
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Immunol., 20 August 2019
Sec. Autoimmune and Autoinflammatory Disorders
Volume 10 - 2019 | https://doi.org/10.3389/fimmu.2019.01974
This article is part of the Research TopicSkin AutoimmunityView all 69 articles
 Sandra Saschenbrecker*
Sandra Saschenbrecker* Ingolf Karl
Ingolf Karl Lars KomorowskiChristian ProbstCornelia DähnrichKai FechnerWinfried Stöcker
Lars KomorowskiChristian ProbstCornelia DähnrichKai FechnerWinfried Stöcker Wolfgang Schlumberger
Wolfgang SchlumbergerAutoimmune bullous dermatoses (AIBD) encompass a variety of organ-specific autoimmune diseases that manifest with cutaneous and/or mucosal blisters and erosions. They are characterized by autoantibodies targeting structural proteins of the skin, which are responsible for the intercellular contact between epidermal keratinocytes and for adhesion of the basal keratinocytes to the dermis. The autoantibodies disrupt the adhesive functions, leading to splitting and blister formation. In pemphigus diseases, blisters form intraepidermally, whereas in all other disease types they occur subepidermally. Early identification of autoimmune bullous dermatoses is crucial for both treatment and prognosis, particularly as regards tumor-associated disease entities. The diagnosis is based on clinical symptoms, histopathology, direct immunofluorescence to detect antibody/complement deposits, and the determination of circulating autoantibodies. The identification of various target antigens has paved the way for the recent development of numerous specific autoantibody tests. In particular, optimized designer antigens and multiplex test formats for indirect immunofluorescence and ELISA have enhanced and refined the laboratory analysis, enabling highly efficient serodiagnosis and follow-up. This review elaborates on the current standards in the serological diagnostics for autoimmune bullous dermatoses.
Autoimmune bullous dermatoses (AIBD) are associated with autoantibodies that bind to structural proteins in the skin and mucous membranes, which are components of desmosomes (e.g., desmogleins, desmocollins, plakins) and hemidesmosomes (e.g., BP180, BP230, plectin, α6β4 integrin, laminin 332, laminin γ1, type VII collagen) [Figure 1, (1)]. These autoimmune reactions interfere with intercellular connections and anchoring mechanisms within the epidermis and dermal-epidermal junction, leading to the separation of skin layers and the formation of blisters and/or erosions (2, 3). The most important AIBD types and corresponding target antigens are summarized in Table 1.
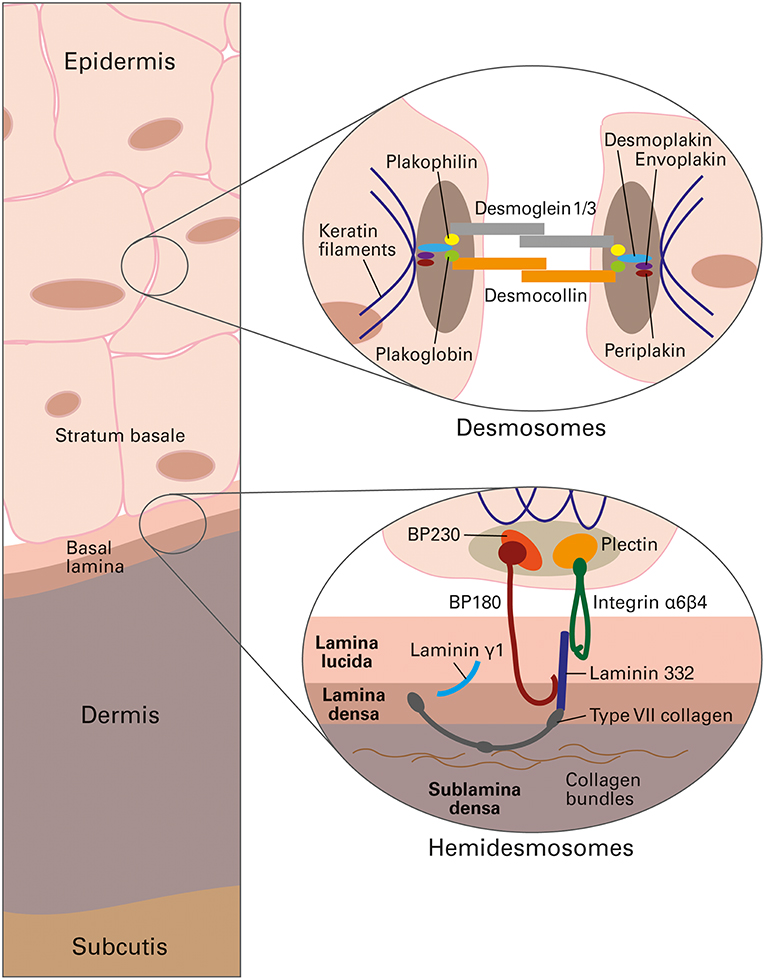
Figure 1. Schematic presentation of human skin, depicting the targets of autoantibodies in autoimmune bullous dermatoses, reproduced from Gosink and Schlumberger, MEDLAB Magazine 2016 (1) with permission of MEDLAB Magazine. Top circle: antigenic structural components of desmosomes, which interconnect the cytoskeletons of neighboring keratinocytes in the epidermis. Bottom circle: antigenic structural components of hemidesmosomes, which anchor the cells of the epidermal stratum basale in the underlying basal lamina at the dermal-epidermal junction.
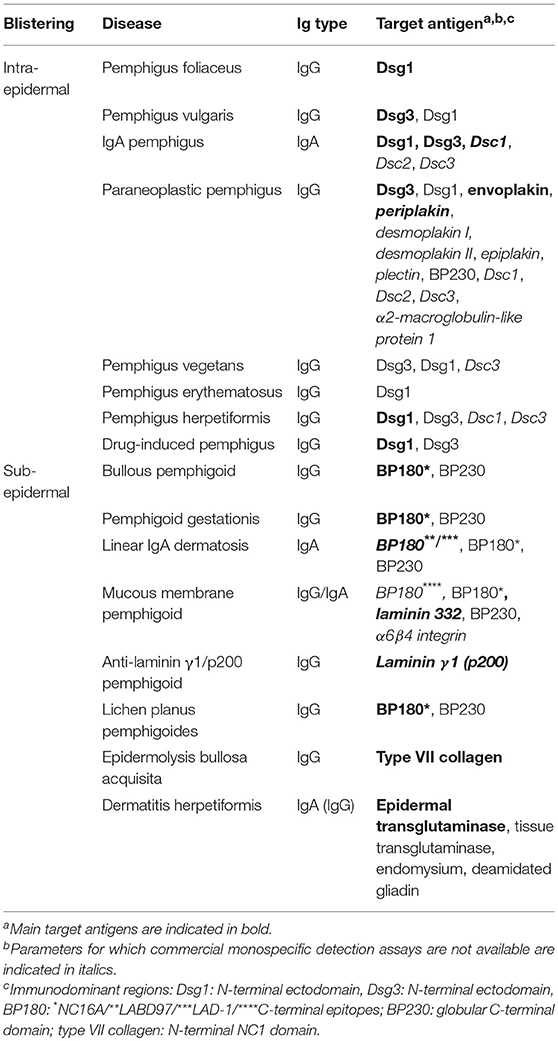
Table 1. Autoantibody specificities in autoimmune bullous dermatoses.
In pemphigus diseases, the autoimmune system targets primarily the cadherin-type transmembrane adhesion molecules desmoglein (Dsg) 1 and 3. Desmogleins, together with desmocollins, provide cohesion between epidermal keratinocytes, and are linked intracellularly to the intermediate filament network via different types of plakins (Figure 1). In response to autoantibody binding, cell metabolism, intracellular signaling and desmosome structure are subject to alterations that cause the loss of cell-to-cell adhesion (acantholysis) and intra-epidermal split formation, resulting in flaccid blisters and erosions in the skin and/or mucous membranes (4, 5).
The clinical phenotype of pemphigus (i.e., the site of blister formation) is determined by the underlying antibody profile and the normal tissue distribution of Dsg1 and Dsg3. Dsg1 is predominantly expressed on the surface of the epidermis, whereas Dsg3 accumulates mainly in deeper epidermal layers and in the mucous membranes. As pemphigus foliaceus (PF) is associated only with IgG autoantibodies against Dsg1, blistering is confined to the upper skin, while there is no apparent mucosal involvement. In pemphigus vulgaris (PV), Dsg3 is the major autoantigen, but 50–60% of patients have additional autoantibodies to Dsg1. PV manifests as three different subtypes (2): [i] in mucosal-dominant PV, antibodies are restricted to Dsg3 and induce blisters in deep layers of the oral mucosa; [ii] patients with mucocutaneous PV exhibit reactivity against both Dsg1 and Dsg3 and show involvement of the epidermis in addition to the mucous membranes; [iii] the cutaneous PV type is less frequent and associated with blistering in deep epidermal layers owing to anti-Dsg1 and pathogenically weak anti-Dsg3. In contrast to PF, acantholysis takes place in the lower skin layers (2, 6–11). PV is the most frequent intraepidermal AIBD, accounting for 80% of all pemphigus cases and, for the most part, affecting middle-aged and elderly persons.
In patients with PV, numerous autoantibodies have been identified that target other structural and metabolic proteins, such as desmocollins (Dsc) 1 and 3, muscarinic and nicotinic acetylcholine receptors, mitochondrial antigens, thyroid peroxidase, hSPCA1, plakophilin 3, plakoglobin, and E-cadherin. Studies on the pathogenic role of some of these non-Dsg autoantibodies suggest that they synergistically complement the classic effects of anti-Dsg autoantibodies in the complex process of pemphigus pathogenesis (12–15).
IgA pemphigus (also referred to as “intercellular IgA dermatosis”) (16, 17) has been found in association with serum IgA reactivity against desmosomal cadherins, i.e., Dsc1, Dsc2, Dsc3, Dsg1, and Dsg3 (18–21).
Paraneoplastic pemphigus is a life-threatening form of pemphigus that is associated with a neoplasm (e.g., non-Hodgkin's lymphoma, chronic lymphocytic leukemia, Castleman tumor, thymoma, sarcoma, Waldenstrom's macroglobulinemia) (22). Pathogenesis is based on a combination of humoral and cellular autoimmune responses (23). Circulating autoantibodies are directed against multiple antigens, including predominantly plakins (envoplakin, periplakin, desmoplakin I, desmoplakin II, epiplakin, plectin, BP230), but also cadherins (Dsg3, Dsg1, Dsc1, Dsc2, Dsc3), α2-macroblobulin-like 1 (24–34). Due to their high specificity (91–100%), anti-envoplakin autoantibodies are considered an important diagnostic marker for paraneoplastic pemphigus (35–38).
In addition, the pemphigus group includes several (atypical) variants, such as pemphigus vegetans (39), pemphigus erythematosus (40, 41), pemphigus herpetiformis (42), endemic pemphigus (fogo selvage etc.) (43), and drug-induced pemphigus (44, 45).
The heterogenous group of pemphigoid diseases is characterized by subepidermal blister formation, which can occur in the skin and mucous membranes (3). Circulating autoantibodies target components of the dermal-epidermal junction (Figure 1) (46). As the targeted hemidesmosomal proteins and structural filaments provide contact between the epidermal cells and the basement membrane, the autoimmune reactions cause the epidermis to peel away from the underlying dermis.
Bullous pemphigoid (BP) is the most common AIBD and occurs primarily in the elderly (onset in the late 70s) (47). It manifests with tense, bulging blisters on inflamed or non-inflamed skin, while mucous membranes are rarely affected. Patient serum contains IgG targeting mainly the hemidesmosomal proteins BP180 and BP230. BP180 is a transmembrane glycoprotein whose major immunogenic epitopes are located in the extracellular 16th non-collagenous domain (BP180-NC16A) (48). Due to their high prevalence, anti-BP180 autoantibodies represent the most important serological marker for BP. BP230 is a cytoplasmic protein which interacts with BP180. Its globular C-terminal domain mediates the attachment of keratin filaments to the hemidesmosomal plaque and contains the majority of immunoreactive sequences (49). Anti-BP230 positivity occurs in a subset of anti-BP180 negative BP patients, making it an important additional marker (50–54). Many BP sera also exhibit reactivity against antigenic sites outside the immunodominant domains of BP180 and BP230, which should be addressed in those BP patients unreactive with the immunodominant domains (<10%) (52, 55).
Pemphigoid gestationis is a manifestation of BP occurring in pregnant women and in puerperium, presenting with urticarial plaques and/or tense blisters. BP180-NC16A is the main target (90%) of autoantibodies in patients with pemphigoid gestationis, while anti-BP230 reactivity is less prevalent (56, 57).
The serological hallmark in linear IgA dermatosis is anti-basement membrane reactivity of class IgA autoantibodies recognizing the 120 kDa ectodomain fragment of BP180, referred to as linear IgA disease antigen 1 (LAD-1) and a derivative thereof (linear IgA bullous disease antigen of 97 kDa, LABD97) (58–61). A small proportion of sera recognizes BP180-NC16A or BP230 (62–64).
Mucous membrane pemphigoid affects one or more mucous membranes (e.g., oral, ocular, genital, anal) and may also involve the skin. Patients exhibit low-titer IgG/IgA autoantibodies directed against components of the basement membrane zone, with BP180 and laminin 332 presenting the two major targets (65). Anti-BP180 reactivity is not only directed against the NC16A domain, but also against C-terminal extracellular epitopes (66–69). The identification of anti-laminin 332 positive patients is vitally important as they have an increased relative risk for cancer, with malignancies occurring in about 25–30% of cases (70–73). Furthermore, patients with mucous membrane pemphigoid may exhibit increased IgG/IgA against BP230 (74, 75) or α6β4 integrin, the latter indicating the presence of ocular lesions (76, 77).
In anti-laminin γ1/p200 pemphigoid, tense blisters can be found on erythematosus or normal skin, with a high tendency to affect acral surfaces (78, 79). The associated autoantibodies target a 200-kDa basement membrane protein, referred to as laminin γ1 (80, 81).
Lichen planus pemphigoides emerges with bullous skin lesions in conjunction with lichen planus. Compared to BP, this disease has a much lower incidence, affects younger patients (onset 40–50 years), is usually less severe and arises mainly on the limbs (82). Serum reactivity is preferentially directed against C-terminal epitopes in the immunodominant NC16A domain of BP180 (83, 84).
Epidermolysis bullosa acquisita (EBA) is a rare, subepidermal blistering disease that can occur at any age. Patients suffer from chronic inflammation, blistering and scarring of the skin and mucous membranes. (85, 86). A characteristic feature is the presence of autoantibodies directed against type VII collagen, the main constituent of anchoring fibrils at the dermal-epidermal junction, with the major antigenic epitopes located within the amino-terminal non-collagenous domain (NC1) (87–90).
Dermatitis herpetiformis (Duhring's disease) is the cutaneous manifestation of coeliac disease (sprue, gluten-sensitive enteropathy), affecting about 10% of coeliac patients. It is characterized by blisters forming in deeper (subepidermal) layers of the skin, while the mucous membranes do not show any blistering. The targets of circulating IgA antibodies are epidermal/tissue transglutaminase, endomysium, and deamidated gliadin (91–95). Since the underlying gluten-sensitive enteropathy is frequently associated with selective IgA deficiency, the additional determination of class IgG antibodies can be diagnostically indicated (96).
