
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Immunol. , 19 October 2020
Sec. Alloimmunity and Transplantation
Volume 11 - 2020 | https://doi.org/10.3389/fimmu.2020.575492
This article is part of the Research Topic Managing Chronic GvHD in the Era of Personalized Medicine View all 8 articles
 Jukka Partanen1*
Jukka Partanen1* Kati Hyvärinen1
Kati Hyvärinen1 Heike Bickeböller2
Heike Bickeböller2 Katarzyna Bogunia-Kubik3
Katarzyna Bogunia-Kubik3 Rachel E. Crossland4
Rachel E. Crossland4 Milena Ivanova5
Milena Ivanova5 Francesca Perutelli4,6
Francesca Perutelli4,6 Ralf Dressel7*
Ralf Dressel7*Chronic graft-versus-host disease (cGvHD) is one of the major complications of allogeneic stem cell transplantation (HSCT). cGvHD is an autoimmune-like disorder affecting multiple organs and involves a dermatological rash, tissue inflammation and fibrosis. The incidence of cGvHD has been reported to be as high as 30% to 60% and there are currently no reliable tools for predicting the occurrence of cGvHD. There is therefore an important unmet clinical need for predictive biomarkers. The present review summarizes the state of the art for genetic variation as a predictive biomarker for cGvHD. We discuss three different modes of action for genetic variation in transplantation: genetic associations, genetic matching, and pharmacogenetics. The results indicate that currently, there are no genetic polymorphisms or genetic tools that can be reliably used as validated biomarkers for predicting cGvHD. A number of recommendations for future studies can be drawn. The majority of studies to date have been under-powered and included too few patients and genetic markers. Like in all complex multifactorial diseases, large collaborative genome-level studies are now needed to achieve reliable and unbiased results. Some of the candidate genes, in particular, CTLA4, HSPE, IL1R1, CCR6, FGFR1OP, and IL10, and some non-HLA variants in the HLA gene region have been replicated to be associated with cGvHD risk in independent studies. These associations should now be confirmed in large well-characterized cohorts with fine mapping. Some patients develop cGvHD despite very extensive immunosuppression and other treatments, indicating that the current therapeutic regimens may not always be effective enough. Hence, more studies on pharmacogenetics are also required. Moreover, all of these studies should be adjusted for diagnostic and clinical features of cGvHD. We conclude that future studies should focus on modern genome-level tools, such as machine learning, polygenic risk scores and genome-wide association study-transcription meta-analyses, instead of focusing on just single variants. The risk of cGvHD may be related to the summary level of immunogenetic differences, or whole genome histocompatibility between each donor-recipient pair. As the number of genome-wide analyses in HSCT is increasing, we are approaching an era where there will be sufficient data to incorporate these approaches in the near future.
Allogeneic hematopoietic stem cell transplantation (HSCT) is a potentially curative treatment for hematological malignancies; up to 400 000 HSCTs have been performed worldwide to date (1). Chronic graft-versus-host disease (cGvHD), together with the acute form of GvHD (aGvHD) and relapse, are major hurdles of successful HSCT. cGvHD is an autoimmune-like disorder affecting multiple organs and involves a rash, tissue inflammation and fibrosis. Despite many advances in HSCT, the incidence of cGvHD has been reported to be between 30-60%. Notably, cGvHD can occur in different forms that likely have important pathophysiological differences. The progressive form develops directly based on an aGvHD, the quiescent form occurs in patients after recovering from aGvHD, while the de novo form is a cGvHD in patients who never had an aGvHD. The symptoms in most cases present within the first year, but may occur up to 3 years after HSCT. The overall incidence of cGvHD may have even increased over time, due to more frequent use of peripheral blood as the stem cell source, or due to reduced intensity conditioning regimens.
A greater likelihood of cGvHD is observed after transplantation from a haploidentical family member, especially from a female donor to her son (2, 3). This may be due to genetic disparities between the mother and her offspring, which can lead to allosensitisation and induce an immune response through antibodies directed against paternal human leukocyte antigens (HLA) and paternal minor histocompatibility antigens (miHA) such as HY-antigens (4). On the other hand, a HLA mismatch in haploidentical settings may be beneficial and facilitate graft-versus-leukemia (GvL) effect.
GvHD, as well as the desired, curative graft-versus-leukemia (GvL) effect, results from immunogenic differences between the donor and recipient. Lack of immunological tolerance by the graft immune cells is a key element. In aGvHD immunological triggers, initiated by microbial structures released from the gut during preconditioning, is a prominent component leading to cytokine storm and activation of cell-mediated immunity against structures detected as foreign by the graft immune cells. The gut along with skin and the liver are key targets of aGvHD. In cGvHD, B cells and an autoimmune-like lack of immunological tolerance are assumed to play central roles. Diagnosis and scoring of cGvHD has been challenging, as it is a heterogeneous disease with pleiotropic symptoms and clinical definitions changed over time. However, the National Institute of Health Consensus Criteria has provided a framework for more defined classification (5).
Genetic disparities between the recipient and donor strongly influence the outcome of HSCT (6). In addition to human leukocyte antigen (HLA) genes, miHAs, and non-HLA polymorphisms may contribute to susceptibility to GvHD, relapse and survival-related outcomes (7–9). The effect of genetic components on GvHD is complex and potentially comprises numerous variants in donor and recipient genomes, related to the initiation and perpetuation of GvHD. To date, the majority of genetic variation studies in the field of GvHD involve selected candidate genes, single nucleotide variants (SNPs) and small study populations (10). The methods employed by the community have rather slowly evolved toward broader approaches, and the first genome-wide association studies (GWASs) on GvHD were published by Sato-Otsubo et al. (11) and Bari et al. (12) in 2015. The absence of variants having large effect sizes, combined with the low and unbalanced case/control numbers, introduces another challenge to overcome. The success of genetic association studies depends on adequate statistical power and detecting causal variants of complex diseases requires thousands of cases and controls (13). Currently, we are not reliably able to predict the risk of developing cGvHD. There is therefore a clear unmet clinical need for predictive biomarkers that could be used prior to HSCT for risk assessment. Biomarkers can also provide us with valuable insight into the key pathogenic pathways and molecules implicated in cGvHD. The present paper reviews the current findings of using genetic variation in the patient and donor for predicting the occurrence of cGvHD. Genetic variation can influence the risk for cGvHD in at least three mutually non-exclusive ways (Table 1).
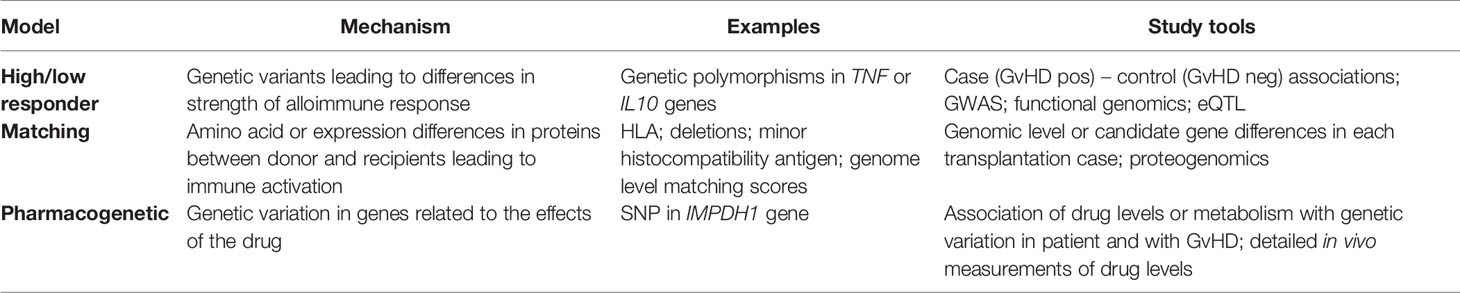
Table 1 Three non-exclusive genetic concepts or models in genetic susceptibility to graft-versus-host disease after allogeneic stem cell transplantation.
I. First, the patient or donor may have genetic variants that regulate the threshold or power of the immune response against foreign molecules. An individual can be a high or low responder as a result of having particular gene variants or an overall genomic profile producing e.g. higher or lower levels of regulatory cytokines, such as interleukin (IL)-10 or tumor necrosis factor (TNF)-α.
II. The second level of genetic variation is related to the level of histocompatibility or “matching” between the donor and recipient. The HLA-matching is the central component, but matching of known miHAs as well as the sum score of antigenic differences may also be related to cGvHD risk. Indeed, any amino acid difference in proteins between the donor and recipient may be recognized by the immune system as foreign, if presented by the major histocompatibility complex (MHC) class I molecules to CD8+ T cells, leading to killing of the cells expressing the protein. Recognizing foreign peptides presented by MHC class II molecules may also lead to the activation of CD4+ T cells.
III. Finally, genetic variation may affect cGvHD risk by pharmacogenetic differences. It should be noted that despite all modern immunosuppression and other treatments, a substantial proportion of HSCTs still results in GvHD. Genetic variants can regulate, for example, the distribution or efficacy of immunosuppressive drugs used in HSCT.
In the present review, we systematically screened published articles related to genetic associations with cGvHD and classified them into these three genetic models (Table 1).
Compared to quantitative biomarkers, such as protein or mRNA levels, determination of genetic variation is technically relatively simple and reliable. As the HLA-matching is anyway performed based on DNA technology, such as sequencing, determination of additional genetic variation for more reliably predicting the outcome of HSCT could be feasible in clinical practice. However, as for any biomarker, candidate genetic markers should be validated in independent series of HSCT studies with sufficient numbers of well-characterized cases. In addition, prospective studies on their specificity and sensitivity should be carried out. Currently, there is no genetic variation, barring HLA-matching, that could fulfill the criteria for a validated biomarker, or that could be in more general clinical use to predict cGvHD, aGvHD or relapse. However, there are substantial advances taking place with candidate gene approaches, GWASs and more sophisticated approaches related to genome level histocompatibility or using kernels such as polygenic risk scores (PRS) for HSCT. In the genome era of today, the value of screening a small number of candidate polymorphisms seems low, although it may be justified if functionally relevant variants are identified that are expected to affect the outcome of HSCT. However, without genome level analysis even positive findings may merely reflect linkage disequilibrium, as opposed to genuine causative variation.
Machine learning for genomic data and the integration of genomic data with other omics data are a highly active area of statistical and bioinformatic research in the field of complex diseases, either for modeling, i.e. understanding the disease, or for prediction. Gene-set analyses might be particularly important. Here, the association of a whole SNP set with an outcome (14) is tested, thus reducing high dimensionality and allowing for biological insights. Selecting genes, pathways or regions for such tests yields possible post-GWAS analyses, even with current available sample sizes. For many complex diseases, e.g. psychosis, the implication of immunological pathways have been shown this way (15). Machine learning tools, such as kernel methods, analyze which part of the variation in the outcome can be explained globally by a non-parametric unknown function, based on the SNP set after adjusting for other variables, e.g. clinical variables, possibly in the usual parametric way. The function does not need to be specified directly, but its impact on variation can be tested via the so-called kernel which measures similarity between individuals (16).
The PRS as an additive sum is a particular, extremely simple kernel which is computationally fast. However, there are much more sophisticated kernels available which, e.g. allow for interactions within pathways (17). It should be noted that the similarity kernel above describes the similarity or dissimilarity between two patients, e.g. with respect to their PRS, and not the similarity between the recipient-donor pair. Thus, for cGvHD this additional similarity needs to be integrated into the model as well. Machine learning tools such as boosting or shrinkage can be used in order to extract the most important features. If features are defined by gene-sets, boosting might be combined with kernel approaches, as in Friedrich et al. (18) for rheumatoid arthritis, which is heavily influenced by the HLA locus. This overwhelming effect might make it challenging to detect other signals without the use of selection approaches that take this into account – similar to the approach needed in cGvHD. In addition to these purely genomic analyses, genomic data might be integrated with other omics data, either by enrichment with external information, such as the gene-expression data base (gtex), or when other omics data are available for the same patients and donors. For the latter, several kernels might be combined in one analysis, thus e.g. assessing similarity on the genomic as well as the transcriptomic level. Most of the research on a consolidated modeling approach has been performed on GWAS-transcription analysis, however, these are quickly extended to other omics data. For prediction, feature selection on several omics levels is computationally more feasible. However, validation is the key issue for the development of prediction tools for all complex diseases, as for cGvHD or outcome of HSCT in general. Due to the pairing of recipient and donor, the dimensionality regarding several omics level is increased, so that feature selection is expected to have a larger influence in HSCT. Some of the mentioned approaches may also need extensions in order to deal with the competing risks in HSCT. The number of GWAS of HSCT is increasing, but the globally available number of recipient-donor pairs to study is clearly lower than many other diseases. Thus, these new methods using dimensionality reduction and the increasing number of available GWASs enable the use of the modern approaches for these patients.
There is an excellent paper by Martin et al. (11), who searched for SNPs reported to be associated with cGvHD prior to August 2014, and then tested which SNPs could be replicated in two independent cohorts of HSCT. The two cohorts had sufficient numbers of cases, 4000 and 3200 cases, for meaningful conclusions to be drawn. The original studies had substantially lower cohort numbers of HSCTs, and were mostly based on very limited candidate gene approaches in retrospective materials.
Martin and co-workers performed a PubMed search using the terms “chronic GvHD” and “polymorphisms” and identified 29 candidate SNPs potentially associated with cGvHD. Only 5 of the 21 SNPs tested, those located near or in the CTLA4, HSPE, IL1R1, CCR6, and FGFR1OP genes, could be replicated in a study setting identical to that described in the original report. As the study by Martin et al. included large cohorts, these five genes, may be regarded as promising genetic biomarkers for cGvHD. However, the few GWAS analyses on GvHD conducted to date, although mostly focussed on aGvHD, have not found supporting evidence for any of these five genes (11, 12, 19). Larger GWAS studies are clearly needed to resolve the discrepancy.
To identify more recent studies we performed a PubMed search identical to that of Martin et al. (20) but focussing on post-August 2014 and identified 7 papers regarded as relevant to the present review. The associations are summarized in Table 2; it is of note that the majority of new studies did not focus on the markers that were confirmed by Martin et al. (20). Supporting evidence for IL1R1 was reported by Kim et al., 2014 (27). On the other hand, no support for IL1R or CTLA4 genes was identified by Hyvärinen et al. (23). Two new studies (21, 22) both report association of IFNG with cGvHD, but no evidence for this locus was found by Hyvärinen et al. (23). The majority of studies have reported or focused on a small number of candidate loci or SNPs, and it is not clear whether negative findings were reported.
