
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol. , 29 June 2021
Sec. Vaccines and Molecular Therapeutics
Volume 12 - 2021 | https://doi.org/10.3389/fimmu.2021.690940
 Evelin A. Leibinger1*
Evelin A. Leibinger1* Gábor Pauler2
Gábor Pauler2 Noémi Benedek1
Noémi Benedek1 Tímea Berki3
Tímea Berki3 István Jankovics4
István Jankovics4 Richard McNally5
Richard McNally5 Gábor Ottóffy1*
Gábor Ottóffy1*Background: In children undergoing chemotherapy yearly influenza vaccination is recommended by treatment protocols. We investigated the relationship between cellular immunity and the antibody response to inactivated influenza vaccines.
Methods: 25 patients (age: 2-18 years) undergoing chemotherapy for different malignancies participated in our study. Flow cytometric detection of peripheral blood lymphocyte subpopulations together with hemagglutination inhibition antibody titers were measured before and 21-28 days after vaccination. We examined the ratio and total numbers of CD3+, CD4+, CD8+ T cells, activated helper (CD3+CD4+CD25low), regulatory (CD3+CD4+CD25high), naive (CD3+CD45RA+) and memory (CD3+CD45RO+) T cells, CD56+NK, and CD3+CD56+ (NKT-like) cells. Relationships between specific antibody responses (seroprotection, seroconversion, geometric mean titer (GMT), geometric mean fold increase (GMFI)) and the ratios and counts of lymphocyte subpopulations were evaluated using one-way ANOVA and the paired sample t test after dichotomization according to age-related reference values.
Results: Patients with CD4+ lymphocyte levels in the normal age-specific range showed significantly better response regarding postvaccination GMT elevation for H1N1 and H3N2 strains (97.52 vs. 19.2, p=0.019, 80 vs. 14.43, p=0.021, respectively). GMFI results were significant only against B strain (2.69-fold vs. 1.23-fold, p=0.046). Prevaccination CD3+CD56+ (NKT-like) cells above predicted values according to age showed significant associations both in postvaccination GMT elevation (H1N1: 75.11 vs. 14.14, p=0.010; H3N2: 62.18 vs. 11.22, p=0.012; B: 22.69 vs. 6.67, p=0.043) and GMFI against all three strains (H1N1: 3.76-fold vs. 1.06-fold, p=0.015; H3N2: 2.74-fold vs. 1, p=0.013; B: 2.57-fold vs. 1, p=0.008). By one-way ANOVA, we found a positive relation between absolute lymphocyte cell count above 1000/µl and the postvaccination GMT elevation against H3N2 (12.81 vs. 56.56, p=0.032), and GMFI regarding H1N1 (1.22-fold vs. 3.48-fold, p=0.044).
Conclusions: In addition to verifying the predictive value of absolute lymphocyte count above 1000/µl, our results suggest an association between NKT-like cell counts and the specific antibody response against all three investigated influenza strains in highly immunosuppressed patients. Furthermore, prevaccination CD4+ lymphocyte levels in the normal age-specific range may influence seroresponse.
Chemotherapy induced cytopenias cause prolonged immunosuppression in patients with malignancies resulting in increased susceptibility for pathogens. An annually recurring potential risk is infection with influenza. It can cause severe illness and complications as well as delays in treatment regimens thus threatening the outcome of cancer treatment (1, 2). The recommended vaccination offers the possibility to prevent infection and its complications (3).
Furthermore, investigating the immune response and factors that might be associated with successful immunization of such an immunocompromised population gives us a unique opportunity to evaluate the underlying immunological mechanisms and find targets for vaccine improvement.
In a previous study we evaluated the immune response and safety of concomitant trivalent-inactivated vaccine for seasonal influenza viruses (H1N1, H3N2 and B), and monovalent-inactivated vaccine for the 2009 pandemic influenza A virus in children undergoing chemotherapy (4). In agreement with several other studies (5–9), we verified that a higher baseline absolute lymphocyte count may enhance the immune response to influenza vaccination. A remaining question is which specific lymphocyte subpopulation could be responsible for this enhancement.
In recent years cellular, especially T cell responses gained increasing importance in influenza vaccine research and development (10–12). One such area of ongoing research are natural killer (NK) T cells, also called as NKT-like cells, a heterogeneous group of T lymphocytes that confer natural immunity. These cells have the phenotypic characteristics of both T cells and NK cells and function as a link between innate and adaptive immunity. NKT-like cells include a wide group of innate T lymphocyte populations, such as γδT cells, and CD1- and MR-1-restricted T cells which have an important immunoregulatory function. Unlike the major histocompatibility complex (MHC)-restricted T cells, these cells possess a restricted repertoire of T cell receptors, perform rapid effector responses and recognize a limited selection of non-peptide molecules, presented by the MHC class I-like molecule CD1d. Upon activation, NKT cells rapidly release large quantities of multiple cytokines and chemokines capable of boosting adaptive immune responses. They are capable of stimulating a wide array of immune cells that enhance vaccine-mediated immune responses (13).
Induction of NKT cells with a special adjuvant has resulted in improved immune responses in several animal models (14) of influenza vaccination. NKT cells show similarity in mammals so induction of these cells during vaccination might be promising in humans as well. Furthermore, based on animal investigations, some authors suggest that NKT cell induction might have a role also in the treatment of influenza infection (15).
Every finding in humans that correlates with results of animal investigations supports a similar role of NKT cells in humans and leads us closer to improved prevention or treatment of influenza virus infection.
In our study we investigated the relationship between cellular immunity and the response to influenza vaccines in children receiving chemotherapy with different types of malignancies.
Twenty-five consecutively treated patients (11 males and 14 females) were enrolled in our study during the influenza season periods of 2016/2017 and 2017/2018. Median age was 6 years (range 2 to 18 years). The underlying diseases were hematologic malignancies in the majority of participants (19 patients), while the remaining 6 cases had various solid tumors. All patients had been receiving chemotherapy at the Division of Pediatric Hematology and Oncology of the University of Pécs within 1 month before vaccination, and all continued to receive scheduled chemotherapy afterwards. Nine patients were undergoing maintenance therapy and sixteen children were receiving intensive cytostatic treatment (Table 1).
