 Tadesse Ayana Fentie1*
Tadesse Ayana Fentie1* Abayneh Aklilu Solomon2
Abayneh Aklilu Solomon2 Mihretu Molla Enyew2
Mihretu Molla Enyew2 Meseret Mekuriaw Beyene3
Meseret Mekuriaw Beyene3 Ayalew Kassie Melese3
Ayalew Kassie Melese3 Alamirew Enyew Belay4
Alamirew Enyew Belay4 Gebrie Getu Alemu5
Gebrie Getu Alemu5
- 1Department of Midwifery, College of Health Sciences, Bahir Dar Health Science College, Bahir Dar, Ethiopia
- 2School of Midwifery, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
- 3Department of Nursing, College of Health Sciences, Bahir Dar Health Science College, Bahir Dar, Ethiopia
- 4Department of Adult Health Nursing, College of Medicine and Health Sciences, Bahirdar University, Bahirdar, Ethiopia
- 5Department of Epidemiology and Biostatistics, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Background: Respectful maternity care is care organized for and provided to all women in a manner that maintains their dignity, privacy, and confidentiality, ensures freedom from harm and mistreatment, and enables informed choice and continuous support during labor and childbirth. However, in many healthcare settings in Ethiopia, the standard practice of respectful obstetric care is not the norm, and a significant proportion of health professionals view patients merely as cases and do not show compassion.
Objectives: To assess respectful maternity care and associated factors among mothers who gave birth at public health institutions in Debre Tabor town, Northwest Ethiopia from December 1, 2023, to January 30, 2024.
Methods: An institution-based cross-sectional study was conducted using qualitative and quantitative data collection methods. Three hundred seventy participants were selected for quantitative analysis using systematic random sampling, while eight were chosen for the qualitative study through purposive sampling. The quantitative data were coded and entered into Epi Data version 4.6, then exported to the Statistical Package for the Social Sciences (SPSS) version 25 for analysis. A multivariable logistic regression analysis was performed to identify factors associated with the outcome variable. Adjusted odds ratios with 95% confidence intervals were computed to determine the significance level. Thematic analysis was used for the qualitative data.
Results: The proportion of respectful maternity care was 34.1% (95%CI: 29.4, 39.2) cesarean delivery [AOR = 3.45, 95%CI: 1.60, 7.42]. Daytime delivery [AOR = 3.14, 95%CI: (1.59, 6.18)] and less than or equal to 1 day stay in a healthcare facility [AOR = 3.03, 95%CI: (1.51, 6.08)] were positively associated with respectful maternity care. Inadequate equipment and supplies, shortage of staffing, and lack of accountability were barriers to providing respectful maternity care.
Conclusions: The proportion of respectful maternity care was low. Therefore, health institutions and other stakeholders should support and strengthen monitoring and evaluation mechanisms for maternal and neonatal healthcare providers and enhance education and constant support for women during their pregnancy and childbirth. Additionally, adequate access to basic equipment and supplies should be given due attention to ensure respectful maternity care.
Background
Respectful maternity care is care organized for and provided to all women in a manner that maintains their dignity, privacy, and confidentiality, ensures freedom from harm and mistreatment, and enables informed choice and continuous support during labor and childbirth (1). However, many women worldwide continue to experience abuse and neglect during childbirth in healthcare facilities (2–4).
A study conducted in six European countries—Sweden, Norway, Belgium, Estonia, Iceland, and Denmark—found that 1 in 5 women who attended antenatal care in maternity health facilities had at least one episode of abuse (5). Several studies provide insight into the alarmingly high prevalence of serious forms of disrespect and abuse in low and middle-income countries around the world, with percentages ranging from 33.3% in Mexico (6) to 71.0% in India (7).
In contrast, a significantly higher number of women in African countries experienced disrespect and abuse (D&A) during facility-based childbirth (8). According to data from sub-Saharan African countries and Eastern African countries, approximately 44% and 46.85% of women experienced D&A during facility-based childbirth, respectively (9, 10).
According to a study in Ethiopia, the prevalence of respectful maternity care (RMC) during childbirth ranges from 12.75% to 77% (11). RMC is influenced by various factors, including the place of delivery, time of delivery, antenatal care (ANC) uptake, planning status of the index pregnancy, educational level, and obstetric complications (11–21). Promoting good interpersonal relationships and support between women and maternity staff (good reception, information provision, promptness of care, dignified care, and psychological support), and privacy and confidential care are essential to ensure respectful maternity care. Ensuring facility-based respectful maternity care (RMC) is essential for improving maternal and neonatal health, especially in sub-Saharan African countries where mortality rates and non-skilled delivery care remain high (22).
In 2019, 50% of Ethiopian women gave birth at home without the assistance of a skilled birth attendant (23). The reasons for not giving birth in a health institution included anticipated poor quality of services, a history of undesirable care from healthcare providers, a failure to adopt a patient-centered approach, and insufficient health system resources (24, 25). Recognizing these, the Ethiopian Ministry of Health has implemented RMC since 2016 as a strategic measure to increase the number of deliveries attended by skilled birth attendants (13). However, in many healthcare settings in Ethiopia, including the study area, respectful obstetric care is not yet the norm, and a significant proportion of health professionals still view patients merely as “cases” and do not show compassion (21).
Despite this, there is scant research about respectful maternity care services and associated factors during facility-based childbirth (2, 26). Moreover, the existing evidence on respectful maternity service provision has primarily been gathered from client reports (13). Providers' perspectives are needed to fully understand the barriers to providing respectful maternal care. As a result, the factors and barriers that hinder the provision of respectful maternity care during facility-based childbirth are not well known. Therefore, this mixed-methods study aims to assess respectful maternity care and associated factors among mothers who gave birth at public health institutions in Debre Tabor town, Northwest Ethiopia from December 1, 2023, to January 30, 2024
Method and materials
Study design and setting
A facility-based, mixed cross-sectional study, comprising a quantitative component followed by a qualitative component, was conducted from December 1, 2023, to January 30, 2024, in public health facilities in Debre Tabor town, Northwest Ethiopia. Debre Tabor is the capital of the South Gondar Zone in the Amhara regional state, located 665 km northwest of Addis Ababa, the capital of Ethiopia, and 103 km east of Lake Tana. The town has a total population of 90,081, with 42,041 (46.7%) males and 48,040 (53.3%) females. Among them, 20.96% (17,968 individuals) fall within the reproductive age range (27, 28). The town comprises nine kebeles and four public health institutions: one comprehensive specialized hospital and three health centers. These are Debre Tabor Comprehensive Specialized Hospital (DTCSH), Leul Alemayehu Health Centre (LAHC), Gaffat Health Centre (GHC), and Atse Seyife Health Centre (ASHC). These institutions provide community health care, including maternal and child health services (29).
