dial Transplant (2016) 31:150–60. doi: 10.1093/ndt/gfv308
41. Le Bas-Bernardet S, Hourmant M, Coupel S, Bignon JD, Soulillou JP, Charreau B. Non-HLA-Type Endothelial Cell Reactive Alloantibodies in Pre-Transplant Sera of Kidney Recipients Trigger Apoptosis. Am J Transplant (2003) 3:167–77. doi: 10.1034/j.1600-6143.2003.00021.x
42. Butler CL, Hickey MJ, Jiang N, Zheng Y, Gjertson D, Zhang Q, et al. Discovery of Non-HLA Antibodies Associated With Cardiac Allograft Rejection and Development and Validation of a Non-HLA Antigen Multiplex Panel: From Bench to Bedside. Am J Transplant (2020) 20(10):2768–80. doi: 10.1111/ajt.15863
43. Porcheray F, DeVito J, Yeap BY, Xue L, Dargon I, Paine R, et al. Chronic Humoral Rejection of Human Kidney Allografts Associates With Broad Autoantibody Responses. Transplantation (2010) 89(10):1239–46. doi: 10.1097/TP.0b013e3181d72091
44. Jackson AM, Sigdel TK, Delville M, Hsieh SC, Dai H, Bagnasco S, et al. Endothelial Cell Antibodies Associated With Novel Targets and Increased Rejection. J Am Soc Nephrol (2015) 26:1161–71. doi: 10.1681/ASN.2013121277
45. Dinavahi R, George A, Tretin A, Akalin E, Ames S, Bromberg JS, et al. Antibodies Reactive to Non-HLA Antigens in Transplant Glomerulopathy. J Am Soc Nephrol (2011) 22:1168–78. doi: 10.1681/ASN.2010111183
46. Lefaucheur C, Viglietti D, Bouatou Y, Philippe A, Pievani D, Aubert O, et al. Non-HLA Agonistic Anti-Angiotensin II Type 1 Receptor Antibodies Induce a Distinctive Phenotype of Antibody-Mediated Rejection in Kidney Transplant Recipients. Kidney Int (2019) 96(1):189–201. doi: 10.1016/j.kint.2019.01.030
47. Zhang J, Wang M, Liang J, Zhang M, Liu XH, Ma L. The Presence of Anti-Angiotensin II Type-1 Receptor Antibodies Adversely Affect Kidney Graft Outcome. Int J Environ Res Public Health (2017) 14:500. doi: 10.3390/ijerph14050500
48. Giral M, Foucher Y, Dufay A, Duong Van Huyen JP, Renaudin K, Moreau A, et al. Pretransplant Sensitization Against Angiotensin II Type 1 Receptor Is a Risk Factor for Acute Rejection and Graft Loss. Am J Transplant (2013) 13:2567–76. doi: 10.1111/ajt.12397
49. Taniguchi M, Rebellato LM, Cai J, Hopfield J, Briley KP, Haisch CE, et al. Higher Risk of Kidney Graft Failure in the Presence of Anti-Angiotensin II Type-1 Receptor Antibodies. Am J Transplant (2013) 13:2577–89. doi: 10.1111/ajt.12395
50. Einecke G, Sis B, Reeve J, Mengel M, Campbell PM, Hidalgo LG, et al. Antibody-Mediated Microcirculation Injury Is the Major Cause of Late Kidney Transplant Failure. Am J Transplant (2009) 9:2520–31. doi: 10.1111/j.1600-6143.2009.02799.x
51. Sellares J, de Freitas DG, Mengel M, Reeve J, Einecke G, Sis B, et al. Understanding the Causes of Kidney Transplant Failure: The Dominant Role of Antibody-Mediated Rejection and Nonadherence. Am J Transplant (2012) 12:388–99. doi: 10.1111/j.1600-6143.2011.03840.x
52. Arias-Cabrales C, Redondo-Pachón D, Pérez-Sáez MJ, Gimeno J, Sánchez-Güerri I, Bermejo S, et al. Renal Graft Survival According to Banff 2013 Classification in Indication Biopsies. Nefrología (English Ed) (2016) 36(6):660–6. doi: 10.1016/j.nefroe.2016.05.012
53. Koenig A, Chen CC, Marcais A, Barba T, Mathias V, Sicard A, et al. Missing Self Triggers NK Cell-Mediated Chronic Vascular Rejection of Solid Organ Transplants. Nat Commun (2019) 10(1):5350. doi: 10.1038/s41467-019-13113-5
Keywords: kidney transplantation, antibody-mediated rejection, HLA antibodies, non-HLA antibodies, HLA epitope mismatch, AT1R antibodies
Citation: Crespo M, Llinàs-Mallol L, Redondo-Pachón D, Butler C, Gimeno J, Pérez-Sáez MJ, Burballa C, Buxeda A, Arias-Cabrales C, Folgueiras M, Sanz-Ureña S, Valenzuela NM, Reed EF and Pascual J (2021) Non-HLA Antibodies and Epitope Mismatches in Kidney Transplant Recipients With Histological Antibody-Mediated Rejection. Front. Immunol. 12:703457. doi: 10.3389/fimmu.2021.703457
Received: 30 April 2021; Accepted: 15 June 2021;
Published: 06 July 2021.
Edited by:
Frans H. J. Claas, Leiden University, NetherlandsReviewed by:
Vincenzo Cantaluppi, Università del Piemonte Orientale, ItalyGonca Emel Karahan, Leiden University Medical Center, Netherlands
Copyright © 2021 Crespo, Llinàs-Mallol, Redondo-Pachón, Butler, Gimeno, Pérez-Sáez, Burballa, Buxeda, Arias-Cabrales, Folgueiras, Sanz-Ureña, Valenzuela, Reed and Pascual. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marta Crespo, bWNyZXNwb0Bwc21hci5jYXQ=
†These authors have contributed equally to this work and share first authorship
‡These authors have contributed equally to this work and share senior authorship