 Qi Huang1
Qi Huang1 Wang-Dong Xu
Wang-Dong Xu An-Fang Huang
An-Fang Huang- 1Department of Evidence-Based Medicine, School of Public Health, Southwest Medical University, Luzhou, China
- 2Department of Rheumatology and Immunology, Minda Hospital of Hubei Minzu University, Enshi, China
- 3Department of Nutrition and Food Hygiene, School of Public Health, Southwest Medical University, Luzhou, China
- 4Department of Rheumatology and Immunology, Affiliated Hospital of Southwest Medical University, Luzhou, China
Systemic lupus erythematosus (SLE) and rheumatoid arthritis (RA) are complex autoimmune diseases. CD40 participates in inflammatory response, and promotes fibroblast proliferation, leading to occurrence and progression of SLE, RA. This study explores CD40 gene polymorphisms in SLE and RA patients from a Chinese Han population. Two hundred SLE patients, 340 RA patients, and 900 healthy controls were enrolled. Genomic DNA was extracted from peripheral blood, and six polymorphisms of CD40 gene (rs3765456, rs1569723, rs73115010, rs13040307, rs1883832, and rs4810485) were detected by KASP method. Frequencies of rs1569723 genotypes AA, AC, AA+AC were significantly higher in RA patients as compared to those in healthy controls (P = 0.049, P = 0.024, P = 0.022). Frequencies of genotypes CT, CC+CT of rs1883832, and GT, GG+GT of rs4810485 were significantly higher in RA patients as compared to those in healthy controls (P = 0.012, P = 0.018, P = 0.009, P = 0.015). RA patients carrying rs13040307 C allele and rs73115010 T allele showed increased number of swollen joints. Moreover, frequency of allele T of rs13040307 was lower in SLE patients with positive anti-dsDNA and hematuria as compared to that in patients without these parameters (P = 0.038, P = 0.045). There were increased frequencies of genotype TT, allele T for rs13040307 and lower frequencies of genotype TT, allele T for rs73115010 in lupus patients with myositis (all P<0.05). Interestingly, frequencies of rs1569723 A allele, rs4810485 T allele were higher in SLE patients with myositis, and frequencies of rs3765456 A allele, rs1883832 T allele were lower in SLE patients with myositis (All P<0.05). In conclusion, CD40 gene polymorphisms may associate with susceptibility to SLE and RA.
Introduction
Systemic lupus erythematosus (SLE) and rheumatoid arthritis (RA) are inflammatory autoimmune diseases, with features of chronic inflammation. The main characteristics of RA are progressive joints lesion, synovial hyperplasia, and production of auto-antibodies. SLE relates to various tissues and organs damage, such as skin, blood vessels, kidney (1, 2). Etiology of these two diseases remains unclear. It is recognized that gene polymorphisms have been involved in these disorders pathogenesis (3, 4). To date, at least 88 genomic regions have been identified associated with SLE susceptibility, such as TNFSF4, STAT4, and TNIP1, and about 106 susceptible genes were reported to associate with RA, such as CD28, IL3-CSF2, NFKBIE (5, 6). However, finding out more risk polymorphisms for RA and SLE will be helpful to better elucidate the pathogenesis of these diseases.
CD40 is a glycoprotein with molecular weight 45 to 50 kDa, consisting of 277 amino acids. It is a member of the tumor necrosis factor family of transmembrane glycoproteins and is expressed in different cells, such as B cells, monocytes, dendritic cells, endothelial and epithelial cells, smooth muscle cells, fibroblasts (7). CD40 is a potent T-cell costimulatory factor. It interacts with ligand CD40L, and plays an important role in adaptive immune response, for example, induction of Th1 cell response (8). Human CD40 gene is composed of eight introns and nine exons, located on chromosome 20q11.2 to 13.2. To date, association of CD40 gene and autoimmune disorders has been discussed widely. Chen et al. analyzed three polymorphisms (rs1883832, rs4810485, and rs1569723) of CD40 gene and risk of SLE in a Chinese population. They found that rs1883832 related to development of SLE (9). Nie et al. found relation between rs4810485 and SLE risk in a Chinese population (10). In European origins, studies showed that rs4810485 polymorphism was a risk factor for SLE, RA, and rs3765456 polymorphism was related to RA susceptibility in Korea population (11–13). However, association of rs73115010, rs13040307, and rs1569723 polymorphisms with SLE and RA were discussed in different ethnicities, and showed inconsistent conclusions. Therefore, to better clarify the relationship between CD40 gene polymorphisms and SLE, RA susceptibility, we conducted the present study in a Chinese Han population to evaluate six polymorphisms (rs3765456, rs1569723, rs73115010, rs13040307, rs1883832, and rs4810485) with relation to SLE and RA patients by co-dominant, dominant, and recessive genetic models.
Materials and Methods
Study Sample
This case-control study recruited 200 SLE patients (age, 38.0 [27.0–48.0] years), 340 RA patients (age, 56.0 [48.5–65.0] years) and 900 healthy controls (age, 38.0 [31.0–48.0] years) in Southern Chinese Han origin. All patients came from Department of Rheumatology and Immunology, Affiliated Hospital of Southwest Medical University. Healthy controls were from Physical Examination Center of Jiangyang District Center for Disease Control and Prevention in Luzhou city. RA and SLE patients were diagnosed according to the American College of Rheumatology and European League Against Rheumatism (ACR/EULAR) classification criteria (14, 15). RA patients disease activity was evaluated according to disease activity score 28 (DAS28) (16), and SLE patients disease activity was evaluated according to SLE disease activity index (SLEDAI) (17) (Table 1). This study was admitted by Ethic Research Committee of Southwest Medical University, and informed consent was collected from individual participant. Demographic and clinical characteristics of patients and controls were obtained as well. For instance, clinical characteristics myositis was diagnosed according to participants who had at least three of four items including clinical symptoms, serum creatine kinase level, electromyography, and muscle biopsy results (18).
