 Guillaume Larid1
Guillaume Larid1 Mikael Pancarte2Géraldine Offer2
Mikael Pancarte2Géraldine Offer2 Cyril Clavel2
Cyril Clavel2 Marielle Martin3Vincent Pradel4Isabelle Auger3Pierre Lafforgue1
Marielle Martin3Vincent Pradel4Isabelle Auger3Pierre Lafforgue1 Jean Roudier1,3Guy Serre2
Jean Roudier1,3Guy Serre2 Nathalie Balandraud1,3*
Nathalie Balandraud1,3*- 1Rhumatologie, Institut du Mouvement et de l'appareil Locomoteur (IML), Assistance Publique - Hôpitaux de Marseille (AP-HM), Marseille, France
- 2Université de Toulouse, INSERM, UMRs 1056, UDEAR, Hôpital Purpan, Toulouse, France
- 3Aix Marseille Université, INSERM UMRs 1097, Arthrites autoimmunes, Marseille, France
- 4CEIP de Marseille (PACA-Corse, Centre Associé), Laboratoire de Santé Publique, Faculté de Médecine, Marseille, France
Objectives: Rheumatoid arthritis (RA) is associated with HLA-DRB1 genes encoding the shared epitope (SE), a 5-amino acid motive. RA is usually preceded by the emergence of anti-citrullinated protein/peptide antibodies (ACPAs). Citrulline is a neutral amino acid resulting from post-translational modification of arginine involved in peptidic bounds (arginyl residue) by PeptidylArginine Deiminases (PADs). ACPAs recognize epitopes from citrullinated human fibrin(ogen) (hFib) and can be specifically detected by the AhFibA assay. Five citrullinated peptides derived from hFib together represent almost all of the epitopes recognized by patients with ACPA-positive RA, namely: α36–50cit, α171–185cit, α501–515cit, α621–635cit, and β60–74cit. The use of antibody fine specificities as markers of clinical phenotypes has become a major challenge. Our objective was to study whether RA clinical characteristics and HLA-DRB1 genetic background were associated with a specific reactivity against the epitopes borne by the five peptides.
Methods: 184 ACPA-positive RA patients fulfilling the 2010 ACR/EULAR criteria were studied. Patient characteristics including HLA-DRB1 genotype, were collected from their medical files. Anti-CCP2 antibodies, AhFibA, and antibodies against the five citrullinated hFib (hFib-cit) peptides were analyzed by ELISA.
Results: Anti-α505-515cit antibodies were associated with HLA-DRB1*04:01 (OR = 5.52 [2.00 – 13.64]; p = 0.0003). High level anti-α505-515cit antibodies were associated with rheumatoid nodules (OR = 2.71 [1.00 – 7.16], p= 0.044).
Conclusion: Immune complexes containing anti-α501-515cit antibodies and rheumatoid factors might be involved in the development of rheumatoid nodules on the HLA-DRB1*04:01 background. Apheresis of these epitope-specific antibodies might be a new therapeutic opportunity for patients with rheumatoid nodules.
Introduction
Rheumatoid arthritis (RA) is the most severe type of chronic autoimmune arthritis. Its prevalence ranges from 0.5% to 1.1% in North America and northern Europe, and between 0.3 and 0.7% in southern Europe (1).
RA features symmetrical bilateral polyarthritis of the small joints. Extra-articular manifestations such as rheumatoid nodules, lung damage, or vasculitis can also be present (2).
RA is usually preceded by the emergence of anti-citrullinated protein/peptide antibodies (ACPAs) and rheumatoid factors of various isotypes. Citrullyl is a neutral residue resulting from post-translational modification of an arginyl residue in the peptidic sequence by PeptidylArginine Deiminases (PADs). The deiminated protein/peptide is said citrullinated.
In ACPA-positive RA, the genetic risk is mostly carried by shared epitope (SE)-positive HLA-DR molecules. The SE (a five-amino acid motif encompassing positions 70 to 74 of the HLA-DRB1 chain) encoded in the major histocompatibility complex (MHC) is present in approximately 70% of patients with ACPA-positive RA (3). Different combinations of HLA-DR alleles (genotypes) confer different relative risks of developing ACPA-positive RA, with highest risks for genotypes encoding two copies of the SE (4).
ACPA present in patients with RA recognize citrullinated epitopes on various proteins (5). A major citrullinated autoantigen expressed in the rheumatoid joint is fibrin, both its alpha and beta chain being recognized by ACPA (6). ACPA are likely to play a role in the pathophysiology of the disease. Indeed, ACPAs have been shown to predict progression of undifferentiated arthritis to RA and are associated with severe disease (7). However, given the heterogeneity of the disease’s clinical features, more reliable prognostic and phenotypic markers are missing.
The discovery of ACPA led to the development of diagnostic tests based on a first synthetic cyclic citrullinated peptides (CCP) (8). Since then, several generations of anti-CCP tests have been commercialized (9). ACPAs have become one of the 2010 American College of Rheumatology (ACR)/EULAR RA classification criteria (10).
Besides anti-CCP tests, a test for autoantibodies to human citrullinated fibrinogen (AhFibA) can be used for the serological diagnosis of early RA (11).
Five peptides from human citrullinated fibrinogen (hFib-cit) together contain almost all of the epitopes recognized by patient’s sera with ACPA-positive RA. These immunodominant epitopes are borne by the peptides α36–50cit38,42, α171–185cit178,181, α501–515cit510,512, α621–635cit621,627,630 and β60–74cit60,72,74 (6, 12, 13). Whether reactivity of sera toward these five peptides might allow definition of subgroups among RA patients that might have different disease phenotypes, is an important question.
Previous studies analyzed the recognition by various samples of patients of only 3 (α36–50cit, β60–74cit and FibCit α621-635) out of the 5 major peptides, and only studied early RA defined by the 1987 ACR criteria (14) and not the 2010 ACR/EULAR criteria.
The primary objective of this work was to study whether, in a cohort of 184 patients with ACPA-positive RA fulfilling the 2010 ACR/EULAR criteria, a particular HLA-DR background or original clinical patterns, were associated with antibodies to the epitopes from the 5 major hFib-cit peptides α36–50cit, α171–185cit, α501–515cit, α621–635cit, and β60–74cit.
Material and Methods
Patients
We undertook a prospective study on 184 patients followed at the rheumatology department of Sainte Marguerite Hospital in Marseille. Patients included were considered ACPA-positive RA based on previous results of anti-CCP2 antibodies obtained with various commercial assays, and fulfilled the 2010 ACR/EULAR criteria. Patients treated with Rituximab were excluded due to its potential effect on ACPA levels.
Patient characteristics were collected from their medical files: presence of rheumatoid nodules, smoking habits, age at diagnosis, HLA-DR genotype, IgM rheumatoid factor (RF), activity and erosive characteristics of the disease, treatment response, dry eye syndrome, cardiovascular event, osteoporosis.
-In order to state the presence or absence of rheumatoid nodules, patients medical files and all available chest CT scans were analyzed.
-Disease activity was measured using the Disease Activity Score calculated with the level of C-reactive protein (DAS28-CRP) on the day of the sample.
-Treatment response was evaluated according to the EULAR response criteria. Patients were considered to have shown a good response if their DAS28 was ≤3.2 or has decreased by >1.2 (15) according to the 2019 update of EULAR recommendations for the management of RA, the time needed to achieve treatment target has been set at 6 months before concluding to treatment failure (16).
-Patient personal history of a cerebrovascular accident, myocardial infarction or heart failure was defined as a major cardiovascular event.
-Patients were categorized as smokers (active or previous smokers) or non-smokers.
