 Iñaki Ortiz de Landazuri1†
Iñaki Ortiz de Landazuri1† Natalia Egri1†
Natalia Egri1† Guillermo Muñoz-Sánchez1†
Guillermo Muñoz-Sánchez1† Valentín Ortiz-Maldonado2
Valentín Ortiz-Maldonado2 Victor Bolaño1
Victor Bolaño1 Carla Guijarro1
Carla Guijarro1 Mariona Pascal1,3,4
Mariona Pascal1,3,4 Manel Juan1,3,5*
Manel Juan1,3,5*- 1Department of Immunology, Centre de Diagnòstic Biomèdic, Hospital Clínic de Barcelona, Barcelona, Spain
- 2Department of Hematology, Institut Clínic de Malalties Hematològiques i Oncològiques, Hospital Clínic de Barcelona, Barcelona, Spain
- 3Institut D’Investigacions Biomèdiques August Pi i Sunyer, University of Barcelona, Banc de Sang i Teixits – Hospital Clínic de Barcelona Immunotherapy Platform, Barcelona, Spain
- 4Allergy Network ARADyAL, Instituto de Salud Carlos III, Madrid, Spain
- 5Hospital Sant Joan de Déu, Esplugues de Llobregat, Barcelona, Spain
The COVID-19 pandemic, caused by Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2), has generated a significant repercussion on the administration of adoptive cell therapies, including chimeric antigen receptor (CAR) T-cells. The closing of borders, the reduction of people transit and the confinement of the population has affected the supply chains of these life-saving medical products. The aim of this mini-review is to focus on how the COVID-19 pandemic has affected CAR T-cell therapy and taking into consideration the differences between the large-scale centralized productions for the pharmaceutical industry versus product manufacturing in the academic/hospital environment. We also review different aspects of CAR T-cell therapy and our managerial experience of patient selection, resource prioritization and some practical aspects to consider for safe administration. Although hospitals have been forced to change their usual workflows to cope with the saturation of health services by hospitalized patients, we recommend centers to continue offering this potentially curative treatment for patients with relapsed/refractory hematologic malignancies. Consequently, we propose appropriate selection criteria, early intervention to attenuate neurotoxicity or cytokine release syndrome with tocilizumab and prophylactic/preventive strategies to prevent infection. These considerations may apply to other emerging adoptive cell treatments and the corresponding manufacturing processes.
Introduction
The SARS-CoV-2 coronavirus has generated an unprecedented global impact on multiple aspects of society, economy and health. SARS-CoV-2 was reported as a new emerging zoonotic pathogen in Wuhan (China) in December 2019, and declared as a pandemic by the World Health Organization in March 2020 (1). Its rapid human-to-human transmission has affected millions of people (2). Indeed, the routine operation of medical systems has been significantly disrupted generating a health crisis in many countries due to limited resources such as hospital beds and personal protective equipment. In early June, the number of infected people had already risen to more than 6 million globally and the number of new cases detected is increasing daily. There is not pre-existing specific immunity placing at risk humanity as a whole to infection by SARS-CoV-2. Taken together with the severe pulmonary and systemic inflammatory complications associated with the disease, it has caused governments to enforce isolation measures to prevent its rapid spread. Hospitals have been forced to change their usual workflows to cope with the saturation of hospitalized services. The closing of borders, the reduction of the transit of people and the confinement of the population has affected the supply chains of products. Access to life-saving drugs has also been affected, negatively impacting on patients with other life-threatening diseases (3).
Chimeric antigen receptor (CAR) T-cell therapy is a life-saving bioengineered cell replacement therapy against leukemia. This adoptive antitumor immunotherapy, based on autologous T-cells transduced with a genetically engineered receptor for CD19 to redirect their cytotoxicity against native CD19 surface antigens expressed in tumor cells, has completely changed the management of patients with hematologic malignancies such as acute lymphoblastic leukemia (ALL) or non-Hodking lymphoma (NHL) (4–6). Tisagenlecleucel (Kymriah, Novartis) and axicabtagen ciloleucel (Yescarta, Kite/Gilead) are both anti-CD19 CAR T-cell (CART19) commercial products that obtained Food and Drug Administration (FDA) approval in 2017 for the treatment of pediatric and young adult patients with CD19+ relapsed/refractory B-cell ALL, relapsed/refractory B-cell NHL [diffuse large B-cell lymphoma (DLBCL), primary mediastinal B-cell lymphoma and transformed follicular lymphoma]. Other regulatory agencies like the European Medicines Agency (EMA) have also recently approved these commercial CART19 use. Therefore, CART19 is considered a potential curative therapeutic option for CD19+ hematologic malignancies with no response to conventional treatments. In addition, approval of other CAR T-cell products developed commercially against other molecular targets are expected as further options for treatment in the coming months. More than 500 clinical trials1 are being carried out testing CAR-based products. Some of them are financed by the industry and others are being developed in the academic ambit. The cohabitation of both is inevitable and necessary. Industry production could supply CAR T-cell therapies to reach the whole population using good manufacturing practice (GMP) accredited large facilities to centralize the manufacturing process. On the other hand, academic centers should be dedicated to develop CAR T-cell therapies against less frequent diseases. Independently, both have been seriously affected by the COVID-19 pandemic despite the differences they present in product manufacturing and management processes (7). The management of CAR T-cell therapy is a complex time-consuming process that requires highly specialized personnel and coordinated work systems including medical management of the patient before and after the infusion due to feasible toxicities (8–10).