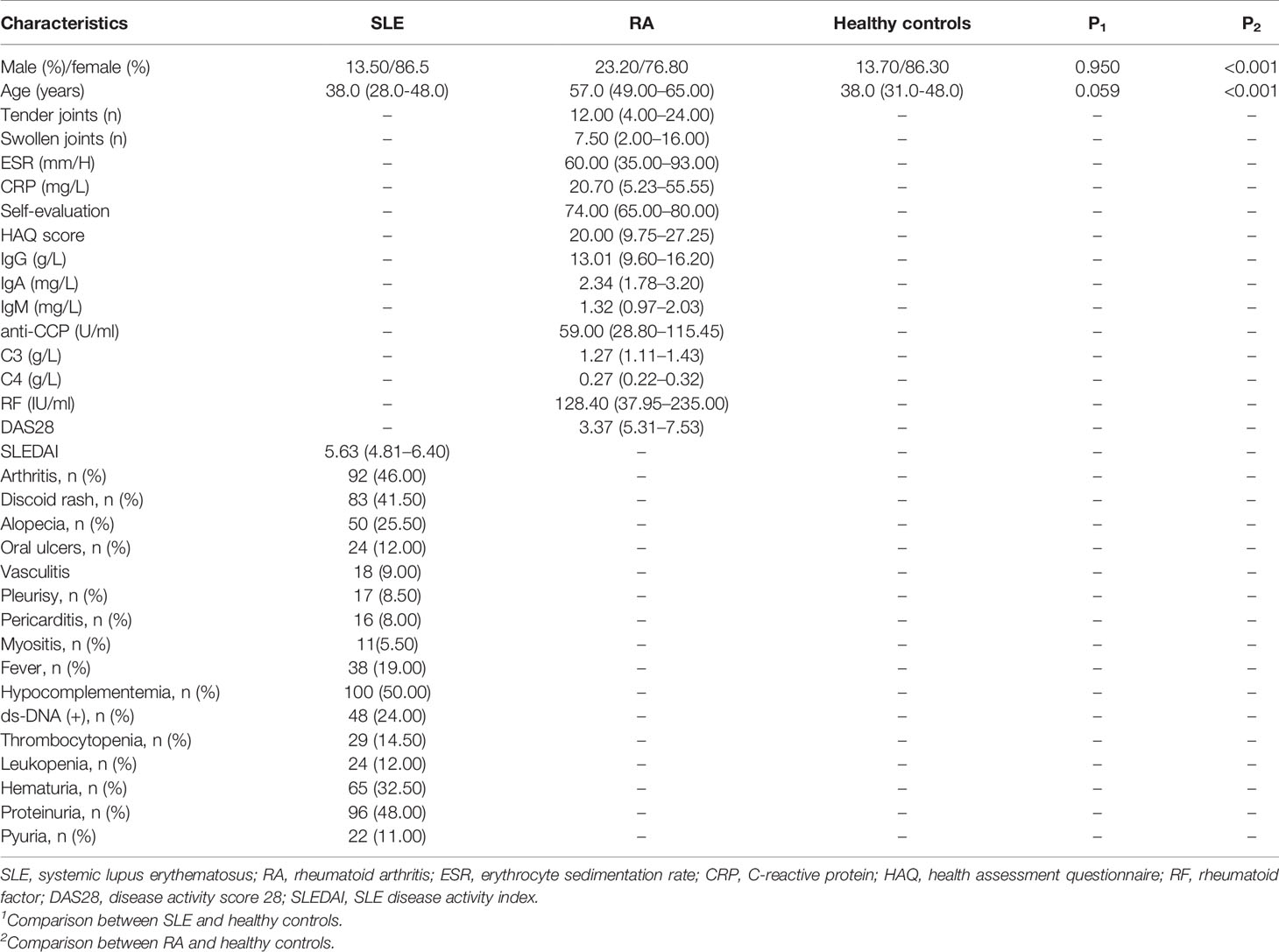
Table 1 Characteristics of patients and controls.
Single Nucleotide Polymorphism Selection
A systemic exploration for previous studies about CD40 gene polymorphism was carried out. According to the online tools: 1000 genomes project (https://www.ncbi.nlm.nih.gov/variation/tools/1000genomes/), all candidate single nucleotide polymorphisms (SNPs) must conform to three standard: pairwise tagging of HapMap population with r2≥0.8; a minor allele frequency (MAF)≥5%; Chinese Han Beijing (CHB) ethnicity. Finally, a total of six SNPs including rs3765456, rs1569723, rs73115010, rs13040307, rs1883832, and rs4810485 were selected.
DNA Extraction and Genotyping
TIANamp Blood DNA kits (Tiangen, Beijing, China) were utilized for extracting genomic DNA. Genotyping of CD40 gene polymorphisms of these samples with qualified DNA concentration and purity was tested by Gene Company using KASP (Gene Company, Shanghai, China). KASP primers were summarized in Supplementary Table 1.
Statistics
Statistical Package for the Social Science (SPSS) version 17.0 (SPSS Inc., Chicago) was used for statistical analysis. Categorical data were presented as frequency, percentage and analyzed by chi-square test. If continuous data was normally distributed, mean ± standard deviation (SD) was displayed, and independent samples t test was adopted. Otherwise, we chose median (interquartile range) and Wilcoxon ranks sum test for comparison. Odds ratio (OR) and 95% confidence interval (CI) were analyzed by logistic regression model. To evaluate deviation of each polymorphism, Hardy-Weinberg equilibrium test was used for SLE patients, RA patients, and healthy controls. There are three inheritance models, including co-dominant model, dominant model, and recessive model. For rs1883832, the co-dominant model includes CC versus TT, CT versus TT, the dominant model is CC+CT versus TT, and the recessive model is CC versus CT+TT. For rs1569723, the co-dominant model includes AA versus CC, AC versus CC, the dominant model is AA+AC versus CC, and the recessive model is AA versus AC+CC. For rs4810485, the co-dominant model includes GG versus TT, GT versus TT, the dominant model is GG+GT versus TT, and the recessive model is GG versus GT+TT. For rs13040307, the co-dominant model includes CC versus TT, CT versus TT, the dominant model is CC+CT versus TT, and the recessive model is CC versus CT+TT. For rs3765456, the co-dominant model includes GG versus AA, GA versus AA, the dominant model is GG+GA versus AA, and the recessive model is GG versus GA+AA. For rs73115010, the co-dominant model includes TT versus CC, TC versus CC, the dominant model is TT+TC versus CC, and the recessive model is TT versus TC+CC. Linkage disequilibrium (LD) and haplotype analysis were calculated by software: HaploView 4.2. A two-sided P value less than 0.05 was recognized as statistical significance.
