 Xianlin Ye1
Xianlin Ye1 Limin Chen
Limin Chen- 1Department of Laboratory, Shenzhen Blood Center, Shenzhen, China
- 2Provincial Key Laboratory for Transfusion-Transmitted Infectious Diseases, Institute of Blood Transfusion, Chinese Academy of Medical Sciences (CAMS) and Peking Union Medical College (PUMC), Chengdu, China
- 3The Joint Laboratory on Transfusion-Transmitted Diseases (TTD) Between Institute of Blood Transfusion, Nanning Blood Center, Chinese Academy of Medical Sciences and Nanning Blood Center, Nanning, China
- 4Toronto General Research Institute, University Health Network, University of Toronto, Toronto, ON, Canada
Background: Most Chinese Blood Centers adopted mini pool (MP) nucleic acid testing (NAT) for HBV screening due to high cost of Individual donation (ID) NAT, and different proportions of MP-reactive but ID-non-reactive donations (MP+/ID−, defined as non-resolved donations) have been observed during daily donor screening process. Some of these non-resolved donations are occult HBV infections (OBIs), which pose potential risk of HBV transmission if they are not deferred. This study is aimed to further analyze these non-resolved donations.
Methods: The non-resolved plasma samples were further analyzed by serological tests and various HBV DNA amplification assays including quantitative PCR (qPCR) and nested PCR amplifying the basic core and pre-core promoter regions (BCP/PC; 295 base pairs) and HBsAg (S) region (496 base pairs). Molecular characterizations of HBV DNA+ non-resolved samples were determined by sequencing analysis.
Results: Of 17,226 MPs from 103,356 seronegative blood donations, 98 MPs were detected reactive for HBV. Fifty-six out of these 98 (57.1%) reactive MPs were resolved as HBV DNA+, but the remaining 42 pools (42.9%, 252 donations) were left non-resolved with a high rate (53.2%) of anti-HBc+. Surprisingly, among 42 non-resolved MPs, 17 contained one donation identified as OBIs by alternative NAT assays. Sequence analysis on HBV DNAs extracted from these OBI donations showed some key mutations in the S region that may lead to failure in HBsAg detection and vaccine escape.
Conclusion: A total of 53.2% of the non-resolved donations were anti-HBc+, and OBIs were identified in 40.5% of these non-resolved pools. Therefore, non-resolved donations with anti-HBc+ might pose potential risk for HBV transmission. Our present analysis indicates that anti-HBc testing in non-resolved donations should be used to identify OBIs in order to further increase blood safety in China.
Introduction
Occult hepatitis B virus (HBV) infection (OBI) is characterized by the presence of very low levels of HBV DNA in the plasma and/or in the liver, with undetectable hepatitis B surface antigen (HBsAg), with or without antibodies to hepatitis B core antigen (anti-HBc) or hepatitis B surface antibody (anti-HBs), outside the pre-seroconversion window period (1), and OBIs may contribute to the exacerbation of acute HBV infection and the development of HBV-associated cirrhosis and hepatocellular carcinoma (HCC) (2). OBI has been found in blood donors, and the prevalence varies from less than 1 to 16% dependent on the endemicity of HBV infection, the screening NAT assays, and confirmation algorithms used (3–6). Although donations with OBI pose a significant risk of transfusion-transmitted HBV infection, OBI screening is very difficult due to intermittent very low virus load and mutations in HBV genome (7, 8).
The blood screening strategy by employing both HBsAg and anti-HBc detection combined with HBV NAT assay in some developed countries allows the detection of window-period infection, OBI, and HBV mutated strains possible to maximally ensure blood safety. However, in HBV endemic countries such as in China, deferral of all anti-HBc positive donations was impractical due to the shortage of blood supply. In addition, high cost of ID-NAT prompt users to adopt screening strategies of pooling of multiple donor samples (9). As a pilot NAT project initiated by the National Health Commission (NHC) of China, Shenzhen Blood Center has been using the Roche Cobas TaqScreen MPX test2.0 for HBV DNA, hepatitis C virus (HCV) RNA, and human immune-deficiency virus (HIV) RNA in routine screening in MP6 (pooled from six individual donations) format since 2017. It turns out this assay is highly specific, sensitive, reproducible, and robust (10, 11). However, different proportions of MP-reactive but individual non-reactive donations (MP+/ID−) have been observed during daily screening. In ID-NAT screening, non-repeat-reactive (NRR) donations are not released for transfusion in most countries. However, for MP6-NAT it is not an option to discard the units implicated in non-resolved pools, leaving a fatal threat to blood safety, particularly in HBV high prevalent countries such as China.
Previously, we have reported nearly half of the initial reactive, but further discriminatory test negative donations were identified as OBIs, which strongly suggested that a proportion of donations with ID-NAT screening NRR results might pose HBV transmission risk even when using highly sensitive NAT assays (12). In this study, we move on to further analyze the non-resolved reactive mini pools in respect to their potential transmission risk for HBV infection. In order to clarify and evaluate the true infection status of the non-resolved donations, alternative Ultrio Plus ID-NAT, nested PCR for S, BCP/PC, and qPCR with high volume extraction were performed (13), and HBV infection status will be characterized from these non-resolved donations. The optimized screening strategy by adding anti-HBc testing will also be discussed.
Materials and Methods
Subjects and Samples
As a routine practice, all donations were collected and screened serologically as reported in our previous study (12). In total, 103,356 seronegative blood samples (17,226 MP6 pools) were enrolled in this study for further analysis.
NAT Screening of Donor Samples
Six individual donated blood were pooled into one mini pool (MP6), and NAT screening of the MP6 was performed on a fully automated Roche Cobas s 201 system using a multiplex polymerase chain reaction kit (Cobas TaqScreen MPX test, version 2.0, Roche Molecular Systems, Branchburg, NJ, USA; 1 ml, LOD: 2.3 IU/ml for HBV DNA, 1 IU/ml=5.6 copies/ml). Donations with negative NAT results were released, and MPX-reactive MP6 were resolved by retesting each individual donation (ID-NAT). Samples individually reactive were classified as MPX repeat reactive (designated as NAT+). If one NAT+ was identified, other five non-reactive donations were designated as NAT− and can be released. If all six individual donations in the pool were detected as MPX non-reactive, they were classified as MP non-resolved donations. These non-resolved donations were further tested individually by an alternative Procleix Ultrio Plus HBV discriminatory assay (Grifols Diagnostic Solutions, Inc. and Hologic; 0.5 ml, LOD: 3.4 IU/ml) to identify the presence of HBV DNA. Donations showing non-reactivity in the Ultrio Plus assay were classified as NAT non-resolved donations by Ultrio Plus MPX. Donations showing reactivity in discriminatory HBV assays were identified as HBV NAT+, and the pool was regarded as resolved pool by Ultrio Plus.
Serological and Molecular Detection
All resolved and non-resolved samples, including frozen plasma, were collected for further determination. HBsAg, anti-HBs, HBeAg, anti-HBe, and anti-HBc were tested by commercially available electrochemiluminescence immunoassay, ECLI (Roche, USA). All samples were retested on anti-HBc by a domestic EIA kits (WanTai Diagnostics, Beijing, China), and only samples with reactivity for both assays were designated as anti-HBc+.
