 Endalkachew Dellie1*†
Endalkachew Dellie1*† Misganaw Guadie Tiruneh1
Misganaw Guadie Tiruneh1 Melak Jejaw1
Melak Jejaw1 Kaleb Assegid Demissie1
Kaleb Assegid Demissie1 Mihret Getnet2
Mihret Getnet2 Tadele Biresaw Belachew1
Tadele Biresaw Belachew1 Getachew Teshale1
Getachew Teshale1 Banchlay Addis1
Banchlay Addis1 Demiss Mulatu Geberu1
Demiss Mulatu Geberu1 Lake Yazachew1
Lake Yazachew1 Tesfahun Zemene Tafere1
Tesfahun Zemene Tafere1 Nigusu Worku1,†
Nigusu Worku1,†
- 1Department of Health Systems and Policy, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
- 2Department of Epidemiology and Biostatics, Institute of Public Health, University of Gondar, Gondar, Ethiopia
Background: Women's empowerment has been a global priority, as countries can achieve significant growth and economic development by empowering women. Understanding the individual and community-level factors that influence women's empowerment is crucial for policymakers to develop effective policies and to improve women's empowerment.
Method: A community-based cross-sectional survey was conducted in 11 administrative regions of Ethiopia. The analysis included a weighted sample of 7,108 married women of reproductive age (15–49 years) from the 2,016 Ethiopian Demographic and Health Survey (EDHS). A multilevel mixed-effect binary logistic regression analysis was used to examine the individual and community-level factors associated with women's empowerment. In the final model, significant variables were identified using a p-value of <0.05 and an adjusted odds ratio (AOR) with a 95% confidence interval (CI).
Results: The overall magnitude of women's empowerment was 23.7% (95% CI: 22.7–24.7). Only 30.9% of women reported participating in household decision-making, and 32.5% disagreed with all the reasons justifying wife-beating. At individual-level, factors positively associated with women's empowerment included secondary (AOR: 2.72 (1.77–4.23), and higher (AOR: 3.65 (1.81–7.34) education. However, belonging to the Muslim religion was negatively associated with women's empowerment (AOR: 0.63 (0.47–0.85). At the community level, wealthy communities were positively associated with women's empowerment (AOR: 1.60 (1.05–2.44). Conversely, residing in rural areas (AOR: 0.49 (0.29–0.83), and living in the Afar (AOR: 0.35 (0.17–0.70), Amhara (AOR: 0.45 (0.26–0.79), Oromia (AOR: 0.43 (0.26–0.73), South Nation Nationalities, and Peoples (SNNP) (AOR: 0.42 (0.24–0.75), and Gambella (AOR: 0.36 (0.20–0.66) regional states were negatively associated with women's empowerment.
Conclusion: The overall magnitude of women's empowerment in this study was low. Factors that positively influenced empowerment included attending secondary and higher education, as well as residing in communities with higher wealth status. On the other hand, being Muslim, residing in rural areas, and living in the Afar, Amhara, Oromia, SNNPR, Gambella, and Tigray regions were negatively associated with women's empowerment. As a result, the government of Ethiopia needs to design community-based women's empowerment strategies and involve women in income-generation activities that improve their participation in household decision-making to empower them.
Introduction
Women's empowerment is a fundamental driver of sustainable development and is a global priority agenda, especially in developing countries where gender disparities are often pronounced (1). It was one of the Millennium Development Goals (MDGs) and remains central to achieving the Sustainable Development Goals (SDGs (2, 3). Despite numerous efforts to promote gender equality, many women still face significant barriers to accessing education, economic opportunities, and healthcare services (4–7).
Women's empowerment is relatively a complex and multidimensional concept that centers on enhancing women's capacity to make strategic life choices, especially in situations where such opportunities have been denied to them (8, 9). Due to its multifaceted nature, objectively measuring women's empowerment poses challenges for researchers. This study assessed women's empowerment using index-based data from the nationally representative 2016 Ethiopian Demographic and Health Survey (EDHS), in terms of decision-making power and attitudes toward the justification of wife-beating.
Women's empowerment is a significant component of the development process. Economically independent and educated women are more likely to seek and utilize healthcare services, leading to better health outcomes for themselves and their families (5). Research conducted in 67 developing countries has shown a positive association between women's empowerment and the use of health services (10). For example, women with higher levels of empowerment are more likely to use reproductive health services, such as family planning, antenatal care, and skilled attended delivery (11, 12). Therefore, it is clear that women's empowerment is essential for promoting the well-being of households and children. Additionally, various studies worldwide have identified several factors contributing to women's empowerment, including women's education, age, media access, employment, place of residence, and income level (13–17).