Results
Characteristics of All Participants
There was no significant difference in gender (P = 0.950) and age (P = 0.059) between SLE patients and healthy controls. Compared RA patients with healthy controls, the age and gender was significantly different (both P<0.05), therefore, when we discussed differences between RA patients and healthy controls for the polymorphism, age and gender were adjusted. Other clinical characteristics were summarized in Table 1. All six polymorphisms were in accordance with Hardy-Weinberg equilibrium (Supplementary Table 2).
Association Between CD40 Gene Polymorphisms and SLE
No differences for alleles and genotypes comparison of six SNPs between SLE patients and healthy controls were identified (Table 2). Subgroup analysis for association of CD40 gene polymorphisms and lupus patients by clinical features and laboratory parameters was carried out. Patients with positive anti-dsDNA had a lower frequency of rs13040307 allele T when compared to those with negative anti-dsDNA (P = 0.038). Patients with hematuria also showed a lower frequency of rs13040307 allele T as compared to that in patients without hematuria (P = 0.045). On the contrary, there was an increased frequency of genotype TT and allele T in lupus patients with myositis when compared to patients without the characteristic (P = 0.020, P = 0.002). A lower frequency of TT genotype and allele T for rs73115010 in lupus patients with myositis was obtained (P = 0.024, P = 0.004). Interestingly, higher frequencies of rs1569723 allele A, rs4810485 allele T and lower frequencies of rs3765456 allele A, rs1883832 allele T were noted in patients with myositis as compared to those in patients without the feature (P = 0.020, P = 0.030, P = 0.021, P = 0.032, respectively) (Table 3 and Supplementary Table 3). SLEDAI was used to analyze disease activity for SLE patients, and association of genotypes for different polymorphisms and SLEDAI was evaluated. We found that none of the genotypes for the six polymorphisms associated with SLEDAI (Supplementary Table 4).
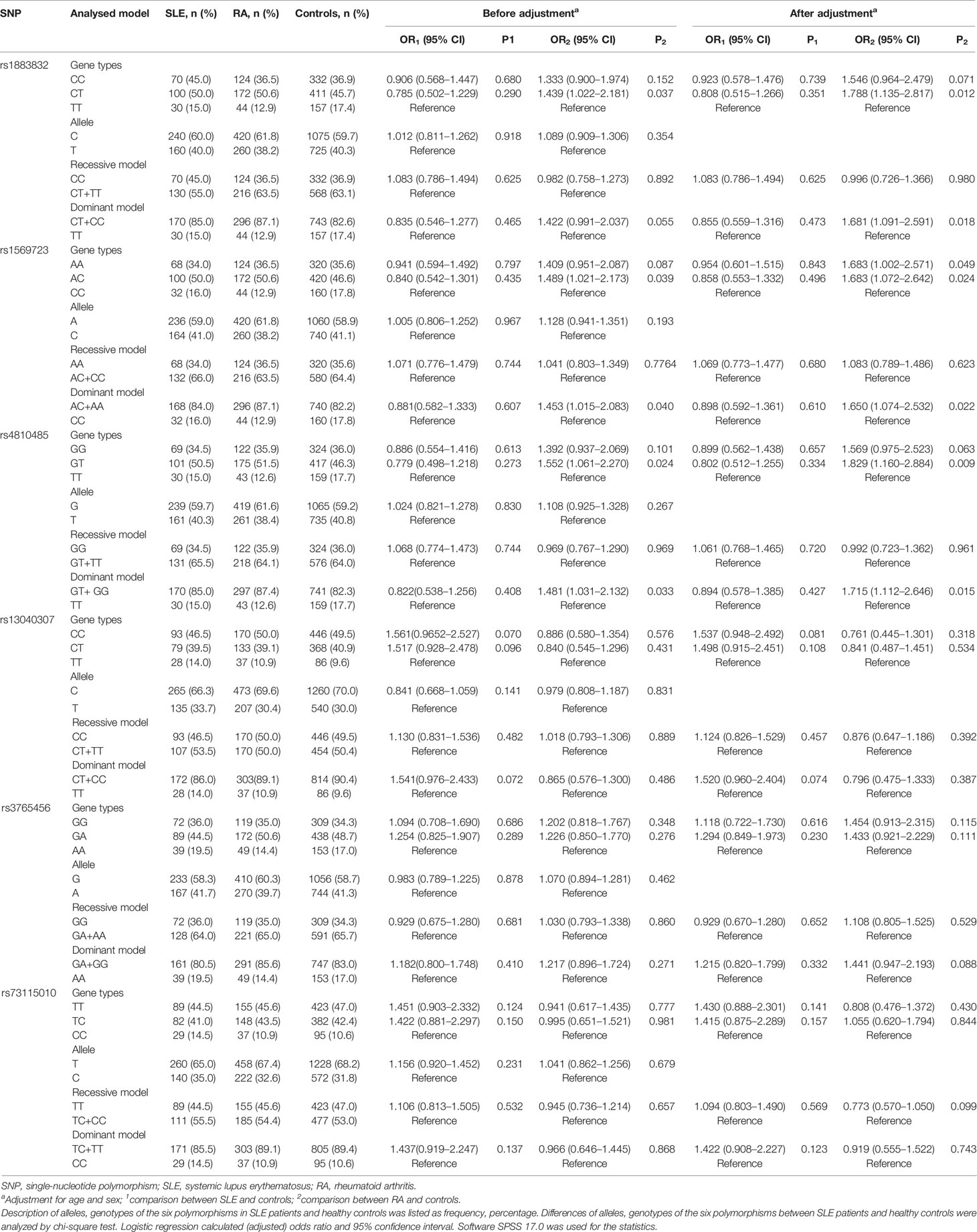
Table 2 Allele and genotype frequencies of six polymorphisms in the CD40 gene in SLE patients, RA patients and healthy controls.
