
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Glob. Womens Health, 11 February 2025
Sec. Quality of Life
Volume 6 - 2025 | https://doi.org/10.3389/fgwh.2025.1521276
 Rebeca Del Prado
Rebeca Del Prado María García-Arrabé*
María García-Arrabé* Ángel González-de-la-Flor
Ángel González-de-la-Flor Marta De La Plaza San Frutos
Marta De La Plaza San Frutos Jaime Almazán PoloFabien Guérineau
Jaime Almazán PoloFabien Guérineau Cecilia Estrada-Barranco
Cecilia Estrada-Barranco
Background: This study explores the relationship between primary dysmenorrhea (PD), pain, pain catastrophizing, and menstruation-related quality of life in young women.
Methods: A cross-sectional study was conducted involving 44 young women, both with and without PD. Various variables including pain intensity, pain catastrophizing, and menstruation-related quality of life were assessed using validated questionnaires. Correlation and regression analyses were performed to examine the relationships between the variables.
Results: Significant associations were found between the presence of PD, tendency to catastrophize pain, and decreased menstruation-related quality of life. A high correlation was observed between pain intensity and catastrophizing, indicating mutual influence between these variables. Menstruation-related quality of life was affected in terms of health perception, psychological aspect, and symptoms among women with PD. The linear regression model demonstrated that catastrophizing explained 42.8% of the variance in menstruation-related quality of life.
Conclusions: These findings underscore the importance of addressing dysmenorrhea in young women, as it significantly impacts their quality of life related to menstruation. Understanding the factors contributing to dysmenorrhea and its effects on quality of life can inform more effective, patient-centered treatment strategies.
Primary dysmenorrhea (PD), also known as menstrual pain, is a common gynecological condition affecting young women during their reproductive years. It is characterized by pain in the lower abdomen accompanying menstruation and may be associated with other symptoms such as nausea, vomiting, fatigue, and lower back pain (1). The prevalence of PD among women of reproductive age is very high worldwide. Data shows percentages ranging from 64% in Mexico (2), 51% in China, 74.8% in Spain (3), 91.5% in Ireland (3), and 90.7% in Brazil (4). These high prevalence rates highlight the substantial burden of primary dysmenorrhea, which can adversely affect various aspects of women's lives, including work, education, and interpersonal relationships, ultimately contributing to a diminished quality of life (5).
The cause of PD is not clear. On one hand, increased prostaglandins at that point in the menstrual cycle may excite nociceptors and cause colicky pain due to increased uterine contractility (6). However, other authors suggest that menstrual pain is primarily associated with mechanisms unrelated to increased prostaglandins, such as inadequate uterine perfusion (7). In most cases, the use of Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) can alleviate symptoms (8); however, 18% of women with PD do not respond positively to administration (9). Furthermore, the presence of PD has been associated with a higher risk of experiencing chronic pelvic pain (10), central sensitization syndrome (11), and even increased pain sensitivity with changes in the central nervous system (12).
On the other hand, the presence of symptoms and such sensitization may extend beyond the days of the menstrual cycle when menstruation occurs (11). Chronic menstrual pain may be associated with a higher risk of developing mood disorders such as depression and anxiety (13), as well as sleep problems (14). It may even result in distortion in attention and cognitive processing (15), tending to magnify or exaggerate pain perception.
Mood disorders are increasingly recognized as both a consequence and a contributing factor to chronic pain conditions. This bidirectional relationship between chronic pain and mood disorders not only exacerbates pain perception but also involves common neurophysiological mechanisms, such as dysfunction of the hypothalamic-pituitary-adrenal axis, alterations in monoaminergic neurotransmission, and increased systemic inflammatory mediators (16–18). Understanding these links is essential to, first, establishing a diagnostic approach, as well as identifying effective interventions that address both the pathophysiological and psychological aspects of primary dysmenorrhea, with the aim of interrupting the cycle of chronic pain and affective comorbidities.
In patients with chronic pain, in addition to the presence of mood disorders, an increase in catastrophizing has been observed as a maladaptive response to pain perception. Its impact has been studied in various types of chronic pain, showing a significant association with pain progression (19), quality of life (15), and intensity of the pain itself (20). In the case of women with PD, catastrophizing may exacerbate the problem and its consequences (21).