Source population and study population
All mothers who gave birth at public health institutions in Debre Tabor town were used as a source population. Mothers who gave birth during the data collection period were used as a study population. Moreover, senior maternal and neonatal health care (MNHC) providers were used as a study population.
Inclusion and exclusion criteria
Mothers who gave birth at public health institutions in Debre Tabor town during the data collection period were included in the study. Mothers unable to communicate due to serious illness were excluded from the study. Moreover, senior maternal and neonatal health care (MNHC) providers were used as study participants for qualitative phase data inquiries.
Sample size and sampling procedure
The sample size was determined using the single population proportion formula, considering a proportion of RMC at 66% (30), a 95% confidence level, and an allowed margin of error of 5%. An additional 10% was added to account for non-response, resulting in a final sample size of 380. Based on a previous delivery report, the sample was proportionally allocated to each health facility. A systematic random sampling technique was employed to recruit study participants according to their admission order. For the qualitative study, purposive sampling was used to recruit senior healthcare providers for key informant interviews (KIIs). The sample size for the qualitative component was determined based on information saturation, which was reached after eight KIIs.
Study variables
The outcome variable for this study was the provision of respectful maternity care during childbirth. The explanatory variables included socio-demographic factors such as age, marital status, residence, religion, educational status, and occupation; obstetric factors such as antenatal care (ANC) visits, mode of delivery, parity, time of delivery, presence of neonatal and/or maternal complications, whether the pregnancy was planned or unplanned, number of ANC visits, and duration of labor; maternal health services factors such as referral status, presence of a companion, HIV status, previous use of the facility for services other than delivery, prior deliveries at the facility, and length of stay at the health facilities; and provider and facility factors, including the sex of the delivery attendant, place of delivery, place of ANC, and profession of the attendant.
Operational definitions
Respectful maternity care was measured by 30 items, which are classified into seven categories, including the right to physical abuse-free care (8 items), the right to informed consent and information (6 items), the right to confidential care (3 items), the right to be treated with dignity (5 items), the right to be treated free of discrimination (3 items), the right not to be neglected or abandoned (3 items), and the right not to be detained or confined in health facilities (2 items). Each item has a “yes” or “no” response developed as part of the respectful maternity toolkit by the Maternal and Child Health Integrated Program (MCHIP) (3, 31). In this study, mothers were considered to be receiving respectful maternity care during childbirth if they replied “no” (which was coded as ″1″) to all questions measuring RMC, or verification criteria used for measuring the seven categories of RMC (14, 32, 33). Mothers were considered not receiving respectful maternity care if they replied “yes” (which was coded as ″0″) to one or more questions measuring RMC, or verification criteria used for measuring the seven categories of RMC (14, 32, 33).
Data collection tools and procedures
A structured and pre-tested interview-administered questionnaire developed from previously done similar literature (14, 17, 30, 32–35) and a validated RMC checklist adopted from the Maternal and Child Health Integrated Program (MCHIP) (3, 31) was used to generate quantitative data. The tool was prepared in English and translated into the local language, Amharic, then backtranslated into English. The tool consists of five parts: the first part contains the socio-demographic factors of the respondent, the second part consists of the obstetric factors of the respondents, the third part contains maternal health service factors, the fourth part contains health facility and provider factors, and the fifth part contains categories of RMC experienced by women during facility-based childbirth. Two diploma midwives carried out the data collection process under the supervision of one BSc midwife. Postpartum exit interviews were conducted with women who had just given birth at the health facility. Additionally, some data were collected by reviewing mothers' delivery cards and interviewing healthcare providers. Each eligible woman was approached privately in a separate room from the maternity ward within the hospital grounds. After checking the completeness, the filled questionnaires were collected and signed by the supervisor. Additionally, the principal investigator provided continuous supervision and follow-up throughout the data collection period.
Following the quantitative data assessment, we collected qualitative data using a semi-structured probing guide questionnaire, which we prepared in English and translated into the local language, Amharic. One author (G.G.), a university lecturer with a master's degree who had previous experience in qualitative interview, conducts key informant interviews (KIIs). Qualitative data collection was performed using face-to-face interviews with the participants. KIIs were tape-recorded, and notes were taken. Each session of the KIIs lasted between 10 and 20 min.
Data quality control
For quantitative data, the questionnaire was initially developed in English and translated into the local language Amharic, then back-translated into English by a different person to check the consistency. Supervisors and data collectors underwent 1-day training on the study objectives, obtaining informed consent, and approaching the participant. Continuous data monitoring was conducted by supervisors and the principal investigator throughout the study. To ensure the trustworthiness of the qualitative data, the criteria from Lincoln and Guba's framework were applied. For dependability, detailed reporting of the research process was carried out; for conformability, an independent person checked interview transcriptions; and transferability was established using the purposive sampling technique.
Data processing and analysis
For quantitative data, after checking completeness, the data were coded and entered into Epi Data version 4.6 and then exported to SPSS version 25 for cleaning and analysis. Descriptive summary measures, such as frequency, percentages, mean, and standard deviation, were employed to describe the characteristics of the respondents. Variance Inflation Factor (VIF) was used to check for multi-colinearity among predictors. The model fitness was checked using the Hosmer and Lemeshow goodness of fitness test, yielding a value of 0.842. Binary logistic regression analyses were carried out to assess the association between each independent variable and the outcome variable. Variables with a p-value < 0.25 were entered into a multivariable logistic regression model, and the selected variables were entered sequentially by using backward stepwise regression to control for potential confounders and identify predictors of the outcome variable. An association between outcome and explanatory variables was presented using an adjusted OR with a 95% confidence interval. Variables with a p-value < 0.05 were considered statistically significant.
Qualitative data were transcribed, translated, coded, and analyzed using Qualitative Data Analysis (QDA) minor lite version 2.0.3. A thematic approach was utilized.
Results
Quantitative part
Socio-demographic characteristics of the participants
This study involved 370 participants, resulting in a response rate of 97.4%. The mean ± SD of respondents' age was 29.04 ± 3.98 years. The minimum and maximum ages of the respondents were 19 and 37 years. The majority (68.6%) fall into the age category of 25–34 years. Approximately two-thirds (67.6%) of the participants were Orthodox. Half the participants had no formal education, and about 58.9% were from rural areas. Most (93.5%) of the study participants were married, and the majority (60.3%) were housewives (Table 1).
