
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol., 18 February 2021
Sec. Cytokines and Soluble Mediators in Immunity
Volume 12 - 2021 | https://doi.org/10.3389/fimmu.2021.613422
 André Santa Cruz1,2,3*†
André Santa Cruz1,2,3*† Ana Mendes-Frias1,2†
Ana Mendes-Frias1,2† Ana Isabel Oliveira3
Ana Isabel Oliveira3 Luís Dias1,2,3
Luís Dias1,2,3 Ana Rita Matos3
Ana Rita Matos3 Alexandre Carvalho1,2,3
Alexandre Carvalho1,2,3 Carlos Capela1,2,3Jorge Pedrosa1,2
Carlos Capela1,2,3Jorge Pedrosa1,2 António Gil Castro1,2
António Gil Castro1,2 Ricardo Silvestre1,2*
Ricardo Silvestre1,2*Hyper-inflammatory responses induced by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) are a major cause of disease severity and death. Predictive prognosis biomarkers to guide therapeutics are critically lacking. Several studies have indicated a “cytokine storm” with the release of interleukin-1 (IL-1), IL-6, and IL-8, along with tumor necrosis factor alpha (TNFα) and other inflammatory mediators. Here, we proposed to assess the relationship between IL-6 and outcomes of patients with coronavirus disease 2019 (COVID-19). Our cohort consisted of 46 adult patients with PCR-proven SARS-CoV-2 infection admitted in a COVID-19 ward of the Hospital de Braga (HB) from April 7 to May 7, 2020, whose IL-6 levels were followed over time. We found that IL-6 levels were significantly different between the disease stages. Also, we found a significant negative correlation between IL-6 levels during stages IIb and III, peripheral oxygen saturation (SpO2), and partial pressure of oxygen in arterial blood (PaO2), showing that IL-6 correlates with respiratory failure. Compared to the inflammatory markers available in the clinic routine, we found a positive correlation between IL-6 and C-reactive protein (CRP). However, when we assessed the predictive value of these two markers, IL-6 behaves as a better predictor of disease progression. In a binary logistic regression, IL-6 level was the most significant predictor of the non-survivors group, when compared to age and CRP. Herein, we present IL-6 as a relevant tool for prognostic evaluation, mainly as a predictor of outcome.
Coronaviruses are a family of single strain RNA viruses that infect several hosts, including humans, mainly causing respiratory infections (1). Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), a novel betacoronavirus, emerged at the end of 2019 in China and has already infected almost 90 million people worldwide, causing more than 1.9 million deaths and becoming a worldwide pandemic (coronavirus disease 2019, COVID-19) (2, 3). Although most cases present only mild symptoms, 20% of the patients develop severe pathology with acute bilateral pneumonia that may evolve to acute respiratory distress syndrome and multi-organ failure. The risk of severe disease and death increases with age and the presence of comorbidities (4).
Infection with SARS-CoV-2 comprehends two overlapping phases: the first, characterized by a high replicative activity of the virus, is then followed by a counteractive host immune response (5). This infection has been divided into three clinical stages, regarding the severity and prognosis (6, 7). Stage I is defined by mild unspecified symptoms, such as myalgia, dry cough, headache, and subfebrile temperature, without any laboratory and radiological abnormalities. Stage II is characterized by cough, high fever, dyspnea, abnormal thoracic imaging, lymphopenia, and increased levels of inflammatory markers. It is further divided into two groups, according to the presence (IIb) or absence (IIa) of hypoxemia. Finally, stage III displays clinical manifestations of a severe systemic inflammatory syndrome, culminating in severe respiratory failure with an unfavorable prognosis. During this last stage of the disease, values of several inflammatory markers are extremely high and macrophage activation syndrome may occur.
Several treatments for COVID-19 have been tested, which can be divided into three main categories: drugs with direct antiviral effect, drugs with immunomodulatory effect, and neutralizing antibodies from convalescent plasma (8). So far, among the first group, remdesivir has been considered the most prominent drug due to the evidence of faster clinical improvement and mortality reduction in the subset of hospitalized patients receiving oxygen (9, 10). However, these data are conflicting with other studies, and doubts remain about treatment efficacy and profile of patients that may benefit the most from this therapeutic (11, 12).
Considering the challenge of controlling virus transmission, and the lack of an unquestionably effective antiviral treatment, a therapeutic strategy of immunomodulation has been advocated (13). This strategy is particularly relevant given the excessive production of proinflammatory cytokines recognized as crucial in the pathophysiologic process of severe COVID-19 (14). In these cases, the loss of negative feedback in the immune response causes excessive production of inflammatory cytokines, leading to deleterious effects and poor prognosis (15). A large group of cytokines has been recognized as significantly increased in severe COVID-19 patients: interleukin-1β (IL-1β), IL-1RA, IL-2, IL-6, IL-7, IL-8 (CXCL8), IL-9, IL-10, IL-17, IL-18, tumor necrosis factor (TNF-α), interferon-gamma (IFN-gamma), granulocyte colony-stimulating factor (G-CSF), granulocyte-macrophage colony-stimulating factor (GM-CSF), macrophage inflammatory protein 1 (MIP-1alpha/CCL3), monocyte chemoattractant protein-1 (MCP-1/CCL2), interferon gamma-induced protein 10 (IP-10/CXCL10), and fibroblast growth factor (FGF) (16–18). Most importantly, some of them (IL-6, IL-8, and TNF-α) are regarded as independent markers of the severe disease (19). A deeper knowledge of the SARS-CoV-2-induced cytokine storm, including its triggering mechanisms, molecular components, and kinetics, is necessary for a better understanding of the pathological process in COVID-19 and therefore for the identification of the most adequate therapeutic targets and timing of drugs administration. So far, several studies have been published on the potential effects of specific (anti-IL-6, anti-IL-1, anti-GM-CSF, and anti-TNF-α) and non-specific therapies (corticosteroids) (13, 20). Among the immunomodulatory therapies for COVID-19, corticosteroids have been the most widely used, particularly dexamethasone, after growing evidence of their benefit in reducing mortality in hospitalized patients receiving oxygen and especially in patients supported with mechanical ventilation (20, 21). Nevertheless, the most adequate dosage for each patient, precise timing of administration, and duration of treatment remain to be elucidated. Also, a more selective drug would be desirable, especially considering the already existing immune dysfunction.