PD has a high prevalence and significant impact on the quality of life of affected women, and various studies have examined the influence of psychological factors, such as catastrophizing, in modulating the pain experience (15, 20, 22). According to the World Health Organization, quality of life is defined as “an individual's perception of their position in life in the context of the culture and value systems in which they live, and in relation to their goals, expectations, standards, and concerns” (23). The assessment of quality of life in this context requires the use of specific and validated tools that address the relevant domains for this population (24, 25).
The Specific Quality of Life Questionnaire Related to Menstruation (M-QOL-22) (26) is a validated and reliable instrument designed to measure quality of life associated with menstrual pain in Spanish-speaking populations. This questionnaire consists of three subscales that assess: (1) self-perception of the situation, (2) psychological aspects, and (3) symptom perception. The subscale structure allows for a more detailed and specific evaluation of the different factors that affect quality of life in women with PD.
Given that catastrophizing has been identified as a maladaptive psychological response that can amplify pain perception and impair quality of life, it is crucial to investigate how it specifically interacts with the domains assessed by the M-QOL-22.
Despite existing research on PD, few studies have specifically examined how catastrophizing influences menstruation-related quality of life in women affected by this condition. This gap in the literature represents a significant knowledge void that the present study aims to address. The primary objective of this study is to analyze the impact of PD on various aspects of quality of life, as well as on the presence of catastrophizing thoughts. Additionally, the study seeks to explore the relationship between physical factors, pain intensity, catastrophizing thoughts, and different domains of menstruation-related quality of life in order to gain a more comprehensive understanding of the phenomenon. Finally, a linear regression model will be established to identify the variables that influence the variance in menstruation-related quality of life.
A cross-sectional observational study with a control group (CG) was conducted at the Universidad Europea de Madrid (UEM), Spain, between September 2022 and March 2023. The study received approval from the Research Ethics Committee of the European University, under the code CIPI/23.146, on April 20, 2023. To ensure methodological quality, the criteria proposed by the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (27) were followed.
Participants were recruited from students and staff at the European University of Madrid.
Recruitment of participants was done through posters placed in public spaces and messages shared on social media. These materials provided detailed information about the study, encouraged participation, described the inclusion criteria, and clarified that participation required attendance at the lab for only one day. This approach ensured transparency, clarity and broad accessibility, while maximising visibility.
Inclusion criteria for the dysmenorrhea group required participants to be women over 18 years old, within reproductive age, nulliparous, and diagnosed with PD by a physician from the UEM medical service. Exclusion criteria included having a previously diagnosed osteoarticular disorder, using hormonal contraceptives or intrauterine devices (IUDs), or having a diagnosis of endometriosis or any other urogynaecological condition, any systemic pathology or chronic pain, and any surgery in the last 6 months. CG participants had to fulfill the same criteria as the dysmenorrhea group, except they were required to be free of PD.
Participants were subsequently classified into two groups based on the physician's diagnosis: 22 women diagnosed with PD and 22 women without PD.
Upon acceptance of participation, participants completed a questionnaire including questions about the regularity of their menstrual cycle and the date of their last period. Additionally, participants completed the Pain Catastrophizing Scale (PCS) and the M-QOL-22. Data on daily lifestyle habits such as smoking habit, age, height, weight, and body mass index (BMI) were also collected. Pain intensity during the first day of the cycle was quantified using the visual analogue scale (VAS) (28). Participants completed the questionnaires under the supervision of a physiotherapist, who was available to address any questions that arose during the process.
To obtain information about quality of life and menstruation-related catastrophizing, several validated instruments were used:
To assess catastrophizing associated with menstrual pain, the PCS (29) was used. It consists of 13 items expressing different thoughts and emotions that may be associated with pain. The items are divided into three spheres: magnification, rumination, and helplessness. Each item is rated on a 5-point Likert scale, from (0) not at all to (4) all the time. Higher scores indicate a higher degree of pain catastrophizing (30).
The M-QOL-22 (26) was specifically developed to assess the impact of menstrual pain on the quality of life of women of childbearing age. It addresses perceptual, psychological, and symptomatic aspects related to menstruation. It consists of 22 items, each rated on 3-point Likert scales, where higher scores indicate poorer quality of life. It is further divided into three subscales exploring three aspects of quality of life: perception of health and physical and functional well-being, psychological and cognitive well-being, and symptomatology associated with menstruation (26). This questionnaire has demonstrated excellent test-retest reliability [intraclass correlation coefficient (ICC) = 0.9] and excellent internal consistency (Cronbach's Alpha = 0.917).