HBV DNA was additionally extracted from 2.5 ml of plasma by HighPure Viral Nucleic Acid Large Volume Kits (Roche Diagnostics Gmbh, Mannhein, Germany) and were analyzed by a combination of qPCR (13) (LOD: 5 IU/ml) and nested PCRs (the LOD for the combination qPCR/nested PCR assay used with high volume extraction can reach as low as 1 IU/ml (5.6 copies/ml)), which amplified BCP/PC (LOD: 10 IU/ml) and S regions (LOD: 10 IU/ml) as previously described (4, 14).
HBV DNA Sequencing and Genotyping
The amplified products of BCP/PC and S regions were sent to Shanghai Invitrogen Co., Ltd. (Guangzhou, China) for sequencing. HBV genotyping was performed by Phylogenetic analysis using MEGA7.1 program, and the neighbor-joining method based on Kimura 2-parameter mode and complete deletion for gaps with 1,000 bootstrap replications was chosen as previously reported (13). So-called wild type consensus sequences were derived from the alignment of 124 genotype B and 95 genotype C sequences from HBsAg+ blood donors (4).
Statistical Analyses
Stata 16.0 was applied for statistical analysis of various data. P < 0.05 (two-tailed) was set as the significant cut-off level.
Results
Screening Results of the Blood Donations
A total of 103,356 seronegative blood donations were collected. A total of 17,226 pools were derived, and 98 pools were reactive for HBV DNA by MPX2.0 NAT in MP6 format. Fifty-six pools (56/98, 57.1%) were resolved with HBV DNA+ (MP+/ID+), and 42 pools (42.9%, 252 donations) were detected non-reactive by MPX2.0 ID-NAT (MP+/ID−, Figure 1), including 169 males and 83 females (Table 1). The first-time and repeat donors were 115 (45.6%) and 137 (54.4%), respectively.
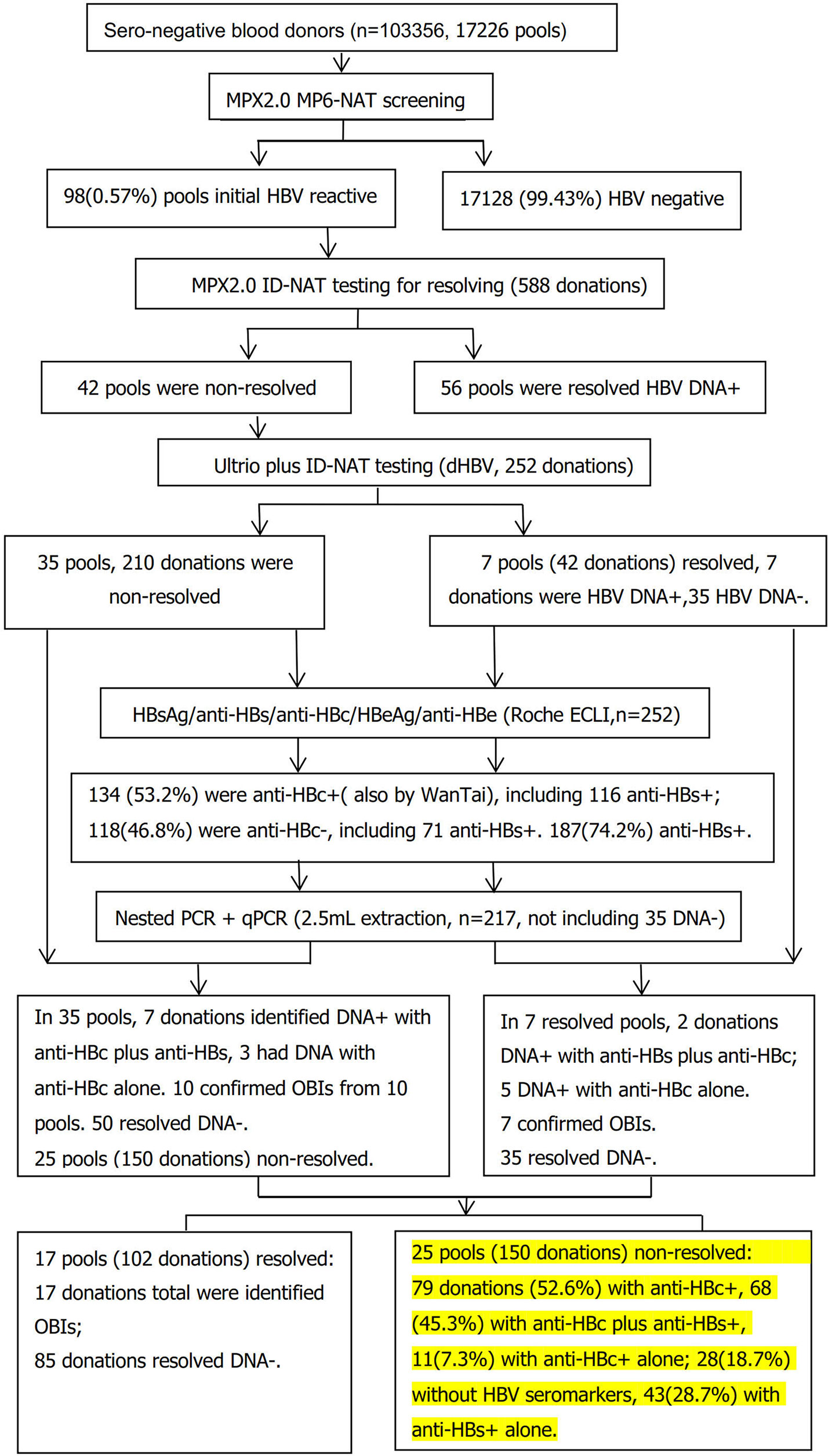
Figure 1 Flow chart of serological and molecular identification of MPX 2.0 MP6-NAT in non-resolved samples.