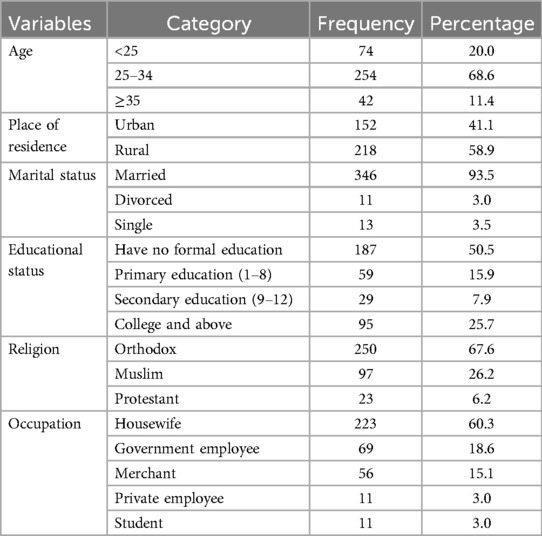
Table 1. Socio-demographic characteristics of mothers who gave birth at public health institutions in Debre Tabor town, Northwest Ethiopia, 2024 (n = 370).
Obstetric factors
Out of 370 participants, the majority (84.3%) were multiparous. While 95.4% had at least one antenatal care (ANC) visit during their index pregnancy, only 22.2% attended four or more ANC visits. Notably, a significant portion (81.6%) of pregnancies among participants were intended. Nearly half (44.9%) gave birth during nighttime hours. The majority (60.3%) did not encounter complications during labor and delivery. Furthermore, a substantial proportion (89.2%) experienced a labor duration of less than 12 h. Of the total respondents, 74.1% gave birth via spontaneous vaginal delivery (Table 2).
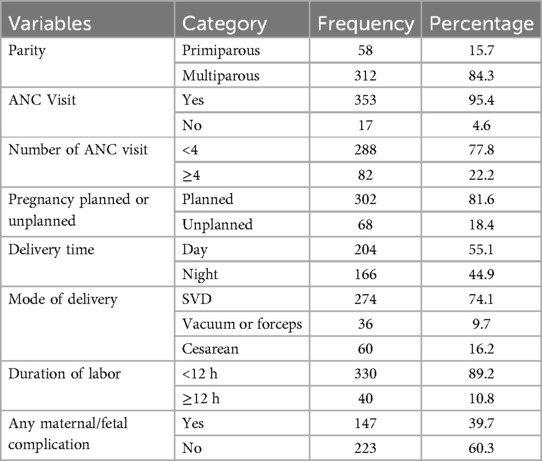
Table 2. Obstetric characteristics of mothers who gave birth at public health institutions in Debre Tabor town, Northwest Ethiopia, 2024 (n = 370).
Maternal health service-related factors
Out of the 370 participants, 51.1% arrived directly for labor and delivery, while 52.2% had previous childbirth experiences within health facilities. Additionally, 55.4% of participants stayed in the health facility for 24 h or more. The majority (69.7%) utilized health facility services beyond mere delivery. Notably, 96.2% of participants were negative for HIV. Furthermore, half (50.3%) of the participants had companions during the labor process (Table 3).
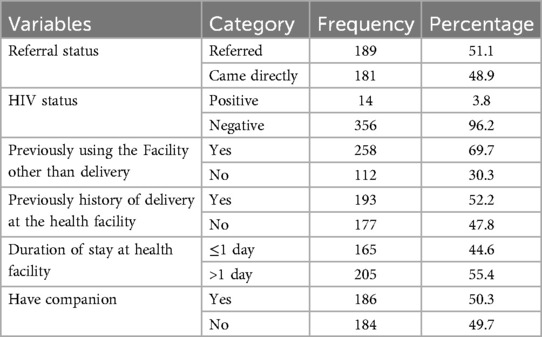
Table 3. Health service history of mothers who gave birth at public health institutions in Debre Tabor town, Northwest Ethiopia, 2024 (n = 370).
Health facility and provider factors
Out of the 370 respondents, 89.2% gave birth in a hospital setting. Midwives managed 53.3% of the deliveries, while 43.8% of the participants were attended by female healthcare providers. Nearly two-thirds (64.1%) of participants received antenatal care at health centers (Table 4).

Table 4. Health facility and provider factors of mothers who gave birth at public health institutions in Debre Tabor town, Northwest Ethiopia, 2024 (n = 370).
Proportion of respectful maternity care
The overall proportion of respectful maternity care provision among laboring mothers in the health facilities of Debre Tabor town was 34.1% (95% CI: 29.2, 39.1). The most common category of respectful maternity care identified by women in this study was providing detention-free care, which was fully respected, followed by almost all (99% and 94%) of the participants receiving discrimination-free care and abandonment-free care, respectively (Table 5).
