
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Immunol. , 20 April 2021
Sec. Cancer Immunity and Immunotherapy
Volume 12 - 2021 | https://doi.org/10.3389/fimmu.2021.670827
This article is part of the Research Topic Cancer Immunotherapies: From Efficacy to Resistance Mechanisms View all 42 articles
 Emilien Billon1,2,3
Emilien Billon1,2,3 Brice Chanez3
Brice Chanez3 Philippe Rochigneux1,2,3
Philippe Rochigneux1,2,3 Laurence Albiges4
Laurence Albiges4 Cécile Vicier3
Cécile Vicier3 Géraldine Pignot5
Géraldine Pignot5 Jochen Walz5
Jochen Walz5 Anne-Sophie Chretien1,2
Anne-Sophie Chretien1,2 Gwenaelle Gravis3
Gwenaelle Gravis3 Daniel Olive1,2*
Daniel Olive1,2*The development of immune checkpoint inhibitors (ICI) has dramatically changed the landscape of therapies for metastatic renal cell carcinoma. However, many patients do not benefit from such therapy and prognostic or predictive validated biomarker validated for ICI are still needed to better select and treat patient. Plasmatic soluble immune checkpoints have been described as potential immune biomarkers in hematological malignancies and solids tumors, then, we would like to explore the prognostic value of different soluble immune checkpoints in patients with mRCC treated with nivolumab after TKI. We prospectively collected plasma samples before nivolumab infusion from 38 patients previously treated for mRCC with TKI at Paoli-Calmettes Institute, from the NIVOREN GETUG-AFU 26 study (NCT03013335). Enzyme-linked immunosorbent assays (ELISA) were performed for soluble forms of PD-1, PD-L1, global BTN3, BTLA, BTN3A1 and BTN2A1. Among the different soluble checkpoints analyzed, only high baseline plasmatic level of BTN2A1 was significantly associated with shorter PFS: median PFS was 3.95 months for sBTN2A1high vs 14.30 months for sBTN2A1low (sBTN2A1 cut-off: 6.7ng/mL; HR = 2.26, 95%CI [0.68 – 4.60], p = 0.0307). There was no statistical difference in OS between sBTN2A1high and sBTN2A1low. Our results suggest that the baseline level of plasmatic BTN2A1 could be an independent prognosis factor of PFS after nivolumab for pre-treated patient with mRCC. However, these results need to be validated in a larger prospective cohort and the biological role of BTN subfamily and γδ T cell immunity in mRCC must be elucidated.
The development of immune checkpoint inhibitors (ICI) has dramatically changed the landscape of therapies for metastatic renal cell carcinoma (mRCC), as such in first line associated to tyrosine kinase inhibitors (TKI) (1) or as monotherapy (2). However, many patients do not benefit from such therapy and prognostic or predictive validated biomarker validated for ICI are still needed to better select and treat patient according to the best genomic profiles. The International Metastatic RCC Database Consortium (IMDC) prognostic model (3) is used to predict survival and adapted treatment strategy of untreated mRCC patients and was validated for patients previously treated with TKI, before second line TKI. Identifying new prognostic biomarkers in this population is needed to improve treatment strategy for mRCC patients.
Plasmatic soluble immune checkpoints, such as programmed death protein (PD-1) with its ligands PD-L1 and PD-L2, the B7/butyrophilin-like receptors such as butyrophilin sub-family 3A (CD277) members (BTN3A) and butyrophilin sub-family 2A (CD209) members, and the B and T lymphocyte attenuator (BTLA) have been described as potential immune biomarkers in hematological malignancies (4) and solids tumors (pancreas (5), gastric (6), lung cancers (7) and hepatocarcinoma (8)). In localized RCC, sBTLA was associated with poorer relapse-free survival and overall survival (OS) after nephrectomy (9).
We aimed to explore the prognostic value of different soluble immune checkpoints in mRCC treated with nivolumab after TKI.