The diagnosis of AIBD is detailed in recent publications (97–104). Commonly recommended approaches are based on several pillars that cover symptomatic evaluation and laboratory tests.
Firstly, the clinical characteristics have to be determined, including patient history, physical examination, and assessment of the disease activity (105).
Secondly, histopathology is performed on lesional skin or mucosal biopsy. Although of limited diagnostic value, the observation of intra-/subepidermal cleavage and inflammatory infiltrates can give a first information for differentiation between pemphigus and pemphigoid diseases.
Thirdly, direct immunofluorescence (DIF) microscopy using cryosections of perilesional biopsy specimens is performed to detect tissue-bound autoantibodies. This method is still the diagnostic gold standard, with a sensitivity in the range of 82–91% and a specificity of 98% (106–110), but it provides only limited information on the target antigens. DIF microscopy narrows down the diagnosis according to the deposited Ig subclass and binding pattern (103). For example, intercellular deposition of IgG and/or C3 in the epidermis is characteristic of PV, PF, and paraneoplastic pemphigus. By contrast, linear binding of IgG and/or C3 at the dermal-epidermal junction can be found in pemphigoid diseases, with further differentiation options based on the serration pattern (u-serration vs. n-serration) (103, 111). Granular IgA deposits along the basement membrane zone and at the dermal papillae tips are observed in dermatitis herpetiformis.
The fourth pillar addresses the serological detection and differentiation of circulating autoantibodies. Serology has the advantage of being minimally invasive, which is particularly helpful in cases where biopsy specimens cannot be obtained (children, uncooperative adults). In many cases, serological testing may even suffice to establish the diagnosis in conjunction with a compatible clinical picture (112). Serum analysis relies on indirect immunofluorescence (IIF) microscopy using native tissue sections and recombinant proteins as substrates. Recombinant antigens are also applied in immunoblot or immunoprecipitation analyses and in enzyme-linked immunosorbent assays (ELISA), the latter having additional relevance to the monitoring of disease activity. Conventionally, the serological diagnosis of AIBD follows a multi-step approach that is based on initial IIF screening using one or two tissue substrates, followed by individual antigen-specific assays (ELISA, immunoblot) that correspond to the clinical suspicion and the IIF screening results. Meanwhile, alternative approaches for highly efficient and expeditious testing are available utilizing multiparametric analysis tools (113, 114). In clinical practice, routine serological results should be interpreted with care, taking into consideration the possibility of discrepancies between IIF and ELISA or negative serology in biopsy-proven patients. Assay results may even be positive in cases without other laboratory or clinical evidence of pemphigus (109, 115). Such inconsistent findings complicate decision-making, bearing the risk of misdiagnosis. Where available, alternative serological methods (e.g., keratinocyte binding assay) may provide additional information to ascertain or rule out a diagnosis, especially when no biopsy is available (115).
Early diagnosis and differentiation of AIBD is crucial for the initiation of an appropriate treatment. In most AIBD entities (e.g., BP, linear IgA disease, anti-laminin γ1/p200 pemphigoid), systemic corticosteroids in combination with further immunosuppressants/-modulants are sufficient to induce clinical remission, whereas treatment of pemphigus remains challenging as reflected by a mortality of 8–42% in mucocutaneous PV (116). However, prognosis has improved due to the development of new therapy options, including immunoadsorption, intravenous immunoglobulins, and anti-CD20 monoclonal antibodies (2, 112, 116–124). In paraneoplastic pemphigus and anti-laminin 332 mucous membrane pemphigoid, the disease prognosis may be unfavorable due to associated neoplasia in 100% and in up to 30% of cases, respectively (73, 125).
IIF microscopy using tissue substrates has traditionally been performed as a standard method for the detection of autoantibodies in AIBD. Due to their high sensitivity, these substrates have priority for screening purposes. However, they do not allow definite determination of the autoantibodies' specificity (e.g., differentiation between anti-Dsg1 and anti-Dsg3).
Esophagus from monkey or guinea pig is a highly sensitive substrate. Two characteristic immunofluorescence patterns can be differentiated on this tissue. [i] Pemphigus-specific autoantibodies result in a honeycomb-like fluorescence of the intercellular substance in the stratum spinosum. These autoantibodies are directed against prickle cell desmosomes, reacting with surface antigens of keratinocytes (Figure 2A). [ii] A fine linear staining between the stratum basale and the connective tissue is caused by anti-basement membrane zone autoantibodies, which are associated with pemphigoid diseases or EBA (Figure 2B).
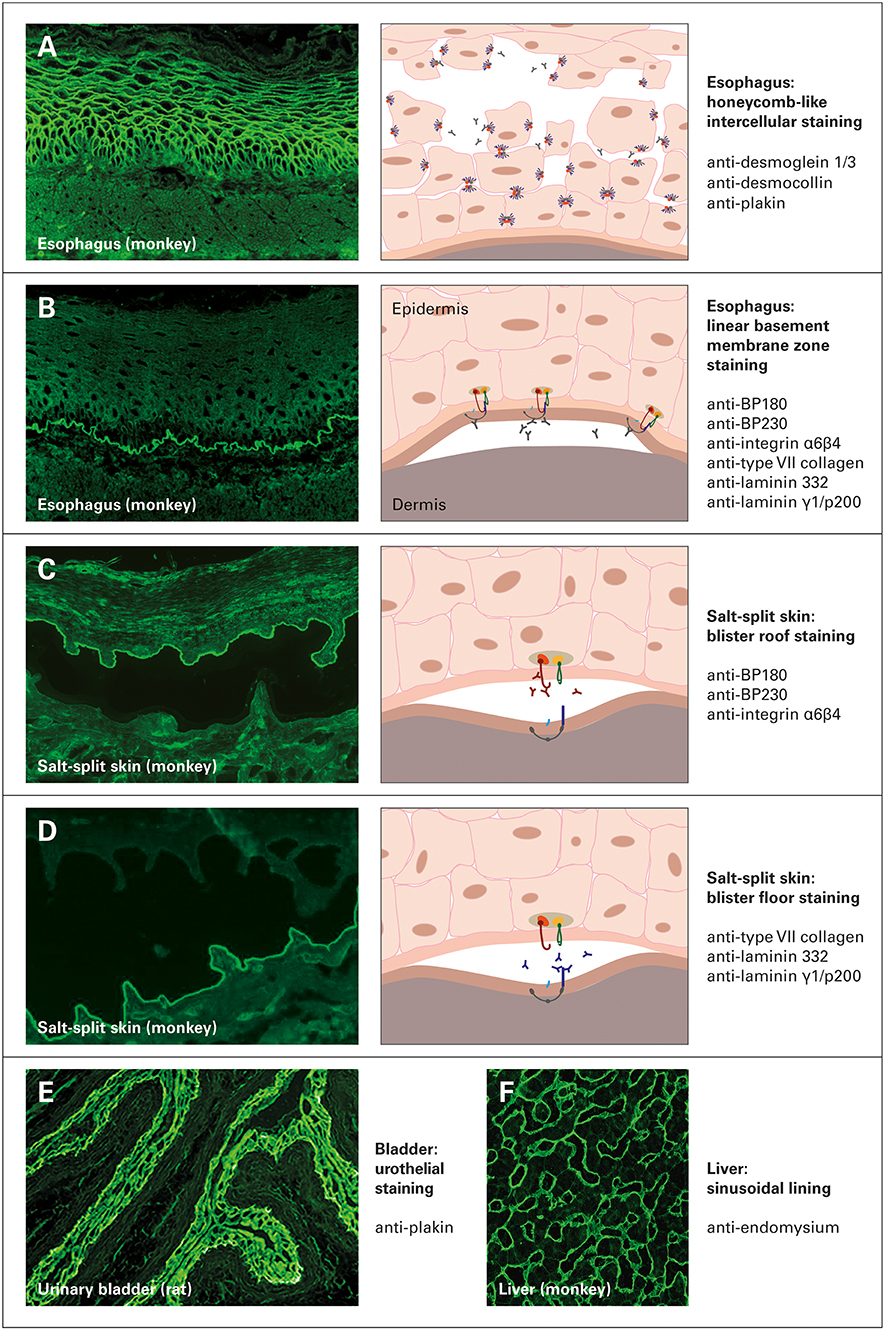
Figure 2. Indirect immunofluorescence staining of different tissue substrates in autoimmune bullous dermatoses. (A,B) Monkey esophagus, (C,D) monkey salt-split skin, (E) rat urinary bladder and (F) monkey liver. Graphics and annotations on the right indicate the staining patterns and possible underlying reactivities, reproduced and modified from Euroimmun customer leaflet, with permission of Euroimmun, Germany.
When pemphigus serum is applied, monkey esophagus yields a sensitivity of 81–100% and a specificity of 89–100%, making it the optimal substrate in the screening for intercellular antibodies in suspected cases of PV and PF (113, 126–132). This substrate has often been reported to be more sensitive for PV than for PF as monkey esophagus is a mucosal tissue with high expression of Dsg3, the major target in PV, in contrast to lower Dsg1 expression (132). The predictive value of a negative test result is highly reliable to exclude the diagnosis of pemphigus, and false-positive results (intercellular staining of non-pemphigus sera) is not associated with an increased risk of developing pemphigus subsequently (132). In BP, 68–73% of cases were reported positive for anti-basement zone antibodies, at a specificity of 97% (51, 106, 133). It should be taken into account that antibodies against blood group antigens A and B may lead to unspecific desmosome fluorescence on monkey esophagus, potentially leading to false positive results. As this interference may account for up to 10% of healthy blood donors, adsorption reagents should be applied in suspected cases (e.g., blocking with soluble A/B antigens or with red blood cells from an AB-positive donor) (134).
Skin, in which partial dermal-epidermal splitting is induced by incubation with a 1 M NaCl solution, presents the IIF substrate of choice when screening for autoantibodies in subepidermal AIBD (135, 136). It is optimally suited for the detection of anti-basement membrane zone autoantibodies, as reflected by a reported sensitivity of 73–96% and a specificity of 97% (106, 108, 133, 137). In addition, it allows the differentiation between autoantibodies with different antigenic binding properties. Anti-BP180, anti-BP230, and anti-α6β4 integrin stain the epidermal side of the artificial split (blister roof), as detectable in BP, pemphigoid gestationis, linear IgA dermatosis, and anti-BP180-type mucous membrane pemphigoid (Figure 2C). In contrast, anti-type VII collagen, anti-laminin 332, and anti-laminin γ1 bind along the dermal side of the split (blister floor), pointing toward EBA, anti-laminin-332-type mucous membrane pemphigoid, and anti-laminin γ1/p200 pemphigoid, respectively (Figure 2D) (100, 138).
In suspected cases of paraneoplastic pemphigus, IIF on rat (or monkey) urinary bladder is performed to detect autoantibodies against plakins and to distinguish paraneoplastic pemphigus from other pemphigus diseases. As envoplakin, periplakin, and desmoplakins (but not Dsg1 and Dsg3) are highly expressed in bladder tissue, and owing to the high specificity of this substrate (74% sensitivity, 99–100% specificity), positive IgG reactivity with the urothelium is considered a diagnostic indication of paraneoplastic pemphigus (38, 139) (Figure 2E). However, negative IIF on bladder does not exclude the diagnosis of paraneoplastic pemphigus and should entail other serological techniques (36, 38).
Tissue sections of primate liver are best suited to visualize autoantibodies (IgA) against endomysium in dermatitis herpetiformis. Positive reactivity is indicated by a fluorescent filamentous lining of the intralobular sinusoids (140) (Figure 2F).
The identification of the autoantibodies' target antigens can be accomplished using monospecific IIF, ELISA and/or immunoblot tests. For this purpose, many antigenic substrates have been made available by means of recombinant expression systems. By selecting only immunoreactive epitopes and deleting domains that cause unspecific reactions, the sensitivity and specificity of the resulting assay can often be improved (141). For example, a recombinant tetramer of the immunodominant NC16A domain of BP180, termed BP180-NC16A-4X, was designed to multiply the number of antibody binding sites per molecule, thereby optimizing the immunoreactivity and diagnostic efficiency in BP serology. A second example concerns a gliadin-analogous fusion peptide (GAF-3X), which contains three repetitive modified copies of formerly described peptides recognized by autoantibodies in most patients with coeliac disease and dermatitis herpetiformis (142). After expression and purification from Escherichia coli, those two antigens were applied in IIF and ELISA (142–145).
Compared to classic tissue sections that contain a multitude of different antigens and sometimes require specialist knowledge for reliable interpretation, recombinant substrates considerably simplify IIF evaluation and may allow a prima vista differentiation between AIBD-associated diseases. Recombinant IIF assays are based on BIOCHIP technology (Euroimmun, Lübeck, Germany), in which the substrates are coated onto millimeter-sized BIOCHIPs and arranged on the reaction fields of microscope slides. The slides are incubated using the Titerplane technique, which provides parallel incubation of multiple samples under standardized, identical conditions (146). Two types of recombinant IIF substrates can be distinguished:
In the first case, the target antigen is expressed in the human cell line HEK293, which provides authentic conformational folding and post-translational modification (141, 147). Since transfected and mock-transfected control cells are coated onto the BIOCHIPs side by side, it is straightforward to distinguish true-positive sera containing antigen-specific antibodies (smooth to fine granular cytosolic fluorescence only in the subset of transfected cells) from sera reacting against other cell components (nuclear or cytoplasmic staining of all cells). Available recombinant cell-based substrates for AIBD serology include Dsg1, Dsg3, BP230, and type VII collagen (Figures 3A–D) (144, 149).