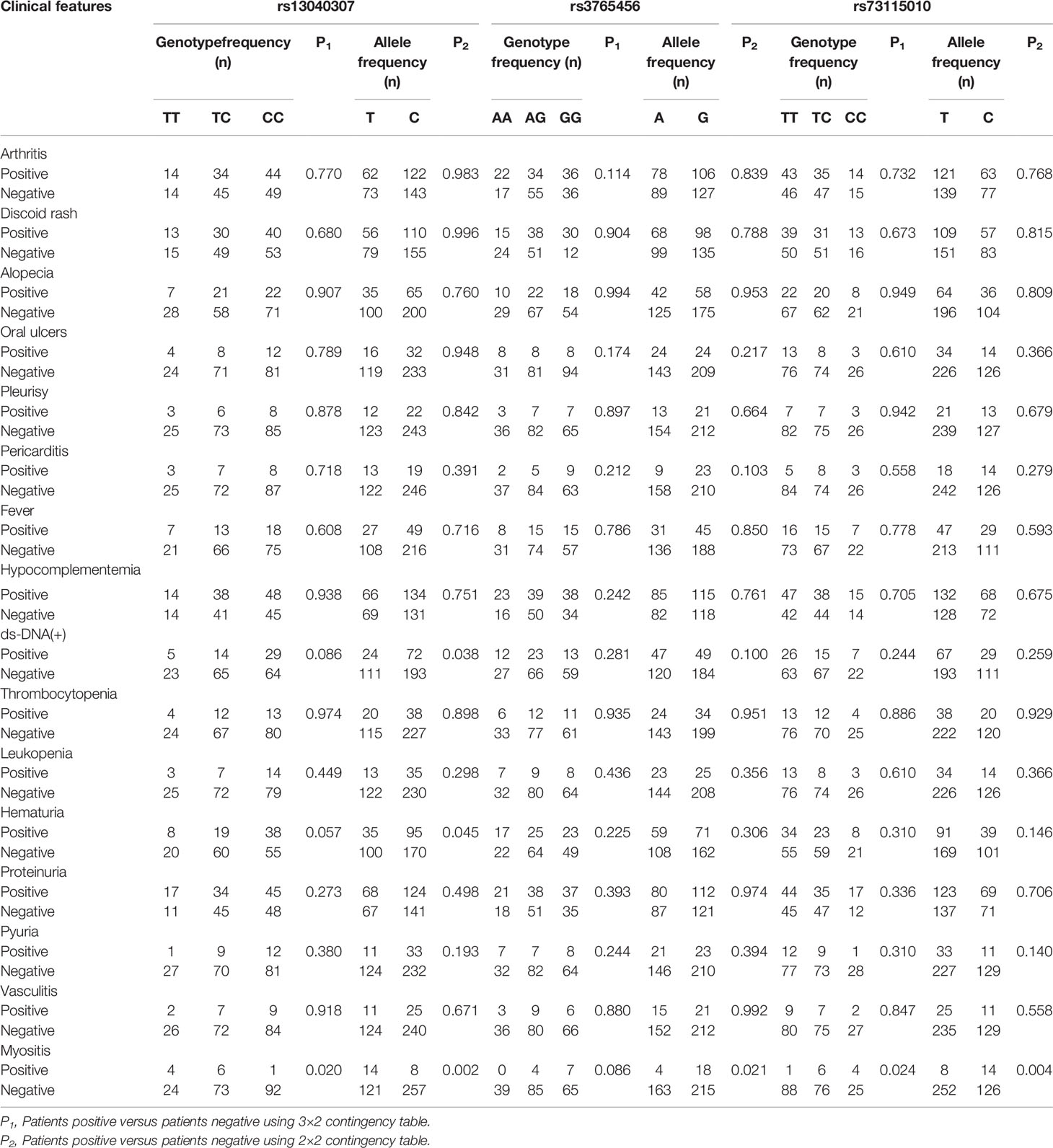
Table 3 Analysis of CD40 gene polymorphisms (rs13040307, rs3765456, rs73115010) in SLE patients by clinical features.
Association Between CD40 Gene Polymorphisms and RA
Differences of alleles and genotypes of CD40 gene polymorphisms between RA patients and healthy controls were shown in Table 2. Frequencies of genotypes AA, AC, and AA+AC of rs1569723 were different between RA patients and healthy controls after age and gender adjustment (AA vs CC, OR, 1.683; 95% CI, 1.002–2.571, P = 0.049; AC vs CC, OR, 1.683; 95% CI, 1.072–2.642, P = 0.024; AA+AC vs CC, OR, 1.650; 95% CI, 1.074–2.534; P = 0.022). Frequencies of genotypes CT, CT+CC of rs1883832 were different between RA patients and healthy controls after age and gender adjustment (CT vs TT; OR, 1.788; 95% CI, 1.135–2.817; P=0.012; CT+CC vs TT: OR, 1.681; 95% CI, 1.091–2.591; P = 0.018). For rs4810485, statistical significance was obtained for comparison of GT with TT, and GT+GG with TT after adjustment by age and gender (GT vs TT: OR, 1.829; 95% CI, 1.160–2.884; P = 0.009; GT+GG vs TT: OR, 1.715; 95% CI, 1.112–2.646; P=0.015). The other three polymorphisms were not related to RA risk.
Association of disease activity in RA patients with CD40 gene polymorphisms was displayed in Table 4. For rs13040307, number of the swollen joints between patients with CC+CT genotype and CC genotype was different (P = 0.010). RA patients carrying rs73115010 TT+TC genotype had higher number of swollen joints as compared to the patients carrying CC genotype (P = 0.038). Other polymorphisms were not related to RA clinical parameters (Supplementary Table 5, Supplementary Table 6).
