 Lu Tang1,2
Lu Tang1,2 Zhinan Yin
Zhinan Yin Yu Hu
Yu Hu Heng Mei
Heng Mei
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Immunol., 30 November 2020
Sec. Viral Immunology
Volume 11 - 2020 | https://doi.org/10.3389/fimmu.2020.570993
Corona virus disease 2019 (COVID-19) has caused a global outbreak and severely posed threat to people’s health and social stability. Mounting evidence suggests that immunopathological changes, including diminished lymphocytes and elevated cytokines, are important drivers of disease progression and death in coronavirus infections. Cytokine storm not only limits further spread of virus in the body but also induces secondary tissue damage through the secretion of large amounts of active mediators and inflammatory factors. It has been determined that cytokine storm is a major cause of deaths in COVID-19; therefore, in order to reverse the deterioration of severe and critically ill patients from this disease, the cytokine storm has become a key therapeutic target. Although specific mechanisms of the occurrences of cytokine storms in COVID-19 have not been fully illuminated, hyper-activated innate immune responses, and dysregulation of ACE2 (angiotensin converting enzyme 2) expression and its downstream pathways might provide possibilities. Tailored immunoregulatory therapies have been applied to counteract cytokine storms, such as inhibition of cytokines, corticosteroids, blood purification therapy, and mesenchymal stem cell therapy. This review will summarize advances in the research of cytokine storms induced by COVID-19, as well as potential intervention strategies to control cytokine storms.
Pathogenic human coronavirus infections, such as severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS), could cause fatal lower respiratory tract infections and extra-pulmonary manifestations (1–3). The Coronavirus Disease 2019 (COVID-19), first reported in Wuhan, China, has raised acute and grave global concern since December 2019 (4, 5). On March 11, 2020, the world health organization (WHO) officially declared a global pandemic status for COVID-19, which is a great threat to people’s health and social stability. In the early stages of COVID-19, severe acute respiratory infection symptoms occurred, and some patients rapidly developed acute respiratory distress syndrome (ARDS), acute respiratory failure, and other serious complications (6, 7). There is considerable evidence to show that immunopathological changes, including diminished lymphocytes and elevated cytokines, are important drivers of disease progression and death of COVID-19 patients, especially those who are critically ill (8). Early detection and control of cytokine storms may effectively prevent disease progression and reduce the mortality rate. This review will summarize research progress on cytokine storms occurring in COVID-19 as well as potential intervention strategies.
The cytokine storm, previously reported in rheumatoid arthritis and graft-versus-host disease (GVHD), has been used to describe the overactive immune responses that can be triggered by a variety of factors, such as virus infection, autoimmune disease, and immunotherapies (8–10). Under the normal physiological state, the levels of pro-inflammatory cytokines and anti-inflammatory cytokines in the body are kept in relative balance, which can be broken by abnormal activation of a variety of immune cells (such as dendritic cells, macrophages, and lymphocytes) during viral infections. These abnormally activated immune cells could release large amounts of cytokines, among which the pro-inflammatory cytokines could promote more immune cells in a positive feedback loop. The formation of cytokine storm leads to “suicide attack” that not only contributes the elimination of pathogenic microorganisms but also causes tissue toxicities affecting a wide variety of organs (Table 1) (9). The cytokine release syndrome (CRS), a kind of systemic inflammation syndrome caused by cytokine storm, was previously observed in patients infected with SARS-CoV and MERS-CoV, as well as in leukemia patients receiving engineered T cell therapy (8, 9, 11, 12). Mild cases are characterized by fever, fatigue, headache, rash, arthralgia, and myalgia. Patients with more severe symptoms usually present with high fever, headache, fatigue, diffuse intravascular coagulation (DIC), shock, multiple organ failure (MOF), or even death (9, 11). Common laboratory abnormalities include cytopenia, elevated creatinine and liver enzymes, high levels of C-reactive protein (CRP), and deranged coagulation parameters (9, 11). Lee et al. reported a modified grading system for the severity of CRS regardless of the inciting agent, which defined mild, moderate, severe, life-threatening symptoms, and even death. This grading system is also used to guide clinical decisions in CRS (11). Vigilant supportive care is recommended for every grade; immunosuppression should be used in all patients with grade 3 or 4 CRS and instituted earlier in patients with extensive comorbidities or the elderly (11).
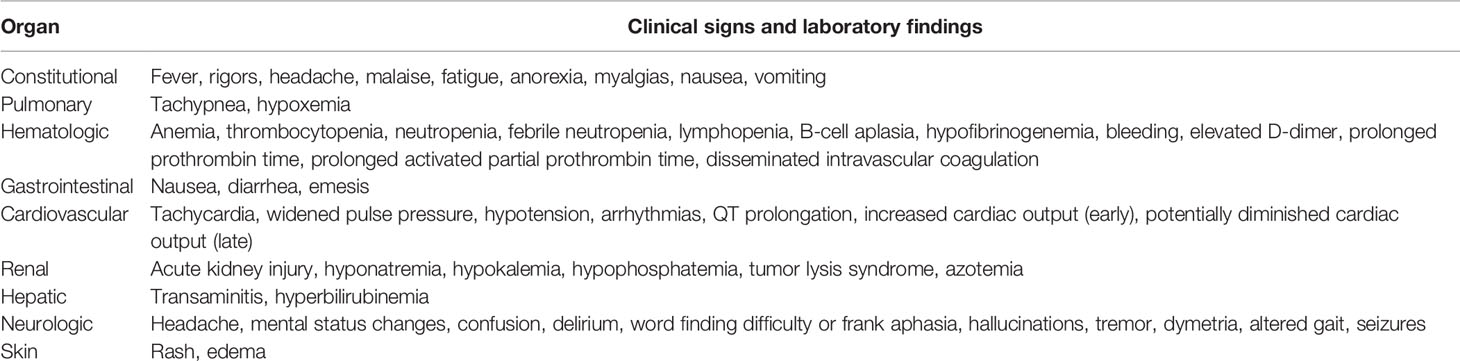
Table 1 Clinical signs and laboratory findings about cytokine storms.
The virus can promote the activation of immune cells (such as T cells, B cells, macrophages, dendritic cells, neutrophils, monocytes) and resident tissue cells, resulting in the production of large amounts of inflammatory cytokines (13, 14). During the flu virus infection, innate immune responses get started through the cascade amplification reactions of interferon stimulated gene expression, and type | interferon (IFN) is mainly produced by monocytes, macrophages and dendritic cells (15). Serum levels of interleukin 8 (IL-8), IP-10 (interferon-induced protein 10), MCP-1 (monocyte chemoattractant protein-1), MIP-1 (macrophage inflammatory protein-1), MIG (monokine induced by IFN-γ) and CXCL-9 (CXC chemokine ligand-9) were abnormally elevated in H5N1 influenza virus infection, while IL-8, IL-9, IL-17, IL-6, IL-15, TNF-α (tumor necrosis factor-α), IL-10 were increased in H1N1 influenza virus infection (16–18). Earlier researches demonstrated that serum levels of proinflammatory factors IFN-γ, IL1β, IL-6, IL-12, IL-18, IP-10, MCP-1, and CCL2 (CC chemokine ligand-2), CXCL-10 and IL-8 are positively correlated with lung inflammation and extensive lung tissue injury in SARS patients (19–21). Whereas, the levels of serum pro-inflammatory cytokines IL-6, IFN-γ, TNF-α, IL-15, IL-17, and chemokines IL-8, CXCL-10, and CCL5 were significantly increased in severe MERS patients (22, 23). Among numerous molecules that increase in virally-mediated cytokine storms, IL-6, IFN-γ, IL-1β, IL-8, IL-10, and TNF-α are of crucial importance (9, 24, 25). The occurrence of cytokine storm has been reported to be one of the main causes of death in patients with SARS-CoV, MERS-CoV, and influenza virus infections (8, 26). Similarly, cytokine storm is also a common feature of severe cases in COVID-19, and elevated levels of serum IL-6 and CRP correlate with respiratory failure, ARDS, MOF and adverse clinical outcomes (27, 28).
