 Mårten Segelmark
Mårten Segelmark Lars Björck
Lars Björck- 1Nephrology, Department of Clinical Sciences, Lund University, Lund, Sweden
- 2Infection Medicine, Department of Clinical Sciences, Lund University, Lund, Sweden
In primary systemic small vessel vasculitis autoantibodies are common and seem to play an important role in the pathogenesis. Autoantibodies in vasculitis are preferentially directed against components of the immune system or directly against components of the vessel wall. Plasmapheresis is often applied in emergency situationists when the function of vital organs is jeopardized, the level of clinical evidence to apply such therapy, however, varies between low and non-existing. Plasmapheresis is a blunt and unspecific instrument that requires several sessions to achieve a substantial reduction of autoantibody levels. IdeS and EndoS are two relatively recently discovered enzymes produced by S. pyogenes, that have a remarkable capacity to degrade and disarm IgG. They have shown positive results in several in vivo models of autoimmunity, and treatment with IdeS has successfully been used to inactivate HLA alloantibodies in patients undergoing renal transplantation. Both IdeS and EndoS have the potential to become precision tools to replace plasmapheresis in the treatment of vasculitic emergencies and a clinical trial of IdeS in anti-GBM vasculitis is now ongoing.
Autoantibodies Are Common
The association of autoantibodies and inflammatory diseases was established more than 60 years ago (1); and now there are several hundred described specificities associated with different diseases. They are utilized for diagnostic purposes to differentiate between diseases and sometimes also as markers of disease activity; and they may participate in the pathogenesis (2). Elevated levels of disease associated autoantibodies can sometimes be found long before onset of symptoms and any diagnosis can be established (3). Autoantibodies can also be found in healthy humans (2, 4) and in mice raised under germfree conditions (5). Such natural autoantibodies are probably instrumental in removing cellular debris and seems to be protective of both arteriosclerosis and autoimmune disease. Most of these natural autoantibodies are thought to be of IgM class with limited avidity and specificity. However, it has been shown that healthy humans also have low levels of IgG antibodies (4) with highly restricted epitope specificity (6).
Autoantibodies in Vasculitis
Vasculitides are broadly divided into primary and secondary forms, where primary vasculitides are diseases where inflamed blood vessel is the defining and most prominent feature. Primary vasculitides are further divided based on vessel size into large vessel, medium-sized vessel and small vessel vasculitis (7). Autoantibodies are common in all diseases in the small vessel group but are rare or at least not yet discovered in large and medium-sized vessel vasculitis (8, 9) (Table 1). Autoantibodies are also common in secondary forms of small vessel vasculitis, such as in systemic lupus erythematosus (1) and drug induced vasculits (10, 11), but in secondary vasculitis treatment should be aimed at underlying condition.
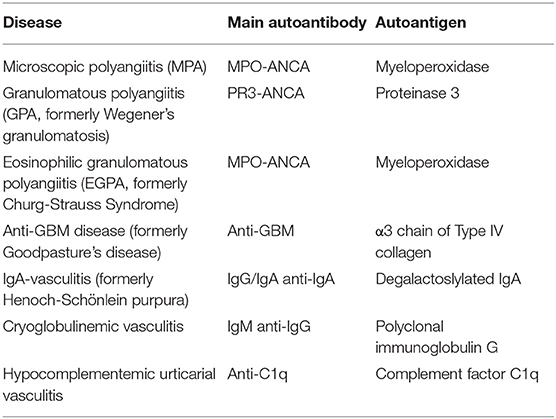
Table 1. Autoantibodies in small vessel vasculitis.