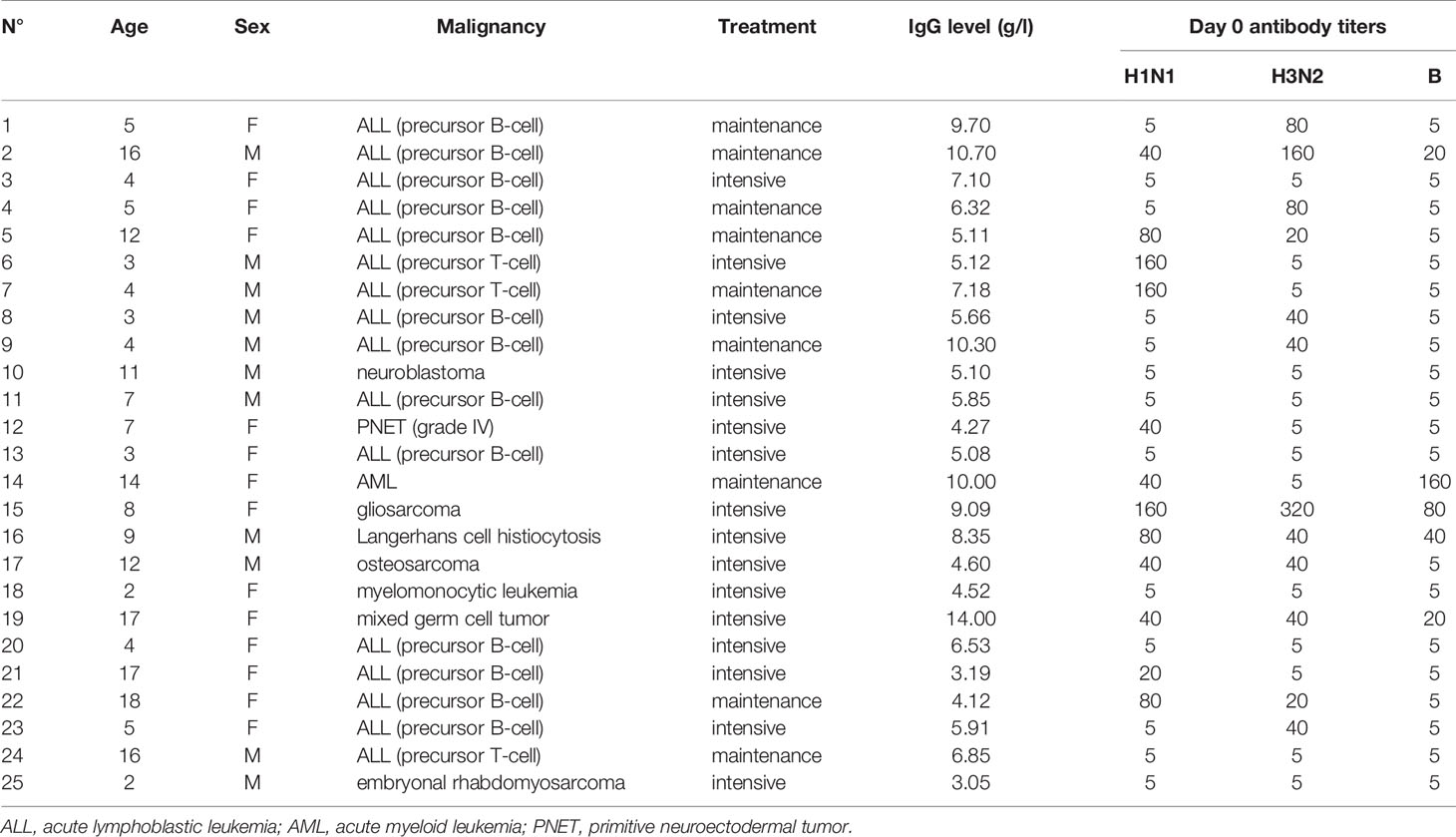
Table 1 Patient characteristics.
Exclusion criteria were the following: recent history of influenza vaccination, confirmed influenza infection prior to vaccination, history of egg allergy, administration of other vaccines during the study period. One patient was eventually excluded from the study due to lack of adherence to follow-up visits.
The protocol for vaccination was designed in accordance with the recommendations of the Infectology Department of the Hungarian National Healthcare Advisory Board, based on data received from the Hungarian National Center of Epidemiology (16, 17).
The Institutional Review Board of the University of Pécs authorized the protocol for this study (3672.316-2954/2010). Sample collections were performed concurrently with the routine blood sampling involved in cancer treatment. Written consent was obtained from the parents of each child.
In both seasons, a whole-virion, trivalent, inactivated, adjuvanted influenza vaccine (3Fluart - Fluart Innovative Vaccines Ltd., Budapest, Hungary) was in use for vaccination. Each preparation contained aluminium phosphate gel adjuvant and 6 µg haemagglutinin of each strain per 0.5 ml. Strains were selected according to the recommendations of the World Health Organization for the northern hemisphere for influenza vaccine composition for respective seasons: A/Hong Kong/4801/2014 (H3N2)-like, B/Brisbane/60/2008-like, A/California/7/2009 (H1N1)pdm09-like (A/California/7/2009, NYMC X-181) in 2016/2017 and A/Michigan/45/2015 (H1N1)pdm09-like in 2017/2018.
Fifteen patients were younger than 10 years old, and therefore received 0.25 ml of the vaccine, while ten participants received 0.5 ml of the vaccine.
In patients receiving maintenance treatment, vaccine was given without discontinuation of therapy. During intensive treatment, vaccination was scheduled in all patients 2-3 days before the next cytostatic treatment according to the recommendations of the Hungarian National Healthcare Advisory Board.
Blood samples were taken from each participant before vaccination and 28 days afterwards, mostly via central venous catheter for measurements of hemagglutination inhibition (HI) titer, immunoglobulin level, white blood cell count and flow cytometric analysis.
Three millilitres of serum were separated by centrifugation, then immediately frozen and stored at -80°C until the laboratory measurements on HI antibody titers were performed. Titers against the virus strains were measured by hemagglutination inhibition with chicken red blood cells following recommended procedures (18). All serologic tests were done at a single central laboratory (Department of Virology, National Center of Epidemiology, Budapest, Hungary). Each pair of sera were tested in complete duplicate series on the same day with the use of identical reagents.
The geometric mean HI antibody titer (GMT), seroprotection (defined as a titer level of ≥1:40) rate, seroconversion (defined a ≥4-fold increase in titer from baseline or a postvaccination titer level of ≥1:40 if the baseline titer was undetectable) rate, and GMT fold increase (GMFI: GMT ratio of postvaccination titer to prevaccination titer) were calculated.
The following anti-human monoclonal antibodies were used: anti-CD3-FITC, anti-CD8-PE, anti-CD4-PerCP, anti-CD56-PECy5, anti-CD25-PE, anti-CD45RA-PE and anti-CD45RO-PerCP (all from BD Biosciences). The 50 µl blood sample (EDTA) was incubated with the appropriate antibody cocktails for 30 minutes on ice, washed twice in phosphate buffered saline and fixed with 1% paraformaldehyde prior flow cytometric analysis using a FACSCalibur cytometer with CellQuestPro software. At least 10,000 cells were collected in the lymphocyte gate and analyzed. CD3+, CD4+, CD5+, CD8+ T cells, CD3+CD4+CD25- “resting Thelper cells”, CD3+CD4+CD25low “activated” and, CD3+CD4+CD25high “regulatory” T cells were detected and their absolute cell numbers were calculated. We followed naive CD3+CD45RA+ and CD3+CD45RO+ memory T cell percentages and absolute cell counts, CD3+CD56+ NKT-like and CD56+ NK cell ratio and absolute cell counts. CD3/CD45 positive cells were further analyzed for their CD4, CD8 and CD25 expression. Naive and memory T cells were detected with simultaneous CD3/CD45RA/CD45RO staining, NK cells and NKT cells were analyzed from the lymphocyte gate based on their CD3/CD56 positivity. For each of the gated cell populations the percentages of cells were analyzed. Gating strategies are presented in Figure 1.