Both damage-associated molecular patterns (DAMPs) and pathogen-associated molecular patterns (PAMPs) are produced upon viral infection, which can activate antiviral responses in neighboring cells as well as recruit innate and adaptive immune cells, such as macrophages, natural killer (NK) cells, and gamma-delta T (γδ T) cells (Figure 1) (24, 29–33). Downstream production of interferons promotes intracellular antiviral defenses in neighboring epithelial cells which may limit viral dissemination, while the release of IL-6 and IL-1β from other immune cells promotes recruitment of neutrophils and T cells (29). Subsequently, the activation of T cells or lysis of immune cells induces secretion of IFN-γ and TNF-α, leading to the activation of immune cells and endothelial cells with further release of pro-inflammatory cytokines in a positive feedback loop manner (9). Although these inflammatory cytokines promote T follicular helper (Tfh) cell differentiation, B cell germinal center formation and antibody production, as well as Th1 (T helper 1) cell differentiation and cytotoxic CD8+ T cell generation to help viral removal, tissue damage caused by them cannot be ignored (34, 35). Activated neutrophils release leukotrienes and reactive oxygen species (ROS) that induce local pneumocyte and endothelial injury, directly leading to acute lung injury (29). Inflammatory mediators promote neutrophil release of nuclear deoxyribonucleic acid (DNA) to form neutrophil extracellular traps (NETs) which can snare pathogens as well as contribute to thrombi formation (33). This process, termed immuno-thrombosis, can also amplify the production of cytokines and is exemplified by links of thrombin with inflammasome activation and production of IL-1 (36). As vascular endothelial cells would be exposed to circulating cytokines and other immune mediators, coagulation disorders (such as capillary leak syndrome, thrombus formation, and even DIC) can also be caused by endothelial cell dysfunction in cytokine storms, indicating the crosstalk between hemostasis and cytokines (24, 33). High levels of circulating inflammatory cytokines can cause cell death as well as tissue damage, whereas their promotion of macrophages activation can lead to erythro-phagocytosis and anemia (24, 33). The successive occurrences of acute lung injury, abnormal alterations in vascular hemostasis, and cytokine-mediated tissue damage can eventually result in MOF (24, 33, 37).
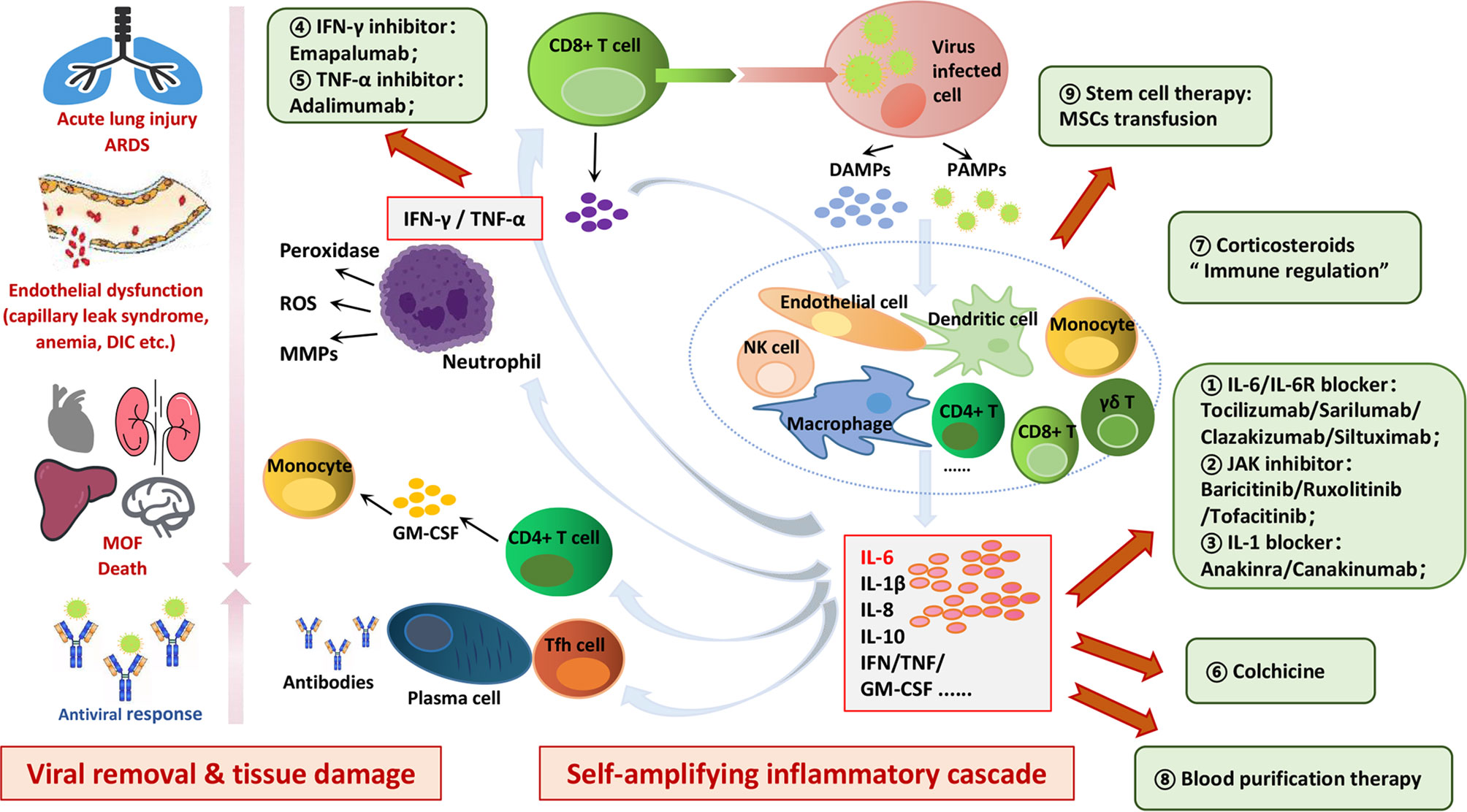
Figure 1 Mechanisms and hazards of cytokine storms induced in COVID-19 and potential therapeutic targets. Viral infection can induce antiviral responses in neighboring cells as well as recruit innate and adaptive immune cells, such as macrophages, dendritic cells, T cells, B cells and NK cells, leading to self-amplifying inflammatory cascade in a positive feedback loop manner. Cytokine storm not only limits further spread of virus in the body but also induces secondary tissue damage through the secretion of a large number of active mediators and inflammatory factors. The successive occurrences of acute lung injury, abnormal alterations in vascular hemostasis, and cytokine-mediated tissue damage can eventually result in MOF. Potential therapeutic targets to control cytokines storms in COVID-19 are as follows: IL-6/IL-6R blocker; JAK inhibitor; IL-1 blocker; IFN-γ inhibitor; TNF-α inhibitor; colchicine; corticosteroids; blood purification therapy; stem cell therapy.
As discussed above, cytokine storm not only limits further spread of virus but also induces secondary tissue damage through the secretion of large amounts of active mediators and inflammatory factors (Figure 1) (24, 29–33, 35, 38, 39). Thus, it can be seen that inhibition of this self-amplifying inflammatory cascade may not only control tissue damage, but also impair viral clearance. Unlike that in viral infection, the occurrence of cytokine storm in CAR-T therapy is secondary to T cell-mediated killing of tumor cells, and inhibition of this self-amplifying inflammatory cascade has no influence on therapeutic efficacy (9, 29). Nevertheless, it has been proved that antiviral immune responses and tissue toxicity could be at least partially uncoupled; therefore, inhibition of select arms of innate immune responses could limit tissue toxicity while not greatly suppressing ongoing antiviral immunity (29).
The incubation period of COVID-19 patients ranged from 1 to 14 days, and mostly from 3 to 7 days (8, 40). Common symptoms at onset of illness were fever, dry cough, myalgia, fatigue, dyspnea, and anorexia; however, a few patients presented initially with atypical symptoms, such as diarrhea and nausea (6, 40). Most patients had good results with treatment, while the elderly patients and those with chronic diseases usually had poor prognoses. Although most patients with COVID-19 had mild and moderate symptoms, severe and critically ill patients progressed rapidly to acute respiratory failure, ARDS, metabolic acidosis, coagulopathy, septic shock, and MOF (7, 40–42). The autopsy report in the journal The Lancet Respiratory Medicine showed typical ARDS-like lung injury with lymphocyte infiltration, liver injury with moderate micro-vesicular steatosis, mild lobular and portal activity (43). COVID-19 patients usually revealed significantly reduced lymphocyte counts and increased inflammatory factors, especially those with severe illnesses (6, 40, 44). Wang et al. reported that the neutrophil count and D-dimer continued to increase in non-survivors, whereas lymphocyte counts continued to decrease until death occurred (40). Neutrophilia may be related to cytokine storms induced by virus invasion, and coagulation activation may be related to sustained inflammatory responses (40).
Huang et al. observed that patients in intensive care unit (ICU) showed higher levels of plasma inflammatory cytokines IL-2, IL-7, IL-10, G-CSF (granulocyte colony-stimulating factor), IFN-γ and MCP and TNF-α than non-ICU patients (6), indicating the positive correlation between the cytokine storm and the severity of illness. These cytokines suggested not only Th1 responses but also Th2 responses in COVID-19, which differed from SARS-CoV infections (6). After being infected with the SARS-CoV-2, CD4+ T cells were activated and differentiated into Th1 cells to secrete pro-inflammatory cytokines, such as IL-6, IFN-γ, and GM-CSF (granulocyte-macrophage colony stimulating factor) (6, 45). GM-CSF could activate mononuclear cells to promote further release of IL-6 and other pro-inflammatory cytokines, leading to the generation of cytokine storms (45). Therefore, IL-6 and GM-CSF released by T lymphocytes and mononuclear cells may be the key link of cytokine storm in COVID-19 (45). Moreover, the activation of monocytes may suggest that the cytokine storm in COVID-19 is closely related to the destruction of the balance between innate and adaptive immunity.