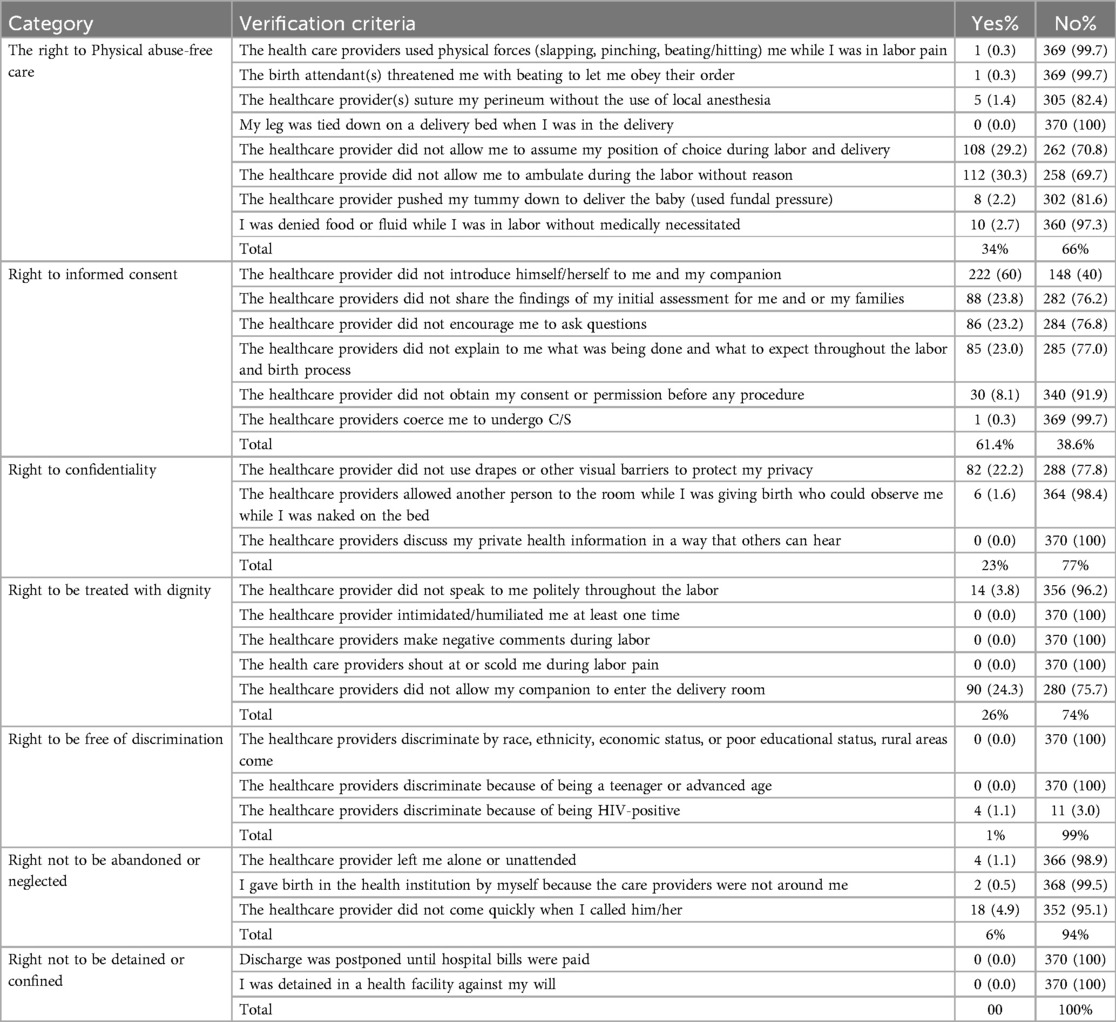
Table 5. Respectful maternity care categories among mothers who gave birth at public health institutions in Debre Tabor town, Northwest Ethiopia, 2024 (n = 370).
Factors associated with respectful maternity care
In the Bivariable logistic regression, 13 variables with a p-value less than 0.25 were considered for multivariable analysis. These variables included place of residence, educational status, occupation of mothers, mode of delivery, pregnancy wanted/intended, referral from another health facility, number of ANC visits, delivery time, sex of health provider, having a birth companion, previous delivery at a health facility, previously using the facility other than delivery, and length of stay in a health facility. The results of the multivariable analysis indicated that cesarean delivery, time of delivery, and length of stay in a health facility were found to have statistical associations with respectful maternity care.
This study identified that those mothers who gave birth by cesarean section were 3.45 times [AOR = 3.45, 95% CI: 1.60, 7.42] more likely to get respectful maternity care compared to those who gave birth by spontaneous vaginal delivery.
This study indicated that those mothers who gave birth at daytime were 3.14 times [AOR = 3.14, 95% CI: 1.59, 6.18) more likely to receive respectful maternity care as compared to those who gave birth at nighttime.
The odds of receiving respectful maternity care were 3.03 times [AOR = 3.03, 95% CI: 1.51, 6.08)] higher among mothers who stayed less than or equal to 1 day compared to those who stayed longer in health facilities (Table 6).
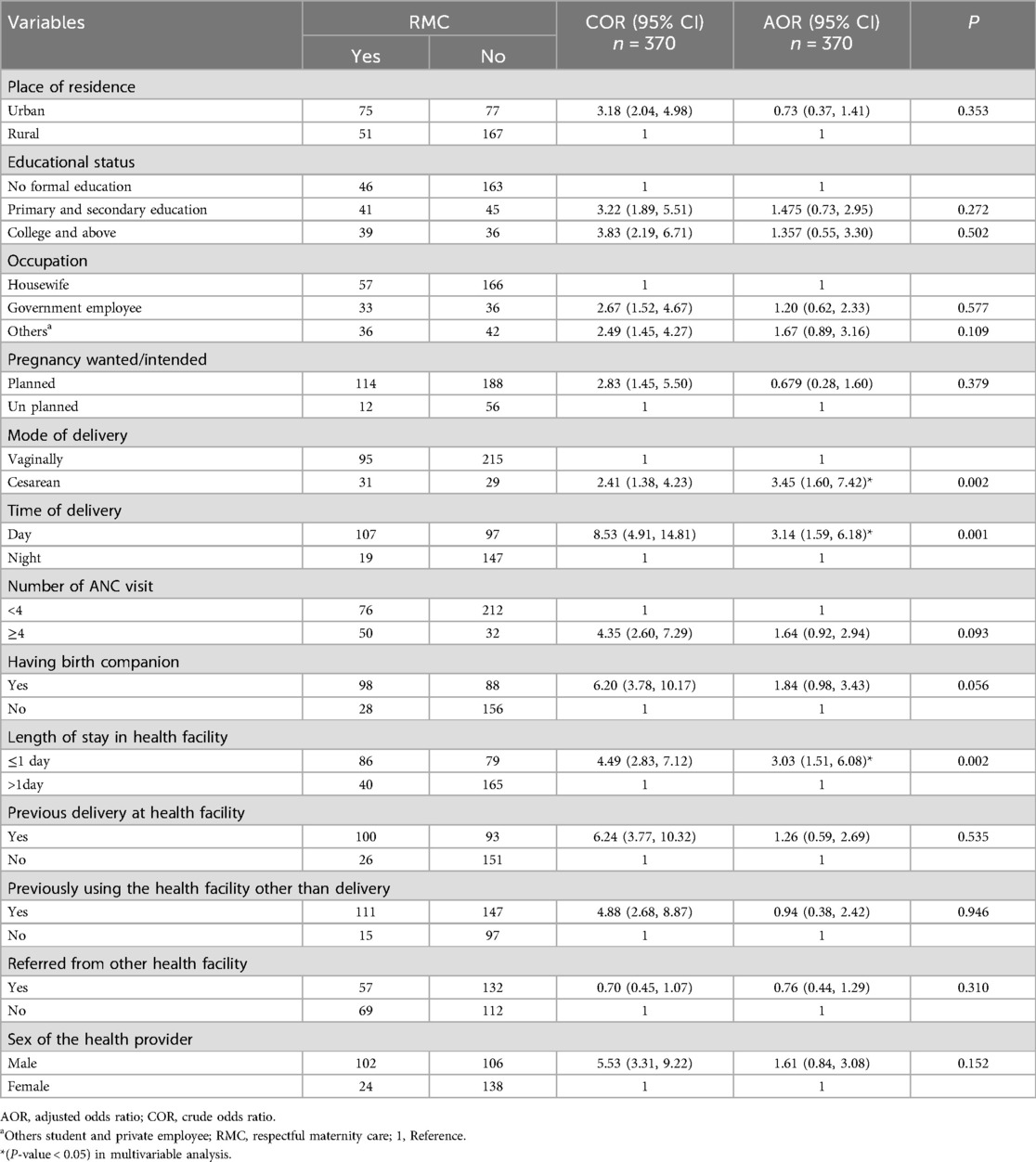
Table 6. Factors associated with respectful maternity care among mothers who gave birth at public health institutions in Debre Tabor town, Northwest Ethiopia, 2024 (n = 370).