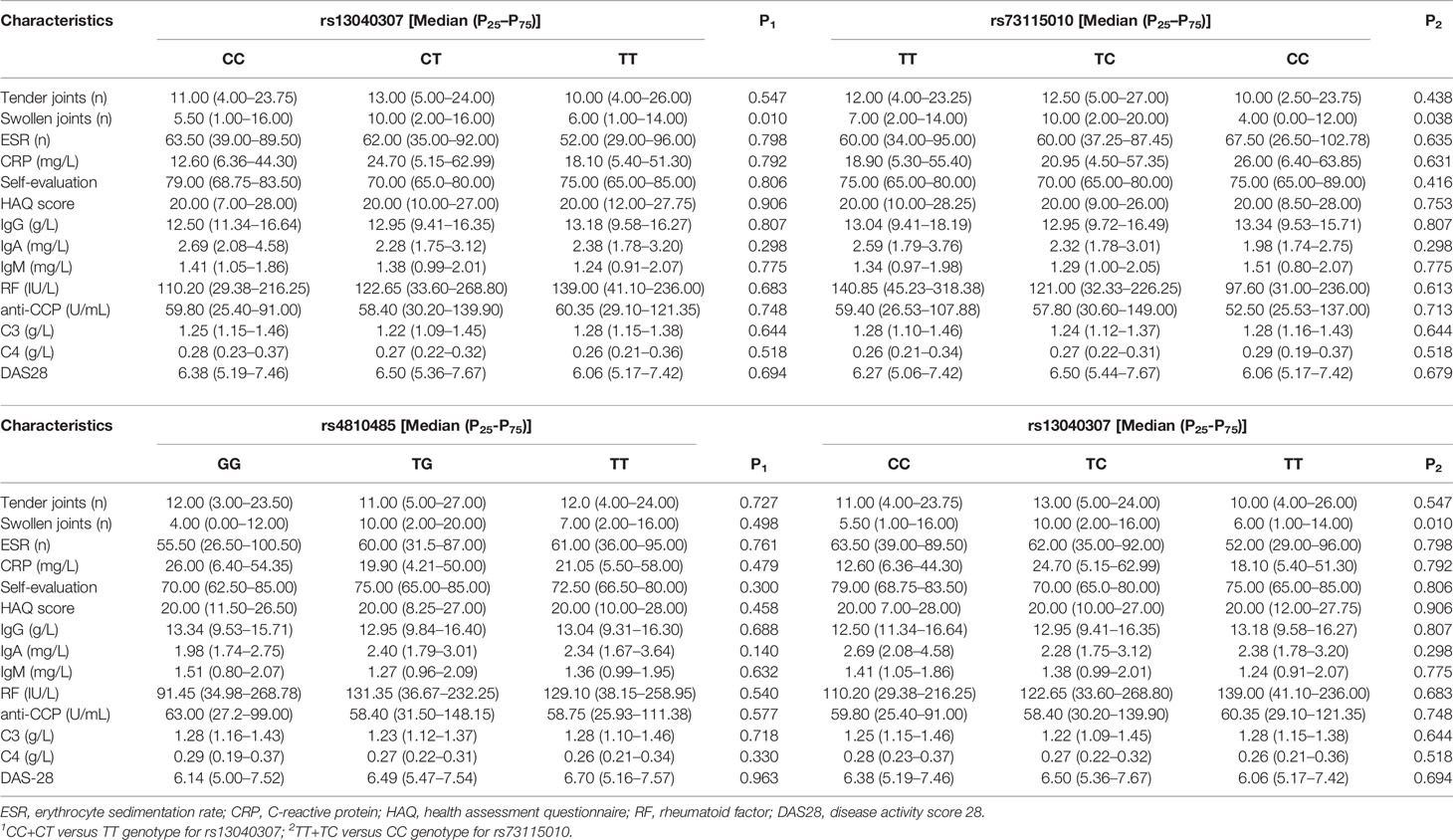
Table 4 Association of disease activity parameters in RA patients with CD40 gene polymorphisms (rs1569723, rs13040307).
CD40 Haplotype Analysis for RA and SLE
Considering linkage disequilibrium of genes, we performed haplotype analysis for CD40 gene polymorphisms. Two blocks were defined by 95% CI (19). The first one consists of four polymorphisms including rs1569723, rs13040307, rs1883832, and rs4810485, and the other one consists of rs3765456 and rs73115010 both for RA and SLE (Figures 1A, B). Results showed that there was no significant difference between patients and controls regarding different haplotypes (Supplementary Table 7).
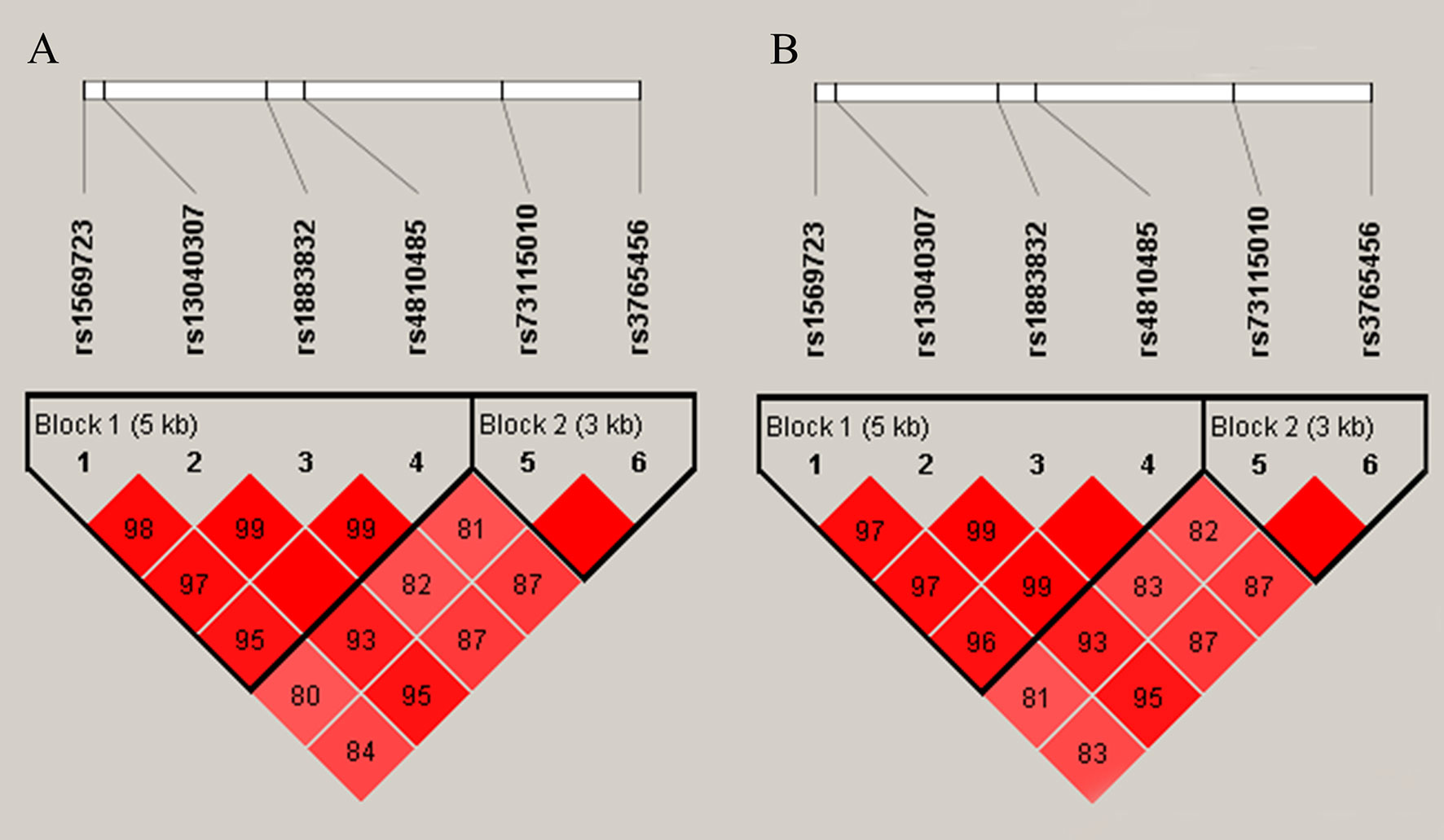
Figure 1 Linkage disequilibrium(LD) of six single nucleotide polymorphisms. The intensity of linkage disequilibrium (LD) is reflected in the color and numeric value (D′) of each box. Bright red means D′ ≥0.95, LOD ≥2. Shade of red means D′<0.95, LOD≥2. (A) LD of RA patients and controls. (B) LD of SLE patients and controls. Both of them show that block 1 consists of four polymorphisms including rs1569723 A/C, rs13040307 T/C, rs1883832 T/C, and rs4810485 T/G, block 2 consists of rs3765456 A/G and rs73115010 T/C.