Autoantibodies Take Part in the Pathogenesis
The role of the autoantibodies in the pathogenesis, and the implicated pathogenic mechanisms, varies between the different diseases. In anti-GBM disease the binding of autoantibodies along the capillary wall of the glomeruli and alveoli start the complement cascade through the classical pathway and attract neutrophils through the C5a fragment (12, 13). Transfer experiments of eluted human antibodies injected into primates show that anti-GBM alone can mediate the disease (14), but there are also reports of anti-GBM models driven by T cells in agammaglobulinemic animals (15). Several in vitro studies indicate a role for anti-neutrophil cytoplasm antibodies (ANCA) in the pathogenesis of small vessel vasculitides such as microscopic polyangiitis (MPA) and granulomatosis with polyangiitis (GPA) (16, 17). There are many ANCA specificities in different autoimmune diseases but only myeloperoxidase (MPO) and proteinase 3 (PR3) that are expressed on the surface of primed neutrophils are major ANCA-antigens in vasculitis (8). The most compelling evidence for a role of ANCA in the pathogenesis comes from animal models of MPO-ANCA, where antibodies alone or antibody producing cells can transfer the disease (18). However, there are also data that do not support a direct role for ANCA in the pathogenesis; all purified IgG preparations from patients do not active neutrophils in a consistent manner (19, 20). IgA vasculitis (21) and cryoglobulinemic vasculitis (22) are immune complex mediated diseases, where polyclonal or monoclonal autoantibodies react with other immunoglobulins to form complexes. In urticarial vasculitis there are often autoantibodies directed to the complement factor C1q, which also lead to immune complex formation (23). Immune complexes activate complement primarily through the classical pathway which results in neutrophil influx and vessel wall damage (23). Physiochemical properties such as size and temperature determine where and when they will deposit, in urticarial vasculitis the direct targeting of the complement system also affect symptoms and signs.
IdeS and EndoS
Streptococcus pyogenes, one of the most significant bacterial pathogens in humans, has evolved multiple mechanisms to avoid antibody attack and complement activation. IdeS, Immunoglobulin G degrading enzyme of Streptococcus pyogenes, is a secreted cysteine proteinase which cleaves all four human IgG subclasses with a unique degree of specificity; apart from IgG no other substrate has been identified (24). Before cleavage can occur in the hinge region of the heavy chain to generate two Fc and one F (ab1)2 fragment the enzyme has to bind to the Fc region, and the remarkable specificity lies in this initial protein-protein interaction (25). S. pyogenes infects only humans, and from an evolutionary point of view it is noteworthy that the cleavage of IgG in other species is more restricted; in mice for instance subclasses 2a/c and 3 are sensitive, but not 1 and 2b (26).
Human IgG contains one N-linked glycan attached to Asn237 on the heavy chain (27). It is of great importance for effector functions such as complement activation and neutrophil recruitment. There are several bacterial enzymes that modifies N-linked glycans, but the first IgG specific glycan hydrolase to be described was EndoS which is also produced Streptococcus pyogenes (28). EndoS cleaves most of the carbohydrate moiety from IgG but leaves an N-acetylglucosamine with an alpha-linked fucose on protein backbone. EndoS treatment in vitro leads to reduced complement activation and phagocytosis of bacteria.
IdeS and EndoS in Experimental Models
The species specificity hampers to use of IdeS in many rodent models. Not surprising is that pretreatment in vitro of pathogenic autoantibodies with IdeS can abolish disease in passive transfer models, such as immune thrombocytopenic purpura, neuromyelitis optica, and collagen induced arthritis (26, 29). What is more encouraging is that is that mice in vivo can be rescued from a lethal dose of rabbit anti-mouse thrombocytes and that arthritis induced by mouse IgG2a antibodies can be reduced in severity by IdeS in vivo (26). EndoS is easier to employ in experimental rodent models and have been shown to be effective to prevent or to treat disease in multiple settings, also in strains that spontaneously develop systemic inflammation (30).
The effect of IdeS and EndoS has also been investigated in experimental models of vasculitis. A mouse/rabbit model had been developed to mimic essential steps in the pathogenesis of anti-GBM disease. Here we took advantage of IgG species differences. Mice are first given a bolus dose of rabbit anti-mouse IgG; since rabbit IgG cannot activate mouse complement (31) this has no consequences. A week later, when there is no longer any circulating rabbit IgG, the animals are challenged with mouse-anti rabbit IgG. This leads to a dose-dependent renal injury mediated by complement induced neutrophil recruitment. When IdeS was given between the two IgG injections, it completely inhibited the development of proteinuria. Histological examinations confirmed that Fc fragments but not F (ab')2 fragment had been removed from the GBM. This was accompanied by a reduction in the deposition of complement and influx of neutrophils in the glomeruli. EndoS was also employed in this model, even though the setup is not ideal for testing EndoS a positive effect was seen.