Of all the upregulated cytokines that may represent selective therapeutic targets, IL-6 has been regarded as particularly important in the COVID-19 pathogenesis and may be antagonized by existing drugs. IL-6 is an inflammatory interleukin mainly produced by macrophages and T lymphocytes in response to pathogens and is pivotal to controlling several viral infections (22–24). While homeostatic values of IL-6 contribute to the resolution of infections and tissue lesions, its exacerbated production contributes decisively to cytokine storms (22–24). In COVID-19, IL-6 has been positively correlated with disease stages and radiologic changes (17, 25–27). Furthermore, the potential prognostic value of IL-6 has been explored regarding the need for mechanical ventilation, mortality, or both, when considered alone or in combination with other variables (28–32). Yet, most studies quantify IL-6 only at patient admission, a strategy that may not be appropriate to accurately predict the outcome or to guide treatment due to the dynamic inflammatory process occurring during infection with SARS-CoV-2. Of all the available drugs that specifically inhibit IL-6 pathway, only tocilizumab (an IL-6 receptor antagonist) has, so far, a reasonable body of evidence in COVID-19. A recently published meta-analysis on the efficacy of tocilizumab in those patients found that cumulative evidence from randomized controlled trials (RCTs) suggests a risk reduction of mechanical ventilation but no effect on mortality, while cumulative evidence from cohort studies suggests an association between tocilizumab and lower mortality (33). However, only 3 of the 19 cohort studies and none of the 5 selected RCTs, used elevated IL-6 level as an inclusion criterion. This fact suggests that tocilizumab and other IL-6R antagonists may be further exploited.
In our work, we performed a characterization of the serum IL-6 levels throughout the entire infectious process with SARS-CoV-2. The IL-6 levels increase according to the disease stage and correlate with respiratory failure. After a kinetic analysis, we showed that the levels of IL-6 may be just temporarily raised, which may have major therapeutic implications. Moreover, the kinetic quantification of IL-6 levels allowed early discrimination between survivors and non-survivors. Overall, we suggest that a kinetic IL-6 quantification is crucial to predict the outcome of patients infected with SARS-CoV-2 and may be very useful to guide treatment.
This is a single-center prospective cohort study, performed at Hospital de Braga (HB), a tertiary Portuguese Hospital. All adult patients with PCR-proven SARS-CoV-2 infection admitted in a COVID-19 ward from 7th April to 7th May 2020 were treated and monitored according to the HB protocol, which was approved by the Clinical Board and Ethics Committee (reference 69_2020). Among other recommendations, this protocol provides guidance on laboratory tests and includes the monitoring of IL-6 serum levels to all patients. Thirty out of the 46 enrolled patients were subjected to a kinetic serum IL-6 quantification at admission and on each 72 h, throughout hospitalization. This study ended when the last patient of this group was discharged. Patients that did not completely follow the protocol, who had evidence of any simultaneous bacterial infection, or patients treated with tocilizumab were excluded from this study.
Whole blood was collected in tubes containing separation gel (VACUETTE) and transported to the Life and Health Sciences Research Institute (ICVS) laboratories to further analysis. After centrifugation, the serum was collected and stored at −80°C. IL-6 was quantified using an ELISA kit (reference 430504, BioLegend, CA, USA), according to the manufacturer's instructions. All other laboratory tests, included in the established protocol, were performed in the HB laboratories, following the standard procedures.
For each patient, data were collected from the medical records and inserted into our study database. Variables comprised of demographics, major comorbidities, disease symptoms, dates of onset, diagnosis, hospital admission, discharge, or death. At baseline and during hospitalization, daily information on the disease stage, existence of fever, peripheral oxygen saturation (SpO2), partial pressure of oxygen in arterial blood (PaO2), radiologic severity index, need for invasive or non-invasive ventilatory support, treatment used, diagnosis of a pulmonary embolism if present, C-reactive protein (CRP) quantification, and clinical impression of patients' evolution were collected.
Statistical analyses were performed using GraphPad Prism version 6 software. Regarding the small sample size and the non-normality observed in our variables, the Kruskal–Wallis test was used to identify statistical differences. For variables that reached global significance, pairwise comparisons were performed by the Mann–Whitney U-test. Correlations were calculated using Spearman's correlation: Spearman coefficient and p-value were reported. For categorical variables, the chi-square test was performed to assess the dependence between variables: Cramer's V and p-value were reported for each comparison. Binary logistic and linear regressions were performed using IBM SPSS statistics 26. Statistically significant values are as follows: *p < 0.05; **p < 0.01; ***p < 0.001.
Of the 63 patients admitted in the COVID-19 ward during the period of the study, 17 were excluded: 10 due to evidence of simultaneous bacterial infection, 5 due to treatment with tocilizumab, and 2 due to insufficient compliance with the protocol. Our final cohort included the remaining 46 patients whose demographic and clinical characteristics are detailed in Table 1. Most patients were hospitalized between the 4th and 10th day of symptoms, with cough being the most prevalent complaint. Two-thirds of the patients were admitted due to bilateral pneumonia with hypoxemia (stage IIb or III). At admission, 41 patients (89%) reported symptoms related to COVID-19. Half of the patients who were admitted in stage IIb eventually progressed to stage III, with most of them requiring ventilatory support. Out of all the patients, five deaths were observed. All the other patients were discharged or transferred to the general ward after meeting cure criteria (complete resolution of the symptomatology and two negative PCR-SARS-CoV-2 results within 24–48 h).