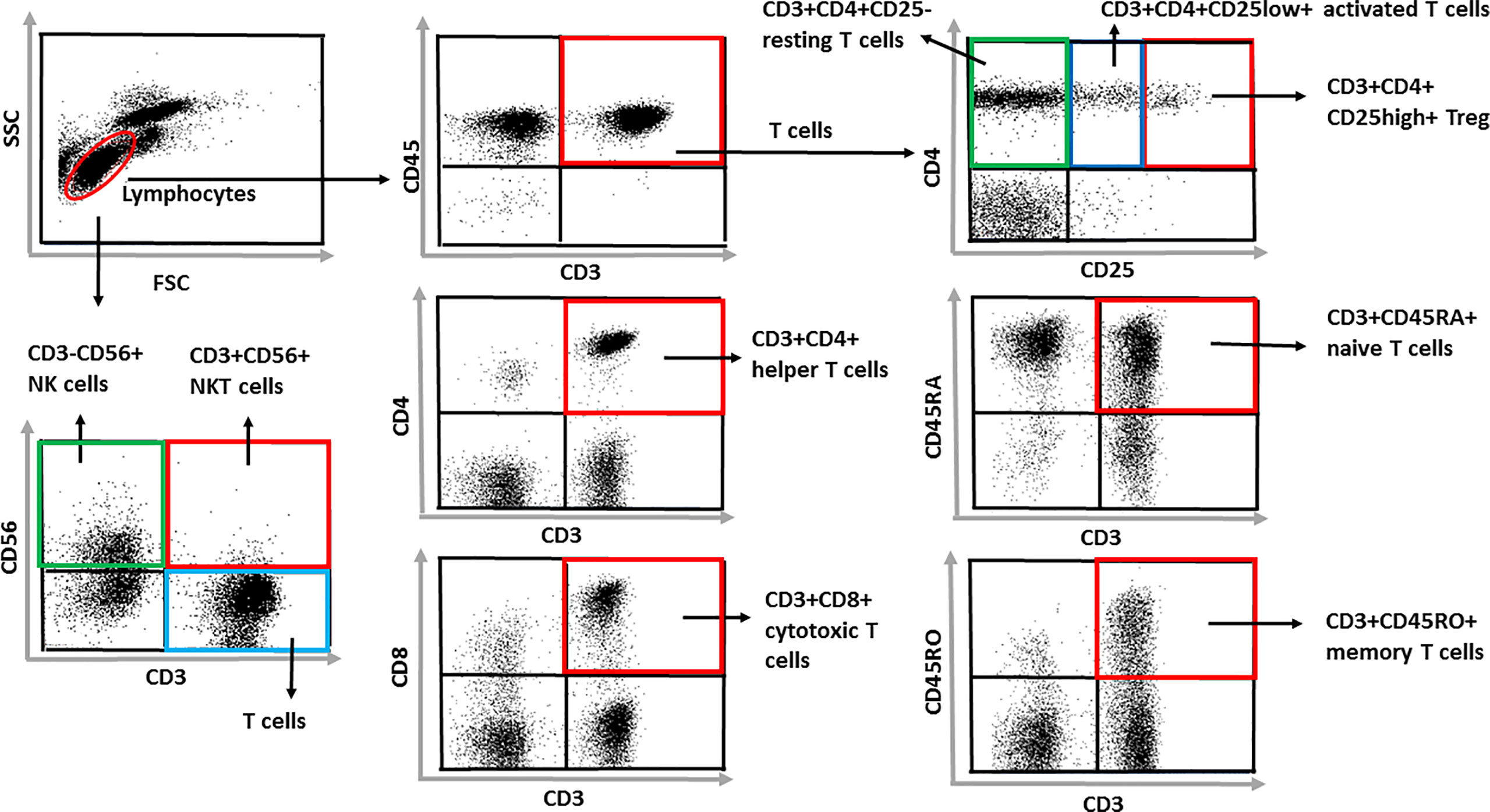
Figure 1 Gating strategies. At least 10,000 cells were collected in the lymphocyte gate and analyzed. CD3+, CD4+, CD5+, CD8+ T cells, CD3+CD4+CD25- “resting Thelper cells”, CD3+CD4+CD25low “activated” and, CD3+CD4+CD25high “regulatory” T cells were detected and their absolute cell numbers were calculated. We followed naive CD3+CD45RA+ and CD3+CD45RO+ memory T cell percentages and absolute cell counts, CD3+CD56+ NKT-like and CD56+ NK cell ratio and absolute cell counts. CD3/CD45 positive cells were further analyzed for their CD4, CD8 and CD25 expression. Naive and memory T cells were detected with simultaneous CD3/CD45RA/CD45RO staining, NK cells and NKT cells were analyzed from the lymphocyte gate based on their CD3/CD56 positivity. For each of the gated cell populations the percentages of cells were analyzed.
Baseline assessments on day 0 consisted of gathering demographic data, medical history and physical examination. We examined each patient on a weekly basis by physical and laboratory (complete blood count) examination during the follow-up period, until the final blood sampling was obtained for serologic study. Possible vaccine-related adverse events were monitored closely. On follow-up visits, standard medical history and medications administered since the last visit were summarized, and physical examination was performed prior to blood sample collection. Safety variables were recorded during follow-up visits for patient history and physical examination.
Data were analyzed using one-way ANOVA and paired sample t test using the package SPSS 20.0. F-tests for main effects were obtained using one-way ANOVA (weighted method). For one-way ANOVA analyses we divided our sample of patients into two groups based on age-related reference values and where these were not available, statistically determined cut-off values for each cellular parameter to investigate whether a certain cell count or ratio might be related to better serologic response.
We handled pre- and postvaccination HI titers in two ways.
We analyzed GMT levels at pre- and postvaccination: due to skewed distributions, analyses were performed on the natural log of HI titer and arithmetic means were converted to GMT with exponential transformation.
We calculated values of GMFI between pre- and postvaccination: as it was discussed earlier (19) that in a population which is not entirely seronegative before immunization, prevaccination HI titer levels have significant influence on postvaccination titers, we examined the ratio of post-/prevaccination GMTs.
Due to the methodology of serologic analyses, negative specimens (undetectable titer levels) were assigned a nominal value of 5 for the purposes of statistical analysis. For each test, a p-value < 0.05 was considered significant.
We analyzed day 0 results for the following parameters: absolute lymphocyte count, total CD3+ T, CD4+ Th and CD8+ Tc cell count, CD4/CD8 ratio, CD3+CD45RA+ naive and CD3+CD45RO+ memory T cell count and naive/memory T cell ratio. Furthermore, we followed Treg cell (CD3+CD4+CD25High) and activated Thelper (CD3+CD4+CD25Low) cell counts, CD3+CD4+CD25High/Low ratio, CD3+CD56+ NKT-like and CD56+ NK cell counts; and compared them with postvaccination HI titers (postvaccination GMT) or with the GMFI between day 0 and day 28. We conducted these studies (postvaccination GMT and GMFI) separately for each virus strain: H1N1pdm09-like, H3N2-like and B/Brisbane strain.