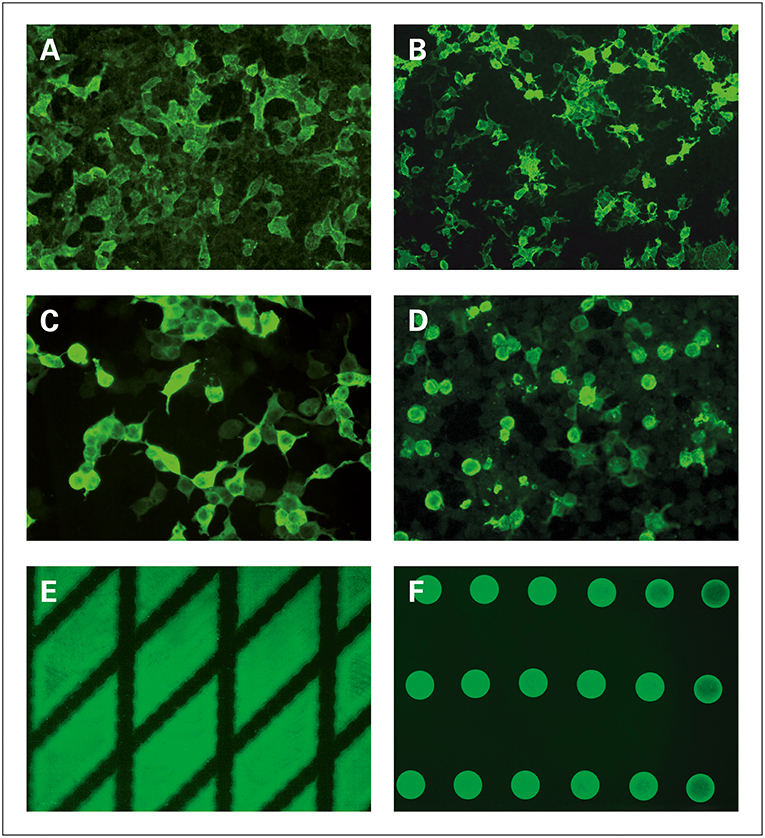
Figure 3. Detection and differentiation of autoantibodies in autoimmune bullous dermatoses using monospecific substrates for BIOCHIP-based indirect immunofluorescence, reproduced (in part) from Gosink and Schlumberger, MEDLAB Magazine 2016 (1) and from Gosink, MEDLAB Magazine 2013 (148) with permission of MEDLAB Magazine. (A–D) Substrates based on human embryonic kidney (HEK293) cells expressing recombinant immunodominant antigen domains: (A) Dsg1 (ectodomain), (B) Dsg3 (ectodomain), (C) BP230gC (globular C-terminal domain), (D) type VII collagen (NC1 domain). (E,F) Substrates generated by spotting purified recombinant protein: (E) BP180-NC16A-4X (tetrameric NC16A domain), (F) GAF-3X (trimeric deamidated gliadin-analogous fusion peptide).
In the second case, purified recombinant antigens (e.g., BP180-NC16A-4X and GAF-3X) are coated directly onto the BIOCHIPs. If a positive serum sample is applied, the antigenic areas will fluoresce in a particular pattern (e.g., diamonds or circles) against a dark background (Figures 3E,F).
The recombinant monospecific IIF substrates can be analyzed side by side with classic tissue sections in standardized BIOCHIP mosaics (Euroimmun; Figure 4). The combination of different substrates in the same test field allows autoantibody screening and confirmatory discrimination to be carried out in a single incubation, thus facilitating differential diagnosis among the various types of AIBD. Particularly in diagnostically difficult cases, this multiparametric technique is cost- and time-effective compared to the conventional multi-step approach (113, 150).
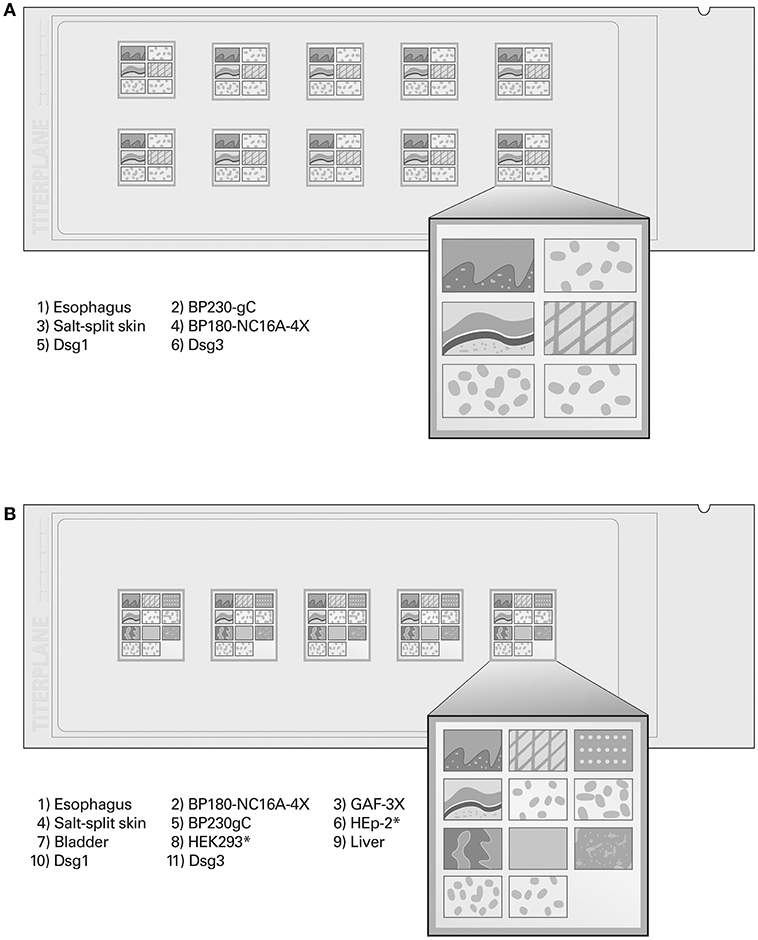
Figure 4. BIOCHIP mosaics for simultaneous screening and monospecific confirmation of autoantibodies using indirect immunofluorescence, modified from Gosink, MEDLAB Magazine 2013 (148) with permission of MEDLAB Magazine. (A) “Dermatology Mosaic 7” (six substrates per reaction field). (B) “Dermatology Mosaic 11” (11 substrates per reaction field for extended analysis including paraneoplastic pemphigus and dermatitis herpetiformis). As indicated, the BIOCHIPs are coated with tissue sections (monkey esophagus, salt-split skin, liver, rat urinary bladder), HEK293 cells expressing recombinant antigens (Dsg1, Dsg3, BP230gC), or spots of purified recombinant antigen (BP180-NC16A-4X, GAF-3X). *HEp-2 and mock-transfected HEK293 cells serve as negative control substrates.
Several studies have been performed on the diagnostic performance of the mosaic-based IIF technique. Cumulative findings indicate that this method is highly sensitive and specific for pemphigus and BP (150–152). For example, monkey esophagus yielded sensitivities of 83–100% (PV), 98% (PF), and 69% (mixed pemphigus panel), with specificities in the range of 89–100%. Anti-Dsg1 was detectable with a sensitivity of 19–52% (PV), 90% (PF), and 38% (mixed pemphigus panel) and a specificity of ≥99%. The sensitivity of anti-Dsg3 detection amounted to 98–100% (PV) and 87% (mixed pemphigus panel), with specificities ranging from 97 to 100% (113, 152–154). In BP, basement membrane zone staining on esophagus and/or salt-split skin provided a sensitivity and specificity of 50–99 and 77–100%, respectively. The sensitivity and specificity for anti-BP180 detection were reported to be 83–100 and 97–100%, respectively, and for anti-BP230 detection 30–67 and 97–100%, respectively (113, 144, 152, 154, 155). van Beek et al. (113) compared the performance of the “Dermatology Mosaic 7” (Figure 4A) with the conventional multi-step procedure (156). Between both approaches, high diagnostic agreement (94%, kappa 0.88–0.97) was observed. In <5% of the cases, final diagnosis could only be made by using the appropriate assays within the multi-step approach, because additional substrates would have to be added to the standard IIF mosaic for these rare disorders. Meanwhile, however, further mosaics adjusted to the diagnosis of particular AIBD types have been evaluated, including the detection of [i] anti-BP180 in pemphigus gestationis (100% sensitivity, 100% specificity) (157), [ii] anti-type VII collagen NC1 in EBA (92% sensitivity, 100% specificity) (149), [iii] anti-laminin 332 in mucous membrane pemphigoid (77–84% sensitivity, 100% specificity) (72), and [iv] anti-Dsc in atypical pemphigus variants (158). Tampoia et al. compared the concordance between results obtained by mosaic-based IIF vs. ELISA (MBL/Euroimmun) and found excellent agreements for the determination of anti-Dsg3 (kappa 0.97–1.00) and anti-BP180 (kappa 0.94–0.90) (154). Özkesici et al. reported correlations between mosaic-based IIF and ELISA (Euroimmun) of 85% (anti-Dsg1), 94% (anti-Dsg3), and 98% (anti-BP180) (152).
ELISA systems based on recombinant target antigens are widely available and increasingly applied in the serological diagnosis of AIBD. They are used to confirm and differentiate autoantibody specificities, supporting the diagnostic attribution of AIBD subtypes. Moreover, ELISA allow quantitative measurement of antibody levels, enabling disease and therapy monitoring, as described below. In most cases, ELISA are sufficient to support the diagnosis and cheaper than other complex techniques. Further advantages include standardization, objective data, easy handling, automated processing, high throughput, and (for most parameters) commercial availability.
Commercial ELISA systems (MBL, Euroimmun) are available for the detection of autoantibodies against Dsg1 and Dsg3 in pemphigus (147, 159) and against envoplakin in paraneoplastic pemphigus (36). In pemphigoid diseases, commercial ELISA (MBL, Euroimmun) include BP180 (143, 160), BP230 (50, 54), and type VII collagen (149, 161). Importantly, the highest detection rate among BP patients is achieved by combining the ELISA results for anti-BP180 and anti-BP230 (87–100%), reflecting a diagnostic added value compared to mere anti-BP180 testing (50–54). Therefore, in cases with clinically suspected cases of BP, where anti-BP180 testing is negative, it is recommended to analyze serum reactivity against BP230 (97). Moreover, ELISA for the detection of autoantibodies against deamidated gliadin and transglutaminase (92) are available, supporting the diagnosis of dermatitis herpetiformis. Besides, less standardized in-house ELISA systems are applied in specialized laboratories, including rare parameters, such as anti-laminin γ1 (162), anti-desmocollin (20, 33), anti-laminin 332 (71, 163), and anti-BP180 (various forms) (52, 164). The diagnostic performance of commercial and in-house ELISA systems has been examined in numerous studies (Table 2) and discussed in reviews by Tampoia et al. (190) and Horvath et al. (165).
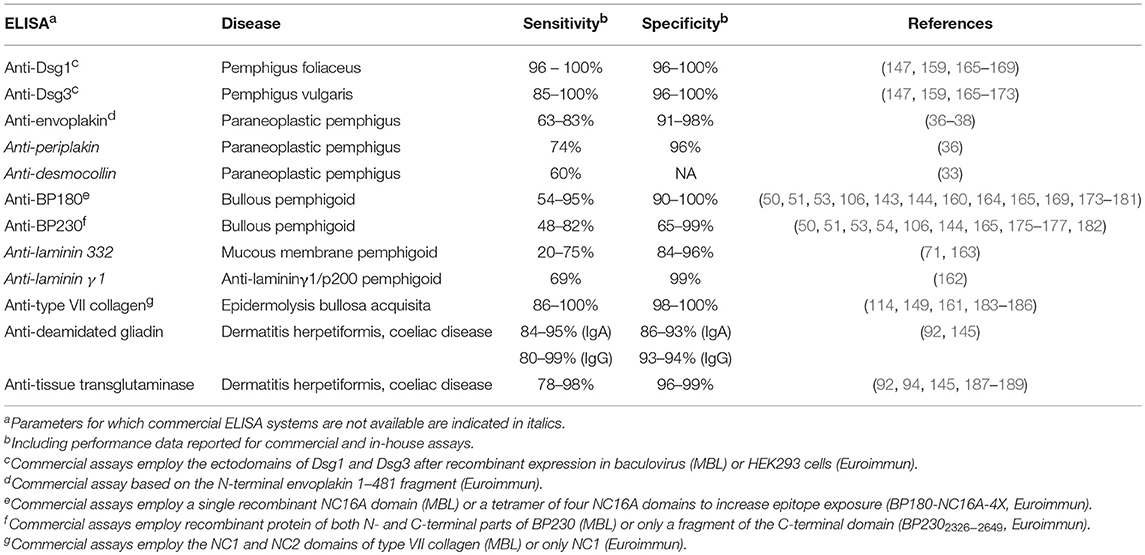
Table 2. Performance characteristics of reported ELISA systems for the detection of autoantibodies in autoimmune bullous dermatoses.
Although being highly sensitive and specific, ELISA may produce positive results without clinical or other laboratory evidence.
In order to further improve and accelerate the routine serological diagnosis of AIBD, two profile ELISA systems have been developed that enable multiparametric antigen-specific testing for autoantibodies in adjacent wells of a microplate. By simultaneous processing of the diagnostically most relevant antigens, multiplex ELISA offer an alternative to IIF as serological first-line approach and to a multi-step single testing strategy.
Horvath et al. analyzed the diagnostic performance of the MESACUP Anti-Skin Profile (MBL), which covers five target antigens: Dsg1, Dsg3, BP180, BP230, and type VII collagen. They reported a 88% concordance with data obtained from the respective individual ELISA systems (MBL), resulting in sensitivities of 92% (anti-Dsg1, PF), 93% (anti-Dsg3, PV), 66% (anti-BP180, BP), 62% (anti-BP230, BP), and 81% (anti-type VII collagen, EBA), and specificities of 98–100% (165).
Van Beek et al. validated the Dermatology Profile ELISA (Euroimmun), comprising the same five parameters plus additional envoplakin. They demonstrated sensitivities of 95% (anti-Dsg1, PF), 100% (anti-Dsg3, PV), 95% (anti-BP180, BP), 60% (anti-BP230, BP), 93% (anti-type VII collagen, EBA), and 86% (anti-envoplakin, paraneoplastic pemphigus), and specificities in the range of 97–100% (114). These performance characteristics were also similar to those obtained with the individual ELISA (Euroimmun) (36, 54, 143, 147, 149). Comparison of the Dermatology Profile to the conventional multi-step approach yielded concordant results in 87%. Incongruent results were attributed to the lack of IgA detection and reactivity against antigens not included in the profile ELISA (114).
Immunoblotting and immunoprecipitation help to determine rather rare autoantibodies (e.g., anti-laminin γ1, anti-laminin 332, anti-LAD-1, anti-α6β4 integrin, anti-desmoplakin, anti-type VII collagen) and are based on recombinant proteins or cell extracts (e.g., epidermis, dermis, cultured keratinocytes) (28, 69, 80, 191–193). These tests, however, are time-consuming and available only as in-house assays in specialized laboratories. They allow for highly specific autoantibody detection, but have proven inadequate for targets with mainly conformational epitopes, such as Dsg1 and Dsg3 (127, 141, 194–196). Immunoblotting for anti-Dsg is thus not recommended in the diagnosis of PF/PV (97). In contrast, there are patients suspected of having pemphigoid disease who show positive DIF results in the absence of autoantibody reactivity by commercial ELISA systems. In such cases, immunoblotting using antigenic fragments outside the immunodominant domains may provide diagnostically relevant information on the autoantibodies' target.
Autoantibodies in several AIBD entities are directly pathogenic (4, 197–205). Their titers correlate with the disease activity over time, as reported for anti-Dsg1, anti-Dsg3 (147, 159, 166, 170, 206–209), anti-BP180 (51, 52, 143, 160, 210–214), and anti-type VII collagen (161, 183, 184, 215). By contrast, anti-BP230 reactivity appears not to fluctuate with changes in the clinical course of BP patients or only in a small subset of cases (50–52).