To explore the prognostic value of different soluble immune checkpoints, we prospectively collected plasma samples before nivolumab infusion from patients previously treated for mRCC with TKI at Paoli-Calmettes Institute (Nivo-Rein cohort), from the NIVOREN GETUG-AFU 26 study (NCT03013335). Enzyme-linked immunosorbent assays (ELISA) were performed for soluble forms of PD-1, PD-L1, global BTN3, BTLA, BTN3A1 and BTN2A1. All patients provided informed consent prior to enrolment. The receiver operating characteristic (ROC) curves were generated for each marker. The areas under the curves (AUC) were assessed to evaluate each marker performance for discriminating short term responder (patients with PFS > median) from long-term responder (patients with PFS < median). Cut-off was selected to obtain the best sensitivity and specificity for discriminating long-term responders from short term responders. Survival analyses were performed using the Kaplan–Meier method and log-rank test. Multivariate analysis of survival was performed using the Cox-regression model, including all variables associated with progression-free survival (PFS) (p < 0.1).
We included 38 patients between March 2016 and November 2017. Patients’ characteristics are summarized in Table 1. With a median follow-up of 19.8 months, 31 (82%) patients had tumor progression and 25 (66%) died. Among the different soluble checkpoints analyzed, only high baseline plasmatic level of BTN2A1 was significantly associated with shorter PFS. Cut-off retained was 6.7ng/mL, that approximate the median value of 6.8ng/mL. There was no significant difference between patients with sBTN2A1low and sBTN2A1high level; excepted for age (Table 1). Median PFS was 3.95 months for sBTN2A1high vs. 14.30 months for sBTN2A1low (Figures 1A–C) (HR = 2.26, 95%CI [0.68 – 4.60], p = 0.0307). There was no statistical difference in OS between sBTN2A1high and sBTN2A1low (median OS = 14.6 vs. 24.5 months, respectively, p = 0.326) (Figures 1D, E). There was no significant impact on survival of plasmatic level of BTLA (median PFS for BTLAhigh 14.3 vs. 7.1 months, HR = 0.57, 95%CI [0.22 – 1.51]; cut-off: 4.33ng/mL), PD-L1 (median PFS for PD-L1high 12.9 vs. 4.1 months, HR = 0.79, 95%CI [0.38 – 1.65]; cut-off: 0.88ng/mL), PD-1 (median PFS for PD-1high 12.9 vs. 4.0 months, HR = 0.59, 95%CI [0.26 – 1.35; cut-off: 0.83ng/mL]), or BTN3A1 (median PFS for BTN3A1high 9.3 vs. 4.7 months, HR = 0.68, 95%CI [0.22 – 2.05]; cut-off: 1.55ng/mL) in this cohort (Supplementary Figure 1).
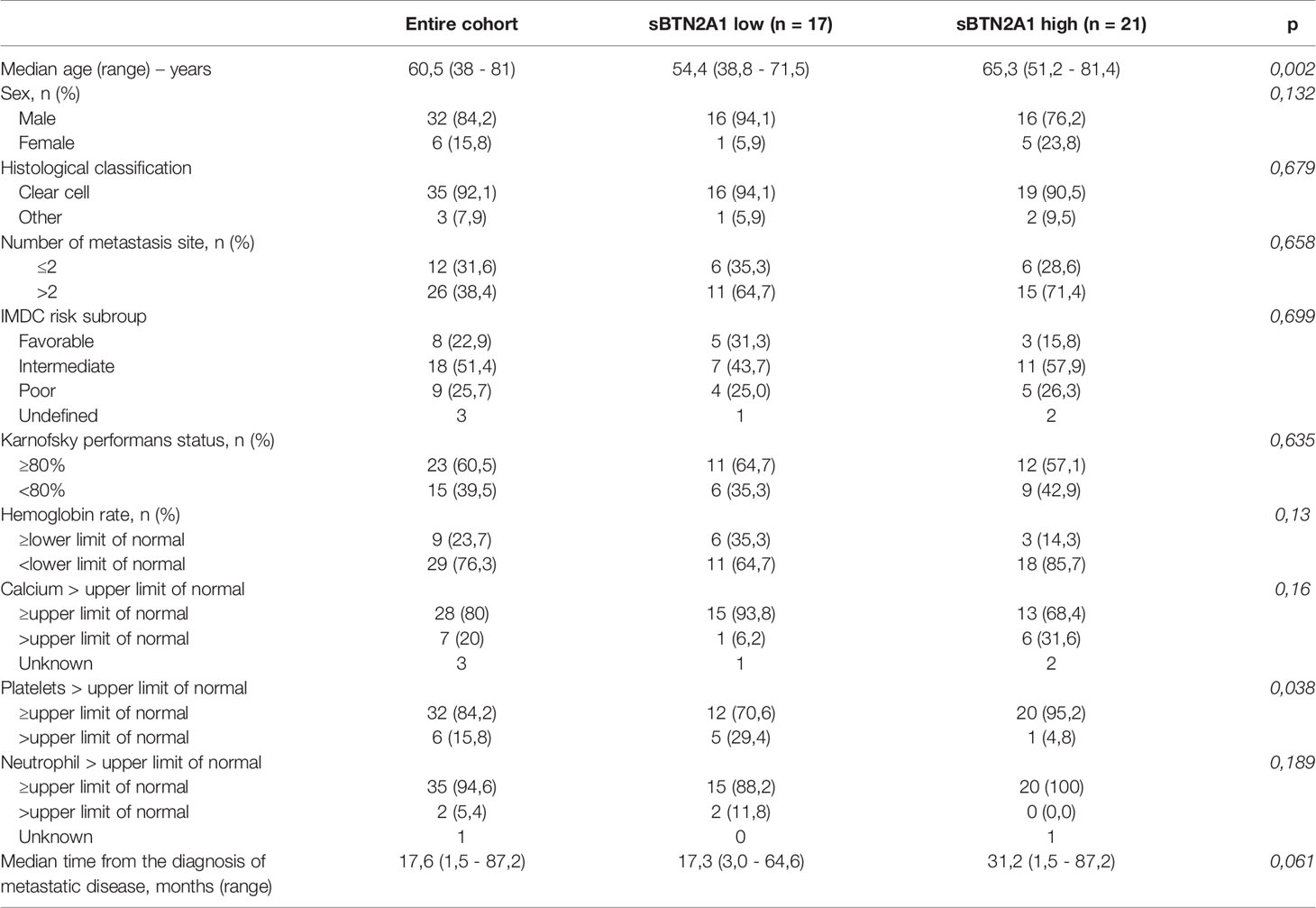
Table 1 Baseline characteristics (n = 38).
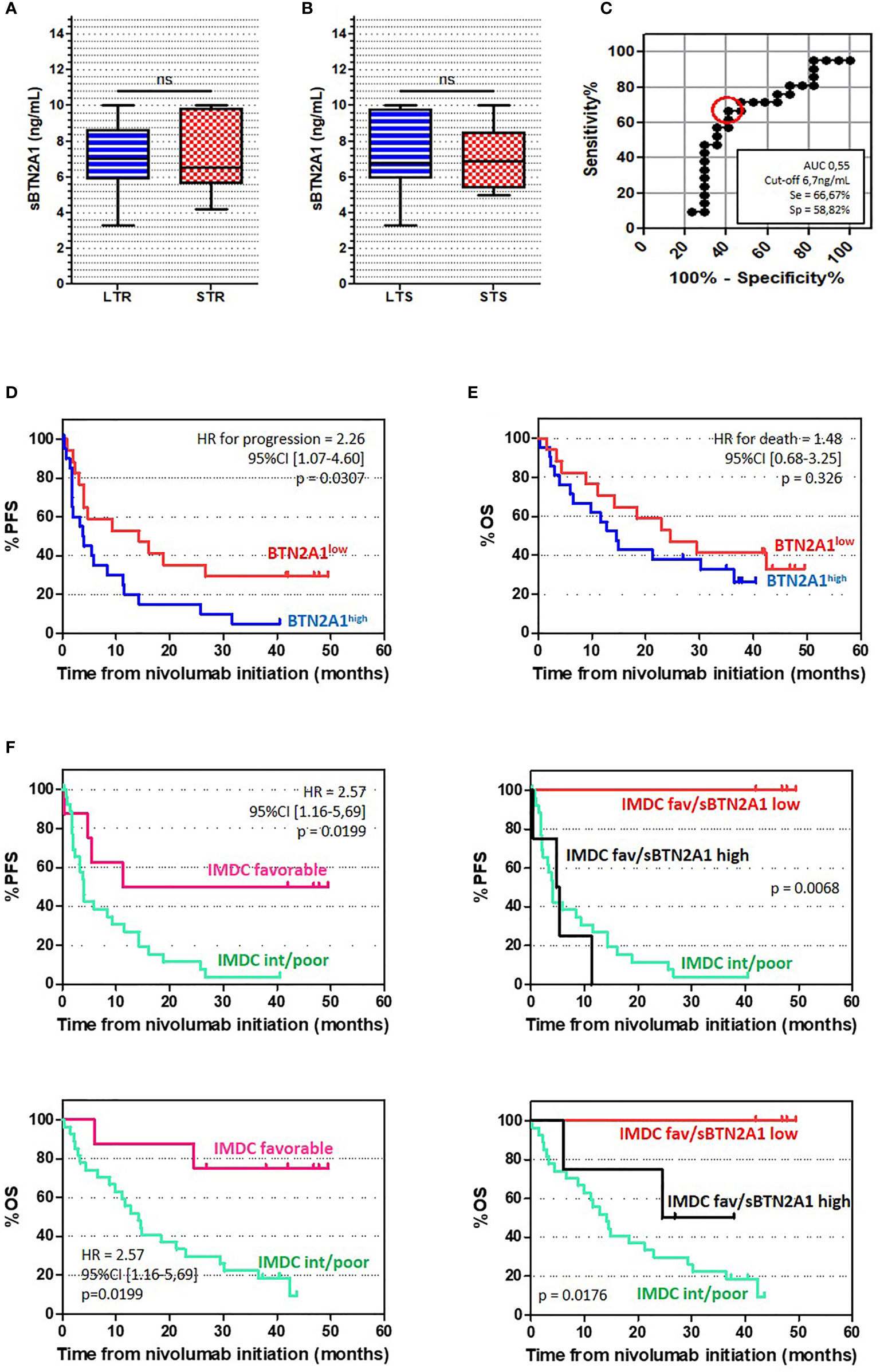