The Ethiopian government has implemented various institutional and policy measures to promote gender equality and empower women. These efforts include the 1993 Ethiopian Constitution (18), the Ethiopian National Policy on Women (19), and the Growth and Transformation Plan (GTP) I and II (20, 21). Despite these measures, gaps in women's empowerment persist. For instance, a significant proportion of women still lack decision-making power in key areas; such as household purchases (21%), healthcare decisions (18%), and visits to their family or relatives (16%). Additionally, a considerable number of women (63%) disapprove of wife-beating for any reason (22). These evidences highlight the persistent challenges in achieving true gender equality in Ethiopia.
Furthermore, a study based on data from the Ethiopian Demographic and Health Survey (EDHS) conducted in 2011 found that about half of the women surveyed disagreed with wife-beating (23). However, this study only measured women's attitudes towards wife-beating and did not thoroughly analyze the individual and community-level factors influencing women's empowerment. Moreover, the previous studies used binary logistic regression, which did not comprehensively analyze both community-level and individual-level factors, potentially overlooking the issue of non-independence.
Understanding individual and community-level factors that are likely to influence women's empowerment may be a commencement in exploring strategies to empower women and cut back on gender inequality. Therefore, this study tried to examine the magnitude of women's empowerment and identify its determinants using a multilevel model, from the 2016 EDHS data.
Methods
Study settings and period
Ethiopia is located in the Horn of Africa and shares borders with Eritrea, Djibouti, Somalia, Sudan, South Sudan, and Kenya. It is the second most populous nation on the African continent after Nigeria, with a population of 109,224,559 (24). Ethiopia is divided into nine geographical regions [Afar, Amhara, Benishangul-Gumuz, Gambela, Harari, Oromia, Somali, Southern Nations, Nationalities, and People's Region (SNNPR), and Tigray] and two administrative cities (Addis Ababa and Dire Dawa). The majority of the Ethiopian population is an agrarian society, and about 83.6% live in rural areas. Agriculture accounts for approximately 43% of the country's Gross Domestic Product (GDP), and over 80% of the total population resides in the regional states of Amhara, Oromia, and SNNP (25).
In Ethiopia, the majority of the population (83.6%) lives in rural areas, and the average household size is 4.7 persons. The population is predominantly young, with more than one-third (44%) being under 15 years old, over half (52%) being between 15 and 65 years old, and only a few (3%) of all persons being over the age of 65 years. Women of reproductive age constitute 24% of the population (26, 27).
The study utilized data from the 2016 Ethiopia Demographic and Health Survey (EDHS), which is a nationally representative survey conducted every five years. Data collection was organized by the Central Statistical Agency (CSA) of Ethiopia (22) and conducted from January 18, 2016, to June 27, 2016. The study participants were women of reproductive age (15–49) who reside permanently in the selected households or stayed the night before the survey in the household (22).
Study design, data source, and sampling procedures
A cross-sectional survey was conducted in eleven administrative regions of Ethiopia using data from the 2016 EDHS datasets, which were led by the Ethiopian Central Statistical Agency (CSA). The EDHS aims to provide valuable information on key demographic and health indicators such as fertility, family planning, infant and child mortality, maternal and child health, and nutrition in the national and sub-national areas of Ethiopia. To date, four rounds of the EDHS have been collected using similar procedures.
The survey utilized a two-stage stratified cluster sampling design. In this design, enumeration areas (EAs) or clusters (defined geographical units) were used as the primary units of data collection. These EAs were stratified based region and urban-rural residency. Each region was divided into urban and rural areas to ensure proper stratification. A total of twenty-one (21) sampling strata were created, representing the urban and rural areas in each of the nine regions and two city administrations. In the first stage of sampling, 645 EAs were randomly chosen from these strata: 202 from urban areas and 443 from rural areas. Independent selection was utilized in each sampling stratum, based on probability proportion. In the second stage, a systematic random sampling technique was used to select 28 households per EAs/cluster, ensuring equal probability (22).
For this study, the women's dataset was used. This dataset included a total of 15,683 women aged 15–49 years old from 16,650 households within 645 clusters. After weighting the sample, 7,108 currently married women were included in the final analysis. Furthermore, potential independent variables at both the individual and community levels were extracted for further analysis.