The sample size estimation was calculated using a commonly accepted rule-of-thumb method for regression analyses, which suggests having a minimum of 10 data points per predictor variable to ensure adequate power for detecting associations and conducting factor analysis (31, 32). Following this recommendation, a minimum requirement of at least 40 participants per model was determined (33).
All statistical analyses were performed using SPSS software v.29 for Windows (IBM SPSS, Armonk, NY, USA). Initially, the normality of data distribution was assessed using the Shapiro–Wilk test and histograms, while variance homogeneity was examined using the Levene test. P-values less than.05 were considered indicative of non-normal distribution, while P-values greater than.05 suggested normal distribution. Descriptive analysis was then conducted to characterize the sample, with measures of central tendency and dispersion presented as mean and standard deviation for normally distributed variables, and median and interquartile range for non-normally distributed variables, respectively.
Differences between cases and controls were evaluated using the Student t-test for independent samples for quantitative data, with a significance threshold set at p < .05.
Associations between variables were estimated by creating a matrix with Pearson correlation coefficients (r). Correlation levels were established as follows: Non-existent (r < 0.1); Low (r = ≥0.1 < 0.3); Moderate (r = ≥0.3 < 0.5); High (r = ≥0.5 < 0.7), Very high (r = ≥0.7 < 0.9), and Almost perfect (r ≥ 0.9) (32). Additionally, r coefficients were used to detect multicollinearity and shared variance (defined as r > 0.80) to mitigate the risk of bias and overestimation in the regression model.
A multivariate linear stepwise regression model was developed to assess menstruation-related quality of life. Variables demonstrating the strongest correlation, without shared variance and achieving statistical significance (p < .05), were sequentially included in the stepwise regression model. The significance criterion for the critical F value was set at p < .05, with changes in adjusted variance (adjusted R2) reported at each step to assess the individual variance contribution (26, 30, 31).
A total of 44 women were recruited randomly from those who volunteered to participate in the study. After being diagnosed by the university medical service, they were divided into 22 participants in the PD group and 22 participants in the CG. Table 1 summarizes the anthropometric characteristics of the study participants and the intensity of pain on the first day of menstruation, collected using the VAS. The data are distributed across the total sample group and the PD and control subgroups.

Table 1. Anthropometric and pain related characteristics of the study participants.
Regarding age, weight, height, and body mass index (BMI), no significant differences were found between the CG and the PD group (p > 0.05 for all comparisons). However, significant differences were found between the groups regarding pain intensity. The PD group exhibited considerably higher pain intensity (8.14 ± 1.28) compared to the CG (3.23 ± 1.38) (p < 0.001). This difference in pain intensity between the groups was statistically significant (mean difference: −4.91 points; 95% CI: −5.72; −4.10), highlighting the significant influence of PD on pain experience in the study participants.
Table 2 presents data on pain catastrophizing and menstruation-related quality of life (M-QOL-22) in the total sample, as well as in the control and PD subgroups. Significant differences between the groups were found in terms of pain catastrophizing. The PD group exhibited a higher score on the PCS, with an average of 25.55 (±9.60), compared to the CG with an average of 7.41 (±8.51) (P < 0.001). This difference in PCS between the groups was statistically significant, with a mean difference of 18.14 points (95% CI: −23.65; −12.62), indicating a greater tendency to catastrophize pain in women with PD. Statistically significant differences were also found between the two groups in all three subscales: Rumination with a mean difference of −6.63 points (95% CI: −8.60; −4.67), Magnification, −2 points (95% CI: −3.48; −0.52), and Helplessness −9.5 points (95% CI: −12; −6.99).
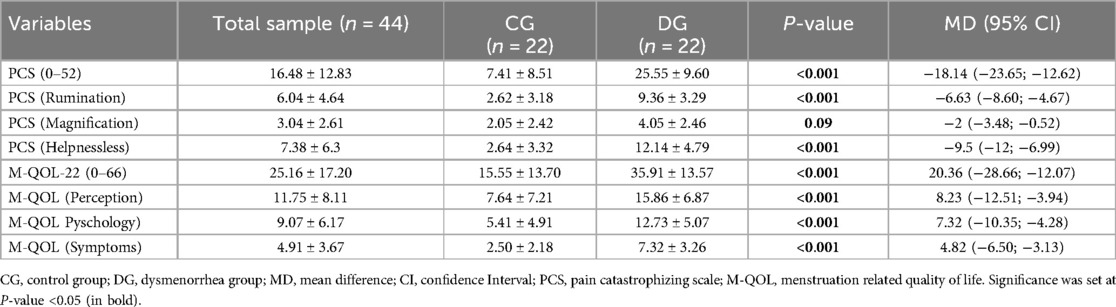
Table 2. Pain catastrophizing and menstruation-related quality of life data of the total sample, control and dysmenorrhea group.