Figure 1 sBTN2A1 seemed to be an independent prognostic factor for PFS in patients with mRCC (A, B) sBTN2A1 expression according to the time of response (A) and the time of overall survival (B), assessed par enzyme linked immunosorbent assay. Paired-t test was used to compare differences between the groups. LTR, Long term responders; patients with PFS > median; STR, short term responders; patients with PFS < median; LTS, Long term survival; patients with OS > median; STS, Short term survival; patients with OS < median. (C) Receiver operating characteristics (ROC) curve analysis of plasma level for sBTN2A1. ROC curve was plotted for sensitivity and specificity of time of response. (D, E) Kaplan Meier analysis of PFS (D) and OS (E) in patients with high and low plasma levels of BTN2A1. (F) Kaplan Meier analysis of PFS (top) and OS (bottom) according to the IMDC prognosis subgroup and sBTN2A1 level.
In univariate analysis, PFS was associated with baseline anemia, IMDC subgroups and sBTN2A1 level (Table 2). sBTN2A1 was associated with PFS in multivariate analysis (HR = 2.80, 95%CI [1.22-6.41], p=0.015) (Table 3). sBTN2A1 was able to discriminate two different prognostic groups among the subgroup of patients with favorable prognosis according to the IMDC model (Figure 1F): favorable IMDC/sBTN2A1high patients had lower PFS than favorable IMDC/sBTN2A1low patients, close to poor/intermediate IMDC patients (median PFS = 5.1months vs. ND, respectively, HR =18.1, p= 0.0067).