-Erosive RA was defined according to the EULAR definition of erosive RA (17).
-Dry eye syndrome was defined as a Schirmer's test value ≤ 5 mm/5 min, or an Ocular Staining Score ≥ 5. Dry mouth was defined as an unstimulated salivary flow rate of ≤ 0,1 mL/min.
-Osteoporosis was defined either by personal history of osteoporosis fracture, or by bone mineral density with a T-score below – 2,5 for at least one of the testing sites.
Samples
Patients gave a single blood sample from which plasma was isolated. Samples were stored at -80°C. AhFibA and ACPA fine specificities were assayed and anti-CCP2 were re-assayed with a same test in all patients.
Ethics
All patients gave informed written consent for this study. Patient data was pseudo-anonymized. Sample collection was approved by the ethics committee under the number DC-2008-327. This study was declared to the Assistance Publique – Hôpitaux de Marseille (AP-HM) under the number PADS19-332.
ACPA Testing
For all the ACPA tests, we used the positivity threshold (N) corresponding to 95% diagnostic specificity.
Plasma anti-CCP2 assays were performed using the ELISA CCPlus® IMMUNOSCAN kit (Euro Diagnostica, Arnhem, The Netherlands) according to the manufacturer’s recommendations. Antibody titers expressed in arbitrary units (AU/mL) were considered positive above 25 AU/mL.
Anti-human citrullinated fibrinogen IgG autoantibodies were detected with a previously described ELISA (AhFibA). Antibody “titers” (ELISA optical density) above 0.056 were considered positive (6, 18).
Rheumatoid Factor Testing
IgM Rheumatoid Factor (RF) was assayed with the RF ELISA from Orgentec and considered positive if >20 UI/mL.
Antibodies to Human Fibrin(ogen) Citrullinated Peptides
Peptides with the following sequences were synthetized with either arginines (R) in control peptides or citrullines (R) in target peptides, and used as immunosorbents:
-α36-50: GPRVVERHQSACKDS
-α171-185: biotin-ahx*-VDIDIKIRSCRGSCS
-α501-515: biotin-ahx*-SGIGTLDGFRHRHPD
-α621-635: RGHAKSRPVRGIHTS
-β60-74: RPAPPPISGGGYRAR
*: ahx: aminohexanoic acid
IgG autoantibodies to the fibrinogen-derived citrullinated peptides α36-50cit, α621-635cit and β60-74cit were tested by ELISA according to a previously described method in which peptides are passively adsorbed on polystyrene microtitration plates (6, 18). IgG autoantibodies to the peptides α171-185cit and α501-515cit were tested by ELISA with biotinylated peptides linked to previously adsorbed Avidin. Briefly, plates (Maxisorp; NUNC, VWR International, Fontenay-sous-Bois, France) were incubated overnight with Avidin at 5 µg/mL. After washing with PBS 0.1% Tween-20 (PBS-T) biotinylated peptides were incubated for 1 hour at 1µg/mL in PBS 2% BSA (PBS-BSA). After 3 washings the plates were incubated for 1 hour with patient plasma diluted to 1/100 in PBS-BSA then washed 3 times in PBS-T. A peroxidase-conjugated goat anti-human IgG antibody (Southern Biotechnology) diluted to 1/2500 in PBS-BSA was incubated for 1h and, after 3 washings, reactivity was revealed by ortho-phenylenediamine dihydrochloride and hydrogen peroxide in a pH5 citrate buffer. The reaction was stopped after 5 min with H2SO4 and optical density (OD) read at 492 nm. All the steps were performed at room temperature around 20°C (6). The specific antibody reactivity was defined as the OD difference between the citrullinated and the non-citrullinated related control peptide. Interassay variations were corrected by linear regression analysis using reference peptide and plasma, tested on each plate. ΔOD below the cut-off value of 0.25 were considered negative. Patients with ΔOD over the cut-off were divided into 3 equal groups (tertiles) with weak (T1), medium (T2) or high titers (T3). Patients from the medium and high-titer groups (T2-T3 combined) were considered together to have a “high level” reactivity.
Statistical Analysis
Association studies were carried out with contingency tables using the Chi2 test and Fisher’s exact test when Chi2 was not applicable.
The Baptista-Pike method was used to obtain the 95% confidence interval for Odds Ratio (OR).
Spearman’s rank correlation coefficient rho was used to measure the correlations between anti-CCP2 antibodies, AhFibA, and antibodies to the 5 peptides and tested against the null hypothesis of rho =0.
Statistical analysis was carried out using PRISM software for Windows (GraphPad Software, 169 San Diego, California, USA) and IBM®SPSS® Statistics version 20. The significance threshold was set at p < 0.05.
Results
Clinical Description of the Population
The clinical characteristics of the 184 patients with ACPA-positive RA are shown in Table 1 (see details in Supplementary Data File 1). Half of patients were treated with methotrexate, 24% in monotherapy, and 76% in association with a bDMARD. Among 30 patients with rheumatoid nodules, 15/93 had methotrexate, 15/97 had not (p = 0.841, OR = 0.923 [0.44 – 1.941]).
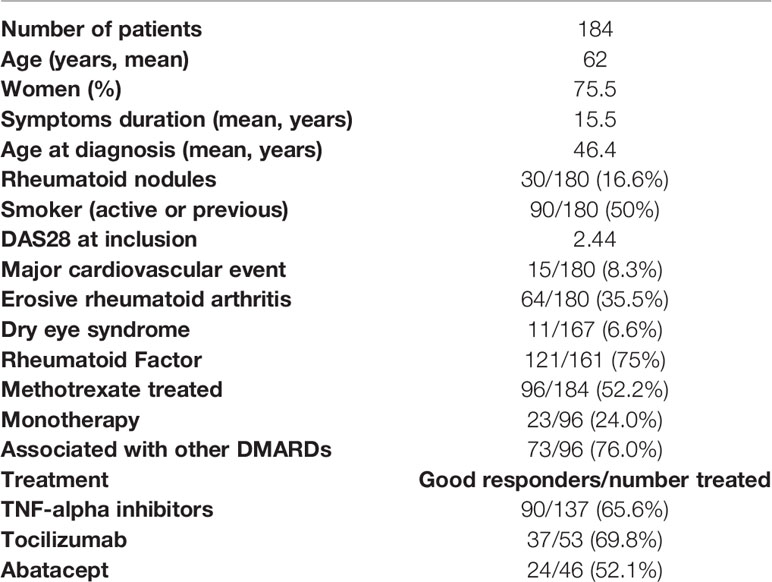
Table 1 Clinical characteristics of patients.
Serological Profile of the 184 Patients With ACPA-Positive RA
The biological characteristics of the 184 patients recruited as ACPA-positive RA based on their anti-CCP2 status are shown in Table 2 (see details in Supplementary Data File 1). When re-assayed with the same reference assay, 98.51% of patients had anti-CCP2 antibodies. On the other hand, 83.23% had AhFibA, and 69.98% had IgM RF.
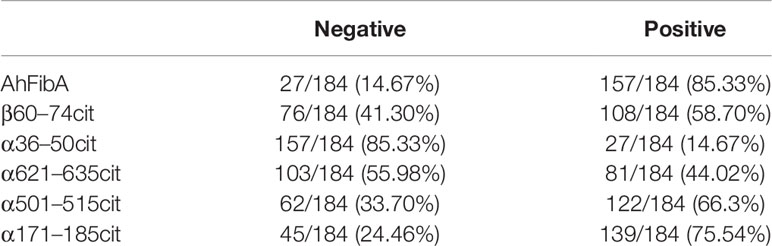
Table 2 AhFibA and five major citrullinated Fibrin peptides antibodies.