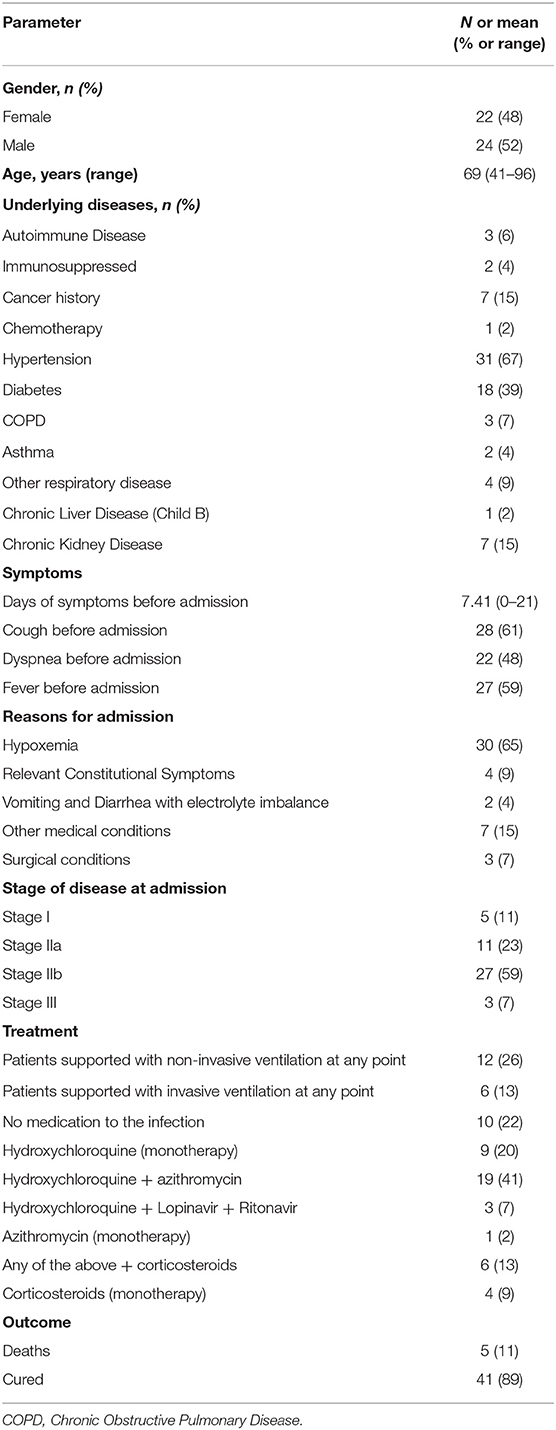
Table 1. Demographic and clinical characterization of the cohort.
Serum samples from subjects enrolled in our study were used for IL-6 quantification. After dividing IL-6 values according to disease stages (I, IIa, IIb, and III), statistical differences were found, with (p < 0.0001) IL-6 levels increasing along with the disease stage (Figure 1A). IL-6 values from patients in stage I are significantly lower than the values observed in the other stages (p = 0.0234, p = 0.0002, and p < 0.0001, compared to stages IIa, IIb, and III, respectively). The levels of CRP throughout the disease stages were also evaluated (Figure 1A). CRP shows a different pattern, as CRP levels were found significantly increased in stage III when compared to the other stages (p = 0.0002, p = 0.0015, and p = 0.0142 to I, IIa, and IIb, respectively). To evaluate the relationship between these two parameters, a Spearman's correlation was performed, and a positive correlation was found between IL-6 and CRP (r = 0.550, p < 0.0001; Figure 1B). Regarding the overall correlation of IL-6 levels with the increased severity of the disease, we hypothesized that IL-6 values could predict the disease progression of patients in the crucial IIb stage. In fact, we found that IL-6 levels were significantly higher in patients in stage IIb who will evolve to stage III, as compared to patients in stage IIb who will recover from their respiratory failure and enter stage IIa (p = 0.0022). These differences were also observed with CRP values (p = 0.0343; Figure 1C). These results were also corroborated by a receiver operating characteristic (ROC) curve, more robust for IL-6 when compared to CRP [area under the curve (AUC) = 0.82 ± 0.08 and Youden's index = 0.63 for IL-6 and AUC = 0.74 ± 0.09 and Youden's index = 0.42 for CRP; Figure 1D]. Of note, a linear regression was performed to assess the influence of any comorbidity in IL-6 levels, ruling out that hypothesis.
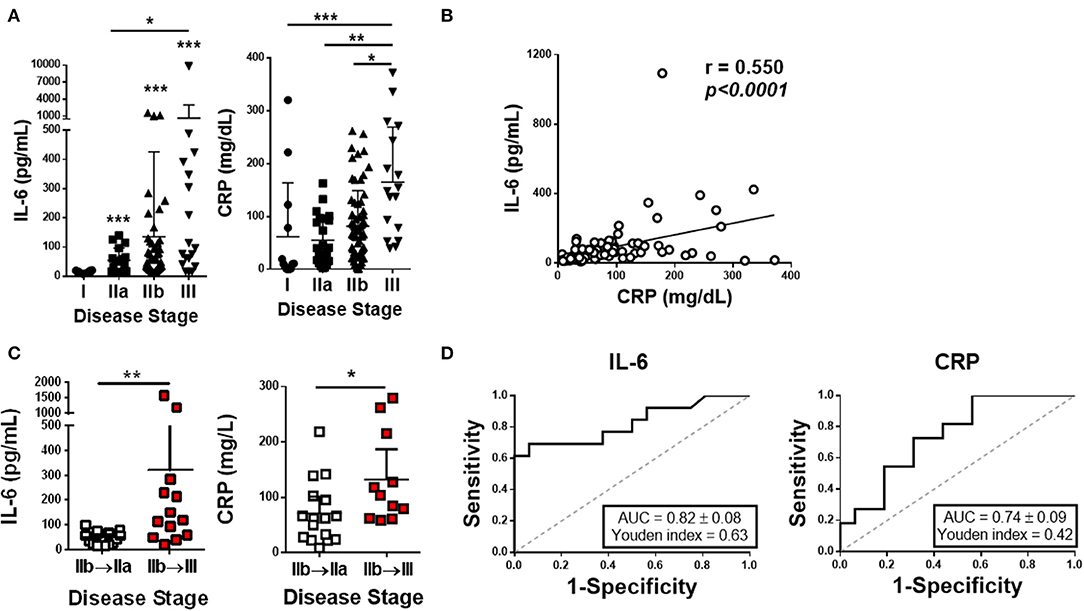
Figure 1. Plasma IL-6 and CRP profile in COVID-19 patients. (A) The levels of IL-6 and CRP were quantified on the plasma of COVID-19 patients segregated by disease stages. (B) Correlation between the plasma IL-6 and CRP levels in all patients. (C) IL-6 and CRP plasma concentration in patients at stage IIb that move to stage IIa or III. (D) ROC curves of IL-6 and CRP. In (A,B), we have included multiple data from each patient (n = 46). Data are shown as mean ± SD *p < 0.05, **p < 0.01, ***p < 0.001.
In stages characterized by hypoxemia (IIb and III), IL-6 levels did correlate with patient's respiratory failure severity, as we observed a significant negative correlation with SpO2 (r = −0.324, p = 0.0075) and a significant negative correlation with PaO2 (r = −0.335, p = 0.0026) (Figures 2A,B).