GMTs, seroprotection and seroconversion rates were calculated on day 0 and on day 28. GMTs of antibodies to different influenza virus strains are listed in Table 2. All postvaccination GMTs were higher than prevaccination GMTs, regarding H1N1, H3N2 and B/Brisbane strains, and examining GMFI, increases between them were significant. Seroprotection and seroconversion rates according to virus strains are shown in Table 3.

Table 2 GMT and GMFI values on day 0 (prevaccination) and day 21-28 (postvaccination) according to virus strains.

Table 3 Pre- and postvaccination rates for seroprotection† and seroconversion‡ by virus strains.
According to the age-matched reference intervals provided by Huenecke et al. (20) we observed that in most cases, total lymphocyte count, CD3+, CD4+, CD8+ and CD56+ counts were under the lower limit of age-related intervals. CD4/CD8 ratio was within the normal range in 52% of our patients. Interestingly, percentages of CD3CD25+ activated T cells and CD4CD25+ activated Th cells were in normal ranges in all of our patients. For certain subpopulations however, no age-dependent reference ranges were available. Since intervals were not available for CD3+CD56+ NKT cells, we used the predicted values and found that 50% of our patients had results under this cut-off value. Descriptive results are summarized in Table 4.
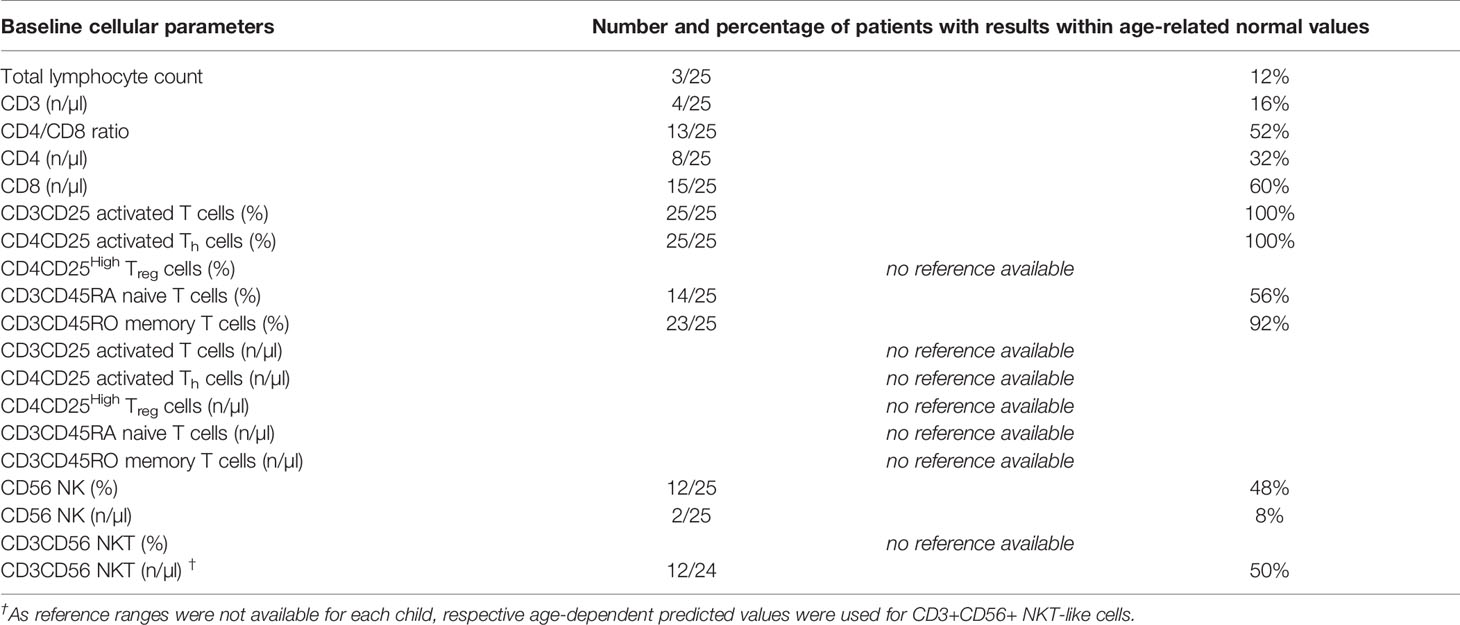
Table 4 Flow cytometry results describing the baseline cellular parameters (absolute counts and percentages) compared to age-related normal values.
Supplementary Table 1. shows the absolute cell numbers and percentages analyzed using flow cytometry and the ratios of certain cells. By assessing specific cell population counts, we examined the relations between lymphocyte subpopulations and their ratios and the outcome of vaccination. The associations of prevaccination T cells and GMT and GMFI by different strains is shown in Tables 5 and 6. As mentioned before, a p-value < 0.05 was considered significant for each test.
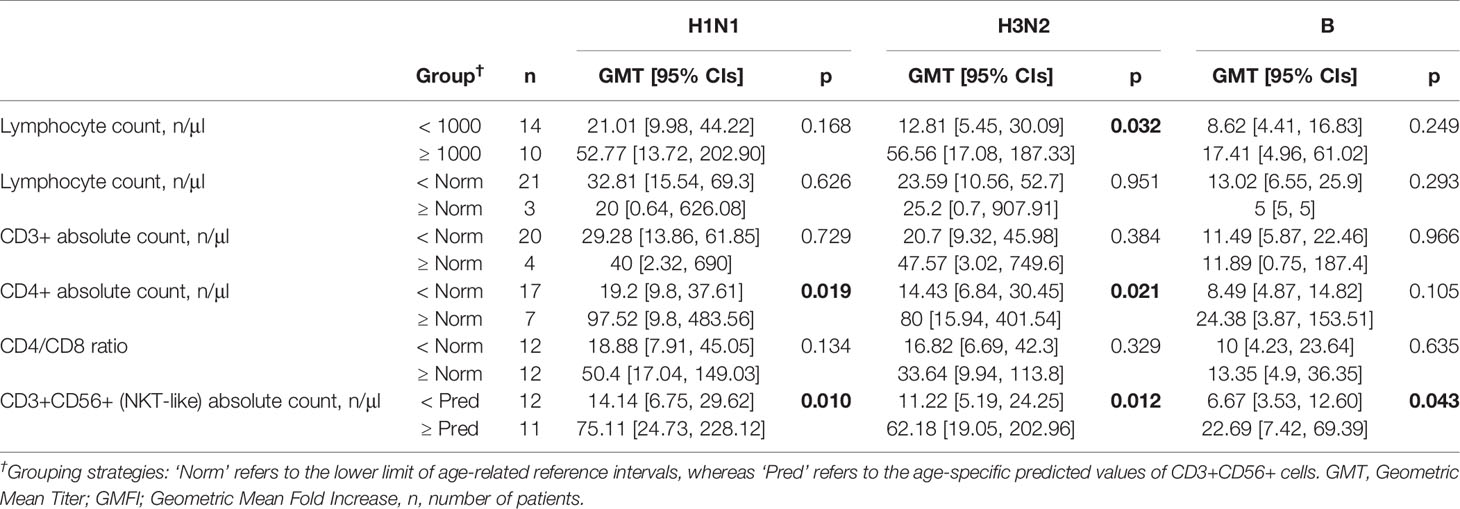
Table 5 Relations between different prevaccination cellular parameters and postvaccination GMT by virus strains. Significant results are written in bold.