Among the Citrullinated Peptides
Among the citrullinated peptides, 76.13% of patients recognized biotin-α171-185cit, 67.10% recognized biotin-α501-515cit, 58.06% recognized β60-74cit, 45.16% recognized α621-635cit, and 14.84% recognized α36-50cit.
Epitopic Profiles of ACPA
Analysis of the profiles of epitope recognition in the 184 patients showed that 19% of patients recognized the 4 peptides α171-185cit, α501-515cit, α621-635cit, and β60-74cit, 15% of patients recognized the 3 peptides α171-185cit, α501-515cit, and β60-74cit, and 6% of patients recognized a single peptide (4%: α171-185cit, 1%: α501–515cit, and 1%: β60–74cit) (see Figure 1).
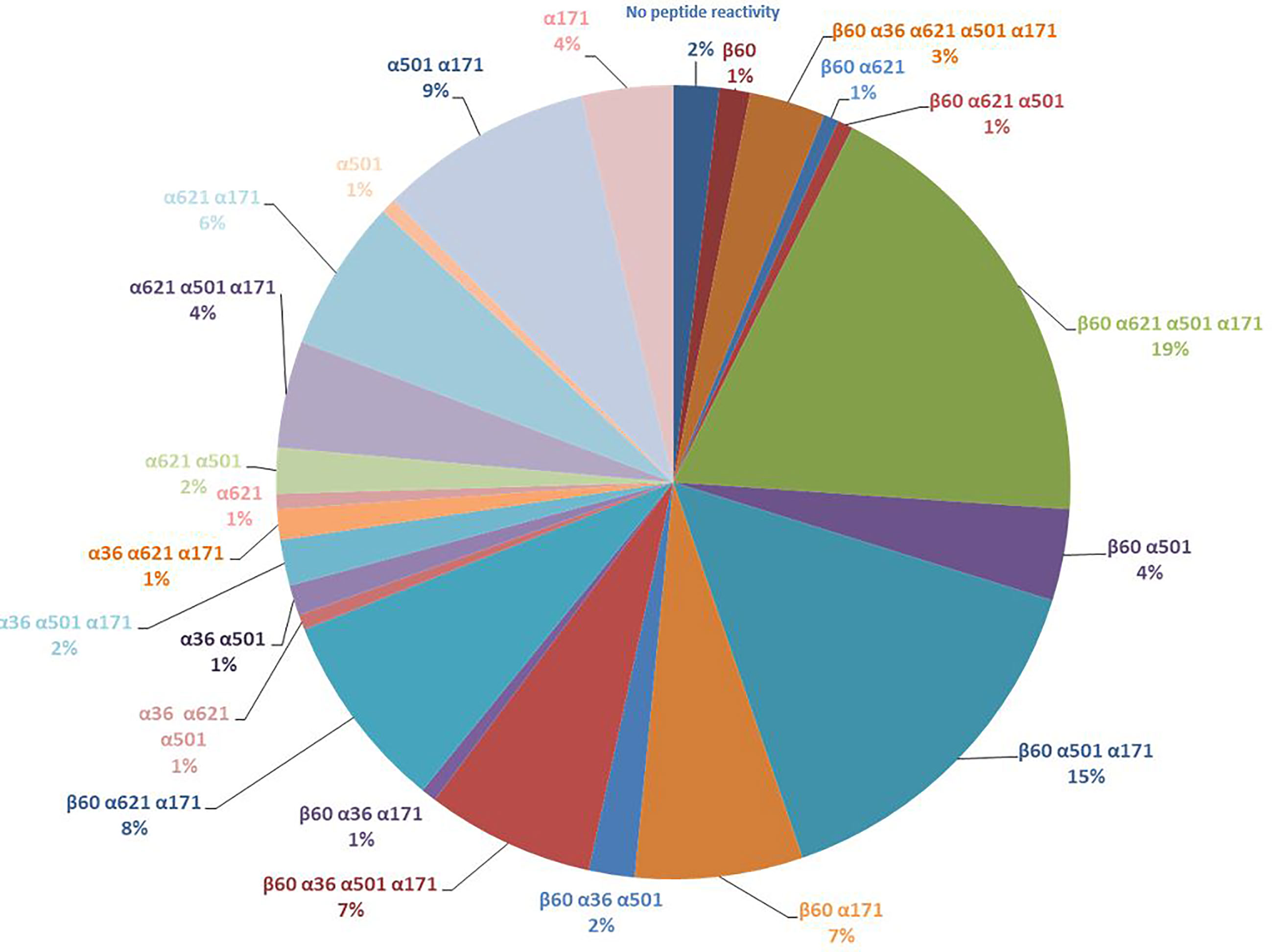
Figure 1 Different profiles of epitopic reactivity in the cohort of 184 patients.
Correlations of the Titers of Anti-CCP2 and Anti-Citrullinated Fibrin Peptide Antibodies
The titers of anti-CCP2 and AhFibA were strongly correlated (Spearman’s rank correlation coefficient rho (rs): 0.706; p= 4.06x10-29).
The titers of anti-CCP2 and anti-citrullinated fibrin peptides antibodies were also significantly correlated for 4 of the 5 peptides: α171-185cit (rs: 0.647; p = 3.2x10-23), α501-515cit (rs: 0.299; p = 3.7x10-5), α621-635cit (rs: 0.271; p= 0.0002), β60-74cit (rs: 0.517; p = 5.5x10-14).
By contrast there was no correlation of anti-CCP2 antibodies titers with those of anti-α36-50cit antibodies (rs: -0.010; p = 0.894) (see Figure 2).