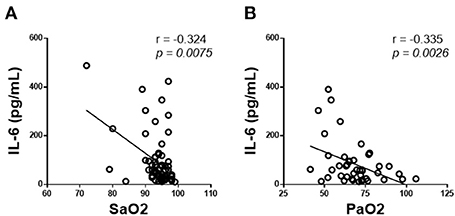
Figure 2. IL-6 correlation with respiratory parameters in COVID-19 patients. Correlation of plasma IL-6 levels with (A) oxygen saturation (SpO2) and (B) oxygen partial pressure (PaO2). We have included multiple data from each patient (n = 46).
We depicted the IL-6 kinetics throughout the infection based on the onset of symptoms and the admission day. Patients were then grouped according to the shape of their IL-6 curve, as represented in Figure 3A. Matching profile and outcome, all patients in profile 1 (red line) died in the first week of hospitalization (non-survivors). All patients in the other profiles survived. In survivors' group 1 (black line), a peak of IL-6 is observed around day 10 after the onset of symptoms, but after admission, IL-6 levels decreased gradually as patients recovered. In survivors' group 2 (blue line), a peak of IL-6 is observed approximately at day 7 after the onset of symptoms and is also detected around day 4 of hospitalization, followed by decreasing values of IL-6 as patients recovered. It shall be noted, however, that patients in the survivors' group 1 were admitted 3 days later (median difference) than patients in the survivors' group 2, counting from disease onset. In both groups, all individuals displayed a peak of IL-6, which was limited in time. Importantly, after the 10th day of hospitalization, all these patients showed an IL-6 value close to normal.
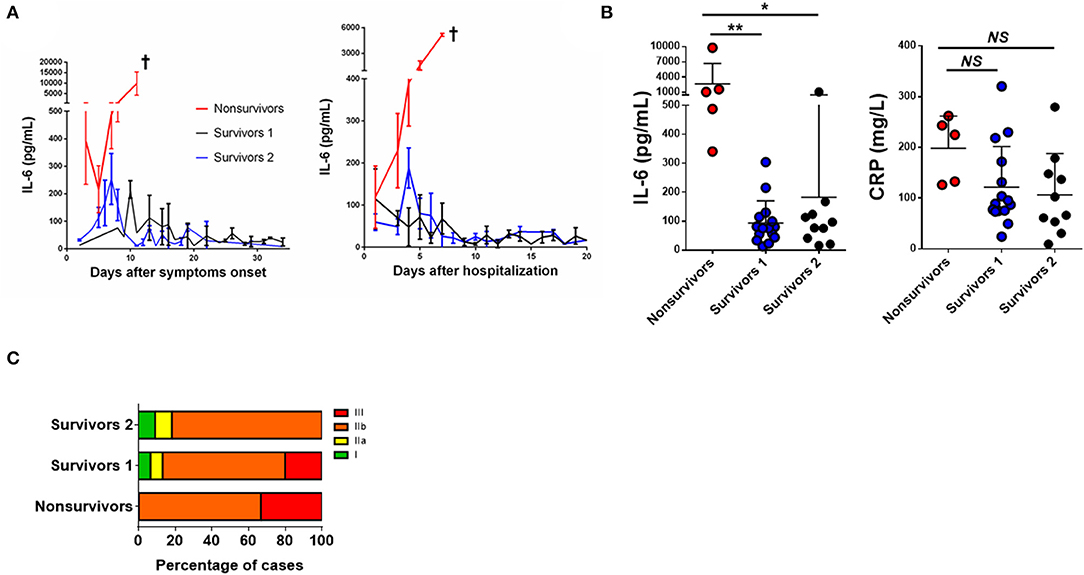
Figure 3. IL-6 as a mortality predictor in COVID-19 Patients. (A) Kinetic analysis of plasma IL-6 concentrations in COVID-19 patients assembled by days after the onset of symptomatology and after hospitalization. Data are represented as the median of plasma IL-6 levels in the non-survivors' group (red n = 5) and two distinguished groups of survivors (blue n = 15 and black n = 10). (B) Plasma levels of IL-6 and CRP. Data depict the number of patients as shown in Table 2, where each dot represents the highest IL-6 level for each patient during hospitalization. (C) Distribution among the disease staging at patient admission assigned to the three groups of non-survivors and survivors. Data are shown as mean ± SD *p < 0.05, **p < 0.01. †patient's death.
Interleukin-6 and CRP levels were evaluated between the three profiles (Figure 3B). IL-6 levels of non-survivors were significantly higher when compared to the survivors' groups (p < 0.0033 and p = 0.0131; for survivors' group 1 and survivors' group 2, respectively), while no significant differences in CRP values were observed among the three profiles. Between the three profiles, there were different distributions of patients between the disease stages: in non-survivors, there were only patients in IIb and III stages, while in both the survivor's groups, patients in the stages I and IIa were also found (Figure 3C).
To identify if these three profiles could be explained by non-infection-related parameters, such as gender, underlying diseases, or treatment, a chi-square dependence test was performed between the profiles and these parameters (Table 2). This is a 3 × 2 chi-square test, thus the p-value was adjusted, being considered dependence only in comparations where p < 0.0042 and with adjusted residual (radj) higher than 2.635. As such, only the treatment with hydroxychloroquine + azithromycin influences the profile (p = 0.0003). However, this dependence is observed only between this treatment and survivors' group 1 and survivors' group 2 (radj=|3.3| and radj=|2.9|, respectively), and it is not observed with the non-survivors' group (radj=|0.8|). Age was also evaluated between profiles: the non-survivors' group has a median age of 86 ± 21 years, the survivors' group 1 has a median age of 64 ± 32 years, and the survivors' group 2 has a median age of 73 ± 21 years. There were no significant differences between these three profiles (p = 0.056).
