
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol. , 07 May 2020
Sec. Inflammation
Volume 11 - 2020 | https://doi.org/10.3389/fimmu.2020.00757
This article is part of the Research Topic Translational Insights into Mechanisms and Therapy of Organ Dysfunction in Sepsis and Trauma View all 31 articles
 Charles Neu1,2,3†
Charles Neu1,2,3† Philipp Baumbach1,2†
Philipp Baumbach1,2† Alina K. Plooij1,2
Alina K. Plooij1,2 Kornel Skitek1,2
Kornel Skitek1,2 Juliane Götze1,2Christian von Loeffelholz1
Juliane Götze1,2Christian von Loeffelholz1 Christiane Schmidt-Winter1,2
Christiane Schmidt-Winter1,2 Sina M. Coldewey1,2,3*
Sina M. Coldewey1,2,3*The imbalance of oxygen delivery and oxygen consumption resulting in insufficient tissue oxygenation is pathognomonic for all forms of shock. Mitochondrial function plays an important role in the cellular oxygen metabolism and has been shown to impact a variety of diseases in the intensive care setting, specifically sepsis. Clinical assessment of tissue oxygenation and mitochondrial function remains elusive. The in vivo protoporphyrin IX-triplet state lifetime technique (PpIX-TSLT) allows the direct, non-invasive measurement of mitochondrial oxygen tension (mitoPO2) in the human skin. Our recently established measurement protocol for the Cellular Oxygen Metabolism (COMET) Monitor, a novel device employing the PpIX-TSLT, additionally allows the evaluation of oxygen consumption (mitoVO2) and delivery (mitoDO2). In the intensive care setting, these variables might provide new insight into mitochondrial oxygen metabolism and especially mitoDO2 might be a surrogate parameter of microcirculatory function. However, the feasibility of the PpIX-TSLT in critically ill patients has not been analyzed systematically. In this interim study analysis, we evaluated PpIX-TSLT measurements of 40 patients during the acute phase of sepsis. We assessed (a) potential adverse side effects of the method, (b) the rate of analyzable measurements, (c) the stability of mitoPO2, mitoVO2, and mitoDO2, and (d) potential covariates. Due to excessive edema in patients with sepsis, we specifically analyzed the association of patients' hydration status, assessed by bioimpedance analysis (BIA), with the aforementioned variables. We observed no side effects and acquired analyzable measurements sessions in 92.5% of patients (n = 37/40). Different measures of stability indicated moderate to good repeatability of the PpIX-TSLT variables within one session of multiple measurements. The determined limits of agreement and minimum detectable differences may be helpful in identifying outlier measurements. In conjunction with signal quality they mark a first step in developing a previously unavailable standardized measurement quality protocol. Notably, higher levels of hydration were associated with lower mitochondrial oxygen tension. We conclude that COMET measurements are viable in patients with sepsis. To validate the clinical and diagnostic relevance of the PpIX-TSLT using the COMET in the intensive care setting, future studies in critically ill patients and healthy controls are needed.
Sepsis is defined as a life-threatening host response toward infection resulting in organ dysfunction (1). Despite advances in the pathophysiological understanding of this condition, research has not led to significant changes in sepsis therapy. It therefore remains one of the most prevalent critical conditions worldwide with only supportive therapy. A major hallmark of sepsis and septic shock in particular is disturbed tissue oxygenation. Hitherto, surrogate parameters of tissue oxygenation have been shown to be of limited reliability. Early goal-directed therapy, focusing on central venous oxygen saturation as a surrogate parameter of tissue oxygenation, for example, has shown no overall benefit in a recent meta-analysis (2) leaving clinicians without any evidence on which to base their decisions. Therefore, there is a need for new research into the direct measurement of tissue oxygenation.
In recent years, the mitochondrion has become a focus of medical research. The mitochondrion, as “powerhouse” of the cell, is responsible for the regulation of cellular oxygen metabolism and could therefore pose a potential target for the measurement of tissue oxygenation. Studies have demonstrated a pathophysiological involvement of mitochondrial function in, among others, cancer, heart, and age-related diseases (3–5). In sepsis, studies have yielded first indications of a dysregulated mitochondrial function. Clinical trials showed increased mitochondrial protein synthesis in patients with sepsis (6, 7). Another study demonstrated a decreased mitochondrial function in biopsies from patients with sepsis (8). Thus far, clinical measurements were performed in muscle biopsies. As the analysis is ex vivo there may be pre-analytical confounders influencing the results. Also, the procedure is invasive and therefore unlikely to be used routinely for diagnostic purposes. Non-invasive direct measurements of mitochondrial function in patients could pose a feasible method to assess tissue oxygenation in patients with sepsis.
Mik et al. introduced the protoporphyrin IX-triplet state lifetime technique (PpIX-TSLT) for non-invasively measuring mitochondrial oxygen tension (mitoPO2) (9). In brief, the method is based on the delayed fluorescence of protoporphyrin IX (PpIX), the naturally occurring precursor of the heme molecule, which can be enriched in skin cells by external application of 5-aminolevulinic acid (5-ALA). The delayed fluorescence is induced by pulses of green light and is inversely correlated with mitochondrial oxygen tension. The recent development of the CE-certified Cellular Oxygen METabolism Monitor (COMET) now enables the application of the PpIX-TSLT in the clinical setting. As this device allows the direct measurement of oxygen metabolism on the cellular level, it could be employed as a diagnostic tool for patients with sepsis. Thus far, the COMET has been employed in a pharmacological study (10) and in healthy controls (11, 12).