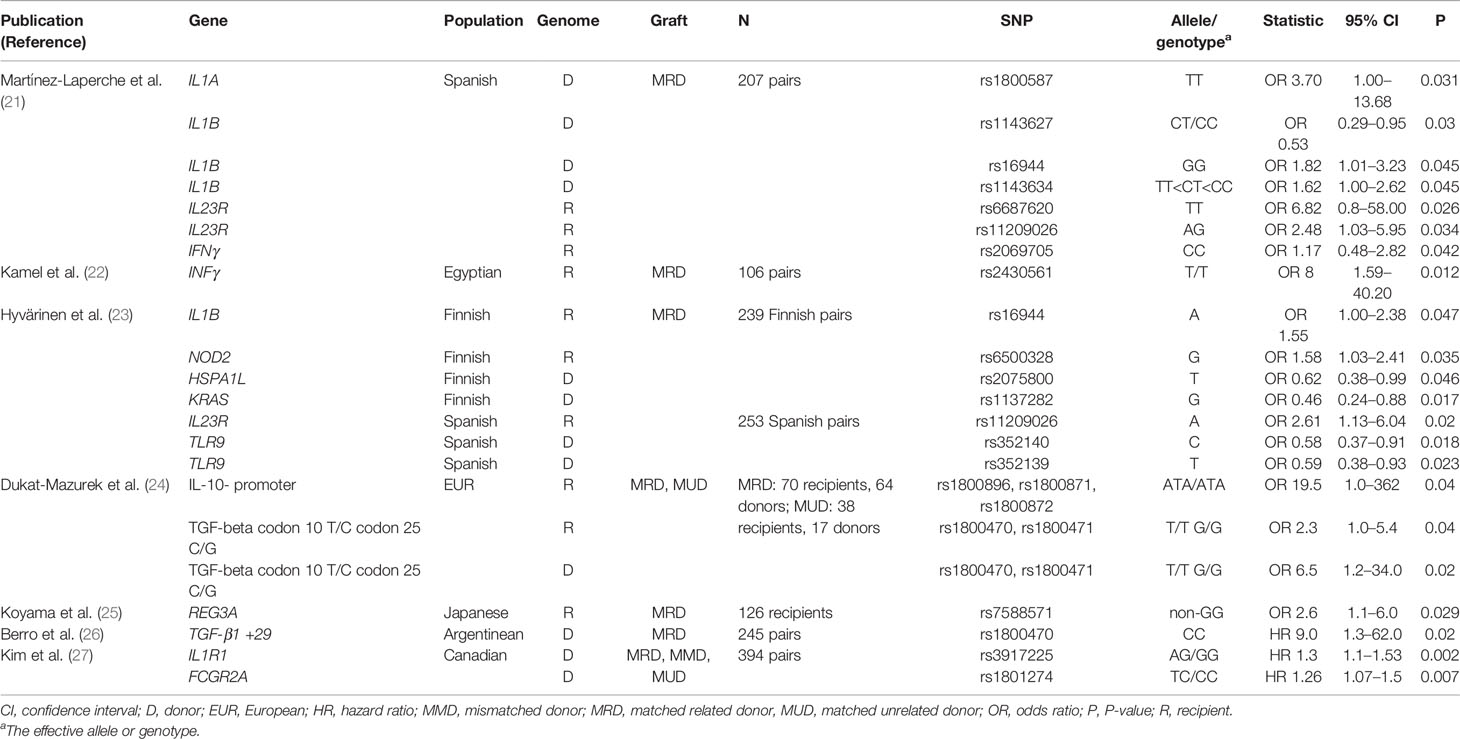
Table 2 Results of PubMed search using the same terms as Martin et al., i.e., “chronic GVHD” and “polymorphisms,” only publications appearing after August 2014 have been listed.
We also performed a broader literature search in the PubMed database, using the terms: “chronic”, “chronic GvHD”, “graft”, “host”, “biomarker”, “gene”, “SNP”, “polymorphism”, “non-HLA”, “genetic risk” and “genetic variant”, and starting from year 2000 to February 2019, in order to identify any additional studies that were previously overlooked (Supplementary Figure 1). In total, we found 674 papers of which 50 were regarded as relevant to the present review. We excluded reviews, seminar papers, acute GvHD only papers, non-genetic papers, papers that analyzed pediatrics only and those that reported poor statistical evidence (p > 0.05). When we further eliminated those already identified in Table 2, 20 additional publications remained. Their findings have been summarized in Table 3. Briefly, there were in total 21 different loci suggested to show association with cGvHD but of these, only recipient IL6 rs1800795 SNP was replicated in at least one additional independent population (42, 44–46).
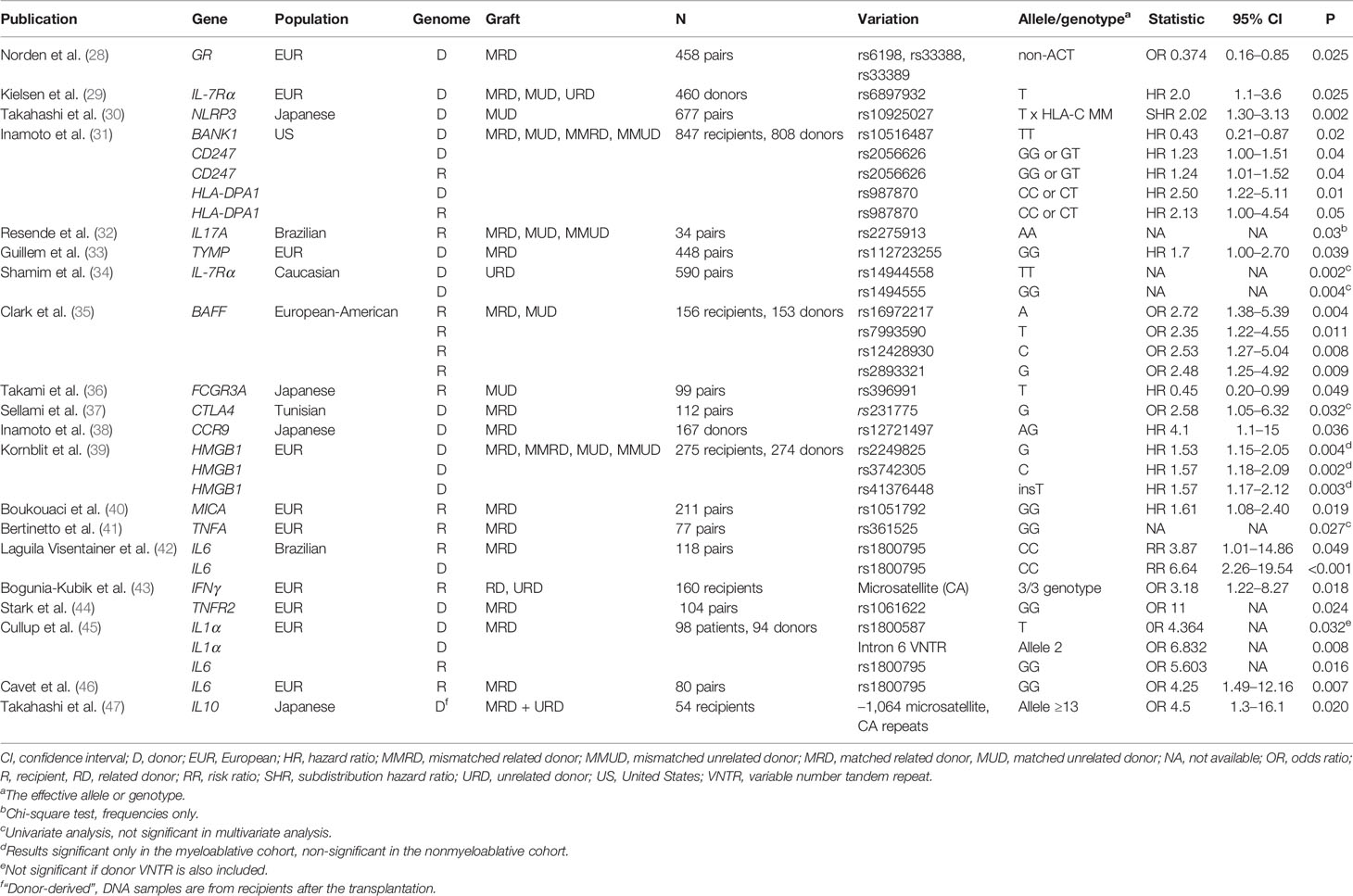
Table 3 20 publications found in addition to those of Table 2, using broader PubMed search terms (Supplementary Figure 1). Only those found relevant to the present chronic GvHD review have been listed.
Based on this analysis, it is clear that there are currently no adequately-proved single genetic biomarkers for cGvHD. It also became apparent that we should no longer focus on just a small number of candidate genes or SNPs in small study populations. Sato-Otsubo et al. (11), Bari et al. (12), Goyal et al. (19) and Hyvärinen et al. (23) have published GWASs on GvHD, however, the results are diverse and have no major focus on the chronic form of GvHD. Hence, larger collaborative GWAS are needed. Another fruitful approach would be to study the entire linkage disequilibrium blocks covering each of the best candidate genes as a whole, considering all markers, genotyped on an array or imputed, in order to elucidate whether the suggested associations remain valid and to identify the primary-associated variation.
The standard candidate gene or SNP approach, as well as GWAS, essentially look for associations of a single gene variant or polymorphism with the trait in question. For example the occurrence of cGvHD after allo-HSCT. Studies on other complex traits have strongly indicated that it is very rare to find a single locus with a strong effect, rather, a high number of common variants each with a small effect as well as a considerable number of rare variants can be assumed. In immunological diseases, the role of HLA variation as a susceptibility factor seems to be the only example of a strong single gene or locus effect (48), whereas the effect sizes of all other susceptibility loci are individually very small. Recent evidence by Khera et al. (49) suggests that it is possible to utilize GWAS data so that once a sufficient number of cases have been analyzed, genome-wide polygenic risk scores (PRSs) can be calculated based on associated markers. The PRS for one outcome is an additive sum of many SNPs, with the lowest p-values in a large GWAS weighted according to their effect size. In a (possibly much) smaller secondary study, interest may lie in how much variation this PRS explains or how well it predicts the same or a related outcome, e.g. identifying magnitude of risk for individuals and thus identifying low, medium, and high risk categories, Khera et al. (49) could identify highest risk individuals, such as for coronary artery disease (CAD), with surprisingly good accuracy by improving standard PRS construction with a Bayesian approach and subsequent shrinkage based on local linkage disequilibrium. In this study the number cases for CAD was >60.000 and the number of controls even higher. There have been no attempts to test PRS for GvHD so far, as crucial GWAS data for PRS construction are missing, but in the future, building of larger consortia, improvements on PRS construction as well as GWAS data on the related autoimmune diseases as primary GWAS may enable this approach as a powerful novel tool to real life practice.
There are some recent interesting attempts toward using a PRS-type of summary effect of associated markers, as well as more sophisticated data analysis methods to create genetic summary risk scores for GvHD. Martinez-Laperche and co-workers (21) built a predictive model based on clinical variables and genetic variation in a set of cytokine genes. The authors analyzed the data using a linear regression model and Lasso approach in 509 HSCTs. The risk scores, albeit not actual PRSs, could identify both severe acute GvHD and extensive cGvHD with good accuracy. The area under the curve in the receiver operating characteristic analysis of the model combining both the clinical and genetic data was 0.8 for extensive cGvHD. Secondly, Ritari et al. utilized machine learning tools to genome-wide polymorphism data to predict for complications of HSCT and reported promising results for predicting relapse (7). For cGvHD, the approach gave more modest results. Finally, Balavarca and co-workers (50) refined the EBMT clinical risk score for survival prediction by adding results of polymorphisms in the MyD88-adapter like, estrogen receptor, IL-10 and IL-6 genes in a cohort of 762 HSCT from 7 European transplantation centers.
There is evidence for an increased risk of cGvHD in patients having an HLA-matched unrelated donor, compared to those with an HLA-identical sibling donor (51, 52). As the determination of HLA alleles can be assumed to be reliable using today’s DNA-based methods, this risk may not therefore derive from hidden allelic differences in unrelated HSCTs. Rather, it could indicate that the MHC region contains alleles or polymorphism associated with cGvHD, in addition to the established role of HLA allele matching in GvHD risk. It is also likely that the higher overall genomic difference between unrelated individuals, as compared to siblings, can explain the higher risk for cGvHD as we later discuss.
The HLA or MHC gene segment is one of the densest genomic regions and encompasses at least 269 genes in ~3.8 Mbp of DNA (53, 54). It is associated with more than 100 diseases (48, 53), but not all of these associations are directly caused by variants of classical HLA class I or II genes, given the linkage disequilibrium within this region and the unexpectedly high polymorphic diversity of other genes encoded in the MHC complex (55). Therefore, MHC-linked, non-HLA genetic variation is an interesting focus area for GvHD-related risk markers. Petersdorf and co-workers screened over 1000 MHC-region SNPs for their role in HSCT-related complications in a total of over 5000 HSCTs (56, 57). Genetic associations between MHC-linked SNPs were found for e.g. mortality, relapse and acute GvHD, but for cGvHD only a matching effect could be seen (see section “Histocompatibility or matching of genetic variation as predictive biomarker for cGvHD”). In the GWAS performed on Finnish and Spanish allo-HSCT, including over 5000 SNPs in the MHC region, no evidence for genetic association between cGvHD and MHC-linked SNPs was found at the genome-wide level (58). Based on these studies and that of Ritari et al. (59) it is likely that the genetic risk to cGvHD may be more related to overall genomic matching, as opposed to associations with single markers.
However, a number of candidate gene approaches indicate that the MHC segment may contain some gene variation associated with cGvHD and we discuss the most promising of these below. In the case of TNFA and the MHC class I chain-related molecules A gene (MICA), we have some understanding of possible mechanisms underlying the association with cGvHD. In our literature search, we identified seven retrospective studies describing an association between MHC-linked non-HLA variants and cGvHD (21, 23, 40, 41, 60, 61). Four of these studies report associations between TNFA variation with cGvHD (21, 41, 60, 61), one reports an association with MICA (40), and another indicates an association with the heat shock protein family A (HSP70) member 1 like gene (HSPA1L) (23). As the MHC segment has a strong linkage disequilibrium (LD), it is very difficult to pinpoint the genuine causative gene for the associations and we cannot rule out that some, or even all, of these findings stem from a single variant. It is also possible that the genes have combinatorial effects.
Mullighan and colleagues studied 22 polymorphisms in 11 candidate genes in a cohort of 160 patients undergoing HSCT, based in three Australian transplant centers between 1991 and 1998 (60). 154 patients had sibling donors and 6 received grafts from other relatives. Of three SNPs in the TNFA gene that were analyzed (+488, -238, and -308), the TNFA +488 A allele in recipients showed association with an increased risk of cGvHD (odds ratio [OR] 12.5, 95% confidence interval [CI] 1.6–99.3, P = 0.003). Unfortunately only a univariate analysis was performed, leaving the genuine value of the result unknown (60).
A single center study from Italy evaluated 15 non-HLA, MHC-linked polymorphisms including seven SNPs in the TNFA gene (-863, rs1800896; -857, rs1799724; -574, -376, rs1800750; -308, rs1800629; -244, rs673; -238, rs361525) in a cohort of only 77 patients transplanted with grafts from HLA-identical sibling donors (41). Presence of the TNFA -238 A allele was found to be associated with a lower risk of cGvHD (P = 0.0027).