Recent studies also showed that the level of IL-6 in severe cases was significantly higher than that in mild and moderate cases, but the levels of CD4+ T cells, CD8+ T cells and NK cells were decreased, indicating the immunosuppression in severe COVID-19 patients (44). Although peripheral CD4+ T cells and CD8+ T cells were significantly reduced, the number of Th17 cells increased and CD8+ T cells were highly cytotoxic, which further suggested that cytokine storms may aggravate tissue damage (43). Meanwhile, T lymphocyte cells were excessively activated during the cytokine storm in COVID-19 patients, which may be accompanied by severe immune dysfunctions (43). The cytokine storm can directly damage the pulmonary capillary mucosa, promote alveolar edema, and further induce the diffusion of inflammatory cytokines, thus resulting in the damage of alveolar structure and pulmonary ventilation dysfunction (25, 46). In addition, the cytokine storm is associated with the sequence and severity of organ dysfunction in multiple organ dysfunction syndrome (MODS) (37). Therefore, the cytokine storm may be an important factor that affects the fate of patients with COVID-19 pneumonia.
During the process of antiviral immune responses, innate and adaptive immune responses interact with each other and cooperate closely to produce immune protection (47). There is a time limit for adaptive immune responses, which usually gets initiated 4 to 7 days after infection. Unlike adaptive immune responses, innate immune responses occur immediately after infection and are fully involved in virus clearance. However, the innate immunity is relatively weak in virus clearance, and adaptive immunity is the key factor in complete elimination of the virus (47). If the body does not generate effective adaptive antiviral responses in time to clear the virus, the innate immune responses will be strengthened, which cannot eliminate the virus effectively and even lead to systematic inflammation responses with uncontrolled release of inflammatory cytokines (48, 49). The latest studies have shown that the average age of severe and critically ill patients is higher than that of mild cases (66-years old vs. 51-years old), and severe cases are more likely to have other chronic diseases (72.2% vs. 37.3%) (40, 50). As for the elderly patients and those with chronic diseases, it takes a longer period of time to generate effective adaptive immune responses due to the deterioration of immune functions. These patients only rely on strengthening the innate antiviral immune responses in the early stages of infection, leading to a higher risk of cytokine storms, earlier onset of severe illness, and a higher mortality rate. Although the kinetics of the responses to SARS-CoV-2 fit with models of the induction of conventional antiviral immunity, it is still unclear whether immune hyperactivity is due to ongoing viral replication or immune dysregulation (33). Pyroptosis is a highly inflammatory and caspase-1-dependent form of programmed cell death that occurs most frequently upon infection with intracellular pathogens and is a part of the antimicrobial responses, which may also play a role in COVID-19 pathogenesis (51, 52). Rapid viral replication that causes increased pyroptosis may lead to a massive release of inflammatory mediators (51). Taken together, viral escape to avoid anti-viral immunity, together with genetic or acquired defects in host defense, may impair viral clearance, resulting in inappropriate immune activation and consequently causing cytokine storms (52). In a word, the exaggerated activation of innate immunity may be an important factor in the formation of cytokine storms in COVID-19 (29).
Angiotensin converting enzyme 2 (ACE2) primarily catalyzes the breakdown of angiotensin II (AngII) to maintain the homeostasis of renin-angiotensin-aldosterone system (RAAS) as a pivotal counter-regulator, which is crucial for the physiology and pathology of most human organs (53, 54). Significant to COVID-19, ACE2 has been established as the functional host receptor for SARS-CoV-2, and many factors have proved to be associated with both altered ACE2 expression and disease severity and progression, including age, sex, ethnicity, medication, and several co-morbidities (such as cardiovascular disease, metabolic syndrome, and lung cancer) (53–57). Recent studies have also revealed potential roles of ACE2 in regulating immune responses rather than merely being a viral-binding receptor in COVID-19 (53–55, 58–61). Chen’s team found the expression axis “mir-125b-5p-ACE2-IL-6” existed in lung adenocarcinoma, in which mir-125b-5p inhibited the expression of IL-6 through promoting the up-regulation of ACE2 (58). Once bound by SARS-CoV-2, the ACE2 expression (including mRNA level and enzyme activity) on the surface of host cells were significantly decreased, and then IL-6 in the toll-like receptor signaling pathway might influence the immune system as the downstream effector (53, 54, 58). Therefore, the dysregulation of ACE2 induced by SARS-CoV-2 infection may further cause cytokine storms and pneumonia, and targeting to the upstream regulator mir-125b-5p may provide a new way for the control of COVID-19 (58, 60). More interestingly, the spike protein of SARS-CoV has been previously demonstrated to downregulate ACE2 expression, thus resulting in over-production of AngII (the downstream of ACE2) by the related enzyme ACE (62, 63). Similarly, it could be hypothesized that SARS-CoV-2 may downregulate ACE2 receptors and thereby leading to an over-production of AngII, which may be another possible explanation of cytokine storm in COVID-19 (59, 61). ACE2 molecules on the cell surface are occupied by SARS-CoV-2, and then AngII increases due to a reduction of ACE2-mediated degradation (59, 61). SARS-CoV-2 itself activates nuclear factor kappa B (NF-κB) via pattern recognition receptors (PPRs), and the accumulated AngII in turn induces the activation of the IL-6 amplifier through enhanced activation of NF-κB pathway and IL-6-STAT3 (signal transducers and activators of transcription family 3) axis (61). IL-6 is a key factor in this positive feedback loop, ultimately leading to the release of cytokines out of control (64). More importantly, IL-6 is a major functional marker of cellular senescence, and the age-dependent enhancement of the IL-6 amplifier may correspond to the age-dependent increase of COVID-19 mortality (61, 64).
Lessons should be learned from the outbreak of SARS-CoV and MERS-CoV to accumulate valuable experience and insights on how to effectively treat COVID-19 pneumonia patients. There are three progressive stages upon SARS-CoV-2 infection: early infection, pulmonary phase, and hyper-inflammation phase (65). Targeted treatments are urgently needed to prevent the occurrence of cytokine storms, and the early infection stage with no or mild symptoms is the key period for active treatment to control further deterioration (65). Antiviral drugs that inhibit virus transmission and destroy virus replication can reduce direct cell damage caused by COVID-19, and appropriate combinations with immunoregulatory therapies that inhibit hyper-activated inflammatory responses can resist cytokine storms triggered by the virus (Figure 1 and Table 2) (72, 73). Multiple clinical trials have been initiated to investigate potential interventions to control cytokine storms in patients with COVID-19, mainly including direct inhibition of cytokines and immunomodulatory therapies (Figure 1 and Table 2).
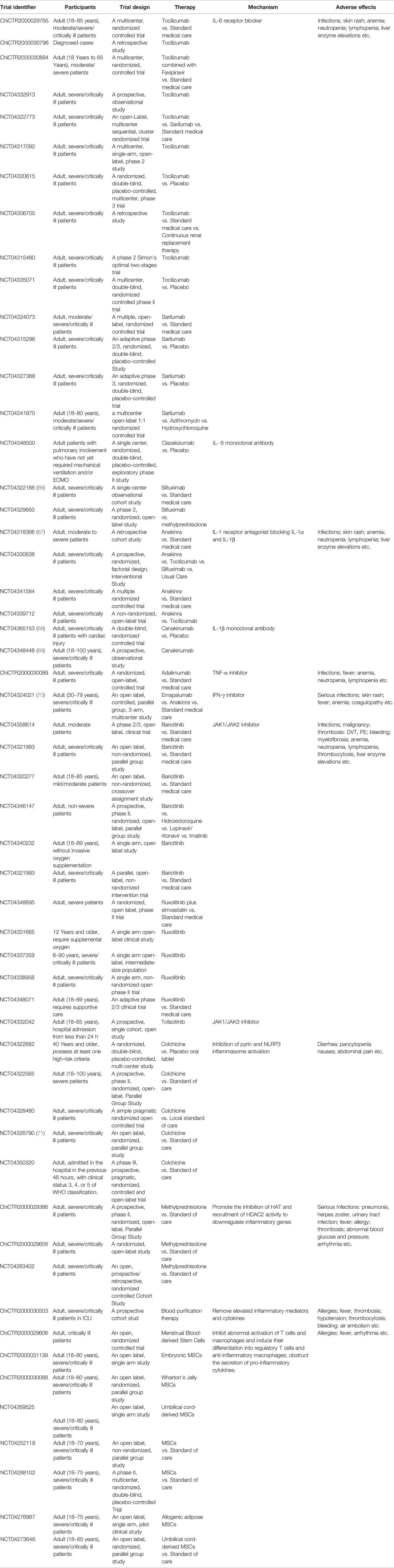
Table 2 Ongoing clinical trials of strategies to control cytokine storms in COVID-19.
