
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol. , 23 February 2021
Sec. Autoimmune and Autoinflammatory Disorders
Volume 11 - 2020 | https://doi.org/10.3389/fimmu.2020.588582
 Christian D. Sadik1,2*†
Christian D. Sadik1,2*† Ewan A. Langan1,3†
Ewan A. Langan1,3† Ralf Gutzmer4Maria Isabel Fleischer5Carmen Loquai5Lydia Reinhardt6Friedegund Meier6Daniela Göppner7Rudolf A. Herbst8
Ralf Gutzmer4Maria Isabel Fleischer5Carmen Loquai5Lydia Reinhardt6Friedegund Meier6Daniela Göppner7Rudolf A. Herbst8 Detlef Zillikens1,2
Detlef Zillikens1,2 Patrick Terheyden1
Patrick Terheyden1Immune-related adverse events (irAEs) are a class-effect of checkpoint inhibitors (CIs). The development of a Bullous pemphigoid (BP)-like blistering disease, driven by autoantibodies against the hemidesmosomal protein BP180, is a potentially serious irAE whose incidence seems to be increasing. We therefore set out to characterize the clinical and (immuno)histopathological features and treatment responses of cases of BP which developed during or after CI therapy collated in six German tertiary referral centers between 2014 and 2018. We identified twelve cases of BP which emerged during and/or after CI therapy. The time interval between the initiation of CI therapy and the diagnosis of BP was 3–74 weeks (median: 23 weeks). Age at the time of diagnosis of BP varied between 62 and 80 years (median: 76 years). The clinical presentation of the patients was diverse but the severity was relatively mild when compared to that seen in most cases of spontaneous BP. Only four patients met all of the immunopathological criteria recommended in the European guidelines for the diagnosis of BP. Topical corticosteroid treatment was sufficient to achieve disease control in most patients. CI therapy could be continued in 8 out of 12 patients. In summary, our study indicates that cases of BP during or after CI therapy bear several peculiarities distinguishing them from spontaneous BP. Given the diversity of the clinical presentation of CI-induced BP the application of existing diagnostic algorithms developed for spontaneous BP can be utilized to uncover the frequency and features of CI-induced BP and to develop and optimize management algorithms.
Checkpoint inhibitors (CIs) constitute a new class of immunomodulatory drugs which block co-inhibitory signals on immune effector cells and result in the generation of potent T-cell mediated immune responses. Among the CIs which are currently licensed are monoclonal antibodies which target the cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) or the programmed cell death protein 1 (PD-1) pathway. For example, the first-in-class drug ipilimumab inhibits CTLA-4, nivolumab and pembrolizumab inhibit PD-1, and atezolizumab and durvalumab target the PD-1 ligand PD-L1 (1). The advent of checkpoint inhibitors has revolutionized the treatment of solid cancers. Initially licensed for the treatment of metastatic melanoma, CIs are employed in an ever increasing number of cancer entities, including Merkel cell carcinoma, head and neck squamous cell carcinoma, renal cell carcinoma, non-small cell lung cancer, urothelial bladder cancer, hepatocellular carcinoma, and Hodgkin’s lymphoma (1).
Given that the CTLA-4 and PD-1 pathways play a central role in regulating cellular immune responses, removal of this control mechanism can result in both generalized and tissue-specific inflammation. These inflammatory responses are collectively termed “immune-related adverse events” (irAEs), and include, but are not limited to, dermatitis, colitis, hypophysitis, hepatitis, and nephritis (1). The skin is the most frequently affected organ, with up to 50% of patients receiving CIs developing skin-related irAEs.
The clinical presentation of cutaneous irAEs is remarkably diverse. Commonly presenting with a non-specific maculopapular rash accompanied by pruritus, they may also present with lichenoid, eczematous, granulomatous, lupus-like, or erythema multiforme-like skin changes and/or vitiligo (2).
Most intriguingly, there is a growing body of literature which reports the development of the antibody-driven autoimmune disease bullous pemphigoid (BP), the most common disease of the group of pemphigoid diseases, in the context of treatment with immune CI (2–8).
The hallmark of BP is the development of autoimmunity against type XVII collagen (BP180) (9). BP presents clinically with the development of widespread urticarial plaques (pre-bullous phase), which evolve into blisters and erosions (10, 11). However, non-bullous and atypical variants of BP also exist. In these variants, patients exhibit localized blister formation with minimal or absent inflammation of the surrounding skin. Additionally, BP may present with predominantly eczematous (including dyshidrosiform) and subacute prurigo-like skin changes (12). Indeed, BP may exist in the absence of skin changes, with the only symptom being widespread, intractable itch. Given the wide spectrum of clinical symptoms and signs in BP, the disease can neither be reliably diagnosed nor excluded based on the clinical presentation alone. The European Academy of Dermatology and Venereology (EADV) guidelines recommend that the diagnosis of BP should be based on both the clinical findings and (immuno)pathological investigations of the patient’s skin, both lesional and perilesional, and serum (12). Central to establishing the diagnosis of BP is the demonstration of linear depositions of autoantibodies, which are in most cases predominantly of the IgG immunoglobulin class, and/or of complement factor 3 (C3) at the dermal-epidermal junction (DEJ) of perilesional skin (12). As the deposition of autoantibodies and/or complement at the DEJ is the defining feature of all pemphigoid diseases and as the clinical features of BP may overlap with those of other pemphigoid diseases, the clear distinction of pemphigoid diseases requires the detection of autoantibodies in the serum and a determination of their antigen specificity. This is achieved by indirect immunofluorescence microscopy on NaCl-split human skin, which detects the presence of autoantibodies against proteins of the dermal-epidermal junction, and by ELISA biochip-based techniques, and/or immunoblot assays to pinpoint the antigen specificity of the autoantibodies. Serological examination alone is not sufficient to diagnose BP given that autoantibodies are reportedly undetectable in the serum of up to 20% of BP patients, but are present in the serum of 0.5% of healthy individuals (12, 13). Histopathologically, an early blister exhibits a subepidermal cleft combined with a dense dermal inflammatory infiltrate mainly consisting of eosinophils and neutrophils. However, the histopathological examination is also non-specific and is therefore not suitable alone to confirm the diagnosis (14).
