 Samuel Wacrenier1,2,3
Samuel Wacrenier1,2,3 Charlotte Boud’hors1
Charlotte Boud’hors1 Giorgina Piccoli2
Giorgina Piccoli2 Jean-François Augusto1,3*
Jean-François Augusto1,3* Benoit Brilland1,3
Benoit Brilland1,3- 1Service de Néphrologie-Dialyse-Transplantation, Université d’Angers, CHU Angers, Angers, France
- 2Service de Néphrologie, Centre Hospitalier du Mans, Le Mans, France
- 3Université d’Angers, INSERM, CRCINA, Angers, France
A Commentary on
Outcome Predictors of Biopsy-Proven Myeloperoxidase-Anti-Neutrophil Cytoplasmic Antibody-Associated Glomerulonephritis
By Ge Y, Yang G, Yu X, Sun B, Zhang B, Yuan Y, Zeng M, Wang N, Mao H and Xing C (2021). Front. Immunol. 11:607261. doi: 10.3389/fimmu.2020.607261
Introduction
Diagnosis of Antineutrophil cytoplasmic antibodies (ANCA) associated vasculitis (AAV) with glomerulonephritis (ANCA-GN) enjoins the start of an immunosuppressive treatment as soon as possible. Its intensity is guided by clinical presentation and histopathologic lesions on kidney biopsy. Individualized and personalized treatment is a key issue for improving outcomes. In this view, markers of AAV severity, renal involvement, and overall prognosis may be useful, not only for a better understanding of the disease pathophysiology, but above all, for guiding therapies and improving patients’ outcomes, especially when histology is not available. Moreover, if chronic lesions in kidney biopsy at diagnosis remain a major determinant of renal outcomes, whether assessed by the international histopathologic classification (1), the Renal Risk Score (2) or the global chronicity score proposed by the Mayo Clinic (3), some intermediate prognostic classes (e.g. crescentic and mixed classes in Berden’s classification) actually seem to have similar renal outcomes (4). Thus, biomarkers are needed to refine the prognosis assessment of these patients.
We therefore read we much interest the publication by Ge et al. regarding the role of several biological markers associated with death and end stage kidney disease (ESKD) in MPO-ANCA vasculitis patients with pauci-immune glomerulonephritis (MPO-ANCA-GN), especially anemia and hypoalbuminemia (5). In their cohort of 112 patients, albuminemia < 30 g/L and hemoglobin < 9g/dL were associated with a greater risk of ESKD occurrence. Moreover, hypoalbuminemia (but not anemia) was associated with patient survival.
Predictors of Death and ESKD in the Maine-Anjou Registry
We aimed to evaluate the predictive value of these biological markers within our cohort of AAV patients with biopsy-proven kidney involvement, included in the Maine-Anjou (France) registry. This population has previously been described in various settings (6–9). Among the 180 patients within the registry, 111 patients presented with MPO-ANCA of whom 98 had ANCA-GN histological confirmation with kidney biopsy. To meet the same inclusion criteria used by Ge et al., we analyzed these 98 patients. Median age was 68 years old [61-75], 61% were male and more than half had hypertension. Median BVAS was 14 [12-18], and, after kidneys, most involved organs were lungs (33%), ear, nose and throat (22%) and skin (13%). At baseline and before any therapeutic intervention, median eGFR was 17 ml/min [12, 33], median hemoglobin was 10 g/dL [8.75 - 10.95] of whom 31% had a hemoglobin level < 9g/dL and median albuminemia was 30 g/L [28 - 34] of whom 45% had an albumin level < 30 g/L. A fifth (21%) required kidney replacement therapy within 30 days from diagnosis. According to Berden’s classification, the proportion of patients within the focal class, the crescentic class, the mixed class and the sclerotic class was 19%, 43%, 20% and 18%, respectively. In addition to oral glucocorticoids, most patients received intravenous methylprednisolone pulses (81%) associated with cyclophosphamide (84%) or rituximab (16%) as induction therapy. Maintenance therapy mostly consisted in azathioprine or rituximab regimens (57% and 41%, respectively). These 98 patients were followed with a median follow-up of 46 months [16-96] during which 25 patients (26%) experienced a relapse (60% with renal involvement), 28 patients (29%) reached ESKD and 24 patients (24%) died.