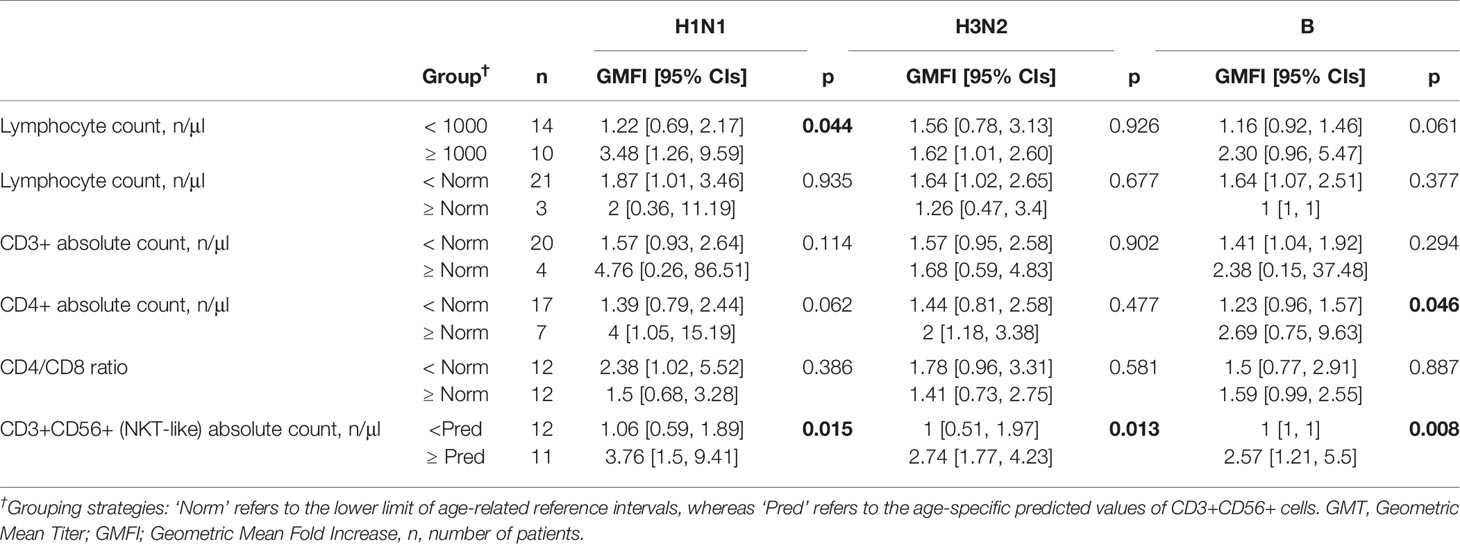
Table 6 Relations between different prevaccination cellular parameters and GMFI by virus strains. Significant results are written in bold.
By one-way ANOVA, we did not find a relation between age-related baseline absolute lymphocyte counts and postvaccination GMT and GMFI against the three influenza strains. However, after comparing the immune response of patients with absolute lymphocyte cell counts below or above 1000/µl, these results suggested a positive association between higher cell counts and vaccine response. We found a positive relation with the postvaccination GMT elevation against H3N2 (12.81 vs. 56.56), and GMFI regarding H1N1 (1.22-fold vs. 3.48-fold).
Regarding CD4+ lymphocytes, we expected better immune responses in patients with CD4+ cell counts in the normal age-specific range and they showed significantly better results in postvaccination GMT elevation for H1N1 and H3N2 strains (97.52 vs. 19.2 and 80 vs. 14.43, respectively). However, GMFI results were significant only against B strain.
Analyses of age-related predicted values of CD3+CD56+ cells showed significant relations both with postvaccination GMT elevation and GMFI against all three strains. Patients with CD3+CD56+ counts above the predicted threshold had better responses in GMT after vaccination (H1N1: 75.11 vs. 14.14; H3N2: 62.18 vs. 11.22; B: 22.69 vs. 6.67). GMFI results were significant regarding all strains as well (H1N1: 3.76-fold vs. 1.06-fold, H3N2: 2.74-fold vs. 1, B: 2.57-fold vs. 1).
Considering that age-specific references were not available for all measured cellular parameters, we tried to establish cut-off values based on statistical methods.
We compared the role of Treg cells and found that the ratio of regulatory/activated T cells (CD3+CD4+CD25High vs. CD3+CD4+CD25Low) above 10% suggested a negative association with postvaccination GMT results in H3N2 strain (42.02 vs. 10.72, respectively). Patients with an absolute Treg (CD3+CD4+CD25High) cell count <10/µl showed a tendency to have higher GMFI (2.46-fold vs. 1.16-fold) against H3N2 strain. The activated T cell (CD3+CD4+CD25Low) count did not show relations with postvaccination GMT or GMFI with any of the strains.
Analyses of CD4/CD8 ratio, CD3+CD45RA+ naive and CD3+CD45RO+ memory T cell counts, naive/memory T cell ratio, CD3+, CD8+, and CD56+ NK cell counts did not show significant associations with immune response against any of the strains.
We recorded no local adverse reactions (injection site induration, erythema, swelling or warmth). No medical intervention was necessary. No vaccine related serious adverse event was observed. There were no breakthrough influenza infections.
Myelosuppressive effects of therapeutic protocols are considerably diverse depending on the underlying malignancy and the cytotoxic agents administered. In hematological malignancies immunosuppressive effects persist during treatment and recovery can take more than 12 months after cessation of therapy. Acute lymphocytic leukemia patients have decreased lymphocyte counts in all major groups compromising both humoral and cellular immunity possibly affecting preexisting humoral protection resulting from childhood vaccinations or previous infections. Total leukocyte and lymphocyte counts were found to be comparable to healthy children after 1 year (21). However, flow cytometry investigations demonstrated that recovery of specific subsets might take much longer (22), CD3+, CD4+, CD8+ cells were affected most (23–25). Recovery of naive T cells to age-related normal levels was found to take 1-6 months (22, 26), which can be explained by the ability of the thymus to produce new naive cells in childhood.
CD4+ cell counts were found to be persistently low in a long term investigation of pediatric ALL patients, with decreases both in CD3+CD45RO and CD3+CD45RA subsets (21, 26). Significant decrease in the ratio of CD4+ and CD8+ cells was reported in multiple studies during and after chemotherapy treatment (27). NK cells did not show significant differences after different time points of treatment completion (21).