IIF evaluation is subjective and produces only semiquantitative data, based on serial serum dilutions, with titers depending on the type of substrate due to variable antigen expression levels. As opposed to this, ELISA provide objective and quantitative scores, which tend to reflect the disease activity better than IIF titers (130, 160). Therefore, ELISA testing is routinely used in many laboratories for the monitoring of disease activity. However, the relationship is not always perfect as there are cases of active disease with negative ELISA results and vice versa, as well as cases where antibody levels do not fluctuate in correlation with clinical activity (116, 209).
As an adjunct to the paramount clinical assessment, the follow-up of autoantibody titers has relevance for disease monitoring and can be helpful in therapeutic decisions, such as adjusting the dose of immunosuppressants. For example, when lesions have healed, decreasing or undetectable autoantibody levels may indicate dosage reduction or omission, respectively. In addition, relapses may be anticipated by the detection of increased autoantibody levels (99). However, the clinical judgement and the above-mentioned imperfections of the assays should always be taken into consideration (97, 116).
Several molecules involved in, e.g., autoimmune and inflammatory responses in AIBD have recently been identified as potential biomarkers for disease development and outcome. The measurement of these biomarkers could help to adapt the duration and intensity of treatment in order to prevent the occurrence of relapses. The relevance of stratifying patients at risk of relapse, preferably at initiation of treatment, is reflected by a rate of about 30% of clinical relapses within the first year of treatment in patients with BP (216).
In BP patients, the value of monitoring anti-BP180 autoantibodies as a potential risk factor for relapse has been demonstrated. It was found that anti-BP180 IgG levels are significantly higher at baseline in patients who experience a relapse compared to non-relapse cases, whereas no such association was observed for anti-BP230 IgG, serum IgE, and peripheral eosinophils (217, 218). A multicenter prospective study demonstrated that the decrease in anti-BP180 titers during the first 60 days of treatment is lower in patients with relapse than in patients with ongoing remission. In addition, high anti-BP180 levels at day 150 provide high sensitivity for a relapse between days 150–360 of treatment (219). Cai et al. confirmed that increasing anti-BP180 IgG titers are associated with a decreasing remission rate (220). Along with anti-BP180, the detection of autoantibodies against type VII collagen may help to stratify BP patients based on the observation that about 40% of relapsing cases display positive and increasing anti-type VII collagen serum levels at the time of relapse (221).
In addition, the follow-up of molecules involved in inflammatory mechanisms can contribute to the prediction of BP outcome. Amongst others, this pertains to serum concentrations of the cytokines interleukin 17 (IL-17) and IL-23. The former shows significant decreases in patients with ongoing remission as well as constantly elevated levels prior to relapse, whereas the latter increases in early treatment stages in patients who later relapse (222). Similarly, an increased release of the chemokine CXCL10 favors BP relapse within the first year of treatment (223). These three inflammatory biomarkers all upregulate the secretion by leukocytes of matrix-metalloproteinase-9 (MMP-9), which was shown to decrease over time upon remission and to remain elevated in patients who relapse. Consequently, the follow-up of protease MMP-9 expression is regarded as another promising tool for the prediction of relapse in BP (222, 223). Also the serum concentrations of eosinophil cationic protein (ECP), as a measure of eosinophil activation, may help to predict a relapse as indicated by the absence of ECP alterations under treatment (224).
Moreover, an increased expression of the glucocorticoid receptor-beta in skin epithelial cells was suggested to be predictive of reduced treatment efficacy and increased risk of BP relapse (225). The presence of extensive disease (more than ten new blisters daily) at baseline and of neurological conditions associated with BP (e.g., dementia) may also play a role in the prediction of BP outcome (219).
In patients with PV, anti-Dsg3 positivity and, to a lesser extent, positive DIF results are predictors of relapse (226). Positivity for anti-Dsg1 and anti-Dsg3 was shown to provide high predictive values for the occurrence of relapses following treatment (209, 227). In addition, B-cell repopulation and low CD4+ T-cell count are associated with relapses in patients with pemphigus (227).
Altogether, this relatively new field warrants further investigation and holds the potential to benefit both clinicians and patients. In particular, to link cytokine/chemokine variations to clinical practice, large prospective studies will have to confirm the findings to date.
Accurate diagnosis and discrimination of the different AIBD forms is crucial for therapeutic decisions and prognosis. Owing to highly sensitive and specific assays, it is estimated that a serological diagnosis can be made in about 90% of patients, subject to clinical expression (99, 112). Both the increasingly aging population and the constantly improved diagnostics cause a steady growth in the incidence of AIBD. In Germany, the annual incidence doubled within a decade, meanwhile amounting to about 25–30 cases per million inhabitants (112, 228). Hence, the continuous development and application of serological assays for known and yet unknown parameters will play a crucial role in the future. Patient management will further benefit from ongoing basic research on pathophysiological mechanisms and from clinical trials on forthcoming treatment options (229). For example, there is a growing number of data regarding the potential pathogenic role of IgE class autoantibodies in BP and the option of anti-IgE treatment (230–233).
SS performed the literature research, acquired and modified the figures, and wrote the first manuscript draft. IK, LK, CP, CD, KF, WSt, and WSc critically revised the manuscript. All authors have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
SS, IK, LK, CP, CD, and KF are employees of Euroimmun AG, a company that develops and manufactures immunoassays for the detection of disease-associated antibodies. WSt and WSc are board members of Euroimmun AG.
1. Gosink J, Schlumberger W. Multiplex serological diagnostics in autoimmune skin-blistering diseases. MEDLAB Magazine. (2016) 4:28–30.
2. Kasperkiewicz M, Ellebrecht CT, Takahashi H, Yamagami J, Zillikens D, Payne AS, et al. Pemphigus. Nat Rev Dis Primers. (2017) 3:17026. doi: 10.1038/nrdp.2017.27
3. Schmidt E, Zillikens D. Pemphigoid diseases. Lancet Lond Engl. (2013) 381:320–32. doi: 10.1016/S0140-6736(12)61140-4
4. Spindler V, Eming R, Schmidt E, Amagai M, Grando S, Jonkman MF, et al. Mechanisms causing loss of keratinocyte cohesion in pemphigus. J Invest Dermatol. (2018) 138:32–7. doi: 10.1016/j.jid.2017.06.022
5. Di Zenzo G, Amber KT, Sayar BS, Muller EJ, Borradori L. Immune response in pemphigus and beyond: progresses and emerging concepts. Semin Immunopathol. (2016) 38:57–74. doi: 10.1007/s00281-015-0541-1
6. Amagai M, Koch PJ, Nishikawa T, Stanley JR. Pemphigus vulgaris antigen (desmoglein 3) is localized in the lower epidermis, the site of blister formation in patients. J Invest Dermatol. (1996) 106:351–5. doi: 10.1111/1523-1747.ep12343081
7. Amagai M. Pemphigus as a paradigm of autoimmunity and cell adhesion. Keio J Med. (2002) 51:133–9. doi: 10.2302/kjm.51.133
8. Shirakata Y, Amagai M, Hanakawa Y, Nishikawa T, Hashimoto K. Lack of mucosal involvement in pemphigus foliaceus may be due to low expression of desmoglein 1. J Invest Dermatol. (1998) 110:76–8. doi: 10.1046/j.1523-1747.1998.00085.x
9. Amagai M, Tsunoda K, Zillikens D, Nagai T, Nishikawa T. The clinical phenotype of pemphigus is defined by the anti-desmoglein autoantibody profile. J Am Acad Dermatol. (1999) 40:167–70. doi: 10.1016/S0190-9622(99)70183-0
10. Ding X, Aoki V, Mascaro JM Jr, Lopez-Swiderski A, Diaz LA, Fairley JA. Mucosal and mucocutaneous (generalized) pemphigus vulgaris show distinct autoantibody profiles. J Invest Dermatol. (1997) 109:592–6. doi: 10.1111/1523-1747.ep12337524
11. Mahoney MG, Wang Z, Rothenberger K, Koch PJ, Amagai M, Stanley JR. Explanations for the clinical and microscopic localization of lesions in pemphigus foliaceus and vulgaris. J Clin Invest. (1999) 103:461–8. doi: 10.1172/JCI5252
12. Kalantari-Dehaghi M, Anhalt GJ, Camilleri MJ, Chernyavsky AI, Chun S, Felgner PL, et al. Pemphigus vulgaris autoantibody profiling by proteomic technique. PLoS ONE. (2013) 8:e57587. doi: 10.1371/journal.pone.0057587
13. Amber KT, Valdebran M, Grando SA. Non-desmoglein antibodies in patients with pemphigus vulgaris. Front Immunol. (2018) 9:1190. doi: 10.3389/fimmu.2018.01190
14. Ahmed AR, Carrozzo M, Caux F, Cirillo N, Dmochowski M, Alonso AE, et al. Monopathogenic vs multipathogenic explanations of pemphigus pathophysiology. Exp Dermatol. (2016) 25:839–46. doi: 10.1111/exd.13106
15. Lakshmi MJD, Jaisankar TJ, Rajappa M, Thappa DM, Chandrashekar L, Divyapriya D, et al. Correlation of antimuscarinic acetylcholine receptor antibody titers and antidesmoglein antibody titers with the severity of disease in patients with pemphigus. J Am Acad Dermatol. (2017) 76:895–902. doi: 10.1016/j.jaad.2016.11.039
16. Tsuruta D, Ishii N, Hamada T, Ohyama B, Fukuda S, Koga H, et al. IgA pemphigus. Clin Dermatol. (2011) 29:437–42. doi: 10.1016/j.clindermatol.2011.01.014
18. Hisamatsu Y, Amagai M, Garrod DR, Kanzaki T, Hashimoto T. The detection of IgG and IgA autoantibodies to desmocollins 1–3 by enzyme-linked immunosorbent assays using baculovirus-expressed proteins, in atypical pemphigus but not in typical pemphigus. Br J Dermatol. (2004) 151:73–83. doi: 10.1111/j.1365-2133.2004.05995.x
19. Hashimoto T, Kiyokawa C, Mori O, Miyasato M, Chidgey MA, Garrod DR, et al. Human desmocollin 1 (Dsc1) is an autoantigen for the subcorneal pustular dermatosis type of IgA pemphigus. J Invest Dermatol. (1997) 109:127–31. doi: 10.1111/1523-1747.ep12319025
20. Muller R, Heber B, Hashimoto T, Messer G, Mullegger R, Niedermeier A, et al. Autoantibodies against desmocollins in European patients with pemphigus. Clin Exp Dermatol. (2009) 34:898–903. doi: 10.1111/j.1365-2230.2009.03241.x
21. Teye K, Numata S, Ohzono A, Ohyama B, Tsuchisaka A, Koga H, et al. Establishment of IgA ELISAs of mammalian recombinant proteins of human desmocollins 1–3. J Dermatol Sci. (2016) 83:75–7. doi: 10.1016/j.jdermsci.2016.04.001
22. Anhalt GJ. Paraneoplastic pemphigus. J Investig Dermatol Symp Proc. (2004) 9:29–33. doi: 10.1111/j.1087-0024.2004.00832.x
23. Kim JH, Kim SC. Paraneoplastic pemphigus: paraneoplastic autoimmune disease of the skin and mucosa. Front Immunol. (2019) 10:1259 doi: 10.3389/fimmu.2019.01259
24. Ohzono A, Sogame R, Li X, Teye K, Tsuchisaka A, Numata S, et al. Clinical and immunological findings in 104 cases of paraneoplastic pemphigus. Br J Dermatol. (2015) 173:1447–52. doi: 10.1111/bjd.14162
25. Schepens I, Jaunin F, Begre N, Laderach U, Marcus K, Hashimoto T, et al. The protease inhibitor alpha-2-macroglobulin-like-1 is the p170 antigen recognized by paraneoplastic pemphigus autoantibodies in human. PLoS ONE. (2010) 5:e12250. doi: 10.1371/journal.pone.0012250
26. Wieczorek M, Czernik A. Paraneoplastic pemphigus: a short review. Clin Cosmet Investig Dermatol. (2016) 9:291–5. doi: 10.2147/CCID.S100802
27. Gallo E, Garcia-Martin P, Fraga J, Teye K, Koga H, Hashimoto T, et al. Paraneoplastic pemphigus with eosinophilic spongiosis and autoantibodies against desmocollins 2 and 3. Clin Exp Dermatol. (2014) 39:323–6. doi: 10.1111/ced.12296
28. Oursler JR, Labib RS, riss-Abdo L, Burke T, O'Keefe EJ, Anhalt GJ. Human autoantibodies against desmoplakins in paraneoplastic pemphigus. J Clin Invest. (1992) 89:1775–82. doi: 10.1172/JCI115781
29. Amagai M, Nishikawa T, Nousari HC, Anhalt GJ, Hashimoto T. Antibodies against desmoglein 3 (pemphigus vulgaris antigen) are present in sera from patients with paraneoplastic pemphigus and cause acantholysis in vivo in neonatal mice. J Clin Invest. (1998) 102:775–82. doi: 10.1172/JCI3647
30. Kiyokawa C, Ruhrberg C, Nie Z, Karashima T, Mori O, Nishikawa T, et al. Envoplakin and periplakin are components of the paraneoplastic pemphigus antigen complex. J Invest Dermatol. (1998) 111:1236–8. doi: 10.1046/j.1523-1747.1998.00449.x
31. Aho S, Mahoney MG, Uitto J. Plectin serves as an autoantigen in paraneoplastic pemphigus. J Invest Dermatol. (1999) 113:422–3. doi: 10.1046/j.1523-1747.1999.00695.x
32. Brandt O, Rafei D, Podstawa E, Niedermeier A, Jonkman MF, Terra JB, et al. Differential IgG recognition of desmoglein 3 by paraneoplastic pemphigus and pemphigus vulgaris sera. J Invest Dermatol. (2012) 132:1738–41. doi: 10.1038/jid.2012.1
33. Ishii N, Teye K, Fukuda S, Uehara R, Hachiya T, Koga H, et al. Anti-desmocollin autoantibodies in nonclassical pemphigus. Br J Dermatol. (2015) 173:59–68. doi: 10.1111/bjd.13711
34. Zimmermann J, Bahmer F, Rose C, Zillikens D, Schmidt E. Clinical and immunopathological spectrum of paraneoplastic pemphigus. J Dtsch Dermatol Ges. (2010) 8:598–606. doi: 10.1111/j.1610-0387.2010.07380.x
35. Joly P, Richard C, Gilbert D, Courville P, Chosidow O, Roujeau JC, et al. Sensitivity and specificity of clinical, histologic, and immunologic features in the diagnosis of paraneoplastic pemphigus. J Am Acad Dermatol. (2000) 43:619–26. doi: 10.1067/mjd.2000.107488
36. Probst C, Schlumberger W, Stocker W, Recke A, Schmidt E, Hashimoto T, et al. Development of ELISA for the specific determination of autoantibodies against envoplakin and periplakin in paraneoplastic pemphigus. Clin Chim Acta. (2009) 410:13–8. doi: 10.1016/j.cca.2009.08.022
37. Powell JG, Grover RK, Plunkett RW, Seiffert-Sinha K, Sinha AA. Evaluation of a newly available ELISA for envoplakin autoantibodies for the diagnosis of paraneoplastic pemphigus. J Drugs Dermatol. (2015) 14:1103–6.