One meta-analysis of mean IL-6 concentrations demonstrated 2.9-fold higher levels in patients with complicated COVID-19 compared with those with non-complicated disease (74), and another meta-analysis also reported the relation between IL-6 levels and severe condition (75), indicating that IL-6 was a good indicator of poor prognosis in COVID-19 (74). At present, blockers of IL-6/IL-6R have been preliminarily applied in a series of ongoing clinical trials of COVID-19 and further multi-center clinical trials are being carried out (Table 2). Tocilizumab (a kind of IL-6 receptor blocker, IL-6R), first approved for rheumatic conditions, can effectively reverse iatrogenic cytokine storms which are caused by CAR-T therapy in patients with hematological malignancies (11, 76). One clinical trial from China (ChiCTR2000029765) reported that tocilizumab made rapid improvements in fever control and respiratory functions in 21 severe patients with COVID-19, and all participants including two seriously ill patients recovered and were discharged from the hospital (77, 78). Roumier et al. reported their experience regarding tocilizumab in 30 COVID-19 patients, suggesting that tocilizumab significantly reduced mechanical ventilation requirements (odd ratio, OR=0.42) and risk of subsequent ICU admissions (OR=0.17) (79). Toniati’s group published a single center study of 100 COVID-19 patients in Italy and also demonstrated that the response to tocilizumab was rapid, sustained, and associated with significant clinical improvements (80). A systematic review and meta-analysis of observational studies found decreased mortality in COVID-19 patients treated with tocilizumab (81). In addition, IL-6 blockade with tocilizumab does not impair the viral specific antibody responses despite of a delayed viral clearance driven by a higher initial viral load, indicating the safety of tocilizumab in patients with COVID-19 (82). Sarilumab is another kind of IL-6R blocker that is being investigated in SARS-CoV-2 infection (83, 84), which may reflect a possible clinical benefit regarding early intervention with IL-6-modulatory therapies for COVID-19 (85). Although not yet approved by Food and Drug Administration (FDA), clazakizumab (a monoclonal antibody against human IL-6) may be helpful in inhibiting the cytokine storms, and related clinical trials are underway worldwide (86). It is also reported that patients with rapidly progressing COVID-19 respiratory failure requiring ventilatory support may benefit from treatment with siltuximab (IL-6 monoclonal antibody) because of reduced mortality and cytokine-driven hyperinflammation (NCT04322188) (66).
There are three important cytokines of IL-1 family in cytokine storms: IL-1β, IL-18, and IL-33, among which the block of IL-1β to counteract the cytokine storms is of great concern (9, 29). Anakinra, a kind of IL-1 receptor antagonist that blocks activity of both IL-1α and IL-1β, has been approved by the FDA and the EDA (European Drug Administration) for the treatment of rheumatoid arthritis, systemic-onset juvenile idiopathic arthritis, and familial Mediterranean fever (67, 87, 88). Anakinra can also be used in the treatment of cytokine storms caused by infection, significantly improving the survival rate of severe sepsis (89). Compared with other cytokine blockers, anakinra has shorter half-life; thus, it is safer and more suitable for severe and critically ill patients. A retrospective cohort study (NCT04324021) reported that high doses of intravenous anakinra inhibit systemic inflammation and were associated with progressive improvement in respiratory function in severe patients with COVID-19 (70). Other clinical trials are also under way to evaluate the use of anakinra in COVID-19 (NCT04330638, NCT04341584, NCT04339712 etc.). Canakinumab, a monoclonal antibody selectively targeting IL-1β, is also being investigated in the treatment for COVID-19. It was proved that canakinumab was safe, well tolerated, and associated with a rapid reduction in the systemic inflammatory response and an improvement in cardiac and respiratory function (68, 69). Nevertheless, strengthened evidence for the application of anakinra and canakinumab in COVID-19 are required in further random controlled trials.
There is no clinical evidence nor any registered clinical trials assessing the possibility of IL-18 blockers and IL-33 blockers in COVID-19. TNF-α and IFN-γ are also key inflammatory cytokines and attractive targets in the control of cytokine storms (6, 90, 91), and clinical trials are ongoing to test these blockers in COVID-19 (ChiCTR2000030089, NCT04324021) (70, 92). JAK/STAT (janus kinase/signal transducers and activators of transcription) signal transduction pathway, a common downstream signaling pathway of various cytokines, can block multiple targeted cytokines at the same time if inhibited (93, 94). However, its possible side effects cannot be ignored, such as increased risk for pulmonary embolism (PE), liver enzyme elevations, hematological abnormalities and suppression of antiviral immunity (94–96). Several representative JAK inhibitors, such as tofacitinib, baricitinib, and ruxolitinib, are currently being investigated to determine whether they can be applied to the treatment of COVID-19 (NCT04332042, NCT04348695, NCT04321993, NCT04348695, etc.) (94). Baricitinib and ruxolitinib are selective inhibitors of JAK1/JAK2 which is responsible for multiple cellular signals including the proinflammatory IL-6 and works as immunomodulator decreasing the cytotoxic T lymphocytes and increasing the regulatory T cells (97, 98). A phase 2/3 clinical trial (NCT04358614) showed that all clinical characteristics and respiratory function parameters significantly improved in the baricitinib-treated group compared to the baseline, and no serious infections, cardiovascular and hematologic adverse effects occurred after treatment (29). Although tofacitinib is a selective inhibitor of JAK1/JAK3, it is suggested that for patients not on tofacitinib that this be initiated, but rather for those already on it that it can potentially be continued during a pandemic (99). Colchicine can inhibit the inflammasome activation of pyrin and NLRP3 (NLR Family Pyrin Domain Containing 3), and are also currently under way to be evaluated in the treatment of COVID-19 (71, 100, 101). A single-center cohort study showed that patients treated with colchicine had a better survival rate as compared with standard care at 21 days of follow-up, and the adverse effects were similar for two groups, which may support the rationale of use of colchicine for the treatment of COVID-19 (100). Another randomized clinical trial of 105 COVID-19 patients also suggested that low-dose of colchicine combined anti-inflammatory action with a favorable safety profile (71). Moreover, it is also recommended as a therapeutic option in patients who have contraindications to other drugs or in the context of shortage/unavailability of anti-viral drugs (such as in underdeveloped countries) due to high availability (101).
Corticosteroids, a type of steroid hormones, exhibit anti-inflammatory activity via binding to the cytoplasmic corticosteroid receptor, which leads to inhibitions of HAT (histone acetyltransferase) and recruitment of HDAC2 (histone deacetylases 2) activity to downregulate inflammatory genes (102). Thus, corticosteroids have been widely used to control cytokine storms. Data from a limited-size trial showed that the early use of low or medium doses of methylprednisolone had a positive effect for patients with severe COVID-19 (103). A single-blind, randomized, controlled trial in Iran (trial identifier: IRCT20200404046947N1) suggested that methylprednisolone pulse could be an efficient therapeutic agent for hospitalized severe COVID-19 patients at the pulmonary phase (104). Although there was no significant difference in mortality, patients receiving methylprednisolone treatment seemed to be with a faster improvement of oxygen saturation, decrease in CRP and IL-6 level, and less demand for invasive ventilation (104, 105). However, adverse effects (including serious infection and edema etc.) were also observed in several patients after the methylprednisolone treatment (103–105). In addition, there are heated debates as to whether corticosteroid therapy will delay viral clearance in COVID-19 (106, 107). Therefore, the pros and cons should be carefully weighed before using glucocorticoids in the treatment of COVID-19 patients. It is very important for clinicians to master the time and dose of corticosteroids for the treatment of severe patients, especially before the infection occurs. In addition, great caution should be exercised for patients who already have hypoxemia for various reasons or those who take glucocorticoids regularly due to other chronic diseases.
It has been demonstrated that the blood purification system, such as plasma exchange, adsorption, perfusion, blood/plasma filtration, can remove inflammatory factors and then reduce tissue damage of hyper-activated inflammatory responses (108). Li et al. demonstrated that the artificial liver blood purification system could rapidly remove inflammatory mediators, block cytokine storms, favor the balance of fluid, electrolytes and acid-base, and thus improve treatment efficacy in critical illnesses (109, 110). Ma et al. reported that three COVID-19 patients who received blood purification therapy were tolerable and effective in limited experiences (111). Successful recovery of a severe patient was also presented in one case report (112). Yang’s group developed a blood purification protocol for patients with severe COVID-19 based on previous experience in SARS and MERS, including four major steps: (i) to assess whether patients with severe COVID-19 require blood purification; (ii) to prescribe a blood purification treatment for patients with COVID-19; (iii) to monitor and adjust parameters of blood purification; (iv) to evaluate the timing of discontinuation of blood purification (113). Last but not least, possible adverse effects in blood purification therapy (such as allergies, thrombocytosis, bleeding, air embolism etc.) should be timely identified and controlled to ensure safe and effective treatment (109–113).