In a cohort from a single center in Brazil, including 122 patients transplanted between 1996 and 2006 with grafts from HLA-identical siblings, one candidate SNP in the TNFA gene and 2 IL2 SNPs were analyzed (61). The GA genotype of recipients in the TNFA -238 SNP was found to be associated with increased incidence (risk ratio [RR] 2.04, 95% CI 1.04–4.04, P = 0.0039) and severity (RR 2.59, 95% CI 1.29–5.19, P = 0.0074) of cGvHD.
A more recent study by Martinez-Laperche et al. (21), analyzed 25 candidate SNPs in 12 genes encoding cytokines in a cohort of 509 Spanish patients who received HLA-identical sibling allo-HSCT. Four SNPs in the TNFA gene were studied: rs1800629 (-308), rs1800610, rs361525 (-238), and rs1799964 (-1031). None of them were associated with cGvHD in the initial univariate analysis, however, all were included in the prediction model for occurrence of cGvHD (see above).
The three first TNFA studies above were disadvantaged by a small number of patients and a univariate approach. As they furthermore report contradictory results, the validity of these findings remain open. In particular, systematic studies (21, 23, 62) with larger cohorts and marker sets failed to find associations of TNFA polymorphisms with cGvHD. Nonetheless, among the non-HLA candidate genes that have been evaluated for association with aGvHD, TNFA SNPs are among the few that have shown some consistency in their associations with outcome in different settings of HSCT. The linkage disequilibrium of the TNFA polymorphisms with HLA-haplotypes leaves room for effects by other genes. Since occurrence of aGvHD is one of the most important clinical risk factors for cGvHD, it is possible that TNFA polymorphisms secondarily affect the risk of cGvHD by modulating the risk of aGvHD, by controlling TNF-α levels during the cytokine storm following HSCT. However, an association of functionally relevant TNFA gene variants with the outcome of HSCT could be biologically plausible. Increased serum levels of TNF-α after HSCT have been associated with an increased risk or increased severity of cGvHD in several, albeit not all, reported studies as reviewed recently by others (63). The rs1799964 (-1031), rs1800629 (-308), and rs361525 (−238) SNPs in the promoter of TNFA have been described in multiple studies (64–75) to affect the expression level of this cytokine, suggesting a potential mechanism by which these SNPs could modulate the risk of cGvHD.
MICA is the most polymorphic non-classical HLA class I-like gene (http://www.ebi.ac.uk/imgt/hla/). MICA is constitutively expressed in only a few tissues, such as gastrointestinal epithelium (76), but it can be induced by cellular or genotoxic stress (76–78). MICA is a ligand for the activating receptor NKG2D, expressed by most natural killer (NK) cells and CD8+ T cells (79). Proteolytic shedding can generate soluble MICA (sMICA), which can induce NKG2D down-regulation resulting in impairment of both NK cell cytotoxicity and activation of CD8+ T cells (79).
SNP rs1051792 at nucleotide position 454 (G/A) of MICA causes a valine (Val) to methionine (Met) exchange at amino acid position 129, which separates MICA alleles into two groups. MICA variants containing a methionine at position 129 bind NKG2D with high affinity, whereas those with a valine bind with low affinity (80, 81). The potential importance of this variation is highlighted by numerous disease associations including GvHD (81) that have been reported for this SNP (82).
Boukouaci and colleagues studied the MICA-129 SNP in a cohort of 211 patients who underwent non-T cell-depleted HSCT between 1994 and 2002 in a single center in France (40). In a multivariate analysis, the recipient MICA-129Val/Val genotype was associated with an increased risk of cGvHD (hazard ratio [HR] 1.61, 95% CI 1.08–2.40, P = 0.019). Other independent risk factors for cGvHD were aGvHD, older age and peripheral blood as the source of stem cells. Notably, the MICA-129Met/Met genotype in patients was associated with an increased risk of relapse (HR 1.91, 95% CI 1.02–3.58, P = 0.04). Moreover, elevated levels of sMICA in sera of patients post transplantation were associated with an increased incidence of cGvHD, whereas the presence of anti-MICA antibodies conferred protection against cGvHD. However, it needs to be mentioned that another recent study from the USA including 552 patients with unrelated donors failed to show any association between the MICA-129 SNP in patients and the outcome of HSCT (83).
The association of high-affinity MICA-129Met variants with an increased risk of relapse and low avidity MICA-129Val variants with an increased risk of cGvHD (40) appears to be counterintuitive, but it might be biologically feasible. Functional studies (81) revealed that the MICA-129Met isoform triggers increased NK cell cytotoxicity and IFN-γ release than the MICA-129Val isoform. Similarly, the MICA-129Met isoform induced an earlier co-stimulatory activation of CD8+ T cells than the MICA-129Val isoform. However, when the expression intensity of MICA is taken into consideration, the biological effects of this SNP can change. The extent of functional responses of NK cells and CD8+ T cells were found to correlate closely with the MICA expression intensity only for the MICA-129Val isoform. Increasing the expression of the MICA-129Met isoform, in contrast, had either none or even negative effects on the activation of NK and CD8+ T cells. This is most likely because high affinity MICA-129Met ligands induced a faster and stronger down-regulation of NKG2D than MICA-129Val ligands. The down-regulation of NKG2D impairs then the capability of NK and CD8+ T cells to receive signals via NKG2D. Thus, MICA-129Met ligands elicit strong NKG2D responses but stimulate in parallel a robust negative feedback signal. Extensive down-regulation of NKG2D appears to limit the initially stronger effects of MICA-129Met ligands. Carriers of the MICA-129Val/Val genotype might therefore be less able to limit the activation of alloreactive CD8+ T cells, resulting in an increased risk of cGvHD. Carriers of the MICA-129Met/Met genotype, on the other hand, might have lower CD8+ T and NK cell responses against malignant cells resulting in an increased risk of relapse. Recently, a well-powered study indicated that patients having a donor carrying MICA-129Met have a lower risk of grade 3 and 4 aGvHD and non-relapse mortality (84). However, the high relation of donor and recipient MICA genotypes is a challenge for ascribing the effects to donor or patient genotypes.
The SNP MICA-129 is an instructive example of how complex the functional consequences of even a single polymorphism can become when taking into consideration the effects on different cells, effects depending on expression intensity, and effects depending on the timing of expression. Notably, the SNP itself also appears to affect MICA expression. The MICA-129Met isoform was found to be retained longer in intracellular compartments and when transported to the cell surface, it was more prone to shedding than the MICA-129Val isoform (85). Both processes could limit expression of the high affinity MICA-129Met isoform at the cell surface. Effects of sMICA and occurrence of anti-MICA antibodies obviously further complicate the situation (40).
HSPA1L (HSP70-HOM) is another non-HLA MHC-linked gene that has recently been associated with cGvHD (23). Hyvärinen and colleagues analyzed 122 SNPs that have been previously described as GvHD-associated in two cohorts receiving grafts from HLA-matched siblings, in Finland (n = 301) and in Spain (n = 264). In the Finnish cohort, the donor T allele of SNP rs2075800 in the HSPA1L (HSP70-HOM) gene was found to be associated with protection from cGvHD (OR 0.62, 95% CI 0.38–0.99, P = 0.046). SNP rs2075800, which leads to a Glu-Lys amino acid change at position 602 of the protein, has been studied previously for an association with aGvHD in Poland (86) and the UK (87). The most convincing evidence for the role of HSPA1L in HSCT comes from Petersdorf et al., who reported in their screen of over 5000 allo-HSCT a protective effect against aGvHD for the rs2075800 AA and AG genotypes, both with the hazard ratio of ~0.7 (62).
HSPA1L is one of three HSP70 genes encoded in the MHC class III region (88). The other two genes HSPA1A (HSP70-1) and HSPA1B (HSP70-2) encode an identical protein, i.e. the major heat-stress inducible HSP70. The heat stress-inducible HSP70 is a molecular chaperone (89) that has in addition to its functions in protein folding, manifold effects in the immune response (90, 91). However, HSPA1L is constitutively expressed at a reasonable level only in the testis and is not heat-stress inducible (92), arguing against direct involvement in GvHD. The three orthologous genes in the rat and mouse MHC show the same expression pattern. Hyvärinen and colleagues reported results from the blood expression quantitative trait loci (eQTL) database (93), showing that the protective donor rs2075800 minor allele T was associated with increased expression of HSPA1A and HSPA1B (23). It is of note that the coding sequence of HSPA1A is within the HSPA1L gene, but in the opposite strand, and the HSPA1L gene is located very closely to the HSPA1B gene. Again, these results cannot pinpoint the variation primarily associated with GvHD.
A direct involvement of the stress-inducible HSP70 in the pathophysiology of GvHD is more plausible than a role for the testis-specific HSP70 isoform. In rat models, expression of HSP70 was induced in spleen and lymph nodes during aGvHD (94) and anti-HSP70 antibodies were found in the serum (95). Anti-HSP70 antibodies were also reported to occur in the serum of patients with aGvHD (96). Moreover,upregulation of HSP70 during an acute GvH reaction has been observed in human skin explant assays, in which recipient skin is co-cultured with donor lymphocytes (97). In rat skin explant assays, mRNA expression of the stress-inducible Hspa1a and Hspa1b genes, but not the Hspa1l gene, correlated with the grade (I to IV) of the acute GvH reaction (98). In human skin biopsies, HSPA1L mRNA expression was lower in patients with severe aGvHD (grades II–III) when compared to those with no or low grade aGvHD (grades 0–I) and normal controls (99). In blood, however, it was upregulated in patients with cGvHD and HSPA1B mRNA expression was also higher in patients with both aGvHD and cGvHD (99). The HSP70 protein, in contrast, was not found in the serum of patients with aGvHD (100). Notably, the inhibition of HSP70 has been recently suggested as a new treatment option for aGvHD. Inhibition of HSP70 appears to decrease the number of intermediate monocytes, which are major producers of pro-inflammatory cytokines during aGvHD (101).
The non-HLA genes in the MHC segment are of great interest for the pathophysiology of cGvHD, because many of the 160+ protein coding genes in this region are directly involved in the immune response (48, 53). However, the linkage disequilibrium with the classical HLA class I and class II genes and other variation in the MHC makes it very challenging to identify causative variants in the MHC region. In HLA-identical sibling transplantations, all MHC genes are assumed to be matched between patients and donors, whereas this is not the case in HLA-matched unrelated donor transplants, adding a further layer of complexity to association studies. Three genes in this region, TNFA, MICA, and HSPA1L have been associated with cGvHD in one or more candidate gene studies. While it is biologically plausible that the associated SNPs have direct effects on cGvHD, via modulating expression of the pro-inflammatory cytokine TNF-α, or the affinity of MICA to the activating NK receptor NKG2D, it is more likely that that the SNP in HSPA1L acts indirectly, e.g. via modulating expression of the neighboring stress-inducible HSP70 genes. SNPs in TNFA, MICA, and HSPA1L have also been associated with the risk of aGvHD. While this further increases the plausibility for involvement of these genes in the pathophysiology of GvHD, it could alternatively suggest that associations with cGvHD are mainly secondary, since occurrence of aGvHD is a strong risk factor for cGvHD. However, some studies, e.g. on the association of MICA-129 with cGvHD (40), adjusted for this effect in the analysis. Larger collaborative and preferably prospective unbiased studies are clearly needed to confirm or reject MHC-linked risk factors for cGvHD. Experimental data on functional consequences of the genetic variants might help to understand why outcome associations after HSCT are variable in different cohorts (81) and provide information on the specific circumstances under with genetic information could be important to guide clinical decisions.
Compared to genetic analyses of other multifactorial traits or diseases, transplantation has a special feature related to the fact that the outcome of transplantation is a summary of two individuals, usually affected by the level of immunogenetic donor-recipient matching. Studies therefore require analysis of both donors and recipients and their combinatory effect. Matching of alleles of classical HLA genes is the golden standard in many transplantations, the exact rules depending on the organ or cells transplanted. It should be noted, however, that haploidentical HSCTs, i.e. those with only one of the HLA haplotypes matched between donor and recipient, are becoming more common. How these change the role of non-HLA matching or associations of other genes is currently unknown. In HSCT, at least three levels of donor-recipient matching can be identified:
1. Matching of HLA alleles, and established testing performed prior to HSCT;
2. Matching of established miHAs known to elicit T-cell response;
3. Matching of other genomic variation, including the killer-cell immunoglobulin-like receptor (KIR) and deletion matching, and whole genome level matching
The MHC region spans approximately 3.8 Mb of the short arm of chromosome 6 at 6p21.3 and includes more than 269 genes (48, 53, 54). Among them are the classical HLA class I (HLA-A, -B, -C) and class II (-DR, -DQ, and -DP) genes as well as non-classical histocompatibility genes coding for e.g. HLA-E, HLA-G or MICA molecules. In addition, the MHC complex harbors a number of genes with immunological functions (48), making it an immunological ‘superlocus’ of utmost interest.
While mismatching classical HLA alleles is a strong risk factor for the development of aGvHD, it appears to have only a limited effect on the risk of cGvHD (102, 103). In a large international study, less than an 8/8 match in the HLA-A, -B, -C, and -DRB1 loci was not associated with an increased risk of cGvHD (102). In a similarly large cohort from Japan by Morishima et al. (104), who studied 7898 unrelated T-cell replete HSCT, only mismatching of HLA-C was found to be associated with an increased risk of cGvHD (103). The authors pointed out the significance of potential differences between donor and recipients in the NK-cell receptor repertoire that should also be considered while studying the effect of HLA-C mismatching. Therefore, further analysis of HLA-C mismatches and KIR ligand/receptor combinations should help to elucidate the mechanism of HLA-C and KIR-related immunologic reactions and their effect on transplant outcome. Arrieta-Bolaños et al. in an in silico study showed association of HLA-DPB1 mismatches with cGvHD (105).
There is increasing evidence that not all allelic differences in classical HLA genes are equal, but some may be permissive. This topic has recently been reviewed by e.g. Fleischhauer and Shaw (106) and will not be summarized further here. A novel view on HLA-matching has emerged from studies on expression differences between HLA alleles. Differences in surface expression of HLA molecules have been associated with SNPs located in the 5’ or 3’ untranslated regions (UTRs) of the genes. These effects have been documented at least for HLA-A (107, 108), HLA-C (109, 110), and HLA-DP (111, 112). For HLA-C, for example, it has been shown that a SNP in the 3’ UTR abrogates the binding of hsa-miR-148 microRNA, which allows HLA-C alleles with this SNP to escape from post-translational control, resulting in a higher cell surface expression (113). The expression model is based on the assumption that alloreactive donor T cells could more efficiently recognize patient-specific HLA alleles with high levels of cell surface expression than those with low levels.
Petersdorf et al. (110) examined the role of HLA-C expression levels in HLA-C-mismatched HSCT. They found that the expression levels were associated with unfavorable outcome. However, no relationship with cGvHD incidence was found. Furthermore, expression differences in HLA-DP molecules, due to rs9277534 SNP (496A/G) variation in 3’ UTR of the gene, were analyzed in relation to GvHD by Petersdorf et al. (112). This polymorphism was not only associated with HLA-DPB1 expression, but was also reported to be associated with an increased risk of aGvHD. No association with cGvHD was reported. In summary, it is currently unclear whether expression differences between HLA alleles play a significant role in cGvHD susceptibility.