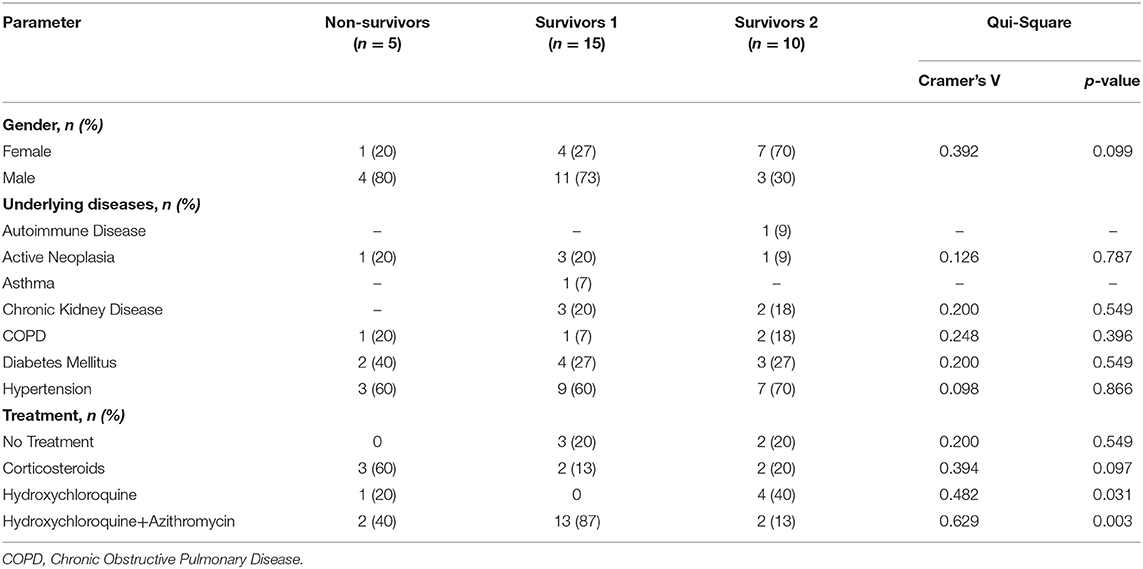
Table 2. Demographic and clinical characterization among different profiles.
Finally, we performed a binary logistic regression to predict the non-survivors' profile. Our model included the variables age, IL-6, and CRP, with a chi-square =24.856, Nagelkerke's R square = 0.752, and p < 0.0001. As presented in Table 3, IL-6 is the most significant variable to predict the non-survivors' profile (p = 0.0430).

Table 3. Logistic binary regression for prediction of profile 1.
There is a high variability across studies in terms of characteristics and outcomes of patients with COVID-19, as these results are influenced by the countries' demographics, clinical settings, and health-systems' available resources. Regarding the studies already published, the best match for ours is a large Spanish cohort, with a similar setting (34). Compared to that study, our cohort was older (median age 8 years higher) and presented more comorbidities; distribution according to sex was very similar (52 vs. 48% males), as was the time from disease onset to admission (7 vs. 6 days). Although the number of patients in our group with respiratory failure and ventilatory support was higher, the mortality was lower (11 vs. 21%). Our cohort was older as compared to the total number of SARS-CoV-2 infected patients in Portugal (median age 17 years higher); this was already expected, considering that older patients are more likely to have severe disease, thus requiring hospitalization (35).
Our study focused on IL-6 due to its reported unique role in the cytokine storm occurring in patients with COVID-19, its good correlation to disease severity, the risk of needing mechanical ventilation, or death, and most importantly, because it can be used as a pharmacological target (14, 17, 25, 28–31, 36, 37). Our results demonstrate that increasing the levels of IL-6 correlate to disease severity and identifying particularly well those patients who evolved to more severe stages of COVID-19, a pattern not observed with other markers such as CRP. Indeed, IL-6 seems to be a potential prognostic marker, as we observed several patients in IIb stage with very high IL-6 levels just before entering stage III, 1 or 2 days later, patterns not observed in CRP levels, despite the positive correlation between IL-6 and CRP (27). This differentiation is critical for patients' monitoring, management of resources, or to support important clinical decisions, like discharging patients safely. Some previous studies have already explored the predictive value of IL-6 on several clinical aspects of COVID-19. At least two of them showed that the level of IL-6 at admission is useful to predict the risk of patients needing mechanical ventilation or high-flow oxygen during hospitalization (26, 29). On the other hand, a Spanish group presented a mortality risk model derived from 443 patients, based on IL-6 at admission (the variable with the highest specificity), SpO2/FiO2 ratio, neutrophil-to-lymphocyte ratio, Lactate dehydrogenase (LDH) level, and age (28). Also, an Italian study suggested a score composed of IL-6 and other six variables as a useful predictor of a composite endpoint of severe COVID-19 and/or in-hospital death (31). Other studies explored the association between IL-6 and the development of lung injury evaluated by CT scan (26, 27). One of these studies evaluated the IL-6 levels throughout hospitalization, recognizing, as in here, the dynamic changes of disease (27). Also, following this concept of variation through time, an Italian retrospective study showed the value of IL-6 combined with CRP and SpO2/FiO2 in signaling patients that would have clinical deterioration at a very short term (in the first 3 days after admission) (32). Interestingly, the score had also a good performance at predicting death at later timepoints. To the best of our knowledge, our work has followed, for the first time, patients over time and showed that IL-6 has special predictive value in patients hospitalized under oxygen therapy (IIb), identifying those who will worsen and eventually die.
From a clinical point of view, IL-6 levels seem to correlate with respiratory failure (PaO2 and SpO2), which is in line with recent studies, showing that SARS-CoV-2 activates innate and adaptive immune responses, resulting in the release of IL-6 and other cytokines, increased vascular permeability, and respiratory failure (38). The fact that injured lungs are the major source of IL-6 may explain the correlations observed between the cytokine levels and oxygen needs (38).
The three profiles of patients characterized in our study are not influenced by gender, comorbidities, or treatment. Once the large majority of our patients were treated with drugs that are now known to be ineffective in COVID-19, we believe this IL-6 kinetics reflects the pathophysiology of disease accurately. It will be interesting, in the future, to evaluate the impact of widely used drugs such as remdesivir and corticosteroids on IL-6 kinetics and their correlation with patient survival. In our study, regarding the non-survivors' profile, the continuously increased levels of IL-6 show that these patients are unable to damp inflammation, leading to patient death. Genetic host factors, impaired viral clearance, low levels of type I interferons, increased neutrophil extracellular traps, T-cell exhaustion, and other miscellaneous factors, have been postulated to increase the individual risk of developing a cytokine storm in response to SARS-CoV-2, a phenomenon where IL-6 has a pivotal role, as previously described (38–40). We did find high levels of IL-6 in survivors, usually preceding patients' clinical worsening, but, in all those cases, IL-6 levels rapidly decreased. Concerning the IL-6 peak, it seems to have a short duration. The peak of IL-6 is observed in both survivors' groups, around 7th and 10th days after the onset of symptoms, respectively. Survivors' group 2 also have a peak at 4th day of hospitalization. As survivors' group 1 were admitted 3 days later than survivors' group 2, we may hypothesize that if they came to the hospital 3 days earlier, we would also observe a peak in that group. Although these data are presented in medians, the critical inflammation point of the disease seems to occur around 1 week to 10 days after the onset of symptoms, reinforcing our clinical observations. Other studies found important clinical deterioration and relevant immunologic or pathophysiologic processes occurring during that period: a peak of viral loads in the sputum and the emergence of dual, antibody, and T-cell dependent, immune response (5, 14, 18, 41). We consider that the novel information on the IL-6 rising kinetics reported here is critical to the successful monitoring of hospitalized patients, but also to patients who remain at home and perhaps need more medical attention on that phase. Furthermore, after 10th day of hospitalization, IL-6 levels tend to become close to normal, even in patients that evolved to stage III. Moreover, we hypothesize that there is a narrow period of time in which immunomodulatory drugs may be particularly effective.