Owing to the doubtless relevance of CAR T-cell therapy for hematologic patients, it is important to have in mind some considerations within the context of the COVID-19 pandemic. Therefore, the aim of this mini-review is to focus on how the effects caused by the pandemic have affected this therapy taking into consideration the differences between the large-scale centralized production of CAR T-cells by the pharmaceutical industry versus the product manufacturing processes employed by the academic/hospital environment. We also review different aspects of CAR T-cell therapy, including patient selection and resource prioritization performed in our center during the COVID-19 pandemic.
Cautious Continuation vs Deferment of CAR T-Cell Therapy During COVID-19 Pandemic
Chimeric antigen receptor T-cell therapy has elicited an unprecedented response against B-cell malignancies, but it is associated with significant toxicity, including prolonged cytopenia, cytokine release syndrome (CRS), and neurotoxicity (10–13). Toxicity is normally associated with the T-cell’s inherent mechanism of action that has been well-described in academic and industry developed CAR T-cells (14). The use of CART19 cell therapy can result in prolonged B-cell aplasia and therefore inability to develop an antibody response necessary to respond against pathogens such as SARS-CoV-2 (15, 16). Furthermore, these patients are usually managed as in-patients to facilitate intensive monitoring due to the severity and rapidity of CRS, neurotoxicity and frequent need the intensive care unit (ICU) (17).
The COVID-19 pandemic is a threat to interrupt any cell therapy. It is priority that each center carefully review the internal policies and procedures to adopt the recommendations needed according to their healthcare needs. Hospitals have instituted measures to defer multiple medical interventions, including adoptive cell treatments or hematopoietic stem cell transplantation. Another relevant consideration is the inconsistent uniformity of clinical cell therapy protocols. This hampers the establishment of standardized strategies during the COVID-19 pandemic. A large proportion of these patients receive therapy in academic or pharmaceutical clinical trials and many stopped to preserve patient’s safety. Indeed, lymphodepletion before final cell-product infusion facilitates the expansion of CAR T-cells as it generates a suitable environment for in vivo modified T-cell expansion and survival (18). However, this generates a severe immunosuppression that can be seriously complicated by SARS-CoV-2 infection. Nevertheless, delaying cell therapy as a consequence of the COVID-19 pandemic could be fatal for the majority of patients with relapsed/refractory malignancies. Alternative therapeutic strategies are also generally associated with significant immunosuppression and subsequent potential hospitalizations. In fact, CAR T-cells are potentially curative for patients with poor prognosis (19).
Required Resources for Safe Cell Therapy During the COVID-19 Pandemic
Not all centers will be affected in the same way during the COVID-19 pandemic. Therefore, a careful evaluation of resources and infrastructures should be performed between the department of hematology and the hospital emergency planning group. The availability of ICU, hospital beds and mechanical ventilation equipment are limited, but required resources. Moreover, staff shortages due to potential exposure and resource constraints on personal protective equipment affect the management of the patient before and after the treatment infusion.
Some practical aspects should be considered for the safe administration of CAR T-cell therapy during the pandemic (Table 1):
• In the case of ICU collapse: establish a triage algorithm to select only patients who are most likely to benefit with no alternative treatment options and in whom the risk of toxicity is lower.
• Guarantee the availability of personnel to perform the leukapheresis and the reception and sample processing in the adoptive cellular immunotherapy unit.
• Initiate lymphodepletion procedure only after receiving CAR T-cell products at the site to avoid potential obstacles on supply chain operations.
• Hospital bed availability should be ensured for the immediate 4 weeks surrounding the treatment. There are few children admitted with COVID-19 so young adult patients who may benefit from this therapy may be transferred to a Pediatric Center with greater availability of beds.
• Guarantee the availability of a member of the medical team with the capacity to respond to complications associated with COVID-19.
• Establish a specific workflow for patients infected with COVID-19.