At least 20 mHAs have been identified to date (9). Their identification is based on studies showing immunogenetic differences in mHA-encoding genes between allo-HSCT pairs, leading to a T-cell alloresponse against the difference. The role of matching mHA in GVHD susceptibility in general is not clear, as concluded in a large collaborative study by Spierings et al. in 2013 (9). However, mismatching of mHAs may be useful for directing GvL effect toward e.g. cells of hematopoietic origin (114, 115). The mHAs identified so far can be regarded as special cases of concept of whole genome histocompatibility, encompassing all immunogenic amino acid differences between allo-HSCT pairs, as discussed in the next sub-chapter.
Genome-wide histocompatibility concept is based on the idea that any SNP that changes an amino acid sequence can be regarded as a potential minor histocompatibility antigen, leading to a GvH reaction if mismatched in a donor/patient pair and presented to the immune system by HLA molecules of antigen presenting cells. Hence, instead of studying only the known minor antigens, it can be hypothesized that in HLA-identical cases where the effect of HLA-mismatch is removed, the risk of GvHD could increase along with the increase in exonic, nonsynonymous SNP differences within each donor/patient pair. In a more refined model, the fact that a particular HLA allele preferentially binds and presents to the immune system at only certain preferred peptides (peptide-binding motifs), can be taken into account by predicting in silico which amino acid changes can be assumed to be relevant in each donor/patient pair. Tissue expression can also be included. It is possible, therefore, to test whether the occurrence of GvHD is associated with the overall level of mismatches in the exomes and in particular, with those differences that are immunologically relevant, i.e., peptides able to bind the patient/donor HLA molecules and peptides expressed in relevant tissues. Ritari et al. (59) estimated, based on exome sequencing of HSCT pairs, that each pair differed on average by 28 000 nine-mer peptides. They were all theoretically, but most likely not all in practice, able to elicit an alloimmune response. The result indicates a high number of potential protein-level mismatches in each transplantation.
We have identified three different types of approaches addressing general, non-HLA-matching:
1. Matching non-HLA MHC-linked variation
2. Matching candidate genes, including effect of deletion mismatching
3. Whole genome matching
As the MHC complex includes a high number of genes many with immunological functions, and as many autoimmune diseases show associations with MHC, it is possible to assume that the effect of MHC in transplantation may be more complex than merely the classical HLA matching. A small number of recent studies support this hypothesis; however, many of these studies are restricted by a very limited number of variants studied. Due to strong LD in MHC, it is impossible to obtain reliable results by focusing on only a few SNPs, instead more systematic screening is required.
Petersdorf et al. (62) screened over 1000 SNPs located in the MHC for their role in HSCT. They tested the hypothesis that clinical outcome of HSCT depends on the cumulative effects of MHC-linked SNP mismatching. Twelve SNPs were found to be significantly associated with the outcome of HLA-matched unrelated HSCT. The risks associated with these SNPs were significant in a multiple regression analysis and were conferred by either donor or recipient SNP genotype or by donor-recipient SNP mismatch. Patient-donor mismatching at rs2523957, located 26.6 kb centromeric to HLA-A, rs2071479 located within the intron of HLA-DOB, and rs3830076, located 240 bp telomeric to FKBPL, were found to be independent risk factors for cGvHD, regardless of grades III–IV aGvHD. Thus, the authors concluded that prospective patient-donor matching for these three SNPs may help to lower the risk of cGvHD that occurs independently of aGvHD symptoms. It is of interest that the three MHC-linked SNPs are located quite far from each other, suggesting e.g. haplotypic differences or multiple factors.
In the same study, Petersdorf et al. analyzed whether patient-donor HLA-mismatches were associated with specific SNPs. Polymorphism in SNP rs3830076, located 240 bp telomeric to FKBPL, differed along with the two most frequent HLA-C-mismatches, C*03:03 vs. C*03:04 and C*01:02 vs. C*02:02. In patients with chronic GvHD, 58.8% of C*03:03/03:04 mismatches had a protective rs3830076 variant, in contrast to 26.1% of C*01:02/02:02 mismatches. These observations suggest that C*03:03 vs. C*03:04 mismatch might be more readily tolerated. This type of information could be further used to select HLA-mismatched donors, which are less likely to result in cGvHD after transplantation.
A similar approach was conducted by Nowak et al. (116), who hypothesized that the increased risk of post-transplant complications might be dependent on disparity in non-routinely-tested polymorphisms in the MHC region, being organized in combinations of two extended MHC haplotypes. They tested the hypothesis that clinical outcome in unrelated HSCT with a certain level of HLA-mismatch is affected by the level of HLA-inferred extended MHC haplotype disparity. In their study, the overall incidence of cGvHD and extended cGvHD were found to be significantly affected by haplotypic disparity level and remained independent prognostic factors in a multiple regression analysis, in which HLA-mismatch levels were excluded from models.
Due to recombination hotspots that are located in the MHC segment, in particular between the HLA-DQB1 and -DPB1 genes (117), matching of HLA-A, -C, -B, -DRB1, -DQB1 alleles only will not necessarily implicate full MHC matching. Indeed, even within families up to 5% of otherwise 10/10-matched siblings will be HLA-DPB1-mismatched (118). Koskela et al. (119) performed detailed genome-level analyses of HLA-matched siblings and showed that the number of hidden mismatching within MHC is more common than assumed. In most cases, the mismatching included not only the known mismatch, but many other additional genes. Furthermore, the authors found evidence that the higher level of mismatching in MHC was associated with an increased risk for both acute and chronic GvHD.
Bogunia-Kubik and co-workers found that patient-donor matching for HLA-E alleles might be of prognostic value for the transplant outcome and reduce the risk of aGvHD in 10/10 HLA-matched transplants (120, 121). However, this association has not been observed in a more recent study (122) and no association with cGvHD was found. HLA-E is an interesting candidate, as it influences both the innate and the adaptive arms of the immune system by engaging inhibitory and activating receptors on NK cells and CD8+ T cells (123). Like classical HLA class I molecules, HLA-E is ubiquitously expressed. However, it is characterized by only a very limited sequence variability, and two dominant functional alleles differing at one amino acid position in the α2 heavy chain domain have been reported. These isoforms vary in peptide binding affinity. In its role in both NK and CD8+ T cell regulation HLA-E resembles that of MICA.
Mismatches in MICA gene, located close to HLA-B, increased complications of HSCT in two large studies that, unfortunately, were limited to screening of MICA only (124, 125). Fuerst and colleagues (124) evaluated 2172 HSCT cases and found that HSCT with a 10/10 HLA-match but a MICA position 129 mismatch resulted in lower overall and disease-free survival and an increased risk of aGvHD. Carapito and co-workers (125) studied 922 French HSCT and concluded that mismatch in MICA alleles increased, among others, the risk of cGvHD with a HR of 1.45–1.55. It is currently unclear how MICA mismatching could confer such profound biological effects, but it might involve an educational tuning of NKG2D responses in NK cells to the presence of high or low affinity ligands in an individual (126).
A number of reports on candidate non-MHC genes associated with occurrence of GvHD have also tested whether their matching between donor and recipient showed association with GvHD. Most studies are limited by too low numbers of patients and in many cases, it has been difficult to understand possible mechanisms behind the matching effect, hence, we do not go into details in this review. One potentially interesting concept was introduced by McCarroll and co-workers, who studied whether mismatched homozygous gene deletions are associated with GvHD (127). When the donor has a homozygous deletion of protein coding gene, thus missing the protein, it can be assumed that donor immune cells detect the protein as foreign, leading to a GvHD reaction. Indeed, the study screened 1345 HLA-identical HSCT and an association with aGvHD was found. No results from cGvHD were reported. It would be of interest to analyze the summary effect of all homozygous deletions between HSCT pairs. The role of copy-number variation has also been indicated in kidney transplantation (128).
Intuitively, the genome-wide histocompatibility concept, in which a summary of all immunogenetic mismatches in the genomes of donor and recipient is taken into account, could be more relevant in autoimmune-like cGvHD compared to its relevance in aGvHD. In aGvHD, the strong cytokine storm may lead to extensive immune activation that overruns the effect of other factors. The concept of genome wide histocompatibility in cGvHD has been tested in a few settings. Martin et al. (129) studied full HLA-matched sibling and unrelated HSCTs and HLA-DP-mismatched unrelated HSCTs for genome-wide minor histocompatibility effects. They found no evidence of an increased risk for cGvHD when genome-wide mismatching was increased, instead they concluded that the higher risk for GvHD in unrelated HSCT was due to mismatching of HLA-DP or other HLA genes. These results strongly pointed to the primary role of HLA-matching. On the other hand, Ritari et al. (59) assessed the exome sequences of 157 HSCT pairs and after various modeling techniques, found evidence that among HLA-identical sibling HSCTs a higher number of genome-wide mismatches predisposed patients to cGvHD. The group of Claude Perreault (130) introduced proteogenomic-based screening of overall mismatching in HSCT and utilized the findings to identify novel cell-therapy targets. Supporting the long-term effect of overall mismatch levels in transplantation, Mesnard et al. (131) reported that in kidney transplantation long-term graft function, rather than acute rejection, was associated with their genome-wide matching score. These studies provide interesting starting points for further analyses, however, at the present time the field is not mature enough for strong conclusions.
The role of KIR receptors is an excellent example of the complexity of biomarkers in HSCT. Their effect is influenced by various factors such as graft source, HLA matching, overall transplantation setting and appear donor or recipient specific. We therefore review the major findings of applying KIR genotypes in predicting for occurrence of cGvHD after HSCT. Many excellent and detailed reviews of KIR genetics and NK cells have been published during the past 5–10 years (132).
The function of NK cells is controlled by various surface receptors, including type I integral proteins with immunoglobulin like domains (KIR), type II integral proteins with lectin-like domains (NKG2D, CD94/NKG2) and natural cytotoxicity receptors (NCR) (133–136). Most studies to date have focused on inhibitory and activating KIRs. KIR haplotypes can be divided into two groups; A and B, depending on their KIR gene content (137). KIR A haplotypes are conserved, containing up to seven genes, most of which encode inhibitory receptors, while KIR B haplotypes have greater variation in gene content, including additional activating genes. KIR molecules recognize polymorphic epitopes at amino acid positions 76–83 of HLA class I molecules. C1 and C2 epitopes of HLA-C are recognized by KIR2DL2/2DL3 and 2DL1/2DS1, respectively. The Bw4 epitope is recognized by KIR3DL1 and the A3/11 epitope is recognized by KIR3DL2. The KIR gene region is located on chromosome 19q13.4, hence, segregating independently from HLA. During recent years, many studies have addressed the association of KIR receptors and their matching in HSCT.
A number of studies have indicated that the donor KIR gene composition, in particular the B haplotype, influences the outcome of HSCT at least in patients with acute myeloid leukemia (AML). However, whether the effect is seen in cGvHD is not clear. The results of associations of cGvHD with single KIR genes are heterogeneous.
In an analysis of patients with AML transplanted from HLA-matched (N = 209) and HLA-mismatched (N = 239) unrelated donors, Cooley et al. (138) showed that overall and relapse free survival were significantly higher in HSCT from a donor with at least one copy of the KIR B haplotype. In this study, the KIR B haplotype was associated with a higher incidence of cGvHD that may be linked to the low relapse rate. In another study, Cooley et al. (139) demonstrated that the centromeric genes in the KIR B haplotype of the donor had a strong effect on improving outcome of HSCT in AML patients. They were associated with a decreased incidence of relapse and improved disease free survival, but showed no significant effect on acute or chronic GvHD. No associations with KIR haplotypes were observed in patients with acute lymphocytic leukemia (ALL). Bachanova et al. (140) analyzed 573 HSCT recipients with chronic lymphocytic leukemia and did not find any effect of donor KIR genotype on transplant outcome. In a study of 281 patients with AML and ALL transplanted from matched sibling or unrelated donors, Faridi et al. (141) observed no effect of KIR B haplotype of the donor.
A study by Venstrom et al. (142) showed that the donor KIR3DS1 genotype had a beneficial effect in HSCT in a cohort of 1087 patients. The incidence of aGvHD, overall mortality and transplant-related mortality decreased with an increase in the number of KIR3DS1 copies in the donor, but there was no association with cGvHD. Giebel et al. (143) studied 100 patients with hematological malignancies transplanted from HLA-matched or single-mismatched donor and showed that the presence of activating KIR genes in the donor and their absence in the recipient was associated with a higher incidence of cGvHD. In a multiple regression analysis, aGvHD was associated with KIR2DS1 and cGvHD with KIR2DS3. Zhao et al. (144) analyzed 65 patients with haploidentical HSCT receiving grafts without T-cell depletion and observed that donor KIR2DS3 was also associated with a higher incidence of acute and chronic GvHD. In contrast, the presence of donor KIR2DS3 was a protective factor for cGvHD in a study of McQueen et al. (132) based on HLA-matched T cell-repleted HSCT from sibling donors. Kamenaric et al. (145) analyzed the impact of alleles of KIR2DS4, the only activating KIR gene in haplotype A, on transplantation outcomes and showed that donor full-length KIR2DS4 alleles were associated with a lower overall survival rate, a higher risk of GvHD and relapse.
The role of NK alloreactivity and KIR HLA matching in HSCT was introduced by Ruggeri et al. (146). They showed that in haploidentical T-cell depleted HSCT from related donors with KIR ligand incompatibility to graft-versus-host direction, NK cell alloreactivity was associated with a reduced occurrence of relapse and GvHD. Alloreactive NK cells were associated with GvL effect and could prevent GvHD by killing recipient`s antigen presenting cells that initiate GvHD (146). A recent study in 144 patients with T cell–replete haploidentical HSCT with post-transplant cyclophosphamide (147) supported earlier observations. Symons et al. (148) showed in 86 patients that mismatches for inhibitory KIR between the donor and recipient were associated with lower relapse and improved overall survival. However, no significant differences regarding the incidence of acute or chronic GvHD were observed.
Other studies showed variable results. Shimoni et al. (149) in a study of 444 patients with AML and ALL after T cell-replete haploidentical transplants with cyclophosphamide showed no significant effect of KIR ligand mismatching on transplant outcome and acute or chronic GvHD. Zhao et al. (142) analyzed 65 patients with haploidentical HSCT receiving grafts without T-cell depletion and observed an increased incidence of cGvHD in patients with only one KIR ligand compared to patients with 2 or 3 KIR ligand groups, based on the number of KIR ligands in recipients (HLA-C1, HLA-C2, or HLA-Bw4).
Analysis of 178 patients (150) transplanted from HLA-identical siblings showed that in patients with AML, lack of ligands for donor inhibitory KIRs was associated with a significantly lower relapse rate, but the risk of GvHD was not different. In a small cohort of HLA-matched sibling HSCT, Wang et al. (151) observed a lower incidence of cGvHD in C1 or C2 homozygotes than in C1/C2 heterozygotes. Thus, HLA-KIR-mismatch was associated with a lower incidence of cGvHD. In a recent study, Sahin et al. (152) analyzed the relevance of KIR gene-gene matching in 96 patients with myeloid malignancies receiving HSCT form HLA-identical siblings. cGvHD occurred less frequently in case of activating or inhibitory KIR matching. The donors positive for the KIR B haplotype were associated with an increased incidence of cGvHD.