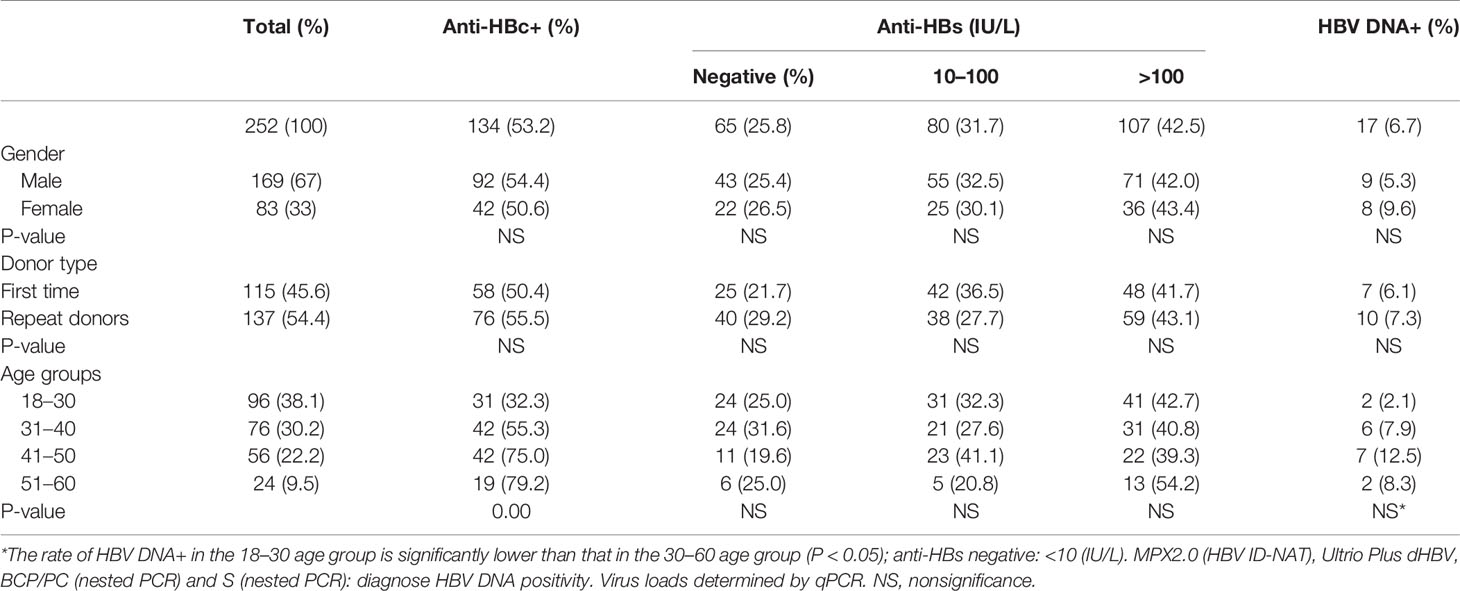
Table 1 Demographic and viral characteristics of 252 (42 pools) non-resolved blood donations.
Supplemental Serological Testing Results for 252 Non-resolved Donations
After tested by Elecsys II assay for HBsAg, anti-HBs, HBeAg, anti-HBe, and anti-HBc, 134 out of the 252 non-resolved donations (53.2%) were reactive for anti-HBc, all of which were confirmed positive by WanTai anti-HBc kit. There was no correlation between the presence of anti-HBc and gender or donor type. In contrast, there was a clear increase of anti-HBc prevalence with age, ranging from 32.3% in the <30 age group to 79.2% in the >50 age group (χ2 = 34.2, p=0.00).
Ultrio Plus ID-NAT, Nested PCR, and qPCR Testing for HBV DNA of Non-Resolved Donations
HBV DNA was further analyzed individually for the 252 non-resolved donations by Ultrio plus dHBV, and seven donations out of 42 MPs (252 donations) (7/252 = 2.8%) were resolved as dHBV+, leaving 210 donations still non-resolved. After the 210 non-resolved samples and 7 dHBV+ samples were further analyzed by nested PCR (BCP/PC and S region) and qPCR with 2.5 ml extraction of DNA individually, 10 donations out of 35 MPs (150 donations) were identified as HBV DNA+ (Table 2). All together, 17 donations from 42 MPs (252 donations) were resolved HBV DNA+ (one per pool).
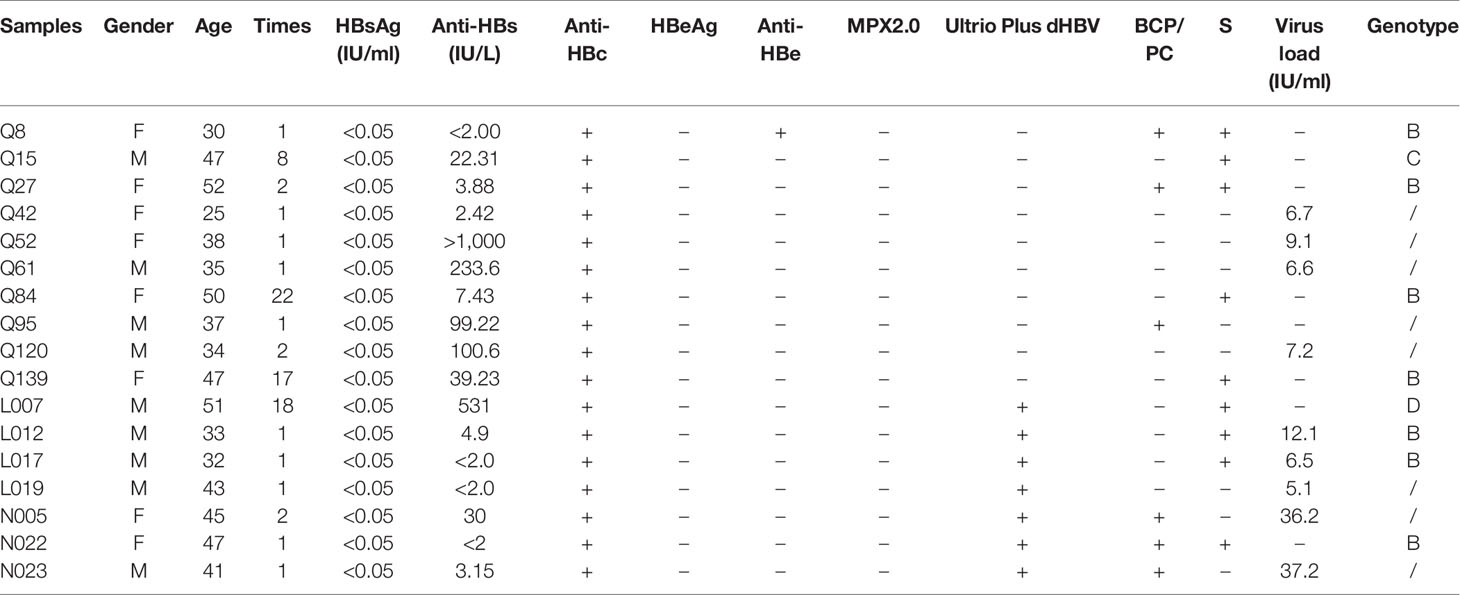
Table 2 The serological and molecular characterization results of the 17 identified HBV DNA+ donations.
Of the 17 identified HBV DNA positive donors, seven were repeat donors and 10 were first-time donors, and eight were males and nine were females with average age of 36.2. Regarding the other viral markers, eight had anti-HBc alone, one carried anti-HBc and anti-HBe, and eight were positive for both anti-HBc and anti-HBs. Three out of the eight anti-HBs positive samples had titers over 100 IU/L. Finally, 150 donations still remained non-resolved, among which 17 were identified as OBIs, and 85 donations were resolved HBV DNA negative.
Comparison of Seromarkers Distribution Among Non-Resolved 252 Donations, Remaining 150 Non-Resolved Donations, and Resolved Negative Donations
In the remaining non-resolved donations, 79/150 (52.6%) donations carried anti-HBc, in which 11 cases (7.3%) were anti-HBc alone. While, in the resolved negative donations from 17 resolved pools (85 donations), 38/85 (44.7%) donations carried anti-HBc, including 1 (1.2%) with anti-HBc alone (Table 3). The rate of anti-HBc alone in the remaining non-resolved donations is six times higher than that in the resolved negative donations (P<0.05).