The complexity and heterogeneity of both BP and cutaneous irAEs means that a comprehensive clinical, serological, and (immuno)histopathological work-up is central to correctly diagnosing suspected cases of BP during or after CI therapy. In the present study, we retrospectively profiled twelve cases of CI-associated BP diagnosed in six German Dermatology centres and contrasted their features with previously reported cases of both immune-checkpoint mediated and spontaneous BP.
We systematically searched the clinical records of patients treated with CIs between 2014 and 2018 in six German Dermatology centres for the diagnosis of BP. The case notes of affected patients were then retrospectively analyzed to determine the salient clinical, histopathological, and immunopathological features. Histo- and immunopathological analyses were conducted by routine autoimmune and dermatohistopathology laboratories. Ethical approval was obtained from the University of Lübeck’s ethics committee 19-332A.
We identified 12 patients diagnosed with BP during immune CI therapy between 2014 and 2018. Seven patients were undergoing CI for metastatic cutaneous melanoma. The remaining patients were receiving CI therapy for metastatic uveal melanoma, metastatic melanoma of unknown primary, squamous cell carcinoma of the lung, and renal cell carcinoma (Table 1).
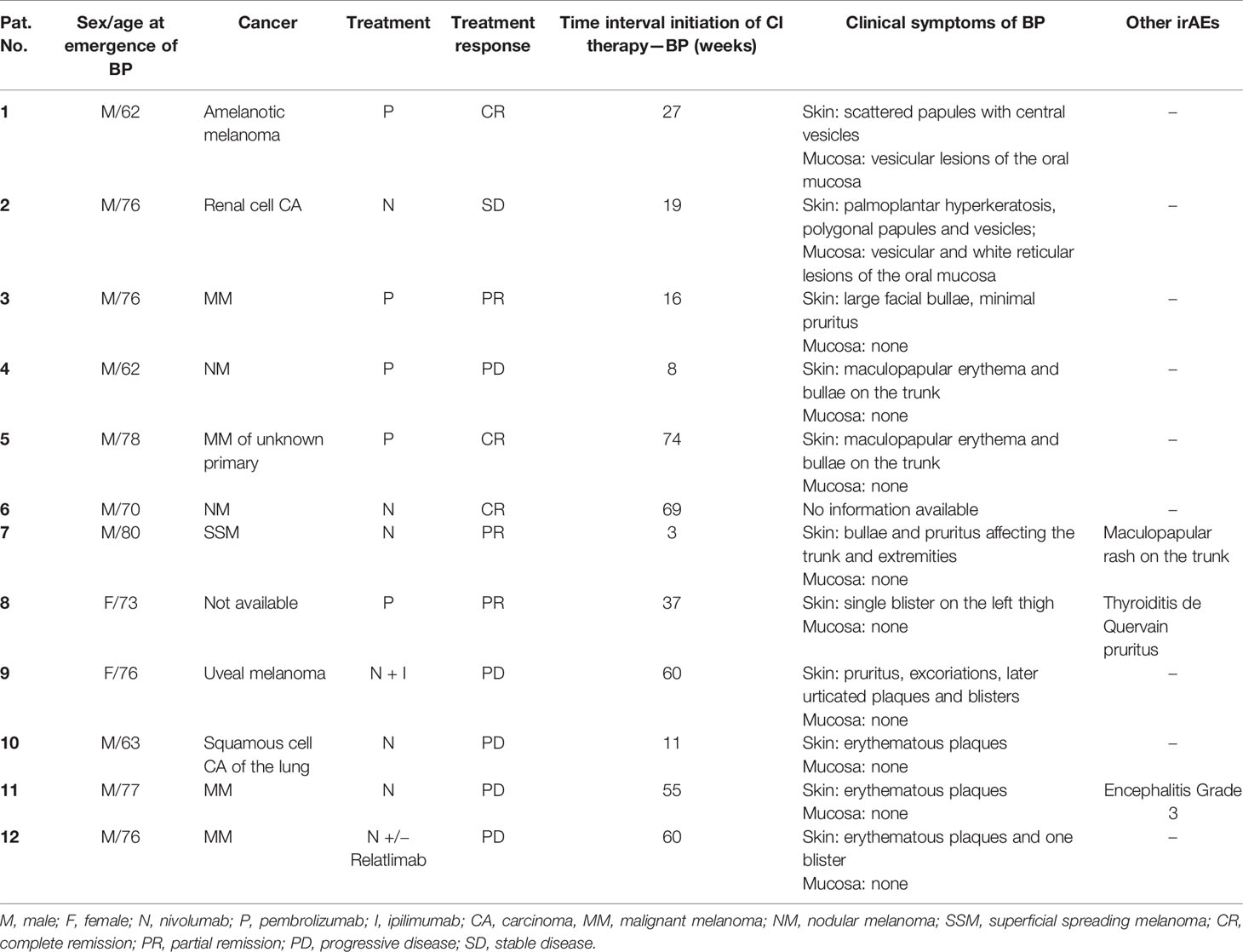
Table 1 Clinical features of patients diagnosed with bullous pemphigoid (BP) under CI therapy.