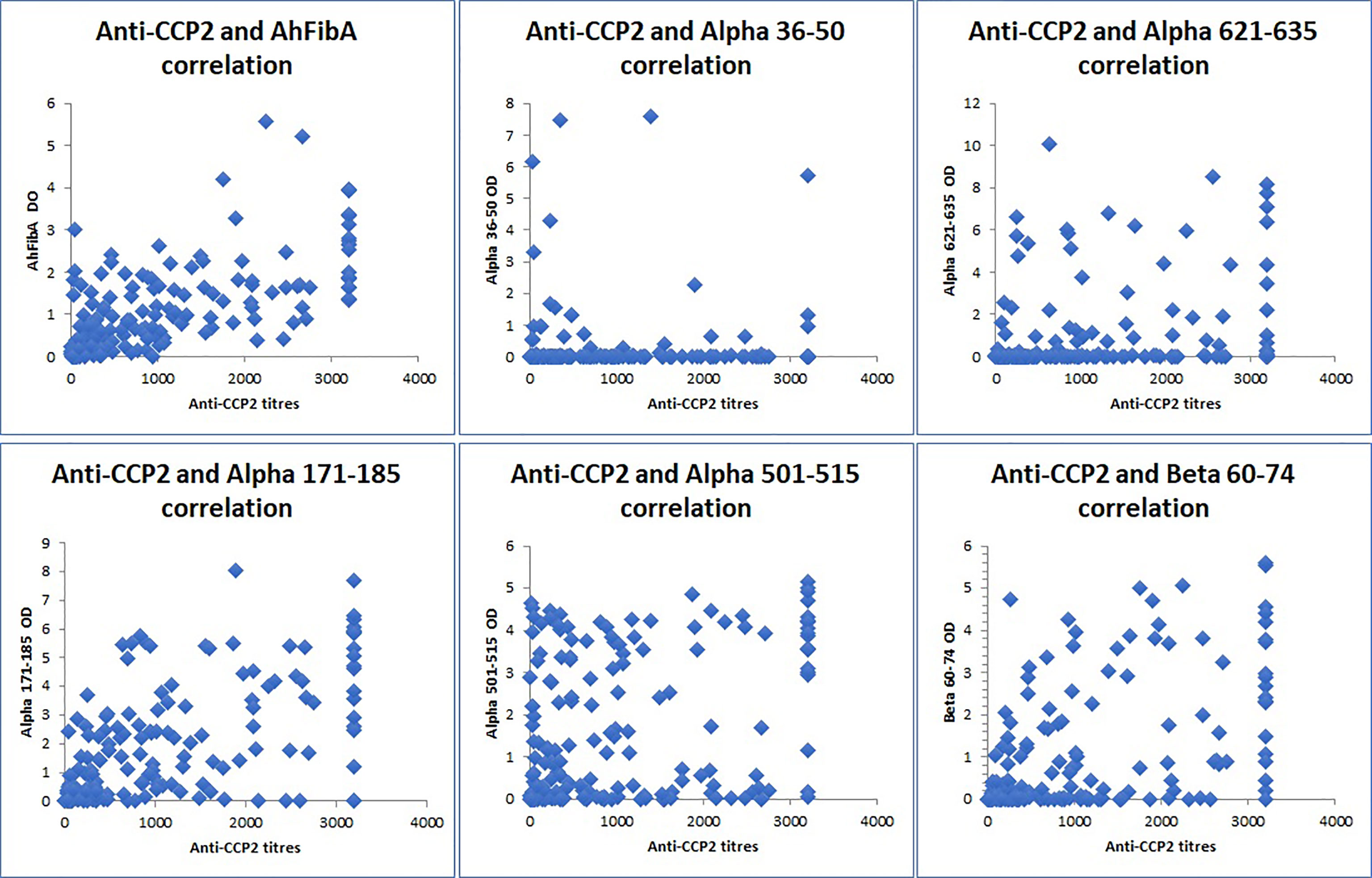
Figure 2 Correlations of anti-CCP2 titers and anti-citrullinated fibrin peptides antibodies (Spearman’s rank correlation coefficient rho (rs). OD , optical density; AhFibA , anti-citrullinated human fibrinogen antibodies; anti-CCP2, anti-cyclic citrullinated peptides. There was a positive correlation between anti-CCP2 and AhFibA (rs : 0.706; p = 4.06x10-29), between anti-CCP2 and anti-α171-185cit (rs: 0.647; p = 3.2x10-23), anti-α501-515cit (rs: 0.299; p = 3.7x10-5),anti-α621-635cit (rs: 0.271; p= 0.0002), and anti-β60-74cit antibodies (rs: 0.517; p = 5.5x10-14). There was no correlation between anti-CCP2 and anti α36–50 (rs: -0.010; p = 0.894) antibodies.
HLA-DRB1 Background
Among the 184 patients with ACPA-positive RA, 155 were genotyped for HLA-DRB1: 67.1% of patients were SE-positive (49% of patients expressed one copy of the SE, 18.1% expressed two copies). Their clinical characteristics were not different from those in the total 184 patients (see Supplementary Tables 1, 2, Supplementary Data File 1).
HLA-DR Status Association With Clinical Characteristics
HLA-DRB1*04:01 was weakly associated with rheumatoid nodules. Indeed, 44/155 patients expressed HLA-DRB1*04:01 of whom 11 (25%) had rheumatoid nodules, 111/155 patients did not express HLA-DRB1*04:01 of whom 19 (17%) had rheumatoid nodules (Chi2, OR = 2.15 [0.91 – 5.25]; p = 0.081). Other clinical characteristics were not associated with any HLA-DRB1 allele.
HLA-DRB1 Status Association With the Recognition of Citrullinated Peptides
SE Dose Effect on the Number of Peptides Recognized
Patients with two copies of the SE were more likely to recognize more than 3 peptides (OR = 3.02 [1.12 – 8.74]; p = 0.034) (see Table 3).

Table 3 Association between epitopic specificity of ACPAs and HLA-DRB1 alleles.
HLA-DRB1 Alleles and Epitopic Specificity
HLA-DRB1*04:01 was associated with antibodies to α501-515 (OR = 5.52 [2.00 – 13.64]; p = 3x10-4). Conversely, HLA-DRB1*04:01 was associated with absence of antibody to α621-625 (OR=0.46 [0.23 – 0.95]; p=0.036) (see Table 3).
Epitopic Specificity of Anti-Citrullinated Fibrin Peptide Antibodies and Clinical Characteristics
Multiple Peptide Recognition
42 of 184 patients recognized more than 3 citrullinated peptides. The 142 remaining patients recognized 3 peptides or less. Patients who recognized more than 3 peptides showed better responses to TNF-alpha inhibitors (OR = 2.93 [1.16 – 7.48]; p = 0.025) and had less often erosive RA (OR = 0.45 [0.19 – 1.04]; p = 0.051) (see Supplementary Table 3).
Recognition of the α501-515 Citrullinated Peptide Was Associated With Rheumatoid Nodules and With RF
Rheumatoid nodules were present in 30/180 patients, absent in 130 patients, data being unknown for 20 patients. On the whole group of patients, reactivity against α501-515cit tended to be associated with rheumatoid nodules (OR= 2.32 [0.95 -5.80], p = 0.08) but high level reactivity against the peptide was significantly associated with rheumatoid nodules (see Table 4). Indeed, 79/184 (43%) patients had high level reactivity against α501-515cit and among them 18/184 (10%) patients had rheumatoid nodules whereas 61/184 (33%) patients had low level reactivity against α501-515cit of whom only 6/184 (3%) patients had rheumatoid nodules (OR=2.71 [1.00 – 7.16], p=0.044).