Solid tumor patients show much faster reconstitution of immune status. Lower immunoglobulin levels mostly recovered within the first six months. Severely decreased CD4+ T cell count resulting in lower CD4+/CD8+ ratio, persisted briefly after therapy compared to leukemia patients. Total T lymphocytes recovered within six to twelve months (28, 29). NK cells were found to be increased immediately after treatment and normalized within 6 months (28).
As we expected, our patients had markedly lower cell counts in most measured subpopulations so we anticipated a modest immune response against influenza vaccination. A recently published multicenter immunogenicity trial with a trivalent influenza vaccine of the same manufacturer and composition as the one used in our study gave us the opportunity to compare our results to healthy children. In two age groups (3-11 years and 12-18 years) postvaccination seroprotection rates varied between 80-96.67% and seroconversion rates were between 58.33-70% (30). Although in our group of patients, postvaccination GMTs were significantly higher than prevaccination values against all three strains, considerably worse seroconversion and seroprotection results were consistent with reports in immunocompromised populations.
Based on our previous results (4) and other reports on the predictive value of baseline lymphocyte counts (5, 8), we expected a positive association between the absolute lymphocyte count above 1000/µl on day 0 and HI titer changes independent of virus strains. We could reconfirm these results against H3N2 in GMT and H1N1 and B in GMFI. Analyses based on age-related normal values did not show significant associations with vaccine response.
We expected to find a positive relation between higher CD4+ (Thelper) cell counts and the serosresponse. In healthy adults, the predictive role of absolute CD4+ T cell count has already been reported. Jürchott et al. (31) found that CD4+ T cell count along with other factors could predict seroprotection against pandemic influenza strain (A(H1N1)pdm09) with 89% accuracy. We found that baseline absolute CD4+ T cell count within the age-related interval showed a positive relation with both postvaccination GMT (H1N1, H3N2) and GMFI (B/Brisbane). Furthermore, this result seems to be consistent with findings in vaccine research regarding other immunocompromised populations such as HIV infected individuals, where the ability to mount a strong response is largely dependent on CD4+ cell count.
The most noteworthy result we recognised was the positive association of day 0 CD3+CD56+ (NKT-like) cell count above the age-specific predicted values and both postvaccination GMT and GMFI. We observed the most predictive role of these cells for the seroresponse against all strains of influenza virus.
According to Romero-Olmedo et al. (32), human peripheral blood CD3+CD56+ cells constitute a phenotypical continuum of different natural T cell subsets such as CD8+ or CD4-CD8- (double negative), γδ+ and MAIT cells. They demonstrated that both in healthy and allergic adults, CD3+CD56+ cells were actually part of all major T cell groups rather than a separate group.
Expression of CD56 has been associated with cytotoxic and immunostimulatory properties (33) and has been found on several activated cell types that also show cytotoxic properties. This finding suggests that CD56 is more of a sign of activation than a characteristic phenotypical marker.
However, we think that these results might have more importance in influenza vaccine research. CD3 and CD56 markers have been associated with NKT cells as well. Although the terminology of these cells is quite discordant (34), they are often referred to as NKT-like cells, a heterogeneous group of T cells that have been the target of extensive research regarding influenza vaccines. CD3+CD56+ (NKT-like) cells can carry out MHC-unrestricted cytotoxicity and secrete many kinds of cytokines. They confer natural immunity and play a part in helping the differentiation of helper T cells.
Several research groups have demonstrated that activation of NKT cells contribute to the humoral immune response to different microbes (35), however, most of these studies were conducted in animals. In connection with influenza vaccination, these studies demonstrated that use of glycolipid adjuvants (e.g. α-galactosylceramide) as NKT cell activators lead to better immunological response (36–38). Regarding recent investigations into the immunology of SARS-CoV-2 infection, lower percentages of CD3+CD56+ (NKT-like) cells have been observed in COVID-19 subjects when compared to healthy controls. Further comparison of patients with severe and non-severe pneumonia showed significantly lower percentages in the former group of subjects (39).
A possible theory is that the relationship between the immune response and the number of NKT-like cells in this immunosuppressed population might originate from their homing characteristics. Most of these cells migrate and reside to different tissues (40), therefore they might form a pool of mobile cells during chemotherapy. However there are only a few reports about findings that support this phenomenon (41, 42).
We would like to further investigate and confirm our results by an extended, nationwide study of the connection between prevaccination lymphocyte subpopulations, especially NKT-like cells (with more detailed identification) and the outcome of influenza vaccination in children undergoing chemotherapy.
As we expected, a modest immunogenicity was observed in our patients. These findings seemed to be in agreement with published reports.
Our study has several limitations. The patient sample was considerably heterogeneous in respect of specific hemato-oncologic diseases and types of cytostatic treatment. Statistically the sample size was quite small and no control group was established. Consequently, our results should be treated with caution. Nevertheless, we tried to compensate it with sampling mostly those patients, who received parenteral cytostatic treatment. Additionally, we used a conventional p value of 0.05.
To our knowledge, we revealed for the first time some possible connections between T-lymphocyte subpopulation counts at the time of vaccination and seroresponse to influenza vaccination in immunosuppressed patients. From a practical point of view, although in a small, but highly immunosuppressed study population our investigation suggests a possible positive association between NKT-like cells and postvaccination GMT and GMFI in all three strains following influenza vaccination.
After verifying our results on a larger sample with a control group, it can outline a promising direction for research to further specify the associations of the previously mentioned cell populations and their ratios and serologic immunity. Our investigation highlights the need for age-specific reference ranges for T cell subpopulations. Moreover, should our results be verified, they could support the possible advantages of incorporating NKT cell-activating adjuvants into influenza vaccines.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Institutional Review Board of the University of Pécs, Pécs, Hungary (3672.316-2954/2010). Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
EL: Data curation (supporting); Writing – Original Draft Preparation (equal); Writing – Review and Editing (equal). GP: Data curation (lead); Formal analysis (lead); Investigation (equal); Visualization; Writing – Review and Editing (equal). NB: Conceptualization (equal); Data curation (equal); Investigation (equal). TB: Conceptualization (equal); Data curation (equal); Investigation (equal); Writing – Review and Editing (equal); IJ: Data curation (equal); Investigation (equal). RM: Supervision; Writing – Review and Editing (equal). GO: Conceptualization (lead); Data curation (equal); Funding acquisition; Investigation (equal); Project administration (lead); Writing – Original Draft Preparation (equal); Writing – Review and Editing (equal). All authors contributed to the article and approved the submitted version.
Statistical work was partially financed by 2020-4.1.1-TKP2020, the Subprogram 3: “Innovation for sustainable life and environment” of “Scientific Field Excellence Program 2020” of the Hungarian Government.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We would like to thank our patients, their parents and our staff at the Division of Pediatric Hematology and Oncology who participated in our study.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2021.690940/full#supplementary-material
ALL, acute lymphoblastic leukemia; AML, acute myeloid leukemia; HI, hemagglutination inhibition; GMT, geometric mean titer; GMFI, geometric mean fold increase; MHC, Major Histocompatibility Complex; MAIT, mucosa associated invariant T cells; MR-1, MHC-related molecule-1; NKT cells, natural killer T cells; PNET, primitive neuroectodermal tumor; SPSS, Statistical Package for Social Sciences; Th, helper T cells; Tc, cytotoxic T cells; Treg, regulatory T cells.