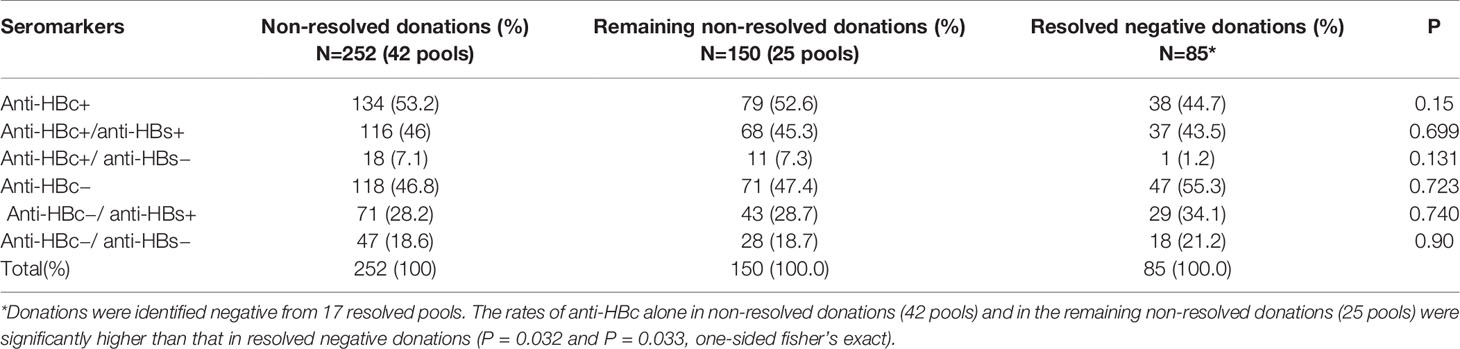
Table 3 HBV seromarker distribution of non-resolved donations, the remaining non-resolved and resolved negative donations.
Genotyping and Mutation Analysis of the S and BCP/PC Regions in the Identified HBV DNA+ Donations
Totally, 17 samples (17/42, 40.5%) in the non-resolved pools were identified HBV DNA+ and classified as OBIs by Ultrio plus and additionally serological and molecular assays. The maximum and median viral loads were 37.2 IU/ml and 5.1 IU/ml, respectively. The phylogenetic analysis identified seven donations with genotype B and one genotype C and one genotype D. The S region amino acid sequences of these nine cases showed that all cases had amino acid substitutions. Regarding the seven genotype B samples, two out of seven (28.6%) samples were observed as wild type (L017 and Q84). Four samples (57.1%) had vaccine escape mutations: G112R (Q8), T126S (L012), M133T (Q27), D144E (Q139), and S174N (Q139). Sample Q27 with anti-HBs harbored a T131N/M133T N-glycosylation mutation, which may interfere with recognition of HBsAg by anti-HBs, therefore contributing to virus escape from the host immune system (15). In addition, 4/7 (57.1%) have mutations that have potential impact on the detection of HBsAg: T126S (L012), M133T (Q27), F134L (Q27), T143L (Q8), L175S (Q139). Various mutations associated with OBIs—Q101R (N022 and Q139), P105R (Q139), T126S (L012), P127H (Q27), M133T (Q27), S174N (Q139), and V177A (Q139)—were also detected in four (57.1%) samples. For the one genotype C sequence, it harbored multiple mutations including Q30K, L53S, T113K, and T118K, and lastly a genotype D sample carrying V96A, L104W, G112E, P127L, Q129P, and S164N mutations.
BCP/PC genes were amplified from six samples by nested PCR. Nucleotide mutations with high frequency were found as follows: 5/6 (83.3%) sequences contain T1719G, which has been previously reported to inhibit HBV replication through Enh II and HBx proteins mutation in vitro (16). Also present were 6/6 (100%) A1726C and 5/6 (83.3%) C1730G mutations. In addition, other mutations such as A1752G/T (33.3%), C1773T (33.3%), G1809T (33.3%), A1846T (33.3%), G1799C (16.7%), C1853T (16.7%), G1896A (16.7%), G1899A (16.7%), and G1915A (16.7%) were also observed.
Discussion
Donor screening is essential to ensure blood safety to prevent transfusion-transmitted infections. To decrease the residual risk for HBV infection, both HBsAg and anti-HBc, together with highly sensitive HBV NAT (ideally ID-NAT) screening, provide the highest level of blood safety for recipients, but this comprehensive screening strategy is only adopted in high income countries due to high cost and strict requirement of NAT (17). In most developing countries, especially China with a high positive rate for anti-HBc, alternative approaches can be used to balance the cost and safety. Currently HBsAg and MP-NAT screening have been used in China to prevent most cases of HBV infections from transfusion. In countries where NAT screening is not implemented, screening HBsAg and anti-HBc could identify donors with OBI at relatively low cost. Then, testing donations with HBsAg negative but anti-HBc positive using a highly sensitive NAT for HBV-DNA could intercept most acute HBV infections within window period (WP) or OBIs. These two different safety procedures applied in sequence could guarantee blood safety at a relatively low cost. As a compromised strategy, most Chinese blood centers adopt both HBsAg and HBV MP-NAT screening to balance the cost and safety by shortening the WP and intercepting most OBIs. The same approach has also been applied in Taiwan (18). In a country with a high positive rate for anti-HBc, the use of anti-HBc positive/HBsAg negative/HBV-DNA negative donations for anti-HBc (>100 UI) and/or HBsAg positive individuals should also be considered if blood shortage exists. Although blood screening strategy has been improved, problems still exist, especially in many countries with high prevalence of blood-borne pathogen infections. While adopting NAT assays greatly shorten the window period that allows detection of many serologically undetectable infections possible, donations with MP-reactive but ID-non-reactive donations (MP+/ID−, defined as non-resolved donations) have been observed during daily screening process. These non-resolved donations may pose a significant risk for transfusion-transmitted infections in recipients, especially in China where HBV infection is endemic and anti-HBc testing cannot be implemented in routine blood screening. A Chinese multicenter study performed on 826,044 serologic negative donations in MPs of six identified that a total of 1,267 pools were reactive, of which 839 donations were reactive by ID-NAT, leaving 428(33.8%) non-resolved MPs (19). These NAT initially reactive (IR)/non-resolved MPs might contain plasma from anti-HBc+ OBI donors with extremely low and intermittently detectable HBV DNA load but still potentially infectious (17, 19), raising urgent need for a practical algorithm to sort out which blood units can be safely transfused.
Previously, we reported nearly half of the initial Ultrio plus NAT reactive, but further discriminatory test negative donations were identified as OBIs in ID-NAT screening setting (12), strongly suggesting a large proportion of samples had viral load below the 95% LOD of the Ultrio Plus ID-NAT assay (LOD: 6.8 IU/donation) and also the MPX2.0 MP6 NAT assay (LOD: 13.8 IU/donation). Donations with such low viral loads had a high probability of being missed by the subsequent HBV ID-NAT, and this probability was determined by Poisson distribution (20). The 5% LOD of the MPX assay is higher when testing in MP6 than in ID format (the 95% LOD of MPX2.0 test: 2.3 IU/ml [ID format] and 13.8 IU/ml [MP format]) (10), but a dilution factor of six is relatively small on the whole NAT detection endpoint probability curve that spans a concentration range of a factor of 100 between the 95 and the 5% LOD (19). Thus, it is likely to have a reactive result in a pool of six samples but not in any of the individual samples. Another possibility of MP-NAT reactive but ID-NAT non-reactive (non-resolved) donations may be due to contamination, although this possibility is very low. To avoid contamination, we established a NAT laboratory with international standard, and all the screening procedures are fully automatic, even for screw capping. Furthermore, we adopted strict standard biosecurity and institutional safety procedures during the screening process.