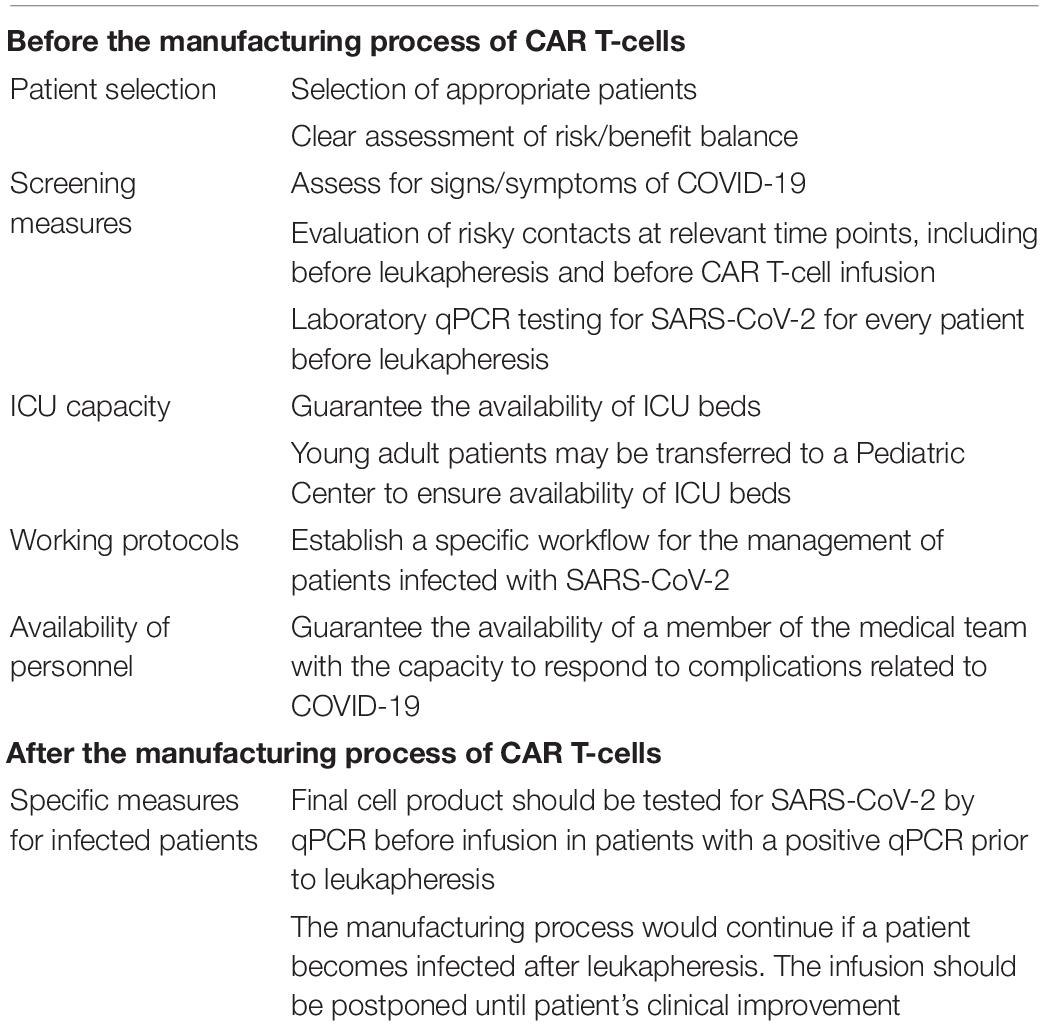
Table 1. Practical aspects before and after the manufacturing process for the safe administration of an academic CAR T-cell therapy during the COVID-19 pandemic.
Patient Selection in the COVID-19 Pandemic Setting
The COVID-19 pandemic has altered inclusion algorithms for the proper selection of patients, that is now associated to ethical dilemma. It is imperative to outline criteria to identify optimal candidates who have the potential to achieve significant remission. The benefit-risk balance should be clear, taking into account the risk of delaying CAR T-cell therapy against the risk of progression of the underlying disease. Therefore, a group of experts should evaluate the inclusion of patients considering, among multiple factors, the lack of avalability in the hospital and alternative treatments if complications appear. In our experience at Hospital Clínic de Barcelona, a medium-sized academic institution, we have continued to administer our academic and other commercial CAR-T cell therapy against aggressive relapsed/refractory B-cell NHL and ALL (20, 21).
Cellular Therapy Support During the COVID-19 Pandemic
During the first month of the COVID-19 state of alarm declared in Spain, every CAR T-cell operation was postponed and only one infusion was performed in our center. Ultimately, no treatment was canceled, although the final product infusions were delayed due to the lack of availability of space in the ICU. Different supportive measures to mitigate the risk of COVID-19 in our patients have been taken (Table 1). Two young patients (aged 26 and 30) were treated in another major hospital of the city, Sant Joan de Déu Children’s Hospital Center. After the first month of the pandemic, one bed at ICU was reserved for CAR T-cell therapy. This allowed the treatment of nine patients at Hospital Clínic de Barcelona. They were patients under the age of 70 with few co-morbidities and 0–2 ECOG functional status. Altogether, six patients were treated with academic CART19 and one patient with CAR T-cell therapy targeting BCMA (20). On the other hand, two patients were treated with CAR-T cells developed by the industry. The feasible impact of the delay on CAR T-cell treatment outcomes will be analyzed in the medium-long term.
CAR T-Cell Guidance: Screening and Preventive Measures
SARS-CoV-2 viral detection tests have been performed in every patient treated with CAR T-cells at various time-points. Before leukapheresis, patients were screened for SARS-CoV-2 by qPCR given that qPCR is the gold standard test to measure viral loads. The determining factor in the start of the cell therapy manufacturing process is the infection status of the patient and the potential ability to transmit the virus. Serological tests report directly on humoral immunization but serology is not a specific marker of infection. A positive IgM result in the serological test is not always equivalent to an acute infection since it could persist for months without viral load being detected in the patient. As with other infections, serological tests are very useful for screening but should only be used for diagnosis if a gold standard test is not available.