Similarly to haploidentical allo-HSCT, Giebel et al. (153) demonstrated that KIR ligand mismatching is associated with a better outcome after HSCT from unrelated donors. KIR ligand mismatches were associated with a higher overall survival and disease free survival. The majority of studies (154–159) have, however, reported adverse effects of KIR ligand mismatching in HSCT from unrelated donors. Unfortunately, only a few of these studies addressed cGvHD, hence, the results are not conclusive. Morishima et al. (156) showed that KIR ligand mismatch in the graft-versus-host direction, defined when the donor`s KIR 2DL epitope on HLA-C was not shared by patient epitope, was associated with an increased rate of aGvHD, but had no effect on the incidence of cGvHD. In another large multicenter study including 1,571 patients with myeloid malignancies transplanted from unrelated donor, Farag et al. (160) did not show significant association of KIR ligand mismatching with acute or chronic GvHD. In a study of 142 leukemic patients receiving HSCT and ATG in vivo T-cell depletion, Kröger et al. (161) showed no associations of KIR ligand mismatch, KIR genotypes or KIR haplotypes with chronic or acute GvHD.
In a study of 281 patients with AML and ALL transplanted from matched sibling or unrelated donors, Faridi et al. (141) found an increased incidence of cGvHD in KIR genotype mismatching between the donor and recipient when the recipients had one or more C1 bearing HLA-C epitopes.
In summary, many studies over the last two decades have focused on the role of KIR receptors and their HLA class I ligands in HSCT. The results, however, are heterogeneous and no general conclusions can be made, in particular as only some studies reported association with cGvHD. In haploidentical HSCT, decrease of cGvHD rate was associated with donor KIR B haplotype, while the opposite association was observed in other types of HSCTs. Presence of donor activating KIR 2DS3 gene was found as a risk factor for an increase of cGvHD in many HSCT settings. The KIR associations were observed mainly in patients with myeloid diseases.
Postgraft immunosuppression is an essential component of allogeneic HSCT, with the primary goal to ensure engraftment and prevent the development of GvHD. Importantly, immunosuppressants are also used to treat GvHD. The most commonly used immunosuppressive agents are calcineurin inhibitors cyclosporine and tacrolimus, dihydrofolate reductase inhibitor methotrexate, and purine metabolism inhibitor mycophenolate mofetil. Genetic polymorphisms may impact the pharmacokinetics, i.e. absorption, distribution, metabolism and elimination of these agents (162, 163).
To date, the majority of GvHD-related pharmacogenetic findings have focused on the effects on aGvHD (10) and e.g. methylenetetrahydrofolate reductase and thymidylate synthase genotypes have been associated with aGvHD in recipients receiving methotrexate (164). In 2015, a review article by Franca et al. (165) summarized studies on pharmacogenetics variants and GvHD in both adult and pediatric cohorts. Despite the observed genotype effects on pharmacokinetic parameters, the studies found no statistically significant effects on cGvHD. In 2018, McCune et al. (166) studied 247 recipient-donor pairs and discovered that in recipient genotype, mycophenolate mofetil metabolism-related inosine monophosphate dehydrogenase type 1 rs2278293 was associated with a reduced risk for cGvHD.
The role of pharmacogenetics in a cGvHD setting is largely unknown and adequately powered pharmacokinetic and pharmacodynamic studies are challenging to complete, due to the substantial heterogeneity in the conditioning regimen, graft type, postgraft immunosuppression, and clinical classifications. However, variants with large effect sizes should be detected in well-powered GWASs. The blood level of immunosuppressants could be targeted and phenotype and meta-analysis approaches may also provide more reliable results. Better understanding of the role pharmacogenetics of immunosuppressants in the initiation and development of cGvHD could be translated to clinics and be of benefit to HSCT patients. Altogether, this important field requires further studies.
The present review screened scientific publications on genetic biomarkers for predicting development of chronic GvHD, a complex, autoimmune complication of HSCT. We modeled three different models for genetic factors: genetic association, genetic matching and pharmacogenetics. The review demonstrates that currently, there are no genetic polymorphisms or genetic tools that are validated, reliable biomarkers for predicting cGvHD.
Current lessons from genetic analyses of other multifactorial diseases suggest that larger, genome-wide studies with well-characterized cohorts are needed. The majority of the studies on HSCT thus far have included too few patients and have focused on only a small number of markers. Some candidate genes, such as CTLA4, HSPE, IL1R1, CCR6, FGFR1OP, and IL10, and HLA-linked MICA have been replicated to be associated with cGvHD risk in independent studies, and replications of these findings with fine mapping arrays or sequencing in various populations are needed.
A notable limitation of studies on cGvHD is the fact that clinical criteria of cGvHD changed over time and that they might not always have been interpreted consistently between centers. Moreover, progressive quiescent and de novo cGvHD, which are usually not distinguished in the studies, could have significant pathophysiological differences. This heterogeneity could also contribute to the inconsistency of results.
It is of note that a number of patients develop cGvHD in spite of very extensive immunosuppression and other treatments. Perhaps the medication is sufficiently effective in patients with specific genome profiles. Only sporadic publications on pharmacogenetic studies in cGvHD were found and this key area clear needs urgent attention. It should be noted, however, that GWAS also address variation in the drug metabolism genes. However, in this regard they are hampered by the variety of treatments in addition to the variety of underlying diseases.
Another line of research that may yield important findings is the use of modern genomic tools for cGvHD. Machine learning for genomic data and the integration of genomic data with other omics data could be employed for modeling and prediction. In addition to summarized effects of PRSs, other modern kernels may enable interactions within pathways. Genomic data might be integrated with other omics data from public gene-expression data bases or from the same individuals. The increased dimensionality induced by recipient-donor pairing could be tackled by machine learning tools selecting important features.
Finally, the risk of developing cGvHD may not be related to any single biomarker, but to the summary level of immunogenetic differences between each donor-recipient pair, that is, to the whole genome histocompatibility level. There is some evidence for this in cGvHD (59, 130) and also in long-term outcome of kidney transplantation (131). The differences may also include gene-deletion mismatches. Intuitively, the whole genome histocompatibility could influence the risk of chronic rather than aGvHD, in which the whole genome histocompatibility differences may be overruled by the cytokine storm and consequent immune activation.
All datasets presented in this study are included in the article/Supplementary Material.
RC, KH, and FP made the literature searches and compiled their results. RC revised the language in the revision. KB-K drafted the HLA sections and a part of Introduction section. MI drafted the KIR section. RD drafted the non-HLA MHC section and a part of Introduction section. JP drafted Introduction, Summary, Conclusions and the whole genome studies sections. KH drafted the pharmacogenetics section and a part of Introduction section. HB drafted parts on statistical/bioinformatics methods in the revision. JP, KH, and RD finalized the manuscript. All authors contributed to the article and approved the submitted version.
The authors are supported by the following grants: JP and KH are supported by the Academy of Finland, the Finnish Cancer Fund, the SalWe “Get it done”-project from the Tekes (currently Business Finland), and the VTR funding from the government of Finland. KB-K is supported by a grant from the National Science Centre (Poland): 2018/31/B/NZ2/03065. RC is supported by the Newcastle upon Tyne Hospitals NHS Charity. RD has been supported by the Deutsche Forschungsgemeinschaft (GRK 1034) and the European Union grant FP7-PEOPLE-2012-ITN-315963 (CELLEUROPE). MI is supported by grant NSF (Bulgaria) project H23/7 (contract KP-06-H23/4). All authors are supported by the COST foundation for project CA17138 cGvHD Eurograft (https://GvHD.eu).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The Supplementary Material for this article can be found online at https://www.frontiersin.org/articles/10.3389/fimmu.2020.575492/full#supplementary-material
Supplementary Figure 1 | Flow chart (top) and search terms (below) of PubMed literature search for genetic biomarkers of chronic GVHD.
1. Gratwohl A, Pasquini MC, Aljurf M, Atsuta Y, Baldomero H, Foeken L, et al. One million haemopoietic stem-cell transplants: a retrospective observational study. Lancet Haematol (2015) 2(3):91–100. doi: 10.1016/S2352-3026(15)00028-9
2. Kongtim P, Ciurea SO. Who is the best donor for haploidentical stem cell transplantation? Semin Hematol (2019) 56:194–200. doi: 10.1053/j.seminhematol.2018.08.003
3. Kim HT, Zhang MJ, Woolfrey AE, Martin AS, Chen J, Saber W, et al. Donor and recipient sex in allogeneic stem cell transplantation: What really matters. Haematologica (2016) 101(10):1260–6. doi: 10.3324/haematol.2016.147645
4. Miklos DB, Kim HT, Miller KH, Guo L, Zorn E, Lee SJ, et al. Antibody responses to H-Y minor histocompatibility antigens correlate with chronic graft-versus-host disease and disease remission. Blood (2005) 105(7):2973–8. doi: 10.1182/blood-2004-09-3660
5. Jagasia MH, Greinix HT, Arora M, Williams KM, Wolff D, Cowen EW, et al. National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: I. The 2014 Diagnosis and Staging Working Group Report. Biol Blood Marrow Transplant (2015) 21(3):389–401. doi: 10.1016/j.bbmt.2015.02.025
6. Warren EH, Zhang XC, Li S, Fan W, Storer BE, Chien JW, et al. Effect of MHC and non-MHC donor/recipient genetic disparity on the outcome of allogeneic HCT. Blood (2012) 120(14):2796–806. doi: 10.1182/blood-2012-04-347286
7. Ritari J, Hyvärinen K, Koskela S, Itälä-Remes M, Niittyvuopio R, Nihtinen A, et al. Genomic prediction of relapse in recipients of allogeneic haematopoietic stem cell transplantation. Leukemia (2019) 33(1):240–8. doi: 10.1038/s41375-018-0229-3
8. Zhu Q, Yan L, Liu Q, Zhang C, Wei L, Hu Q, et al. Exome chip analyses identify genes affecting mortality after HLA-matched unrelated-donor blood and marrow transplantation. Blood (2018) 131(22):2490–9. doi: 10.1182/blood-2017-11-817973
9. Spierings E, Kim Y-H, Hendriks M, Borst E, Sergeant R, Canossi A, et al. Multicenter Analyses Demonstrate Significant Clinical Effects of Minor Histocompatibility Antigens on GvHD and GvL after HLA-Matched Related and Unrelated Hematopoietic Stem Cell Transplantation. Biol Blood Marrow Transplant (2013) 19(8):1244–53. doi: 10.1016/j.bbmt.2013.06.001
10. Bogunia-Kubik K, Łacina P. From genetic single candidate gene studies to complex genomics of GvHD. Br J Haematol (2017) 178:661–75. doi: 10.1111/bjh.14704
11. Sato-Otsubo A, Nannya Y, Kashiwase K, Onizuka M, Azuma F, Akatsuka Y, et al. Genome-wide surveillance of mismatched alleles for graft-versus-host disease in stem cell transplantation. Blood (2015) 126(25):2752–63. doi: 10.1182/blood-2015-03-630707
12. Bari R, Hartford C, Keung Chan W, Vong Q, Li Y, Gan K, et al. Genome-wide single-nucleotide polymorphism analysis revealed SUFU suppression of acute graft-versus-host disease through downregulation of HLA-DR expression in recipient dendritic cells. Sci Rep (2015) 5:11098. doi: 10.1038/srep11098
13. Sham PC, Purcell SM. Statistical power and significance testing in large-scale genetic studies. Nat Rev Genet (2014) 15(5):335–46. doi: 10.1038/nrg3706
14. De Leeuw CA, Neale BM, Heskes T, Posthuma D. The statistical properties of gene-set analysis. Nat Rev Genet (2016) Jun 117(6):353–64. doi: 10.1038/nrg.2016.29
15. O’Dushlaine C, Rossin L, Lee PH, Duncan L, Parikshak NN, Newhouse S, et al. Psychiatric genome-wide association study analyses implicate neuronal, immune and histone pathways. Nat Neurosci (2015) 18(2):199–209. doi: 10.1038/nn.3922
16. Larson NB, Chen J, Schaid DJ. A review of kernel methods for genetic association studies. Genet Epidemiol (2019) 43(2):122–36. doi: 10.1002/gepi.22180
17. Freytag S, Manitz J, Schlather M, Kneib T, Amos CI, Risch A, et al. A network-based kernel machine test for the identification of risk pathways in genome-wide association studies. Hum Hered (2014) 76(2):64–75. doi: 10.1159/000357567
18. Friedrichs S, Manitz J, Burger P, Amos CI, Risch A, Chang-Claude J, et al. Pathway-Based Kernel Boosting for the Analysis of Genome-Wide Association Studies. Comput Math Methods Med (2017) 2017. doi: 10.1155/2017/6742763
19. Goyal RK, Lee SJ, Wang T, Trucco M, Haagenson M, Spellman SR, et al. Novel HLA-DP region susceptibility loci associated with severe acute GvHD. Bone Marrow Transplant (2017) 52(1):95–100. doi: 10.1038/bmt.2016.210
20. Martin PJ, Fan W, Storer BE, Levine DM, Zhao LP, Warren EH, et al. Replication of associations between genetic polymorphisms and chronic graft-versus-host disease. Blood (2016) 128(20):2450–6. doi: 10.1182/blood-2016-07-728063
21. Martínez-Laperche C, Buces E, Aguilera-Morillo MC, Picornell A, González-Rivera M, Lillo R, et al. A novel predictive approach for GVHD after allogeneic SCT based on clinical variables and cytokine gene polymorphisms. Blood Adv (2018) 2(14):1719–37. doi: 10.1182/bloodadvances.2017011502