Measurements of variables
This study examines women's empowerment as the dependent variable measured using index-based data from two key dimensions of the 2016 EDHS: decision-making power and attitudes toward the justification of wife-beating. These dimensions were chosen based on the availability of data from the 2016 Ethiopian Demographic and Health Survey (EDHS) and alignment with existing literature. To assess decision-making power, three questions were asked about women's involvement in decisions regarding their own healthcare, household purchases, and visits to family or relatives. Women's responses were categorized based on whether they made these decisions alone or jointly with their husbands. For the justification of wife-beating, respondents were asked five questions to determine whether they believed a man was justified in beating his wife under certain circumstances, such as burning food, arguing with her husband, going out without informing him, refusing sexual intercourse, and neglecting the children.
Responses to these empowerment indicators were then categorized as either empowered (scored as 1) or unempowered (scored as 0). These scores were then summed to create a composite women's empowerment score. A sum score ranging from 0 to 7 was classified as unempowered, while a score of 8 was classified as empowered. Thus, women were considered empowered if they participated in all decision-making instances either alone or jointly with their husbands, and never justified wife-beating (28). The relevant questions regarding women's participation in household decision-making and their attitudes toward wife-beating can be found in DHS Module 9 within questions 922–932 (29).
The independent variables for this study were categorized as individual, household, and community-level factors. Individual and household-level factors included sociodemographic and economic variables. On the other hand, community-level factors consisted of place of residence, region, community poverty level, and community-level media exposure.
To measure community-level media exposure, we used the proportion of women exposed to specific media as an aggregate value. Mothers’ exposure to mass media was then categorized as no exposure, less than once a week, and greater than once a week.
Data processing and statistical analysis
The outcome variables with important predictors were extracted from the 2016 EDHS women's dataset and editing, recoding, and analysis were done using STATA 14. Descriptive statistics such as frequencies and proportions of variables were presented using tables and narrations.
Bivariable logistic and multilevel regression models were used to analyze factors associated with women's empowerment at two levels: individual and community. To capture the impact of cluster and individual-level factors on women's empowerment, a multilevel regression model that accounts for variation at these levels was used (30). Likelihood ratio, Intra-Class Correlation (ICC), and Proportional Change in Variance (PCV) were computed to measure the variation between clusters, and model comparison was conducted using deviances. The ICC coefficient quantifies the degree of heterogeneity of women's empowerment between clusters, ICC = ϭ2/(ϭ2 + π2/3) (31), with ϭ2 indicating cluster variance. PCV measures the total variation attributed to individual and community-level factors in the multilevel model compared to the null model; .
A two-level (individual and community), multilevel multivariable logistic regression analysis was used to explore factors related to women's empowerment. Furthermore, four models were created for the analysis. The first model had no variables and was used to determine the extent of cluster variation in women's empowerment. The second model included individual-level variables, the third model included community-level variables, and the fourth model included both individual and community-level variables. The model with the lowest deviance was chosen. Variables with a p-value of <0.2 in the bivariate analysis for both individual and community-level factors were included in the multivariable model. An adjusted odds ratio (AOR) with a 95% confidence interval (CI) and a p-value of <0.05 in the multivariable model indicated a significant association between the independent variables and women's empowerment.
Results
Individual and community-level sociodemographic and economic characteristics
A total of 7,108 women were included in the final analysis. The mean ages of the respondents were 29.3 (SD ± 6.8) years. The majority (87.6%) were rural dwellers, 41.1% were from the Oromia region and 37.4% of the participants were Muslim. Moreover, 63.4% and 56.1% of the women had no education and were not employed, respectively. Similarly, 47.7% and 64.8% of their husbands had no education and worked in agriculture, respectively. Additionally, 88.8% of the household heads were male, 42.2% of the participants were in poor wealth status, had no access to media (65.31%), and had four or more living children (48%) (Table 1).