Regarding menstruation-related quality of life (M-QOL), significant differences were observed between the groups in the perception, psychology, and symptoms subscales. The DG reported significantly lower scores in all M-QOL subscales compared to the CG (P < 0.001 for all comparisons). Specifically, the DG showed lower average scores in M-QOL (Perception), M-QOL (Psychology), and M-QOL (Symptoms) compared to the CG, with mean differences of 8.23 points (95% CI: −12.51; −3.94), 7.32 points (95% CI: −10.35; −4.28), and 4.82 points (95% CI: −6.50; −3.13) respectively.
The correlation data presented in Table 3 show significant relationships between the evaluated variables in the sample of young women in the DG, while in the CG no significant correlations were found in any of the studied variables. In the DG, a very high significant correlation was observed between pain intensity and pain catastrophizing (PCS) [r = 0.73 (p < 0.001)], high with the PCS (Rumination) subscale [r = 0.57 (p = 0.005)] and PCS (Magnification) [r = 0.662 (p < 0.001)], and very high with the PCS (Helplessness) subscale [r = 0.73 (p < 0.001)]. Moderate correlations were found between pain intensity and quality of life [r = 0.45 (p = 0.03)], as well as the different subscales: M-QOL (Perception) [R = 0.438 (p = 0.04)], M-QOL (Psychology) [r = 0.42 (p = 0.05)], and M-QOL (Symptoms) [r = 0.46 (p = 0.03)]. Also, with the different subscales of catastrophizing (r = 0.784, P < 0.01), as well as between pain catastrophizing and the subscales of menstruation-related quality of life (M-QOL) (r = 0.448–0.689, P < 0.01). A high level of correlation was also found between quality of life and catastrophizing [r = 0.65 (p = 0.001)]. The correlation between the total M-QOL-22 score and the different subscales of the PCS was significant in all cases and moderate for rumination [r = 0.47 (p = 0.027)] and high for magnification [r = 0.69 (p < 0.001)] and helplessness [r = 0.62 (p = 0.002)]. The other subscales of quality of life and catastrophizing also correlated positively with each other, except M-QOL (Psychology) and M-QOL (Symptoms) with PCS (Rumination) whose correlations were not significant.
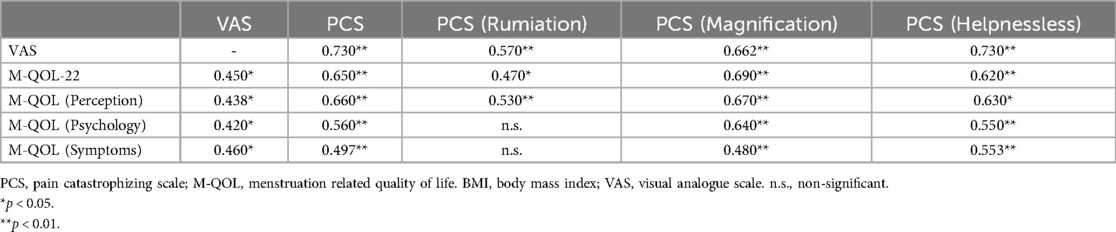
Table 3. Correlation analysis of evaluated variables in the dysmenorrhea group.
Given the high correlation between catastrophizing and quality of life, a linear regression model was conducted to further explore this relationship. Table 4 shows the parameters of the linear regression models. A model was established in which PCS scores could substantially explain (42.8% of the variance) the score on the M-QOL-22 scale for the total sample.

Table 4. Summary of the regression analyses to determine predictors of M-QOL-22.
These findings indicate a significant relationship between PD, pain, pain catastrophizing, and decreased menstrual-related quality of life in young women. The presence of PD was associated with a greater tendency to catastrophize pain, both in the aspect of rumination, magnification and helplessness, and a worse menstrual-related quality of life in terms of perception, psychology and symptoms with respect to CG. These data reveal a worrisome reality given the enormous prevalence of PD in women of childbearing age worldwide.