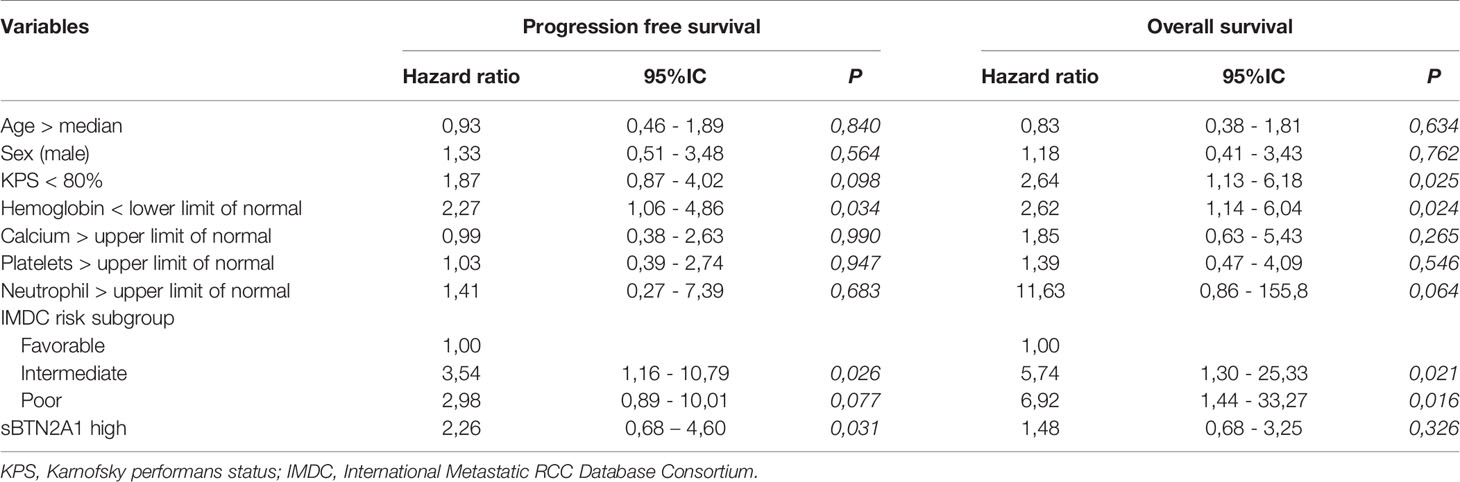
Table 2 Univariate hazard ratio for PFS and OS.
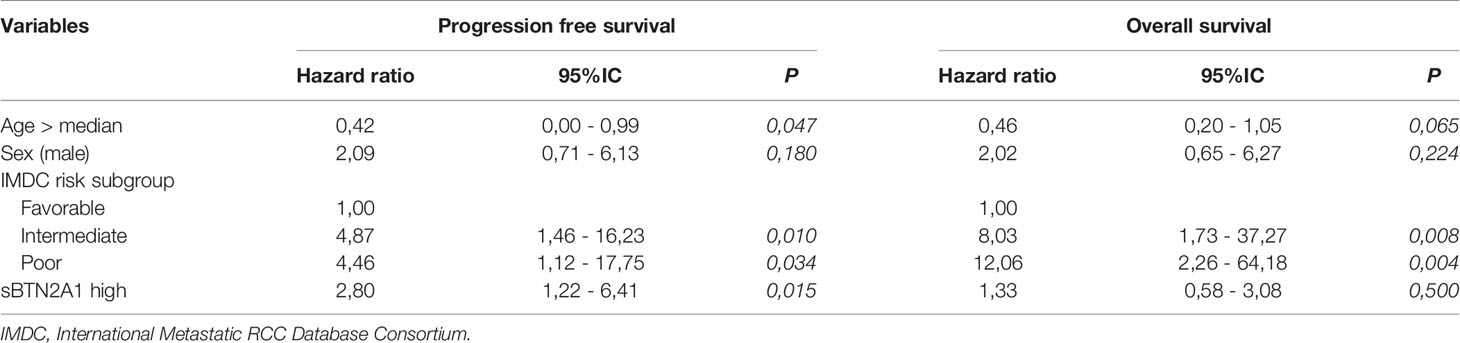
Table 3 Multivariate hazard ratio for PFS and OS.