In our cohort, among clinical or biological parameters at diagnosis, albuminemia (either considered as a continuous variable or as a dichotomized one) was neither associated with death nor with ESKD (5-years censured Multivariable Cox Analysis). Among the different models used, age and proteinuria were the best predictors for death occurrence. The predictive value of anemia appeared to be inconsistent (Table 1. The best predictor for ESKD occurrence was the severity of renal involvement at admission (amount of proteinuria and the need for kidney replacement therapy within 30 days from diagnosis). Similarly to albuminemia, hemoglobin (either considered as a continuous variable or dichotomized at anemia threshold) was not associated with ESKD (Table 1).
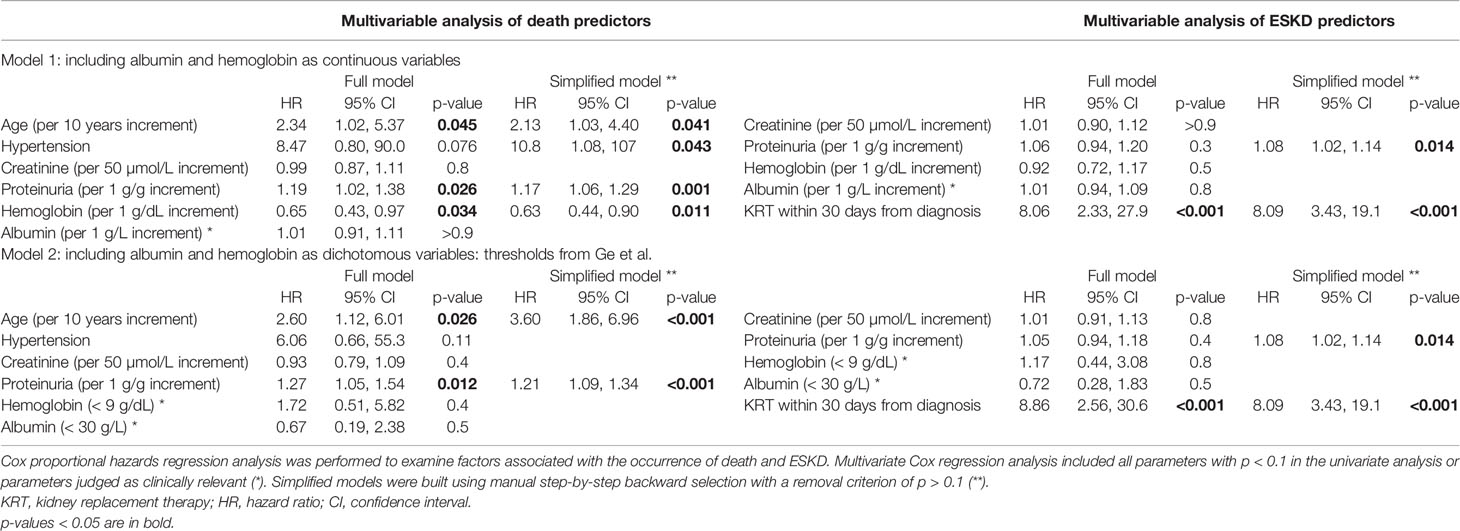
Table 1 5-years censured Cox Multivariable analysis of patient survival (death) or renal survival (ESKD).