Discussion
This study explored association of CD40 gene polymorphisms with susceptibility to SLE and RA in a Southern Chinese Han population. A total of six polymorphisms, rs3765456, rs1569723, rs73115010, rs13040307, rs1883832, and rs4810485 were recruited. For RA, the co-dominant model and dominant model of rs1569723, rs1883832, and rs4810485 polymorphisms associated with increased susceptibility to RA. Number of swollen joints were increased in RA patients with genotypes CC+TC of rs13040307 and TT+TC of rs373115010. For SLE, rs13040307 of CD40 gene was related to clinic features, including hematuria and anti-dsDNA. Interestingly, the six polymorphisms may be related to SLE patients with myositis.
SLE and RA are autoimmune disorders with genetic pathogenesis. For rs3765456, this polymorphism may be a risk factor for SLE susceptibility and associated with disease activity in Korea population (12), whereas this polymorphism was not significantly related to SLE in Northern Chinese population (10). In our study, there was no significant difference regarding this polymorphism and SLE risk in Southern Chinese Han population. Interestingly, SLE patients with myositis associated with a lower frequency of rs3765456 allele A, suggesting that rs3765456 allele A may affect the patients complicated with this feature. To date, no study has discussed association of rs3765456 polymorphism with RA risk. In this study, we found that this polymorphism was not related to RA risk. For rs1569723, a previous genome-wide association study reported that there was relation between RA and rs1569732 in European population (20). In our study, we confirmed that this polymorphism related to Chinese RA patients. With respect to relationship between rs1569732 and SLE, a study in Chinese population showed that there was significant difference between rs1569723 and SLE (9). The present study did not find significant association of this polymorphism and SLE risk in our Southern Chinese Han population. However, higher frequency of rs1569723 allele A was related to SLE patients with myositis in this study. Regarding rs13040307 and rs73115010, there were limited studies evaluating association of the two polymorphisms with disease susceptibility, including lupus or arthritis. Wu et al. reported that these two polymorphisms may not associate with SLE in Chinese population by a relatively small sample size (21). By contrast, a study in Korea population indicated that rs73115010 may increase the risk of SLE (12). In this study, there was no significant association of these polymorphisms and SLE, RA risk in our Southern Chinese Han population. Interestingly, rs13040307 polymorphism was related to disease activity parameters of SLE, including anti-dsDNA, hematuria, and myositis. In addition, RA patients carrying genotype CC+CT of rs13040307 and genotype TT+TC of rs73115010 had higher number of swollen joints. However, further studies with larger sample size and different ethnicities are needed to illustrate the relationship of these two polymorphisms (rs13040307 and rs73115010) in SLE and RA.
For another two polymorphisms (rs1883832 and rs4810485), several studies have discussed the association with SLE, RA risk. Rs1883832 was significantly associated with SLE in a Tunisian population (22). However, a study in Egypt population and a study in Korea population did not find significant results (12, 23). For RA, there was no association of rs1883832 in Eastern Chinese and Iran population (24, 25) and the study published by Liu et al. showed that genotype TT versus CC+CT was significant in men (24). On the contrary, rs1883832 was related to RA risk in a Tunisian population (22). According to rs4810485, this polymorphism was confirmed related to SLE and RA risk in European population (11), but not in Korea and Tunisian population (12, 22). In the present study for Southern Chinese Han population, rs1883832 and rs4810485 was related to RA risk, whereas these two polymorphisms were not related to SLE by analyzing genetic models. However, these two polymorphisms were related to SLE patients complicated with myositis. Compared our findings with Liu et al., the differences may correlate with several reasons. First, Liu et al. genotyped the polymorphism by MALDI-TOF MS using the MassARRAY Nanodispenser, and we used KASP method. Second, we have larger sample size not only in RA patients but in healthy controls. Third, the author found a significant result regarding genotype TT versus CC+CT in men, while in our study, we did not find a significant result regarding genotype TT versus CC+CT in men (OR, 1.650; 95% CI, 0.651–4.180;P = 0.288), suggesting that whether this polymorphism may relate to RA risk either in all RA patients or male patients needs to be further discussed with larger sample size especially with larger men patients, the same genotyping method. Collectively, all these differences for SLE, RA risk as compared to our findings may relate to several possibilities. First, RA, SLE are complex diseases, and they have different pathogenesis, therefore, different polymorphisms may have distinct relation to SLE, RA risk, and it is possible that the same polymorphism may have different relation to SLE, RA. Second, different studies selected different methods to detect the polymorphisms may have distinct results. Third, different ethnicities may associate with different results.