In this study we screened 17,226 pools (103,356 donations) by Roche MPX2.0 MP6-NAT, and we identified 98 (0.57%, 95% CI 0.46–0.69%) MPs were initial reactive, among which 56/98 (57.1%) were resolved HBV DNA+. HBV DNA+ rate is 0.054% in this study cohort and is lower than screened by ID-NAT format reported in our previous study (12), likely because of dilution factor in MP-NAT and low-viral-load donations. Forty-two of 17,226 (0.24%, 95% CI 0.18–0.33%) MPs were initially reactive, but all six donations from each MP were non-reactive (designated as non-resolved) when tested individually. This non-resolved percentage is in concordance with the study in Australia (21), but it is lower than the result from a national survey (19), probably due to the fact that the implementation of NAT in routine blood screening in Shenzhen Blood Center was 10 years earlier than other Chinese blood centers. After 42 non-resolved pools were further tested by Ultrio Plus ID-NAT, seven donations from 42 MPs (252 donations) were identified HBV DNA+ with anti-HBc+, and they became resolved. Since the probability of detection by NAT in low-viral-load samples follows a Poisson distribution, we tested a total of 210 (0.20%) donations in the remaining 35 non-resolved pools by 2.5 ml large-volume extraction followed by nested PCR amplification and qPCR, and 10 donations from 35 MPs (210 donations) were further identified HBV DNA+ with anti-HBc, indicating they were OBIs. It is undoubted that some low-viral-load donations were detected in MP6 format but missed by ID-NATs. To sum up, 17 donations from 17/42 (40.4%) non-resolved pools (252 donations) containing HBV DNA+ were detected by additional alternative NATs, leaving 25/98 (25.5%) remaining non-resolved pools including 150 donations. These donations were released and transfused to recipients, posing potential threat to blood safety.
Previous studies estimated OBI transmission rate for all components varied between 3 and 48% (8, 22, 23), which might be underestimated. A recent mathematical model estimated that 3.3 and 14% of OBI donations undetected by NAT with LOD of 3.4 IU/ml might cause recipient infection by a blood component containing 20 ml and 200 ml of plasma, respectively (24). Infectious donations not detected by MP-NAT but reactive with ID-NAT have been reported (25, 26). According to clinical evidence and sequence identity, HBV transfusion transmission in 9/31 recipients (29%) of blood components from donations undetected by the currently most sensitive NAT and HBsAg showed that even low levels of DNA in donors can be infectious, and the revised lowest infectious dose was down to 0.14 IU/ml (7). Furthermore, two cases of transfusion-transmitted HBV infection were identified by donor-recipient sequence identity following transfusion of 14 OBI donations missed by MP6 HBV DNA screening (8). In ID-NAT screening, NRR donations are not released for transfusion in most countries. However, for MP6 NAT, it is not an option to discard the units implicated in non-resolved pools. In this study, we used large-volume viral nucleic acid extraction, together with the highly sensitive nested PCR, to detect viral fragments, and we identified that 40% of non-resolved pools contained HBV DNA with anti-HBc. These donations could transmit HBV especially in immune compromised recipients. Our results indicated that even after MP-NAT screening in China, donations with OBI still pose a potential residual threat for blood safety. Although transfusion-transmission evidence is needed to substantiate this risk and anti-HBc and anti-HBs prevalence in recipients should also be considered, our data still suggest that a proportion of non-resolved pools still contain extremely low levels of HBV that may be infectious, and more comprehensive resolving strategy should be considered for MP-NAT.
The presence of anti-HBs in addition to anti-HBc indicates a resolved infection with persistent HBV DNA (27). In some countries such as Germany and Austria, blood units with anti-HBs levels greater than 100 IU/L are considered to be safe (28), and in Japan, anti-HBc-positive blood containing 200 IU/L or more of anti-HBs appears safe as a transfusion component (29). However, transmission of HBV from occult hepatitis B subjects occurred in the presence of concurrent neutralizing anti-HBs in the same specimen (30, 31). Data from organ transplantation also clearly proved that HBV DNA in the presence of anti-HBs could be infectious in immunosuppressed patients (32). HBV DNA detected in some anti-HBs-positive samples in this study suggests that the absence of HBsAg and the presence of anti-HBs do not necessarily guarantee full safety. In the present study, 74.2% donors were anti-HBs+ including 46% with anti-HBc and 28.2% anti-HBs only, suggesting only a small part of donors (28.2%) had a certain protection; most were induced by immune response when non-vaccinated donor exposed to HBV or an anamnestic response to HBV when vaccinated donor exposed. Eight of 17 (47.1%) OBIs detected in non-resolved donations carry anti-HBs, suggesting that OBIs occur largely in individuals who have recovered from the infection but are unable to develop a totally effective immune control (33, 34). Anti-HBc alone has been observed either in a stage of late HBV immunity after the decline of anti-HBs to undetectable levels or in the resolving phase of acute infection. Consistent with OBI, donated samples carrying anti-HBc alone are more infectious than those with low levels of anti-HBs (35). Even certain PCR negative “anti-HBc alone” individuals have been suspected to be potentially infectious (36). According to a recent study, blood donors negative for both HBsAg and HBV DNA but reactive for anti-HBc might be HBV carriers with viral loads below the detection limit (37). In our present study, 8/17 non-resolved donations were identified as OBIs with anti-HBc alone, and these OBIs may pose significant threat to blood safety.
It is well-known that anti-HBc is detectable during asymptomatic infections as well as throughout life after recovery from HBV infection with or without the presence of anti-HBs (38); therefore, anti-HBc is considered a key seromarker for OBI. Anti-HBc screening assays have the potential to exclude the majority of OBIs undetectable by NAT (27, 39, 40), leaving only rare cases with escape mutants associated with the presence of anti-HBs alone (41). Many studies supported the use of serological markers such as anti-HBc to compensate less-sensitive NAT assays (42, 43). However, only a relatively small portion of OBIs can be identified by MP-NAT, which emphasizes the importance of anti-HBc testing and ID-NAT screening. In line with this, an American comprehensive study from 22.4 million blood donors screened by HBsAg, anti-HBc, and NAT revealed that only 43/404 (10.6%) OBIs could be detected by MP-NAT, while most of OBIs (361/404, 89.4%) could only be identified by ID-NAT (44). These results indicated that the potential relative risk of OBI among MP- positive donations may be small compared to that in MP-negative donations. Nevertheless, in countries such as in China, where HBV endemic infections are high, anti-HBc screening may cause blood shortage. Considering the cost, ID-NAT is not a mandatory requirement for donor screening in China; therefore, an alternative approach is to screen MP-positive donations with anti-HBc to identify those donations with potential OBIs to balance the cost and safety. Ideally, blood centers should adopt ID-NAT screening especially in regions with high HBV endemicity, but in reality, different strategies have been used. We made a rough analysis of cost-effectiveness by comparing three strategies: (1) HBsAg+ anti-HBc, (2) HBsAg+ MP6 NAT, (3) HBsAg+ MP6+ anti-HBc in MP+/ID− (Table 4). Undoubtedly, HBsAg and anti-HBc screening is the most highly cost-effective, but it would overkill about 40% anti-HBc+ donations, resulting in blood shortage. Adding anti-HBc screening for MP+/ID− non-resolved donations would cost 5,004 RMB more but at least benefit from preventing the occurrence of six transfusion-transmitted HBV cases (Table 4) with only deferring 0.11% anti-HBc+ donations to transfusion, but obtaining 67.6 times benefit (46).