Our patients were assessed for specific symptoms during the whole process. In addition, in-person visits have been avoided as a preventive measure and patients were asked about their potential risky contacts. The major importance of extreme confinement measures has been therefore repeatedly emphasized. The use of EPI facemasks in patient’s environment was essential to maximally reduce infection risk. The final cell product should be tested for SARS-CoV-2 by qPCR before infusion in those patients with a positive qPCR prior to leukapheresis.
The special committee formed in our center to evaluate SARS-CoV-2-positive cases initially decided to avoid the CAR T-cell manufacturing process if COVID-19 was diagnosed in order to reduce possible contagions among medical staff and contamination of manufacturing facilities. This decision was controversial considering the low risk of contamination in a closed-circuit manufacturing process and the low viral load in blood samples (22). Currently, we have established to perform the leukapheresis 12 days after a positive qPCR result to ensure that the viral load in patient’s samples are virtually undetectable (23).
Diverse complications that could emerge from SARS-CoV-2 infection could actually worsen CAR T-cell therapy outcomes. Thorough monitoring of these patients is required in order to detect eventual neutropenia or other infection. Post-infusion standard antiviral, antifungal and antimicrobial prophylaxis protocols were recommended.
Manufacturing Time for Academic vs Pharmaceutical CAR T-Cell Therapies
Autologous CAR T-cell therapy requires a personalized manufacturing process based on several critical steps that demands good coordination between different medical disciplines. For those heavily treated patients, time is crucial and well-established workflows are essential for academic or commercial cell-based therapies. After the theoretical design of the synthetic chimeric receptor and the corresponding pre-clinical studies, the complete process for CAR T-cell therapy includes (i) obtaining the starting patient’s cell population by leukapheresis followed by the (ii) ex vivo genetic introduction of the synthetic CAR into these cells using mainly lentiviruses or retroviruses, previously generated. These modified T-cells are then (iii) activated and expanded in bioreactors and the resulting product might be (iv) adequately prepared and cryopreserve in infusible media for the final (v) product re-infusion into the patient (24, 25). All these steps can be affected by the pandemic setting. Along with inherent complexity in any cell therapy, limitations and obstacles in academic hospitals and pharmaceutical industry must be added. In this way, the standard manufacturing period of 9–11 days until the final product could be fatally extended (Figure 1).
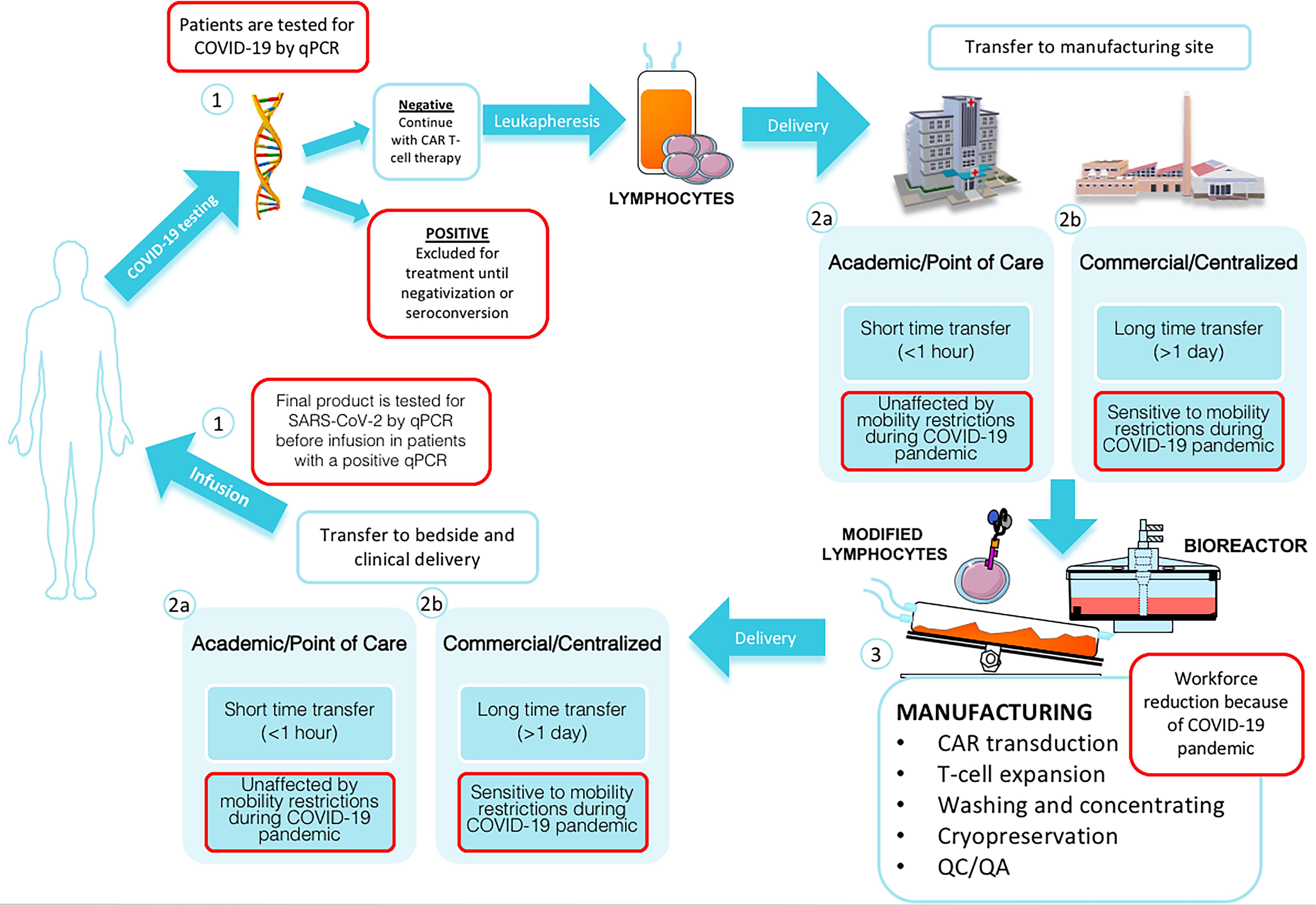
Figure 1. Standardized CAR T-cell manufacturing process during COVID-19 pandemic. Patients have to be tested by qPCR for SARS-Cov2 before leukapheresis (1); in case of a negative result, peripheral blood mononuclear cells (PBMCs) are collected from patient via leukapheresis. Timing of delivery to manufacturing site and the susceptibility to mobility restriction varies between Academic/Point of Care (2a) and Commercial/centralized (2b) production. Manufacturing process is affected by workforce reduction (3). T-cells are selected, activated, transduced with a viral or non-viral vector to express the desired CAR and expanded in a bioreactor. After that, resulting CAR T-cells are isolated and cryopreservated and assessed by quality control (QC) and quality assurance (QA) programs. Finally, the patient’s modified own cells are transferred to bedside. Timing of delivery to bedside and the susceptibility to mobility restriction varies between Academic/Point of Care (2a) and Commercial/centralized (2b) production. Before CAR T-cell product infusion, final product is tested for SARS-CoV-2 by qPCR before infusion in patients with a positive qPCR result prior to leukapaheresis (1).