As an important member of the stem cell family, mesenchymal stem cells (MSCs) not only have potentials for self-renewal and multidirectional differentiation but also have strong anti-inflammatory and immune regulatory functions (114–117). In addition, MSCs inhibit abnormal activation of T lymphocyte cells and macrophages and induce their differentiation into regulatory T cells and anti-inflammatory macrophages (117). MSCs also obstruct the secretion of pro-inflammatory cytokines, thereby reducing the occurrence of cytokine storms (114, 115, 117, 118). Currently, over thirty clinical trials about intravenous administration of MSCs in COVID-19 patients have been officially registered (www.clinicaltrials.gov), but most of them are under the recruitment phase. Recently, Zhao et al. reported the results of seven severe and critically ill patients with COVID-19 receiving MSCs transplantation therapy, which showed improved prognosis and effective avoidance of cytokine storms with no obvious side effects (119). Furthermore, other stem cell therapies have been initiated in clinical trials, such as human menstrual blood-derived stem cells (ChiCTR2000029606) and embryonic stem cells (ChiCTR2000031139).
COVID-19 has been listed as an international public health emergency by WHO and the treatment of severe and critically ill patients is the burning issue in current prevention and control. As cytokine storm is one of the most common causes of mortality in COVID-19, therapeutic approaches to manage cytokine storm may provide a novel avenue to decrease the COVID-19 associated morbidity and mortality. Hyperactivated innate immune responses, dysregulation of ACE2 expression and its downstream pathway may be possible mechanisms. In the treatment of COVID-19, high levels of attention must be paid to the identification of the occurrence cytokine storm. Tailored immunoregulatory therapies to control and resist the progress of cytokine storms in early stages of COVID-19 can greatly improve prognosis and reduce mortality rates. Although several therapies used to control cytokine storm have entered the stage of clinical trials for the treatment of COVID-19, the limited source and potential adverse effects have delayed widespread application in clinical treatment. Moreover, the best timing of anti-cytokine storm therapies remains to be explored, as well as novel therapeutic methods which are more effective and tolerated.
LT, YH, and HM: writing, original draft preparation. LT: table and figure preparation and editing. ZY, YH, and HM: review and editing. All authors contributed to the article and approved the submitted version.
This research was supported by funds from the Key Special Project of Ministry of Science and Technology of China (no. 2020YFC0845700), Scientific Research Projects of Chinese Academy of Engineering of China no. 2020-XY-70 (2020-KYGG-01-07), and Fundamental Research Funds for the Central Universities of China (no. 2020kfyXGYJ029).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Ren LL, Wang YM, Wu ZQ, Xiang ZC, Guo L, Xu T, et al. Identification of a novel coronavirus causing severe pneumonia in human: a descriptive study. Chin Med J (Engl) (2020) 133(9):1015–24. doi: 10.1097/cm9.0000000000000722
2. Zaki AM, van Boheemen S, Bestebroer TM, Osterhaus ADME, Fouchier RAM. Isolation of a novel coronavirus from a man with pneumonia in Saudi Arabia. New Engl J Med (2012) 367(19):1814–20. doi: 10.1056/NEJMoa1211721
3. Drosten C, Günther S, Preiser W, van der Werf S, Brodt H-R, Becker S, et al. Identification of a novel coronavirus in patients with severe acute respiratory syndrome. New Engl J Med (2003) 348(20):1967–76. doi: 10.1056/NEJMoa030747
4. Bogoch II, Watts A, Thomas-Bachli A, Huber C, Kraemer MUG, Khan K. Potential for global spread of a novel coronavirus from China. J Travel Med (2020) 27(2):taaa011. doi: 10.1093/jtm/taaa011
5. Wang C, Horby PW, Hayden FG, Gao GF. A novel coronavirus outbreak of global health concern. Lancet (2020) 395(10223):470–3. doi: 10.1016/S0140-6736(20)30185-9
6. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet (London England) (2020) 395(10223):497–506. doi: 10.1016/S0140-6736(20)30183-5
7. Guan W-J, Ni Z-Y, Hu Y, Liang W-H, Ou C-Q, He J-X, et al. Clinical Characteristics of Coronavirus Disease 2019 in China. New Engl J Med (2020) 382(18):1708–20. doi: 10.1056/NEJMoa2002032.
8. Channappanavar R, Perlman S. Pathogenic human coronavirus infections: causes and consequences of cytokine storm and immunopathology. Semin Immunopathol (2017) 39(5):529–39. doi: 10.1007/s00281-017-0629-x
9. Shimabukuro-Vornhagen A, Gödel P, Subklewe M, Stemmler HJ, Schlößer HA, Schlaak M, et al. Cytokine release syndrome. J Immunother Cancer (2018) 6(1):56. doi: 10.1186/s40425-018-0343-9
10. Ferrara JL, Abhyankar S, Gilliland DG. Cytokine storm of graft-versus-host disease: a critical effector role for interleukin-1. Transplant Proc (1993) 25(1 Pt 2):1216–7.
11. Lee DW, Gardner R, Porter DL, Louis CU, Ahmed N, Jensen M, et al. Current concepts in the diagnosis and management of cytokine release syndrome. Blood (2014) 124(2):188–95. doi: 10.1182/blood-2014-05-552729
12. Fehr AR, Channappanavar R, Perlman S. Middle East Respiratory Syndrome: Emergence of a Pathogenic Human Coronavirus. Annu Rev Med (2017) 68:387–99. doi: 10.1146/annurev-med-051215-031152
13. Krischuns T, Günl F, Henschel L, Binder M, Willemsen J, Schloer S, et al. Phosphorylation of TRIM28 Enhances the Expression of IFN-β and Proinflammatory Cytokines During HPAIV Infection of Human Lung Epithelial Cells. Front Immunol (2018) 9:2229. doi: 10.3389/fimmu.2018.02229
14. Behrens EM, Koretzky GA. Review: Cytokine Storm Syndrome: Looking Toward the Precision Medicine Era. Arthritis Rheumatol (2017) 69(6):1135–43. doi: 10.1002/art.40071
15. Klinkhammer J, Schnepf D, Ye L, Schwaderlapp M, Gad HH, Hartmann R, et al. IFN-λ prevents influenza virus spread from the upper airways to the lungs and limits virus transmission. Elife (2018) 7:e33354. doi: 10.7554/eLife.33354
16. Liu Q, Zhou YH, Yang ZQ. The cytokine storm of severe influenza and development of immunomodulatory therapy. Cell Mol Immunol (2016) 13(1):3–10. doi: 10.1038/cmi.2015.74
18. Thomas M, Mani RS, Philip M, Adhikary R, Joshi S, Revadi SS, et al. Proinflammatory chemokines are major mediators of exuberant immune response associated with Influenza A (H1N1) pdm09 virus infection. J Med Virol (2017) 89(8):1373–81. doi: 10.1002/jmv.24781
19. Wong CK, LAM CWK, WU AKL, IP WK, LEE NLS, CHAN IHS, et al. Plasma inflammatory cytokines and chemokines in severe acute respiratory syndrome. Clin Exp Immunol (2004) 136(1):95–103. doi: 10.1111/j.1365-2249.2004.02415.x
20. Zhang Y, Li J, Zhan Y, Wu L, Yu X, Zhang W, et al. Analysis of serum cytokines in patients with severe acute respiratory syndrome. Infect Immun (2004) 72(8):4410–5. doi: 10.1128/iai.72.8.4410-4415.2004
21. Chien JY, Hsueh PR, Cheng WC, Yu CJ, Yang PC. Temporal changes in cytokine/chemokine profiles and pulmonary involvement in severe acute respiratory syndrome. Respirology (2006) 11(6):715–22. doi: 10.1111/j.1440-1843.2006.00942.x
22. Mahallawi WH, Khabour OF, Zhang Q, Makhdoum HM, Suliman BAJC. MERS-CoV infection in humans is associated with a pro-inflammatory Th1 and Th17 cytokine profile. Cytokine (2018) 104:8–13. doi: 10.1016/j.cyto.2018.01.025
23. Kim ES, Choe PG, Park WB, Oh HS, Kim EJ, Nam EY, et al. Clinical Progression and Cytokine Profiles of Middle East Respiratory Syndrome Coronavirus Infection. J Korean Med Sci (2016) 31(11):1717–25. doi: 10.3346/jkms.2016.31.11.1717
24. Chousterman BG, Swirski FK, Weber GF. Cytokine storm and sepsis disease pathogenesis. Semin Immunopathol (2017) 39(5):517–28. doi: 10.1007/s00281-017-0639-8