1. Zawitkowska J, Lejman M, Drabko K, Zaucha-Prażmo A. Diagnostic Difficulties of AH1N1 Influenza Infection in Children With Acute Lymphoblastic Leukemia: Two Case Reports. Med (Baltimore) (2020) 99(43):e22790. doi: 10.1097/MD.0000000000022790
2. Lee GE, Fisher BT, Xiao R, Coffin SE, Feemster K, Seif AE, et al. Burden of Influenza-Related Hospitalizations and Attributable Mortality in Pediatric Acute Lymphoblastic Leukemia. J Pediatr Infect Dis Soc (2015) 4(4):290–6. doi: 10.1093/jpids/piu066
3. Kersun LS, Reilly AF, Coffin SE, Sullivan KE. Protecting Pediatric Oncology Patients From Influenza. Oncologist (2013) 18(2):204–11. doi: 10.1634/theoncologist.2012-0401
4. Ottóffy G, Horváth P, Muth L, Sólyom A, Garami M, Kovács G, et al. Immunogenicity of a 2009 Pandemic Influenza Virus a H1N1 Vaccine, Administered Simultaneously With the Seasonal Influenza Vaccine, in Children Receiving Chemotherapy: Influenza Vaccination During Chemotherapy. Pediatr Blood Cancer (2014) 61(6):1013–6. doi: 10.1002/pbc.24893
5. Yen T-Y, Jou S-T, Yang Y-L, Chang H-H, Lu M-Y, Lin D-T, et al. Immune Response to 2009 Pandemic H1N1 Influenza Virus a Monovalent Vaccine in Children With Cancer. Pediatr Blood Cancer (2011) 57(7):1154–8. doi: 10.1002/pbc.23113
6. Mavinkurve-Groothuis AMC, van der Flier M, Stelma F, van Leer-Buter C, Preijers FW, Hoogerbrugge PM. Absolute Lymphocyte Count Predicts the Response to New Influenza Virus H1N1 Vaccination in Pediatric Cancer Patients. Clin Vaccine Immunol (2013) 20(1):118–21. doi: 10.1128/CVI.00585-12
7. Kotecha RS, Wadia UD, Jacoby P, Ryan AL, Blyth CC, Keil AD, et al. Immunogenicity and Clinical Effectiveness of the Trivalent Inactivated Influenza Vaccine in Immunocompromised Children Undergoing Treatment for Cancer. Cancer Med (2016) 5(2):285–93. doi: 10.1002/cam4.596
8. Choi DK, Fuleihan RL, Walterhouse DO. Serologic Response and Clinical Efficacy of Influenza Vaccination in Children and Young Adults on Chemotherapy for Cancer. Pediatr Blood Cancer (2016) 63(11):2011–8. doi: 10.1002/pbc.26110
9. Doganis D, Kafasi A, Dana H, Spanakis N, Baka M, Pourtsidis A, et al. Immune Response to Influenza Vaccination in Children With Cancer. Hum Vaccines Immunother (2018) Sep 214(9):2310–7. doi: 10.1080/21645515.2018.1470734
10. Pawelec G, McElhaney J. Recent Advances in Influenza Vaccines. F1000Research (2020) 9:305. doi: 10.12688/f1000research.22611.1
11. Wong-Chew RM, Frías MN, García-León ML, Arriaga-Pizano L, Sanson AM, Lopez-Macías C, et al. Humoral and Cellular Immune Responses to Influenza Vaccination in Children With Cancer Receiving Chemotherapy. Oncol Lett (2012) 4(2):329–33. doi: 10.3892/ol.2012.721
12. Kersun LS, Reilly A, Coffin SE, Boyer J, Luning Prak ET, McDonald K, et al. A Prospective Study of Chemotherapy Immunologic Effects and Predictors of Humoral Influenza Vaccine Responses in a Pediatric Oncology Cohort: Influenza Vaccine Efficacy. Influenza Other Respir Viruses (2013) 7(6):1158–67. doi: 10.1111/irv.12058
13. Driver JP, de Carvalho Madrid DM, Gu W, Artiaga BL, Richt JA. Modulation of Immune Responses to Influenza a Virus Vaccines by Natural Killer T Cells. Front Immunol (2020) 11:2172. doi: 10.3389/fimmu.2020.02172
14. Ho L, Denney L, Luhn K, Teoh D, Clelland C, McMichael AJ. Activation of Invariant NKT Cells Enhances the Innate Immune Response and Improves the Disease Course in Influenza a Virus Infection. Eur J Immunol (2008) 38(7):1913–22. doi: 10.1002/eji.200738017
15. Artiaga BL, Yang G, Hutchinson TE, Loeb JC, Richt JA, Lednicky JA, et al. Rapid Control of Pandemic H1N1 Influenza by Targeting NKT-Cells. Sci Rep (2016) 6(1):37999. doi: 10.1038/srep37999
16. Csohán A, Zsuzsanna M, Márta M, Zsuzsanna P, Krisztina B, Zsuzsanna J. Az Országos Epidemiológiai Központ módszertani levele a 2016. évi védőoltásokról (Methodological manual of vaccinations in 2016) [Internet]. Epinfo; 2016. Available from: http://www.oek.hu/oek.web?nid=444&pid=1.
17. EMMI módszertani levele a 2017. évi védőoltásokról (Methodological manual of vaccinations in 2017). Egészségügyi Közlöny [Internet]. 2017 66(7). Available from: https://www.antsz.hu/data/cms83440/VML2017_EMMI.pdf.
18. World Health Organization. Manual for the Laboratory Diagnosis and Virological Surveillance of Influenza. Geneva: World Health Organization (2011). 139 p.