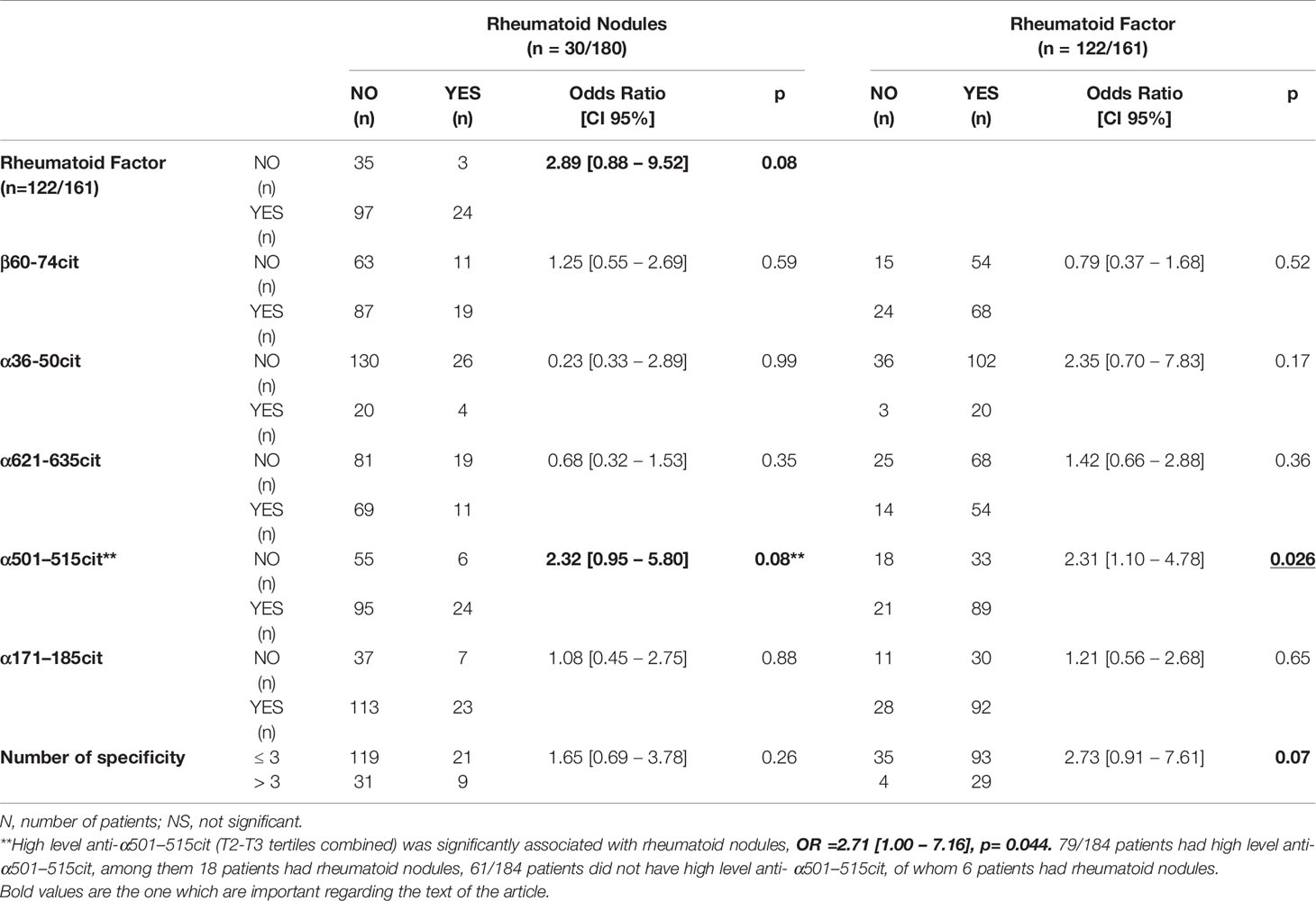
Table 4 Rheumatoid nodules and Rheumatoid factor association with peptide reactivity.
Anti-α501-515cit antibodies were also associated with RF (OR=2.31 [1.10 – 4.78], p= 0.026).
Discussion
We studied the associations between HLA-DR background, specificity of ACPAs to epitopes borne by citrullinated fibrin peptides and clinical characteristics in 184 patients with ACPA-positive RA fulfilling the ACR/EULAR 2010 criteria.
The Clinical and Biological Characteristics
The clinical and biological characteristics of the RA population studied here were classical. In our population of patients with ACPA-positive RA, 17% of patients had rheumatoid nodules which is in accordance with other European populations prevalence of 18%-22.4% and less than in northern European population (30-40%) (19). It was previously reported that cvDMARDs or bDMARDs could accelerate rheumatoid nodulosis, particularly methotrexate (20) and TNF-alpha inhibitors (21). In our cohort we could not find any over-representation of rheumatoid nodules in patients treated with DMARDs, specially with methotrexate.
Prevalence of ACPAs to the Citrullinated Fibrin Peptides
The prevalence of antibodies to the peptides α36-50cit (15%), α621-635cit (45%), and β60-74cit (58%), were in close agreement with those previously described with the same ELISAs (11, 13, 22–26) and also those recently described in very large cohorts of patients with a multiplex peptide chip (27–32). The pilot study (6) which identified the peptides bearing the immunodominant epitopes, only used sera selected for highest titers of ACPA, therefore leading to prevalences which are not representative of patient population.
The prevalence of antibodies to the peptides α171-185cit (76%) and α501-515cit (67%) had been previously studied by ELISA only in the pilot study (6) and were 45% for the 2 peptides. However in the present study, the peptides were used biotinylated and linked to Avidin versus immunoadsorbed on solid phase in the pilot study. Such an increased reactivity when using biotinylated peptides, depending on a different presentation of the peptides, was clearly demonstrated with the peptide β60-74cit in a recently published study (33).
Association Between Multiple Peptide Recognition and Clinical Characteristics
Multiple peptide recognition (>3) was not associated with erosive arthritis, in accordance with previous studies that showed that the diversity of recognized epitopes was not associated with the severity of the disease (34, 35). Multiple peptide recognition (>3) was associated with a better response to TNF-alpha inhibitors in our cohort. In the literature, ACPA have been associated either with a reduced response (36), no effect (37) or a better response (38). A better response to TNF-alpha inhibitors may explain the less erosive pattern observed in our patients with multiple peptide recognition. Indeed, TNF-alpha inhibitors limit radiographic progression in patients with RA as already demonstrated (39).
A study of van Beers et al. (40) failed to find association between ACPA fine-specificity profiles in early rheumatoid arthritis patients and clinical features at baseline or with disease progression, however, the citrullinated peptides used in our study were not analyzed, neither rheumatoid nodules.
Recently, Manca et al. studied the clinico-serological association of ACPA detected using VCP1 and VCP2 (EBV-derived citrullinated peptides) and HCP1 and HCP2 (histone-H4-derived citrullinated peptides) in 413 established RA. Higher number/levels of ACPA subtypes were associated with lung involvement but not with erosive disease (41).
In Joshua and al. association between ACPA fine specificities and lung abnormalities were studied. Three out of our 5 antibodies (FibCit α36-50, FibCit β60-74, and FibCit α621-635) were used in the study. There was no association between reactivity to any of them and lung abnormalities studied by HR-CT scan but in contrast a significant correlation when reactivity to the various fibrin peptides was considered as a whole (42).
Here, CT scanners were not available for the whole population studied, so we could not confirm any association between number of specificities and lung involvement.
Association Between Particular Anti-Citrullinated Fibrin Peptide Antibodies, HLA Background, and Clinical Characteristics
We found that: 1/HLA-DRB1*04:01 was associated with anti-α501-515cit antibodies, 2/Rheumatoid nodules were associated with HLA-DRB1*04:01, 3/”High level” anti-α501–515cit antibodies were associated with rheumatoid nodules and with IgM rheumatoid factor.
HLA-DRB1*04:01 Was Associated With Anti-α501–515cit Antibodies
Associations between fine-specificity antibodies and the presence of the SE have been already analyzed.
Pratesi et al. studied viral citrullinated peptides (VCP) derived from Epstein-Barr virus nuclear proteins EBNA-1 and EBNA-2. Analyzing the contribution of individual SE alleles, the *0401 allele conferred an increased risk to produce anti-VCP2 (p = 0.007) and anti-CCP2 (p = 0.02) antibodies whereas *0404 was associated with the production of anti-VCP1 (p = 0.05) and anti-VCP2 (p = 0.04) antibodies (43).
The C. Terao et al. study (29) investigated whether subtle differences in ACPA serological profiles might be connected to different driving HLA alleles, by analyzing 18 ACPA fine-specificities in RA-affected individuals. A clustering of the peptide reactivities led to divide the patients as having “non-canonical” (including CCP2-negative) or “canonical” serologies (including CCP2-positive). When associations with HLA-A, B, and DR alleles were analyzed, a significant association with aspartic acid residue at Bpos-9 was found between patients with non canonical serologies and an inverse correlation with the canonical ones. In the multiplex peptide array used in that study, 7 peptides from Fibrinogen were present among the 18 tested but only 3 of our 5 peptides, namely α36–50cit, α621–635cit, and β60–74cit. Thus, our study appears as the first correlation analysis of HLA-DR and reactivities to α171–185cit and α501–515cit.
Here, HLA-DRB1*04:01 was associated with anti-α501–515cit antibodies.