25. Tisoncik JR, Korth MJ, Simmons CP, Farrar J, Martin TR, Katze MG. Into the eye of the cytokine storm. Microbiol Mol Biol Rev MMBR (2012) 76(1):16–32. doi: 10.1128/MMBR.05015-11
26. Dawood FS, Iuliano AD, Reed C, Meltzer MI, Shay DK, Cheng PY, et al. Estimated global mortality associated with the first 12 months of 2009 pandemic influenza A H1N1 virus circulation: a modelling study. Lancet Infect Dis (2012) 12(9):687–95. doi: 10.1016/s1473-3099(12)70121-4
27. Chen G, Wu D, Guo W, Cao Y, Huang D, Wang H, et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J Clin Invest (2020) 130(5):2620–9. doi: 10.1172/jci137244
28. Ruan Q, Yang K, Wang W, Jiang L, Song J. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med (2020) 46(5):846–8. doi: 10.1007/s00134-020-05991-x
29. Vardhana SA, Wolchok JD. The many faces of the anti-COVID immune response. J Exp Med (6) (2020) 217(216):e20200678. doi: 10.1084/jem.20200678
30. Akira S, Uematsu S, Takeuchi O. Pathogen recognition and innate immunity. Cell (2006) 124(4):783–801. doi: 10.1016/j.cell.2006.02.015
31. Kawai T, Akira S. Innate immune recognition of viral infection. Nat Immunol (2006) 7(2):131–7. doi: 10.1038/ni1303
32. Medzhitov R. Recognition of microorganisms and activation of the immune response. Nature (2007) 449(7164):819–26. doi: 10.1038/nature06246
33. Mangalmurti N, Hunter CA. Cytokine Storms: Understanding COVID-19. Immunity (2020) 53(1):19–25. doi: 10.1016/j.immuni.2020.06.017
34. Harker JA, Lewis GM, Mack L, Zuniga EI. Late interleukin-6 escalates T follicular helper cell responses and controls a chronic viral infection. Science (2011) 334(6057):825–9. doi: 10.1126/science.1208421
35. Azkur AK, Akdis M, Azkur D, Sokolowska M, van de Veen W, Brüggen MC, et al. Immune response to SARS-CoV-2 and mechanisms of immunopathological changes in COVID-19. Allergy (2020) 75(7):1564–81. doi: 10.1111/all.14364
36. Engelmann B, Massberg S. Thrombosis as an intravascular effector of innate immunity. Nat Rev Immunol (2013) 13(1):34–45. doi: 10.1038/nri3345
37. Wang H, Ma S. The cytokine storm and factors determining the sequence and severity of organ dysfunction in multiple organ dysfunction syndrome. Am J Emergency Med (2008) 26(6):711–5. doi: 10.1016/j.ajem.2007.10.031
38. Iwasaki A, Pillai PS. Innate immunity to influenza virus infection. Nat Rev Immunol (2014) 14(5):315–28. doi: 10.1038/nri3665
39. Betakova T, Kostrabova A, Lachova V, Turianova L. Cytokines Induced During Influenza Virus Infection. Curr Pharm Des (2017) 23(18):2616–22. doi: 10.2174/1381612823666170316123736
40. Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA (2020) 323(11):1061–9. doi: 10.1001/jama.2020.1585
41. Tang N, Li D, Wang X, Sun Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J Thromb Haemost (2020) 18(4):844–7. doi: 10.1111/jth.14768
42. Liao D, Zhou F, Luo L, Xu M, Wang H, Xia J, et al. Haematological characteristics and risk factors in the classification and prognosis evaluation of COVID-19: a retrospective cohort study. Lancet Haematol (2020) 7(9):e671–8. doi: 10.1016/s2352-3026(20)30217-9
43. Xu Z, Shi L, Wang Y, Zhang J, Huang L, Zhang C, et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir Med (2020) 8(4):420–2. doi: 10.1016/S2213-2600(20)30076-X
44. Wan S, Yi Q, Fan S, Lv J, Zhang X, Guo L, et al. Characteristics of lymphocyte subsets and cytokines in peripheral blood of 123 hospitalized patients with 2019 novel coronavirus pneumonia (NCP). medRxiv (2020) 2020.02.10.20021832. doi: 10.1101/2020.02.10.20021832.
45. Zhou Y, Fu B, Zheng X, Wang D, Zhao C, Qi Y, et al. Pathogenic T-cells and inflammatory monocytes incite inflammatory storms in severe COVID-19 patients. Natl Sci Rev (2020) 7(6):998–1002. doi: 10.1093/nsr/nwaa041
46. Zhang B, Swamy S, Balijepalli S, Panicker S, Mooliyil J, Sherman MA, et al. Direct pulmonary delivery of solubilized curcumin reduces severity of lethal pneumonia. FASEB J (2019) 33(12):13294–309. doi: 10.1096/fj.201901047RR
47. Iwasaki A, Medzhitov R. Regulation of adaptive immunity by the innate immune system. Science (2010) 327(5963):291–5. doi: 10.1126/science.1183021
48. Braciale TJ, Sun J, Kim TS. Regulating the adaptive immune response to respiratory virus infection. Nat Rev Immunol (2012) 12(4):295–305. doi: 10.1038/nri3166
49. Newton AH, Cardani A, Braciale TJ. The host immune response in respiratory virus infection: balancing virus clearance and immunopathology. Semin Immunopathol (2016) 38(4):471–82. doi: 10.1007/s00281-016-0558-0
50. Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet (2020) 395(10223):507–13. doi: 10.1016/s0140-6736(20)30211-7
51. Bergsbaken T, Fink SL, Cookson BT. Pyroptosis: host cell death and inflammation. Nat Rev Microbiol (2009) 7(2):99–109. doi: 10.1038/nrmicro2070
52. Soy M, Keser G, Atagündüz P, Tabak F, Atagündüz I, Kayhan S. Cytokine storm in COVID-19: pathogenesis and overview of anti-inflammatory agents used in treatment. Clin Rheumatol (2020) 39(7):2085–94. doi: 10.1007/s10067-020-05190-5
53. Datta PK, Liu F, Fischer T, Rappaport J, Qin X. SARS-CoV-2 pandemic and research gaps: Understanding SARS-CoV-2 interaction with the ACE2 receptor and implications for therapy. Theranostics (2020) 10(16):7448–64. doi: 10.7150/thno.48076
54. Li Y, Zhou W, Yang L, You R. Physiological and pathological regulation of ACE2, the SARS-CoV-2 receptor. Pharmacol Res (2020) 157:104833. doi: 10.1016/j.phrs.2020.104833
55. Bourgonje AR, Abdulle AE, Timens W, Hillebrands JL, Navis GJ, Gordijn SJ, et al. Angiotensin-converting enzyme 2 (ACE2), SARS-CoV-2 and the pathophysiology of coronavirus disease 2019 (COVID-19). J Pathol (2020) 251(3):228–48. doi: 10.1002/path.5471
56. Liang W, Guan W, Chen R, Wang W, Li J, Xu K, et al. Cancer patients in SARS-CoV-2 infection: a nationwide analysis in China. Lancet Oncol (2020) 21(3):335–7. doi: 10.1016/s1470-2045(20)30096-6
57. Jia X, Yin C, Lu S, Chen Y, Liu Q, Bai J, et al. Two Things about COVID-19 Might Need Attention. Preprints (2020) 2020020315. doi: 10.20944/preprints202002.0315.v1
58. Chen L, Zhong L. Lung Adenocarcinoma Patients Own Higher Risk of SARS-CoV-2 Infection. Preprints (2020) 2020020386.
59. Catanzaro M, Fagiani F, Racchi M, Corsini E, Govoni S, Lanni C. Immune response in COVID-19: addressing a pharmacological challenge by targeting pathways triggered by SARS-CoV-2. Signal Transduct Target Ther (2020) 5(1):84. doi: 10.1038/s41392-020-0191-1
60. Imai Y, Kuba K, Rao S, Huan Y, Guo F, Guan B, et al. Angiotensin-converting enzyme 2 protects from severe acute lung failure. Nature (2005) 436(7047):112–6. doi: 10.1038/nature03712
61. Hirano T, Murakami M. COVID-19: A New Virus, but a Familiar Receptor and Cytokine Release Syndrome. Immunity (2020) 52(5):731–3. doi: 10.1016/j.immuni.2020.04.003
62. Kuba K, Imai Y, Rao S, Gao H, Guo F, Guan B, et al. A crucial role of angiotensin converting enzyme 2 (ACE2) in SARS coronavirus-induced lung injury. Nat Med (2005) 11(8):875–9. doi: 10.1038/nm1267
63. Glowacka I, Bertram S, Herzog P, Pfefferle S, Steffen I, Muench MO, et al. Differential downregulation of ACE2 by the spike proteins of severe acute respiratory syndrome coronavirus and human coronavirus NL63. J Virol (2010) 84(2):1198–205. doi: 10.1128/jvi.01248-09
64. Murakami M, Kamimura D, Hirano T. Pleiotropy and Specificity: Insights from the Interleukin 6 Family of Cytokines. Immunity (2019) 50(4):812–31. doi: 10.1016/j.immuni.2019.03.027
65. Siddiqi HK, Mehra MR. COVID-19 illness in native and immunosuppressed states: A clinical-therapeutic staging proposal. J Heart Lung Transplant (2020) 39(5):405–7. doi: 10.1016/j.healun.2020.03.012
66. Gritti G, Raimondi F, Ripamonti D, Riva I, Landi F, Alborghetti L, et al. IL-6 signalling pathway inactivation with siltuximab in patients with COVID-19 respiratory failure: an observational cohort study. medRxiv (2020) 2020.2004.2001.20048561. doi: 10.1101/2020.04.01.20048561.