Ten patients were males, two were females. The age at diagnosis of BP ranged between 62 and 80 years with a median age of 76 years (Figure 1). Five patients received pembrolizumab, six received nivolumab, and in one case the combination of nivolumab and ipilimumab was administered (Table 1). The median time interval from the initiation of CI therapy to the diagnosis of BP was 23 weeks and ranged between 3 and 74 weeks (Figure 1).
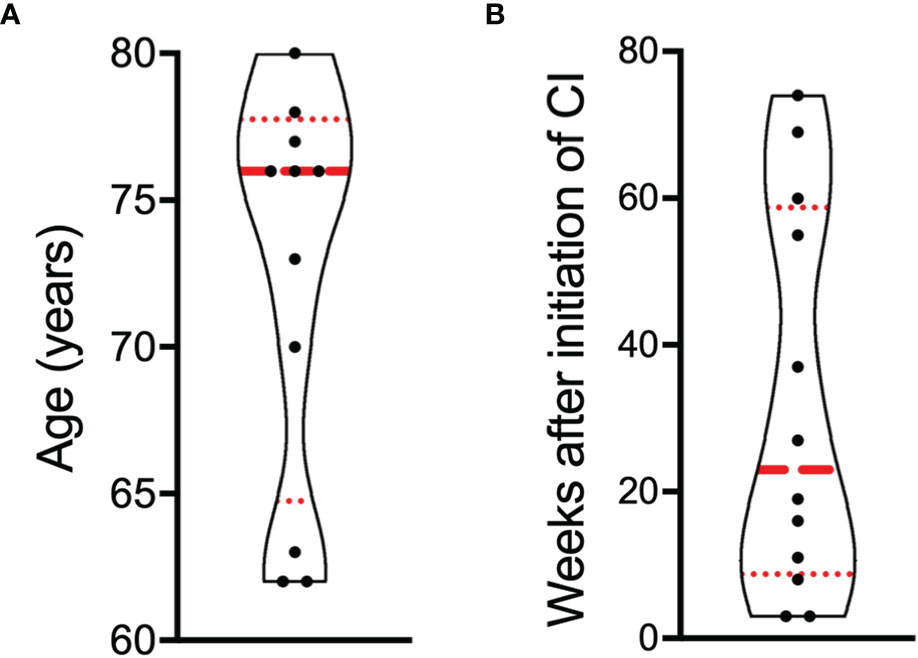
Figure 1 Distribution of age and latency after the initiation of CI therapy to the diagnosis of bullous pemphigoid (BP). (A) Age of patients at the diagnosis of BP. (B) Time interval in weeks between the initiation of CI therapy and the diagnosis of BP. Results are presented as violin plot. Each dot represents one patient (n = 12). The red dashed line represents the median, the red dotted lines the 25 and 75% percentiles.
The clinical presentation of the 12 patients at the time of diagnosis of BP is detailed in Table 1, and illustrations of their clinical presentation are compiled in Figure 2.
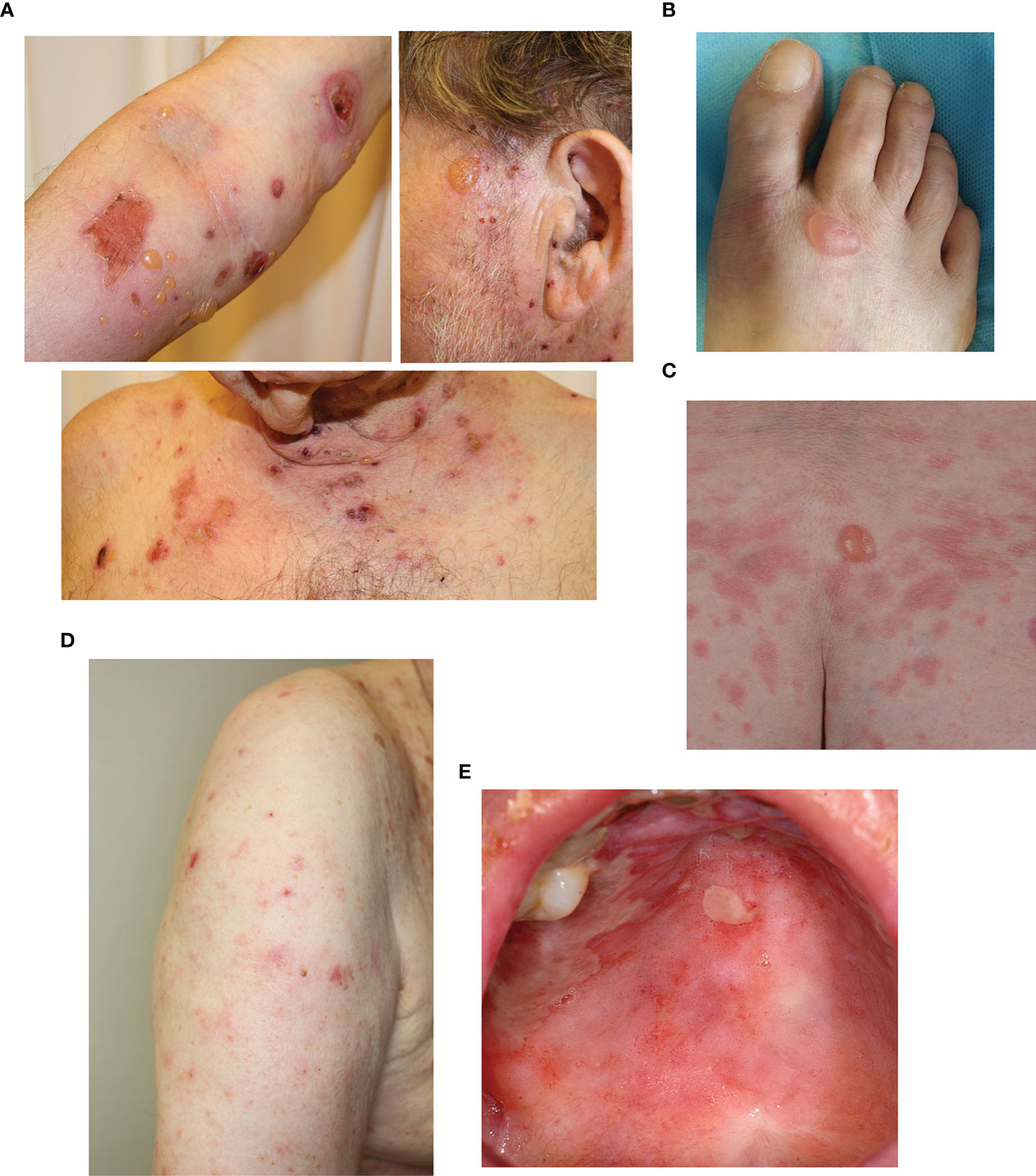
Figure 2 Examples of clinical manifestations of cases diagnosed as bullous pemphigoid (BP) under CI therapy. (A) Patient presenting with erythematous urticaria and tense blisters and erosions scattered over larger areas of the body, typical for classical BP. Patients presenting with (B) a single blister and (C) a single blister and erythematous urticaria. (D) Eczematous skin changes. (E) Oral mucosal erosions.