The primary objective of this study was to test how feasible the PpIX-TSLT measurements are in the acute phase of sepsis during the treatment at the critical care unit. The secondary objectives were to assess the distribution and the stability of PpIX-TSLT variables for single measurements and to identify potential covariates, in particular the patients' fluid status.
This study is an intermediate analysis of patients from the study Identification of cardiovascular and molecular prognostic factors for the medium- and long-term outcomes of sepsis (ICROS, DRKS00013347, and NCT03620409). Patients with sepsis were recruited at the intensive care units of the Jena University Hospital. The inclusion and exclusion criteria of the study are presented in Table 1. For PpIX-TSLT measurements, contraindications were: allergies to contents of the Alacare® plaster (photonamic, Wedel, Germany), porphyria, skin conditions aggravated by sunlight, or increased sensitivity to light. For BIA measurements contraindications were: electronic implants (e.g., pacemaker) or active prostheses. Study physicians obtained written informed consent from either the patient or the patient's legal proxy if the patient was incapacitated. The study was approved by the ethics committee of the Friedrich Schiller University Jena (5276-09/17).
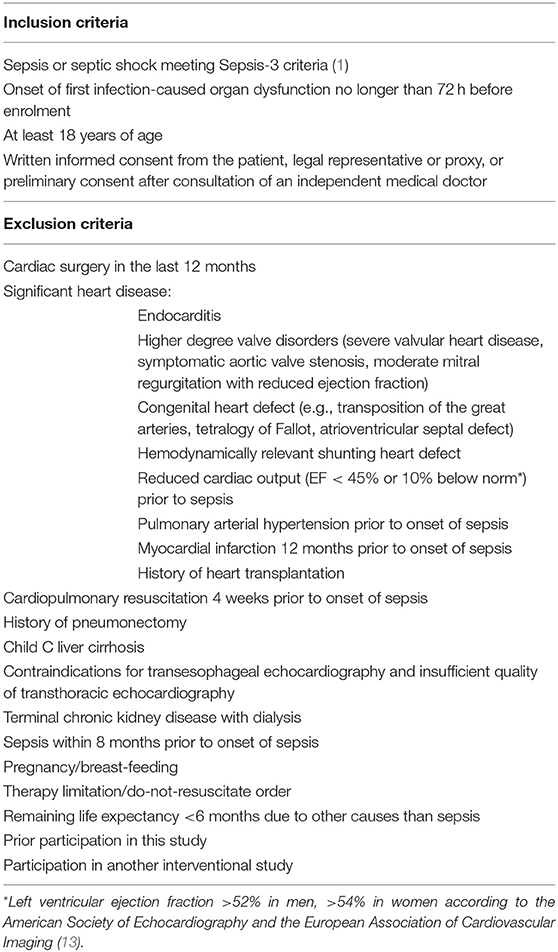
Table 1. Inclusion and exclusion criteria for the study.
PpIX-TSLT measurements took place within 3 ± 1 days after the onset of sepsis. A 4 cm2 patch containing 5-ALA (Alacare®, photonamic, Wedel, Germany) was applied to the clavipectoral triangle at least 5 h before the planned measurement to ensure sufficient accumulation of PpIX. Before application, the skin was cleaned and prepared with an abrasive paste (skinPure®, Nihon Kohden, Rosbach, Germany). For 48 h after application, the skin was protected from light with an additional patch. The measurements were performed with the COMET measurement system (Photonics Healthcare, Utrecht, Netherlands). Before the measurement session, the sensor was shielded from light and applied to the prepared skin. During one session multiple measurements with the following parameters were performed (see also Figure 1): In the first 30 s, the mitoPO2 : baseline was measured. Thereafter, we applied pressure to the sensor for 45 s to inhibit the microcirculation of that part of the skin and to measure oxygen consumption (mitoVO2 : maximum and mitoVO2 : average). Finally, the pressure was released to evaluate the re-oxygenation (mitoDO2 : maximum and mitoDO2 : average) and post-re-oxygenation mitoPO2 (mitoPO2 : post). A single measurement took 105 s and was performed at least three times per session. We used two complementary sigmoid functions to fit the raw PpIX-TSLT signals of each single measurement:
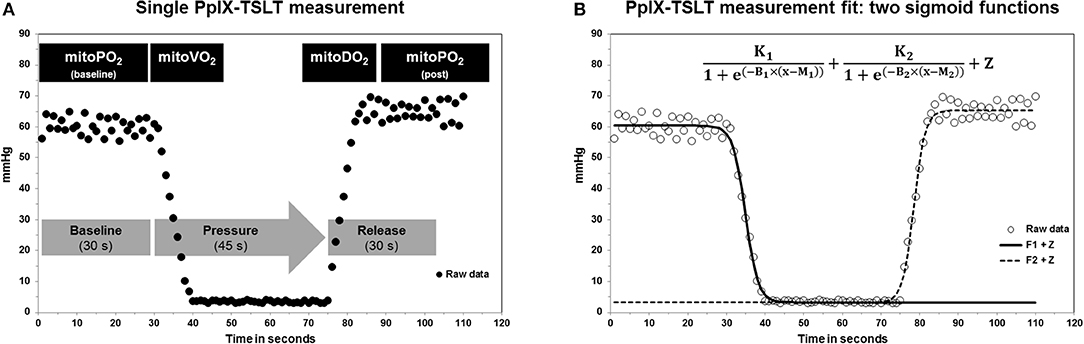
Figure 1. (A) Description of a single PpIX-TSLT measurement to obtain mitochondrial oxygen tension (mitoPO2), mitochondrial oxygen consumption (mitoVO2), and mitochondrial oxygen delivery (mitoDO2). (B) Illustration of the raw PpIX-TSLT data and the two sigmoid fit functions to estimate the PpIX-TSLT variables.