To our knowledge, this study is the first that described sBTN2A1 as potential prognostic biomarker in patients with pre-treated mRCC. In the previous NIVOREN GETUG-AFU 26 study, it was reported that tissue PD-1 and AXL expression by immunohistochemistry were associated with PFS and confirmed that PBRM-1 loss was a strong prognostic factor (10). Incorvaia et al. explored the prognostic value of soluble forms of PD-1, PD-L1, global BTN3, BTN3A1 and BTN2A1 in a prospective cohort of metastatic renal cell carcinoma patients (11). They identified sPD-1, sPD-L1 and sBTN3A1 as potential biomarkers. However, our study did not significantly confirm these results, with only a tendency for sPD-1 and sPD-L1 and this difference could be explained by the small number of patients in our cohort. Conversely, sBTN2A1 was not significantly associated with survival in their study but patients with PFS > 18 months seemed to have lower level of sBTN2A1 than patients with PFS < 18 months. The small number of patients in their learning cohort (n=21) could also explain the difference between the two works; and reinforce the necessity to validate these results in a larger prospective cohort.
The BTN sub-family plays an important role in Vϒ9Vδ2 T-cells activation and regulation by direct or indirect presentation of self and nonself phosphoantigens. The cell surface molecule BTN2A1 binds to the γδ TCR, in conjunction with BTN3A1, and signals the presence of phosphoantigens to γδ T cells (12). Gamma delta T (γδT) lymphocytes are members of the immune system which display both innate and adaptive functions (13). They recognize low molecular mass nonpeptide ligands named “phosphoantigens” that comprise isoprenoid pathway metabolites, as (E)-4-hydroxy-3-methyl-but-2-enyl PPi (HMB-PP) derived from bacteria and protozoa (14) and isopentenyl PPi (IPP) derived from host cells (15). There are evidence of their cytotoxic activity against tumor cells in certain cancers (16), and they are able to recognize tumor cells without the need for major histocompatibility complex (MHC) antigen presentation. However, there also evidence that suggested that γδT lymphocytes may also have a pro-tumorigenic role (17), by impairing the function of other antitumor immune cells or enhancing immunosuppressive cell function such as MDSCs.
We can hypothesize that high level of circulating BTN2A1 could lead to Vγ9Vδ2 T-cells exhaustion that facilitate tumor immune escape mechanisms (18), and/or activate Vγ9Vδ2 T cells with pro-tumorigenic characteristics, and explain the poorer outcomes of patients with high level of circulating BTN2A1. These Vγ9Vδ2 T-cells alterations could also impaired anti-PD-1 activities on these cells and then, impaired clinical efficacy of anti-PD-1 agents in patients with mRCC.
Soluble BTN2A1 could be a new approach to predict resistance and avoiding toxicities for mRCC treated by nivolumab. Targeting BTN sub-family molecule could represent a new therapy approach for mRCC patients. Despite the small number of patients in this cohort, our results suggest that the baseline level of plasmatic BTN2A1 could be an independent prognosis factor of PFS after nivolumab for pre-treated patient with mRCC. However, these results need to be validated in a larger prospective cohort and the biological role of BTN subfamily and γδ T cell immunity in mRCC must be elucidated.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Institut Paoli Calmettes. The patients/participants provided their written informed consent to participate in this study.