Qualitative part
Barriers to the provision of respectful maternity care
Barriers to respectful maternity care during childbirth from health care providers' perspectives resulted in three main themes: facility-related barriers, health care provider-related barriers, maternal-related barriers, and nine sub-themes. Inadequate health facility equipment and supply, lack of accountability, lack of professional advancement, staffing shortages, task-oriented approach, insufficient nighttime staffing, lack of maternal health education, maternal perceived neglect during early labor, and presence of maternal and fetal complications (Table 7).
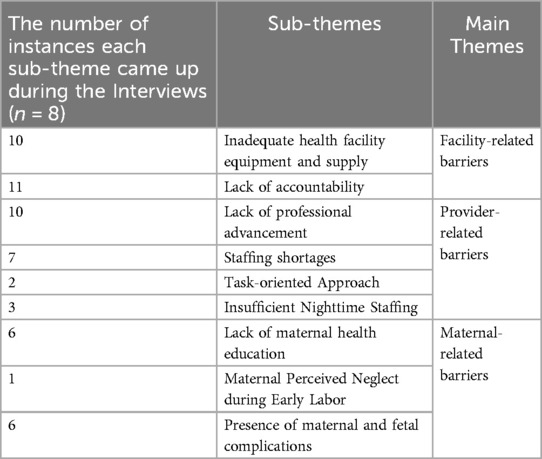
Table 7. The main themes and sub-themes emerged from key informants at public health institutions in Debre Tabor town, Northwest Ethiopia, 2024 (n = 8).
Main theme: facility-related barriers
This theme encompasses barriers within healthcare facilities that impede respectful maternity care. It includes deficiencies in facility resources and a lack of accountability practices that impact the quality of care.
Sub-theme: inadequate health facility equipment and supply
Inadequate or absence of essential medical equipment, and supplies, can severely impact the quality of care provided, increasing the risk of occupational hazards for healthcare providers and potentially leading to suboptimal or disrespectful treatment of patients.
“Health facilities were not always fully equipped with all necessary equipment, such as screens, and there was often a shortage of personal protective equipment, leading to a risk of exposure to blood splashes, which might, in turn, result in disrespectful care.” (KII7)
Sub-theme: lack of accountability
The absence or insufficiency of mechanisms and practices that ensure healthcare providers are held responsible for their actions and behaviors. This leads to disrespectful behaviors towards patients and escalating negative behaviors, as individuals may feel emboldened to act without fear of consequences.
“I believe that the lack of accountability is a pivotal factor contributing to disrespectful or hurtful behavior towards others. When individuals are not held accountable, the potential for the escalation of misconduct is significantly heightened.”(KII6)
Main themes: healthcare provider-related barriers
This theme encompasses barriers related to healthcare providers that impede the provision of respectful maternity care. These barriers stem from issues within the professional environment of healthcare providers, affecting their performance, satisfaction, and ability to deliver high-quality, respectful care to patients.
Sub-themes: lack of professional advancement
Insufficient opportunities for career growth, promotions, and continuing education for healthcare providers. When healthcare professionals are not recognized for their experience and dedication through promotions or opportunities to further their education, it can lead to dissatisfaction and demoralization. Over time, this can erode their passion for the profession and negatively affect their performance and commitment to patient care.
“Despite eight years of service, during which I have earned only 8,000 Birr, I have not received any promotions or educational opportunities. This lack of professional advancement has led to dissatisfaction, causing a gradual decline in my passion for the profession, consequently affecting the quality of service provided to mothers and resulting in a diminished level of dedication and commitment. It is imperative to address these underlying issues to ensure the provision of complete and comprehensive care to mothers.” (KII1)
“Certain service providers might lack adequate training, potentially resulting in the delivery of services that fall below the expected or desired quality.” (KII5)
Sub-themes: staffing shortages
When there are not enough midwife professionals to adequately cover all necessary responsibilities, the quality and safety of patient care can be compromised. This shortage of skilled staff can lead to increased workloads, burnout among existing professionals, and a decline in the standard of care provided.
“In this hospital, there are seven beds in the intrapartum ward, but only three midwife professionals are assigned. The remaining responsibilities are covered by students and university staff who may not possess the requisite expertise. This situation poses a significant challenge in ensuring the provision of respectful maternal health services.” (KII8)
Sub-themes: task-oriented approach
A focus on completing specific responsibilities and tasks, often with the primary goal of preventing complications, sometimes at the expense of considering broader ethical or moral implications. While this approach can be effective in preventing adverse outcomes, it may limit the scope for compassionate and individualized patient care, potentially leading to a more mechanistic and less empathetic healthcare environment.
“My emphasis lies in fulfilling my responsibilities; instead of dwelling on notions of right or wrong, our primary focus is to preemptively prevent any complications from arising.” (KII3)
Sub-theme: insufficient nighttime staffing
Inadequate number of healthcare professionals available during night shifts, where a limited number of staff must manage a high volume of patients, leading to significant strain and fatigue. This exhaustion can impede their respectful and thorough attention to each patient.
“I experience fatigue, particularly during nighttime, as the presence of only three midwives becomes challenging when faced with an average of ten to twelve mothers in need of delivery. This overwhelming situation hinders my ability to provide respectful care.” (KII2)
Main theme: maternal-related barriers
This theme encompasses aspects of maternal health, knowledge, and perception that impede the provision of respectful maternity care. These barriers stem from gaps in maternal education, perceived neglect during labor, and complications affecting maternal and fetal health, all of which impact the quality and experience of maternity care.
Sub-themes: lack of maternal health education
The gap in knowledge and understanding among expectant mothers regarding the natural processes of labor and childbirth often leads to a more negative experience and perception of the care received.