EndoS has also been used in a model of ANCA associated vasculitis (32). Pre-treatment of human MPO-ANCA containing IgG with EndoS prevented neutrophil respiratory burst. When mouse anti-MPO was exposed to EndoS before injection into mice, the antibodies did not induce disease. In addition, when EndoS was given to the mice after challenge with anti-MPO IgG antibodies this attenuated the disease (32).
IdeS in Humans
In a phase I trial, IdeS was given in different doses to healthy human volunteers (33). Doses as low as 0.12 mg/kg body weight led to a complete cleavage of not only plasma IgG but the entire extracellular IgG pool in all subjects without any obvious side effects. Intact IgG started to reappear after a few days and reached pre-treatment levels within a month. Varying titer of anti-IdeS antibodies were detected in the healthy volunteers; these levels rose after IdeS infusion, peaked after 2 weeks and was back to pre-treatment levels after 6 months.
IdeS is being developed as a pharmaceutical agent by Hansa-Biopharma; the non-proprietary name for the compound is Imlifidase. It has been tested in clinical trials to enable transplantation in patients with multiple HLA alloantibodies (34). A single dose given prior to transplantation enabled transplantations in 24 out 25 such sensitized patients who if they ultimately receive a kidney at all, may have to wait for years for a matching kidney (35). In many of the patients HLA antibodies rebounded, but 6 months after transplantation all 24 patients had functioning grafts.
IdeS like all other therapies can have side effects, total depletion of IgG take away an important protection against microorganisms. This is done also by plasma exchange but not as effective, on the other hand IdeS treated patients still have intact levels of IgA and IgM. Most individuals have measurable levels of anti-IdeS this introduces the risk of immune-complex formation and the development serum sickness. Furthermore, there is a theoretical risk of formation of neo-eptiopes by IdeS cleavage which can trigger autoantibody formation to IgG bound to different surfaces. Vigilance is always needed when introducing new pharma.
The Potential Role IdeS and EndoS in Treatment of Human Vasculitis
The rapid depletion of autoantibodies that can be achieved by IdeS is potentially beneficial in acute settings where vasculits threatens the function of vital organs. Today plasma exchange or immunadsorption therapy is used to lower levels of pathogenic IgG antibodies in such settings (36). With plasma exchange only about one third of the total body IgG is removed in each session. That means that it takes several days to reduce the levels with one order of magnitude, and many times a greater reduction is needed. Immunadsorption is more effective, but so far there are no randomized trials showing that this therapy leads to an improved clinical outcome in any condition, as compared to standard plasma exchange. The question is whether depleting autoantibodies with IdeS or disarming them with EndoS would make a clinical meaningful difference.
Most patients with anti-GBM disease have rapidly progressive glomerulonephritis (13). The standard therapy today is the combination of cyclophosphamide to stop autoantibody production, plasma exchange to remove autoantibodies and steroids to dampen inflammation (37, 38). This therapy is effective if started early, but most patients are diagnosed late. More than 2/3 are diagnosed when glomerular filtration rate is below 15 ml/min and in such cases <10% achieve renal survival. Anti-GBM disease is in most cases a monophasic disease, where autoantibodies are only produced during a few months. This period is substantially shortened by immunosuppression (39). We treated three patients on compassionate basis with refractory anti-GBM disease after an individual permit from the Swedish Medicinal Agency (40). All there were dialysis dependent and had high levels of circulating anti-GBM despite intense plasma-exchange. In all three cases anti-GBM levels dropped to levels within the normal range. Using Fc-gamma specific antisera we could show that IdeS had cleaved IgG bound to the kidney. None of three, however, regained kidney function enough to stop dialysis. We are now conducting an investigator driven clinical trial (EdraCT2016-004082-39) where 0.25 mg/kg of imlifidase (IdeS) is given as a single injection early in the course. Anti-GBM disease is rare, and considering inclusion and exclusion criteria, we need a very large catchment area to include the goal of 15 patients. So far 15 tertiary referral hospitals in major European cities participate in the study and 11 out 15 patients have been included.