The estimation of these function parameters allows a direct inference of the PpIX-TSLT variables. For details please [see (12)].
We used a self-developed program (Halley) under MATLAB (MATLAB and Statistics Toolbox Release 2017a, The MathWorks, Inc., Natick, Massachusetts, United States) for data management, data preparation and PpIX-TSLT variable estimation.
The patient's fluid status was evaluated using the seca medical Body Composition Analyzer 525 (seca Germany, Hamburg, Germany). For bioimpedance vector analysis (BIVA), raw impedance variables, resistance (R) and reactance (Xc), were standardized to body height (R/height, Xc/height) in meters (14). Two characteristics of the resulting bivariate vector were analyzed: the phase angle [arc tangent of (Xc/R) × 180°/π] as vector orientation and the vector length (square root of + ). Especially the latter one is an indicator of the hydration status (14, 15) and has already been proven to be applicable in the critical care setting (16). Short vectors, resulting from decreased resistance, indicate high levels of hydration and can indicate the presence of edema secondary to low oncotic pressure or endothelial barrier dysfunction. Long vectors, resulting from increased resistance, are an indicator of a low hydration status, i.e., dehydration. Where feasible, body height, and weight were obtained by means of a measuring tape and the Seca bed scale 985 (Seca Germany, Hamburg, Germany), respectively. Otherwise, information from the medical history was used.
In descriptive analysis, means, standard deviations (SD), medians, as well as first and third quartiles (Q1/Q3) are reported. For categorical and dichotomous variables we report absolute and relative frequencies. The distribution of the PpIX-TSLT variables was assessed using histograms, Q-Q-plots, Shapiro-Wilk-Tests, and an estimation of kurtosis and skewness with corresponding standard errors (SE) and kurtosis excess (kurtosis – 3).
To analyze the repeatability, i.e., stability, of PpIX-TSLT variables during one measurement session we took the following steps: First, descriptive mean differences between measurement pairs and corresponding p-values of the paired samples t-tests are reported. Second, Pearson correlation coefficients of all available measurement pairs are presented. Correlation coefficients can be interpreted in the following way: r < 0.10 negligible, r 0.1–0.39 weak, 0.40–0.69 moderate, 0.70–0.89 strong, 0.90–1.00 very strong (17). Third, measurement pairs were analyzed using Bland-Altman plots to assess limits of agreement (LOA) (18, 19). In detail, the mean of a measurement pair is plotted against the difference between both single measurements (LOA = mean of the differences ± 1.96 × SD of the differences). The corresponding 95% confidence intervals (95%CI) for LOA were obtained using two-sided tolerance factors (20). At population level, 95% of PpIX-TSLT variable differences between single PpIX-TSLT measurements within one session, according to our protocol, should lie within these LOA. Fourth, intra-class correlation coefficients (ICC) for all available measurement pairs using the two-way mixed effects analysis of variance (ANOVA) for single measures with absolute agreement were obtained (21). ICCs and corresponding confidence intervals can be interpreted as follows: ICC < 0.5 poor, 0.5 ≤ ICC ≤ 0.75 moderate, 0.75 ≤ ICC ≤ 0.90 good, and ICC > 0.90 excellent reliability (21). Finally, the standard error of measurement (SEM) as the square root of the mean square error term from repeated-measures ANOVA for all available measurement pairs (22) and the Minimum Detectable Difference (MDD, SEM × 1.96 × 21/2) are reported.
Potential covariates for PpIX-TSLT variables were analyzed parametrically and non-parametrically with Pearson correlation coefficients and Spearman's rank correlation coefficients, respectively. PpIX-TSLT variables from multiple single measurements were averaged before correlative analysis. Results were additionally visualized with scatterplots and regression lines from the simple linear regression models (PpIX-TSLT variables served as dependent variables). We considered the following variables: sex, age, BIVA variables (see above), PpIX-TSLT-associated variables (duration of 5-ALA application, average signal quality, room, sensor, skin, and body temperature, goodness of fit of the fitting procedure), physiological data (heart rate, systolic and diastolic blood pressure, SpO2, hemoglobin, fluid balance), and treatment-associated data (initial SOFA score, catecholamine status, ventilation status). Treatment-related variables were obtained from electronic patient records on ICU (Copra System, Berlin, Germany).
For statistical analysis we used SPSS Statistics 24 (IBM Corporation, Armonk, NY, USA) and R [Version 3.5.1, Vienna, Austria (23)]. We applied a significance level of 5% and report two-sided p-values.