Nine patients developed vesico-bullous skin changes, but in two of these patients this comprised only a single blister (Table 1). Two patients exhibited urticarial plaques without blistering, the typical presentation of the pre-bullous state of BP (15). Two patients additionally developed vesicles affecting the oral mucosa; the only patients to exhibit involvement of the mucous membranes.
Direct immunofluorescence (DIF) microscopy was only conducted in six of the patients. Linear IgG and C3 depositions were present in the skin biopsies from five patients, and only linear C3 deposition in one patient (Table 2). Indirect immunofluorescence (IIF) microscopy using monkey esophagus and/or salt-split human skin was performed in eleven patients. IgG antibodies were thereby detected in seven patients (Table 2). One of these patients additionally had low levels of IgA autoantibodies in the serum. Circulating IgA but not IgG antibodies, binding to the epidermal side of salt-split skin, were detected in one patient who presented with a single blister affecting the left thigh (Tables 1 and 2). IIF microscopy was negative in three patients (Table 2). The sera of nine patients were examined for anti-BP180 IgG by ELISA. Anti-BP180 IgG was detectable in four of these patients, and in another patient anti-LAD IgG was detected by immunoblot (Table 2). In the sera of two patients positive for anti-BP180 IgG, anti-BP230 IgG was additionally present. The histopathological findings were variable (Table 2), but the histopathological picture was often summarized as interface dermatitis.
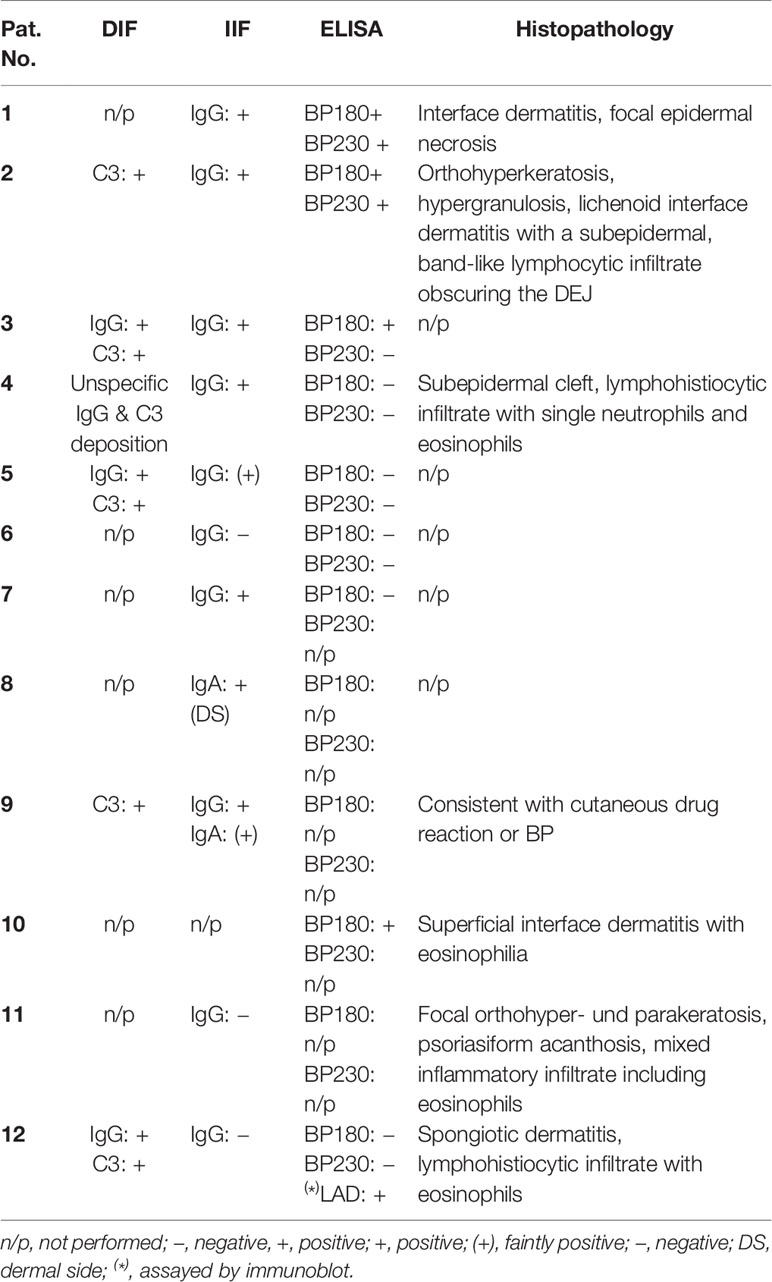
Table 2 Summary of immuno- and histopathology.