Discussion
Our results underline the inconsistent predictive value of these biological markers (hemoglobin and albumin) when applied to our cohort. Indeed, as stated by Ge et al., literature is very heterogeneous on this subject. Hemoglobin has been found irregularly as a predictor of death (10–12) or not (13) and as a predictor of ESKD (11) or not (14, 15). In the same way, albumin has been found as a predictor of death (16) or not (17, 18) and as a predictor of ESKD (19) or not (20, 21). These inconsistent results may be explained by various collinear variables that can unspecifically and falsely bring out biological predictors. For example, the amount and duration of inflammatory syndrome, the nutritional status before ANCA-GN onset, and the severity (and chronicity) of kidney failure can all influence these parameters. Moreover, these studies vary in term of number of patients, ANCA type, severity at presentation and management. While we included a similar number of patients with biopsy-proven MPO-ANCA-GN, approximatively followed for the same duration as compared to Ge et al. study, the discrepancy between the two cohorts may be explained by additional factors. First, the Asian population experienced more severe outcomes (death and ESKD rate reached 41% and 39%, respectively) possibly related to a more severe initial clinical presentation (median BVAS 18 and need for KRT 42%). Moreover, remission induction regimen was based on glucocorticoids and mycophenolate mofetil (MMF) for a non-negligible proportion of patients (20.5%). This is not surprising as MMF-based induction regimen was associated with better outcomes in Chinese patients when compared with conventional European immunosuppressant induction therapy such as cyclophosphamide (22). Maintenance regimen was also different as MMF and cyclophosphamide was predominantly used in Ge et al. cohort, whereas we mostly used azathioprine and rituximab. Thus, ethnicity, a more severe initial presentation and different therapeutic management may explain these differences.
To conclude, in the quest of the perfect biological marker, we would like to bring out that hemoglobin and albumin may not be the eagerly awaited ones. Beyond the classical aphorism “the worse it is, the worse it gets”, various biomarkers are currently under careful examination to reach this goal (23). Some may seem duller than others but nevertheless just as promising. Indeed, we recently reported lymphopenia as a strong independent predictor of ESKD (9) and think that exploring abnormalities in lymphocytes phenotype, whether considering kidney infiltrating cells or circulating lymphocytes, would be enlightening in this setting. Indeed, lymphopenia by itself (9) but also the underlying mechanisms (e.g. loss of regulatory cells, regulatory/inflammatory cells imbalance, and, activated T cells infiltration) (24–27) could be of great value to help predict bad outcomes in ANCA-GN.
Author Contributions
SW, BB, and JFA designed the study. SW, CB, and BB gathered the information included in the database. SW and BB analyzed the data. SW wrote the first draft of the manuscript. BB and J-FA revised the manuscript. All authors participated in patient care. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Berden AE, Ferrario F, Hagen EC, Jayne DR, Jennette JC, Joh K, et al. Histopathologic Classification of ANCA-Associated Glomerulonephritis. JASN (2010) 21:1628–36. doi: 10.1681/ASN.2010050477
2. Brix SR, Noriega M, Tennstedt P, Vettorazzi E, Busch M, Nitschke M, et al. Development and Validation of a Renal Risk Score in ANCA-associated Glomerulonephritis. Kidney Int (2018) 94:1177–88. doi: 10.1016/j.kint.2018.07.020
3. Berti A, Cornec-Le Gall E, Cornec D, Casal Moura M, Matteson EL, Crowson CS, et al. Incidence, Prevalence, Mortality and Chronic Renal Damage of Anti-Neutrophil Cytoplasmic Antibody-Associated Glomerulonephritis in a 20-Year Population-Based Cohort. Nephrol Dialysis Transplant (2019) 34:1508–17. doi: 10.1093/ndt/gfy250
4. van Daalen EE, Wester Trejo MAC, Göçeroğlu A, Ferrario F, Joh K, Noël L-H, et al. Developments in the Histopathological Classification of ANCA-Associated Glomerulonephritis. CJASN (2020) 15:1103–11. doi: 10.2215/CJN.14561119
5. Ge Y, Yang G, Yu X, Sun B, Zhang B, Yuan Y, et al. Outcome Predictors of Biopsy-Proven Myeloperoxidase-Anti-Neutrophil Cytoplasmic Antibody-Associated Glomerulonephritis. Front Immunol (2021) 11:607261. doi: 10.3389/fimmu.2020.607261
6. Guibert F, Garnier A-S, Wacrenier S, Piccoli G, Djema A, Gansey R, et al. Patients With ANCA-Associated Glomerulonephritis and Connective Tissue Diseases: A Comparative Study From the Maine-Anjou Aav Registry. J Clin Med (2019) 8. doi: 10.3390/jcm8081218
7. Henry N, Brilland B, Wacrenier S, Djema A, Garnier AS, Gansey R, et al. Incidence and Risk Factors of Venous Thromboembolic Events in Patients With ANCA-Glomerulonephritis: A Cohort Study From the Maine-Anjou Registry. JCM (2020) 9:3177. doi: 10.3390/jcm9103177
8. Jourdain P, Brilland B, Medhioub O, Caron J, Samoreau C, Djema A, et al. Incidence and Temporal Trend in Risk Factors of Severe Infections in ANCA-Glomerulonephritis Patients. Kidney Int Rep (2021) 6(4):1161–5. doi: 10.1016/j.ekir.2020.12.037. S2468024920318714.