22. Kamel AM, Gameel A, Ebid GTA, Radwan ER, Saleh MFM, Abdelfattah R. The impact of cytokine gene polymorphisms on the outcome of HLA matched sibling hematopoietic stem cell transplantation. Cytokine (2018) 110:404–11. doi: 10.1016/j.cyto.2018.05.003
23. Hyvärinen K, Ritari J, Koskela S, Niittyvuopio R, Nihtinen A, Volin L, et al. Genetic polymorphism related to monocyte-macrophage function is associated with graft-versus-host disease. Sci Rep (2017) 7(1):15666. doi: 10.1038/s41598-017-15915-3
24. Dukat-Mazurek A, Bieniaszewska M, Hellmann A, Moszkowska G, Trzonkowski P. Association of cytokine gene polymorphisms with the complications of allogeneic haematopoietic stem cell transplantation. Hum Immunol (2017) 78(11–12):672–83. doi: 10.1016/j.humimm.2017.09.005
25. Koyama D, Murata M, Hanajiri R, Okuno S, Kamoshita S, Julamanee J, et al. High incidence of extensive chronic graft-versus-host disease in patients with the REG3A rs7588571 non-GG genotype. PloS One (2017) 12(9):e0185213. doi: 10.1371/journal.pone.0185213
26. Berro M, Palau Nagore MV, Rivas MM, Longo P, Foncuberta C, Vitriú A, et al. Transforming growth factor-β1 functional polymorphisms in myeloablative sibling hematopoietic stem cell transplantation. Bone Marrow Transplant (2017) 52(5):739–44. doi: 10.1038/bmt.2016.355
27. Kim D, Won H-HH, Su S, Cheng L, Xu W, Hamad N, et al. Risk stratification of organ-specific GVHD can be improved by single-nucleotide polymorphism-based risk models. Bone Marrow Transplant (2014) 49(5):649–56. doi: 10.1038/bmt.2014.20
28. Norden J, Pearce KF, Irving JAE, Collin MP, Wang XN, Wolff D, et al. The influence of glucocorticoid receptor single nucleotide polymorphisms on outcome after haematopoietic stem cell transplantation. Int J Immunogenet (2018) 45:247–56. doi: 10.1111/iji.12380
29. Kielsen K, Enevold C, Heilmann C, Sengeløv H, Pedersen AE, Ryder LP, et al. Donor genotype in the Interleukin-7 receptor α-chain predicts risk of graft-versus-host disease and cytomegalovirus infection after allogeneic hematopoietic stem cell transplantation. Front Immunol (2018) 9:109. doi: 10.3389/fimmu.2018.00109
30. Takahashi H, Okayama N, Yamaguchi N, Miyahara Y, Morishima Y, Suehiro Y, et al. Associations of interactions between NLRP3 SNPs and HLA mismatch with acute and extensive chronic graft-versus-host diseases. Sci Rep (2017) 7(1):13097. doi: 10.1038/s41598-017-13506-w
31. Inamoto Y, Martin PJ, Flowers MED, Lee SJ, Carpenter PA, Warren EH, et al. Genetic risk factors for sclerotic graft-versus-host disease. Blood (2016) 128(11):1516–24. doi: 10.1182/blood-2016-05-715342
32. Resende RG, Correia-Silva J de F, Silva TA, Salomão UE, Marques-Silva L, Vieira ÉLM, et al. IL-17 genetic and immunophenotypic evaluation in chronic graft-versus-host disease. Mediators Inflammation (2014) 2014:571231. doi: 10.1155/2014/571231
33. Guillem V, Carlos Hern andez-Boluda J, Gallardo D, Bu I, Bosch A, Mart ınez-Laperche C, et al. A polymorphism in the TYMP gene is associated with the outcome of HLA-identical sibling allogeneic stem cell transplantation. Am J Hematol (2013) 88(10):883–9. doi: 10.1002/ajh.23523
34. Shamim Z, Spellman S, Haagenson M, Wang T, Lee SJ, Ryder LP, et al. Polymorphism in the interleukin-7 receptor-alpha and outcome after allogeneic hematopoietic cell transplantation with matched unrelated donor. Scand J Immunol (2013) 78(2):214–20. doi: 10.1111/sji.12077
35. Clark WB, Brown-Gentry KD, Crawford DC, Fan K-H, Snavely J, Chen H, et al. Genetic variation in recipient B-cell activating factor modulates phenotype of GVHD. Blood (2011) 118(4):1140–4. doi: 10.1182/blood-2010-09-310011
36. Takami A, Espinoza JL, Onizuka M, Ishiyama K, Kawase T, Kanda Y, et al. A single-nucleotide polymorphism of the Fcγ receptor type IIIA gene in the recipient predicts transplant outcomes after HLA fully matched unrelated BMT for myeloid malignancies. Bone Marrow Transplant (2011) 46(2):238–43. doi: 10.1038/bmt.2010.88
37. Sellami MH, Bani M, Torjemane L, Kaabi H, Ladeb S, Othmane TB, et al. Effect of donor CTLA-4 alleles and haplotypes on graft-versus-host disease occurrence in Tunisian patients receiving a human leukocyte antigen-identical sibling hematopoietic stem cell transplant. Hum Immunol (2011) 72(2):139–43. doi: 10.1016/j.humimm.2010.11.008
38. Inamoto Y, Murata M, Katsumi A, Kuwatsuka Y, Tsujimura A, Ishikawa Y, et al. Donor single nucleotide polymorphism in the CCR9 gene affects the incidence of skin GVHD. Bone Marrow Transplant (2010) 45(2):363–9. doi: 10.1038/bmt.2009.131
39. Kornblit B, Masmas T, Petersen SL, Madsen HO, Heilmann C, Schejbel L, et al. Association of HMGB1 polymorphisms with outcome after allogeneic hematopoietic cell transplantation. Biol Blood Marrow Transplant (2010) 16(2):239–52. doi: 10.1016/j.bbmt.2009.10.002
40. Boukouaci W, Busson M, Peffault de Latour R, Rocha V, Suberbielle C, Bengoufa D, et al. MICA-129 genotype, soluble MICA, and anti-MICA antibodies as biomarkers of chronic graft-versus-host disease. Blood (2009) 114(25):5216–24. doi: 10.1182/blood-2009-04-217430
41. Bertinetto FE, Dall’Omo AM, Mazzola GA, Rendine S, Berrino M, Bertola L, et al. Role of non-HLA genetic polymorphisms in graft-versus-host disease after haematopoietic stem cell transplantation. Int J Immunogenet (2006) 33(5):375–84. doi: 10.1111/j.1744-313X.2006.00630.x
42. Laguila Visentainer JE, Lieber SR, Lopes Persoli LB, Dutra Marques SB, Vigorito AC, Penteado Aranha FJ, et al. Relationship between cytokine gene polymorphisms and graft-versus-host disease after allogeneic stem cell transplantation in a Brazilian population. Cytokine (2005) 32(3–4):171–7. doi: 10.1016/j.cyto.2005.09.002
43. Bogunia-Kubik K, Mlynarczewska A, Wysoczanska B, Lange A. Recipient interferon-gamma 3/3 genotype contributes to the development of chronic graft-versus-host disease after allogeneic hematopoietic stem cell transplantation. Haematologica (2005) 90(3):425–6.
44. Stark GL, Dickinson AM, Jackson GH, Taylor PR, Proctor SJ, Middleton PG. Tumour necrosis factor receptor type II 196M/R genotype correlates with circulating soluble receptor levels in normal subjects and with graft-versus-host disease after sibling allogeneic bone marrow transplantation. Transplantation (2003) 76(12):1742–9. doi: 10.1097/01.TP.0000092496.05951.D5
45. Cullup H, Dickinson AM, Cavet J, Jackson GH, Middleton PG. Polymorphisms of interleukin-1α constitute independent risk factors for chronic graft-versus-host disease after allogeneic bone marrow transplantation. Br J Haematol (2003) 122(5):778–87. doi: 10.1046/j.1365-2141.2003.04510.x
46. Cavet J, Dickinson AM, Norden J, Taylor PRA, Jackson GH, Middleton PG. Interferon-α and interleukin-6 gene polymorphisms associate with graft-versus-host disease in HLA-matched sibling bone marrow transplantation. Blood (2001) 98(5):1594–600. doi: 10.1182/blood.V98.5.1594
47. Takahashi H, Furukawa T, Hashimoto S, Suzuki N, Kuroha T, Yamazaki F, et al. Contribution of TNF-alpha and IL-10 gene polymorphisms to graft-versus-host disease following allo-hematopoietic stem cell transplantation. Bone Marrow Transplant (2000) 26(12):1317–23. doi: 10.1038/sj.bmt.1702724
48. Trowsdale J, Knight JC. Major Histocompatibility Complex Genomics and Human Disease. Annu Rev Genomics Hum Genet (2013) 14(1):301–23. doi: 10.1146/annurev-genom-091212-153455
49. Khera AV, Chaffin M, Aragam KG, Haas ME, Roselli C, Choi SH, et al. Genome-wide polygenic scores for common diseases identify individuals with risk equivalent to monogenic mutations. Nat Genet (2018) 50(September):1219–24. doi: 10.1038/s41588-018-0183-z
50. Balavarca Y, Pearce K, Norden J, Collin M, Jackson G, Holler E, et al. Predicting survival using clinical risk scores and non-HLA immunogenetics. Bone Marrow Transplant (2015) 50(11):1445–52. doi: 10.1038/bmt.2015.173
51. Saber W, Opie S, Rizzo JD, Zhang MJ, Horowitz MM, Schriber J. Outcomes after matched unrelated donor versus identical sibling hematopoietic cell transplantation in adults with acute myelogenous leukemia. Blood (2012) 119(17):3908–16. doi: 10.1182/blood-2011-09-381699
52. Segal E, Martens M, Wang H-L, Brazauskas R, Weisdorf D, Sandmaier BM, et al. Comparing outcomes of matched related donor and matched unrelated donor hematopoietic cell transplants in adults with B-Cell acute lymphoblastic leukemia. Cancer (2017) 123(17):3346–55. doi: 10.1002/cncr.30737
53. Stewart CA, Horton R, Allock RJN, Ashurst JL, Atrazhev AM, Coggill P, et al. Complete MHC haplotype sequencing for common disease gene mapping. Genome Res (2004) 14(6):1176–87. doi: 10.1101/gr.2188104
54. The MHC Sequence Consortium. Complete sequence and gene map of a human major histocompatibility complex. Nature (1999) 401(6756):921–3. doi: 10.1038/44853
55. Norman PJ, Norberg SJ, Guethlein LA, Nemat-Gorgani N, Royce T, Wroblewski EE, et al. Sequences of 95 human MHC haplotypes reveal extreme coding variation in genes other than highly polymorphic HLA class I and II. Genome Res (2017) 27(5):813–23. doi: 10.1101/gr.213538.116
56. Petersdorf EW. The major histocompatibility complex: a model for understanding graft-versus-host disease. Blood (2013) 122(11):1863–72. doi: 10.1182/blood-2013-05-355982
57. Petersdorf EW, Malkki M, Gooley TA, Spellman SR, Haagenson MD, Horowitz MM, et al. MHC-Resident Variation Affects Risks After Unrelated Donor Hematopoietic Cell Transplantation. Sci Transl Med (2012) 4(144):144ra101. doi: 10.1126/scitranslmed.3003974
58. Hyvärinen K, Koskela S, Niittyvuopio R, Nihtinen A, Volin L, Salmenniemi U, et al. Meta-Analysis of Genome-Wide Association and Gene Expression Studies Implicates Donor T Cell Function and Cytokine Pathways in Acute GvHD. Front Immunol (2020) 3(11):19. doi: 10.3389/fimmu.2020.00019
59. Ritari J, Hyvärinen K, Koskela S, Niittyvuopio R, Nihtinen A, Salmenniemi U, et al. Computational analysis of HLA-presentation of non-synonymous recipient mismatches indicates effect on the risk of chronic graft-versus-host disease after allogeneic HSCT. Front Immunol (2019) 10:1625. doi: 10.3389/fimmu.2019.01625
60. Mullighan C, Heatley S, Doherty K, Szabo F, Grigg A, Hughes T, et al. Non-HLA immunogenetic polymorphisms and the risk of complications after allogeneic hemopoietic stem-cell transplantation. Transplantation (2004) 77(4):587–96. doi: 10.1097/01.TP.0000111769.45088.A2
61. Viel DO, Tsuneto LT, Sossai CR, Lieber SR, Marques SBD, Vigorito AC, et al. IL2 and TNFA Gene Polymorphisms and the Risk of Graft-versus-Host Disease after Allogeneic Haematopoietic Stem Cell Transplantation. Scand J Immunol (2007) 66(6):703–10. doi: 10.1111/j.1365-3083.2007.02021.x
62. Petersdorf EW, Malkki M, Horowitz MM, Spellman SR, Haagenson MD, Wang T. Mapping MHC haplotype effects in unrelated donor hematopoietic cell transplantation. Blood (2013) 121(10):1896–905. doi: 10.1182/blood-2012-11-465161
63. Pidala J, Sarwal M, Roedder S, Lee SJ. Biologic markers of chronic GVHD. Bone Marrow Transplant (2014) 49(3):324–31. doi: 10.1038/bmt.2013.97
64. Sandoval-Pinto E, Padilla-Gutiérrez JR, Valdés-Alvarado E, García-González IJ, Valdez-Haro A, Muñoz-Valle JF, et al. Association of the -1031T<C polymorphism and soluble TNF-α levels with Acute Coronary Syndrome. Cytokine (2016) 78:37–43. doi: 10.1016/j.cyto.2015.11.014
65. Umapathy D, Krishnamoorthy E, Mariappanadar V, Viswanathan V, Ramkumar KM. Increased levels of circulating (TNF-α) is associated with (-308G/A) promoter polymorphism of TNF-α gene in Diabetic Nephropathy. Int J Biol Macromol (2018) 107(Pt B):2113–21. doi: 10.1016/j.ijbiomac.2017.10.078
66. Cui G, Wang H, Li R, Zhang L, Li Z, Wang Y, et al. Polymorphism of tumor necrosis factor alpha (TNF-alpha) gene promoter, circulating TNF-alpha level, and cardiovascular risk factor for ischemic stroke. J Neuroinflammation (2012) 9(1):235. doi: 10.1186/1742-2094-9-235
67. Helmig S, Aliahmadi N, Stephan P, Döhrel J, Schneider J. TNF-α –308 genotypes are associated with TNF-α and TGF-β1 mRNA expression in blood leucocytes of humans. Cytokine (2011) 53(3):306–10. doi: 10.1016/j.cyto.2010.11.018
68. Nordlander A, Uzunel M, Mattsson J, Remberger M. The TNFd4 allele is correlated to moderate-to-severe acute graft-versus-host disease after allogeneic stem cell transplantation. Br J Haematol (2002) 119(4):1133–6. doi: 10.1046/j.1365-2141.2002.03965.x
69. Silkov AN, Sennikova NS, Goreva EP, Lopatnikova YA, Sennikov SV. Production of TNF-α and IL-1β by Peripheral Blood Mononuclear Cells in Carriers of Different Allele Variants of the Gene. Bull Exp Biol Med (2012) 153(1):68–71. doi: 10.1007/s10517-012-1646-3
70. Reich K, Mössner R, König IR, Westphal G, Ziegler A, Neumann C. Promoter polymorphisms of the genes encoding tumor necrosis factor-alpha and interleukin-1beta are associated with different subtypes of psoriasis characterized by early and late disease onset. J Invest Dermatol (2002) 118(1):155–63. doi: 10.1046/j.0022-202x.2001.01642.x
71. Powrózek T, Mlak R, Brzozowska A, Mazurek M, Gołębiowski P, Małecka-Massalska T. Relationship between TNF-α -1031T/C gene polymorphism, plasma level of TNF-α, and risk of cachexia in head and neck cancer patients. J Cancer Res Clin Oncol (2018) 144(8):1423–34. doi: 10.1007/s00432-018-2679-4
72. Nourian M, Chaleshi V, Pishkar L, Azimzadeh P, Baradaran Ghavami S, Balaii H, et al. Evaluation of tumor necrosis factor (TNF)-α mRNA expression level and the rs1799964 polymorphism of the TNF-α gene in peripheral mononuclear cells of patients with inflammatory bowel diseases. BioMed Rep (2017) 6(6):698–702. doi: 10.3892/br.2017.908
73. Wei B-F, Feng Z, Wei W, Chen X. Associations of TNF-α -238 A/G and IL-10 -1082 G/A Genetic Polymorphisms With the Risk of NONFH in the Chinese Population. J Cell Biochem (2017) 118(12):4872–80. doi: 10.1002/jcb.26167
74. Peng Y, Li L-J. TNF-α-308G/A polymorphism associated with TNF-α protein expression in patients with diabetic nephropathy. Int J Clin Exp Pathol (2015) 8(3):3127–31.