After the diagnosis of BP, CI therapy was permanently discontinued in four patients but switched or continued in the remaining eight patients (Table 3). The treatment of the skin lesions in the different centers in 11 cases included topical corticosteroids (classes II to IV according to Niedner’s classification) (Table 3). Three patients additionally required treatment with systemic corticosteroids, one of these patients also received three cycles of rituximab. Treatment resulted in a complete resolution of the skin findings in six patients and a partial resolution in the remaining six patients. Eleven patients remain alive, but one patient has subsequently died of metastatic melanoma.
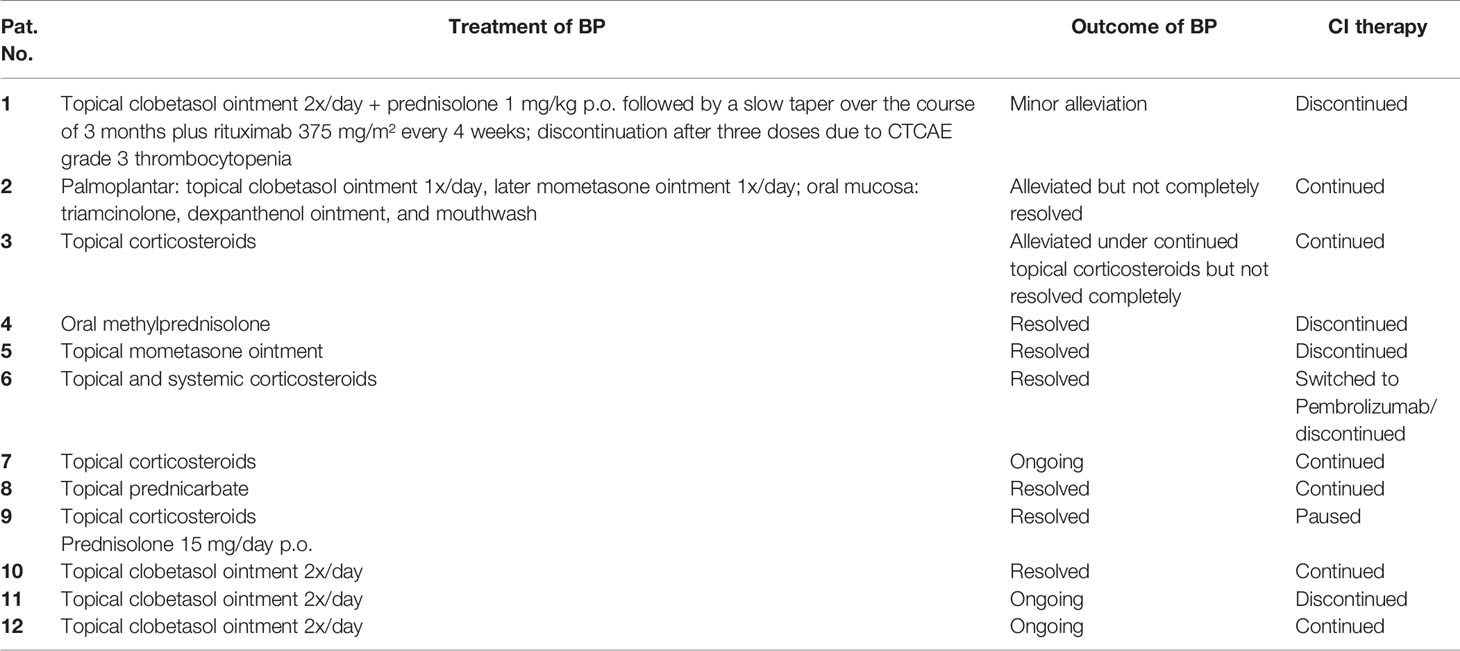
Table 3 Management and outcome of bullous pemphigoid (BP).
We identified 12 patients who developed BP, while undergoing CI therapy for metastatic cancer, via a retrospective analysis of case notes at six Departments of Dermatology in Germany. Our analysis reveals that the minimal diagnostic requirements needed to confirm the presence of BP were not met in all cases, suggesting that diagnostic algorithms for BP have not been fully incorporated into routine clinical practice and testing for linear deposition of autoantibodies and/or C3 at the DEJ was not performed as standard.
In fact, linear depositions of autoantibodies or C3 at the DEJ were demonstrated in six out of twelve cases recorded as “BP during CI therapy.” It must be borne in mind that these minimal requirements do not allow a clear distinction between BP and other pemphigoid diseases such as the inflammatory variant of epidermolysis bullosa acquisita and anti-p200 pemphigoid, which cannot be clearly distinguished from BP by the clinical presentation alone. Given that linear deposition of autoantibodies at the DEJ is also present in epidermolysis bullosa acquisita and anti-p200 pemphigoid, the diagnosis of BP can only be confirmed by additionally detecting anti-BP180 IgG in the serum. This criterion was only met in four of our cases. The detection of linear depositions of IgG at the DEJ and the demonstration of anti-BP180 IgG antibodies in the serum was only met in three cases. The absence of confirmatory serum anti-BP180 IgG antibodies is a frequent finding in the hitherto reported cases of BP during CI therapy. Therefore, it is difficult to determine the true incidence and prevalence of BP during CI therapy. Nevertheless, a temporal relationship between the use of CI therapy and the development of BP and/or the development of BP during a re-challenge with CI therapy provide evidence for an irAE aetiology.