9. Wacrenier S, Riou J, Jourdain P, Guibert F, Henry N, Djema A, et al. Lymphopenia At Diagnosis of ANCA-vasculitis With Renal Involvement is Correlated With Severity and Renal Prognosis. Nephrol Dialysis Transplant (2021) gfab158. doi: 10.1093/ndt/gfab158
10. Flossmann O, Berden A, de Groot K, Hagen C, Harper L, Heijl C, et al. Long-Term Patient Survival in ANCA-associated Vasculitis. Ann Rheum Dis (2011) 70:488–94. doi: 10.1136/ard.2010.137778
11. Crnogorac M, Horvatic I, Toric L, Galesic Ljubanovic D, Tisljar M, Galesic K. Clinical, Serological and Histological Determinants of Patient and Renal Outcome in ANCA-associated Vasculitis With Renal Involvement: An Analysis From a Referral Centre. Int Urol Nephrol (2017) 49:1419–31. doi: 10.1007/s11255-017-1610-2
12. Solans-Laqué R, Fraile G, Rodriguez-Carballeira M, Caminal L, Castillo MJ, Martínez-Valle F, et al. Clinical Characteristics and Outcome of Spanish Patients With ANCA-associated Vasculitides: Impact of the Vasculitis Type, ANCA Specificity, and Treatment on Mortality and Morbidity. Medicine (2017) 96:e6083. doi: 10.1097/MD.0000000000006083
13. Titeca-Beauport D, Francois A, Lobbedez T, Guerrot D, Launay D, Vrigneaud L, et al. Early Predictors of One-Year Mortality in Patients Over 65 Presenting With ANCA-associated Renal Vasculitis: A Retrospective, Multicentre Study. BMC Nephrol (2018) 19:317. doi: 10.1186/s12882-018-1102-3
14. Ahn JK, Hwang J-W, Lee J, Jeon CH, Cha H-S, Koh E-M. Clinical Features and Outcome of Microscopic Polyangiitis Under a New Consensus Algorithm of ANCA-associated Vasculitides in Korea. Rheumatol Int (2012) 32:2979–86. doi: 10.1007/s00296-011-2079-4
15. Andreiana I, Stancu S, Avram A, Taran L, Mircescu G. ANCA Positive Crescentic Glomerulonephritis Outcome in a Central East European Cohort: A Retrospective Study. BMC Nephrol (2015) 16:90. doi: 10.1186/s12882-015-0091-8
16. Aasarød K, Iversen BM, Hammerstrøm J, Bostad L, Vatten L, Jørstad S. Wegener’s Granulomatosis: Clinical Course in 108 Patients With Renal Involvement. Nephrol Dial Transplant (2000) 15:611–8. doi: 10.1093/ndt/15.5.611
17. Itabashi M, Takei T, Yabuki Y, Suzuki H, Ando M, Akamatsu M, et al. Clinical Outcome and Prognosis of Anti-Neutrophil Cytoplasmic Antibody-Associated Vasculitis in Japan. Nephron Clin Pract (2010) 115:c21–7. doi: 10.1159/000286346
18. Bakoush O, Segelmark M, Torffvit O, Ohlsson S, Tencer J. Urine IgM Excretion Predicts Outcome in ANCA-associated Renal Vasculitis. Nephrol Dialysis Transplant (2006) 21:1263–9. doi: 10.1093/ndt/gfk074
19. Chen Y-X, Xu J, Pan X-X, Shen P-Y, Li X, Ren H, et al. Histopathological Classification and Renal Outcome in Patients With Antineutrophil Cytoplasmic Antibodies-associated Renal Vasculitis: A Study of 186 Patients and Metaanalysis. J Rheumatol (2017) 44:304–13. doi: 10.3899/jrheum.160866
20. Moroni G, Binda V, Leoni A, Raffiotta F, Quaglini S, Banfi G, et al. Predictors of Renal Survival in ANCA-associated Vasculitis. Validation of a Histopatological Classification Schema and Review of the Literature. Clin Exp Rheumatol (2015) 33:S–56-63.