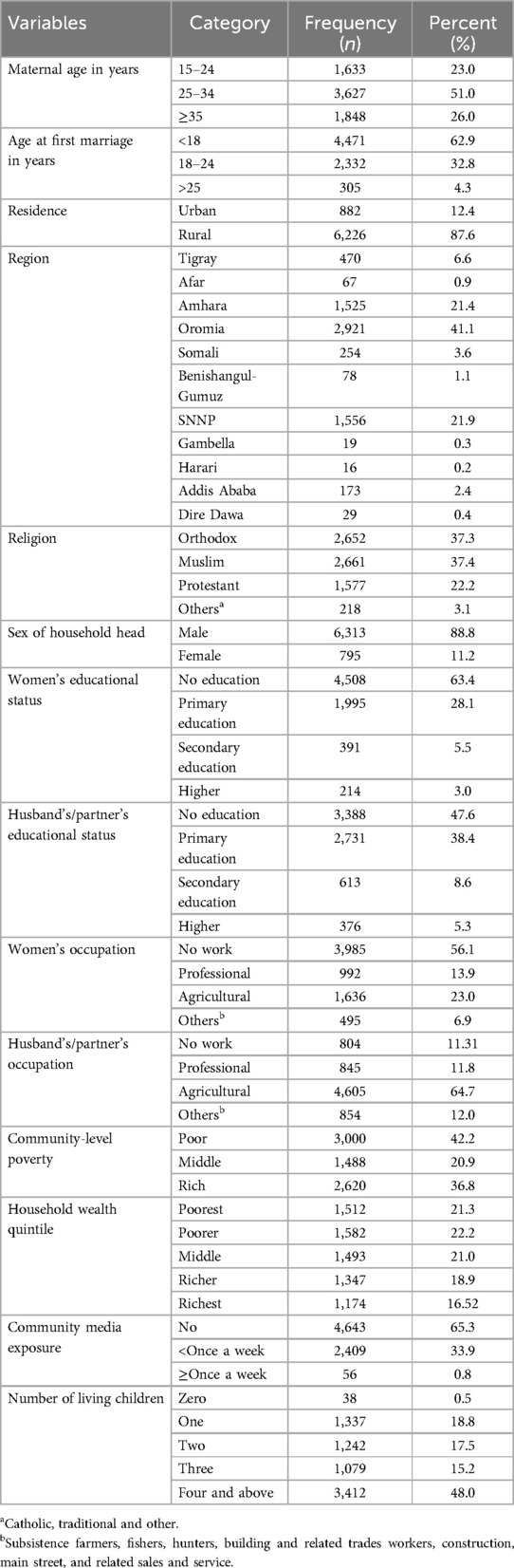
Table 1. Individual and community-level sociodemographic and economic characteristics of study participants in Ethiopia, EDHS 2016 (n = 7,108).
The magnitude of women's empowerment
In this study, the overall magnitude of women's empowerment was 23.7% (95% CI: 22.7–24.7). Specifically, only 30.9% of women were involved in household decision-making, either alone or jointly with their husbands. The lowest level of women's decision-making power was seen in decisions regarding visits to family or relatives, with only 17.2% of women participating. Another aspect of women's empowerment was their attitude toward wife-beating, with 32.5% of women disagreeing with all justifications for it. Among these women, the highest level of empowerment was observed in cases where husbands beat their wives for refusing sexual intercourse (59.9%) (Table 2).
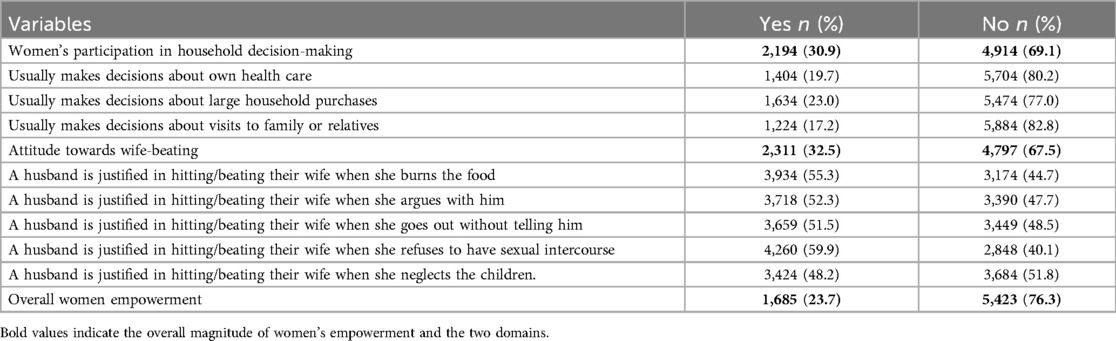
Table 2. Magnitude of women's empowerment with their respective domain in Ethiopia, EDHS 2016 (n = 7,108).
The overall magnitude of women's empowerment varied significantly across different regions of the country. The lowest level of women's empowerment was observed in the Afar region (16.6%), while the highest was seen in Addis Ababa (69.3%) (Table 3).