38. Poot AM, Diercks GF, Kramer D, Schepens I, Klunder G, Hashimoto T, et al. Laboratory diagnosis of paraneoplastic pemphigus. Br J Dermatol. (2013) 169:1016–24. doi: 10.1111/bjd.12479
39. Mergler R, Kerstan A, Schmidt E, Goebeler M, Benoit S. Atypical clinical and serological manifestation of pemphigus vegetans: a case report and review of the literature. Case Rep Dermatol. (2017) 9:121–30. doi: 10.1159/000468919
40. Perez-Perez ME, valos-Diaz E, Herrera-Esparza R. Autoantibodies in senear-usher syndrome: cross-reactivity or multiple autoimmunity? Autoimmune Dis. (2012) 2012:296214. doi: 10.1155/2012/296214
41. Amerian ML, Ahmed AR. Pemphigus erythematosus. Senear-Usher syndrome. Int J Dermatol. (1985) 24:16–25. doi: 10.1111/j.1365-4362.1985.tb05349.x
42. Kasperkiewicz M, Kowalewski C, Jablonska S. Pemphigus herpetiformis: from first description until now. J Am Acad Dermatol. (2014) 70:780–7. doi: 10.1016/j.jaad.2013.11.043
43. Aoki V, Rivitti EA, Diaz LA. Update on fogo selvagem, an endemic form of pemphigus foliaceus. J Dermatol. (2015) 42:18–26. doi: 10.1111/1346-8138.12675
44. Brenner S, Bialy-Golan A, Ruocco V. Drug-induced pemphigus. Clin Dermatol. (1998) 16:393–7. doi: 10.1016/S0738-081X(98)00010-8
45. Yoshimura K, Ishii N, Hamada T, Abe T, Ono F, Hashikawa K, et al. Clinical and immunological profiles in 17 Japanese patients with drug-induced pemphigus studied at Kurume University. Br J Dermatol. (2014) 171:544–53. doi: 10.1111/bjd.12925
46. Goletz S, Zillikens D, Schmidt E. Structural proteins of the dermal-epidermal junction targeted by autoantibodies in pemphigoid diseases. Exp Dermatol. (2017) 26:1154–62. doi: 10.1111/exd.13446
47. Kridin K, Ludwig RJ. The growing incidence of bullous pemphigoid: overview and potential explanations. Front Med. (2018) 5:220. doi: 10.3389/fmed.2018.00220
48. Zillikens D, Rose PA, Balding SD, Liu Z, Olague-Marchan M, Diaz LA, et al. Tight clustering of extracellular BP180 epitopes recognized by bullous pemphigoid autoantibodies. J Invest Dermatol. (1997) 109:573–9. doi: 10.1111/1523-1747.ep12337492
49. Skaria M, Jaunin F, Hunziker T, Riou S, Schumann H, Bruckner-Tuderman L, et al. IgG autoantibodies from bullous pemphigoid patients recognize multiple antigenic reactive sites located predominantly within the B and C subdomains of the COOH-terminus of BP230. J Invest Dermatol. (2000) 114:998–1004. doi: 10.1046/j.1523-1747.2000.00893.x
50. Yoshida M, Hamada T, Amagai M, Hashimoto K, Uehara R, Yamaguchi K, et al. Enzyme-linked immunosorbent assay using bacterial recombinant proteins of human BP230 as a diagnostic tool for bullous pemphigoid. J Dermatol Sci. (2006) 41:21–30. doi: 10.1016/j.jdermsci.2005.11.002
51. Charneux J, Lorin J, Vitry F, Antonicelli F, Reguiai Z, Barbe C, et al. Usefulness of BP230 and BP180-NC16a enzyme-linked immunosorbent assays in the initial diagnosis of bullous pemphigoid: a retrospective study of 138 patients. Arch Dermatol. (2011) 147:286–91. doi: 10.1001/archdermatol.2011.23
52. Di Zenzo G, Thoma-Uszynski S, Fontao L, Calabresi V, Hofmann SC, Hellmark T, et al. Multicenter prospective study of the humoral autoimmune response in bullous pemphigoid. Clin Immunol. (2008) 128:415–26. doi: 10.1016/j.clim.2008.04.012
53. Roussel A, Benichou J, Randriamanantany ZA, Gilbert D, Drenovska K, Houivet E, et al. Enzyme-linked immunosorbent assay for the combination of bullous pemphigoid antigens 1 and 2 in the diagnosis of bullous pemphigoid. Arch Dermatol. (2011) 147:293–8. doi: 10.1001/archdermatol.2011.21
54. Blocker IM, Dahnrich C, Probst C, Komorowski L, Saschenbrecker S, Schlumberger W, et al. Epitope mapping of BP230 leading to a novel enzyme-linked immunosorbent assay for autoantibodies in bullous pemphigoid. Br J Dermatol. (2012) 166:964–70. doi: 10.1111/j.1365-2133.2012.10820.x
55. Di Zenzo G, Grosso F, Terracina M, Mariotti F, De Pita O, Owaribe K, et al. Characterization of the anti-BP180 autoantibody reactivity profile and epitope mapping in bullous pemphigoid patients. J Invest Dermatol. (2004) 122:103–10. doi: 10.1046/j.0022-202X.2003.22126.x
56. Sitaru C, Powell J, Messer G, Brocker EB, Wojnarowska F, Zillikens D. Immunoblotting and enzyme-linked immunosorbent assay for the diagnosis of pemphigoid gestationis. Obstet Gynecol. (2004) 103:757–63. doi: 10.1097/01.AOG.0000115506.76104.ad
57. Di Zenzo G, Calabresi V, Grosso F, Caproni M, Ruffelli M, Zambruno G. The intracellular and extracellular domains of BP180 antigen comprise novel epitopes targeted by pemphigoid gestationis autoantibodies. J Invest Dermatol. (2007) 127:864–73. doi: 10.1038/sj.jid.5700594
58. Zone JJ, Taylor TB, Kadunce DP, Meyer LJ. Identification of the cutaneous basement membrane zone antigen and isolation of antibody in linear immunoglobulin A bullous dermatosis. J Clin Invest. (1990) 85:812–20. doi: 10.1172/JCI114508
59. Marinkovich MP, Taylor TB, Keene DR, Burgeson RE, Zone JJ. LAD-1, the linear IgA bullous dermatosis autoantigen, is a novel 120-kDa anchoring filament protein synthesized by epidermal cells. J Invest Dermatol. (1996) 106:734–8. doi: 10.1111/1523-1747.ep12345782
60. Fortuna G, Marinkovich MP. Linear immunoglobulin A bullous dermatosis. Clin Dermatol. (2012) 30:38–50. doi: 10.1016/j.clindermatol.2011.03.008
61. Hirako Y, Nishizawa Y, Sitaru C, Opitz A, Marcus K, Meyer HE, et al. The 97-kDa (LABD97) and 120-kDa (LAD-1) fragments of bullous pemphigoid antigen 180/type XVII collagen have different N-termini. J Invest Dermatol. (2003) 121:1554–6. doi: 10.1046/j.1523-1747.2003.12607.x
62. Zillikens D, Herzele K, Georgi M, Schmidt E, Chimanovitch I, Schumann H, et al. Autoantibodies in a subgroup of patients with linear IgA disease react with the NC16A domain of BP1801. J Invest Dermatol. (1999) 113:947–53. doi: 10.1046/j.1523-1747.1999.00808.x
63. Arechalde A, Braun RP, Calza AM, Hertl M, Didierjean L, Saurat JH, et al. Childhood bullous pemphigoid associated with IgA antibodies against BP180 or BP230 antigens. Br J Dermatol. (1999) 140:112–8. doi: 10.1046/j.1365-2133.1999.02618.x
64. Ghohestani RF, Nicolas JF, Kanitakis J, Claudy A. Linear IgA bullous dermatosis with IgA antibodies exclusively directed against the 180- or 230-kDa epidermal antigens. J Invest Dermatol. (1997) 108:854–8. doi: 10.1111/1523-1747.ep12292581
65. Kamaguchi M, Iwata H. The diagnosis and blistering mechanisms of mucous membrane pemphigoid. Front Immunol. (2019) 10:34. doi: 10.3389/fimmu.2019.00034
66. Balding SD, Prost C, Diaz LA, Bernard P, Bedane C, Aberdam D, et al. Cicatricial pemphigoid autoantibodies react with multiple sites on the BP180 extracellular domain. J Invest Dermatol. (1996) 106:141–6. doi: 10.1111/1523-1747.ep12329728
67. Bedane C, McMillan JR, Balding SD, Bernard P, Prost C, Bonnetblanc JM, et al. Bullous pemphigoid and cicatricial pemphigoid autoantibodies react with ultrastructurally separable epitopes on the BP180 ectodomain: evidence that BP180 spans the lamina lucida. J Invest Dermatol. (1997) 108:901–7. doi: 10.1111/1523-1747.ep12292701
68. Oyama N, Setterfield JF, Powell AM, Sakuma-Oyama Y, Albert S, Bhogal BS, et al. Bullous pemphigoid antigen II (BP180) and its soluble extracellular domains are major autoantigens in mucous membrane pemphigoid: the pathogenic relevance to HLA class II alleles and disease severity. Br J Dermatol. (2006) 154:90–8. doi: 10.1111/j.1365-2133.2005.06998.x
69. Schmidt E, Skrobek C, Kromminga A, Hashimoto T, Messer G, Brocker EB, et al. Cicatricial pemphigoid: IgA and IgG autoantibodies target epitopes on both intra- and extracellular domains of bullous pemphigoid antigen 180. Br J Dermatol. (2001) 145:778–83. doi: 10.1046/j.1365-2133.2001.04471.x
70. Lazarova Z, Salato VK, Lanschuetzer CM, Janson M, Fairley JA, Yancey KB. IgG anti-laminin-332 autoantibodies are present in a subset of patients with mucous membrane, but not bullous, pemphigoid. J Am Acad Dermatol. (2008) 58:951–8. doi: 10.1016/j.jaad.2008.02.035
71. Bekou V, Thoma-Uszynski S, Wendler O, Uter W, Schwietzke S, Hunziker T, et al. Detection of laminin 5-specific auto-antibodies in mucous membrane and bullous pemphigoid sera by ELISA. J Invest Dermatol. (2005) 124:732–40. doi: 10.1111/j.0022-202X.2005.23646.x
72. Goletz S, Probst C, Komorowski L, Schlumberger W, Fechner K, van BN, et al. A sensitive and specific assay for the serological diagnosis of antilaminin 332 mucous membrane pemphigoid. Br J Dermatol. (2019) 180:149–56. doi: 10.1111/bjd.17202
73. Egan CA, Lazarova Z, Darling TN, Yee C, Cote T, Yancey KB. Anti-epiligrin cicatricial pemphigoid and relative risk for cancer. Lancet. (2001) 357:1850–1. doi: 10.1016/S0140-6736(00)04971-0
74. Bernard P, Prost C, Lecerf V, Intrator L, Combemale P, Bedane C, et al. Studies of cicatricial pemphigoid autoantibodies using direct immunoelectron microscopy and immunoblot analysis. J Invest Dermatol. (1990) 94:630–5. doi: 10.1111/1523-1747.ep12876206
75. Leverkus M, Bhol K, Hirako Y, Pas H, Sitaru C, Baier G, et al. Cicatricial pemphigoid with circulating autoantibodies to beta4 integrin, bullous pemphigoid 180 and bullous pemphigoid 230. Br J Dermatol. (2001) 145:998–1004. doi: 10.1046/j.1365-2133.2001.04543.x
76. Bhol KC, Dans MJ, Simmons RK, Foster CS, Giancotti FG, Ahmed AR. The autoantibodies to alpha 6 beta 4 integrin of patients affected by ocular cicatricial pemphigoid recognize predominantly epitopes within the large cytoplasmic domain of human beta 4. J Immunol. (2000) 165:2824–9. doi: 10.4049/jimmunol.165.5.2824
77. Li X, Qian H, Sogame R, Hirako Y, Tsuruta D, Ishii N, et al. Integrin beta4 is a major target antigen in pure ocular mucous membrane pemphigoid. Eur J Dermatol. (2016) 26:247–53. doi: 10.1684/ejd.2016.2772
78. Amber KT, Murrell DF, Schmidt E, Joly P, Borradori L. Autoimmune subepidermal bullous diseases of the skin and mucosae: clinical features, diagnosis, and management. Clin Rev Allergy Immunol. (2018) 54:26–51. doi: 10.1007/s12016-017-8633-4
79. Dilling A, Rose C, Hashimoto T, Zillikens D, Shimanovich I. Anti-p200 pemphigoid: a novel autoimmune subepidermal blistering disease. J Dermatol. (2007) 34:1–8. doi: 10.1111/j.1346-8138.2007.00208.x
80. Zillikens D, Kawahara Y, Ishiko A, Shimizu H, Mayer J, Rank CV, et al. A novel subepidermal blistering disease with autoantibodies to a 200-kDa antigen of the basement membrane zone. J Invest Dermatol. (1996) 106:1333–8. doi: 10.1111/1523-1747.ep12349283
81. Dainichi T, Koga H, Tsuji T, Ishii N, Ohyama B, Ueda A, et al. From anti-p200 pemphigoid to anti-laminin gamma1 pemphigoid. J Dermatol. (2010) 37:231–8. doi: 10.1111/j.1346-8138.2009.00793.x
82. Hubner F, Langan EA, Recke A. Lichen planus pemphigoides: from lichenoid inflammation to autoantibody-mediated blistering. Front Immunol. (2019) 10:1389. doi: 10.3389/fimmu.2019.01389
83. Tamada Y, Yokochi K, Nitta Y, Ikeya T, Hara K, Owaribe K. Lichen planus pemphigoides: identification of 180 kd hemidesmosome antigen. J Am Acad Dermatol. (1995) 32:883–7. doi: 10.1016/0190-9622(95)91554-0
84. Zillikens D, Caux F, Mascaro JM, Wesselmann U, Schmidt E, Prost C, et al. Autoantibodies in lichen planus pemphigoides react with a novel epitope within the C-terminal NC16A domain of BP180. J Invest Dermatol. (1999) 113:117–21. doi: 10.1046/j.1523-1747.1999.00618.x
85. Mehren CR, Gniadecki R. Epidermolysis bullosa acquisita: current diagnosis and therapy. Dermatol Rep. (2011) 3:e38. doi: 10.4081/dr.2011.e38
86. Koga H, Prost-Squarcioni C, Iwata H, Jonkman MF, Ludwig RJ, Bieber K. Epidermolysis bullosa acquisita: the 2019 update. Front Med. (2018) 5:362. doi: 10.3389/fmed.2018.00362
87. Ishii N, Hamada T, Dainichi T, Karashima T, Nakama T, Yasumoto S, et al. Epidermolysis bullosa acquisita: what's new? J Dermatol. (2010) 37:220–30. doi: 10.1111/j.1346-8138.2009.00799.x
88. Woodley DT, Briggaman RA, O'Keefe EJ, Inman AO, Queen LL, Gammon WR. Identification of the skin basement-membrane autoantigen in epidermolysis bullosa acquisita. N Engl J Med. (1984) 310:1007–13. doi: 10.1056/NEJM198404193101602
89. Jones DA, Hunt SW III, Prisayanh PS, Briggaman RA, Gammon WR. Immunodominant autoepitopes of type VII collagen are short, paired peptide sequences within the fibronectin type III homology region of the noncollagenous (NC1) domain. J Invest Dermatol. (1995) 104:231–5. doi: 10.1111/1523-1747.ep12612780
90. Lapiere JC, Woodley DT, Parente MG, Iwasaki T, Wynn KC, Christiano AM, et al. Epitope mapping of type VII collagen. Identification of discrete peptide sequences recognized by sera from patients with acquired epidermolysis bullosa. J Clin Invest. (1993) 92:1831–9. doi: 10.1172/JCI116774
91. Chorzelski TP, Beutner EH, Sulej J, Tchorzewska H, Jablonska S, Kumar V, et al. IgA anti-endomysium antibody. A new immunological marker of dermatitis herpetiformis and coeliac disease. Br J Dermatol. (1984) 111:395–402. doi: 10.1111/j.1365-2133.1984.tb06601.x
92. Kasperkiewicz M, Dahnrich C, Probst C, Komorowski L, Stocker W, Schlumberger W, et al. Novel assay for detecting celiac disease-associated autoantibodies in dermatitis herpetiformis using deamidated gliadin-analogous fusion peptides. J Am Acad Dermatol. (2012) 66:583–8. doi: 10.1016/j.jaad.2011.02.025
93. Dieterich W, Ehnis T, Bauer M, Donner P, Volta U, Riecken EO, et al. Identification of tissue transglutaminase as the autoantigen of celiac disease. Nat Med. (1997) 3:797–801. doi: 10.1038/nm0797-797
94. Rose C, Armbruster FP, Ruppert J, Igl BW, Zillikens D, Shimanovich I. Autoantibodies against epidermal transglutaminase are a sensitive diagnostic marker in patients with dermatitis herpetiformis on a normal or gluten-free diet. J Am Acad Dermatol. (2009) 61:39–43. doi: 10.1016/j.jaad.2008.12.037
95. Sardy M, Karpati S, Merkl B, Paulsson M, Smyth N. Epidermal transglutaminase (TGase 3) is the autoantigen of dermatitis herpetiformis. J Exp Med. (2002) 195:747–57. doi: 10.1084/jem.20011299
96. Villalta D, Tonutti E, Prause C, Koletzko S, Uhlig HH, Vermeersch P, et al. IgG antibodies against deamidated gliadin peptides for diagnosis of celiac disease in patients with IgA deficiency. Clin Chem. (2010) 56:464–8. doi: 10.1373/clinchem.2009.128132
97. Schmidt E, Goebeler M, Hertl M, Sardy M, Sitaru C, Eming R, et al. S2k guideline for the diagnosis of pemphigus vulgaris/foliaceus and bullous pemphigoid. J Dtsch Dermatol Ges. (2015) 13:713–27. doi: 10.1111/ddg.12612
98. Kneisel A, Hertl M. Autoimmune bullous skin diseases. Part 2: diagnosis and therapy. J Dtsch Dermatol Ges. (2011) 9:927–47. doi: 10.1111/j.1610-0387.2011.07809.x
99. Schmidt E, Zillikens D. Modern diagnosis of autoimmune blistering skin diseases. Autoimmun Rev. (2010) 10:84–9. doi: 10.1016/j.autrev.2010.08.007
100. van Beek N, Zillikens D, Schmidt E. Diagnosis of autoimmune bullous diseases. J Dtsch Dermatol Ges. (2018) 16:1077–91. doi: 10.1111/ddg.13637
101. Prost-Squarcioni C, Caux F, Schmidt E, Jonkman MF, Vassileva S, Kim SC, et al. International Bullous Diseases Group: consensus on diagnostic criteria for epidermolysis bullosa acquisita. Br J Dermatol. (2018) 179:30–41. doi: 10.1111/bjd.16138
102. Murrell DF, Peña S, Joly P, Marinovic B, Hashimoto T, Diaz LA, et al. Diagnosis and Management of Pemphigus: recommendations by an International Panel of Experts. J Am Acad Dermatol. (2018). doi: 10.1016/j.jaad.2018.02.021. [Epub ahead of print].