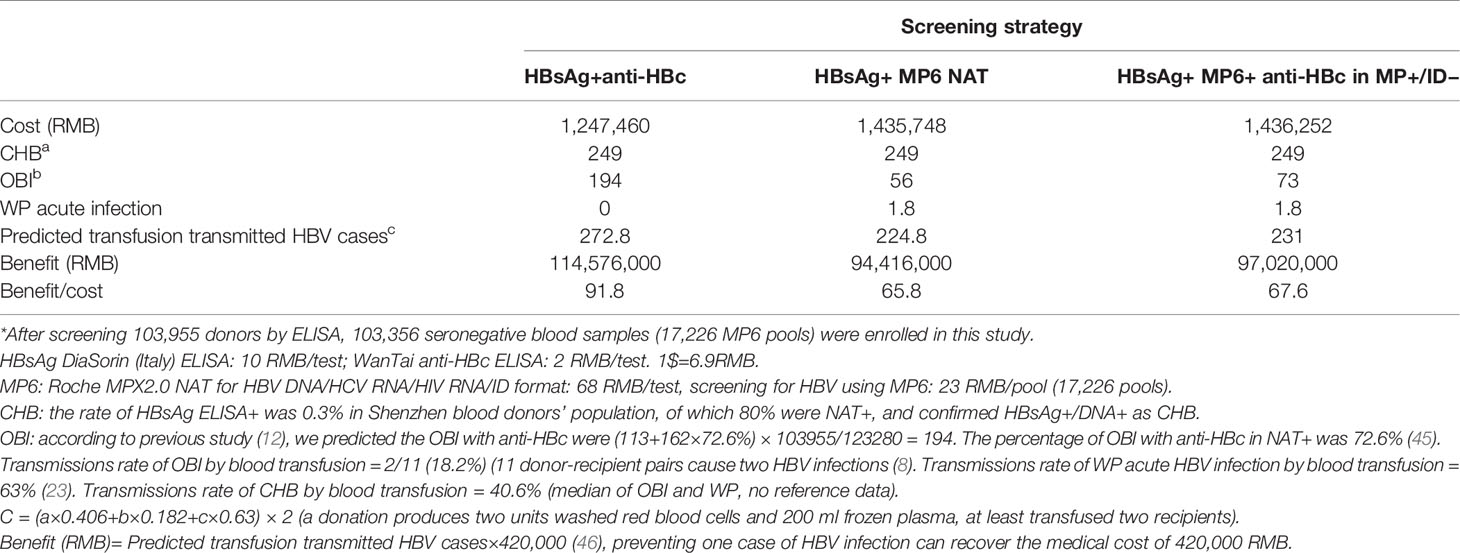
Table 4 Cost-effectiveness analysis of 103,955 donors* in Chinese Shenzhen Blood Center.
It has been reported that mutations in S gene or promoter and enhancer sequences of HBV genome could result in false negative in HBsAg detection and NAT assays (47, 48). Although mutations from the consensus (wild type) may also be present in a minority of non-OBI sequences, according to our sequence analysis, some OBIs indeed carry mutations in S gene or in BCP/PC, which most likely affect HBsAg detection (T126S, M133T, F134L, T143L, L175S) or inhibit HBV DNA replication (T1719G). The mutation impact remains speculative without functional analysis, and we are in the process of setting up these assays to further confirm the biological significance of some of these mutations, especially in evasion of immune surveillance and detection.
Although more specific and sensitive NATs are urgently needed for donor screening in MP format, it is a long way to guarantee blood safety. As the majority of individuals with OBI have very low viral loads together with various mutations, the application of anti-HBc testing to evaluate non-resolved donors provides a better way to enhance blood safety in China. Additionally, some sensitive molecular methods like nested PCR and real-time PCR assay with high extraction volume or nucleic acid hybridization for HBV DNA should be applied to identify OBIs in non-resolved blood donors.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics Statement
This study was reviewed and approved by the ethics committee of the Shenzhen Blood Center. The written and informed consent form was obtained from each donor before donation.
Author Contributions
XY designed the experiments and wrote and reviewed the manuscript. LC reviewed, revised, and edited the manuscript. YZ, RL, TL, XZ, WX, JZ, MX participated in the study design, performed the experiments, and collected and analyzed the data. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by the Nature and Science Fund of Shenzhen and Guangdong (JCYJ20190806112201646 and 2021A515010979) and Shenzhen Key Medical Discipline Construction Fund (SZXK070) to XY and CAMS Initiative for Innovative Medicine (CAMS-2016-I2M-3-025 and CAMS-2017-I2M-B&R-15), National Key Research and Development Program (2018YFE0107500), Science and Technology Partnership Program, Ministry of Science and Technology of China (KY201904011) to LC.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
HBV, Hepatitis B virus; HCV, hepatitis C virus; HIV, human immunodeficiency virus; HBsAg, hepatitis B surface antigen; anti-HBc, hepatitis B core antigen; anti-HBs, hepatitis B surface antibody; HCC, hepatocellular carcinoma; NAT, nucleic acid testing; ELISA(s), enzyme-linked immuno-absorbent assay(s); ECLI, electrochemiluminescence immunoassay; ID, individual donation; LOD, limit of detection; MP(s), mini pool(s); ID, individual donation; NRR, non-repeat reactive; MP6, mini pools of six donations; OBI, occult hepatitis B virus infection; BCP/PC, basic core and pre-core promoter regions.