In the development of IgG antibody responses, HLA-DR molecules intervene by presenting antigenic peptides to T follicular helper (Tfh) lymphocytes that provide help to B lymphocytes with surface IgM of a given specificity. Specificity of the antibody response relies on the IgM molecule on the B lymphocyte, not on the antigenic peptide presented by-HLA-DR. Thus, association of HLA-DRB1*04:01 with anti-α501-515cit antibodies does not indicate that this RA-associated allele is capable to choose between different B cell epitopes. Rather it suggests that HLA-DRB1*04:01 can provide help to B lymphocytes specific for the α501-515cit peptide and that others HLA-DR alleles can’t. This suggests special efficacy of HLA-DRB1*04:01 as a peptide processor and presentator which in turn allows the development of a more efficient Tfh response. HLA-DR molecules encoded by HLA-DRB1*04:01 have been shown to undergo a shortcut from endoplasmic reticulum to lysosomes which allows association with better processed antigenic peptide (44, 45).
HLA-DRB1*04:01 Was Associated With Rheumatoid Nodules
Association of HLA-DRB1*04:01 with rheumatoid nodules is classical. More, in a studied population, rheumatoid nodule frequency correlates directly with the prevalence of HLA-DRB1*04:01 of this population (19).
“High Level” Anti-α501-515cit Antibodies Were Associated With Rheumatoid Nodules and With IgM Rheumatoid Factor
Association between high level anti-α501-515cit antibodies, RF and rheumatoid nodules refers to rheumatoid nodules nature. As previously described, they contain fibrin and IgG but nothing is known about the specificity of those IgG. Necrotic centers were shown to contain citrullinated proteins and RF (46, 47). Our data suggests that at least some of the IgG are anti-α501-515cit antibodies. They might form immune complexes with citrullinated fibrin secondarily transformed in macroimmune complexes by rheumatoid factors (48, 49) and be at the origin of rheumatoid nodules.
That link of reactivity to a particular fibrinogen peptide and the presence of rheumatoid nodules needs to be further examined and replication studies must be performed. Moreover, while these findings raise new hypothesis about the pathogenesis of rheumatoid nodules, no study of antigen specificity of the IgG present in the nodules has been performed to date. It could be the purpose of further investigations.
In this cohort we analyzed the epitopic specificity of ACPAs using five major citrullinated fibrin peptides which bear the immunodominant ACPA epitopes and checked whether the specificity was associated with particular clinical, biological, or genetic patterns. Our main finding is the association of antibodies to the epitope borne by the citrullinated peptide α501–515 on the alpha chain of fibrin, with HLA-DRB1*04:01 and with rheumatoid nodules. This unexpected epitope specificity of ACPAs in HLA-DRB1*04:01 patients may relate to the original intracellular route of HLA-DRB1*04:01. The association of anti-α501-515cit antibodies with rheumatoid nodules may suggest that the antibodies to the epitope borne by the α501-515cit peptide particularly contribute to the immune complexes in rheumatoid nodules. This finding pave the way of a potential treatment of rheumatoid nodules by purifying patient’s serum from this particular ACPA subtype.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Comité d’éthique Aix Marseille Université - DC-2008-327. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
NB, GS, and GL designed research and analyzed data. MM, NB, and IA collected samples. MP, GO, and CC tested and analyzed fine specificities. VP performed statistical analysis. GL, NB, and PL analyzed patients files. GL, NB, and JR wrote the manuscript. NB, JR, and GS corrected the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This study was supported by INSERM.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors would like to thank all physicians who participated in the diagnostics and therapy of the presented patients.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2021.692041/full#supplementary-material
References
1. Alamanos Y, Drosos A. Epidemiology of Adult Rheumatoid Arthritis. Autoimmun Rev (2005) 4:130–6. doi: 10.1016/j.autrev.2004.09.002
2. Smolen JS, Aletaha D, McInnes IB. Rheumatoid Arthritis. Lancet (2016) 388:2023–38. doi: 10.1016/S0140-6736(16)30173-8
3. Gregersen PK, Silver J, Winchester RJ. The Shared Epitope Hypothesis. An Approach to Understanding the Molecular Genetics of Susceptibility to Rheumatoid Arthritis. Arthritis Rheum (1987) 30:1205–13. doi: 10.1002/art.1780301102
4. Balandraud N, Picard C, Reviron D, Landais C, Toussirot E, Lambert N, et al. Hla-Drb1 Genotypes and the Risk of Developing Anti Citrullinated Protein Antibody (Acpa) Positive Rheumatoid Arthritis. PloS One (2013) 8:e64108. doi: 10.1371/journal.pone.0064108
5. Schellekens GA, de Jong BA, van den Hoogen FH, van de Putte LB, van Venrooij WJ. Citrulline Is an Essential Constituent of Antigenic Determinants Recognized by Rheumatoid Arthritis-Specific Autoantibodies. J Clin Invest (1998) 101:273–81. doi: 10.1172/JCI1316
6. Sebbag M, Moinard N, Auger I, Clavel C, Arnaud J, Nogueira L, et al. Epitopes of Human Fibrin Recognized by the Rheumatoid Arthritis-Specific Autoantibodies to Citrullinated Proteins. Eur J Immunol (2006) 36:2250–63. doi: 10.1002/eji.200535790
7. Meyer O, Nicaise-Roland P, Santos M, Labarre C, Dougados M, Goupille P, et al. Serial Determination of Cyclic Citrullinated Peptide Autoantibodies Predicted Five-Year Radiological Outcomes in a Prospective Cohort of Patients With Early Rheumatoid Arthritis. Arthritis Res Ther (2006) 8:R40. doi: 10.1186/ar1896
8. Schellekens GA, Visser H, de Jong BA, van den Hoogen FH, Hazes JM, Breedveld FC, et al. The Diagnostic Properties of Rheumatoid Arthritis Antibodies Recognizing a Cyclic Citrullinated Peptide. Arthritis Rheum (2000) 43:155–63. doi: 10.1002/1529-0131(200001)43:1<155::AID-ANR20>3.0.CO;2-3
9. Ji M, Hur M, Moon H-W, Park M, Yun Y-M, Lee S-H. Comparison of Second- and Third-Generation Immunoassays for Detection of Anti-Cyclic Citrullinated Peptide Antibodies. Scand J Clin Lab Invest (2018) 78:477–82. doi: 10.1080/00365513.2018.1499957
10. Aletaha D, Neogi T, Silman AJ, Funovits J, Felson DT, Bingham CO, et al. 2010 Rheumatoid Arthritis Classification Criteria: An American College of Rheumatology/European League Against Rheumatism Collaborative Initiative. Arthritis Rheumatism (2010) 62:2569–81. doi: 10.1002/art.27584
11. Nicaise-Roland P, Nogueira L, Demattei C, de Chaisemartin L, Rincheval N, Cornillet M, et al. Autoantibodies to Citrullinated Fibrinogen Compared With Anti-MCV and Anti-CCP2 Antibodies in Diagnosing Rheumatoid Arthritis at an Early Stage: Data From the French ESPOIR Cohort. Ann Rheum Dis (2013) 72:357–62. doi: 10.1136/annrheumdis-2011-201056
12. Iobagiu C, Magyar A, Nogueira L, Cornillet M, Sebbag M, Arnaud J, et al. The Antigen Specificity of the Rheumatoid Arthritis-Associated ACPA Directed to Citrullinated Fibrin Is Very Closely Restricted. J Autoimmun (2011) 37:263–72. doi: 10.1016/j.jaut.2011.07.003
13. Nogueira L, Cornillet M, Singwe-Ngandeu M, Viatte S, Bas S, Gabay C, et al. In Black Africans With Rheumatoid Arthritis, ACPA Recognize Citrullinated Fibrinogen and the Derived Peptides α36-50Cit38,42 and β60-74Cit60,72,74, Like in Caucasians. Clin Immunol (2014) 152:58–64. doi: 10.1016/j.clim.2014.02.011
14. Arnett FC, Edworthy SM, Bloch DA, Mcshane DJ, Fries JF, Cooper NS, et al. The American Rheumatism Association 1987 Revised Criteria for the Classification of Rheumatoid Arthritis. Arthritis Rheumatism (1988) 31:315–24. doi: 10.1002/art.1780310302
15. van Gestel AM, Haagsma CJ, van Riel PL. Validation of Rheumatoid Arthritis Improvement Criteria That Include Simplified Joint Counts. Arthritis Rheum (1998) 41:1845–50. doi: 10.1002/1529-0131(199810)41:10<1845::AID-ART17>3.0.CO;2-K
16. Smolen JS, Landewé RBM, Bijlsma JWJ, Burmester GR, Dougados M, Kerschbaumer A, et al. EULAR Recommendations for the Management of Rheumatoid Arthritis With Synthetic and Biological Disease-Modifying Antirheumatic Drugs: 2019 Update. Ann Rheum Dis. (2020) 79(6):685–99. doi: 10.1136/annrheumdis-2019-216655. annrheumdis-2019-216655.