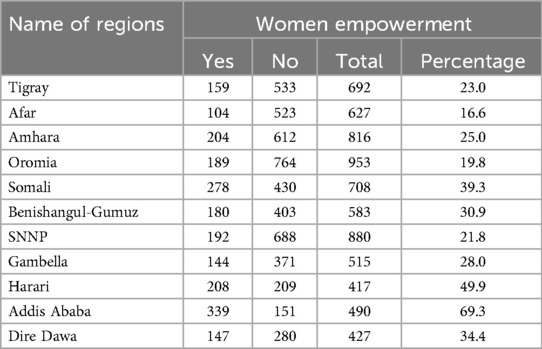
Table 3. The magnitude of women's empowerment across regions in Ethiopia, EDHS, 2016.
Individual and community-level determinants for women empowerment
Random effect analysis
The ICC in the empty model indicated that 24.4% of the total variability of women empowerment was due to cluster differences, while the remaining unexplained 75.6% was attributable to individual differences. Fifty-three percent of the variability in women's empowerment was explained by the full model and deviance was used for model comparison. As a result, the final model was the best-fitted model since it had the lowest deviance (Table 4).
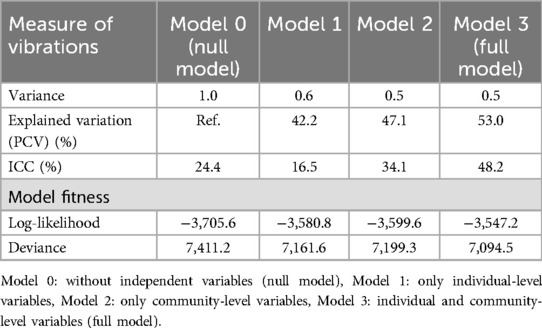
Table 4. A random intercept model (variations) for women empowerment at cluster level by multilevel logistic regression analysis, EDHS 2016.
Fixed effects analysis
A multilevel mixed-effects binary logistic regression analysis was conducted to identify potential individual and community-level determinants of women's empowerment. In the final model (model 3), individual-level factors such as women's educational status and religion, as well as community-level variables including place of residence, region, and community wealth status, were found to be significantly associated with women's empowerment.
Accordingly, Women who attended secondary and higher education were 2.7 times (AOR: 2.7, 95% CI: 1.8–4.2) and 3.6 times (AOR: 3.6, 95% CI: 1.8–7.3) more likely to be empowered compared to those who were not educated, respectively. Additionally, Muslim women were 37% less likely to be empowered compared to Orthodox Christian women (AOR: 0.6, 95% CI: 0.5–0.8).
Women living in rural areas were 51% less likely to be empowered compared to their urban counterparts (AOR: 0.49, 95% CI: 0.3–0.8). The odds of women's empowerment in the Afar, Amhara, Oromia, SNNPR, and Gambella regions were lower by 65% (AOR: 0.35, 95% CI: 0.2–0.7), 55% (AOR: 0.45, 95% CI: 0.3–0.8), 57% (AOR: 0.43, 95% CI: 0.3–0.7), 58% (AOR: 0.42, 95% CI: 0.2–0.7), 64% (AOR: 0.36, 95% CI: 0.2–0.6), and 68% (AOR: 0.32, 95% CI: 0.2–0.5), respectively, compared to women living in Addis Ababa. Moreover, women who live in wealthy communities had a 1.6 times higher chance of empowerment compared to women from poor communities (AOR: 1.6, 95% CI: 1.1–2.4) (Table 5).