Our findings align with previous research demonstrating a connection between heightened pain perception and increased catastrophizing, which in turn diminishes quality of life (21). One possible explanation for this relationship is that intensified pain perception amplifies the psychological impact of PD, leading to maladaptive coping strategies like catastrophizing, creating a feedback loop that worsens both pain intensity and emotional distress (20, 21). Central sensitization has also been suggested as a mechanism driving this cycle, as it has been implicated in both chronic pelvic pain and pain catastrophizing (11). These interrelated mechanisms underscore the need for multidimensional treatment approaches. Interventions targeting catastrophizing behaviors could disrupt this feedback loop, reducing pain perception and improving quality of life. Further studies should examine whether such interventions can mitigate the effects of central sensitization in PD.
Menstrual pain intensity may be mediated by physiological factors such as the presence of heavy bleeding, certain dietary habits (34), or vitamin D levels (35). However, our findings corroborate that PD is a multifactorial phenomenon in which psychological, social, and cultural factors coexist that can influence the perception of such pain, such as educational level, adequate information, or economic status (35). Psychosocial factors, including parental education and care regarding girls’ menstrual health (36), may also play a role in shaping the perception of pain (21). Moreover, although none of the participants were menstruating when completing the questionnaires, our results align with those of Gagnon et al. (11), suggesting that quality of life alterations and increased catastrophizing persist throughout the menstrual cycle.
No relationships between catastrophizing and quality of life were found in any of the subscales in the CG, unlike the DG. This may be explained because, while both variables may be influenced by other factors in CG women, the level of quality of life, in the absence of pain, is high enough for the correlation not to be significant.
In this study, the PCS was used, allowing the analysis of different aspects of catastrophization such as rumination, magnification, and helplessness. Rumination has been more related to the cognitive and attentional aspect, focusing on the phenomenon, magnification is related to an evaluation of the event as a threat, and helplessness is related to a sense of defenselessness or incapacity to cope, following a secondary evaluation (37, 38). According to our results, all three subscales showed high significant correlations with pain intensity. Although some studies, such as that by Cosic et al. (39), reported higher levels of catastrophization during the first day of the menstrual cycle, the participants in this study were not in this moment and yet reported higher levels of catastrophism.
The scale used in this study, the M-QOL-22, is a scale developed and validated in Spanish that specifically studies quality of life in relation to menstruation. To our knowledge, the relationship between quality of life restricted to aspects related to menstruation and catastrophization had not been previously studied. The M-QOL-22 subdivides quality of life spheres into three different aspects: health perception, psychological, and symptom-related. Our findings show that all three spheres are affected by pain intensity in the case of women with PD. However, rumination only showed significant correlations with the health perception subscale, not with the psychological or symptomatology subscale. This could be explained by the fact that focusing attention on one's own health status modifies the perception we have of it. These results coincide with those found by Craner et al. (40), where rumination was the only one of the three subscales that was not clearly associated with the other variables studied.
None of the anthropometric variables showed significant correlations with quality of life or catastrophization. However, the relationship between total scores of PCS and M-QOL-22 in the total sample and in the PD group is established by the regression model obtained in this study. These data allow us to delve into the capacity of the PCS to predict values of quality of life, which may allow for establishing strategies for catastrophization that improve the quality of life of women with PD.
These findings underscore the need for a comprehensive approach to managing dysmenorrhea (PD), recognizing its significant impact on menstrual-related quality of life and pain perception. Effective management should integrate physical and psychological interventions to address the multifaceted nature of PD. Interventions targeting pain catastrophizing, alongside symptom alleviation strategies, hold promise for reducing pain intensity and improving overall well-being in affected women. Chronic pain management strategies should not only aim to reduce symptoms but also foster adaptation and coping, emphasizing a holistic approach to improving quality of life (41).
Recent evidence supports the efficacy of manual therapy and pelvic floor exercises in reducing pain associated with PD (42), while cognitive-behavioral approaches targeting catastrophizing may further enhance outcomes. Future studies should explore the integration of these strategies into a holistic treatment model to evaluate their combined impact on pain management and quality of life. Additionally, pelvic manipulation has demonstrated potential in altering pain perception in PD (43), highlighting the value of integrating manual therapy into routine care. Future research should focus on evaluating the effectiveness of such multidisciplinary interventions in clinical settings.
Expanding research to explore the benefits of physiotherapeutic techniques, cognitive-behavioral therapies, and lifestyle modifications—including dietary changes and physical activity—would provide valuable insights into PD management. Furthermore, assessing these interventions across different phases of the menstrual cycle could deepen our understanding of their efficacy and inform more personalized treatment strategies.