Conception and design: DO, GG. Acquisition of data: EB and BC. Analysis and interpretation of data: EB, BC, and DO. Drafting of the manuscript: EB, PR, and DO. Critical revision of the manuscript for important intellectual content: EB, BC, PR, LA, CV, GP, JW, A-SC, GG, and DO. Statistical analysis: EB. Administrative, technical, or material support: DO. Supervision: DO and GG. All authors contributed to the article and approved the submitted version.
DO is supported by research grant of FRM (Equipe FRM 2018 DEQ20180339209) and RHU Pioneer. EB is supported by ITMO Cancer of Aviesan on funds administered by Inserm.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2021.670827/full#supplementary-material
BTLA, B and T lymphocyte attenuator; BTN, butyrophilin; CI, confidence interval; ELISA, Enzyme-linked immunosorbent assays; HR, hazard ratio; ICI, immune checkpoint inhibitors; IMDC, International Metastatic RCC Database Consortium; mRCC, metastatic renal cell carcinoma; OS, overall survival; PD-1, programmed death protein 1; PDL-1, programmed death ligand 1; PFS, progression-free survival; TKI, tyrosine kinase inhibitor.
1. Rini BI, Plimack ER, Stus V, Gafanov R, Hawkins R, Nosov D, et al. Pembrolizumab Plus Axitinib Versus Sunitinib for Advanced Renal-Cell Carcinoma. N Engl J Med (2019) 380:1116–27. doi: 10.1056/NEJMoa1816714
2. Rini BI, Battle D, Figlin RA, George DJ, Hammers H, Hutson T, et al. The Society for Immunotherapy of Cancer consensus statement on immunotherapy for the treatment of advanced renal cell carcinoma (RCC). J Immunother Cancer (2019) 7(1):354. doi: 10.1186/s40425-019-0813-8
3. Ko JJ, Xie W, Kroeger N, Lee J, Rini BI, Knox JJ, et al. The International Metastatic Renal Cell Carcinoma Database Consortium Model as a Prognostic Tool in Patients With Metastatic Renal Cell Carcinoma Previously Treated With First-Line Targeted Therapy: A Population-Based Study. Lancet Oncol (2015) 16:293–300. doi: 10.1016/S1470-2045(14)71222-7
4. Wang L, Wang H, Chen H, Wang W, Chen X-Q, Geng Q-R, et al. Serum Levels of Soluble Programmed Death Ligand 1 Predict Treatment Response and Progression Free Survival in Multiple Myeloma. Oncotarget (2015) 6:41228–36. doi: 10.18632/oncotarget.5682
5. Benyamine A, Loncle C, Foucher E, Blazquez J-L, Castanier C, Chrétien A-S, et al. BTN3A is a Prognosis Marker and a Promising Target for Vγ9vδ2 T Cells Based-Immunotherapy in Pancreatic Ductal Adenocarcinoma (Pdac). Oncoimmunology (2017) 7:e1372080. doi: 10.1080/2162402X.2017.1372080
6. Takahashi N, Iwasa S, Sasaki Y, Shoji H, Honma Y, Takashima A, et al. Serum Levels of Soluble Programmed Cell Death Ligand 1 as a Prognostic Factor on the First-Line Treatment of Metastatic or Recurrent Gastric Cancer. J Cancer Res Clin Oncol (2016) 142:1727–38. doi: 10.1007/s00432-016-2184-6
7. Okuma Y, Hosomi Y, Nakahara Y, Watanabe K, Sagawa Y, Homma S. High Plasma Levels of Soluble Programmed Cell Death Ligand 1 are Prognostic for Reduced Survival in Advanced Lung Cancer. Lung Cancer Amst Neth (2017) 104:1–6. doi: 10.1016/j.lungcan.2016.11.023