103. Witte M, Zillikens D, Schmidt E. Diagnosis of Autoimmune Blistering Diseases. Front Med. (2018) 5:296. doi: 10.3389/fmed.2018.00296
104. Hashimoto T, Tsuruta D, Koga H, Fukuda S, Ohyama B, Komai A, et al. Summary of results of serological tests and diagnoses for 4774 cases of various autoimmune bullous diseases consulted to Kurume University. Br J Dermatol. (2016) 175:953–65. doi: 10.1111/bjd.14692
105. Kneisel A, Hertl M. Autoimmune bullous skin diseases. Part 1: clinical manifestations. J Dtsch Dermatol Ges. (2011) 9:844–56. doi: 10.1111/j.1610-0387.2011.07793.x
106. Sardy M, Kostaki D, Varga R, Peris K, Ruzicka T. Comparative study of direct and indirect immunofluorescence and of bullous pemphigoid 180 and 230 enzyme-linked immunosorbent assays for diagnosis of bullous pemphigoid. J Am Acad Dermatol. (2013) 69:748–53. doi: 10.1016/j.jaad.2013.07.009
107. Inchara YK, Rajalakshmi T. Direct immunofluorescence in cutaneous vesiculobullous lesions. Indian J Pathol Microbiol. (2007) 50:730–2.
108. Chan YC, Sun YJ, Ng PP, Tan SH. Comparison of immunofluorescence microscopy, immunoblotting and enzyme-linked immunosorbent assay methods in the laboratory diagnosis of bullous pemphigoid. Clin Exp Dermatol. (2003) 28:651–6. doi: 10.1046/j.1365-2230.2003.01419.x
109. Giurdanella F, Diercks GF, Jonkman MF, Pas HH. Laboratory diagnosis of pemphigus: direct immunofluorescence remains the gold standard. Br J Dermatol. (2016) 175:185–6. doi: 10.1111/bjd.14408
110. Kamaguchi M, Iwata H, Ujiie I, Ujiie H, Sato J, Kitagawa Y, et al. Direct immunofluorescence using non-lesional buccal mucosa in mucous membrane pemphigoid. Front Med. (2018) 5:20. doi: 10.3389/fmed.2018.00020
111. Meijer JM, Atefi I, Diercks GFH, Vorobyev A, Zuiderveen J, Meijer HJ, et al. Serration pattern analysis for differentiating epidermolysis bullosa acquisita from other pemphigoid diseases. J Am Acad Dermatol. (2018) 78:754–9. doi: 10.1016/j.jaad.2017.11.029
112. Schmidt E, Zillikens D. The diagnosis and treatment of autoimmune blistering skin diseases. Dtsch Arztebl Int. (2011) 108:399–III. doi: 10.3238/arztebl.2011.0399
113. van Beek N, Rentzsch K, Probst C, Komorowski L, Kasperkiewicz M, Fechner K, et al. Serological diagnosis of autoimmune bullous skin diseases: prospective comparison of the BIOCHIP mosaic-based indirect immunofluorescence technique with the conventional multi-step single test strategy. Orphanet J Rare Dis. (2012) 7:49. doi: 10.1186/1750-1172-7-49
114. van Beek N, Dahnrich C, Johannsen N, Lemcke S, Goletz S, Hubner F, et al. Prospective studies on the routine use of a novel multivariant enzyme-linked immunosorbent assay for the diagnosis of autoimmune bullous diseases. J Am Acad Dermatol. (2017) 76:889–94. doi: 10.1016/j.jaad.2016.11.002
115. Giurdanella F, Nijenhuis AM, Diercks GFH, Jonkman MF, Pas HH. Keratinocyte binding assay identifies anti-desmosomal pemphigus antibodies where other tests are negative. Front Immunol. (2018) 9:839. doi: 10.3389/fimmu.2018.00839
116. Harman KE, Brown D, Exton LS, Groves RW, Hampton PJ, Mohd Mustapa MF, et al. British Association of Dermatologists' guidelines for the management of pemphigus vulgaris 2017. Br J Dermatol. (2017) 177:1170–201. doi: 10.1111/bjd.15930
117. Kasperkiewicz M, Schmidt E, Zillikens D. Current therapy of the pemphigus group. Clin Dermatol. (2012) 30:84–94. doi: 10.1016/j.clindermatol.2011.03.014
118. Martin LK, Werth VP, Villaneuva EV, Murrell DF. A systematic review of randomized controlled trials for pemphigus vulgaris and pemphigus foliaceus. J Am Acad Dermatol. (2011) 64:903–8. doi: 10.1016/j.jaad.2010.04.039
119. Joly P, Roujeau JC, Benichou J, Delaporte E, D'Incan M, Dreno B, et al. A comparison of two regimens of topical corticosteroids in the treatment of patients with bullous pemphigoid: a multicenter randomized study. J Invest Dermatol. (2009) 129:1681–7. doi: 10.1038/jid.2008.412
120. Behzad M, Mobs C, Kneisel A, Moller M, Hoyer J, Hertl M, et al. Combined treatment with immunoadsorption and rituximab leads to fast and prolonged clinical remission in difficult-to-treat pemphigus vulgaris. Br J Dermatol. (2012) 166:844–52. doi: 10.1111/j.1365-2133.2011.10732.x
121. Eming R, Hertl M. Immunoadsorption in pemphigus. Autoimmunity. (2006) 39:609–16. doi: 10.1080/08916930600972040
122. Arin MJ, Engert A, Krieg T, Hunzelmann N. Anti-CD20 monoclonal antibody (rituximab) in the treatment of pemphigus. Br J Dermatol. (2005) 153:620–5. doi: 10.1111/j.1365-2133.2005.06651.x
123. Hertl M, Zillikens D, Borradori L, Bruckner-Tuderman L, Burckhard H, Eming R, et al. Recommendations for the use of rituximab (anti-CD20 antibody) in the treatment of autoimmune bullous skin diseases. J Dtsch Dermatol Ges. (2008) 6:366–73. doi: 10.1111/j.1610-0387.2007.06602.x
124. Amagai M, Hashimoto T, Shimizu N, Nishikawa T. Absorption of pathogenic autoantibodies by the extracellular domain of pemphigus vulgaris antigen (Dsg3) produced by baculovirus. J Clin Invest. (1994) 94:59–67. doi: 10.1172/JCI117349
125. Anhalt GJ, Kim SC, Stanley JR, Korman NJ, Jabs DA, Kory M, et al. Paraneoplastic pemphigus. An autoimmune mucocutaneous disease associated with neoplasia. N Engl J Med. (1990) 323:1729–35. doi: 10.1056/NEJM199012203232503
126. Harman KE, Gratian MJ, Bhogal BS, Challacombe SJ, Black MM. The use of two substrates to improve the sensitivity of indirect immunofluorescence in the diagnosis of pemphigus. Br J Dermatol. (2000) 142:1135–9. doi: 10.1046/j.1365-2133.2000.03538.x
127. Jiao D, Bystryn JC. Sensitivity of indirect immunofluorescence, substrate specificity, and immunoblotting in the diagnosis of pemphigus. J Am Acad Dermatol. (1997) 37:211–6. doi: 10.1016/S0190-9622(97)80127-2
128. Hahn K, Kippes W, Amagai M, Rzany B, Brocker EB, Zillikens D. [Clinical aspects and immunopathology in 48 patients with pemphigus]. Hautarzt. (2000) 51:670–7. doi: 10.1007/s001050051193
129. Zagorodniuk I, Weltfriend S, Shtruminger L, Sprecher E, Kogan O, Pollack S, et al. A comparison of anti-desmoglein antibodies and indirect immunofluorescence in the serodiagnosis of pemphigus vulgaris. Int J Dermatol. (2005) 44:541–4. doi: 10.1111/j.1365-4632.2004.02541.x
130. Ng PP, Thng ST, Mohamed K, Tan SH. Comparison of desmoglein ELISA and indirect immunofluorescence using two substrates (monkey oesophagus and normal human skin) in the diagnosis of pemphigus. Australas J Dermatol. (2005) 46:239–41. doi: 10.1111/j.1440-0960.2005.00191.x
131. Sabolinski ML, Beutner EH, Krasny S, Kumar V, Huang J, Chorzelski TP, et al. Substrate specificity of anti-epithelial antibodies of pemphigus vulgaris and pemphigus foliaceus sera in immunofluorescence tests on monkey and guinea pig esophagus sections. J Invest Dermatol. (1987) 88:545–9. doi: 10.1111/1523-1747.ep12470131
132. Kridin K, Bergman R. The usefulness of indirect immunofluorescence in pemphigus and the natural history of patients with initial false-positive results: a Retrospective Cohort Study. Front Med. (2018) 5:266. doi: 10.3389/fmed.2018.00266
133. Kippes W, Schmidt E, Roth A, Rzany B, Brocker EB, Zillikens D. [Immunopathologic changes in 115 patients with bullous pemphigoid]. Hautarzt. (1999) 50:866–72. doi: 10.1007/s001050051001
134. Lee FJ, Silvestrini R, Fulcher DA. False-positive intercellular cement substance antibodies due to group A/B red cell antibodies: frequency and approach. Pathology. (2010) 42:574–7. doi: 10.3109/00313025.2010.508792
135. Ghohestani RF, Nicolas JF, Rousselle P, Claudy AL. Diagnostic value of indirect immunofluorescence on sodium chloride-split skin in differential diagnosis of subepidermal autoimmune bullous dermatoses. Arch Dermatol. (1997) 133:1102–7. doi: 10.1001/archderm.133.9.1102
136. Gammon WR, Fine JD, Forbes M, Briggaman RA. Immunofluorescence on split skin for the detection and differentiation of basement membrane zone autoantibodies. J Am Acad Dermatol. (1992) 27:79–87. doi: 10.1016/0190-9622(92)70161-8
137. Ghohestani R, Kanitakis J, Nicolas JF, Cozzani E, Claudy A. Comparative sensitivity of indirect immunofluorescence to immunoblot assay for the detection of circulating antibodies to bullous pemphigoid antigens 1 and 2. Br J Dermatol. (1996) 135:74–9. doi: 10.1111/j.1365-2133.1996.tb03611.x
138. Lau I, Goletz S, Holtsche MM, Zillikens D, Fechner K, Schmidt E. Anti-p200 pemphigoid is the most common pemphigoid disease with serum antibodies against the dermal side by indirect immunofluorescence microscopy on human salt-split skin. J Am Acad Dermatol. (2019). doi: 10.1016/j.jaad.2019.03.077. [Epub ahead of print].