Since CD40 gene polymorphisms may correlate with RA, SLE susceptibility, it is convinced that clarification of how polymorphism or what polymorphism of CD40 gene has affected mRNA expression and protein expression, and how does the protein perform in the pathogenesis of these diseases is meaningful and helpful. It is widely accepted that mRNA may be regulated by SNPs (26). Therefore, dysregulated expression of CD40 may be caused by upregulation of transcription and translation owing to mutated polymorphism. Studies showed that genotype TT, TC of rs1883832 associated with increased CD40 expression in Chinese and Egypt SLE patients (9, 23). Genotype GG of rs4810485 was related to increased CD40 expression in Greek and Turkish SLE patients (27, 28). CD40 is expressed on smooth muscle fibroblasts and synovial cells, which can be upregulated by pro-inflammatory cytokines, such as IFN-γ and TNFα. In turn, elevated expression of CD40 may further involve in the inflammatory response, leading to fibroblast proliferation, adhesion molecule upregulation, and generation of pro-inflammatory cytokines and chemokines, and finally causing diseases development and progression (7, 29). To date, several studies have showed that expression of CD40 was elevated in SLE, RA patients and associated with diseases activity (30–32). Therefore, mutation in CD40 gene may have affected CD40 expression, and promoted SLE, RA development. In our study, we did not discuss association of these polymorphism and CD40 expression in RA patients or SLE patients. Functional study in the future is necessary to elucidate how polymorphism regulates CD40 expression, especially the role in RA, SLE pathogenesis.
There are some limitations in the present study. First, selection bias cannot be avoided because patients were selected from a hospital. Second, this study focuses on association of SNPs with susceptibility to SLE, RA, however, exploring the process of transcription and translation of CD40 gene by the polymorphisms is of importance. Third, more SNPs of CD40 gene are needed to discuss association with SLE, RA risk, and discussion of gene-environment interaction should be investigated in the future. Fourth, we found association of myositis with the six polymorphisms, however, the conclusion is to take with caution because of the very low number of patients. Finally, replication of the results on other ethnics is lacking.
In conclusion, our study showed that CD40 gene polymorphisms may relate to SLE and RA susceptibility.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethic Research Committee of Southwest Medical University. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
QH, W-DX, L-CS, X-YL, and A-FH designed and wrote this paper. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by grants from the National Natural Science Foundation of China (81701606) and the Sichuan Provincial Science and Technology Program (2019YJ0540).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2021.642929/full#supplementary-material
References
1. Smolen JS, Aletaha D, McInnes IB. Rheumatoid arthritis [published correction appears in Lancet (2016) Oct 22;388(10055):1984]. Lancet (2016) 388(10055):2023–38. doi: 10.1016/S0140-6736(16)30173-8
2. Durcan L, O’Dwyer T, Petri M. Management strategies and future directions for systemic lupus erythematosus in adults. Lancet (2019) 393(10188):2332–43. doi: 10.1016/S0140-6736(19)30237-5
3. Aleman-Avila I, Jimenez-Morales M, Beltran-Ramirez O, Barbosa-Cobos RE, Jimenez-Morales S, Sanchez-Munoz F, et al. Functional polymorphisms in pre-miR146a and pre-miR499 are associated with systemic lupus erythematosus but not with rheumatoid arthritis or Graves’ disease in Mexican patients. Oncotarget (2017) 8(54):91876–86. doi: 10.18632/oncotarget.19621
4. Zhao YL, Zhang TP, Wu J, Li BZ, Li XM, Pan HF, et al. Association of adiponectin and adiponectin receptor gene polymorphisms with rheumatoid arthritis in a Chinese population. Postgrad Med J (2020) 96(1133):149–55. doi: 10.1136/postgradmedj-2018-136372
5. Oparina N, Martinez-Bueno M, Alarcon-Riquelme ME. An update on the genetics of systemic lupus erythematosus. Curr Opin Rheumatol (2019) 31(6):659–68. doi: 10.1097/BOR.0000000000000654
6. Amariuta T, Luo Y, Knevel R, Okada Y, Raychaudhuri S. Advances in genetics toward identifying pathogenic cell states of rheumatoid arthritis. Immunol Rev (2020) 294(1):188–204. doi: 10.1111/imr.12827
7. Karnell JL, Rieder SA, Ettinger R, Kolbeck R. Targeting the CD40-CD40L pathway in autoimmune diseases: Humoral immunity and beyond. Adv Drug Deliv Rev (2019) 141:92–103. doi: 10.1016/j.addr.2018.12.005
8. Nathan MJ, Mold JE, Wood SC, Csencsits K, Lu G, Eichwald EJ, et al. Requirement for donor and recipient CD40 expression in cardiac allograft rejection: induction of Th1 responses and influence of donor-derived dendritic cells. J Immunol (2004) 172:6626–33. doi: 10.4049/jimmunol.172.11.6626
9. Chen JM, Guo J, Wei CD, Wang CF, Luo HC, Wei YS, et al. The association of CD40 polymorphisms with CD40 serum levels and risk of systemic lupus erythematosus. BMC Genet (2015) 16:121. doi: 10.1186/s12863-015-0279-8
10. Nie D, Li H, Yan G, Wang Z, He Z, Zhou W. Gene-gene interaction between CD40 and CD226 gene on systemic lupus erythematosus in the Chinese Han population. Rheumatol Int (2016) 36(12):1657–62. doi: 10.1007/s00296-016-3570-8
11. Lee YH, Bae SC, Choi SJ, Ji JD, Song GG. Associations between the functional CD40 rs4810485 G/T polymorphism and susceptibility to rheumatoid arthritis and systemic lupus erythematosus: a meta-analysis. Lupus (2015) 24(11):1177–83. doi: 10.1177/0961203315583543
12. Joo YB, Park BL, Shin HD, Park SY, Kim I, Bae SC. Association of genetic polymorphisms in CD40 with susceptibility to SLE in the Korean population. Rheumatol (Oxford) (2013) 52(4):623–30. doi: 10.1093/rheumatology/kes339