75. Kothari N, Bogra J, Abbas H, Kohli M, Malik A, Kothari D, et al. Tumor Necrosis Factor gene polymorphism results in high TNF level in sepsis and septic shock. Cytokine (2013) 61(2):676–81. doi: 10.1016/j.cyto.2012.11.016
76. Groh V, Bahram S, Bauer S, Herman A, Beauchamp M, Spies T. Cell stress-regulated human major histocompatibility complex class I gene expressed in gastrointestinal epithelium. Proc Natl Acad Sci (1996) 93(22):12445–50. doi: 10.1073/pnas.93.22.12445
77. Gasser S, Orsulic S, Brown EJ, Raulet DH. The DNA damage pathway regulates innate immune system ligands of the NKG2D receptor. Nature (2005) 436(7054):1186–90. doi: 10.1038/nature03884
78. Raulet DH, Gasser S, Gowen BG, Deng W, Jung H. Regulation of ligands for the NKG2D activating receptor. Annu Rev Immunol (2013) 31(1):413–41. doi: 10.1146/annurev-immunol-032712-095951
79. Chitadze G, Bhat J, Lettau M, Janssen O, Kabelitz D. Generation of soluble NKG2D ligands: proteolytic cleavage, exosome secretion and functional implications. Scand J Immunol (2013) 78(2):120–9. doi: 10.1111/sji.12072
80. Steinle A, Li P, Morris DL, Groh V, Lanier LL, Strong RK, et al. MICB, and homologs of the mouse RAE-1 protein family. Immunogenetics (2001) 53(4):279–87. doi: 10.1007/s002510100325
81. Isernhagen A, Malzahn D, Viktorova E, Elsner L, Monecke S, Bonin F, et al. The MICA-129 dimorphism affects NKG2D signaling and outcome of hematopoietic stem cell transplantation. EMBO Mol Med (2015) 7(11):1480–502. doi: 10.15252/emmm.201505246
82. Isernhagen A, Malzahn D, Bickeböller H, Dressel R. Impact of the MICA-129Met/Val Dimorphism on NKG2D-Mediated Biological Functions and Disease Risks. Front Immunol (2016) 12:7. doi: 10.3389/fimmu.2016.00588
83. Askar M, Sobecks R, Wang T, Haagenson M, Majhail N, Madbouly A, et al. MHC Class I Chain-Related Gene A (MICA) Donor-Recipient Mismatches and MICA-129 Polymorphism in Unrelated Donor Hematopoietic Cell Transplantations Has No Impact on Outcomes in Acute Lymphoblastic Leukemia, Acute Myeloid Leukemia, or Myelodysplastic Syndr. Biol Blood Marrow Transplant (2017) 23(3):436–44. doi: 10.1016/j.bbmt.2016.11.021
84. Martin PJ, Levine DM, Storer BE, Nelson SC, Dong X, Hansen JA. Recipient and donor genetic variants associated with mortality after allogeneic hematopoietic cell transplantation. Blood Adv (2020) 4(14):3224–33. doi: 10.1182/bloodadvances.2020001927
85. Isernhagen A, Schilling D, Monecke S, Shah P, Elsner L, Walter L, et al. The MICA-129Met/Val dimorphism affects plasma membrane expression and shedding of the NKG2D ligand MICA. Immunogenetics (2016) 68(2):109–23. doi: 10.1007/s00251-015-0884-8
86. Bogunia-Kubik K, Lange A. HSP70-hom Gene Polymorphism in Allogeneic Hematopoietic Stem-Cell Transplant Recipients Correlates with the Development of Acute Graft-versus-Host Disease. Transplantation (2005) 79(7):815–20. doi: 10.1097/01.TP.0000153157.97736.2C
87. Bogunia-Kubik K, Uklejewska A, Dickinson A, Jarvis M, Lange A. HSP70-hom Gene Polymorphism as a Prognostic Marker of Graft-Versus-Host Disease. Transplantation (2006) 82(8):1116–7. doi: 10.1097/01.tp.0000232673.44579.47
88. Milner CM, Campbell RD. Structure and expression of the three MHC-linked HSP70 genes. Immunogenetics (1990) 32(4):242–51. doi: 10.1007/BF00187095
89. Fernández-Fernández MR, Valpuesta JM. Hsp70 chaperone: a master player in protein homeostasis. F1000Research (2018) 7:1497. doi: 10.12688/f1000research.15528.1
90. Dressel R. Collaboration of Heat Shock Protein 70 and Stress-induced NKG2D Ligands in the Activation of NK Cells against Tumors. Curr Immunol Rev (2017) 13:56–63. doi: 10.2174/1573395513666170316105859
91. Boudesco C, Cause S, Jego G, Garrido C. Hsp70: A Cancer Target Inside and Outside the Cell. Methods Mol Biol (2018) 1709:371–96. doi: 10.1007/978-1-4939-7477-1_27
92. Fourie AM, Peterson PA, Yang Y. Characterization and regulation of the major histocompatibility complex–encoded proteins Hsp70-Hom and Hsp70-1/2. Cell Stress Chaperones (2001) 6(3):282. doi: 10.1379/1466-1268(2001)006<0282:CAROTM>2.0.CO;2
93. Westra HJ, Peters MJ, Esko T, Yaghootkar H, Schurmann C, Kettunen J, et al. Systematic identification of trans eQTLs as putative drivers of known disease associations. Nat Genet (2013) 45(10):1238–43. doi: 10.1038/ng.2756
94. Goral J, Mathews HL, Clancy J. Expression of 70-kDa heat-shock protein during acute graft-versus-host disease. Clin Immunol Immunopathol (1998) 86(3):252–8. doi: 10.1006/clin.1997.4473
95. Goral J, Mathews HL, Clancy J. Antibodies specific for the 70-kDa heat-shock protein parallel the development of acute graft-versus-host disease in (DA x LEW)F1 rats. Clin Immunol Immunopathol (1995) 75(2):147–53. doi: 10.1006/clin.1995.1064
96. Goral J, Shenoy S, Mohanakumar T, Clancy J. Antibodies to 70 kD and 90 kD heat shock proteins are associated with graft-versus-host disease in peripheral blood stem cell transplant recipients. Clin Exp Immunol (2002) 127(3):553–9. doi: 10.1046/j.1365-2249.2002.01770.x
97. Jarvis M, Marzolini M, Wang XN, Jackson G, Sviland L, Dickinson AM. Heat shock protein 70: correlation of expression with degree of graft-versus-host response and clinical graft-versus-host disease1. Transplantation (2003) 76(5):849–53. doi: 10.1097/01.TP.0000083556.73555.78
98. Novota P, Sviland L, Zinöcker S, Stocki P, Balavarca Y, Bickeböller H, et al. Correlation of Hsp70-1 and Hsp70-2 Gene Expression With the Degree of Graft-Versus-Host Reaction in a Rat Skin Explant Model. Transplantation (2008) 85(12):1809–16. doi: 10.1097/TP.0b013e31817753f7
99. Atarod S, Turner B, Pearce KF, Ahmed SS, Norden J, Bogunia-Kubik K, et al. Elevated level of HSPA1L mRNA correlates with graft-versus-host disease. Transpl Immunol (2015) 32(3):188–94. doi: 10.1016/j.trim.2015.02.002
100. Mirza N, Prokop L, Kowalewski D, Gouttefangeas C, Faul C, Bethge WA, et al. Soluble heat shock protein 70 members in patients undergoing allogeneic hematopoietic cell transplantation. Transpl Immunol (2016) 36:25–31. doi: 10.1016/j.trim.2016.03.003
101. Reinhardt-Heller K, Hirschberg I, Vogl T, Handgretinger R, Holzer U. Characterization of monocyte subtypes regarding their phenotype and development in the context of graft-versus-host disease. Transpl Immunol (2018) 50:48–54. doi: 10.1016/j.trim.2018.06.004
102. Kollman C, Spellman SR, Zhang M-J, Hassebroek A, Anasetti C, Antin JH, et al. The effect of donor characteristics on survival after unrelated donor transplantation for hematologic malignancy. Blood (2016) 127(2):260–7. doi: 10.1182/blood-2015-08-663823
103. Morishima Y, Kashiwase K, Matsuo K, Azuma F, Morishima S, Onizuka M, et al. Biological significance of HLA locus matching in unrelated donor bone marrow transplantation. Blood (2014) 125(7):1189–97. doi: 10.1182/blood-2014-10-604785
104. Morishima Y, Kashiwase K, Matsuo K, Azuma F, Morishima S, Onizuka M, et al. Biological significance of HLA locus matching in unrelated donor bone marrow transplantation. Blood (2015) 125:1189–97.
105. Arrieta-Bolaños E, Crivello P, Shaw BE, Ahn KW, Wang H-L, Verneris MR, et al. In silico prediction of nonpermissive HLA-DPB1 mismatches in unrelated HCT by functional distance. Blood Adv (2018) 2(14):1773–83. doi: 10.1182/bloodadvances.2018019620
106. Fleischhauer K, Shaw BE. HLA-DP in unrelated hematopoietic cell transplantation revisited: challenges and opportunities. Blood (2017) 130(9):1089–96. doi: 10.1182/blood-2017-03-742346
107. René C, Lozano C, Villalba M, Eliaou J-F. 5′ and 3′ untranslated regions contribute to the differential expression of specific HLA-A alleles. Eur J Immunol (2015) 45(12):3454–63. doi: 10.1002/eji.201545927
108. Kulkarni S, Ramsuran V, Rucevic M, Singh S, Lied A, Kulkarni V, et al. Posttranscriptional Regulation of HLA-A Protein Expression by Alternative Polyadenylation Signals Involving the RNA-Binding Protein Syncrip. J Immunol (2017) 199(11):3892–9. doi: 10.4049/jimmunol.1700697
109. Apps R, Qi Y, Carlson JM, Chen H, Gao X, Thomas R, et al. Influence of HLA-C Expression Level on HIV Control. Sci (80- ) (2013) 340(6128):87–91. doi: 10.1126/science.1232685
110. Petersdorf EW, Gooley TA, Malkki M, Bacigalupo AP, Cesbron A, Du Toit E, et al. HLA-C expression levels define permissible mismatches in hematopoietic cell transplantation. Blood (2014) 124(26):3996–4003. doi: 10.1182/blood-2014-09-599969
111. Thomas R, Thio CL, Apps R, Qi Y, Gao X, Marti D, et al. A Novel Variant Marking HLA-DP Expression Levels Predicts Recovery from Hepatitis B Virus Infection. J Virol (2012) 86(12):6979–85. doi: 10.1128/JVI.00406-12
112. Petersdorf EW, Malkki M, O’hUigin C, Carrington M, Gooley T, Haagenson MD, et al. High HLA-DP Expression and Graft-versus-Host Disease. N Engl J Med (2015) 373(7):599–609. doi: 10.1056/NEJMoa1500140
113. Kulkarni S, Savan R, Qi Y, Gao X, Yuki Y, Bass SE, et al. Differential microRNA regulation of HLA-C expression and its association with HIV control. Nature (2011) 472(7344):495–8. doi: 10.1038/nature09914
114. Fontaine P, Roy-Proulx G, Knafo L, Baron C, Roy DC, Perreault C. Adoptive transfer of minor histocompatibility antigen-specific T lymphocytes eradicates leukemia cells without causing graft-versus-host disease. Nat Med (2001) 7(7):789–94. doi: 10.1038/89907
115. Turpeinen H, Ojala PJ, Ojala K, Miettinen M, Volin L, Partanen J. Minor histocompatibility antigens as determinants for graft-versus-host disease after allogeneic haematopoietic stem cell transplantation. Int J Immunogenet (2013) 40(6):495–501. doi: 10.1111/iji.12051
116. Nowak J, Nestorowicz K, Graczyk-Pol E, Mika-Witkowska R, Rogatko-Koros M, Jaskula E, et al. HLA-inferred extended haplotype disparity level is more relevant than the level of HLA mismatch alone for the patients survival and GvHD in T cell-replate hematopoietic stem cell transplantation from unrelated donor. Hum Immunol (2018) 79(6):403–12. doi: 10.1016/j.humimm.2018.03.011
117. Cullen M, Noble J, Erlich H, Thorpe K, Beck S, Klitz W, et al. Characterization of recombination in the HLA class II region. Am J Hum Genet (1997) 60(2):397–407.