This study is not without limitations, which should be carefully considered when interpreting the findings. First, the cross-sectional design of the study allows for the identification of associations but precludes establishing causal relationships between variables. Second, while validated questionnaires were used to mitigate concerns about the accuracy of self-reported measures for assessing musculoskeletal conditions, the inherent limitations of self-reports, such as potential recall or response bias, remain. Third, the relatively small sample size (n = 44) limits the statistical power of the study and may reduce the generalizability of the findings. Future research should include larger, more diverse populations to enhance external validity and provide a more comprehensive understanding of these relationships. Finally, while all participants were in a similar phase of the menstrual cycle, which strengthens group comparisons, the study did not capture longitudinal data across different phases of the cycle. It would be valuable to replicate the study with a longitudinal design to explore the evolution of variables throughout the menstrual cycle.
Women with PD present lower quality of life related to menstruation both globally and in the perception of health status, psychological aspect and symptoms associated with menstruation, as well as higher levels of catastrophizing, the variables being related to each other. The linear regression model showed that catastrophizing explained 42.8% of the variance in menstruation-related quality of life.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Research Ethics Committee of the European University with code CIPI/23.146. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
RDP: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. MG-A: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. ÁG-d-l-F: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. MDLPSF: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. JAP: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. FG: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. CE-B: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Bernardi M, Lazzeri L, Perelli F, Reis FM, Petraglia F. Dysmenorrhea and related disorders. F1000Res. (2017) 6:1645. doi: 10.12688/f1000research.11682.1
2. Ortiz MI. Primary dysmenorrhea among Mexican university students: prevalence, impact and treatment. Eur J Obstet Gynecol Reprod Biol. (2010) 152:73–7. doi: 10.1016/j.ejogrb.2010.04.015
3. Durand H, Monahan K, McGuire BE. Prevalence and impact of dysmenorrhea among university students in Ireland. Pain Med. (2021) 22:2835–45. doi: 10.1093/pm/pnab122
4. Barbosa-Silva J, Avila MA, de Oliveira RF, Dedicação AC, Godoy AG, Rodrigues JC, et al. Prevalence, pain intensity and symptoms associated with primary dysmenorrhea: a cross-sectional study. BMC Womens Health. (2024) 24:92. doi: 10.1186/s12905-023-02878-z
5. Stokes R, Mikocka-Walus A, Dowding C, Druitt M, Evans S. “It’s just another unfortunate part of being female”: a qualitative study on dysmenorrhea severity and quality of life. J Clin Psychol Med Settings. (2023) 30:628–35. doi: 10.1007/s10880-022-09930-4
6. Dawood MY. Primary dysmenorrhea: advances in pathogenesis and management. Obstet Gynecol. (2006) 108(2):428–41. doi: 10.1097/01.AOG.0000230214.26638.0c
7. Dmitrović R. Transvaginal color Doppler study of uterine blood flow in primary dysmenorrhea. Acta Obstet Gynecol Scand. (2000) 79(12):1112–6. doi: 10.1034/j.1600-0412.2000.0790121112.x
8. Marjoribanks J, Ayeleke RO, Farquhar C, Proctor M. Nonsteroidal anti-inflammatory drugs for dysmenorrhoea. Cochrane Database Syst Rev. (2015) 2015(7):CD001751. doi: 10.1002/14651858.CD001751.pub3
9. Oladosu FA, Tu FF, Hellman KM. Nonsteroidal antiinflammatory drug resistance in dysmenorrhea: epidemiology, causes, and treatment. Am J Obstet Gynecol. (2018) 218(4):390–400. doi: 10.1016/j.ajog.2017.08.108