Given the complexity and clinical heterogeneity of BP as an autoimmune blistering dermatosis, let alone as an irAE, diagnostic algorithms for the accurate diagnosis of cutaneous irAEs under CI therapy are necessary not only to optimize CI therapy and improve the management of its side-effects, but also to gain new insight into the pathophysiology of autoimmune blistering diseases in general. We therefore suggest that in all cases of cutaneous irAEs under CI, including cases where severe pruritus is the only symptom, DIF microscopy for linear depositions of autoantibodies at the DEJ should be considered. If positive, serological analyses searching for autoantibodies against proteins of the dermal-epidermal adhesion complex should be conducted. The analyses should include IIF microscopy to screen for autoantibodies directed to proteins of the dermal-epidermal adhesion complex and should optimally be conducted on NaCl-split human skin because it, in contrast to the alternative substrate monkey esophagus, allows BP to be distinguished from epidermolysis bullosa acquisita and anti-p200 pemphigoid depending on where the antibodies bind. IIF microscopy should be followed by ELISA and immunoblotting analyses to precisely determine the antigen specificity of the autoantibodies. Employing this diagnostic algorithm may ensure the accurate determination of the frequency of pemphigoid diseases, possibly induced by CIs, and to pinpoint their specific features, central to improving the management of cutaneous irAEs. In fact, determination of the presence and serum concentration of autoantibodies directed to proteins of the dermal-epidermal adhesion complex could even be considered prior to the initiation of CI therapy. This may help to determine whether CI inhibition may promote the emergence of BP by facilitating the break of tolerance against proteins of the dermal-epidermal adhesion complex or by promoting the initiation of the effector phase in individuals in whom tolerance had already been broken before the administration of CIs. Ultimately, patient subgroups with increased susceptibility to BP under CI therapy could be identified to facilitate earlier recognition and treatment. Interestingly, it has recently been suggested that the development of skin autoantibodies may even be associated with improved response to CI therapy, albeit in lung cancer (16). Therefore, the detection of skin autoantibodies may actually provide additional prognostic information.
Furthermore, it is worth bearing in mind that CI therapy has also been associated with the development of lichen planus pemphigoides (LPP) (17, 18). While the clinical presentation of LPP may mimic BP, a careful correlation of the clinical, histopathological, and immunopathological features usually permits differentiation between these two conditions.
The twelve cases of BP during CI therapy reported here were mild to moderate in their clinical severity. In contrast to spontaneous BP, the skin lesions were often restricted to single body areas and treatment with topical or oral corticosteroids alone was sufficient to achieve disease control in 11 patients. Topical therapy for spontaneous BP, according to the European guidelines, usually includes whole body treatment with superpotent corticosteroids twice daily (12). However, topical therapy alone is often not sufficient to control the disease and the addition of one or two systemic treatment options, including dapsone, azathioprine, mycophenolate mofetil, doxycycline, high-dose intravenous corticosteroid pulses, intravenous immunoglobulins, or rituximab is often necessary.
It is striking that no patient required the topical treatment regimen recommended by the European guidelines and that only one patient required systemic treatment with rituximab. Although rituximab has been highlighted in a recent case report to be effective in the treatment of CI-induced BP, in our patient the effect was poor, consistent with its limited efficacy in spontaneous BP (19).
Furthermore, the histopathological analysis of lesional skin in our study, as well as in many case reports, revealed a minimal inflammatory infiltrate in the dermis. These features are reminiscent of the findings reported recently in BP induced by dipeptidyl peptidase IV inhibitors (“gliptins”) used in the treatment of diabetes (20–22), although a causal link between gliptin intake and BP has not yet been established. Similar to CI-associated disease, gliptin-associated cases tend to feature milder skin inflammation (22), and discontinuing gliptins does not lead to spontaneous reversal of disease as is the case for most other drug-induced cutaneous side-effects (20). Intriguingly, dipeptidyl peptidase IV (CD26) exerts diverse immunomodulatory roles, including regulatory functions in T cell activation similar to PD-1 and its ligands (23). It is therefore tempting to speculate that gliptins and CIs elicit BP by related molecular mechanisms.
Collectively, our retrospective analysis reveals important differences between spontaneous BP and BP-induced during CI therapy. Firstly, BP during CI therapy was milder than as is case in spontaneous BP. Secondly, the immunopathological features of spontaneous BP were only confirmed in a minority of CI-induced cases. Whilst this may result from a lack of familiarity of the diagnostic algorithms for BP in oncology, it may also reflect a milder immune response to BP180 in IC-induced BP, potentially explaining the less severe phenotype. Consequently, the immunopathological analyses usually used for the diagnosis of BP may be not sensitive enough and, with respect to ELISA assays, the cut-lines defined for BP to distinguish pathological and non-pathological autoantibody levels may be not completely applicable to diagnose CI-induced BP. In line with this latter notion, it has recently been reported that levels of anti-BP180 IgG are often increased in patients under CI therapy but in the vast majority of cases still do not reach the defined cut-off lines between the pathological and non-pathological range. Furthermore, commercially available ELISAs for the detection of anti-BP180 IgG only detect autoantibodies directed to one or both terminal ends of the NC16A domain of BP180. It cannot be excluded that blistering disease induced by CI therapy results from the production of autoantibodies against other parts of the protein. Indeed, there are also reports of CI inducing rare BP variants, including anti-LAD-1 IgG-positive, anti-BP180 NC16A IgG-negative BP (24).