In ANCA associated vasculitis plasma exchange is often used when complicated by rapidly progressive glomerulonephritis with severe renal failure or alveolar hemorrhage with respiratory distress (41). However, the use of plasma exchange in ANCA vasculitis is controversial. The MEPEX study published in 2003, show positive effect on 1-year renal survival (42). The more recently conducted PEXIVAS trial, that is so far only available as congress abstracts, did not show any benefit of plasma exchange, neither in cases with rapidly progressive glomerulonephritis nor in cases with alveolar hemorrhage. The reason for the negative results could be that plasma exchange is not effective enough to lower autoantibody levels in acute settings. In such cases treatment with IdeS or EndoS would be attractive treatment options. On the other hand, it also possible that the autoantibodies only play a minor role in the pathogenesis and that their removal does not lead to any meaningful clinical effect.
IgA vasculitis, urticarial vasculitis and cryoglobulinemic vasculitis are all considered to be immune complex mediated diseases. Plasma exchange is being used in all three diseases, but the evidence level is low (36, 43, 44). The potential effect of IdeS and EndoS is only speculative and might not even be beneficial. IgA vasculitis is the most common form of primary systemic vasculitis in children. The yearly incidence is reported to be as high as 176 per million children (45). Most cases are, however, mild and heal without any treatment. The disease is much less common in adults, but on the other hand also more severe. The high rate of spontaneous recovery makes clinical trials difficult. IgA is not effective when it comes to complement activation; the presence of IgG in the complexes may therefore be instrumental for the development of vasculitis.
In cryoglobulinemic vasculitis IgG is the target of the autoantibodies. Removing them could also alleviate the inflammation. However, the short duration of the effect would only provide transient benefit, and severe vasculitic crises are rare in cryoglobulinemic vasculitis. The same is true for urticarial vasculitis. The role of the autoantibodies against complement component C1q is uncertain, and it must be kept in mind that F (ab')2 fragments can continue to form immune complexes also after losing their Fc tail.
Conclusion
IgG class autoantibodies are common in primary small vessel vasculitis and they seem to participate in the pathogenesis. Today plasma exchange is often employed to reduce levels, but this treatment is unselective and rather ineffective. IdeS and EndoS are novel precision tools the rapidly either cleaves or disarms the IgG molecules. Whether this would lead to meaningful clinical responses remains to be determined in each individual disease. Anti-GBM disease, where the pathogenesis seems to be most straight forward, is first in line and a clinical trial is already ongoing.
Author Contributions
MS wrote the first draft of the manuscript and then both authors contributed on an equal basis.
Funding
LB's work was supported by the Foundations of Knut and Alice Wallenberg and Alfred Österlund, the Swedish Government Funds for Clinical Research (ALF), the Medical Faculty of Lund University, and Hansa Biopharma AB. MS work was supported the Swedish Rheumatic Disease Foundation, Swedish Government Funds for Clinical Research (ALF), The Ingrid Asp Foundation, Hansa Biopharma AB, Skåne University Hospital Funds.
Conflict of Interest
Hansa Biopharma AB owns the commercial rights for IdeS and EndoS as pharmaceuticals, and LB is listed as an inventor on the patents. MS and LB received research grants from Hansa Biopharma AB, and LB has an extensive research contract with the company.