References
1. Raimondo R, Allain J-P, Brunetto MR, Buendia MA, Chen DS, Colombo M, et al. Statements From the Taormina Expert Meeting on Occult Hepatitis B Virus Infection. J Hepatol (2008) 49(4):652–7. doi: 10.1016/j.jhep.2008.07.014
2. Pollicino T, Squadrito G, Cerenzia G, Cacciola I, Raffa G, Craxi A, et al. Hepatitis B Virus Maintains its Prooncogenic Properties in the Case of Occult HBV Infection. Gastroenterology (2004) 126(1):102–10. doi: 10.1053/j.gastro.2003.10.048
3. Fopa D, Candotti D, Tagny CT, Doux C, Mbanya D, Murphy EL, et al. Occult Hepatitis B Infection Among Blood Donors From Yaoundé, Cameroon. Blood Transfus (2019) 17(6):403–8. doi: 10.2450/2019.0182-19
4. Candotti D, Lin CK, Belkhiri D, Sakuldamrongpanich T, Biswas S, Lin S, et al. Occult Hepatitis B Infection in Blood Donors From South East Asia: Molecular Characterisation and Potential Mechanisms of Occurrence. Gut (2012) 61:1744–53. doi: 10.1136/gutjnl-2011-301281
5. Huang CH, Yuan Q, Chen PJ, Zhang YL, Chen CR, Zheng QB, et al. Influence of Mutations in Hepatitis B Virus Surface Protein on Viral Antigenicity and Phenotype in Occult HBV Strains From Blood Donors. J Hepatol (2016) 57(2):720–9. doi: 10.1016/j.jhep.2012.05.009
6. Yuen MF, Lee CK, Wong DK, Fung J, Hung I, Hsu A, et al. Prevalence of Occult Hepatitis B Infection in a Highly Endemic Area for Chronic Hepatitis B: A Study of a Large Blood Donor Population. Gut (2006) 59:1389–93. doi: 10.1136/gut.2010.209148
7. Candotti D, Assennato SM, Laperche S, Allain J, Levicnik-Stezinar S. Multiple HBV Transfusion Transmissions From Undetected Occult Infections: Revising the Minimal Infectious Dose. Gut (2019) 68:313–21. doi: 10.1136/gutjnl-2018-316490
8. Spreafico M, Berzuini A, Foglieni B, Candotti D, Raffaele L, Guarnori I, et al. Poor Efficacy of Nucleic Acid Testing in Identifying Occult HBV Infection and Consequences for Safety of Blood Supply in Italy. J Hepatol (2015) 63(5):1068–76. doi: 10.1016/j.jhep.2015.06.016
9. Roth WK, Busch MP, Schuller A, Ismay S, Cheng A, Seed CR, et al. International Survey on NAT Testing of Blood Donations: Expanding Implementation and Yield From 1999 to 2009. Vox Sang (2012) 102(1):82–90. doi: 10.1111/j.1423-0410.2011.01506.x
10. Ohhashi Y, Pai A, Halait H, Ziermann R. Analytical and Clinical Performance Evaluation of the Cobas TaqScreen MPX Test for Use on the Cobas s 201 System. J Virol Methods (2010) 165(2):246–53. doi: 10.1016/j.jviromet.2010.02.004
11. Jarvis L, Becker J, Tender A, Cleland A, Queiros L, Aquiar A, et al. Evaluation of the Roche Cobas s 201 System and Cobas TaqScreen Multiplex Test for Blood Screening: A European Multicenter Study. Transfusion (2008) 48(9):1853–61. doi: 10.1111/j.1537-2995.2008.01779.x
12. Ye X, Li T, Shao W, Zeng J, Hong W, Lu L, et al. Nearly Half of Ultrio Plus NAT Nondiscriminated Reactive Blood Donors Were Identified as Occult HBV Infection in South China. BMC Infect Dis (2019) 19:577–87. doi: 10.1186/s12879-019-4215-9
13. Enjalbert F, Krysztof DE, Candotti D, Allain JP, Stramer SL. Comparison of Seven Hepatitis B Virus (HBV) Nucleic Acid Testing Assays in Selected Samples With Discrepant HBV Markers Results From United States Blood Donors. Transfusion (2014) 54:2485–95. doi: 10.1111/trf.12653
14. Zheng X, Ye X, Zhang L, Wang W, Shuai L, Wang A, et al. Characterization of Occult Hepatitis B Virus Infection From Blood Donors in China. J Clin Microbiol (2011) 49:1730–7. doi: 10.1128/JCM.00145-11
15. Yu D, Li X, Mon V, Lu ZH, Liao XW, Han Y, et al. N-Glycosylation Mutations Within Hepatitis B Virus Surface. J hepat (2014) 62(3):515–22. doi: 10.1016/j.jhep.2013.11.004
16. Jiao F, Shen C, Ning J, Zhang T, Chen X, Lu F. HBV T1719G Mutation Reduced HBV Replication Through Mutant Enh II and Hbx Protein in Vitro. J Viral Hepat (2019) 26(6):710–17. doi: 10.1111/jvh.13070
17. Candotti D, Boizeau L, Laperche S. Occult Hepatitis B Infection and Transfusion-Transmission Risk. Transfus Clin Biol (2017) 24(3):189–95. doi: 10.1016/j.tracli.2017.06.014
18. Matanhire TB, Lin SW. An Economic Reappraisal of Hepatitis B Virus Testing Strategy for Blood Donors in Taiwan. Vox Sang (2021) 116(5):564–73. doi: 10.1111/vox.13045
19. Wang L, Chang L, Xie Y, Huang C, Xu L, Qian R, et al. What is The Meaning of a Nonresolved Viral Nucleic Acid Test-Reactive Minipool? Transfusion (2015) 55(2):395–404. doi: 10.1111/trf.12818
20. Weusten J, Vermeulen M, van Drimmelen H, Lelie N. Refinement of a Viral Transmission Risk Model for Blood Donations in Seroconversion Window Phase Screened by Nucleic Acid Testing in Different Pool Sizes and Repeat Test Algorithms. Transfusion (2011) 51(1):203–15. doi: 10.1111/j.1537-2995.2010.02804.x
21. Margaritis AR, Brown SM, Seed CR, Kiely P, D'Agostino B, Keller AJ. Comparison of Two Automated Nucleic Acid Testing Systems for Simultaneous Detection of Human Immunodeficiency Virus and Hepatitis C Virus RNA and Hepatitis B Virus DNA. Transfusion (2007) 47(10):1783–93. doi: 10.1111/j.1537-2995.2007.01343.x
22. Allain J, Mihaljevic I, Gonzalez-Fraile MI, Gubbe K, Holm-Harritshøj L, Garcia JM, et al. Infectivity of Blood Products From Donors With Occult Hepatitis B Virus Infection. Transfusion (2013) 53(7):1405–15. doi: 10.1111/trf.12096
23. Kleinman SH, Lelie N, Busch MP. Infectivity of Human Immunodeficiency Virus-1, Hepatitis C Virus, and Hepatitis B Virus and Risk of Transmission by Transfusion. Transfusion (2009) 49:2454–89. doi: 10.1111/j.1537-2995.2009.02322.x
24. Weusten J, van Drimmelen H, Vermeulen M, Lelie N. A Mathematical Model for Estimating Residual Transmission Risk of Occult Hepatitis B Virus Infection With Different Blood Safety Scenarios. Transfusion (2017) 57(3):841–9. doi: 10.1111/trf.14050
25. Laperche S, Morel P, Deschaseaux M, Bouchardeau F, Alimardani G, Guillaume N, et al. HIV Antibody Screening Remains Indispensable for Ensuring Viral Safety of Blood Components Despite NAT Implementation. Transfusion (2013) 43(10):1428–32. doi: 10.1046/j.1537-2995.2003.00541.x