COVID-19 Impact to Delivery and Critical Supply Chains
The main difference between academic and pharmaceutical CAR T-cells, regarding the timeline of the manufacturing process, is obtaining the “living drug.” As for academic products, commercial CART19 are based on autologous T-cells and each patient requires his own T-cells. In the academic CAR T-cell manufacturing, all steps are carried out in the hospital facilities enabling a more flexible, personalized and coordinated “patient-friendly process.” It allows short transfer times from the leukapheresis site to the production facilities and from the production center to the patient’s bed, both being less than 1 hour (26). In commercial manufacturing, the same process takes place in distant geographical locations and depends on delivery protocols established by pharmaceutical companies. Logically, the transfer times from the leukapheresis site to large-scale production GMP facilities and from this production center to the patient’s bed could be, at least, 1 day (27).
However, COVID-19 has rapidly constrained travel and mobility, extending the delivery times of commercial CAR T-cell products. Another side effect of reduced mobility are the potential disruptions in the resources supply line essential to the manufacturing process. This may affect both academic CAR T-cell products and those produced by industry. For example, the parallel process to obtain vectors with the CAR transgene like lentiviruses is a compendium of GMP skilled steps where different reagents are needed. Similarly, other specialized products are essential for the activation and expansion of T-cells in a bioreactor like CliniMACS Prodigy (28, 29). These critical steps can be seriously aggravated in countries where the production of these reagents is scarce and are imported from other regions. However, the large-scale production that takes place by industrial facilities ensures a greater storage capacity and a robust supply chain.
COVID-19 Impact to Availability of Personnel in Every Step of the Manufacturing Process
The reduction of personnel due to possible contagions among the staff, the restructuring of the workforce to treat infected patients and the limited resources and protective equipment has been a cause for concern (Table 1). All of these factors can impact equally on the academic or pharmaceutical production modalities.
The staff and the reagent shortage can affect the leukapheresis process and cell processing in the laboratory. There exist strict regulations associateds with cell therapy where personnel who develop “living drugs” must work under sterile and GMP conditions. For this reason, a contagion that could spread between qualified personnel and the consequent imposing quarantine that would be imposed on the rest of the personnel can become a bottleneck in the global production of the adoptive cell therapy. The stringent and immobile regulation has not been amended in the context of the COVID-19 pandemic to ensure the safety of patients, medical staff and laboratory personnel.
Similarly, within the associated legislation, a series of quality controls are imposed and must be complied with before CAR T-cell product infusion. Among them, the confirmation of the product sterility is essential. In addition, it must be ensured that the product is free of endotoxins, adventitious viruses and mycoplasma. There are other non-microbiological controls that must be carried out as the number of copies of the CAR per genome, flow cytometry experiments to determine the percentage of cells with CAR, among others. Having these controls in place for each cell product requires precious time in COVID-19 pandemic setting and is highly dependent on human work. Therefore, any delay in verifying all of these control points may delay the infusion.