10. Li R, Li B, Kreher DA, Benjamin AR, Gubbels A, Smith SM. Association between dysmenorrhea and chronic pain: a systematic review and meta-analysis of population-based studies. Am J Obstet Gynecol. (2020) 223:350–71. doi: 10.1016/j.ajog.2020.03.002
11. Gagnon MM, Elgendy R. Comorbid pain experiences in young women with dysmenorrhea. Women Health. (2020) 60:946–57. doi: 10.1080/03630242.2020.1781741
12. Liu J, Liu H, Mu J, Xu Q, Chen T, Dun W, et al. Altered white matter microarchitecture in the cingulum bundle in women with primary dysmenorrhea: a tract-based analysis study. Hum Brain Mapp. (2017) 38:4430–43. doi: 10.1002/hbm.23670
13. Uçar T, Timur Taşhan S, Aksoy Derya Y, Nacar G. An analysis of dysmenorrhoea and depressive symptoms in university students: a case-control study. Int J Nurs Pract. (2018) 24:e12678. doi: 10.1111/ijn.12678
14. Jeon B, Baek J. Menstrual disturbances and its association with sleep disturbances: a systematic review. BMC Womens Health. (2023) 23:470. doi: 10.1186/s12905-023-02629-0
15. Talaei-Khoei M, Ogink PT, Jha R, Ring D, Chen N, Vranceanu AM. Cognitive intrusion of pain and catastrophic thinking independently explain interference of pain in the activities of daily living. J Psychiatr Res. (2017) 91:156–63. doi: 10.1016/j.jpsychires.2017.04.005
16. Yamauchi N, Sato K, Sato K, Murakawa S, Hamasaki Y, Nomura H, et al. Chronic pain–induced neuronal plasticity in the bed nucleus of the stria terminalis causes maladaptive anxiety. Sci Adv. (2022) 8(17). doi: 10.1126/sciadv.abj5586
17. Rogers AH, Farris SG. A meta-analysis of the associations of elements of the fear-avoidance model of chronic pain with negative affect, depression, anxiety, pain-related disability and pain intensity. Eur J Pain. (2022) 26(8):1611–35. doi: 10.1002/ejp.1994
18. Werneck AO, Stubbs B. Bidirectional relationship between chronic pain and depressive symptoms in middle-aged and older adults. Gen Hosp Psychiatry. (2024) 91:190. doi: 10.1016/j.genhosppsych.2024.11.004
19. Angst F, Lehmann S, Sandor PS, Benz T. Catastrophizing as a prognostic factor for pain and physical function in the multidisciplinary rehabilitation of fibromyalgia and low back pain. Eur J Pain. (2022) 26:1569–80. doi: 10.1002/ejp.1983
20. Evans S, Dowding C, Olive L, Payne LA, Druitt M, Seidman LC, et al. Pain catastrophizing, but not mental health or social support, is associated with menstrual pain severity in women with dysmenorrhea: a cross-sectional survey. Psychol Health Med. (2022) 27:1410–20. doi: 10.1080/13548506.2021.1948581
21. Walsh TM, LeBlanc L, McGrath PJ. Menstrual pain intensity, coping, and disability: the role of pain catastrophizing. Pain Med. (2003) 4:352–61. doi: 10.1111/j.1526-4637.2003.03039.x
22. Leon-Larios F, Silva-Reus I, Puente Martínez MJ, Renuncio Roba A, Ibeas Martínez E, Lahoz Pascual I, et al. Influence of menstrual pain and symptoms on activities of daily living and work absenteeism: a cross-sectional study. Reprod Health. (2024) 21:25. doi: 10.1186/s12978-024-01757-6
23. The world health organization quality of life assessment (WHOQOL): position paper from the world health organization. Soc Sci Med. (1995) 41:1403–9. doi: 10.1016/0277-9536(95)00112-K
24. Camas-Castillo MA, Gallardo-Alvarado N, Yánez-Sánchez P, Makuch MY, Osis MJD, Bahamondes L. Menstrual health: inequities in a cohort of menstruating people in the Brazilian southeastern region. Int J Gynaecol Obstet. (2024) 164(3):1160–6. doi: 10.1002/ijgo.15223
25. Mizuta R, Maeda N, Tashiro T, Suzuki Y, Oda S, Komiya M, et al. Quality of life by dysmenorrhea severity in young and adult Japanese females: a web-based cross-sectional study. PLoS One. (2023) 18(3):e0283130. doi: 10.1371/journal.pone.0283130
26. Torres-Pascual C, Torrell-Vallespín S, Mateos-Pedreño E, García-Serra J. Development and validation of the specific quality of life questionnaire related to menstruation CVM-22. Rev Cuba Obstetr Ginecol. (2019) 45(1):48–59.
27. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Bull World Health Organ. (2007) 85:867–72. doi: 10.2471/BLT.07.045120
28. Maeda-Minami A, Kawamoto A, Yoshino T, Yokoyama Y, Suzuki S, Horiba Y, et al. Patient prognosis and prediction model for taking Kampo formulas in dysmenorrhea: an observational study. Medicine (Baltimore). (2023) 102:e36191. doi: 10.1097/MD.0000000000036191
29. García Campayo J, Rodero B, Alda M, Sobradiel N, Montero J, Moreno S. Validation of the Spanish version of the pain catastrophizing scale in fibromyalgia. Med Clin (Barc). (2008) 131:487–92. doi: 10.1157/13127277
30. Wheeler CHB, Williams ACC, Morley SJ. Meta-analysis of the psychometric properties of the pain catastrophizing scale and associations with participant characteristics. Pain. (2019) 160:1946–53. doi: 10.1097/j.pain.0000000000001494
31. Wilson Van Voorhis CR, Morgan BL. Understanding power and rules of thumb for determining sample sizes. Tutor Quant Methods Psychol. (2007) 3(2):43–50. doi: 10.20982/tqmp.03.2.p043
32. Green SB. How many subjects does it take to do A regression analysis. Multivariate Behav Res. (1991) 26(3):499–510. doi: 10.1207/s15327906mbr2603_7
34. Abu Helwa HA, Mitaeb AA, Al-Hamshri S, Sweileh WM. Prevalence of dysmenorrhea and predictors of its pain intensity among Palestinian female university students. BMC Womens Health. (2018) 18:18. doi: 10.1186/s12905-018-0516-1
35. Zeynali M, Haghighian HK. Is there a relationship between serum vitamin D with dysmenorrhea pain in young women? J Gynecol Obstetr Hum Reprod. (2019) 48:711–4. doi: 10.1016/j.jogoh.2019.03.002
36. Bellis EK, Li AD, Jayasinghe YL, Girling JE, Grover SR, Peate M, et al. Exploring the unmet needs of parents of adolescent girls with heavy menstrual bleeding and dysmenorrhea: a qualitative study. J Pediatr Adolesc Gynecol. (2020) 33(3):271–7. doi: 10.1016/j.jpag.2019.12.007
37. Sullivan MJL, Thorn B, Haythornthwaite JA, Keefe F, Martin M, Bradley LA, et al. Theoretical perspectives on the relation between catastrophizing and pain. Clin J Pain. (2001) 17(1):52–64. doi: 10.1097/00002508-200103000-00008
38. Bonafé FSS, Campos LA, Marôco J, Campos JADB. Pain catastrophizing: rumination is a discriminating factor among individuals with different pain characteristic. Braz Oral Res. (2019) 33:e113. doi: 10.1590/1807-3107bor-2019.vol33.0113
39. Cosic A, Ferhatovic L, Banozic A, Kraljevic S, Maric A, Sapunar D, et al. Pain catastrophizing changes during the menstrual cycle. Psychol Health Med. (2013) 18(6):735–41. doi: 10.1080/13548506.2013.769609
40. Craner JR, Gilliam WP, Sperry JA. Rumination, magnification, and helplessness: how do different aspects of pain catastrophizing relate to pain severity and functioning? Clin J Pain. (2016) 32(12):1028–35. doi: 10.1097/AJP.0000000000000355
41. Wippert PM, Wiebking C. Adaptation to physical activity and mental stress in the context of pain: psychobiological aspects. Schmerz. (2016) 30(5):429–36. doi: 10.1007/s00482-016-0147-0
42. Deodato M, Grosso G, Drago A, Martini M, Dudine E, Murena L, et al. Efficacy of manual therapy and pelvic floor exercises for pain reduction in primary dysmenorrhea: a prospective observational study. J Bodyw Mov Ther. (2023) 36:185–91. doi: 10.1016/j.jbmt.2023.07.002
Keywords: dysmenorrhea, pain, pain catastrophizing, quality of life, menstruation
Citation: Del Prado R, García-Arrabé M, González-de-la-Flor Á, De La Plaza San Frutos M, Almazán Polo J, Guérineau F and Estrada-Barranco C (2025) Exploration of the relationship between primary dysmenorrhea, pain perception, and menstruation-related quality of life in young women: a cross-sectional observational study. Front. Glob. Womens Health 6:1521276. doi: 10.3389/fgwh.2025.1521276
Received: 1 November 2024; Accepted: 28 January 2025;
Published: 11 February 2025.
Edited by:
Manuela Deodato, University of Trieste, ItalyCopyright: © 2025 Del Prado, García-Arrabé, González-de-la-Flor, De La Plaza San Frutos, Almazán Polo, Guérineau and Estrada-Barranco. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: María García-Arrabé, bWFyaWEuZ2FyYXJyYWJlQHVuaXZlcnNpZGFkZXVyb3BlYS5lcw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.