26. Nübling CM, Heiden M, Chudy M, Kress J, Seitz R, Keller-Stanislawski B, et al. Experience of Mandatory Nucleic Acid Testing (NAT) Screening Across All Blood Organizations in Germany: NAT Yield Versus Breakthrough Transmissions. Transfusion (2009) 49(9):1850–8. doi: 10.1111/j.1537-2995.2009.02212.x
27. Taira R, Satake M, Momose S, Hino S, Suzuki Y, Murokawa H, et al. Residual Risk of Transfusion Transmitted Hepatitis B Virus (HBV) Infection Caused by Blood Components Derived From Donors With Occult HBV Infection in Japan. Transfusion (2013) 53(7):1393–404. doi: 10.1111/j.1537-2995.2012.03909.x
28. Hollinger FB. Hepatitis B Virus Infection and Transfusion Medicine: Science and the Occult. Transfusion (2008) 48(5):1001–26. doi: 10.1111/j.1537-2995.2012.03909.x
29. Hoshi Y, Hasegawa T, Yamagishi N, Mizokami M, Sugiyama M, Matsubayashi K, et al. Optimal Titer of Anti-HBs in Blood Components Derived From Donors With Anti-HBc. Transfusion (2009) 59(8):2602–11. doi: 10.1111/trf.15393
30. Matsumoto C, Tadokoro K, Fujimura K, Hirakawa S, Mitsunaga S, Juji T. Analysis of HBV Infection After Blood Transfusion in Japan Through Investigation of a Comprehensive Donor Specimen Repository. Transfusion (2001) 41(3):878–84. doi: 10.1046/j.1537-2995.2001.41070878.x
31. Levicnik-Stezinar S, Rahne-Potokar U, Candotti D, Lieli N, Allain JP. Anti-Hbs Positive Occult Hepatitis B Virus Carrier Blood Infectious in Two Transfusion Recipients. J Hepatol (2008) 48(5):1022–5. doi: 10.1016/j.jhep.2008.02.016
32. Castells L, Vargas V, Rodríguez-Frías F, Allende H, Jardí R, Margarit C, et al. Transmission of Hepatitis B by Transplantation of Livers From Donors Positive for Antibody to Hepatitis B Core Antigen. Transplant Proc (1999) 31(6):2464–5. doi: 10.1016/s0041-1345(99)00419-4
33. Candotti D, Grabarczyk P, Ghiazza P, Roig R, Casamitjana N, Iudiconeb P, et al. Characterization of Occult Hepatitis B Virus Form Blood Donors Carrying Genotype A2 or Genotype D Strains. J Hepatol (2008) 49(4):537–47. doi: 10.1016/j.jhep.2008.04.017
34. Candotti D, Allain JP. Transfusion-Transmitted Hepatitis B Virus Infection. J Hepatol (2009) 51(4):798–809. doi: 10.1016/j.jhep.2009.05.020
35. Allain JP, Cox L. Challenges in Hepatitis B Detection Among Blood Donors. Curr Opin Hematol (2011) 18:461–6. doi: 10.1097/MOH.0b013e32834bac10
36. Akcam FZ, Demir C. Acute Hepatitis B Infection Due to Erythrocyte Suspension Obtained From 'Anti-HBc Alone' Positive Donor. Transf Med (2005) 15:61–2. doi: 10.1111/j.1365-3148.2005.00551.x
37. Oluyinka OO, Tong HV, Bui Tien S, Fagbami AH, Adekanle O, Ojurongbe O, et al. Occult Hepatitis B Virus Infection in Nigerian Blood Donors and Hepatitis B Virus Transmission Risks. PloS One (2005) 10(1):131–9. doi: 10.1371/journal.pone.0131912
38. Urbani S, Fagnoni F, Missale G, Franchini M. The Role of Anti-Core Antibody Response in the Detection of Occult Hepatitis B Virus Infection. Clin Chem Lab Med (2010) 48(1):23–9. doi: 10.1515/CCLM.2010.002
39. Vermeulen M, Coleman C, Walker E, Koppleman M, Lelie N, Reddy R. Transmission of Occult HBV Infection by ID-NAT Screened Blood. Vox Sang (2014) 107(Suppl 1):146–8. doi: 10.1111/trf.12218
40. Seed CR, Maloney R, Kiely P, Bell B, Keller A, Pink J, et al. Infectivity of Blood Components From Donors With Occult Hepatitis B Infection – Results From an Australian Look Back Programme. Vox Sang (2015) 108(1):113–22. doi: 10.1111/vox.12198
41. Stramer SL, Wend U, Candotti D, Foster GA, Hollinger FB, Dodd RY, et al. Nucleic Acid Testing to Detect HBV Infection in Blood Donors. N Engl J Med (2011) 364(3):236–47. doi: 10.1056/NEJMoa1007644
42. Hourfar MK, Walch LA, Geusendam G, Dengler T, Janetzko K, Gubbe K, et al. Sensitivity and Specificity of Anti-HBc Screening Assays – Which Assay Is Best for Blood Donor Screening? Int J Lab Hematol (2009) 31:649–56. doi: 10.1111/j.1751-553X.2008.01092.x
43. Busch MP. Should HBV DNA NAT Replace HBsAg and/or Anti-HBc Screening of Blood Donors? Transfus Clin Biol (2004) 11:26–32. doi: 10.1016/j.tracli.2003.12.003
44. Dodd RY, Nguyen ML, Krysztof DE, Notari EP, Stramer SL. Blood Donor Testing for Hepatitis B Virus in the United States: Is There a Case for Continuation of Hepatitis B Surface Antigen Detection? Transfusion (2018) 58:2166–70. doi: 10.1111/trf.14784
45. Ye X, Yang B, Zhu W, Zheng X, Du P, Zeng J, et al. Six-Year Pilot Study on Nucleic Acid Testing for Blood Donations in China. Trans Aphe Sci (2013) 49(2):318–22. doi: 10.1016/j.transci.2013.08.005
46. Cun W, He Q, Zhang J, Xiang Z. Cost Benefit Analysis of 43 714 Donors Blood Nucleic Acid Testing Applied to Screening in Wuhan, China. Chin J Blood Transfusion (2014) 27:166–8. doi: 10.13303/j.cjbt.issn.1004-549x.2014.02.0019
47. Hass M, Hannoun C, Kalinina T, Sommer G, Manegold C, Gunther S. Functional Analysis of Hepatitis B Virus Reactivating in Hepatitis B Surface Antigen-Negative Individuals. Hepatology (2005) 42(1):93–103. doi: 10.1002/hep.20748
Keywords: blood safety, occult hepatitis B infection, nucleic acid testing, anti-HBc, minipool
Citation: Ye X, Zhao Y, Li R, Li T, Zheng X, Xiong W, Zeng J, Xu M and Chen L (2021) High Frequency Occult Hepatitis B Virus Infection Detected in Non-Resolved Donations Suggests the Requirement of Anti-HBc Test in Blood Donors in Southern China. Front. Immunol. 12:699217. doi: 10.3389/fimmu.2021.699217
Received: 26 April 2021; Accepted: 12 July 2021;
Published: 28 July 2021.
Edited by:
Wolfram Gerlich, Justus Liebig University, GermanyReviewed by:
Roger Dodd, American Red Cross, United StatesFerruccio Bonino, Institute of Biostructure and Bioimaging (CNR), Italy
Tomasz I. Michalak, Memorial University of Newfoundland, Canada
Copyright © 2021 Ye, Zhao, Li, Li, Zheng, Xiong, Zeng, Xu and Chen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Limin Chen, bGltaW5fY2hlbl85OUAxMjYuY29t; bGltaW4uY2hlbkBpYnQucHVtYy5lZHUuY24=