Cytokine Release Syndrome and Tocilizumab Prioritization
Once the manufactured CAR T-cell product is infused, a resulting CRS is the widest described associated side effect. A compilation of different symptoms from hypotension to fever due to a massive pro-inflammatory cytokine release (IL-6, IL-1β, TNF-α) have been reported (30). Serum IL-6 level has been correlated with CRS severity (15). Hence, tocilizumab (TCZ), an anti-IL-6 receptor monoclonal antibody, has become the drug of choice for the management of moderate or severe CRS (10). This IL-6 cytokine release profile resembles the virally driven hyper-inflammation (CRS-like) suggested as predictor of fatality in COVID-19 (31). This fact has led to the setting-up of several clinical trials with the aim of studying the impact of TCZ administration in the evolution of the acute respiratory distress syndrome and the off-label use of this drug in symptomatic COVID-19 patients.
The management of CRS is extremely relevant given that viral infections (not only COVID-19) may promote CRS (32). CRS requires treatment with TCZ or corticosteroids depending on severity of symptoms. The notable increase in TCZ use has raised a concern about supply during COVID-19 pandemic. However, availability of 2 TCZ doses for each patient is a mandatory condition before CAR-T infusion. Two patients treated with CAR T-cell therapy have received TCZ to treat CRS in our center in the pandemic setting. Tocilizumab administration protocol has not been reconsidered despite supply problems. This protocol consists on early TCZ use at the onset of grade 2 CRS. We have dealt with TCZ scarcity through the use of other drugs such as sarilumab (human anti-IL-6 receptor) or siltuximab (chimeric anti-IL-6) to face the CRS-like complications. If ICU is collapsed, CRS management protocols should initiate earlier to reduce the probability of using ICU. As a practical option, we propose TCZ administration from grade 1 CRS (and not grade 2 as is usually done), or even prophylactic TCZ administration in those patients considered to be at high risk of severe CRS, with high tumor burden. Corticosteroids used as CRS treatment when TCZ has failed could promote potentially disadvantageous effects on COVID-19 outcomes (33). Nevertheless, corticosteroids should be cautiously used in COVID-19 patients that suffer from CRS after CAR T-cell infusion (34).
In fact, the current pandemic has exposed us to an ethical dilemma regarding the prioritization of TCZ. Each case must be thoroughly evaluated to ensure the availability of this drug. Tocilizumab could decrease the duration and severity of COVID-19 symptoms allowing the weaning of the ventilatory support (34). On the other hand, TCZ supply prior to infusion must be ensured for the hematologic patients during CAR T-cell therapy to mitigate the toxicity of an eventual CRS complication.
Conclusion
CAR T-cell therapy has been consolidated as a potential curative therapy for patients with refractory/relapsed hematologic malignancies. The COVID-19 pandemic represents an unprecedented challenge to continue safely treating patients with this adoptive cell therapy. Nevertheless, centers should continue offering this potentially curative treatment with CAR T-cell therapy for critical patients using appropriate selection criteria, early intervention to attenuate side effects like CRS with standardized TCZ protocols, and prophylactic/preventive strategies to prevent infection. For those heavily treated patients, time is crucial. Mobility and personnel restrictions add obstacles to a truly personalized therapy in which multidisciplinary teams intervenes. This has affected both academic CAR T-cell therapies and those commercially available. There are several limitations related to delivery and the time-consuming manufacturing processes that create new concepts concerning the benefit of academic point of care proposals. Also, some regulatory rules should be re-evaluated to become more flexible during this pandemic.
Author Contributions
MJ and MP proposed, directed, discussed, and revised the development of the manuscript. GM-S, NE, and IOL had equally contributed to the data gathering and writing of the review. VO-M reviewed and collaborated particularly on aspects related to the hematological issue. VB and CG had been in charge of analyzing the technical aspects related to the product manufacturing. All authors contributed to the article and approved the submitted version.
Funding
This review was included as a work sponsored by grants PI18/000775 and AC18/00072 (CE_ERA Net_Nanomed18) from Instituto de Salud Carlos III with Fondos FEDER. This work is also funded by the “Fundació bancaria la Caixa” (3922-19 FCRB) and CELLNEX TELECOM (5234-20/CPO42837). The funder bodies were not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Conflict of Interest
VO-M is a recipient of a research grant from Fundación Española de Hematología y Hemoterapia (FEHH), also declares travel grants (Kite, Celgene, Novartis, Roche, Takeda and Janssen), consultant or advisory fees (Kite, Celgene, and Novartis) and honoraria (Kite).
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank Dr. Michael J. Edel for proofreading the manuscript and Montserrat Riego for administrative tasks.