Figure 2 summarizes the study inclusion. Of 332 screened patients, 45 patients with sepsis were enrolled in the study. After excluding patients who withdrew consent, died before the measurement or had contraindications, PpIX-TSLT measurements were performed on 40 patients. 37 patients with reliable PpIX-TSLT measurements were included in the primary analysis. Demographic and clinical characteristics of the study sample are displayed in Table 2.
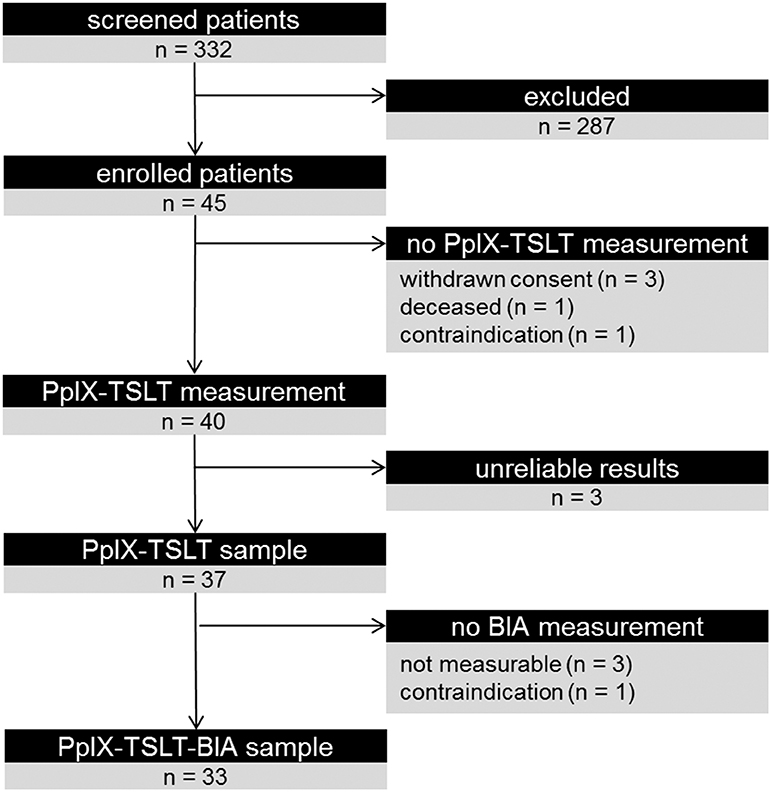
Figure 2. Overview of the patient inclusion and analytical cohorts. Results for primary analysis are reported from the PpIX-TSLT sample. Results for Bioimpedance Analysis (BIA) and additional correlative analyses with PpIX-TSLT variables are reported for the PpIX-TSLT-BIA sample.
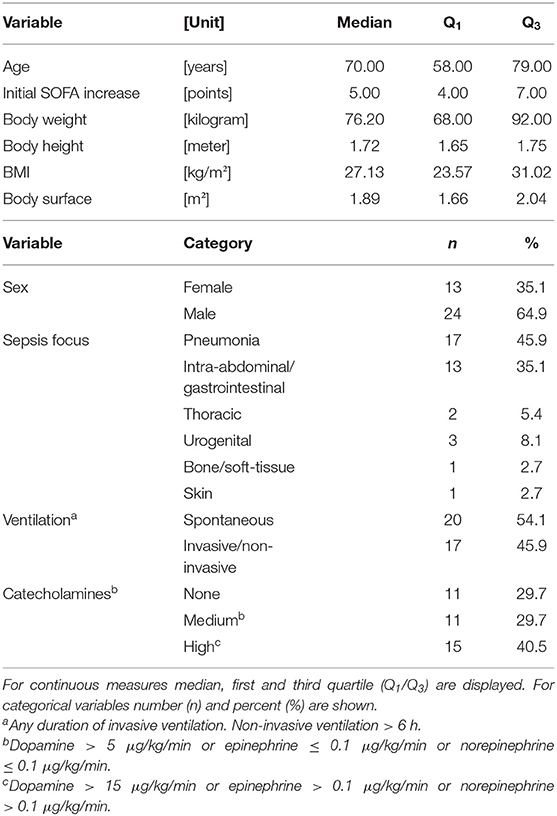
Table 2. Demographics and clinical characteristics (n = 37 patients).
In 37 (92.5%) of the 40 included patients with sepsis, reliable PpIX-TSLT measurement sessions could be recorded. In the 3 patients with unreliable measurement sessions either the signal quality was too low and/or mitoVO2 could not be induced consistently during multiple measurements. We did not observe any side effects of the 5-ALA application or the PpIX-TSLT measurement itself in any patient.
The descriptive statistics of the PpIX-TSLT variables are displayed in Table 3. Additional information on variable distribution is provided in Supplement S-1. Shapiro-Wilk tests indicated that mitoPO2 variables were normally distributed (p > 0.05). The p-values of the Shapiro-Wilk tests for the other PpIX-TSLT variables were significant (p < 0.01). All PpIX-TSLT parameters were positively skewed and kurtosis excess values ranged between −2.4 (mitoPO2 : baseline, platykurtic) to 3.0 (mitoVO2 : average, leptokurtic). After removing outlier values (values >Q3 + 1.5 times the interquartile range, see also Table 3) none of the p-values of the Shapiro-Wilk tests reached significance (p > 0.05) indicating normally distributed values.