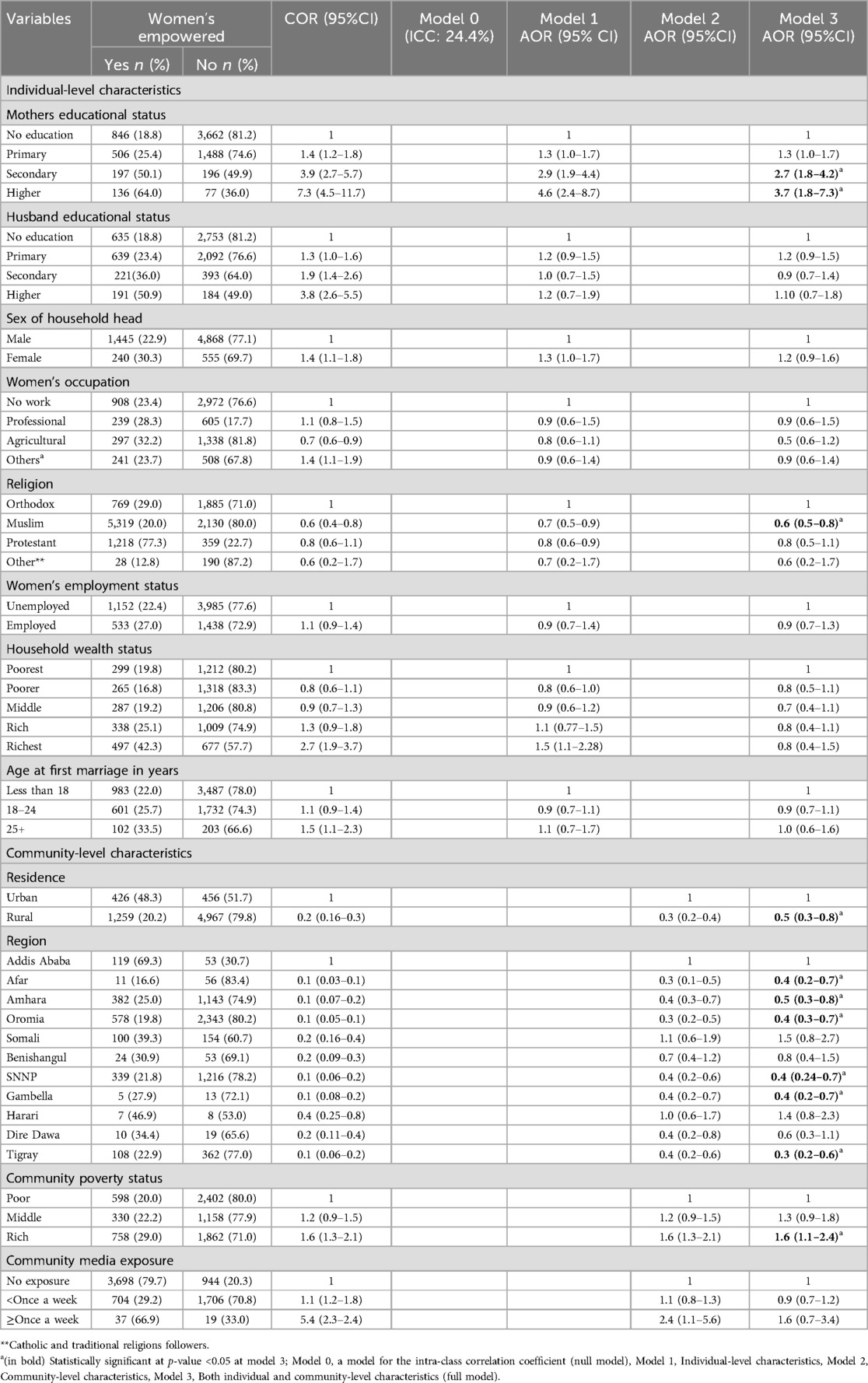
Table 5. Multilevel logistic regression analysis of individual and community-level factors associated with women's empowerment in Ethiopia, EDHS 2016 (n = 7,108).
Discussion
The overall magnitude of women's empowerment in Ethiopia was found to be 23.7% (95% CI: 22.7–24.7), with 30.9% of women participating in household decision-making. Specifically, only 19.75% of women were involved in decisions regarding their healthcare. This finding was unexpectedly lower than a previous study using EDHS 2005 data, which showed that 29.3% of women had a say in their healthcare needs (32). The possible reason for the discrepancy might be due to the donor-driven nature of maternal and child healthcare programs, which may lack sustainability after the termination of funding, the reduced functionality of women's associations, and the poor involvement of husbands in maternal and child health decisions. Furthermore, it is possible that in 2016, women were more willing to express the limitations they faced in decision-making due to increased awareness of gender issues. This awareness could have led to more honest reporting compared to 2005, when they might not have openly acknowledged these constraints.
However, our results were significantly lower than a study in Bangladesh, where nearly 45% of women participated in healthcare decisions, large household purchases, and family visits (33). Similarly, our findings were lower than those in Pakistan and India. In Pakistan, 36.6% of women were involved in household decision-making (34), while in North India, 53% participated in major household decisions (35). In Nepal, 72% of women were involved in decisions regarding household purchases (36).