References
1. Holman HR, Deicher HR, Kunkel HG. The L. E. cell and the L. E. serum factors. Bull NY Acad Med. (1959) 35:409–18.
2. Elkon K, Casali P. Nature and functions of autoantibodies. Nat Clin Pract Rheumatol. (2008) 4:491–8. doi: 10.1038/ncprheum0895
3. Leslie D, Lipsky P, Notkins AL. Autoantibodies as predictors of disease. J Clin Invest. (2001) 108:1417–22. doi: 10.1172/JCI14452
4. Nagele EP, Han M, Acharya NK, DeMarshall C, Kosciuk MC, Nagele RG. Natural IgG autoantibodies are abundant and ubiquitous in human sera, and their number is influenced by age, gender, and disease. PLoS ONE. (2013) 8:e60726. doi: 10.1371/journal.pone.0060726
5. Haury M, Sundblad A, Grandien A, Barreau C, Coutinho A, Nobrega A. The repertoire of serum IgM in normal mice is largely independent of external antigenic contact. Eur J Immunol. (1997) 27:1557–63. doi: 10.1002/eji.1830270635
6. Yang R, Cui Z, Hellmark T, Segelmark M, Zhao MH, Wang HY. Natural anti-GBM antibodies from normal human sera recognize alpha3 (IV)NC1 restrictively and recognize the same epitopes as anti-GBM antibodies from patients with anti-GBM disease. Clin Immunol. (2007) 124:207–12. doi: 10.1016/j.clim.2007.05.001
7. Jennette JC, Falk RJ, Bacon PA, Basu N, Cid MC, Ferrario F, et al. 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum. (2013) 65:1–11. doi: 10.1002/art.37715.
8. Weiner M, Segelmark M. The clinical presentation and therapy of diseases related to anti-neutrophil cytoplasmic antibodies (ANCA). Autoimmun Rev. (2016) 15:978–82. doi: 10.1016/j.autrev.2016.07.016
9. Kallenberg CG. Usefulness of antineutrophil cytoplasmic autoantibodies in diagnosing and managing systemic vasculitis. Curr Opin Rheumatol. (2016) 28:8–14. doi: 10.1097/BOR.0000000000000233
10. Jin Q, Kant S, Alhariri J, Geetha D. Levamisole adulterated cocaine associated ANCA vasculitis: review of literature and update on pathogenesis. J Community Hosp Intern Med Perspect. (2018) 8:339–44. doi: 10.1080/20009666.2018.1536242
11. Chen TK, Murakami C, Manno RL, Geetha D. Hematuria duration does not predict kidney function at 1 year in ANCA-associated glomerulonephritis. Semin Arthritis Rheum. (2014) 44:198–201. doi: 10.1016/j.semarthrit.2014.03.008
12. Hellmark T, Segelmark M. Diagnosis and classification of Goodpasture's disease (anti-GBM). J Autoimmun. (2014) 48–49:108–12. doi: 10.1016/j.jaut.2014.01.024
13. Hudson BG, Tryggvason K, Sundaramoorthy M, Neilson EG. Alport's syndrome, Goodpasture's syndrome, and type IV collagen. N Engl J Med. (2003) 348:2543–56. doi: 10.1056/NEJMra022296
14. Lerner RA, Glassock RJ, Dixon FJ. The role of anti-glomerular basement membrane antibody in the pathogenesis of human glomerulonephritis. J Exp Med. (1967) 126:989–1004. doi: 10.1084/jem.126.6.989
15. Bolton WK, Tucker FL, Sturgill BC. New avian model of experimental glomerulonephritis consistent with mediation by cellular immunity. Nonhumorally mediated glomerulonephritis in chickens. J Clin Invest. (1984) 73:1263–76. doi: 10.1172/JCI111328
16. van Rossum AP, Limburg PC, Kallenberg CG. Membrane proteinase 3 expression on resting neutrophils as a pathogenic factor in PR3-ANCA-associated vasculitis. Clin Exp Rheumatol. (2003) 21 (6 Suppl. 32):S64–8.