139. Liu AY, Valenzuela R, Helm TN, Camisa C, Melton AL, Bergfeld WF. Indirect immunofluorescence on rat bladder transitional epithelium: a test with high specificity for paraneoplastic pemphigus. J Am Acad Dermatol. (1993) 28:696–9. doi: 10.1016/0190-9622(93)70095-B
140. Vainio E, Kalimo K, Reunala T, Viander M, Palosuo T. Circulating IgA- and IgG-class antigliadin antibodies in dermatitis herpetiformis detected by enzyme-linked immunosorbent assay. Arch Dermatol Res. (1983) 275:15–8. doi: 10.1007/BF00516548
141. Wandinger KP, Probst C, Komorowski L, Saschenbrecker S, Rosemann A, Mothes T, et al. Novel recombinant antigenic targets for the determination of (auto)antibodies in autoimmune dermatoses, neurological disorders and gastrointestinal diseases. In: Conrad K, Chan EKL, Fritzler MJ, Humbel RL, von Landenberg P, Shoenfeld Y, editors. From Pathogenesis to Therapy of Autoimmune Diseases. Lengerich: Pabst Science Publishers (2009). p 179–90.
142. Schwertz E, Kahlenberg F, Sack U, Richter T, Stern M, Conrad K, et al. Serologic assay based on gliadin-related nonapeptides as a highly sensitive and specific diagnostic aid in celiac disease. Clin Chem. (2004) 50:2370–5. doi: 10.1373/clinchem.2004.036111
143. Sitaru C, Dahnrich C, Probst C, Komorowski L, Blocker I, Schmidt E, et al. Enzyme-linked immunosorbent assay using multimers of the 16th non-collagenous domain of the BP180 antigen for sensitive and specific detection of pemphigoid autoantibodies. Exp Dermatol. (2007) 16:770–7. doi: 10.1111/j.1600-0625.2007.00592.x
144. Damoiseaux J, van Rijsingen M, Warnemunde N, Dahnrich C, Fechner K, Tervaert JW. Autoantibody detection in bullous pemphigoid: clinical evaluation of the EUROPLUS Dermatology Mosaic. J Immunol Methods. (2012) 382:76–80. doi: 10.1016/j.jim.2012.05.007
145. Prause C, Ritter M, Probst C, Daehnrich C, Schlumberger W, Komorowski L, et al. Antibodies against deamidated gliadin as new and accurate biomarkers of childhood coeliac disease. J Pediatr Gastroenterol Nutr. (2009) 49:52–8. doi: 10.1097/MPG.0b013e318195dae3
146. Stöcker W. [Rational histochemistry using a new microanalytic technic]. Acta Histochem Suppl. (1985) 31:269–81.
147. Schmidt E, Dahnrich C, Rosemann A, Probst C, Komorowski L, Saschenbrecker S, et al. Novel ELISA systems for antibodies to desmoglein 1 and 3: correlation of disease activity with serum autoantibody levels in individual pemphigus patients. Exp Dermatol. (2010) 19:458–63. doi: 10.1111/j.1600-0625.2010.01069.x
148. Gosink J. Autoantibody diagnostics in skin-blistering diseases. MEDLAB Magazine. (2013) 4:16–8.
149. Komorowski L, Muller R, Vorobyev A, Probst C, Recke A, Jonkman MF, et al. Sensitive and specific assays for routine serological diagnosis of epidermolysis bullosa acquisita. J Am Acad Dermatol. (2013) 68:e89–95. doi: 10.1016/j.jaad.2011.12.032
150. Xuan RR, Yang A, Murrell DF. New biochip immunofluorescence test for the serological diagnosis of pemphigus vulgaris and foliaceus: a review of the literature. Int J Womens Dermatol. (2018) 4:102–8. doi: 10.1016/j.ijwd.2017.10.001
151. Yang A, Xuan R, Murrell DF. A new indirect immunofluorescence BIOCHIP method for the serological diagnosis of bullous pemphigoid: a review of literature. Australas J Dermatol. (2019) 60:e173–7. doi: 10.1111/ajd.13034
152. Özkesici B, Mutlu D, Donmez L, Uzun S. The value of the BIOCHIP mosaic-based indirect immunofluorescence technique in the diagnosis of pemphigus and bullous pemphigoid in Turkish patients. Acta Dermatovenerol Croat. (2017) 25:202–9.
153. Russo I, Saponeri A, Peserico A, Alaibac M. The use of biochip immunofluorescence microscopy for the diagnosis of Pemphigus vulgaris. Acta Histochem. (2014) 116:713–6. doi: 10.1016/j.acthis.2013.12.012
154. Tampoia M, Zucano A, Villalta D, Antico A, Bizzaro N. Anti-skin specific autoantibodies detected by a new immunofluorescence multiplex biochip method in patients with autoimmune bullous diseases. Dermatology. (2012) 225:37–44. doi: 10.1159/000339776
155. Zarian H, Saponeri A, Michelotto A, Zattra E, Belloni-Fortina A, Alaibac M. Biochip technology for the serological diagnosis of bullous pemphigoid. ISRN Dermatol. (2012) 2012:237802. doi: 10.5402/2012/237802
156. Schmidt E, Zillikens D. Diagnosis and treatment of patients with autoimmune bullous disorders in Germany. Dermatol Clin. (2011) 29:663–71. doi: 10.1016/j.det.2011.06.007
157. Sadik CD, Pas HH, Bohlmann MK, Mousavi S, Benoit S, Sardy M, et al. Value of BIOCHIP technology in the serological diagnosis of pemphigoid gestationis. Acta Derm Venereol. (2017) 97:128–30. doi: 10.2340/00015555-2460
158. Mindorf S, Dettmann IM, Kruger S, Fuhrmann T, Rentzsch K, Karl I, et al. Routine detection of serum antidesmocollin autoantibodies is only useful in patients with atypical pemphigus. Exp Dermatol. (2017) 26:1267–70. doi: 10.1111/exd.13409
159. Ishii K, Amagai M, Hall RP, Hashimoto T, Takayanagi A, Gamou S, et al. Characterization of autoantibodies in pemphigus using antigen-specific enzyme-linked immunosorbent assays with baculovirus-expressed recombinant desmogleins. J Immunol. (1997) 159:2010–7.
160. Kobayashi M, Amagai M, Kuroda-Kinoshita K, Hashimoto T, Shirakata Y, Hashimoto K, et al. BP180 ELISA using bacterial recombinant NC16a protein as a diagnostic and monitoring tool for bullous pemphigoid. J Dermatol Sci. (2002) 30:224–32. doi: 10.1016/S0923-1811(02)00109-3
161. Marzano AV, Cozzani E, Fanoni D, De PO, Vassallo C, Berti E, et al. Diagnosis and disease severity assessment of epidermolysis bullosa acquisita by ELISA for anti-type VII collagen autoantibodies: an Italian multicentre study. Br J Dermatol. (2013) 168:80–4. doi: 10.1111/bjd.12011
162. Groth S, Recke A, Vafia K, Ludwig RJ, Hashimoto T, Zillikens D, et al. Development of a simple enzyme-linked immunosorbent assay for the detection of autoantibodies in anti-p200 pemphigoid. Br J Dermatol. (2011) 164:76–82. doi: 10.1111/j.1365-2133.2010.10056.x
163. Bernard P, Antonicelli F, Bedane C, Joly P, Le Roux-Villet C, Duvert-Lehembre S, et al. Prevalence and clinical significance of anti-laminin 332 autoantibodies detected by a novel enzyme-linked immunosorbent assay in mucous membrane pemphigoid. JAMA Dermatol. (2013) 149:533–40. doi: 10.1001/jamadermatol.2013.1434
164. Hofmann S, Thoma-Uszynski S, Hunziker T, Bernard P, Koebnick C, Stauber A, et al. Severity and phenotype of bullous pemphigoid relate to autoantibody profile against the NH2- and COOH-terminal regions of the BP180 ectodomain. J Invest Dermatol. (2002) 119:1065–73. doi: 10.1046/j.1523-1747.2002.19529.x
165. Horvath ON, Varga R, Kaneda M, Schmidt E, Ruzicka T, Sardy M. Diagnostic performance of the “MESACUP anti-Skin profile TEST”. Eur J Dermatol. (2016) 26:56–63. doi: 10.1684/ejd.2015.2692
166. Amagai M, Komai A, Hashimoto T, Shirakata Y, Hashimoto K, Yamada T, et al. Usefulness of enzyme-linked immunosorbent assay using recombinant desmogleins 1 and 3 for serodiagnosis of pemphigus. Br J Dermatol. (1999) 140:351–7. doi: 10.1046/j.1365-2133.1999.02752.x
167. Harman KE, Gratian MJ, Seed PT, Bhogal BS, Challacombe SJ, Black MM. Diagnosis of pemphigus by ELISA: a critical evaluation of two ELISAs for the detection of antibodies to the major pemphigus antigens, desmoglein 1 and 3. Clin Exp Dermatol. (2000) 25:236–40. doi: 10.1046/j.1365-2230.2000.00624.x
168. Huang CH, Chen CC, Wang CJ, Chang YT, Liu HN. Using desmoglein 1 and 3 enzyme-linked immunosorbent assay as an adjunct diagnostic tool for pemphigus. J Chin Med Assoc. (2007) 70:65–70. doi: 10.1016/S1726-4901(09)70304-1
169. D'Agosto G, Latini A, Carducci M, Mastroianni A, Vento A, Fei PC. Evaluation of recombinant antigen-based assays for diagnosis of bullous autoimmune diseases. Clin Diagn Lab Immunol. (2004) 11:762–5. doi: 10.1128/CDLI.11.4.762-765.2004
170. Daneshpazhooh M, Chams-Davatchi C, Khamesipour A, Mansoori P, Taheri A, Firooz A, et al. Desmoglein 1 and 3 enzyme-linked immunosorbent assay in Iranian patients with pemphigus vulgaris: correlation with phenotype, severity, and disease activity. J Eur Acad Dermatol Venereol. (2007) 21:1319–24. doi: 10.1111/j.1468-3083.2007.02254.x
171. Hallaji Z, Mortazavi H, Lajevardi V, Tamizifar B, AmirZargar A, Daneshpazhooh M, et al. Serum and salivary desmoglein 1 and 3 enzyme-linked immunosorbent assay in pemphigus vulgaris: correlation with phenotype and severity. J Eur Acad Dermatol Venereol. (2010) 24:275–80. doi: 10.1111/j.1468-3083.2009.03408.x
172. Sharma VK, Prasad HR, Khandpur S, Kumar A. Evaluation of desmoglein enzyme-linked immunosorbent assay (ELISA) in Indian patients with pemphigus vulgaris. Int J Dermatol. (2006) 45:518–22. doi: 10.1111/j.1365-4632.2006.02593.x
173. Atzori L, Deidda S, Aste N. Enzyme-linked immunosorbent assay in autoimmune blistering diseases: preliminary experience of the Dermatology Department of Cagliari. G Ital Dermatol Venereol. (2008) 143:1–8.
174. Zillikens D, Mascaro JM, Rose PA, Liu Z, Ewing SM, Caux F, et al. A highly sensitive enzyme-linked immunosorbent assay for the detection of circulating anti-BP180 autoantibodies in patients with bullous pemphigoid. J Invest Dermatol. (1997) 109:679–83. doi: 10.1111/1523-1747.ep12338088
175. Keller JJ, Kittridge AL, Debanne SM, Korman NJ. Evaluation of ELISA testing for BP180 and BP230 as a diagnostic modality for bullous pemphigoid: a clinical experience. Arch Dermatol Res. (2016) 308:269–72. doi: 10.1007/s00403-016-1631-1
176. Tampoia M, Lattanzi V, Zucano A, Villalta D, Filotico R, Fontana A, et al. Evaluation of a new ELISA assay for detection of BP230 autoantibodies in bullous pemphigoid. Ann N Y Acad Sci. (2009) 1173:15–20. doi: 10.1111/j.1749-6632.2009.04630.x
177. Thoma-Uszynski S, Uter W, Schwietzke S, Hofmann SC, Hunziker T, Bernard P, et al. BP230- and BP180-specific auto-antibodies in bullous pemphigoid. J Invest Dermatol. (2004) 122:1413–22. doi: 10.1111/j.0022-202X.2004.22603.x
178. Sakuma-Oyama Y, Powell AM, Oyama N, Albert S, Bhogal BS, Black MM. Evaluation of a BP180-NC16a enzyme-linked immunosorbent assay in the initial diagnosis of bullous pemphigoid. Br J Dermatol. (2004) 151:126–31. doi: 10.1111/j.1365-2133.2004.06082.x
179. Mariotti F, Grosso F, Terracina M, Ruffelli M, Cordiali-Fei P, Sera F, et al. Development of a novel ELISA system for detection of anti-BP180 IgG and characterization of autoantibody profile in bullous pemphigoid patients. Br J Dermatol. (2004) 151:1004–10. doi: 10.1111/j.1365-2133.2004.06245.x
180. Barnadas MA, Rubiales MV, Gonzalez MJ, Puig L, Garcia P, Baselga E, et al. Enzyme-linked immunosorbent assay (ELISA) and indirect immunofluorescence testing in a bullous pemphigoid and pemphigoid gestationis. Int J Dermatol. (2008) 47:1245–9. doi: 10.1111/j.1365-4632.2008.03824.x
181. Messingham KA, Noe MH, Chapman MA, Giudice GJ, Fairley JA. A novel ELISA reveals high frequencies of BP180-specific IgE production in bullous pemphigoid. J Immunol Methods. (2009) 346:18–25. doi: 10.1016/j.jim.2009.04.013
182. Kromminga A, Sitaru C, Hagel C, Herzog S, Zillikens D. Development of an ELISA for the detection of autoantibodies to BP230. Clin Immunol. (2004) 111:146–52. doi: 10.1016/j.clim.2003.12.007
183. Schmidt T, Hoch M, Lotfi Jad SS, Solimani F, Di ZG, Marzano AV, et al. Serological diagnostics in the detection of IgG autoantibodies against human collagen VII in epidermolysis bullosa acquisita: a multicentre analysis. Br J Dermatol. (2017) 177:1683–92. doi: 10.1111/bjd.15800
184. Saleh MA, Ishii K, Kim YJ, Murakami A, Ishii N, Hashimoto T, et al. Development of NC1 and NC2 domains of type VII collagen ELISA for the diagnosis and analysis of the time course of epidermolysis bullosa acquisita patients. J Dermatol Sci. (2011) 62:169–75. doi: 10.1016/j.jdermsci.2011.03.003
185. Kim JH, Kim YH, Kim S, Noh EB, Kim SE, Vorobyev A, et al. Serum levels of anti-type VII collagen antibodies detected by enzyme-linked immunosorbent assay in patients with epidermolysis bullosa acquisita are correlated with the severity of skin lesions. J Eur Acad Dermatol Venereol. (2013) 27:e224–30. doi: 10.1111/j.1468-3083.2012.04617.x
186. Chen M, Chan LS, Cai X, O'Toole EA, Sample JC, Woodley DT. Development of an ELISA for rapid detection of anti-type VII collagen autoantibodies in epidermolysis bullosa acquisita. J Invest Dermatol. (1997) 108:68–72. doi: 10.1111/1523-1747.ep12285634
187. Sardy M, Odenthal U, Karpati S, Paulsson M, Smyth N. Recombinant human tissue transglutaminase ELISA for the diagnosis of gluten-sensitive enteropathy. Clin Chem. (1999) 45:2142–9.