67. Quartier P, Allantaz F, Cimaz R, Pillet P, Messiaen C, Bardin C, et al. A multicentre, randomised, double-blind, placebo-controlled trial with the interleukin-1 receptor antagonist anakinra in patients with systemic-onset juvenile idiopathic arthritis (ANAJIS trial). Ann Rheum Dis (2011) 70(5):747–54. doi: 10.1136/ard.2010.134254
68. Sheng CC, Sahoo D, Dugar S, Prada RA, Wang TKM, Abou Hassan OK, et al. Canakinumab to reduce deterioration of cardiac and respiratory function in SARS-CoV-2 associated myocardial injury with heightened inflammation (canakinumab in Covid-19 cardiac injury: The three C study). Clin Cardiol (2020) 43(10):1055–63. doi: 10.1002/clc.23451
69. Ucciferri C, Auricchio A, Di Nicola M, Potere N, Abbate A, Cipollone F, et al. Canakinumab in a subgroup of patients with COVID-19. Lancet Rheumatol (2020) 2(8):e457–ee458. doi: 10.1016/s2665-9913(20)30167-3
70. Cavalli G, De Luca G, Campochiaro C, Della-Torre E, Ripa M, Canetti D, et al. Interleukin-1 blockade with high-dose anakinra in patients with COVID-19, acute respiratory distress syndrome, and hyperinflammation: a retrospective cohort study. Lancet Rheumatol (2020) 2(6):e325–31. doi: 10.1016/S2665-9913(20)30127-2
71. Deftereos SG, Giannopoulos G, Vrachatis DA, Siasos GD, Giotaki SG, Gargalianos P, et al. Effect of Colchicine vs Standard Care on Cardiac and Inflammatory Biomarkers and Clinical Outcomes in Patients Hospitalized With Coronavirus Disease 2019: The GRECCO-19 Randomized Clinical Trial. JAMA Netw Open (2020) 3(6):e2013136. doi: 10.1001/jamanetworkopen.2020.13136
72. Li JY, You Z, Wang Q, Zhou ZJ, Qiu Y, Luo R, et al. The epidemic of 2019-novel-coronavirus (2019-nCoV) pneumonia and insights for emerging infectious diseases in the future. Microbes Infect (2020) 22(2):80–5. doi: 10.1016/j.micinf.2020.02.002
73. Liu J, Zheng X, Tong Q, Li W, Wang B, Sutter K, et al. Overlapping and discrete aspects of the pathology and pathogenesis of the emerging human pathogenic coronaviruses SARS-CoV, MERS-CoV, and 2019-nCoV. J Med Virol (2020) 92(5):491–4. doi: 10.1002/jmv.25709
74. Coomes EA, Haghbayan H. Interleukin-6 in COVID-19: A Systematic Review and Meta-Analysis. medRxiv (2020) 2020.2003.2030.20048058. doi: 10.1101/2020.03.30.20048058.
75. Ulhaq ZS, Soraya GV. Interleukin-6 as a potential biomarker of COVID-19 progression. Méd Maladies Infectieuses (2020) 50(4):382–3. doi: 10.1016/j.medmal.2020.04.002
76. Grupp SA, Kalos M, Barrett D, Aplenc R, Porter DL, Rheingold SR, et al. Chimeric antigen receptor-modified T cells for acute lymphoid leukemia. N Engl J Med (2013) 368(16):1509–18. doi: 10.1056/NEJMoa1215134
77. Xu X, Han M, Li T, Sun W, Wang D, Fu B, et al. Effective Treatment of Severe COVID-19 Patients with Tocilizumab. ChinaXiv (2020) 117(20):10970–5. doi: 10.1073/pnas.2005615117
78. Xu X, Han M, Li T, Sun W, Wang D, Fu B, et al. Effective treatment of severe COVID-19 patients with tocilizumab. Proc Natl Acad Sci USA (2020) 117(20):10970–5. doi: 10.1073/pnas.2005615117
79. Roumier M, Paule R, Groh M, Vallee A, Ackermann F. Interleukin-6 blockade for severe COVID-19. MedRxiv (2020) 2020.2004.2040.20061861. doi: 10.1101/2020.04.20.20061861
80. Toniati P, Piva S, Cattalini M, Garrafa E, Regola F, Castelli F, et al. Tocilizumab for the treatment of severe COVID-19 pneumonia with hyperinflammatory syndrome and acute respiratory failure: A single center study of 100 patients in Brescia, Italy. Autoimmun Rev (2020) 19(7):102568. doi: 10.1016/j.autrev.2020.102568
81. Malgie J, Schoones JW, Pijls BG. Decreased mortality in COVID-19 patients treated with Tocilizumab: a rapid systematic review and meta-analysis of observational studies. Clin Infect Dis (2020) ciaa1445. doi: 10.1093/cid/ciaa1445
82. Masiá M, Fernández-González M, Padilla S, Ortega P, García JA, Agulló V, et al. Impact of interleukin-6 blockade with tocilizumab on SARS-CoV-2 viral kinetics and antibody responses in patients with COVID-19: A prospective cohort study. EBioMedicine (2020) 60:102999. doi: 10.1016/j.ebiom.2020.102999
83. Caballero Bermejo AF, Ruiz-Antorán B, Fernández Cruz A, Diago Sempere E, Callejas Díaz A, Múñez Rubio E, et al. Sarilumab versus standard of care for the early treatment of COVID-19 pneumonia in hospitalized patients: SARTRE: a structured summary of a study protocol for a randomised controlled trial. Trials (2020) 21(1):794. doi: 10.1186/s13063-020-04633-3
84. Garcia-Vicuña R, Abad-Santos F, González-Alvaro I, Ramos-Lima F, Sanz JS. Subcutaneous Sarilumab in hospitalised patients with moderate-severe COVID-19 infection compared to the standard of care (SARCOVID): a structured summary of a study protocol for a randomised controlled trial. Trials (2020) 21(1):772. doi: 10.1186/s13063-020-04588-5
85. Montesarchio V, Parrela R, Iommelli C, Bianco A, Manzillo E, Fraganza F, et al. Outcomes and biomarker analyses among patients with COVID-19 treated with interleukin 6 (IL-6) receptor antagonist sarilumab at a single institution in Italy. J Immunother Cancer (2020) 8(2):e001089. doi: 10.1136/jitc-2020-001089
86. Vaidya G, Czer LSC, Kobashigawa J, Kittleson M, Patel J, Chang D, et al. Successful Treatment of Severe COVID-19 Pneumonia With Clazakizumab in a Heart Transplant Recipient: A Case Report. Transplant Proc (2020) 52(9):2711–4. doi: 10.1016/j.transproceed.2020.06.003
87. Cavalli G, Dinarello CA. Treating rheumatological diseases and co-morbidities with interleukin-1 blocking therapies. Rheumatol (Oxford) (2015) 54(12):2134–44. doi: 10.1093/rheumatology/kev269
88. Ben-Zvi I, Kukuy O, Giat E, Pras E, Feld O, Kivity S, et al. Anakinra for Colchicine-Resistant Familial Mediterranean Fever: A Randomized, Double-Blind, Placebo-Controlled Trial. Arthritis Rheumatol (2017) 69(4):854–62. doi: 10.1002/art.39995
89. Shakoory B, Carcillo JA, Chatham WW, Amdur RL, Zhao H, Dinarello CA, et al. Interleukin-1 Receptor Blockade Is Associated With Reduced Mortality in Sepsis Patients With Features of Macrophage Activation Syndrome: Reanalysis of a Prior Phase III Trial. Crit Care Med (2016) 44(2):275–81. doi: 10.1097/ccm.0000000000001402
90. Feldmann M, Maini RN, Woody JN, Holgate ST, Winter G, Rowland M, et al. Trials of anti-tumour necrosis factor therapy for COVID-19 are urgently needed. Lancet (2020) 395(10234):1407–9. doi: 10.1016/S0140-6736(20)30858-8
91. Qin C, Zhou L, Hu Z, Zhang S, Yang S, Tao Y, et al. Dysregulation of Immune Response in Patients With Coronavirus 2019 (COVID-19) in Wuhan, China. Clin Infect Dis (2020) 71(15):762–8. doi: 10.1093/cid/ciaa248
92. Blaszczak A, Trinidad JCL, Cartron AM. Adalimumab for treatment of hidradenitis suppurativa during the COVID-19 pandemic: Safety considerations. J Am Acad Dermatol (2020) 83(1):e31. doi: 10.1016/j.jaad.2020.04.030
93. Maschalidi S, Sepulveda FE, Garrigue A, Fischer A, de Saint Basile G. Therapeutic effect of JAK1/2 blockade on the manifestations of hemophagocytic lymphohistiocytosis in mice. Blood (2016) 128(1):60–71. doi: 10.1182/blood-2016-02-700013
94. Peterson D, Damsky W, King B. The use of Janus kinase inhibitors in the time of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). J Am Acad Dermatol (2020) 82(6):e223–6. doi: 10.1016/j.jaad.2020.03.099
95. El Jammal T, Gerfaud-Valentin M, Sève P, Jamilloux Y. JAK inhibitors: Perspectives in internal medicine. Rev Med Interne (2019) 40(12):816–25. doi: 10.1016/j.revmed.2019.07.016
96. Claire B. FDA issues tofacitinib safety alert. RheumatologyMedicinemattersCom (2019). Available at: https://rheumatology.medicinematters.com/rheumatoid-arthritis-/tofacitinib/fda-issues-tofacitinib-safety-alert/16527134.