19. Beyer WEP, Palache AM, Lüchters G, Nauta J, Osterhaus ADME. Seroprotection Rate, Mean Fold Increase, Seroconversion Rate: Which Parameter Adequately Expresses Seroresponse to Influenza Vaccination? Virus Res (2004) 103(1–2):125–32. doi: 10.1016/j.virusres.2004.02.024
20. Huenecke S, Behl M, Fadler C, Zimmermann SY, Bochennek K, Tramsen L, et al. Age-Matched Lymphocyte Subpopulation Reference Values in Childhood and Adolescence: Application of Exponential Regression Analysis: Continuous Lymphocyte Reference Values. Eur J Haematol (2008) 80(6):532–9. doi: 10.1111/j.1600-0609.2008.01052.x
21. Mazur B, Szczepański T, Karpe J, Sońta-Jakimczyk D, Bubała H, Torbus M. Decreased Numbers of CD4+ T Lymphocytes in Peripheral Blood After Treatment of Childhood Acute Lymphoblastic Leukemia. Leuk Res (2006) 30(1):33–6. doi: 10.1016/j.leukres.2005.05.024
22. Alanko S, Salmi TT, Pelliniemi T-T. Recovery of Blood T-Cell Subsets After Chemotherapy for Childhood Acute Lymphoblastlc Leukemia. Pediatr Hematol Oncol (1994) 11(3):281–92. doi: 10.3109/08880019409141671
23. Kosmidis S, Baka M, Bouhoutsou D, Doganis D, Kallergi C, Douladiris N, et al. Longitudinal Assessment of Immunological Status and Rate of Immune Recovery Following Treatment in Children With ALL. Pediatr Blood Cancer (2008) 50(3):528–32. doi: 10.1002/pbc.21327
24. Reilly A, Kersun LS, Luning Prak E, Boyer J, McDonald K, Jawad AF, et al. Immunologic Consequences of Chemotherapy for Acute Myeloid Leukemia. J Pediatr Hematol Oncol (2013) 35(1):46–53. doi: 10.1097/MPH.0b013e318266c0c8
25. Geerlinks AV, Issekutz T, Wahlstrom JT, Sullivan KE, Cowan MJ, Dvorak CC, et al. Severe, Persistent, and Fatal T-Cell Immunodeficiency Following Therapy for Infantile Leukemia. Pediatr Blood Cancer (2016) 63(11):2046–9. doi: 10.1002/pbc.26108
26. van Tilburg CM, van Gent R, Bierings MB, Otto SA, Sanders EAM, Nibbelke EE, et al. Immune Reconstitution in Children Following Chemotherapy for Haematological Malignancies: A Long-Term Follow-Up: Immune Reconstitution Following Childhood Cancer Treatment. Br J Haematol (2011) 152(2):201–10. doi: 10.1111/j.1365-2141.2010.08478.x
27. Lovat PE, Robinson JH, Windebank KP, Kernahan J, Watson JG. Serial Study of T Lymphocytes in Childhood Leukemia During Remission. Pediatr Hematol Oncol (1993) 10(2):129–39. doi: 10.3109/08880019309016546
28. Kantar M. Immune Deficiencies Following Cancer Treatment in Children. J Trop Pediatr (2003) 49(5):286–90. doi: 10.1093/tropej/49.5.286
29. Alanko S, Pelhiemi T-T, Salmi TT. Recovery of Blood Lymphocytes and Serum Immunoglobulins After Treatment of Solid Tumors in Children. Pediatr Hematol Oncol (1994) 11(1):33–45. doi: 10.3109/08880019409141899
30. Vajo Z, Balaton G, Vajo P, Torzsa P. A Reduced Dose Whole Virion Aluminum Adjuvanted Seasonal Influenza Vaccine Is Immunogenic, Safe, and Well Tolerated in Pediatric Patients. Viruses (2021) 13(3):500. doi: 10.3390/v13030500
31. Jürchott K, Schulz AR, Bozzetti C, Pohlmann D, Stervbo U, Warth S, et al. Highly Predictive Model for a Protective Immune Response to the a(H1N1)Pdm2009 Influenza Strain After Seasonal Vaccination. Kang S-M editor PloS One (2016) 11(3):e0150812. doi: 10.1371/journal.pone.0150812
32. Romero-Olmedo AJ, Schulz AR, Huber M, Brehm CU, Chang H, Chiarolla CM, et al. Deep Phenotypical Characterization of Human CD3 + CD56 + T Cells by Mass Cytometry. Eur J Immunol (2021) 51(3):672–81. doi: 10.1002/eji.202048941
33. Van Acker HH, Capsomidis A, Smits EL, Van Tendeloo VF. CD56 in the Immune System: More Than a Marker for Cytotoxicity? Front Immunol (2017) 8:892. doi: 10.3389/fimmu.2017.00892
34. Godfrey DI, MacDonald HR, Kronenberg M, Smyth MJ, Kaer LV. NKT Cells: What’s in a Name? Nat Rev Immunol (2004) 4(3):231–7. doi: 10.1038/nri1309
35. Lang ML. The Influence of Invariant Natural Killer T Cells on Humoral Immunity to T-Dependent and -Independent Antigens. Front Immunol (2018) 9:305. doi: 10.3389/fimmu.2018.00305
36. Galli G, Pittoni P, Tonti E, Malzone C, Uematsu Y, Tortoli M, et al. Invariant NKT Cells Sustain Specific B Cell Responses and Memory. Proc Natl Acad Sci (2007) 104(10):3984–9. doi: 10.1073/pnas.0700191104
37. Dwivedi V, Manickam C, Dhakal S, Binjawadagi B, Ouyang K, Hiremath J, et al. Adjuvant Effects of Invariant NKT Cell Ligand Potentiates the Innate and Adaptive Immunity to an Inactivated H1N1 Swine Influenza Virus Vaccine in Pigs. Vet Microbiol (2016) 186:157–63. doi: 10.1016/j.vetmic.2016.02.028
38. Artiaga BL, Yang G, Hackmann TJ, Liu Q, Richt JA, Salek-Ardakani S, et al. α-Galactosylceramide Protects Swine Against Influenza Infection When Administered as a Vaccine Adjuvant. Sci Rep (2016) 6(1):23593. doi: 10.1038/srep23593
39. Zingaropoli MA, Perri V, Pasculli P, Cogliati Dezza F, Nijhawan P, Savelloni G, et al. Major Reduction of NKT Cells in Patients With Severe COVID-19 Pneumonia. Clin Immunol Orlando Fla (2021) 222:108630. doi: 10.1016/j.clim.2020.108630
40. Slauenwhite D, Johnston B. Regulation of NKT Cell Localization in Homeostasis and Infection(2015) (Accessed 2021 May 23).
41. Rico MJ, Rozados VR, Mainetti LE, Zacarias Fluck MF, Matar P, Scharovsky OG. Regulatory T Cells But Not NKT I Cells Are Modulated by a Single Low-Dose Cyclophosphamide in a B Cell Lymphoma Tumor Model. Exp Oncol (2012) 5(1):38–42.
Keywords: influenza vaccines, pediatrics, immunosuppression, natural killer T-cells, lymphocyte subsets, cellular immunity, CD4+ T-cells
Citation: Leibinger EA, Pauler G, Benedek N, Berki T, Jankovics I, McNally R and Ottóffy G (2021) Baseline CD3+CD56+ (NKT-like) Cells and the Outcome of Influenza Vaccination in Children Undergoing Chemotherapy. Front. Immunol. 12:690940. doi: 10.3389/fimmu.2021.690940
Received: 04 April 2021; Accepted: 15 June 2021;
Published: 29 June 2021.
Edited by:
Jochen Mattner, University of Erlangen Nuremberg, GermanyReviewed by:
Martin R. Goodier, London School of Hygiene and Tropical Medicine, United KingdomCopyright © 2021 Leibinger, Pauler, Benedek, Berki, Jankovics, McNally and Ottóffy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Evelin A. Leibinger, bGVpYmluZ2VyLmV2ZWxpbkBwdGUuaHU=; Gábor Ottóffy, b3R0b2ZmeS5nYWJvckBwdGUuaHU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.