“In our community, many of our mothers are uneducated; they consider that they give birth as soon as they arrive at the hospital because they do not understand the natural process of labor.” (KII4)
Sub-themes: maternal perceived neglect during early labor
The feelings of abandonment and inadequate attention experienced by mothers in the initial stage of labor due to infrequent monitoring and interaction from healthcare providers lead to feelings of neglect and abandonment among early laboring mothers, leading to a negative perception of the care received.
“Mothers who are in the first stage of labor sometimes feel like they have not been treated well. After providing them with a bed and conducting an initial examination, we typically check on them every hour unless they have an obstetric issue. However, we tend to check on mothers who are co-sleeping every thirty minutes or every fifteen minutes, which can make the first stage of laboring mothers feel neglected. As a result, mothers in the first stage of labor may feel like they have been abandoned.” (KII4)
Sub-themes: presence of maternal and fetal complications
In the presence of maternal or fetal complications, healthcare providers are committed to preserving lives through any necessary means. Any complication affecting either the mother or newborn can present a substantial barrier to providing respectful delivery services.
“In certain situations, a patient's life or well-being might be at risk, necessitating decisive action even if it contradicts the patient's wishes. For instance, in the event of severe bleeding, immediate intervention may be required to save their life, even if the patient opposes such measures. Striking a delicate balance between respecting the client's autonomy and taking essential steps to safeguard their health is imperative in such critical scenarios.” (KII5)
Discussion
The proportion of respectful maternity care was 34.1%. This finding is consistent with studies conducted in Harar, 38.4%, and West Shewa, Ethiopia, 35.8% (15, 32). However, this finding is higher than studies conducted in Benishangul Gumuz Region (12.6%), Addis Ababa (24.6%), and Arba Minch town, Ethiopia (1.1%) (13, 36, 37). This might be due to variations in the study period, healthcare practices, and cultural norms within different regions or settings. Additionally, this disparity might be due to the exclusion of mothers who underwent emergency cesarean sections in a study carried out in Addis Ababa. However, this result is lower than that of research conducted in Tanzania (85%), India (71%), and Kenya (81%) (38–40). This might be variations in research periods, socioeconomic characteristics, and access to maternal and child health services because the quality of care is significantly affected when an institution's infrastructure, personnel, supplies, and equipment do not meet recognized standards of care (41) This study indicated that mothers who gave birth during the day were 3.14 times more likely to receive respectful maternity care than mothers who gave birth at night. This finding is consistent with studies conducted in Kenya, West Shewa, and Debre Birhan, Ethiopia (32, 40, 42). One reason for this discrepancy may be that healthcare providers offer more respectful care during the day when they are more likely to be supervised by senior staff and managers. Additionally, more staff members and better resources are often available during daytime hours. In contrast, mothers giving birth at night may experience less respectful care due to a smaller night-shift staff and the resulting heavier workload. Fatigue from disrupted sleep schedules may also contribute to these differences in care quality between day and night shifts.
This study identified that those mothers who gave birth by cesarean section were 3.45 times more likely to get respectful maternity care compared to those who gave birth by spontaneous vaginal delivery. This finding is consistent with studies conducted in the Hadiya zone, Ethiopia, and Rwanda (43, 44). This might be because mothers who gave birth through cesarean section might have received special attention and support from healthcare providers due to concerns regarding potential complications associated with the surgical procedure. This increased attention could lead to a more positive experience and perception of the care received. This finding contrasts with studies conducted in Bahirdar and Arba Minch, Ethiopia (17, 36). This might be explained by a study in Arbaminch town, Ethiopia, which excluded mothers who underwent elective cesarean sections. Furthermore, this discrepancy may be explained by differences in cultural norms and healthcare practices within different regions or settings.
The odds of receiving respectful maternity care were 3.03 times higher among mothers who stayed less than or equal to one day compared to those who stayed longer in health facilities. This finding is consistent with studies conducted in Tanzania, Bahirdar town, Ethiopia, and Nepal (33, 34, 45). This might be because mothers who stayed for a shorter period may have better continuity of care. With consistent support from healthcare providers throughout their stay, this continuity of care can contribute to a more positive experience and perception of respectful maternity care. This finding contrasts with a study conducted in West Shewa, Ethiopia (32). This might be due to differences in a study setting, staffing, and resources.
Strengths and limitations of the study
The strength of this study is the triangulation of quantitative with qualitative inquiry to get robust data in determining factors affecting RMC services Despite these strengths, the limitation of this study was the use of nurses as data collectors and interviews in hospital settings, which might introduce bias due to its sensitivity nature of the study.
Conclusions
As per this study, the proportion of respectful maternity care in public health facilities in Debre Tabor town was low. Factors such as giving birth in the daytime, cesarean delivery, and less than or equal to 1 day stay in a healthcare facility were positively associated with RMC. Additionally; Inadequate equipment and supplies, lack of accountability mechanisms, lack of professional advancement, Health care provider shortages, Task-oriented Approach, lack of maternal Health education, Maternal Perceived Neglect during early labor, and the presence of maternal and fetal complications were barriers to the provision of respectful maternity care service. Therefore, health institutions and other stakeholders should support and reinforce monitoring and evaluation mechanisms for MNHC providers and enhance education and constant support for women during their pregnancy and childbirth. Additionally, access to basic equipment and supplies should be given due attention to ensure respectful maternity care.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/Supplementary Material.
Ethics statement
The studies involving humans were approved by Ethical review committee of the School of Midwifery on behalf of the Internal Review Board of the University of Gondar, College of Medicine and Health Sciences (Ethical approval number Mid/W.H/28/2016). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
TF: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. AS: Conceptualization, Methodology, Software, Writing – original draft, Writing – review & editing. ME: Conceptualization, Methodology, Software, Writing – original draft, Writing – review & editing. MB: Conceptualization, Methodology, Software, Writing – original draft, Writing – review & editing. AM: Conceptualization, Methodology, Software, Writing – original draft, Writing – review & editing. AB: Conceptualization, Methodology, Software, Writing – original draft, Writing – review & editing. GA: Conceptualization, Methodology, Software, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
The authors would like to thank all data collectors, study participants, and staff for their willingness to give their time and information for this study.