Perhaps the most important question for the clinical management of CI-induced BP is whether CI therapy can be continued. Whilst the decision to continue IC therapy in patients with IC-induced BP should be made on an individual basis, carefully weighing up the risks and benefits, it is reassuring that treatment could be continued in a number of our patients. In fact, it is worth noting that similar to the case in IC-induced vitiligo (25, 26), IC-induced BP may be associated with improved treatment response and increased overall survival (27), although this remains to be confirmed in larger, prospective studies.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Ethics Committee of the University of Lübeck.
CS, EAL, PT, RG, MF, CL, LR, FM, DG, RH, and DZ identified patients and characterized these cases. CS, EAL, and PT planned the study, analyzed the data, and wrote the paper. RG, MF, CL, LR, FM, DG, RH, and DZ revised the paper. All authors contributed to the article and approved the submitted version.
This research was supported by DFG funding for the Clinician Research Unit 303 Pemphigoid Diseases—Molecular Pathways and their therapeutic Potential and for the Excellence Cluster 2167 Precision Medicine in Chronic Inflammation.
DG reports personal fees and other from Pierre Fabre Pharma Gmbh, personal fees and other from Roche Pharma AG, personal fees and other from Bristol-Myers Squibb GmbH & Co. KGaA, personal fees and other from Novartis Pharma GmbH, personal fees and other from Sanofi-Aventis GmbH, during the conduct of the study; other from Amgen GmbH, other from Janssen-Cilag GmbH, other from Galderma Laberatorium GmbH, outside the submitted work. RG reports personal fees and non-financial support from BristolMyersSquibb, personal fees and non-financial support from Roche Pharma, grants, personal fees and non-financial support from Merck Serono, grants, personal fees and non-financial support from Amgen, personal fees and non-financial support from Pierre Fabre, grants, personal fees and non-financial support from Sanofi Regeneron, personal fees from MerckSharpDohme, grants, personal fees and non-financial support from Novartis, personal fees from Almirall Hermal, grants and personal fees from Pfizer, personal fees from SUN Pharma, personal fees from 4SC, grants from Johnson&Johnson outside the submitted work. RH reports personal fees from ROCHE, personal fees from BMS, personal fees from MSD, personal fees from Novartis, personal fees from Pierre-Fabre, outside the submitted work. EL reports personal fees and non-financial support from BristolMyersSquibb, personal fees and non-financial support from Novartis, Meeting and travel support from Curevac and advisory board fees from Sun Pharma. CL reports personal fees from BMS, personal fees from MSD, personal fees from Sanofi, personal fees from Novartis, personal fees from Roche, personal fees from Pierre Fabre, personal fees from Amgen, personal fees from Kyowa Kirin, personal fees from Biontech, personal fees from Almiral Hermal, personal fees from Sun Pharma, personal fees from Merck, outside the submitted work. PT: speaker´s honoraria from BMS, Novartis, MSD, Pierre-Fabre, CureVac and Roche, consultant´s honoraria from BMS, Novartis, Pierre-Fabre, Merck Serono, Sanofi und Roche and travel support fom BMS, Pierre-Fabre and Roche.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Callahan MK, Postow MA, Wolchok JD. Targeting T Cell Co-receptors for Cancer Therapy. Immunity (2016) 44(5):1069–78. doi: 10.1016/j.immuni.2016.04.023
2. Sibaud V. Dermatologic Reactions to Immune Checkpoint Inhibitors : Skin Toxicities and Immunotherapy. Am J Clin Dermatol (2018) 19(3):345–61. doi: 10.1007/s40257-017-0336-3
3. Siegel J, Totonchy M, Damsky W, Berk-Krauss J, Castiglione F Jr., Sznol M, et al. Bullous disorders associated with anti-PD-1 and anti-PD-L1 therapy: A retrospective analysis evaluating the clinical and histopathologic features, frequency, and impact on cancer therapy. J Am Acad Dermatol (2018) 79(6):1081–8. doi: 10.1016/j.jaad.2018.07.008
4. Sun CW, Grossman SK, Aphale A, Hsu S. Pembrolizumab-induced bullous pemphigoid. JAAD Case Rep (2019) 5(4):362–4. doi: 10.1016/j.jdcr.2019.02.008
5. Heinzerling L, de Toni EN, Schett G, Hundorfean G, Zimmer L. Checkpoint Inhibitors. Dtsch Arztebl Int (2019) 116(8):119–26. doi: 10.3238/arztebl.2019.0119
6. Jour G, Glitza IC, Ellis RM, Torres-Cabala CA, Tetzlaff MT, Li JY, et al. Autoimmune dermatologic toxicities from immune checkpoint blockade with anti-PD-1 antibody therapy: a report on bullous skin eruptions. J Cutan Pathol (2016) 43(8):688–96. doi: 10.1111/cup.12717
7. Hirotsu K, Chiou AS, Chiang A, Kim J, Kwong BY, Pugliese S. Localized bullous pemphigoid in a melanoma patient with dual exposure to PD-1 checkpoint inhibition and radiation therapy. JAAD Case Rep (2017) 3(5):404–6. doi: 10.1016/j.jdcr.2017.06.004