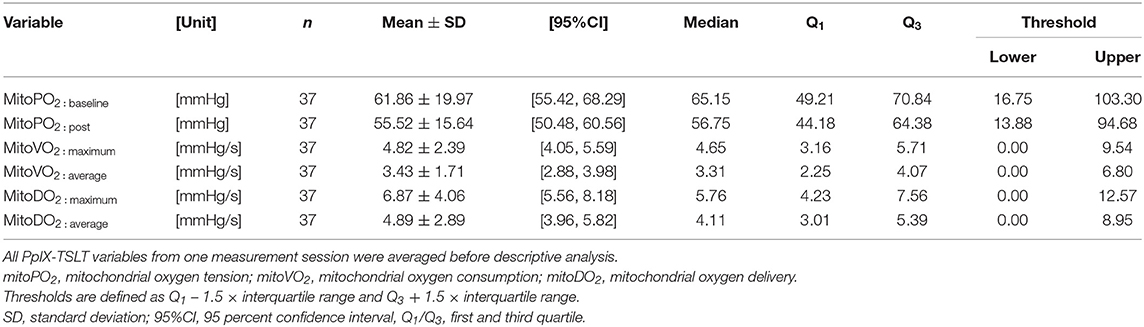
Table 3. Descriptive statistics for PpIX-TSLT variables.
MitoPO2 : baseline values showed a mean difference of 4.42 mmHg between subsequent measurements, resulting in a significant p-value of the corresponding paired t-test (Table 4). In addition, both mitoDO2 variables differed significantly between subsequent measurements (p < 0.01) with a mean difference of 1.07 (mitoDO2 : maximum) and 0.76 (mitoDO2 : average), respectively. MitoPO2 : Post and both mitoVO2 variables did not differ significantly between subsequent measurements. All variables were moderately (mitoDO2) to strongly (all others) correlated between subsequent measurements (Table 4). The limits of agreement and corresponding Bland-Altman-Plots for subsequent measurements are displayed in Table 4 and Supplement S-2. The intraclass correlation coefficients for all PpIX-TSLT variables showed significant p-values (p < 0.001) and ranged between 0.652 (moderate) for mitoDO2 variables and 0.805 (good) for mitoVO2 variables (Table 5). Finally, the standard error of measurement (SEM) and Minimum Detectable Difference (MDD) of PpIX-TSLT variables are displayed in Table 5.
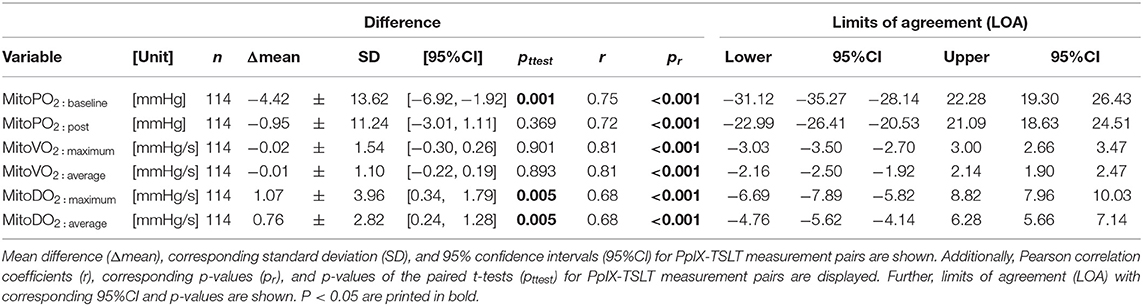
Table 4. Intra-session stability of the PpIX-TSLT variables (n = 36 patients with at least 2 reliable PpIX-TSLT measurements).
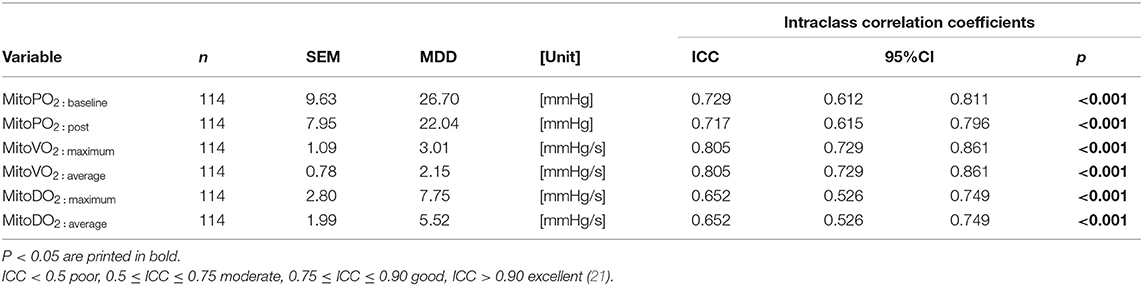
Table 5. Intraclass correlation coefficients (ICC) with corresponding 95% confidence intervals, standard error of measurement (SEM), and minimum detectable difference (MDD) for PpIX-TSLT variables (n = 36 patients with at least 2 reliable PpIX-TSLT measurements).