Conflict of interest
The authors declare that the research was conducted without any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fgwh.2025.1513906/full#supplementary-material
Abbreviations
AIDS, acquired immune deficiency syndrome; ANC, antenatal care; AOR, adjusted odd ratio; BSc, Bachelor of science; CI, confidence interval; COR, crude odd ratio; CRC, compassionate and respectful care; D or A, disrespect or abuse; E.C., Ethiopian calendar; ETB, Ethiopian birr; FMOH, federal ministry of health; HIV, human immunodeficiency virus; HC, health center; MCHIP, maternal and child health integrated program; MNH, maternal and newborn health; RMC, respectful maternity care; SPSS, statistical package for social science.
References
2. Bohren MA, Vogel JP, Hunter EC, Lutsiv O, Makh SK, Souza JP, et al. The mistreatment of women during childbirth in health facilities globally: a mixed-methods systematic review. PLoS Med. (2015) 12(6):e1001847. doi: 10.1371/journal.pmed.1001847
3. Reis V, Deller B, Catherine Carr C, Smith J. Respectful Maternity Care. Washington DC: USAID (2012).
4. Windau-Melmer T. A guide for advocating for respectful maternity care. Washington, DC: Futures Group. Health Policy Proj. (2013) 1:1–8.
5. Lukasse M, Schroll AM, Karro H, Schei B, Steingrimsdottir T, Van Parys AS, et al. Prevalence of experienced abuse in healthcare and associated obstetric characteristics in six European countries. Acta Obstet Gynecol Scand. (2015) 94(5):508–17. doi: 10.1111/aogs.12593
6. Castro R, Frías SM. Obstetric violence in Mexico: results from a 2016 national household survey. Violence Against Women. (2020) 26(6–7):555–72. doi: 10.1177/1077801219836732
7. Ansari H, Yeravdekar R. Respectful maternity care during childbirth in India: a systematic review and meta-analysis. J Postgrad Med. (2020) 66(3):133–40. doi: 10.4103/jpgm.JPGM_648_19
8. Rosen HE, Lynam PF, Carr C, Reis V, Ricca J, Bazant ES, et al. Direct observation of respectful maternity care in five countries: a cross-sectional study of health facilities in east and Southern Africa. BMC Pregnancy Childbirth. (2015) 15:1–11. doi: 10.1186/s12884-015-0728-4
9. Gebeyehu NA, Adella GA, Tegegne KD. Disrespect and abuse of women during childbirth at health facilities in Eastern Africa: systematic review and meta-analysis. Front Med (Lausanne). (2023) 10:1117116. doi: 10.3389/fmed.2023.1117116
10. Kassa ZY, Tsegaye B, Abeje A. Disrespect and abuse of women during the process of childbirth at health facilities in Sub-Saharan Africa: a systematic review and meta-analysis. BMC Int Health Hum Rights. (2020) 20:1–9. doi: 10.1186/s12914-020-00242-y
11. Melkamu E, Tesfaye G, Yetwale A. Provision of respectful maternity care during labor and delivery and associated factors among postnatal mothers at Jimma university medical center, Jimma, South West Ethiopia, 2021. Int J Childbirth. (2021) 11(4):166–77. doi: 10.1891/IJCBIRTH-D-21-00013
12. Adane D, Bante A, Wassihun B. Respectful focused antenatal care and associated factors among pregnant women who visit Shashemene town public hospitals, Oromia region, Ethiopia: a cross-sectional study. BMC Women’s Health. (2021) 21:1–8. doi: 10.1186/s12905-021-01237-0
13. Amsalu B, Aragaw A, Sintayehu Y, Sema A, Belay Y, Tadese G, et al. Respectful maternity care among laboring women in public hospitals of Benishangul Gumuz region, Ethiopia: a mixed cross-sectional study with direct observations. SAGE Open Med. (2022) 10:20503121221076995. doi: 10.1177/20503121221076995
14. Asefa A, Bekele D. Status of respectful and non-abusive care during facility-based childbirth in a hospital and health centers in Addis Ababa, Ethiopia. Reprod Health. (2015) 12:1–9. doi: 10.1186/s12978-015-0024-9
15. Bante A, Teji K, Seyoum B, Mersha A. Respectful maternity care and associated factors among women who delivered at Harar hospitals, eastern Ethiopia: a cross-sectional study. BMC Pregnancy Childbirth. (2020) 20:1–9. doi: 10.1186/s12884-020-2757-x
16. Tarekegne AA, Giru BW, Mekonnen B. Person-centered maternity care during childbirth and associated factors at selected public hospitals in Addis Ababa, Ethiopia, 2021: a cross-sectional study. Reprod Health. (2022) 19(1):199. doi: 10.1186/s12978-022-01503-w
17. Wassihun B, Zeleke S. Compassionate and respectful maternity care during facility based child birth and women’s intent to use maternity service in Bahir Dar, Ethiopia. BMC Pregnancy Childbirth. (2018) 18:1–9. doi: 10.1186/s12884-018-1909-8
18. Wochefu B, Abdo A, Koboto D. Compassionate and respectful maternity care and associated factors among women attending delivery services at public health facilities of Hawassa city, southern Ethiopia. Int Arch Nurs Health Care. (2021) 7:165. doi: 10.23937/2469-5823/1510165
19. Yalew M, Nigatu D, Yasin T, Kefale B, Damtie Y. Respectful delivery care and associated factors among mothers delivered in public health facilities of Dessie city, Northeast Ethiopia: a cross-sectional study. BMC Women’s Health. (2022) 22(1):127. doi: 10.1186/s12905-022-01713-1
20. Yismaw WS, Teklu TS, Panduragman H. Respectful maternity care during facility-based child birth and associated factors in public health facilities of Ilu AbaBor zone, Southwest Ethiopia. Reprod Health. (2022) 19(1):98. doi: 10.1186/s12978-022-01368-z
21. Yosef A, Kebede A, Worku N. Respectful maternity care and associated factors among women who attended delivery services in referral hospitals in Northwest Amhara, Ethiopia: a cross-sectional study. J Multidiscip Healthc. (2020) 13:1965–73. doi: 10.2147/JMDH.S286458
22. Mgawadere F, Shuaibu U. Enablers and barriers to respectful maternity care in low and middle-income countries: a literature review of qualitative research. Int J Clin Med. (2021) 12(5):224–49. doi: 10.4236/ijcm.2021.125021
23. Ethiopian Public Health Institute (EPHI) [Ethiopia] and ICF. Ethiopia Mini Demographic and Health Survey 2019: Final Report. Rockville, MD: EPHI and ICF (2021).