188. Sardy M, Karpati S, Peterfy F, Rasky K, Tomsits E, Zagoni T, et al. Comparison of a tissue transglutaminase ELISA with the endomysium antibody test in the diagnosis of gluten-sensitive enteropathy. Z Gastroenterol. (2000) 38:357–64. doi: 10.1055/s-2000-14883
189. Mankai A, Sakly W, Landolsi H, Gueddah L, Sriha B, Ayadi A, et al. Tissue transglutaminase antibodies in celiac disease, comparison of an enzyme linked immunosorbent assay and a dot blot assay. Pathol Biol. (2005) 53:204–9. doi: 10.1016/j.patbio.2004.07.022
190. Tampoia M, Giavarina D, Di GC, Bizzaro N. Diagnostic accuracy of enzyme-linked immunosorbent assays (ELISA) to detect anti-skin autoantibodies in autoimmune blistering skin diseases: a systematic review and meta-analysis. Autoimmun Rev. (2012) 12:121–6. doi: 10.1016/j.autrev.2012.07.006
191. Hisamatsu Y, Nishiyama T, Amano S, Matsui C, Ghohestani R, Hashimoto T. Usefulness of immunoblotting using purified laminin 5 in the diagnosis of anti-laminin 5 cicatricial pemphigoid. J Dermatol Sci. (2003) 33:113–9. doi: 10.1016/S0923-1811(03)00158-0
192. Mignogna M, Lanza A, Rossiello L, Ruocco V, Ahmed AR. Comparison of reactivity and epitope recognition between sera from American and Italian patients with oral pemphigoid. Clin Exp Immunol. (2006) 145:28–35. doi: 10.1111/j.1365-2249.2006.03103.x
193. Ishii N, Yoshida M, Hisamatsu Y, Ishida-Yamamoto A, Nakane H, Iizuka H, et al. Epidermolysis bullosa acquisita sera react with distinct epitopes on the NC1 and NC2 domains of type VII collagen: study using immunoblotting of domain-specific recombinant proteins and postembedding immunoelectron microscopy. Br J Dermatol. (2004) 150:843–51. doi: 10.1111/j.1365-2133.2004.05933.x
194. Futei Y, Amagai M, Sekiguchi M, Nishifuji K, Fujii Y, Nishikawa T. Use of domain-swapped molecules for conformational epitope mapping of desmoglein 3 in pemphigus vulgaris. J Invest Dermatol. (2000) 115:829–34. doi: 10.1046/j.1523-1747.2000.00137.x
195. Amagai M, Ishii K, Hashimoto T, Gamou S, Shimizu N, Nishikawa T. Conformational epitopes of pemphigus antigens (Dsg1 and Dsg3) are calcium dependent and glycosylation independent. J Invest Dermatol. (1995) 105:243–7. doi: 10.1111/1523-1747.ep12317587
196. Kowalczyk AP, Anderson JE, Borgwardt JE, Hashimoto T, Stanley JR, Green KJ. Pemphigus sera recognize conformationally sensitive epitopes in the amino-terminal region of desmoglein-1. J Invest Dermatol. (1995) 105:147–52. doi: 10.1111/1523-1747.ep12316680
197. Bieber K, Sun S, Ishii N, Kasperkiewicz M, Schmidt E, Hirose M, et al. Animal models for autoimmune bullous dermatoses. Exp Dermatol. (2010) 19:2–11. doi: 10.1111/j.1600-0625.2009.00948.x
198. Culton DA, Qian Y, Li N, Rubenstein D, Aoki V, Filhio GH, et al. Advances in pemphigus and its endemic pemphigus foliaceus (Fogo Selvagem) phenotype: a paradigm of human autoimmunity. J Autoimmun. (2008) 31:311–24. doi: 10.1016/j.jaut.2008.08.003
199. Liu Z, Sui W, Zhao M, Li Z, Li N, Thresher R, et al. Subepidermal blistering induced by human autoantibodies to BP180 requires innate immune players in a humanized bullous pemphigoid mouse model. J Autoimmun. (2008) 31:331–8. doi: 10.1016/j.jaut.2008.08.009
200. Schiltz JR, Michel B. Production of epidermal acantholysis in normal human skin in vitro by the IgG fraction from pemphigus serum. J Invest Dermatol. (1976) 67:254–60. doi: 10.1111/1523-1747.ep12513454
201. Anhalt GJ, Labib RS, Voorhees JJ, Beals TF, Diaz LA. Induction of pemphigus in neonatal mice by passive transfer of IgG from patients with the disease. N Engl J Med. (1982) 306:1189–96. doi: 10.1056/NEJM198205203062001
202. Lazarova Z, Hsu R, Yee C, Yancey KB. Human anti-laminin 5 autoantibodies induce subepidermal blisters in an experimental human skin graft model. J Invest Dermatol. (2000) 114:178–84. doi: 10.1046/j.1523-1747.2000.00829.x
203. Woodley DT, Chang C, Saadat P, Ram R, Liu Z, Chen M. Evidence that anti-type VII collagen antibodies are pathogenic and responsible for the clinical, histological, and immunological features of epidermolysis bullosa acquisita. J Invest Dermatol. (2005) 124:958–64. doi: 10.1111/j.0022-202X.2005.23702.x
204. Ludwig RJ, Vanhoorelbeke K, Leypoldt F, Kaya Z, Bieber K, McLachlan SM, et al. Mechanisms of autoantibody-induced pathology. Front Immunol. (2017) 8:603. doi: 10.3389/fimmu.2017.00603
205. Genovese G, Di Zenzo G, Cozzani E, Berti E, Cugno M, Marzano AV. New insights into the pathogenesis of bullous pemphigoid: 2019 update. Front Immunol. (2019) 10:1506. doi: 10.3389/fimmu.2019.01506
206. Pfutze M, Eming R, Kneisel A, Kuhlmann U, Hoyer J, Hertl M. Clinical and immunological follow-up of pemphigus patients on adjuvant treatment with immunoadsorption or rituximab. Dermatology. (2009) 218:237–45. doi: 10.1159/000187431
207. Cheng SW, Kobayashi M, Kinoshita-Kuroda K, Tanikawa A, Amagai M, Nishikawa T. Monitoring disease activity in pemphigus with enzyme-linked immunosorbent assay using recombinant desmogleins 1 and 3. Br J Dermatol. (2002) 147:261–5. doi: 10.1046/j.1365-2133.2002.04838.x
208. Harman KE, Seed PT, Gratian MJ, Bhogal BS, Challacombe SJ, Black MM. The severity of cutaneous and oral pemphigus is related to desmoglein 1 and 3 antibody levels. Br J Dermatol. (2001) 144:775–80. doi: 10.1046/j.1365-2133.2001.04132.x
209. Abasq C, Mouquet H, Gilbert D, Tron F, Grassi V, Musette P, et al. ELISA testing of anti-desmoglein 1 and 3 antibodies in the management of pemphigus. Arch Dermatol. (2009) 145:529–35. doi: 10.1001/archdermatol.2009.9
210. Schmidt E, Obe K, Brocker EB, Zillikens D. Serum levels of autoantibodies to BP180 correlate with disease activity in patients with bullous pemphigoid. Arch Dermatol. (2000) 136:174–8. doi: 10.1001/archderm.136.2.174
211. Tsuji-Abe Y, Akiyama M, Yamanaka Y, Kikuchi T, Sato-Matsumura KC, Shimizu H. Correlation of clinical severity and ELISA indices for the NC16A domain of BP180 measured using BP180 ELISA kit in bullous pemphigoid. J Dermatol Sci. (2005) 37:145–9. doi: 10.1016/j.jdermsci.2004.10.007
212. Feng S, Wu Q, Jin P, Lin L, Zhou W, Sang H, et al. Serum levels of autoantibodies to BP180 correlate with disease activity in patients with bullous pemphigoid. Int J Dermatol. (2008) 47:225–8. doi: 10.1111/j.1365-4632.2008.03473.x
213. Amo Y, Ohkawa T, Tatsuta M, Hamada Y, Fujimura T, Katsuoka K, et al. Clinical significance of enzyme-linked immunosorbent assay for the detection of circulating anti-BP180 autoantibodies in patients with bullous pemphigoid. J Dermatol Sci. (2001) 26:14–8. doi: 10.1016/S0923-1811(00)00149-3
214. Zone JJ, Taylor T, Hull C, Schmidt L, Meyer L. IgE basement membrane zone antibodies induce eosinophil infiltration and histological blisters in engrafted human skin on SCID mice. J Invest Dermatol. (2007) 127:1167–74. doi: 10.1038/sj.jid.5700681
215. Terra JB, Jonkman MF, Diercks GF, Pas HH. Low sensitivity of type VII collagen enzyme-linked immunosorbent assay in epidermolysis bullosa acquisita: serration pattern analysis on skin biopsy is required for diagnosis. Br J Dermatol. (2013) 169:164–7. doi: 10.1111/bjd.12300
216. Giusti D, Le Jan S, Gatouillat G, Bernard P, Pham BN, Antonicelli F. Biomarkers related to bullous pemphigoid activity and outcome. Exp Dermatol. (2017) 26:1240–7. doi: 10.1111/exd.13459
217. Koga H, Teye K, Ishii N, Ohata C, Nakama T. High index values of enzyme-linked immunosorbent assay for BP180 at baseline predict relapse in patients with bullous pemphigoid. Front Med. (2018) 5:139. doi: 10.3389/fmed.2018.00139
218. Bernard P, Reguiai Z, Tancrede-Bohin E, Cordel N, Plantin P, Pauwels C, et al. Risk factors for relapse in patients with bullous pemphigoid in clinical remission: a multicenter, prospective, cohort study. Arch Dermatol. (2009) 145:537–42. doi: 10.1001/archdermatol.2009.53
219. Fichel F, Barbe C, Joly P, Bedane C, Vabres P, Truchetet F, et al. Clinical and immunologic factors associated with bullous pemphigoid relapse during the first year of treatment: a multicenter, prospective study. JAMA Dermatol. (2014) 150:25–33. doi: 10.1001/jamadermatol.2013.5757
220. Cai SC, Lim YL, Li W, Allen JC, Chua SH, Tan SH, et al. Anti-BP180 NC16A IgG titres as an indicator of disease activity and outcome in asian patients with bullous pemphigoid. Ann Acad Med Singapore. (2015) 44:119–26.
221. Giusti D, Gatouillat G, Le Jan S, Plee J, Bernard P, Antonicelli F, et al. Anti-type VII collagen antibodies are identified in a subpopulation of bullous pemphigoid patients with relapse. Front Immunol. (2018) 9:570. doi: 10.3389/fimmu.2018.00570
222. Plee J, Le Jan S, Giustiniani J, Barbe C, Joly P, Bedane C, et al. Integrating longitudinal serum IL-17 and IL-23 follow-up, along with autoantibodies variation, contributes to predict bullous pemphigoid outcome. Sci Rep. (2015) 5:18001. doi: 10.1038/srep18001
223. Riani M, Le Jan S, Plee J, Durlach A, Le Naour R, Haegeman G, et al. Bullous pemphigoid outcome is associated with CXCL10-induced matrix metalloproteinase 9 secretion from monocytes and neutrophils but not lymphocytes. J Allergy Clin Immunol. (2017) 139:863–72. doi: 10.1016/j.jaci.2016.08.012
224. Giusti D, Gatouillat G, Le Jan S, Plee J, Bernard P, Antonicelli F, et al. Eosinophil Cationic Protein (ECP), a predictive marker of bullous pemphigoid severity and outcome. Sci Rep. (2017) 7:4833. doi: 10.1038/s41598-017-04687-5
225. Brulefert A, Le Jan S, Plee J, Durlach A, Bernard P, Antonicelli F, et al. Variation of the epidermal expression of glucocorticoid receptor-beta as potential predictive marker of bullous pemphigoid outcome. Exp Dermatol. (2017) 26:1261–6. doi: 10.1111/exd.13444
226. Daneshpazhooh M, Zafarmand Sedigh V, Balighi K, Hosseini SH, Ramezani A, Kalantari MS, et al. Immunologic prediction of relapse in patients with pemphigus vulgaris (PV) in clinical remission. J Am Acad Dermatol. (2016) 74:1160–5. doi: 10.1016/j.jaad.2015.10.051
227. Albers LN, Liu Y, Bo N, Swerlick RA, Feldman RJ. Developing biomarkers for predicting clinical relapse in pemphigus patients treated with rituximab. J Am Acad Dermatol. (2017) 77:1074–82. doi: 10.1016/j.jaad.2017.07.012
228. Schmidt E, Eming R. [Autoimmune bullous dermatoses : update on treatments and rare forms]. Hautarzt. (2019) 70:234–5. doi: 10.1007/s00105-019-4391-y
229. Izumi K, Bieber K, Ludwig RJ. Current clinical trials in pemphigus and pemphigoid. Front Immunol. (2019) 10:978. doi: 10.3389/fimmu.2019.00978
230. Hashimoto T, Ohzono A, Teye K, Numata S, Hiroyasu S, Tsuruta D, et al. Detection of IgE autoantibodies to BP180 and BP230 and their relationship to clinical features in bullous pemphigoid. Br J Dermatol. (2017) 177:141–51. doi: 10.1111/bjd.15114
231. van Beek N, Schulze FS, Zillikens D, Schmidt E. IgE-mediated mechanisms in bullous pemphigoid and other autoimmune bullous diseases. Expert Rev Clin Immunol. (2016) 12:267–77. doi: 10.1586/1744666X.2016.1123092
232. Fairley JA, Baum CL, Brandt DS, Messingham KA. Pathogenicity of IgE in autoimmunity: successful treatment of bullous pemphigoid with omalizumab. J Allergy Clin Immunol. (2009) 123:704–5. doi: 10.1016/j.jaci.2008.11.035
233. Dopp R, Schmidt E, Chimanovitch I, Leverkus M, Brocker EB, Zillikens D. IgG4 and IgE are the major immunoglobulins targeting the NC16A domain of BP180 in Bullous pemphigoid: serum levels of these immunoglobulins reflect disease activity. J Am Acad Dermatol. (2000) 42:577–83. doi: 10.1067/mjd.2000.103986
Keywords: autoantibody, autoimmune bullous dermatosis, biochip, ELISA, indirect immunofluorescence, pemphigoid, pemphigus, serology
Citation: Saschenbrecker S, Karl I, Komorowski L, Probst C, Dähnrich C, Fechner K, Stöcker W and Schlumberger W (2019) Serological Diagnosis of Autoimmune Bullous Skin Diseases. Front. Immunol. 10:1974. doi: 10.3389/fimmu.2019.01974
Received: 06 June 2019; Accepted: 05 August 2019;
Published: 20 August 2019.
Edited by:
Ralf J. Ludwig, Universität zu Lübeck, GermanyReviewed by:
Wataru Nishie, Hokkaido University, JapanCopyright © 2019 Saschenbrecker, Karl, Komorowski, Probst, Dähnrich, Fechner, Stöcker and Schlumberger. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sandra Saschenbrecker, cy5zYXNjaGVuYnJlY2tlckBldXJvaW1tdW4uZGU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.