Statistically significant associations between PpIX-TSLT variables and tested covariates are shown in Table 6. The descriptive statistics for BIVA-variables and potential covariates are shown in Supplement S-3. In summary, mitoPO2 : baseline correlated positively with height-standardized vector length of BIVA. Maximum and average mitoVO2-variables showed correlation coefficients of 1. The same applies for mitoDO2 variables. For this reason, only results for mitoVO2 : average and mitoDO2 : average are reported. MitoVO2 variables were positively correlated with the goodness of fit (R2) of the fitting function. MitoDO2 variables were negatively correlated with the duration of 5-ALA application, the average signal quality during PpIX-TSLT measurement and body height. In addition, mitoDO2 variables were positively correlated with the room temperature. Finally, the mean signal quality of one measurement was positively correlated with the duration of the 5-ALA application and negatively correlated with the room temperature. All other tested covariates showed no statistically significant correlation coefficients with PpIX-TSLT variables (data not shown). MitoPO2 : baseline tended to differ between female (median: 69.95, Q1|3: 54.03 | 74.08) and male patients (median: 57.19, Q1|3: 44.36 | 69.25). In addition, we found significant sex differences between mitoDO2 : average with higher values for females (median: 5.25, Q1|3: 3.45 | 9.98) compared to males (median: 3.73, Q1|3: 2.55 | 5.27, U = 84, p = 0.022). Neither the ventilation status nor the catecholamine dosage was significantly associated with any of the PpIX-TSLT variables. After adjusting for multiple testing using the Bonferroni-Holm method, only the p-value for the association between mitoVO2 variables and the goodness of fit (R2) reached significance (adjusted p-values not shown).
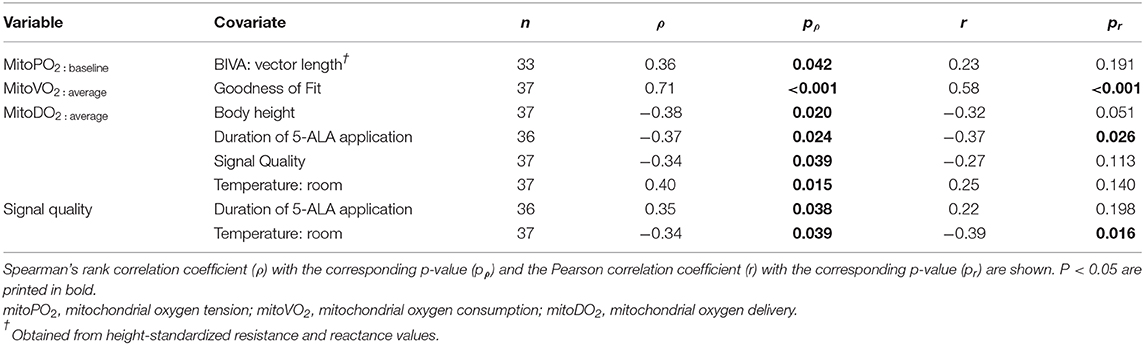
Table 6. Main findings of the correlation analyses for the PpIX-TSLT variables and potential covariates.
In this study, we report for the first time direct in vivo assessment of mitochondrial oxygen metabolism by PpIX-TSLT measurements in a cohort of patients with sepsis. Thus far, only reports in healthy subjects or surgical patients have been published. In our cohort of 40 patients, PpIX-TSLT measurements yielded analyzable datasets in 92.5% of patients. Also, no side effects of the measurements were observed. We therefore conclude that PpIX-TSLT measurements with the COMET are feasible in patients with sepsis in the ICU setting. In our previous study, analyzable results were obtained from 75% of healthy subjects (12). We believed at the time that compliance problems concerning 5-ALA application may have contributed to this relatively low success rate. As the ICU offers a standardized environment, protocol adherence was very high. Hence, our results may confirm our assumption and stress the importance of controlling the duration of 5-ALA application. Of the three measurements that failed in this study, one was due to low signal quality. This may have been due to inadequate skin absorption of 5-ALA despite using a standardized protocol. In the other two cases, mitoVO2 could not be induced. This phenomenon is not entirely understood and deserves future attention.
After removing outliers, all variables were normally or near-to-normally distributed. In our previous trial, PpIX-TSLT variables were also distributed near to normal (12). Therefore, we conclude both parametric and non-parametric analyses may be applicable for PpIX-TSLT variables.
All variables were moderately to highly correlated between replicate measurements. All ICCs of PpIX-TSLT variables showed significant p-values and ranged from moderate to good. Although t-tests showed significant differences in mitoPO2 : baseline and both mitoDO2 variables between iterative measurements, the corresponding effect sizes were low (d = 0.32, d = 0.27, and d = 0.27, respectively). Taken together, the stability of replicate measurements in one session can be seen as moderate to good. We nonetheless recommend multiple measurements in one session. Judging from the LOA and MDD, we can determine that an increase in mitoPO2 : baseline of 35 mmHg or a decrease of 25 mmHg between measurements is probably due to incorrect measurement and the measurement should be repeated. Similarly, absolute changes of 2 mmHg/s for mitoVO2 : average and 5 mmHg/s for mitoDO2 : average could indicate incorrect measurements. All these results are very similar to values determined in our previous study of healthy controls (12).