24. Bohren MA, Hunter EC, Munthe-Kaas HM, Souza JP, Vogel JP, Gülmezoglu AM. Facilitators and barriers to facility-based delivery in low-and middle-income countries: a qualitative evidence synthesis. Reprod Health. (2014) 11:1–17. doi: 10.1186/1742-4755-11-71
25. Shiferaw S, Spigt M, Godefrooij M, Melkamu Y, Tekie M. Why do women prefer home births in Ethiopia? BMC Pregnancy Childbirth. (2013) 13:1–10. doi: 10.1186/1471-2393-13-5
26. Bowser D, Hill K. Exploring evidence for disrespect and abuse in facility-based childbirth: report of a landscape analysis. USAID-Traction project. (2010).
27. Aragaw TJ, Afework DT, Getahun KA. Assessment of knowledge, attitude, and utilization of traditional medicine among the communities of Debre Tabor town, Amhara regional state, North Central Ethiopia: a cross-sectional study. Evid-Based Complement Altern Med. (2020) 2020:6565131. doi: 10.1155/2020/6565131
28. Bezie M, Biru S. Prevalence and its associated factors of episiotomy practice among mothers who gave birth in Debre Tabor town Northwest Ethiopia: an institutional based-cross-sectional study. Matern Child Health J. (2023) 27(5):873–7. doi: 10.1007/s10995-023-03603-w
29. Ayele AD, Tilahun ZA. Determinants of pre-eclampsia among women attending delivery services in public health institutions of Debre Tabor town: a case–control study. Reprod Health. (2022) 19(1):1–8. doi: 10.1186/s12978-021-01314-5
30. Sheferaw ED, Bazant E, Gibson H, Fenta HB, Ayalew F, Belay TB, et al. Respectful maternity care in Ethiopian public health facilities. Reprod Health. (2017) 14(1):1–12. doi: 10.1186/s12978-017-0323-4
31. Kebede AA, Taye BT, Wondie KY, Tiguh AE, Eriku GA, Mihret MS. Adherence to respectful maternity care guidelines during COVID-19 pandemic and associated factors among healthcare providers working at hospitals in Northwest Ethiopia: a multicenter, observational study. Clin Epidemiol Glob Health. (2021) 12:100830. doi: 10.1016/j.cegh.2021.100830
32. Bulto GA, Demissie DB, Tulu AS. Respectful maternity care during labor and childbirth and associated factors among women who gave birth at health institutions in the West Shewa zone, oromia region, central Ethiopia. BMC Pregnancy Childbirth. (2020) 20:1–12. doi: 10.1186/s12884-019-2665-0
33. Wassihun B, Deribe L, Worede N, Gultie T. Prevalence of disrespect and abuse of women during child birth and associated factors in Bahir Dar town, Ethiopia. Epidemiol Health. (2018) 40:e2018029. doi: 10.4178/epih.e2018029
34. Kruk ME, Kujawski S, Mbaruku G, Ramsey K, Moyo W, Freedman LP. Disrespectful and abusive treatment during facility delivery in Tanzania: a facility and community survey. Health Policy Plan. (2018) 33(1):e26–33. doi: 10.1093/heapol/czu079
35. Sheferaw ED, Mengesha TZ, Wase SB. Development of a tool to measure women’s perception of respectful maternity care in public health facilities. BMC Pregnancy Childbirth. (2016) 16:1–8. doi: 10.1186/s12884-016-0848-5
36. Ukke GG, Gurara MK, Boynito WG. Disrespect and abuse of women during childbirth in public health facilities in Arba Minch town, south Ethiopia–a cross-sectional study. PLoS One. (2019) 14(4):e0205545. doi: 10.1371/journal.pone.0205545
37. Abebe AH, Mmusi-Phetoe R. Respectful maternity care in health centers of Addis Ababa city: a mixed method study. BMC Pregnancy Childbirth. (2022) 22(1):792. doi: 10.1186/s12884-022-05129-5
38. Bhattacharya S, Sundari Ravindran T. Silent voices: institutional disrespect and abuse during delivery among women of Varanasi district, northern India. BMC Pregnancy Childbirth. (2018) 18:1–8. doi: 10.1186/s12884-018-1970-3
39. Sando D, Ratcliffe H, McDonald K, Spiegelman D, Lyatuu G, Mwanyika-Sando M, et al. The prevalence of disrespect and abuse during facility-based childbirth in urban Tanzania. BMC Pregnancy Childbirth. (2016) 16:1–10. doi: 10.1186/s12884-016-1019-4
40. Abuya T, Ndwiga C, Ritter J, Kanya L, Bellows B, Binkin N, et al. The effect of a multi-component intervention on disrespect and abuse during childbirth in Kenya. BMC Pregnancy Childbirth. (2015) 15:1–14. doi: 10.1186/s12884-015-0645-6
41. Freedman LP, Kruk ME. Disrespect and abuse of women in childbirth: challenging the global quality and accountability agendas. Lancet. (2014) 384(9948):e42–4. doi: 10.1016/S0140-6736(14)60859-X
42. Wubetu YA, Sharew NT, Mohammed OY. Respectful Delivery Care and Associated Factors in Public Health Facilities in Debre Berhan Town, Ethiopia. (2021).
43. Mengistie T, Mulatu T, Alemayehu A, Dheresa M. Respectful maternity care among women who gave birth at public hospitals in Hadiya Zone, Southern Ethiopia. Front Public Health. (2022) 10:949943. doi: 10.3389/fpubh.2022.949943
44. Muhayimana A, Kearns I, Darius G, Olive T, Thierry UC. Reported respectful maternity care received during childbirth at health facilities: a cross sectional survey in Eastern province, Rwanda. Midwifery. (2024) 133:103996. doi: 10.1016/j.midw.2024.103996
Keywords: respectful care, maternity care, health facilities, Debre Tabor town, Ethiopia
Citation: Fentie TA, Solomon AA, Enyew MM, Beyene MM, Melese AK, Belay AE and Alemu GG (2025) Respectful maternity care and associated factors among mothers who gave birth at public health institutions in Debre Tabor town, Northwest Ethiopia: a mixed-methods study. Front. Glob. Womens Health 6:1513906. doi: 10.3389/fgwh.2025.1513906
Received: 18 November 2024; Accepted: 9 January 2025;
Published: 23 January 2025.
Edited by:
David Ramiro-Cortijo, Autonomous University of Madrid, SpainReviewed by:
Projestine Selestine Muganyizi, University of Dar es Salaam, TanzaniaClaudia Susana Silva Fernández, Autonomous University of Madrid, Spain
Copyright: © 2025 Fentie, Solomon, Enyew, Beyene, Melese, Belay and Alemu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tadesse Ayana Fentie, dGFkZXNzZWF5YW5hMkBnbWFpbC5jb20=