Abbreviations
SARS-CoV-2, Severe Acute Respiratory Syndrome Coronavirus-2; CAR, chimeric antigen receptor; ALL, acute lymphoblastic leukemia; NHL, non-hodking lymphoma; CART19, anti-CD19 CAR T-cell; FDA, Food and Drug Administration; DLCL, diffuse large B-cell lymphoma; GMP, good manufacturing practice; CRS, cytokine release syndrome; ICU, Intensive Care Unit; TCZ, tocilizumab; PBMCs, peripheral blood mononuclear cells.
Footnotes
References
1. Tay MZ, Poh CM, Rénia L, MacAry PA, Ng LFP. The Trinity of COVID-19: Immunity, Inflammation and Intervention. Natural Review Immunology [Internet]. (2020). Available online at: http://www.nature.com/articles/s41577-020-0311-8 (accessed April 28, 2020).
2. Vabret N, Britton GJ, Gruber C, Hegde S, Kim J, Kuksin M, et al. Immunology of COVID-19: current state of the science. Immunity. (2020) 52:910–41.
3. Bachanova V, Bishop MR, Dahi P, Dholaria B, Grupp SA, Hayes-Lattin B, et al. Chimeric Antigen Receptor T Cell Therapy During the COVID-19 Pandemic. Biology of Blood and Marrow Transplantation. Amsterdam: Elsevier Inc (2020).
4. Grupp SA, Kalos M, Barrett D, Aplenc R, Porter DL, Rheingold SR, et al. Chimeric antigen receptor-modified T cells for acute lymphoid leukemia. N Engl J Med. (2013) 368:1509–18. doi: 10.1056/NEJMoa1215134
5. Schuster SJ, Svoboda J, Chong EA, Nasta SD, Mato AR, Anak Ö, et al. Chimeric antigen receptor T Cells in refractory B-Cell lymphomas. N Engl J Med. (2017) 377:2545–54. doi: 10.1056/NEJMoa1708566
6. Maude SL, Laetsch TW, Buechner J, Rives S, Boyer M, Bittencourt H, et al. Tisagenlecleucel in children and young adults with B-cell lymphoblastic leukemia. N Engl J Med. (2018) 378:439–48. doi: 10.1056/NEJMoa1709866
7. Egri N, Ortiz de Landazuri I, San Bartolomé C, Ortega JR, Español-Rego M, Juan M. CART manufacturing process and reasons for academy-pharma collaboration. Immunol Lett. (2020) 217:39–48. doi: 10.1016/j.imlet.2019.10.014
8. Ruella M, June CH. Chimeric antigen receptor T cells for B cell neoplasms: choose the right CAR for you. Curr Hematol Malig Rep. (2016) 11:368–84. doi: 10.1007/s11899-016-0336-z
9. Gill S, Maus MV, Porter DL. Chimeric antigen receptor T cell therapy: 25 years in the making. Blood Rev. (2016) 30:157–67. doi: 10.1016/j.blre.2015.10.003
10. Brudno JN, Kochenderfer JN. Toxicities of chimeric antigen receptor T cells: recognition and management. Blood. (2016) 127:3321–30. doi: 10.1182/blood-2016-04-703751
11. Rubin DB, Danish HH, Ali AB, Li K, LaRose S, Monk AD, et al. Neurological toxicities associated with chimeric antigen receptor T-cell therapy. Brain. (2019) 142:1334–48. doi: 10.1093/brain/awz053
12. Morgan RA, Yang JC, Kitano M, Dudley ME, Laurencot CM, Rosenberg SA. Case report of a serious adverse event following the administration of t cells transduced with a chimeric antigen receptor recognizing ERBB2. Mol Ther. (2010) 18:843–51. doi: 10.1038/mt.2010.24
13. Bachanova V, Perales MA, Abramson JS. Modern management of relapsed and refractory aggressive B-cell lymphoma: a perspective on the current treatment landscape and patient selection for CAR T-cell therapy. Blood Rev. (2020) 40:100640. doi: 10.1016/j.blre.2019.100640
14. Neelapu SS. Managing the toxicities of CAR T−cell therapy. Hematol Oncol. (2019) 37:48–52. doi: 10.1002/hon.2595
15. Maude SL, Frey N, Shaw PA, Aplenc R, Barrett DM, Bunin NJ, et al. Chimeric antigen receptor T cells for sustained remissions in leukemia. N Engl J Med. (2014) 371:1507–17. doi: 10.1056/NEJMoa1407222
16. Bhoj VG, Arhontoulis D, Wertheim G, Capobianchi J, Callahan CA, Ellebrecht CT, et al. Persistence of long-lived plasma cells and humoral immunity in individuals responding to CD19-directed CAR T-cell therapy. Blood. (2016) 128:360–70. doi: 10.1182/blood-2016-01-694356
17. June CH, Sadelain M. Chimeric antigen receptor therapy. N Engl J Med. (2018) 379:64–73. doi: 10.1056/NEJMra1706169
18. Shah NN, Fry TJ. Mechanisms of resistance to CAR T cell therapy. Nat Rev Clin Oncol. (2019) 16:372–85. doi: 10.1038/s41571-019-0184-6
19. Brown CE, Mackall CL. Year in Review response and resistance. Nat Rev Immunol. (2019) 19:73–4. doi: 10.1038/s41577-018-0119-y
20. Castella M, Caballero-Baños M, Ortiz-Maldonado V, Azucena González-Navarro E, Suñé G, Antoñana-Vidósola A, et al. Point-Of-Care CAR T-Cell production (ARI-0001) using a closed semi-automatic bioreactor: experience from an academic phase I clinical trial. Front Immunol. (2020) 11:482. doi: 10.3389/fimmu.2020.00482
21. Ortíz-Maldonado V, Rives S, Castellà M, et al. CART19-BE-01: a multicenter Trial of ARI-0001 Cell Therapy in Patients with CD19+ Relapsed/Refractory malignancies. Mol Ther. (in press).