We identified potential covariates of the PpIX-TSLT measurements. We demonstrated a positive association between mitoPO2 : baseline and BIVA vector length, which in turn correlates negatively with hydration status (14, 16). Therefore, more hydrated patients (i.e., with edema), may show lower mitoPO2: baseline values. Thus, we recommend considering the presence of edema or conditions with low intravascular oncotic pressure as influence factors when employing the PpIX-TSLT in patients with sepsis. The duration of the 5-ALA plaster application was positively associated with signal quality. One should therefore perform the measurement using a standardized minimum duration of 5-ALA application. Furthermore, room temperature was associated with mitoDO2 : average and signal quality. Signal quality could be improved by performing measurements in a cool environment if possible. The patient's sex posed another covariate. MitoPO2 : average tended to differ between female and male patients. In addition, we found significant sex differences between mitoDO2 : average. Both variables showed higher values for females compared to males. This result could indicate the need for sex-specific normal values of PpIX-TSLT variables. Interestingly, neither the status of ventilation nor the dosage of catecholamines showed significant associations with PpIX-TSLT variables.
The generalizability of the results for our secondary objectives are limited by the relatively small number of patients (n = 37) and selective exclusion criteria (i.e., exclusion of patients with pre-existing cardiac conditions). Furthermore, in correlative analysis for the identification of potential covariates we did not adjust for multiple testing. Thus, our results need to be confirmed in larger trials. Especially the potential influence of the patient's hydration status on PpIX-TSLT variables should be examined. A direct estimation of total body water using BIA may be useful but is strongly dependent on body weight and height. As measuring body weight accurately in intensive care patients is difficult, we restricted our analyses to the weight-independent BIA variables (BIVA). Due to the fluctuation of physiological variables in critically ill patients, we only analyzed the short-term stability of PpIX-TSLT variables, with iterative measurements within minutes. The long-term stability of PpIX-TSLT variables was not analyzed.
We conclude that PpIX-TSLT measurements with the COMET are feasible in the critical care setting. Despite the moderate to good stability of the PpIX-TSLT variables using our protocol, we recommend the recording of multiple measurements during one session to increase the reliability of results. The determined limits of agreement and the minimum detectable differences may help to identify potential outlier measurements and additionally improve data quality. Future studies in larger cohorts of critically ill patients are needed to determine the clinical and diagnostic relevance of the PpIX-TSLT using the COMET. Furthermore, healthy controls should be measured to generate normal values for the PpIX-TSLT variables. This study poses a first step toward an evidence-based approach in the assessment of tissue oxygenation in the intensive care unit.
The datasets generated for this study are available on request to the corresponding author.
The studies involving human participants were reviewed and approved by Ethics Committee of the Friedrich Schiller University Jena. The patients/participants provided their written informed consent to participate in this study.
SC, CN, and PB: conception and design of the study. CN, PB, AP, KS, JG, and CS-W: performance of measurements. PB, CN, AP, KS, and JG: clinical data collection. PB, KS, and AP: data analysis and statistical analysis. CN, PB, AP, KS, JG, CS-W, and SC: drafting the manuscript for important intellectual content. CN, CL, PB, and SC: revising the manuscript prior to submission. All authors carefully reviewed and approved the manuscript.
This study was funded by the Federal Ministry of Education and Research within the Centre for Innovation Competence Septomics (Research Group Translational Septomics, Grant 03Z22JN12 to SC). The funding source had no involvement in the study design, the collection, analysis, and interpretation of data, in the writing of the report, or in the decision to submit the article for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We thank the study nurse team of the department of Anesthesiology and Intensive Care Medicine of the Jena University Hospital for their support.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2020.00757/full#supplementary-material
5-ALA, 5-aminolevulinic acid; BIA, bioimpedance analysis; BIVA, bioimpedance vector analysis; COMET, Cellular Oxygen Metabolism Monitor; mitoDO2 : average, average mitochondrial oxygen delivery; mitoDO2 : maximum, maximum mitochondrial oxygen delivery; mitoPO2 : baseline, baseline mitochondrial oxygen tension; mitoPO2 : post, post-mitochondrial oxygen tension; mitoVO2 : average, average mitochondrial oxygen consumption; mitoVO2 : maximum, maximum mitochondrial oxygen consumption; PpIX, protoporphyrin IX; PpIX-TSLT, protoporphyrin IX-triplet state lifetime; SEM, standard error of measurement.
1. Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. (2016) 315:801–10. doi: 10.1001/jama.2016.0287
2. Rowan KM, Angus DC, Bailey M, Barnato AE, Bellomo R, Canter RR, et al. Early, goal-directed therapy for septic shock - a patient-level meta-analysis. N Engl J Med. (2017) 376:2223–34. doi: 10.1056/NEJMoa1701380
3. Lane RK, Hilsabeck T, Rea SL. The role of mitochondrial dysfunction in age-related diseases. Biochim Biophys Acta. (2015) 1847:1387–400. doi: 10.1016/j.bbabio.2015.05.021
4. Giampazolias E, Tait SW. Mitochondria and the hallmarks of cancer. FEBS J. (2016) 283:803–14. doi: 10.1111/febs.13603
5. Murphy E, Ardehali H, Balaban RS, Dilisa F, Dorn GW II, Kitsis RN, Otsu K, et al. Mitochondrial function, biology, and role in disease: a scientific statement from the american heart association. Circ Res. (2016) 118:1960–91. doi: 10.1161/RES.0000000000000104
6. Fredriksson K, Tjader I, Keller P, Petrovic N, Ahlman B, Scheele C, et al. Dysregulation of mitochondrial dynamics and the muscle transcriptome in ICU patients suffering from sepsis induced multiple organ failure. PLoS ONE. (2008) 3:e3686. doi: 10.1371/annotation/68d951f9-a236-472f-98af-24e4cc4c1a20
7. Carre JE, Orban JC, Re L, Felsmann K, Iffert W, Bauer M, et al. Survival in critical illness is associated with early activation of mitochondrial biogenesis. Am J Respir Crit Care Med. (2010) 182:745–51. doi: 10.1164/rccm.201003-0326OC
8. Brealey D, Brand M, Hargreaves I, Heales S, Land J, Smolenski R, et al. Association between mitochondrial dysfunction and severity and outcome of septic shock. Lancet. (2002) 360:219–23. doi: 10.1016/S0140-6736(02)09459-X
9. Mik EG, Stap J, Sinaasappel M, Beek JF, Aten JA, Van Leeuwen TG, et al. Mitochondrial PO2 measured by delayed fluorescence of endogenous protoporphyrin IX. Nat Methods. (2006) 3:939–45. doi: 10.1038/nmeth940
10. Van Diemen MPJ, Berends CL, Akram N, Wezel J, Teeuwisse WM, Mik BG, et al. Validation of a pharmacological model for mitochondrial dysfunction in healthy subjects using simvastatin: a randomized placebo-controlled proof-of-pharmacology study. Eur J Pharmacol. (2017) 815:290–7. doi: 10.1016/j.ejphar.2017.09.031
11. Harms FA, Stolker RJ, Mik EG. Cutaneous respirometry as novel technique to monitor mitochondrial function: a feasibility study in healthy volunteers. PLoS ONE. (2016) 11:e0159544. doi: 10.1371/journal.pone.0163399
12. Baumbach P, Neu C, Derlien S, Bauer M, Nisser M, Buder A, et al. A pilot study of exercise-induced changes in mitochondrial oxygen metabolism measured by a cellular oxygen metabolism monitor (PICOMET). Biochim Biophys Acta Mol Basis Dis. (2019) 1865:749–58. doi: 10.1016/j.bbadis.2018.12.003
13. Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. (2015) 28:1–39.e14. doi: 10.1016/j.echo.2014.10.003
14. Piccoli A, Rossi B, Pillon L, Bucciante G. A new method for monitoring body fluid variation by bioimpedance analysis: the RXc graph. Kidney Int. (1994) 46:534–9. doi: 10.1038/ki.1994.305
15. Norman K, Stobaus N, Pirlich M, Bosy-Westphal A. Bioelectrical phase angle and impedance vector analysis–clinical relevance and applicability of impedance parameters. Clin Nutr. (2012) 31:854–61. doi: 10.1016/j.clnu.2012.05.008
16. Jones SL, Tanaka A, Eastwood GM, Young H, Peck L, Bellomo R, et al. Bioelectrical impedance vector analysis in critically ill patients: a prospective, clinician-blinded investigation. Crit Care. (2015) 19:290. doi: 10.1186/s13054-015-1009-3
17. Schober P, Boer C, Schwarte LA. Correlation coefficients: appropriate use and interpretation. Anesth Analg. (2018) 126:1763–8. doi: 10.1213/ANE.0000000000002864
18. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. (1986) 1:307–10. doi: 10.1016/S0140-6736(86)90837-8
19. Bland JM, Altman DG. Agreed statistics: measurement method comparison. Anesthesiology. (2012) 116:182–5. doi: 10.1097/ALN.0b013e31823d7784
20. Carkeet A. Exact parametric confidence intervals for Bland-Altman limits of agreement. Optom Vis Sci. (2015) 92:e71–80. doi: 10.1097/OPX.0000000000000513
21. Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. (2016) 15:155–63. doi: 10.1016/j.jcm.2016.02.012
22. Weir JP. Quantifying test-retest reliability using the intraclass correlation coefficient and the SEM. J Strength Cond Res. (2005) 19:231–40. doi: 10.1519/00124278-200502000-00038
Keywords: sepsis, COMET, mitochondrial dysfunction, critically ill patients, protoporphyrin IX-triplet state lifetime technique, cellular oxygen metabolism, mitochondrial oxygen metabolism, mitochondrial oxygen tension
Citation: Neu C, Baumbach P, Plooij AK, Skitek K, Götze J, von Loeffelholz C, Schmidt-Winter C and Coldewey SM (2020) Non-invasive Assessment of Mitochondrial Oxygen Metabolism in the Critically Ill Patient Using the Protoporphyrin IX-Triplet State Lifetime Technique—A Feasibility Study. Front. Immunol. 11:757. doi: 10.3389/fimmu.2020.00757
Received: 23 December 2019; Accepted: 03 April 2020;
Published: 07 May 2020.
Edited by:
Pietro Ghezzi, Brighton and Sussex Medical School, United KingdomReviewed by:
Robert Campbell, The University of Utah, United StatesCopyright © 2020 Neu, Baumbach, Plooij, Skitek, Götze, von Loeffelholz, Schmidt-Winter and Coldewey. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sina M. Coldewey, c2luYS5jb2xkZXdleUBtZWQudW5pLWplbmEuZGU=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.