17. van der Heijde D, van der Helm-van Mil AHM, Aletaha D, Bingham CO, Burmester GR, Dougados M, et al. EULAR Definition of Erosive Disease in Light of the 2010 ACR/EULAR Rheumatoid Arthritis Classification Criteria. Ann Rheum Dis (2013) 72:479–81. doi: 10.1136/annrheumdis-2012-202779
18. Chapuy-Regaud S, Nogueira L, Clavel C, Sebbag M, Vincent C, Serre G. Igg Subclass Distribution of the Rheumatoid Arthritis-Specific Autoantibodies to Citrullinated Fibrin. Clin Exp Immunol (2005) 139:542–50. doi: 10.1111/j.1365-2249.2004.02708.x
19. Turesson C, Jacobsson L. Epidemiology of Extra-Articular Manifestations in Rheumatoid Arthritis. Scand J Rheumatol (2004) 33:65–73. doi: 10.1080/03009740310004621
20. Nakamura T, Higashi S, Tomoda K, Tsukano M, Iyama K. Cutaneous Nodules in Patients With Rheumatoid Arthritis: A Case Report and Review of Literatures. Clin Rheumatol (2011) 30:719–22. doi: 10.1007/s10067-010-1602-4
21. Toussirot E, Berthelot JM, Pertuiset E, Bouvard B, Gaudin P, Wendling D, et al. Pulmonary Nodulosis and Aseptic Granulomatous Lung Disease Occurring in Patients With Rheumatoid Arthritis Receiving Tumor Necrosis Factor-α-Blocking Agent: A Case Series. J Rheumatol (2009) 36:2421–7. doi: 10.3899/jrheum.090030
22. Cornillet M, Sebbag M, Verrouil E, Magyar A, Babos F, Ruyssen-Witrand A, et al. The Fibrin-Derived Citrullinated Peptide β60-74Cit₆₀,₇₂,₇₄ Bears the Major ACPA Epitope Recognised by the Rheumatoid Arthritis-Specific Anticitrullinated Fibrinogen Autoantibodies and Anti-CCP2 Antibodies. Ann Rheum Dis (2014) 73:1246–52. doi: 10.1136/annrheumdis-2012-202868
23. Degboé Y, Constantin A, Nigon D, Tobon G, Cornillet M, Schaeverbeke T, et al. Predictive Value of Autoantibodies From Anti-CCP2, Anti-MCV and Anti-Human Citrullinated Fibrinogen Tests, in Early Rheumatoid Arthritis Patients With Rapid Radiographic Progression at 1 Year: Results From the ESPOIR Cohort. RMD Open (2015) 1:e000180. doi: 10.1136/rmdopen-2015-000180
24. Cornillet M, Verrouil E, Cantagrel A, Serre G, Nogueira L. In ACPA-Positive RA Patients, Antibodies to EBNA35-58Cit, a Citrullinated Peptide From the Epstein-Barr Nuclear Antigen-1, Strongly Cross-React With the Peptide β60-74Cit Which Bears the Immunodominant Epitope of Citrullinated Fibrin. Immunol Res (2015) 61:117–25. doi: 10.1007/s12026-014-8584-2
25. Cornillet M, Ajana S, Ruyssen-Witrand A, Constantin A, Degboé Y, Cantagrel A, et al. Autoantibodies to Human Citrullinated Fibrinogen and Their Subfamilies to the α36-50Cit and β60-74Cit Fibrin Peptides Similarly Predict Radiographic Damages: A Prospective Study in the French ESPOIR Cohort of Very Early Arthritides. Rheumatology (2016) 55:1859–70. doi: 10.1093/rheumatology/kew014
26. Rönnelid J, Hansson M, Mathsson-Alm L, Cornillet M, Reed E, Jakobsson P-J, et al. Anticitrullinated Protein/Peptide Antibody Multiplexing Defines an Extended Group of ACPA-positive Rheumatoid Arthritis Patients With Distinct Genetic and Environmental Determinants. Ann Rheum Dis (2018) 77:203–11. doi: 10.1136/annrheumdis-2017-211782
27. Sohrabian A, Mathsson-Alm L, Hansson M, Knight A, Lysholm J, Cornillet M, et al. Number of Individual ACPA Reactivities in Synovial Fluid Immune Complexes, But Not Serum Anti-CCP2 Levels, Associate With Inflammation and Joint Destruction in Rheumatoid Arthritis. Ann Rheum Dis (2018) 77:1345–53. doi: 10.1136/annrheumdis-2017-212627
28. Jonsson MK, Hensvold AH, Hansson M, Aga A-B, Sexton J, Mathsson-Alm L, et al. The Role of Anti-Citrullinated Protein Antibody Reactivities in An Inception Cohort of Patients With Rheumatoid Arthritis Receiving Treat-to-Target Therapy. Arthritis Res Ther (2018) 20:146. doi: 10.1186/s13075-018-1635-7
29. Terao C, Brynedal B, Chen Z, Jiang X, Westerlind H, Hansson M, et al. Distinct HLA Associations With Rheumatoid Arthritis Subsets Defined by Serological Subphenotype. Am J Hum Genet (2019) 105:616–24. doi: 10.1016/j.ajhg.2019.08.002
30. Boman A, Brink M, Lundquist A, Hansson M, Mathsson-Alm L, Rönnelid J, et al. Antibodies Against Citrullinated Peptides Are Associated With Clinical and Radiological Outcomes in Patients With Early Rheumatoid Arthritis: A Prospective Longitudinal Inception Cohort Study. RMD Open (2019) 5:e000946. doi: 10.1136/rmdopen-2019-000946
31. Reed E, Hedström AK, Hansson M, Mathsson-Alm L, Brynedal B, Saevarsdottir S, et al. Presence of Autoantibodies in “Seronegative” Rheumatoid Arthritis Associates With Classical Risk Factors and High Disease Activity. Arthritis Res Ther (2020) 22:170. doi: 10.1186/s13075-020-02191-2
32. Westerlind H, Rönnelid J, Hansson M, Alfredsson L, Mathsson-Alm L, Serre G, et al. Anti-Citrullinated Protein Antibody Specificities, Rheumatoid Factor Isotypes, and Incident Cardiovascular Events in Patients With Rheumatoid Arthritis. Arthritis Rheumatol (2020) 72:1658–67. doi: 10.1002/art.41381
33. Cornillet M, Babos F, Magyar A, Sebbag M, Verrouil E, Hudecz F, et al. Seropositivity and Antibody Profiling of Patients Are Dramatically Impacted by the Features of Peptides Used as Immunosorbents: A Lesson From Anti–Citrullinated Protein/Peptide Antibody. JI (2018) 201:3211–7. doi: 10.4049/jimmunol.1800330