17. Falk RJ, Terrell RS, Charles LA, Jennette JC. Anti-neutrophil cytoplasmic autoantibodies induce neutrophils to degranulate and produce oxygen radicals in vitro. Proc Natl Acad Sci USA. (1990) 87:4115–9. doi: 10.1073/pnas.87.11.4115
18. Xiao H, Heeringa P, Hu P, Liu Z, Zhao M, Aratani Y, et al. Antineutrophil cytoplasmic autoantibodies specific for myeloperoxidase cause glomerulonephritis and vasculitis in mice. J Clin Invest. (2002) 110:955–63. doi: 10.1172/JCI0215918
19. Popat RJ, Robson MG. Neutrophils are not consistently activated by antineutrophil cytoplasmic antibodies in vitro. Ann Rheum Dis. (2019) 78:709–11. doi: 10.1136/annrheumdis-2018-214405
20. Ohlsson SM, Ohlsson S, Soderberg D, Gunnarsson L, Pettersson A, Segelmark M, et al. Neutrophils from vasculitis patients exhibit an increased propensity for activation by anti-neutrophil cytoplasmic antibodies. Clin Exp Immunol. (2014) 176:363–72. doi: 10.1111/cei.12301
21. Heineke MH, Ballering AV, Jamin A, Ben Mkaddem S, Monteiro RC, Van Egmond M. New insights in the pathogenesis of immunoglobulin A vasculitis (Henoch-Schonlein purpura). Autoimmun Rev. (2017) 16:1246–53. doi: 10.1016/j.autrev.2017.10.009
22. Damoiseaux J. The diagnosis and classification of the cryoglobulinemic syndrome. Autoimmun Rev. (2014) 13:359–62. doi: 10.1016/j.autrev.2014.01.027
23. Mahler M, van Schaarenburg RA, Trouw LA. Anti-C1q autoantibodies, novel tests, and clinical consequences. Front Immunol. (2013) 4:117. doi: 10.3389/fimmu.2013.00117
24. von Pawel-Rammingen U, Johansson BP, Bjorck L. IdeS, a novel streptococcal cysteine proteinase with unique specificity for immunoglobulin G. EMBO J. (2002). 21:1607–15. doi: 10.1093/emboj/21.7.1607
25. Vincents B, von Pawel-Rammingen U, Bjorck L, Abrahamson M. Enzymatic characterization of the streptococcal endopeptidase, IdeS, reveals that it is a cysteine protease with strict specificity for IgG cleavage due to exosite binding. Biochemistry. (2004) 43:15540–9. doi: 10.1021/bi048284d
26. Nandakumar KS, Johansson BP, Bjorck L, Holmdahl R. Blocking of experimental arthritis by cleavage of IgG antibodies in vivo. Arthritis Rheum. (2007) 56:3253–60. doi: 10.1002/art.22930
27. Rudd PM, Elliott T, Cresswell P, Wilson IA, Dwek RA. Glycosylation and the immune system. Science. (2001) 291:2370–6. doi: 10.1126/science.291.5512.2370
28. Collin M, Olsen A. EndoS, a novel secreted protein from Streptococcus pyogenes with endoglycosidase activity on human IgG. EMBO J. (2001) 20:3046–55. doi: 10.1093/emboj/20.12.3046
29. Johansson BP, Shannon O, Bjorck L. IdeS: a bacterial proteolytic enzyme with therapeutic potential. PLoS ONE. (2008) 3:e1692. doi: 10.1371/journal.pone.0001692
30. Collin M, Shannon O, Bjorck L. IgG glycan hydrolysis by a bacterial enzyme as a therapy against autoimmune conditions. Proc Natl Acad Sci USA. (2008) 105:4265–70. doi: 10.1073/pnas.0711271105
31. Yang R, Otten MA, Hellmark T, Collin M, Bjorck L, Zhao MH, et al. Successful treatment of experimental glomerulonephritis with IdeS and EndoS, IgG-degrading streptococcal enzymes. Nephrol Dial Transplant. (2010) 25:2479–86. doi: 10.1093/ndt/gfq115
32. van Timmeren MM, van der Veen BS, Stegeman CA, Petersen AH, Hellmark T, Collin M, et al. IgG glycan hydrolysis attenuates ANCA-mediated glomerulonephritis. J Am Soc Nephrol. (2010) 21:1103–14. doi: 10.1681/ASN.2009090984
33. Winstedt L, Jarnum S, Nordahl EA, Olsson A, Runstrom A, Bockermann R, et al. Complete removal of extracellular IgG antibodies in a randomized dose-escalation phase I study with the bacterial enzyme IdeS–a novel therapeutic opportunity. PLoS ONE. (2015) 10:e0132011. doi: 10.1371/journal.pone.0132011
34. Lorant T, Bengtsson M, Eich T, Eriksson BM, Winstedt L, Jarnum S, et al. Safety, immunogenicity, pharmacokinetics, and efficacy of degradation of anti-HLA antibodies by IdeS (imlifidase) in chronic kidney disease patients. Am J Transplant. (2018) 18:2752–62. doi: 10.1111/ajt.14733
35. Jordan SC, Lorant T, Choi J, Kjellman C, Winstedt L, Bengtsson M, et al. IgG endopeptidase in highly sensitized patients undergoing transplantation. N Engl J Med. (2017) 377:442–53. doi: 10.1056/NEJMoa1612567
36. Black AK. Urticarial vasculitis. Clin Dermatol. (1999) 17:565–9. doi: 10.1016/S0738-081X(99)00062-0
37. Segelmark M, Hellmark T. Anti-glomerular basement membrane disease: an update on subgroups, pathogenesis and therapies. Nephrol Dial Transplant. (2018). doi: 10.1093/ndt/gfy327. [Epub ahead of print].