118. Büchler T, Gallardo D, Rodríguez-Luaces M, Pujal J, Grañena A. Frequency of HLA-DPB1 disparities detected by reference strand-mediated conformation analysis in HLA-A, -B, and -DRB1 matched siblings. Hum Immunol (2002) 63(2):139–42. doi: 10.1016/S0198-8859(01)00376-7
119. Koskela S, Ritari J, Hyvärinen K, Kwan T, Niittyvuopio R, Itälä-Remes M, et al. Hidden genomic MHC disparity between HLA-matched sibling pairs in hematopoietic stem cell transplantation. Sci Rep (2018) 8(1):5396. doi: 10.1038/s41598-018-23682-y
120. Bogunia-Kubik K, Polak M, Kościńska K, Jaskuła E, Lange A. Chromosome 6 gene polymorphisms as the factors affecting the risk of HSCT outcome. Eur J Immunol (2009) 39(S1):S734. doi: 10.1002/eji.200990056
121. Bogunia-Kubik K, Jaskula E, Polak M, Kościńska K, Sędzimirska M, Lange A. Non classical HLA-E and G gene polymorphisms affect the HSCT outcome. Bone Marrow Transplant (2010) 45(S2):S135. doi: 10.1038/bmt.2010.40
122. Fürst D, Bindja J, Arnold R, Herr W, Schwerdtfeger R, Müller CH, et al. HLA-E polymorphisms in hematopoietic stem cell transplantation. Tissue Antigens (2012) 79(4):287–90. doi: 10.1111/j.1399-0039.2011.01832.x
123. Iwaszko M, Bogunia-Kubik K. Clinical significance of the HLA-E and CD94/NKG2 interaction. Arch Immunol Ther Exp (Warsz) (2011) 59(5):353–67. doi: 10.1007/s00005-011-0137-y
124. Fuerst D, Neuchel C, Niederwieser D, Bunjes D, Gramatzki M, Wagner E, et al. Matching for the MICA-129 polymorphism is beneficial in unrelated hematopoietic stem cell transplantation. Blood (2016) 128(26):3169–76. doi: 10.1182/blood-2016-05-716357
125. Carapito R, Jung N, Kwemou M, Untrau M, Michel S, Pichot A, et al. Matching for the nonconventional MHC-I MICA gene significantly reduces the incidence of acute and chronic GVHD. Blood (2016) 128(15):1979–86. doi: 10.1182/blood-2016-05-719070
126. Shafi S, Vantourout P, Wallace G, Antoun A, Vaughan R, Stanford M, et al. An NKG2D-Mediated Human Lymphoid Stress Surveillance Response with High Interindividual Variation. Sci Transl Med (2011) 3(113):113ra124–113ra124. doi: 10.1126/scitranslmed.3002922
127. McCarroll SA, Bradner JE, Turpeinen H, Volin L, Martin PJ, Chilewski SD, et al. Donor-recipient mismatch for common gene deletion polymorphisms in graft-versus-host disease. Nat Genet (2009) 41(12):1341–4. doi: 10.1038/ng.490
128. Steers NJ, Li Y, Drace Z, D’Addario JA, Fischman C, Liu L, et al. Genomic Mismatch at LIMS1 Locus and Kidney Allograft Rejection. N Engl J Med (2019) 380(20):1918–28. doi: 10.1056/NEJMoa1803731
129. Martin PJ, Levine DM, Storer BE, Warren EH, Zheng X, Nelson SC, et al. Genome-wide minor histocompatibility matching as related to the risk of graft-versus-host disease. Blood (2017) 129(6):791–8. doi: 10.1182/blood-2016-09-737700
130. Granados DP, Rodenbrock A, Laverdure J-P, Côté C, Caron-Lizotte O, Carli C, et al. Proteogenomic-based discovery of minor histocompatibility antigens with suitable features for immunotherapy of hematologic cancers. Leukemia (2016) 30(6):1344–54. doi: 10.1038/leu.2016.22
131. Mesnard L, Muthukumar T, Burbach M, Li C, Shang H, Dadhania D, et al. Exome Sequencing and Prediction of Long-Term Kidney Allograft Function. PloS Comput Biol (2016) 12(9):1–15. doi: 10.1371/journal.pcbi.1005088
132. Parham P, Guethlein LA. Genetics of Natural Killer Cells in Human Health, Disease, and Survival. Annu Rev Immunol (2018) 36(1):519–48. doi: 10.1146/annurev-immunol-042617-053149
133. Martin AM, Freitas EM, Witt CS, Christiansen FT. The genomic organization and evolution of the natural killer immunoglobulin-like receptor (KIR) gene cluster. Immunogenetics (2000) 51(4–5):268–80. doi: 10.1007/s002510050620
134. Lopez-Botet M, Perez-Villar JJ, Carretero M, Rodriguez A, Melero I, Bellon T, et al. Structure and function of the CD94 C-type lectin receptor complex involved in recognition of HLA class I molecules. Immunol Rev (1997) 155(1):165–74. doi: 10.1111/j.1600-065X.1997.tb00949.x
135. Bottino C, Biassoni R, Millo R, Moretta L, Moretta A. The human natural cytotoxicity receptors (NCR) that induce HLA class I-independent NK cell triggering. Hum Immunol (2000) 61(1):1–6. doi: 10.1016/S0198-8859(99)00162-7
136. Wilson MJ, Torkar M, Haude A, Milne S, Jones T, Sheer D, et al. Plasticity in the organization and sequences of human KIR/ILT gene families. Proc Natl Acad Sci U S A (2000) 97(9):4778–83. doi: 10.1073/pnas.080588597
137. Uhrberg M, Valiante NM, Shum BP, Shilling HG, Lienert-Weidenbach K, Corliss B, et al. Human Diversity in Killer Cell Inhibitory Receptor Genes. Immunity (1997) 7(6):753–63. doi: 10.1016/S1074-7613(00)80394-5
138. Cooley S, Trachtenberg E, Bergemann TL, Saeteurn K, Klein J, Le CT, et al. Donors with group B KIR haplotypes improve relapse-free survival after unrelated hematopoietic cell transplantation for acute myelogenous leukemia. Blood (2009) 113(3):726–32. doi: 10.1182/blood-2008-07-171926
139. Cooley S, Weisdorf DJ, Guethlein LA, Klein JP, Wang T, Le CT, et al. Donor selection for natural killer cell receptor genes leads to superior survival after unrelated transplantation for acute myelogenous leukemia. Blood (2010) 116(14):2411–9. doi: 10.1182/blood-2010-05-283051
140. Bachanova V, Weisdorf DJ, Wang T, Marsh SGE, Cereb N, Haagenson MD, et al. Donor Killer Cell Immunoglobulin-Like Receptor Genotype Does Not Improve Graft-versus-Leukemia Responses in Chronic Lymphocytic Leukemia after Unrelated Donor Transplant: A Center for International Blood and Marrow Transplant Research Analysis. Biol Blood Marrow Transplant (2019) 25(5):949–54. doi: 10.1016/j.bbmt.2018.12.763
141. Faridi RM, Kemp TJ, Dharmani-Khan P, Lewis V, Tripathi G, Rajalingam R, et al. Donor-Recipient Matching for KIR Genotypes Reduces Chronic GVHD and Missing Inhibitory KIR Ligands Protect against Relapse after Myeloablative, HLA Matched Hematopoietic Cell Transplantation. PloS One (2016) 11(6):e0158242. doi: 10.1371/journal.pone.0158242
142. Venstrom JM, Gooley TA, Spellman S, Pring J, Malkki M, Dupont B, et al. Donor activating KIR3DS1 is associated with decreased acute GVHD in unrelated allogeneic hematopoietic stem cell transplantation. Blood (2010) 115(15):3162–5. doi: 10.1182/blood-2009-08-236943
143. Giebel S, Nowak I, Dziaczkowska J, Czerw T, Wojnar J, Krawczyk-Kulis M, et al. Activating killer immunoglobulin-like receptor incompatibilities enhance graft-versus-host disease and affect survival after allogeneic hematopoietic stem cell transplantation. Eur J Haematol (2009) 83(4):343–56. doi: 10.1111/j.1600-0609.2009.01280.x
144. Zhao X, Huang X, Liu K, Xu L, Liu D. Prognosis after unmanipulated HLA-haploidentical blood and marrow transplantation is correlated to the numbers of KIR ligands in recipients. Eur J Haematol (2007) 78(4):338–46. doi: 10.1111/j.1600-0609.2007.00822.x
145. Burek Kamenaric M, Stingl Jankovic K, Grubic Z, Serventi Seiwerth R, Maskalan M, Nemet D, et al. The impact of KIR2DS4 gene on clinical outcome after hematopoietic stem cell transplantation. Hum Immunol (2017) 78(2):95–102. doi: 10.1016/j.humimm.2016.11.010
146. Ruggeri L, Capanni M, Urbani E, Perruccio K, Shlomchik WD, Tosti A, et al. Effectiveness of donor natural killer cell alloreactivity in mismatched hematopoietic transplants. Science (2002) 295(5562):2097–100. doi: 10.1126/science.1068440
147. Wanquet A, Bramanti S, Harbi S, Fürst S, Legrand F, Faucher C, et al. Killer Cell Immunoglobulin-Like Receptor-Ligand Mismatch in Donor versus Recipient Direction Provides Better Graft-versus-Tumor Effect in Patients with Hematologic Malignancies Undergoing Allogeneic T Cell-Replete Haploidentical Transplantation Followed b. Biol Blood Marrow Transplant (2018) 24(3):549–54. doi: 10.1016/j.bbmt.2017.11.042
148. Symons HJ, Leffell MS, Rossiter ND, Zahurak M, Jones RJ, Fuchs EJ. Improved Survival with Inhibitory Killer Immunoglobulin Receptor (KIR) Gene Mismatches and KIR Haplotype B Donors after Nonmyeloablative, HLA-Haploidentical Bone Marrow Transplantation. Biol Blood Marrow Transplant (2010) 16(4):533–42. doi: 10.1016/j.bbmt.2009.11.022
149. Shimoni A, Labopin M, Lorentino F, Van Lint MT, Koc Y, Gülbas Z, et al. Killer cell immunoglobulin-like receptor ligand mismatching and outcome after haploidentical transplantation with post-transplant cyclophosphamide. Leukemia (2019) 33(1):230–9. doi: 10.1038/s41375-018-0170-5
150. Hsu KC, Keever-Taylor CA, Wilton A, Pinto C, Heller G, Arkun K, et al. Improved outcome in HLA-identical sibling hematopoietic stem-cell transplantation for acute myelogenous leukemia predicted by KIR and HLA genotypes. Blood (2005) 105(12):4878–84. doi: 10.1182/blood-2004-12-4825
151. Wang H, He Y, Zhai W, Wang M, Zhou Z, Zhao Y, et al. The impact of recipient HLA-Cw and donor killer immunoglobulin-like receptor genotyping on the outcome of patients receiving HLA-matched sibling donor hematopoietic stem cell transplantation for myeloid malignancies. Swiss Med Wkly (2013) 143:w13717. doi: 10.4414/smw.2013.13717
152. Sahin U, Dalva K, Gungor F, Ustun C, Beksac M. Donor-recipient killer immunoglobulin like receptor (KIR) genotype matching has a protective effect on chronic graft versus host disease and relapse incidence following HLA-identical sibling hematopoietic stem cell transplantation. Ann Hematol (2018) 97(6):1027–39. doi: 10.1007/s00277-018-3274-0
153. Giebel S, Locatelli F, Lamparelli T, Velardi A, Davies S, Frumento G, et al. Survival advantage with KIR ligand incompatibility in hematopoietic stem cell transplantation from unrelated donors. Blood (2003) 102(3):814–9. doi: 10.1182/blood-2003-01-0091
154. Davies SM, Ruggieri L, DeFor T, Wagner JE, Weisdorf DJ, Miller JS, et al. Evaluation of KIR ligand incompatibility in mismatched unrelated donor hematopoietic transplants. Killer immunoglobulin-like receptor Blood (2002) 100(10):3825–7. doi: 10.1182/blood-2002-04-1197
155. De Santis D, Bishara A, Witt CS, Nagler A, Brautbar C, Slavin S, et al. Natural killer cell HLA-C epitopes and killer cell immunoglobulin-like receptors both influence outcome of mismatched unrelated donor bone marrow transplants. Tissue Antigens (2005) 65(6):519–28. doi: 10.1111/j.1399-0039.2005.00396.x
156. Morishima Y, Yabe T, Matsuo K, Kashiwase K, Inoko H, Saji H, et al. Effects of HLA allele and killer immunoglobulin-like receptor ligand matching on clinical outcome in leukemia patients undergoing transplantation with T-cell-replete marrow from an unrelated donor. Biol Blood Marrow Transplant (2007) 13(3):315–28. doi: 10.1016/j.bbmt.2006.10.027
157. Hsu KC, Gooley T, Malkki M, Pinto-Agnello C, Dupont B, Bignon J-D, et al. KIR ligands and prediction of relapse after unrelated donor hematopoietic cell transplantation for hematologic malignancy. Biol Blood Marrow Transplant (2006) 12(8):828–36. doi: 10.1016/j.bbmt.2006.04.008
158. Sobecks RM, Wang T, Askar M, Gallagher MM, Haagenson M, Spellman S, et al. Impact of KIR and HLA Genotypes on Outcomes after Reduced-Intensity Conditioning Hematopoietic Cell Transplantation. Biol Blood Marrow Transplant (2015) 21(9):1589–96. doi: 10.1016/j.bbmt.2015.05.002
159. Ludajic K, Balavarca Y, Bickeböller H, Rosenmayr A, Fae I, Fischer GF, et al. KIR genes and KIR ligands affect occurrence of acute GVHD after unrelated, 12/12 HLA matched, hematopoietic stem cell transplantation. Bone Marrow Transplant (2009) 44(2):97–103. doi: 10.1038/bmt.2008.432
160. Farag SS, Bacigalupo A, Eapen M, Hurley C, Dupont B, Caligiuri MA, et al. The effect of KIR ligand incompatibility on the outcome of unrelated donor transplantation: a report from the center for international blood and marrow transplant research, the European blood and marrow transplant registry, and the Dutch registry. Biol Blood Marrow Transplant (2006) 12(8):876–84. doi: 10.1016/j.bbmt.2006.05.007
161. Kröger N, Binder T, Zabelina T, Wolschke C, Schieder H, Renges H, et al. Low number of donor activating killer immunoglobulin-like receptors (KIR) genes but not KIR-ligand mismatch prevents relapse and improves disease-free survival in leukemia patients after in vivo T-cell depleted unrelated stem cell transplantation. Transplantation (2006) 82(8):1024–30. doi: 10.1097/01.tp.0000235859.24513.43
162. McCune JS, Bemer MJ. Pharmacokinetics, Pharmacodynamics and Pharmacogenomics of Immunosuppressants in Allogeneic Haematopoietic Cell Transplantation: Part I. Clin Pharmacokinet (2016) 55(5):525–50. doi: 10.1007/s40262-015-0339-2
163. McCune JS, Bemer MJ, Long-Boyle J. Pharmacokinetics, Pharmacodynamics, and Pharmacogenomics of Immunosuppressants in Allogeneic Hematopoietic Cell Transplantation: Part II. Clin Pharmacokinet (2016) 55(5):551–93. doi: 10.1007/s40262-015-0340-9
164. Robien K, Bigler J, Yasui Y, Potter JD, Martin P, Storb R, et al. Methylenetetrahydrofolate Reductase and Thymidylate Synthase Genotypes and Risk of Acute Graft-versus-Host Disease Following Hematopoietic Cell Transplantation for Chronic Myelogenous Leukemia. Biol Blood Marrow Transplant (2006) 12(9):973–80. doi: 10.1016/j.bbmt.2006.05.016
165. Franca R, Stocco G, Favretto D, Giurici N, Decorti G, Rabusin M. Role of Pharmacogenetics in Hematopoietic Stem Cell Transplantation Outcome in Children. Int J Mol Sci (2015) 16(8):18601–27. doi: 10.3390/ijms160818601
Keywords: graft versus host disease (GvHD), biomarkers, genetic screen, stem cell transplantation (HSCT), gene marker
Citation: Partanen J, Hyvärinen K, Bickeböller H, Bogunia-Kubik K, Crossland RE, Ivanova M, Perutelli F and Dressel R (2020) Review of Genetic Variation as a Predictive Biomarker for Chronic Graft-Versus-Host-Disease After Allogeneic Stem Cell Transplantation. Front. Immunol. 11:575492. doi: 10.3389/fimmu.2020.575492
Received: 23 June 2020; Accepted: 28 September 2020;
Published: 19 October 2020.
Edited by:
Daniel Wolff, University Hospital Regensburg, GermanyReviewed by:
Jacqueline W. Mays, National Institutes of Health (NIH), United StatesCopyright © 2020 Partanen, Hyvärinen, Bickeböller, Bogunia-Kubik, Crossland, Ivanova, Perutelli and Dressel. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jukka Partanen, anVra2EucGFydGFuZW5AdmVyaXBhbHZlbHUuZmk=; Ralf Dressel, cmRyZXNzZUBnd2RnLmRl
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.