97. Zhang X, Zhang Y, Qiao W, Zhang J, Qi Z. Baricitinib, a drug with potential effect to prevent SARS-COV-2 from entering target cells and control cytokine storm induced by COVID-19. Int Immunopharmacol (2020) 86:106749. doi: 10.1016/j.intimp.2020.106749
98. Modi B, Hernandez-Henderson M, Yang D, Klein J, Dadwal S, Kopp E, et al. Ruxolitinib as Salvage Therapy for Chronic Graft-versus-Host Disease. Biol Blood Marrow Transplant (2019) 25(2):265–9. doi: 10.1016/j.bbmt.2018.09.003
99. Jacobs J, Clark-Snustad K, Lee S. Case Report of a SARS-CoV-2 Infection in a Patient With Ulcerative Colitis on Tofacitinib. Inflammation Bowel Dis (2020) 26(7):e64. doi: 10.1093/ibd/izaa093
100. Scarsi M, Piantoni S, Colombo E, Airó P, Richini D, Miclini M, et al. Association between treatment with colchicine and improved survival in a single-centre cohort of adult hospitalised patients with COVID-19 pneumonia and acute respiratory distress syndrome. Ann Rheum Dis (2020) 79(10):1286–9. doi: 10.1136/annrheumdis-2020-217712
101. Piantoni S, Patroni A, Toniati P, Furloni R, Franceschini F, Andreoli L, et al. Why not to use colchicine in COVID-19? An oldanti-inflammatory drug for a novel auto-inflammatory disease. Rheumatol (Oxford) (2020) 59(7):1769–70. doi: 10.1093/rheumatology/keaa217
102. Darwish I, Mubareka S, Liles WC. Immunomodulatory therapy for severe influenza. Expert Rev Anti Infect Ther (2011) 9(7):807–22. doi: 10.1586/eri.11.56
103. Yang R, Xiong Y, Ke H, Chen T, Gao S. The Role of Methylprednisolone on Preventing Disease Progression for Hospitalized Patients with Severe COVID-19. Eur J Clin Invest (2020) 50(11):e13412. doi: 10.1111/eci.13412
104. Edalatifard M, Akhtari M, Salehi M, Naderi Z, Jamshidi A, Mostafaei S, et al. Intravenous methylprednisolone pulse as a treatment for hospitalised severe COVID-19 patients: results from a randomised controlled clinical trial. Eur Respir J (2020) 2002808. doi: 10.1183/13993003.02808-2020
105. Nelson BC, Laracy J, Shoucri S, Dietz D, Zucker J, Patel N, et al. Clinical Outcomes Associated with Methylprednisolone in Mechanically Ventilated Patients with COVID-19. Clin Infect Dis (2020) ciaa1163. doi: 10.1093/cid/ciaa1163
106. Ji J, Zhang J, Shao Z, Xie Q, Zhong L, Liu Z. Glucocorticoid therapy does not delay viral clearance in COVID-19 patients. Crit Care (2020) 24(1):565. doi: 10.1186/s13054-020-03287-6
107. Huang R, Zhu C, Jian W, Xue L, Li C, Yan X, et al. Corticosteroid therapy is associated with the delay of SARS-CoV-2 clearance in COVID-19 patients. Eur J Pharmacol (2020) 889:173556. doi: 10.1016/j.ejphar.2020.173556
108. Ye Q, Wang B, Mao J. The pathogenesis and treatment of the `Cytokine Storm’ in COVID-19. J Infect (2020) 80(6):607–13. doi: 10.1016/j.jinf.2020.03.037
109. Xu K, Cai H, Shen Y, Ni Q, Chen Y, Hu S, et al. Management of corona virus disease-19 (COVID-19): the Zhejiang experience. Zhejiang Da Xue Xue Bao (2020) 49(41):40. doi: 10.3785/j.issn.1008-9292.2020.02.02
110. Zhang Y, Yu L, Tang L, Zhu M, Jin Y, Wang Z, et al. A Promising Anti-Cytokine-Storm Targeted Therapy for COVID-19: The Artificial-Liver Blood-Purification System. Eng (Beijing) (2020). doi: 10.1016/j.eng.2020.03.006
111. Ma J, Xia P, Zhou Y, Liu Z, Zhou X, Wang J, et al. Potential effect of blood purification therapy in reducing cytokine storm as a late complication of critically ill COVID-19. Clin Immunol (2020) 214:108408. doi: 10.1016/j.clim.2020.108408
112. Wang Q, Hu Z. Successful recovery of severe COVID-19 with cytokine storm treating with extracorporeal blood purification. Int J Infect Dis (2020) 96:618–20. doi: 10.1016/j.ijid.2020.05.065
113. Yang XH, Sun RH, Zhao MY, Chen EZ, Liu J, Wang HL, et al. Expert recommendations on blood purification treatment protocol for patients with severe COVID-19: Recommendation and consensus. Chronic Dis Transl Med (2020) 6(2):106–14. doi: 10.1016/j.cdtm.2020.04.002
114. Li N, Hua J. Interactions between mesenchymal stem cells and the immune system. Cell Mol Life Sci (2017) 74(13):2345–60. doi: 10.1007/s00018-017-2473-5
115. Galipeau J, Sensébé L. Mesenchymal Stromal Cells: Clinical Challenges and Therapeutic Opportunities. Cell Stem Cell (2018) 22(6):824–33. doi: 10.1016/j.stem.2018.05.004
116. Atluri S, Manchikanti L, Hirsch JA. Expanded Umbilical Cord Mesenchymal Stem Cells (UC-MSCs) as a Therapeutic Strategy in Managing Critically Ill COVID-19 Patients: The Case for Compassionate Use. Pain Physician (2020) 23(2):E71–e83.
117. Yagi H, Soto-Gutierrez A, Parekkadan B, Kitagawa Y, Tompkins RG, Kobayashi N, et al. Mesenchymal stem cells: Mechanisms of immunomodulation and homing. Cell Transplant (2010) 19(6):667–79. doi: 10.3727/096368910x508762
118. Uccelli A, de Rosbo NK. The immunomodulatory function of mesenchymal stem cells: mode of action and pathways. Ann N Y Acad Sci (2015) 1351:114–26. doi: 10.1111/nyas.12815
Keywords: COVID-19, cytokine storm, ACE2, IL-6, immunoregulatory therapy
Citation: Tang L, Yin Z, Hu Y and Mei H (2020) Controlling Cytokine Storm Is Vital in COVID-19. Front. Immunol. 11:570993. doi: 10.3389/fimmu.2020.570993
Received: 09 June 2020; Accepted: 04 November 2020;
Published: 30 November 2020.
Edited by:
Zhiwei Wu, Nanjing University, ChinaReviewed by:
Aikaterini Alexaki, United States Food and Drug Administration, United StatesCopyright © 2020 Tang, Yin, Hu and Mei. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Heng Mei, aG1laUBodXN0LmVkdS5jbg==; Yu Hu, ZHJfaHV5dUAxMjYuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.