13. Raychaudhuri S, Remmers EF, Lee AT, Hackett R, Guiducci C, Burtt NP, et al. Common variants at CD40 and other loci confer risk of rheumatoid arthritis. Nat Genet (2008) 40(10):1216–23. doi: 10.1038/ng.233
14. Hochberg MC. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthrit Rheum (1997) 40(9):1725. doi: 10.1002/art.1780400928
15. Neogi T, Aletaha D, Silman AJ, Naden RL, Felson DT, Aggarwal R, et al. The 2010 American College of Rheumatology/European League Against Rheumatism classification criteria for rheumatoid arthritis: Phase 2 methodological report. Arthritis Rheum (2010) 62(9):2582–91. doi: 10.1002/art.27580
16. Prevoo ML, van ‘t Hof MA, Kuper HH, van Leeuwen MA, van de Putte LB, van Riel PL. Modified disease activity scores that include twenty-eight-joint counts. Development and validation in a prospective longitudinal study of patients with rheumatoid arthritis. Arthritis Rheumatol (1995) 38(1):44–8. doi: 10.1002/art.1780380107
17. Bombardier C, Gladman DD, Urowitz MB, Caron D, Chang CH. Derivation of the SLEDAI. A disease activity index for lupus patients. The Committee on Prognosis Studies in SLE. Arthritis Rheumatol (1992) 35(6):630–40. doi: 10.1002/art.1780350606
18. Hoogendijk JE, Amato AA, Lecky BR, Choy EH, Lundberg IE, Rose MR, et al. 119th ENMC international workshop: trial design in adult idiopathic inflammatory myopathies, with the exception of inclusion body myositis, 10-12 October 2003, Naarden, The Netherlands. Neuromuscul Disord (2004) 14(5):337–45. doi: 10.1016/j.nmd.2004.02.006
19. Gabriel SB, Schaffner SF, Nguyen H, Moore JM, Roy J, Blumenstiel B, et al. The structure of haplotype blocks in the human genome. Science (2002) 296(5576):2225–9. doi: 10.1126/science.1069424
20. Australia and New Zealand Multiple Sclerosis Genetics Consortium (ANZgene). Genome-wide association study identifies new multiple sclerosis susceptibility loci on chromosomes 12 and 20. Nat Genet (2009) 41(7):824–8. doi: 10.1038/ng.396
21. Wu CJ, Guo J, Luo HC, Wei CD, Wang CF, Lan Y, et al. Association of CD40 polymorphisms and haplotype with risk of systemic lupus erythematosus. Rheumatol Int (2016) 36(1):45–52. doi: 10.1007/s00296-015-3345-7
22. Soussi M, Kallel A, Ben Wafi S, Ben Halima M, Sanhaji H, Mourali MS, et al. Associations of rs1883832 and rs4810485 polymorphisms of CD40 gene with myocardial infarction in the Tunisian population. Biomarkers (2019) 24(6):530–7. doi: 10.1080/1354750X.2019.1602168
23. Mousa TG, Omar HH, Emad R, Salama MI, Omar W, Fawzy M, et al. The association of CD40 polymorphism (rs1883832C/T) and soluble CD40 with the risk of systemic lupus erythematosus among Egyptian patients. Clin Rheumatol (2019) 38(3):777–84. doi: 10.1007/s10067-018-4349-y
24. Liu R, Xu N, Wang X, Shen L, Zhao G, Zhang H, et al. Influence of MIF, CD40, and CD226 polymorphisms on risk of rheumatoid arthritis. Mol Biol Rep (2012) 39(6):6915–22. doi: 10.1007/s11033-012-1518-y
25. Hosseini N, Tahoori MT, Mohammadzadeh A, Zarei Jaliani H, Bitaraf Sani M, Soleimani Salehabadi H. IRAK1 Gene Polymorphism in Rheumatoid Arthritis. Immunol Invest (2021) 50(2–3):304–21. doi: 10.1080/08820139.2020.1764028
26. Lu YF, Mauger DM, Goldstein DB, Urban TJ, Weeks KM, Bradrick SS. IFNL3 mRNA structure is remodeled by a functional non-coding polymorphism associated with hepatitis C virus clearance. Sci Rep (2015) 5:16037. doi: 10.1038/srep16037
27. Vazgiourakis VM, Zervou MI, Choulaki C, Bertsias G, Melissourgaki M, Yilmaz N, et al. A common SNP in the CD40 region is associated with systemic lupus erythematosus and correlates with altered CD40 expression: implications for the pathogenesis. Ann Rheum Dis (2011) 70:2184–90. doi: 10.1136/ard.2010.146530
28. Tapia-Llanos R, Muñoz-Valle JF, Román-Fernández IV, Marín-Rosales M, Salazar-Camarena DC, Cruz A, et al. Association of soluble CD40 levels with -1 C > T CD40 polymorphism and chronic kidney disease in systemic lupus erythematosus. Mol Genet Genomic Med (2019) 7(12):e1014. doi: 10.1002/mgg3.1014
29. Peters AL, Stunz LL, Bishop GA. CD40 and autoimmunity: the dark side of a great activator. Semin Immunol (2009) 21(5):293–300. doi: 10.1016/j.smim.2009.05.012
30. Perper SJ, Westmoreland SV, Karman J, Twomey R, Seagal J, Wang R, et al. Treatment with a CD40 Antagonist Antibody Reverses Severe Proteinuria and Loss of Saliva Production and Restores Glomerular Morphology in Murine Systemic Lupus Erythematosus. J Immunol (2019) 203(1):58–75. doi: 10.4049/jimmunol.1900043
31. Chamberlain C, Colman PJ, Ranger AM, Burkly LC, Johnston GI, Otoul C, et al. Repeated administration of dapirolizumab pegol in a randomised phase I study is well tolerated and accompanied by improvements in several composite measures of systemic lupus erythematosus disease activity and changes in whole blood transcriptomic profiles. Ann Rheum Dis (2017) 76(11):1837–44. doi: 10.1136/annrheumdis-2017-211388
Keywords: CD40, polymorphism, systemic lupus erythematosus, rheumatoid arthritis, susceptibility, clinical features, disease activity parameters
Citation: Huang Q, Xu W-D, Su L-C, Liu X-Y and Huang A-F (2021) Association of CD40 Gene Polymorphisms With Systemic Lupus Erythematosus and Rheumatoid Arthritis in a Chinese Han Population. Front. Immunol. 12:642929. doi: 10.3389/fimmu.2021.642929
Received: 17 December 2020; Accepted: 22 March 2021;
Published: 22 April 2021.
Edited by:
Philippe Saas, INSERM U1098 Interactions Hôte-Greffon-Tumeur & Ingénierie Cellulaire et Génique, FranceReviewed by:
Frank Verhoeven, Centre Hospitalier Universitaire de Besançon, FranceMatheus Braga, State University of Maringá, Brazil
Copyright © 2021 Huang, Xu, Su, Liu and Huang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wang-Dong Xu, bG91dGNoMTIzQDE2My5jb20=; An-Fang Huang, bG91dGNoMjExQDE2My5jb20=