Moreover, our finding is also slightly lower compared to other African countries. For instance, approximately 37% of women participated in at least one household decision in Mali (37) and 35.9% in the Democratic Republic of the Congo (DRC) (38). The possible reason for the discrepancy might be measurement and study setting differences, in this study women's participation in decision-making was measured by considering the composite value of decision-making indicators like decision-making on health care, household purchases, and a family visit whereas empowerment in India was measured in terms of women's autonomy, which is slightly different. Additionally, the study settings might contribute to discrepancies. Gender equality and women's participation in many aspects are higher in developing countries like Bangladesh, Nepal, and Pakistan compared to Ethiopia. However, in Ethiopia, women's participation remains a significant public health policy concern.
This study showed that educational status significantly impacts women's empowerment, with respondents who had completed primary education or higher being more empowered than those with no formal education. This result aligns with studies conducted in southern Ethiopia (39) and other African countries, where higher educational attainment is linked to increased empowerment for women (40–44). Similarly, studies from different Asian countries highlight education as a significant factor in positively influencing women's empowerment (33, 34, 41, 45–51). This might be due to the fact that education increases individuals’ awareness and enhances self-esteem. When women become more educated, they become more informed about their rights and are more likely to advocate for and uphold these rights (52). This finding is also supported by the Human Capabilities Theory by Martha Nussbaum and Amartya Sen, which emphasizes the role of education in expanding individual capabilities, fostering autonomy, and promoting overall empowerment and well-being (53, 54).
Besides, the findings of this study revealed a significant association between residency and women's empowerment. Respondents from rural areas were less empowered compared to those from urban settings. This finding is consistent with studies from various African and Asian countries, indicating that women in urban areas experience higher levels of empowerment than their rural counterparts (17, 44, 55, 56). This disparity may be attributed to limited access to information on women's rights and autonomy among women living in rural settings. Additionally, awareness levels within rural communities regarding women's rights and autonomy tend to be lower compared to urban areas.
Participants who identify as Muslim exhibit lower levels of empowerment compared to their Christian counterparts. Research conducted in Africa on the impact of religion on the Millennium Development Goals has similarly shown that being Muslim is associated with lower female school participation rates, less non-agricultural employment among women, and lower representation of women in government (57). Other studies also highlighted that gender inequality tends to be more pronounced among Muslims and Hindus compared to Christians and Buddhists (58, 59). This disparity may stem from cultural challenges in reconciling religious values with traditional beliefs and practices. Gender inequality often persists due to cultural norms and interpretations of religious teachings, which are prevalent in Muslim societies.
The level of community poverty significantly influences women's empowerment. Women residing in the wealthy communities exhibit higher levels of empowerment compared to those in poorer communities. It is well known that poverty constrains women's self-determination and limits their participation in economic, social, and political spheres. It is widely recognized that poverty is a fundamental driver of gender inequality, which hinders women's economic and social empowerment (60, 61). Moreover, women and girls living in poverty are more vulnerable to sexual exploitation due to their lack of income and resources (62–64).
In this study, the geographical region where women reside was found to significantly impact their empowerment. Women living in Afar, Amhara, Oromia, SNNPR, Gambella, and Tigray regions exhibited lower levels of empowerment compared to those residing in Addis Ababa city administration. This disparity can be attributed to the greater investment by the government and non-governmental organizations in Addis Ababa in areas such as education, decision-making and economic empowerment initiatives for women. Additionally, differences in socio-economic status between urban and rural settings may also contribute to variations in women's empowerment levels.
In this study, variables such as occupation and community media exposure, previously identified as key contributors to women's empowerment (65–67), did not show statistically significant associations with empowerment. This contrast may stem from contextual differences between study populations, as the impact of these factors can be highly context-dependent. Additionally, variations in the definition or measurement of empowerment might account for the discrepancy. Furthermore, unmeasured variables such as cultural norms or regional policies may have played a more dominant role, minimizing the influence of occupation and media exposure.
Strengths and limitations
The study utilizes nationally representative datasets, enhancing the generalizability of its findings to married women of reproductive age across Ethiopia. Besides, employing a multilevel modelling technique takes into consideration the hierarchical structure of the survey data, thereby ensuring more robust and valid results. However, a limitation of the study is the absence of qualitative methods, which could have been valuable in exploring the attitudes and beliefs of women in greater depth.