8. Thomsen K, Diernaes J, Ollegaard TH, Spaun E, Vestergaard C. Bullous Pemphigoid as an Adverse Reaction to Pembrolizumab: Two Case Reports. Case Rep Dermatol (2018) 10(2):154–7. doi: 10.1159/000489661
9. Sadik CD, Schmidt E, Zillikens D, Hashimoto T. Recent progresses and perspectives in autoimmune bullous diseases. J Allergy Clin Immunol (2020) 145(4):1145–7. doi: 10.1016/j.jaci.2020.02.020
10. Sadik CD, Schmidt E. Resolution in bullous pemphigoid. Semin Immunopathol (2019) 41(6):645–54. doi: 10.1007/s00281-019-00759-y
11. Egami S, Yamagami J, Amagai M. Autoimmune bullous skin diseases, pemphigus and pemphigoid. J Allergy Clin Immunol (2020) 145(4):1031–47. doi: 10.1016/j.jaci.2020.02.013
12. Feliciani C, Joly P, Jonkman MF, Zambruno G, Zillikens D, Ioannides D, et al. Management of bullous pemphigoid: the European Dermatology Forum consensus in collaboration with the European Academy of Dermatology and Venereology. Br J Dermatol (2015) 172(4):867–77. doi: 10.1111/bjd.13717
13. Prussmann W, Prussmann J, Koga H, Recke A, Iwata H, Juhl D, et al. Prevalence of pemphigus and pemphigoid autoantibodies in the general population. Orphanet J Rare Dis (2015) 10:63. doi: 10.1186/s13023-015-0278-x
14. Schmidt E, Zillikens D. Pemphigoid diseases. Lancet (2013) 381(9863):320–32. doi: 10.1016/S0140-6736(12)61140-4
15. Sadik CD, Lima AL, Zillikens D. Pemphigoid gestationis: Toward a better understanding of the etiopathogenesis. Clin Dermatol (2016) 34(3):378–82. doi: 10.1016/j.clindermatol.2016.02.010
16. Ali OH, Bomze D, Ring S, Berner F, Fassler M, Diem S, et al. BP180-specific IgG is associated with skin adverse events, therapy response and overall survival in non-small cell lung cancer patients treated with checkpoint inhibitors. J Am Acad Dermatol (2020) 82(4):854–61. doi: 10.1016/j.jaad.2019.08.045
17. Strickley JD, Vence LM, Burton SK, Callen JP. Nivolumab-induced lichen planus pemphigoides. Cutis (2019) 103(4):224–6.
18. Sato Y, Fujimura T, Mizuashi M, Aiba S. Lichen planus pemphigoides developing from patient with non-small-cell lung cancer treated with nivolumab. J Dermatol (2019) 46(10):e374–e5. doi: 10.1111/1346-8138.14906
19. Lamberts A, Euverman HI, Terra JB, Jonkman MF, Horvath B. Effectiveness and Safety of Rituximab in Recalcitrant Pemphigoid Diseases. Front Immunol (2018) 9:248. doi: 10.3389/fimmu.2018.00248
20. Plaquevent M, Tetart F, Fardet L, Ingen-Housz-Oro S, Valeyrie-Allanore L, Bernard P, et al. Higher Frequency of Dipeptidyl Peptidase-4 Inhibitor Intake in Bullous Pemphigoid Patients than in the French General Population. J Invest Dermatol (2019) 139(4):835–41. doi: 10.1016/j.jid.2018.10.045
21. Varpuluoma O, Forsti AK, Jokelainen J, Turpeinen M, Timonen M, Huilaja L, et al. Vildagliptin Significantly Increases the Risk of Bullous Pemphigoid: A Finnish Nationwide Registry Study. J Invest Dermatol (2018) 138(7):1659–61. doi: 10.1016/j.jid.2018.01.027
22. Tasanen K, Varpuluoma O, Nishie W. Dipeptidyl Peptidase-4 Inhibitor-Associated Bullous Pemphigoid. Front Immunol (2019) 10:1238. doi: 10.3389/fimmu.2019.01238
23. Zhao Y. CD26 in autoimmune diseases: The other side of “moonlight protein”. Int Immunopharmacol (2019) 75:105757. doi: 10.1016/j.intimp.2019.105757
24. Sadik CD, Langan EA, Gratz V, Zillikens D, Terheyden P. Checkpoint Inhibition May Trigger the Rare Variant of Anti-LAD-1 IgG-Positive, Anti-BP180 NC16A IgG-Negative Bullous Pemphigoid. Front Immunol (2019) 10:1934. doi: 10.3389/fimmu.2019.01934
25. Hua C, Boussemart L, Mateus C, Routier E, Boutros C, Cazenave H, et al. Association of Vitiligo With Tumor Response in Patients With Metastatic Melanoma Treated With Pembrolizumab. JAMA Dermatol (2016) 152(1):45–51. doi: 10.1001/jamadermatol.2015.2707
26. Sanlorenzo M, Vujic I, Daud A, Algazi A, Gubens M, Luna SA, et al. Pembrolizumab Cutaneous Adverse Events and Their Association With Disease Progression. JAMA Dermatol (2015) 151(11):1206–12. doi: 10.1001/jamadermatol.2015.1916
Keywords: checkpoint inhibitors, autoimmunity, pemphigoid disease, autoantibodies, pembrolizumab, nivolumab, PD-1 - PD-L1 axis, ipilimumab
Citation: Sadik CD, Langan EA, Gutzmer R, Fleischer MI, Loquai C, Reinhardt L, Meier F, Göppner D, Herbst RA, Zillikens D and Terheyden P (2021) Retrospective Analysis of Checkpoint Inhibitor Therapy-Associated Cases of Bullous Pemphigoid From Six German Dermatology Centers. Front. Immunol. 11:588582. doi: 10.3389/fimmu.2020.588582
Received: 29 July 2020; Accepted: 22 December 2020;
Published: 23 February 2021.
Edited by:
Nobuo Kanazawa, Hyogo College of Medicine, JapanReviewed by:
Jun Yamagami, Keio University Hospital, JapanCopyright © 2021 Sadik, Langan, Gutzmer, Fleischer, Loquai, Reinhardt, Meier, Göppner, Herbst, Zillikens and Terheyden. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christian D. Sadik, Q2hyaXN0aWFuLlNhZGlrQHVrc2guZGU=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.