21. Iwakiri T, Fujimoto S, Kitagawa K, Furuichi K, Yamahana J, Matsuura Y, et al. Validation of a Newly Proposed Histopathological Classification in Japanese Patients With Anti-Neutrophil Cytoplasmic Antibody-Associated Glomerulonephritis. BMC Nephrol (2013) 14:125. doi: 10.1186/1471-2369-14-125
22. Hu W, Liu C, Xie H, Chen H, Liu Z, Li L. Mycophenolate Mofetil Versus Cyclophosphamide for Inducing Remission of ANCA Vasculitis With Moderate Renal Involvement. Nephrol Dialysis Transplant (2007) 23:1307–12. doi: 10.1093/ndt/gfm780
23. Tedesco M, Gallieni M, Pellegata F, Cozzolino M, Alberici F. Update on ANCA-associated Vasculitis: From Biomarkers to Therapy. J Nephrol (2019) 32:871–82. doi: 10.1007/s40620-019-00628-9
24. Martinez Valenzuela L, Bordignon Draibe J, Fulladosa Oliveras X, Bestard Matamoros O, Cruzado Garrit JM, Torras Ambrós J. T-Lymphocyte in ANCA-associated Vasculitis: What do We Know? A Pathophysiological and Therapeutic Approach. Clin Kidney J (2019) 12:503–11. doi: 10.1093/ckj/sfz029
25. Wilde B, Thewissen M, Damoiseaux J, Knippenberg S, Hilhorst M, van Paassen P, et al. Regulatory B Cells in ANCA-associated Vasculitis. Ann Rheum Dis (2013) 72:1416–9. doi: 10.1136/annrheumdis-2012-202986
26. von Borstel A, Sanders JS, Rutgers A, Stegeman CA, Heeringa P, Abdulahad WH. Cellular Immune Regulation in the Pathogenesis of ANCA-associated Vasculitides. Autoimmun Rev (2018) 17:413–21. doi: 10.1016/j.autrev.2017.12.002
Keywords: ANCA-associated vasculitis, glomerulonephritis, predictor, death, end stage kidney disease
Citation: Wacrenier S, Boud’hors C, Piccoli G, Augusto J-F and Brilland B (2021) Commentary: Outcome Predictors of Biopsy-Proven Myeloperoxidase-Anti-Neutrophil Cytoplasmic Antibody-Associated Glomerulonephritis. Front. Immunol. 12:691179. doi: 10.3389/fimmu.2021.691179
Received: 05 April 2021; Accepted: 17 May 2021;
Published: 02 June 2021.
Edited by:
Carmelo Carmona-Rivera, National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), United StatesReviewed by:
Alvise Berti, Santa Chiara Hospital, ItalyLuis Felipe Flores-Suárez, Instituto Nacional de Enfermedades Respiratorias-México (INER), Mexico
Copyright © 2021 Wacrenier, Boud’hors, Piccoli, Augusto and Brilland. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jean-François Augusto, amZhdWd1c3RvQGNodS1hbmdlcnMuZnI=