38. Pusey CD, Lockwood CM, Peters DK. Plasma exchange and immunosuppressive drugs in the treatment of glomerulonephritis due to antibodies to the glomerular basement membrane. Int J Artif Organs. (1983) 6 (Suppl. 1):15–8.
39. Pusey CD, Bowman C, Peters DK, Lockwood CM. Effects of cyclophosphamide on autoantibody synthesis in the Brown Norway rat. Clin Exp Immunol. (1983) 54:697–704.
40. Soveri I, Mölne J, Uhlin F, Nilsson T, Kjellman C, Sonesson E, et al. Rapid clearance of anti-GBM antibodies by IgG degrading enzyme of streptococcus pyogenes (IdeS) in three patients with refractory anti-GBM disease. Kidney Int. (2019). doi: 10.1016/j.kint.2019.06.019
41. Szpirt WM. Plasma exchange in antineutrophil cytoplasmic antibody-associated vasculitis–a 25-year perspective. Nephrol Dial Transplant. (2015) 30 (Suppl. 1):i146–9. doi: 10.1093/ndt/gfv051
42. Jayne DR, Gaskin G, Rasmussen N, Abramowicz D, Ferrario F, Guillevin L, et al. Randomized trial of plasma exchange or high-dosage methylprednisolone as adjunctive therapy for severe renal vasculitis. J Am Soc Nephrol. (2007) 18:2180–8. doi: 10.1681/ASN.2007010090
43. Augusto JF, Sayegh J, Delapierre L, Croue A, Tollis F, Cousin M, et al. Addition of plasma exchange to glucocorticosteroids for the treatment of severe Henoch-Schonlein purpura in adults: a case series. Am J Kidney Dis. (2012) 59:663–9. doi: 10.1053/j.ajkd.2011.12.015
44. Marson P, Monti G, Montani F, Riva A, Mascia MT, Castelnovo L, et al. Apheresis treatment of cryoglobulinemic vasculitis: a multicentre cohort study of 159 patients. Transfus Apher Sci. (2018) 57:639–45. doi: 10.1016/j.transci.2018.06.005
Keywords: vasculitis, ANCA, Streptococcus pygenes, anti-GBM antibody disease, autoantibodies
Citation: Segelmark M and Björck L (2019) Streptococcal Enzymes as Precision Tools Against Pathogenic IgG Autoantibodies in Small Vessel Vasculitis. Front. Immunol. 10:2165. doi: 10.3389/fimmu.2019.02165
Received: 13 June 2019; Accepted: 28 August 2019;
Published: 20 September 2019.
Edited by:
Giacomo Emmi, University of Florence, ItalyReviewed by:
Luca Quartuccio, University of Udine, ItalyHaner Direskeneli, Marmara University, Turkey
Copyright © 2019 Segelmark and Björck. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mårten Segelmark, bWFydGVuLnNlZ2VsbWFya0BtZWQubHUuc2U=