Several studies have already been published about the effect of anti-IL6 agents in COVID-19. Most of them result from observational studies, when anti-IL-6 agents were used empirically, according to hospital protocols that were very diverse in terms of severity criteria and timing of administration. So far, only five RCTs using tocilizumab have their results available. An interventional tocilizumab clinical trial (CORIMUNO-TOCI) was developed with 131 patients with moderate, severe, or critical pneumonia, requiring at least 3 L/min of oxygen but without the need for mechanical ventilation (42). RCT-TCZ-COVID-19 was conducted on a sample of 126 patients with pneumonia, PaO2/FiO2 between 200 and 300 mmHg and an inflammatory phenotype defined by fever and elevated CRP and also excluded patients requiring mechanical ventilation (43). BACC Bay Tocilizumab Trial recruited 242 adult patients with documented SARS-CoV-2 infection with at least two out of three severity criteria (fever, pulmonary infiltrates, or need of supplemental oxygen) and elevation of at least one laboratory parameter associated with inflammation (CRP, ferritin, d-dimer, or lactate dehydrogenase) (44). Patients were excluded if they were receiving more than 10 L of oxygen per minute. COVACTA and EMPACTA enrolled 438 and 391 individuals, respectively (45, 46). In these studies, patients were included if they had evidence of pneumonia and need of supplemental oxygen, with the latter excluding patients needing mechanical ventilatory support.
It seems obvious from this description that IL-6 level was not an inclusion criterion in any of these RCTs. As shown in our study, despite there was some correlation with SpO2, a ratio of PaO2/FiO2, or with CRP, the IL-6 level varies significantly during the infection and has independent meaning, which leaves space to optimizing patient selection. We may hypothesize that therapeutics guided by the IL-6 level, in which randomization would occur only in patients with levels of IL-6 above a certain cut-off, could have produced different, perhaps, better results. In this study, the IL-6 cut-off value as the prognostic value for worse outcome was defined as 86.95 pg/ml, which is in accordance with previous studies. Based on our observations, it is our conviction that IL-6 shall be monitored throughout the infection and not only at admission and that anti-IL-6 therapy should be performed in patients with high IL-6 levels but before the expected peak, to try to avoid clinical deterioration. Even so, pooled data from these RCTs indicate there is a significant reduction in the need for mechanical ventilation when tocilizumab is used, but there is no mortality reduction (33). If we compare to dexamethasone data from RECOVERY, there is a clear difference in sample size, but also in patients' profile: ventilated patients, in whom corticosteroids proved to be more beneficial, were almost always excluded from tocilizumab trials (20). An observational study developed exclusively with critical-ill patients, which compared the evolution of patients at baseline and 1 week after tocilizumab or standard-of-care, showed a significant improvement in FiO2, PaO2:FiO2 and SpO2:FiO2, total radiographic score, and total vascular score, despite the small sample size (47). We, therefore, hope to have contributed to the development of new studies, where IL-6 levels are considered and used to guide therapy at the individual level.
Finally, we assessed the potential of IL-6 to predict the outcome of patients. First, IL-6 levels were significantly lower in each group of survivors than in non-survivors, while CRP was not significantly different across groups. Then, besides our small sample size, we built up a model with only three variables to predict non-survivors, in which IL-6 was a more significant predictor than CRP or age. Overall, our study demonstrates that, in association with clinical observations, the kinetic measurement of IL-6 during SARS-CoV-2 infection is a crucial tool to predict the prognosis, response to therapy, and outcome of patients with COVID-19.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Clinical Board and Ethics Committee. The patients/participants provided their written informed consent to participate in this study.
AS, CC, JP, ACas, and RS designed the experiments. AS, AM-F, AO, LD, AM, and ACar performed the experiments. AS, AM-F, and RS analyzed the data. AS, AM-F, CC, JP, ACas, and RS interpreted the results. AS, AM-F, and RS drafted the manuscript and prepared the tables and figures. AS, AM-F, AO, LD, AM, ACar, CC, JP, ACas, and RS revised the paper and approved the final version of the manuscript. All authors contributed to the article and approved the submitted version.
This work has been funded by National funds, through the Foundation for Science and Technology (FCT)—project UIDB/50026/2020 and UIDP/50026/2020, and by the projects NORTE-01-0145-FEDER-000013 and NORTE-01-0145-FEDER-000023, supported by the Norte Portugal Regional Operational Programme (NORTE 2020), under the PORTUGAL 2020 Partnership Agreement, through the European Regional Development Fund (ERDF) and the FCT contracts UMINHO/BD/57/2018 to AM-F and IF/00021/2014 to RS and the Fundação para a Ciência e Tecnologia (FCT).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
IL-6, interleukin-6; CRP, C-reactive protein; COVID-19, coronavirus disease 2019; ROC, receiver operating characteristic.
1. Channappanavar R, Perlman S. Pathogenic human coronavirus infections: causes and consequences of cytokine storm and immunopathology. Semin Immunopathol. (2017) 39:529–39. doi: 10.1007/s00281-017-0629-x
2. WHO. World Health Organization: Coronavirus Disease (COVID-19) Pandemic. Available online at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019?adgroupsurvey=%7Badgroupsurvey%7D&gclid=Cj0KCQiAlsv_BRDtARIsAHMGVSZmPpAcTMonNgOV8uzphIIPSZXtzAMjm_1Lyq4rVpku0CZc3bE3ZW8aAm_CEALw_wcB (accessed January 4, 2021).
3. Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, et al. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. (2020) 382:727–33. doi: 10.1056/NEJMoa2001017
4. Wiersinga WJ, Rhodes A, Cheng AC, Peacock SJ, Prescott HC. Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (COVID-19): a review. J Am Med Assoc. (2020) 324:782–93. doi: 10.1001/jama.2020.12839
5. To KKW, Tsang OTY, Leung WS, Tam AR, Wu TC, Lung DC, et al. Temporal profiles of viral load in posterior oropharyngeal saliva samples and serum antibody responses during infection by SARS-CoV-2: an observational cohort study. Lancet Infect Dis. (2020) 20:565–74. doi: 10.1016/S1473-3099(20)30196-1
6. Siddiqi HK, Mehra MR. COVID-19 illness in native and immunosuppressed states: a clinical-therapeutic staging proposal. J Hear Lung Transplant. (2020) 39:405–7. doi: 10.1016/j.healun.2020.03.012
7. Romagnoli S, Peris A, Gaudio De AR, Geppetti P. SARS-CoV-2 and COVID-19: from the bench to the bedside. Physiol Rev. (2020) 100:1455–66. doi: 10.1152/physrev.00020.2020
8. Fragkou PC, Belhadi D, Peiffer-Smadja N, Moschopoulos CD, Lescure FX, Janocha H, et al. Review of trials currently testing treatment and prevention of COVID-19. Clin Microbiol Infect. (2020) 26:988–98. doi: 10.1016/j.cmi.2020.05.019
9. Spinner CD, Gottlieb RL, Criner GJ, Arribas López JR, Cattelan AM, Soriano Viladomiu A, et al. Effect of remdesivir vs standard care on clinical status at 11 days in patients with moderate COVID-19: a randomized clinical trial. JAMA J Am Med Assoc. (2020) 324:1048–57. doi: 10.1001/jama.2020.16349
10. Beigel JH, Tomashek KM, Dodd LE, Mehta AK, Zingman BS, Kalil AC, et al. Remdesivir for the treatment of covid-19 — final report. N Engl J Med. (2020) 383:1813–26. doi: 10.1056/nejmoa2007764
11. Piscoya A, Ng-Sueng LF, Parra del Riego A, Cerna-Viacava R, Pasupuleti V, Thota P, et al. Efficacy and harms of convalescent plasma for the treatment of COVID-19 patients: a systematic review and meta-analysis. PLoS ONE. (2020) 15:1–19. doi: 10.2139/ssrn.3697162
12. WHO Solidarity Trial Consortium, Pan H, Peto R, Henao-Restrepo AM, Preziosi MP, Sathiyamoorthy V, et al. Repurposed antiviral drugs for covid-19 - interim WHO solidarity trial results. N Engl J Med. (2020) 1–15. doi: 10.1056/NEJMoa2023184
13. Harrison C. Focus shifts to antibody cocktails for COVID-19 cytokine storm. Nat Biotechnol. (2020) 38:905–8. doi: 10.1038/s41587-020-0634-9
14. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. (2020) 395:497–506. doi: 10.1016/S0140-6736(20)30183-5
15. Behrens EM, Koretzky GA. Cytokine storm syndrome: looking toward the precision medicine era. Arthritis Rheumatol. (2017) 69:1135–43. doi: 10.1002/art.40071
16. Ye Q, Wang B, Mao J. The pathogenesis and treatment of the ‘cytokine storm' in COVID-19. J Infect. (2020) 80:607–13. doi: 10.1016/j.jinf.2020.03.037
17. Iannaccone G, Scacciavillani R, Del Buono MG, Camilli M, Ronco C, Lavie CJ, et al. Weathering the cytokine storm in COVID-19: therapeutic implications. CardioRenal Med. (2020) 10:277–87. doi: 10.1159/000509483
18. Manjili RH, Zarei M, Habibi M, Manjili MH. COVID-19 as an Acute Inflammatory Disease. J Immunol. (2020) 205:12–9. doi: 10.4049/jimmunol.2000413
19. Del Valle DM, Kim-Schulze S, Huang HH, Beckmann ND, Nirenberg S, Wang B, et al. An inflammatory cytokine signature predicts COVID-19 severity and survival. Nat Med. (2020) 26:1636–43. doi: 10.1038/s41591-020-1051-9
20. RECOVERY Collaborative Group, Horby P, Lim WS, Emberson JR, Mafham M, Bell JL, et al. Dexamethasone in hospitalized patients with covid-19 — preliminary report. N Engl J Med. (2020). doi: 10.1056/nejmoa2021436. [Epub ahead of print].
21. Sterne JAC, Murthy S, Diaz JV, Slutsky AS, Villar J, Angus DC, et al. Association between administration of systemic corticosteroids and mortality among critically Ill patients with COVID-19: a meta-analysis. JAMA J Am Med Assoc. (2020) 324:1330–41. doi: 10.1001/jama.2020.17023
22. Velazquez-Salinas L, Verdugo-Rodriguez A, Rodriguez LL, Borca MV. The role of interleukin 6 during viral infections. Front Microbiol. (2019) 10:6–11. doi: 10.3389/fmicb.2019.01057
23. Dienz O, Rud JG, Eaton SM, Lanthier PA, Burg E, Drew A, et al. Essential role of IL-6 in protection against H1N1 influenza virus by promoting neutrophil survival in the lung. Mucosal Immunol. (2012) 5:258–66. doi: 10.1038/mi.2012.2
24. Tanaka T, Narazaki M, Kishimoto T. Immunotherapeutic implications of IL-6 blockade for cytokine storm. Immunotherapy. (2016) 8:959–70. doi: 10.2217/imt-2016-0020
25. Han H, Ma Q, Li C, Liu R, Zhao L, Wang W, et al. Profiling serum cytokines in COVID-19 patients reveals IL-6 and IL-10 are disease severity predictors. Emerg Microbes Infect. (2020) 9:1123–30. doi: 10.1080/22221751.2020.1770129
26. Liu T, Zhang J, Yang Y, Ma H, Li Z, Zhang J, et al. The role of interleukin-6 in monitoring severe case of coronavirus disease 2019. EMBO Mol Med. (2020) 12:1–12. doi: 10.15252/emmm.202012421
27. Liu Z, Li J, Chen D, Gao R, Zeng W, Chen S, et al. Dynamic interleukin-6 level changes as a prognostic indicator in patients with COVID-19. Front Pharmacol. (2020) 11:1093. doi: 10.3389/fphar.2020.01093
28. Rocio LG, Alberto UR, Paloma T, Maria LL, Angel RF, Laura N, et al. Interleukin-6-based mortality risk model for hospitalised COVID-19 patients. J Allergy Clin Immunol. (2020) 146:799–807. doi: 10.1016/j.jaci.2020.07.009
29. Herold T, Jurinovic V, Arnreich C, Lipworth BJ, Hellmuth JC, von Bergwelt-Baildon M, et al. Elevated levels of IL-6 and CRP predict the need for mechanical ventilation in COVID-19. J Allergy Clin Immunol. (2020) 146:128–36. doi: 10.1016/j.jaci.2020.05.008
30. Aziz M, Fatima R, Assaly R. Elevated interleukin-6 and Severe COVID-19: a meta-analysis. J Med Virol. (2020) 92:1–3. doi: 10.1002/jmv.25948
31. Grifoni E, Valoriani A, Cei F, Lamanna R, Gelli AMG, Ciambotti B, et al. Interleukin-6 as prognosticator in patients with COVID-19. J Infect. (2020) 81:452–82. doi: 10.1016/j.jinf.2020.06.008
32. Vultaggio A, Vivarelli E, Virgili G, Lucenteforte E, Bartoloni A, Nozzoli C, et al. Prompt predicting of early clinical deterioration of moderate-to-severe COVID-19 patients: usefulness of a combined score using IL-6 in a preliminary study. J Allergy Clin Immunol Pract. (2020) 8:2575–81. doi: 10.1016/j.jaip.2020.06.013
33. Tleyjeh IM, Kashour Z, Damlaj M, Riaz M, Tlayjeh H, Altannir M, et al. Efficacy and safety of tocilizumab in COVID-19 patients: a living systematic review and meta-analysis. Clin Microbiol Infect. (2020). doi: 10.1016/j.cmi.2020.10.036. [Epub ahead of print].