34. Joo YB, Park Y-J, Park K-S, Kim K-J. Association of Cumulative Anti-Cyclic Citrullinated Protein Antibodies With Radiographic Progression in Patients With Rheumatoid Arthritis. Clin Rheumatol (2019) 38:2423–32. doi: 10.1007/s10067-019-04554-w
35. Scherer HU, van der Woude D, Willemze A, Trouw LA, Knevel R, Syversen SW, et al. Distinct ACPA Fine Specificities, Formed Under the Influence of HLA Shared Epitope Alleles, Have No Effect on Radiographic Joint Damage in Rheumatoid Arthritis. Ann Rheum Dis (2011) 70:1461–4. doi: 10.1136/ard.2010.146506
36. Potter C, Hyrich KL, Tracey A, Lunt M, Plant D, Symmons DPM, et al. Association of Rheumatoid Factor and Anti-Cyclic Citrullinated Peptide Positivity, But Not Carriage of Shared Epitope or PTPN22 Susceptibility Variants, With Anti-Tumour Necrosis Factor Response in Rheumatoid Arthritis. Ann Rheum Dis (2009) 68:69–74. doi: 10.1136/ard.2007.084715
37. Lv Q, Yin Y, Li X, Shan G, Wu X, Liang D, et al. The Status of Rheumatoid Factor and Anti-Cyclic Citrullinated Peptide Antibody Are Not Associated With the Effect of Anti-Tnfα Agent Treatment in Patients With Rheumatoid Arthritis: A Meta-Analysis. PloS One (2014) 9:e89442. doi: 10.1371/journal.pone.0089442
38. Sokolove J, Schiff M, Fleischmann R, Weinblatt ME, Connolly SE, Johnsen A, et al. Impact of Baseline Anti-Cyclic Citrullinated Peptide-2 Antibody Concentration on Efficacy Outcomes Following Treatment With Subcutaneous Abatacept or Adalimumab: 2-Year Results From the AMPLE Trial. Ann Rheum Dis (2016) 75:709–14. doi: 10.1136/annrheumdis-2015-207942
39. Murray E, Ellis A, Butylkova Y, Skup M, Kalabic J, Garg V. Systematic Review and Network Meta-Analysis: Effect of Biologics on Radiographic Progression in Rheumatoid Arthritis. J Comp Eff Res (2018) 7:959–74. doi: 10.2217/cer-2017-0106
40. van Beers JJ, Willemze A, Stammen-Vogelzangs J, Drijfhout JW, Toes RE, M Pruijn GJ. Anti-Citrullinated Fibronectin Antibodies in Rheumatoid Arthritis Are Associated With Human Leukocyte Antigen-DRB1 Shared Epitope Alleles. Arthritis Res Ther (2012) 14:R35. doi: 10.1186/ar3744
41. Manca ML, Alunno A, D’Amato C, Bistoni O, Puxeddu I, Gerli R, et al. Anti -Citrullinated Peptide Antibodies Profiling in Established Rheumatoid Arthritis. Joint Bone Spine (2018) 85:441–5. doi: 10.1016/j.jbspin.2017.07.009
42. Joshua V, Hensvold AH, Reynisdottir G, Hansson M, Cornillet M, Nogueira L, et al. Association Between Number and Type of Different ACPA Fine Specificities With Lung Abnormalities in Early, Untreated Rheumatoid Arthritis. RMD Open (2020) 6:e001278. doi: 10.1136/rmdopen-2020-001278
43. Pratesi F, Petit-Teixeira E, Sidney J, Teixeira VH, Puxeddu I, Sette A, et al. Effect of Rheumatoid Arthritis (Ra) Susceptibility Genes on the Immune Response to Viral Citrullinated Peptides in RA. J Rheumatol (2012) 39:1490–3. doi: 10.3899/jrheum.111548
44. Auger I, Escola JM, Gorvel JP, Roudier J. Hla-DR4 and HLA-DR10 Motifs That Carry Susceptibility to Rheumatoid Arthritis Bind 70-Kd Heat Shock Proteins. Nat Med (1996) 2:306–10. doi: 10.1038/nm0396-306
45. Roth S, Willcox N, Rzepka R, Mayer MP, Melchers I. Major Differences in Antigen-Processing Correlate With a Single Arg 71 ↔Lys Substitution in HLA-DR Molecules Predisposing to Rheumatoid Arthritis and With Their Selective Interactions With 70-Kda Heat Shock Protein Chaperones. J Immunol (2002) 169:3015–20. doi: 10.4049/jimmunol.169.6.3015
46. Turunen S, Huhtakangas J, Nousiainen T, Valkealahti M, Melkko J, Risteli J, et al. Rheumatoid Arthritis Antigens Homocitrulline and Citrulline are Generated by Local Myeloperoxidase and Peptidyl Arginine Deiminases 2, 3 and 4 in Rheumatoid Nodule and Synovial Tissue. Arthritis Res Ther (2016) 18:239. doi: 10.1186/s13075-016-1140-9
47. Athanasou NA, Quinn J, Woods CG, Mcgee JO. Immunohistology of Rheumatoid Nodules and Rheumatoid Synovium. Ann Rheum Dis (1988) 47:398–403. doi: 10.1136/ard.47.5.398
48. Anquetil F, Clavel C, Offer G, Serre G, Sebbag M. Igm and IgA Rheumatoid Factors Purified From Rheumatoid Arthritis Sera Boost the Fc Receptor- and Complement-Dependent Effector Functions of the Disease-Specific Anti-Citrullinated Protein Autoantibodies. J Immunol (2015) 194:3664–74. doi: 10.4049/jimmunol.1402334
49. Laurent L, Anquetil F, Clavel C, Ndongo-Thiam N, Offer G, Miossec P, et al. Igm Rheumatoid Factor Amplifies the Inflammatory Response of Macrophages Induced by the Rheumatoid Arthritis-Specific Immune Complexes Containing Anticitrullinated Protein Antibodies. Ann Rheum Dis (2015) 74:1425–31. doi: 10.1136/annrheumdis-2013-204543
Keywords: ACPA, rheumatoid arthritis, HLA-DRB1, AhFibA, citrullinated peptides 2
Citation: Larid G, Pancarte M, Offer G, Clavel C, Martin M, Pradel V, Auger I, Lafforgue P, Roudier J, Serre G and Balandraud N (2021) In Rheumatoid Arthritis Patients, HLA-DRB1*04:01 and Rheumatoid Nodules Are Associated With ACPA to a Particular Fibrin Epitope. Front. Immunol. 12:692041. doi: 10.3389/fimmu.2021.692041
Received: 07 April 2021; Accepted: 04 June 2021;
Published: 24 June 2021.
Edited by:
Philippe Saas, U1098 Interactions Hôte-Greffon-Tumeur & Ingénierie Cellulaire et Génique (INSERM), FranceCopyright © 2021 Larid, Pancarte, Offer, Clavel, Martin, Pradel, Auger, Lafforgue, Roudier, Serre and Balandraud. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nathalie Balandraud, TmF0aGFsaWUuYmFsYW5kcmF1ZEBhcC1obS5mcg==