22. Wang W, Xu Y, Gao R, Lu R, Han K, Wu G, et al. Detection of SARS-CoV-2 in different types of clinical specimens. JAMA. (2020) 323:1843–4. doi: 10.1001/jama.2020.3786
23. Arons MM, Hatfield KM, Reddy SC, Kimball A, James A, Jacobs JR, et al. Presymptomatic SARS-CoV-2 infections and transmission in a skilled nursing facility. N Engl J Med. (2020) 382:2081–90. doi: 10.1056/NEJMoa2008457
24. Levine BL. Performance-enhancing drugs: design and production of redirected chimeric antigen receptor (CAR) T cells. Cancer Gene Ther. (2015) 22:79–84. doi: 10.1038/cgt.2015.5
25. Salter AI, Pont MJ, Riddell SR. Chimeric antigen receptor-modified T cells: CD19 and the road beyond. Blood. (2018) 131:2621–9. doi: 10.1182/blood-2018-01-785840
26. Ittershagen S, Ericson S, Eldjerou L, Shojaee A, Bleickardt E, Patel M, et al. Industry’s Giant leap into cellular therapy: catalyzing chimeric antigen receptor T Cell (CAR-T) immunotherapy. Curr Hematol Malig Rep. (2019) 14:47–55. doi: 10.1007/s11899-019-0498-6
27. Levine BL, Miskin J, Wonnacott K, Keir C. Global manufacturing of CAR T cell therapy. Mol Ther Methods Clin Dev. (2017) 4:92–101. doi: 10.1016/j.omtm.2016.12.006
28. Castella M, Boronat A, Martín-Ibáñez R, Rodríguez V, Suñé G, Caballero M, et al. Development of a novel anti-CD19 Chimeric antigen receptor: a paradigm for an affordable CAR T cell production at academic institutions. Mol Ther Methods Clin Dev. (2019) 12:134–44. doi: 10.1016/j.omtm.2018.11.010
29. Mock U, Nickolay L, Philip B, Cheung GWK, Zhan H, Johnston ICD, et al. Automated manufacturing of chimeric antigen receptor T cells for adoptive immunotherapy using CliniMACS prodigy. Cytotherapy. (2016) 18:1002–11. doi: 10.1016/j.jcyt.2016.05.009
30. Davila ML, Riviere I, Wang X, Bartido S, Park J, Curran K, et al. Efficacy and toxicity management of 19-28z CAR T cell therapy in B cell acute lymphoblastic leukemia. Sci Transl Med. (2014) 6:224.
31. Mehta P, McAuley DF, Brown M, Sanchez E, Tattersall RS, Manson JJ. COVID-19: consider cytokine storm syndromes and immunosuppression. Lancet. (2020) 395:1033–4. doi: 10.1016/s0140-6736(20)30628-0
32. Frey NV, Shaw PA, Hexner EO, Edward P, Saar G, Luger SM, et al. Optimizing chimeric antigen receptor T-cell therapy for adults with acute lymphoblastic leukemia. J Clin Oncol. (2019) 38:415–22. doi: 10.1200/JCO.19.01892
33. Shang L, Zhao J, Hu Y, Du R, Cao B. On the use of corticosteroids for 2019-nCoV pneumonia. Lancet. (2020) 395:683–4. doi: 10.1016/s0140-6736(20)30361-5
Keywords: chimeric antigen receptor, adoptive cell immunotherapy, SARS-CoV-2 coronavirus, manufacturing process, good manufacturing practice
Citation: Ortiz de Landazuri I, Egri N, Muñoz-Sánchez G, Ortiz-Maldonado V, Bolaño V, Guijarro C, Pascal M and Juan M (2020) Manufacturing and Management of CAR T-Cell Therapy in “COVID-19’s Time”: Central Versus Point of Care Proposals. Front. Immunol. 11:573179. doi: 10.3389/fimmu.2020.573179
Received: 16 June 2020; Accepted: 07 September 2020;
Published: 15 October 2020.
Edited by:
Cristina Maccalli, Sidra Medicine, QatarReviewed by:
Luis Alvarez-Vallina, Aarhus University, DenmarkFrancisco Martin, Andalusian Autonomous Government of Genomics and Oncological Research (GENYO), Spain
Copyright © 2020 Ortiz de Landazuri, Egri, Muñoz-Sánchez, Ortiz-Maldonado, Bolaño, Guijarro, Pascal and Juan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Manel Juan, mjuan@clinic.cat
†These authors have contributed equally to this work