8. Dong MP, Enomoto M, Thuy LTT, Hai H, Hieu VN, Hoang DV, et al. Clinical Significance of Circulating Soluble Immune Checkpoint Proteins in Sorafenib-Treated Patients With Advanced Hepatocellular Carcinoma. Sci Rep (2020) 10:3392. doi: 10.1038/s41598-020-60440-5
9. Wang Q, Zhang J, Tu H, Liang D, Chang DW, Ye Y, et al. Soluble Immune Checkpoint-Related Proteins as Predictors of Tumor Recurrence, Survival, and T Cell Phenotypes in Clear Cell Renal Cell Carcinoma Patients. J Immunother Cancer (2019) 7:334. doi: 10.1186/s40425-019-0810-y
10. Vano Y-A, Rioux-Leclercq N, Dalban C, Sautes-Fridman C, Bougoüin A, Chaput N, et al. Nivoren GETUG-AFU 26 Translational Study: Association of PD-1, AXL, and PBRM-1 With Outcomes in Patients (Pts) With Metastatic Clear Cell Renal Cell Carcinoma (Mccrcc) Treated With Nivolumab (N). J Clin Oncol (2020) 38:618–8. doi: 10.1200/JCO.2020.38.6_suppl.618
11. Incorvaia L, Fanale D, Badalamenti G, Porta C, Olive D, De Luca I, et al. Baseline Plasma Levels of Soluble Pd-1, PD-L1, and BTN3A1 Predict Response to Nivolumab Treatment in Patients With Metastatic Renal Cell Carcinoma: A Step Toward a Biomarker for Therapeutic Decisions. OncoImmunology (2020) 9:1832348. doi: 10.1080/2162402X.2020.1832348
12. Payne KK, Mine JA, Biswas S, Chaurio RA, Perales-Puchalt A, Anadon CM, et al. BTN3A1 governs antitumor responses by coordinating αβ and γδ T cells. Science (2020) 369(3506):942. doi: 10.1126/science.aay2767
13. Davey MS, Willcox CR, Joyce SP, Ladell K, Kasatskaya SA, McLaren JE, et al. Clonal Selection in the Human Vδ1 T Cell Repertoire Indicates γδ TCR-dependent Adaptive Immune Surveillance. Nat Commun (2017) 8:14760. doi: 10.1038/ncomms14760
14. Eberl M, Hintz M, Reichenberg A, Kollas A-K, Wiesner J, Jomaa H. Microbial Isoprenoid Biosynthesis and Human Gammadelta T Cell Activation. FEBS Lett (2003) 544:4–10. doi: 10.1016/s0014-5793(03)00483-6
15. Tanaka Y, Morita CT, Tanaka Y, Nieves E, Brenner MB, Bloom BR. Natural and Synthetic non-Peptide Antigens Recognized by Human Gamma Delta T Cells. Nature (1995) 375:155–8. doi: 10.1038/375155a0
16. Rei M, Pennington DJ, Silva-Santos B. The Emerging Protumor Role of γδ T Lymphocytes: Implications for Cancer Immunotherapy. Cancer Res (2015) 75:798–802. doi: 10.1158/0008-5472.CAN-14-3228
17. Zhao Y, Niu C, Cui J. Gamma-delta (γδ) T cells: friend or foe in cancer development? J Transl Med (2018) 16(1):3. doi: 10.1186/s12967-017-1378-2
Keywords: renal cell carcinoma, butyrophilin, nivolumab, immunotherapy, γδ T cells
Citation: Billon E, Chanez B, Rochigneux P, Albiges L, Vicier C, Pignot G, Walz J, Chretien A-S, Gravis G and Olive D (2021) Soluble BTN2A1 Is a Potential Prognosis Biomarker in Pre-Treated Advanced Renal Cell Carcinoma. Front. Immunol. 12:670827. doi: 10.3389/fimmu.2021.670827
Received: 22 February 2021; Accepted: 06 April 2021;
Published: 20 April 2021.
Edited by:
Nathalie Labarriere, Institut National de la Santé et de la Recherche Médicale (INSERM), FranceReviewed by:
Maeva Dufies, Centre Scientifique de Monaco, MonacoCopyright © 2021 Billon, Chanez, Rochigneux, Albiges, Vicier, Pignot, Walz, Chretien, Gravis and Olive. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Daniel Olive, ZGFuaWVsLm9saXZlQGluc2VybS5mcg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.