34. Borobia AM, Carcas AJ, Arnalich F, Álvarez-Sala R, Monserrat-Villatoro J, Quintana M, et al. A cohort of patients with COVID-19 in a major teaching hospital in Europe. J Clin Med. (2020) 9:1–10. doi: 10.1017/CBO9781107415324.004
35. Ferreira A, Oliveira-e-Silva A, Bettencourt P. Chronic treatment with hydroxychloroquine and SARS-CoV-2 infection. J Med Virol. (2020) 93:755–9. doi: 10.1111/cjag.12228
36. Guaraldi G, Meschiari M, Cozzi-Lepri A, Milic J, Tonelli R, Menozzi M, et al. Tocilizumab in patients with severe COVID-19: a retrospective cohort study. Lancet Rheumatol. (2020) 2:e474–84. doi: 10.1016/S2665-9913(20)30173-9
37. Atal S, Fatima Z. IL-6 inhibitors in the treatment of serious COVID-19: a promising therapy? Pharmaceut Med. (2020) 34:223–31. doi: 10.1007/s40290-020-00342-z
38. Hadjadj J, Yatim N, Barnabei L, Corneau A, Boussier J, Smith N, et al. Impaired type I interferon activity and inflammatory responses in severe COVID-19 patients. Science. (2020) 369:718–24.
39. Soy M, Keser G, Atagündüz P, Tabak F, Atagündüz I, Kayhan S. Cytokine storm in COVID-19: pathogenesis and overview of anti-inflammatory agents used in treatment. Clin Rheumatol. (2020) 39:2085–94. doi: 10.1007/s10067-020-05190-5
40. Blanco-Melo D, Nilsson-Payant BE, Liu WC, Uhl S, Hoagland D, Møller R, et al. Imbalanced host response to SARS-CoV-2 drives development of COVID-19. Cell. (2020) 181:1036–45.e9. doi: 10.1016/j.cell.2020.04.026
41. Wölfel R, Corman VM, Guggemos W, Seilmaier M, Zange S, Müller MA, et al. Virological assessment of hospitalized patients with COVID-2019. Nature. (2020) 581:465–9. doi: 10.1038/s41586-020-2196-x
42. Hermine O, Mariette X, Tharaux PL, Resche-Rigon M, Porcher R, Ravaud P. Effect of tocilizumab vs usual care in adults hospitalized with COVID-19 and moderate or severe pneumonia: a randomized clinical trial. JAMA Intern Med. (2020) 181:32–40. doi: 10.1001/jamainternmed.2020.6820
43. Salvarani C, Dolci G, Massari M, Merlo DF, Cavuto S, Savoldi L, et al. Effect of tocilizumab vs standard care on clinical worsening in patients hospitalized with COVID-19 pneumonia: a randomized clinical trial. JAMA Intern Med. (2021) 181:24–31. doi: 10.1001/jamainternmed.2020.6615
44. Stone JH, Frigault MJ, Serling-Boyd NJ, Fernandes AD, Harvey L, Foulkes AS, et al. Efficacy of tocilizumab in patients hospitalized with covid-19. N Engl J Med. (2020) 383:2333–44. doi: 10.1056/nejmoa2028836
45. CONVACTA. A Study to Evaluate the Safety and Efficacy of Tocilizumab in Patients With Severe COVID-19 Pneumonia. (2020). Available online at: https://clinicaltrials.gov/ct2/show/NCT04320615 (accessed January 1, 2021).
46. EMPACTA. A Study to Evaluate the Efficacy and Safety of Tocilizumab in Hospitalized Participants With COVID-19 Pneumonia. (2020). Available online at: https://clinicaltrials.gov/ct2/show/NCT04372186 (accessed January 2, 2021).
Keywords: COVID-19, IL-6, SARS-CoV-2, fatal pneumonia, biomarker
Citation: Santa Cruz A, Mendes-Frias A, Oliveira AI, Dias L, Matos AR, Carvalho A, Capela C, Pedrosa J, Castro AG and Silvestre R (2021) Interleukin-6 Is a Biomarker for the Development of Fatal Severe Acute Respiratory Syndrome Coronavirus 2 Pneumonia. Front. Immunol. 12:613422. doi: 10.3389/fimmu.2021.613422
Received: 02 October 2020; Accepted: 21 January 2021;
Published: 18 February 2021.
Edited by:
Giuseppe Sciumè, Sapienza University of Rome, ItalyReviewed by:
Alessio Mazzoni, University of Florence, ItalyCopyright © 2021 Santa Cruz, Mendes-Frias, Oliveira, Dias, Matos, Carvalho, Capela, Pedrosa, Castro and Silvestre. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: André Santa Cruz, YW5kcmVzY2pvYW9AbWVkLnVtaW5oby5wdA==; Ricardo Silvestre, cmljYXJkb3NpbHZlc3RyZUBtZWQudW1pbmhvLnB0
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.