Conclusion
This study reveals a low overall magnitude of women's empowerment. Maternal education level and religion appeared as significant individual-level factors, while community wealth status, place of residence, and region were notable community-level variables associated with women's empowerment. To address these findings, the Ethiopian government needs to prioritize strategies that enhance maternal education and increase women's involvement in household decision-making, thereby promoting empowerment. Additionally, implementing community-based empowerment programs, including enhancing women's access to media and health information, and involving them in income-generating activities, could serve as effective interventions to empower women.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
Ethical approval and permission to access the data were granted by MEASURE DHS (available at https://www.dhsprogram.com/Data/ and accessed on March 24, 2020) following the submission of a brief study concept. As the data used is secondary and publicly available, participant consent was not required. All procedures were carried out in accordance with the Helsinki Declaration.
Author contributions
ED: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. MT: Conceptualization, Data curation, Methodology, Visualization, Writing – original draft, Writing – review & editing. MJ: Conceptualization, Data curation, Formal Analysis, Methodology, Validation, Writing – original draft, Writing – review & editing. KD: Conceptualization, Formal Analysis, Methodology, Software, Validation, Writing – original draft, Writing – review & editing. MG: Formal Analysis, Methodology, Software, Supervision, Validation, Writing – original draft, Writing – review & editing. TB: Data curation, Methodology, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. GT: Data curation, Formal Analysis, Methodology, Software, Validation, Writing – original draft, Writing – review & editing. BA: Writing – review & editing, Conceptualization, Data curation, Methodology, Software, Validation, Writing – original draft. DG: Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing, Data curation. LY: Investigation, Methodology, Writing – original draft, Writing – review & editing, Conceptualization, Software, Supervision. TT: Data curation, Investigation, Methodology, Validation, Writing – original draft, Writing – review & editing. NW: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
The authors would like to thank MEASURE DHS for permission to use the EDHS 2016 survey data sets for further analysis.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
ANC, antenatal care; AOR, adjusted odds ratio; COR, crude odds ratio; EDHS, Ethiopian demographic and health survey; ICC, intra-class correlation coefficient; PCV, proportional change in variance; PNC, postnatal care.
References
1. Miedema SS, Haardörfer R, Girard AW, Yount KM. Women’s empowerment in East Africa: development of a cross-country comparable measure. World Dev. (2018) 110:453–64. doi: 10.1016/j.worlddev.2018.05.031
2. Sustainable Development Goals (SDGs). (2015). Available online at: https://www.undp.org/content/dam/undp/library/corporate/brochure/SDGs_Booklet_Web_En.pdf (accessed July 02, 2024).
3. Millennium Development Goals (MDGs). (2018). Available online at: https://www.undp.org/content/undp/en/home/sdgoverview/mdg_goals.html (accessed July 02, 2024).
4. Bayeh E. The role of empowering women and achieving gender equality to the sustainable development of Ethiopia. Pac Sci Rev B Hum Soc Sci. (2016) 2(1):37–42. doi: 10.1016/j.psrb.2016.09.013
5. Abreha SK, Zereyesus YA. Women’s empowerment and infant and child health status in sub-Saharan Africa: a systematic review. Matern Child Health J. (2021) 25:95–106. doi: 10.1007/s10995-020-03025-y
6. Wei W, Sarker T, Żukiewicz-Sobczak W, Roy R, Alam GM, Rabbany MG, et al. The influence of women’s empowerment on poverty reduction in the rural areas of Bangladesh: focus on health, education and living standard. Int J Environ Res Public Health. (2021) 18(13):6909. doi: 10.3390/ijerph18136909
7. Sserwanja Q, Mukunya D, Musaba MW, Mutisya LM, Kamara K, Ziaei S. Women empowerment indices and utilization of health facilities during childbirth: evidence from the 2019 Sierra Leone demographic health survey. BMC Health Serv Res. (2023) 23(1):109. doi: 10.1186/s12913-023-09122-2
8. Kabeer N. Resources, agency, achievements: reflections on the measurement of women’s empowerment. Dev Change. (1999) 30(3):435–64. doi: 10.1111/1467-7660.00125
9. Krishna A. Social Capital, Community Driven Development, and Empowerment: a Short Note on Concepts and Operations. World Bank Working Paper. (2003) 33077:22–31.
10. Pratley P. Associations between quantitative measures of women’s empowerment and access to care and health status for mothers and their children: a systematic review of evidence from the developing world. Soc Sci Med. (2016) 169:119–31. doi: 10.1016/j.socscimed.2016.08.001
11. Ahmed S, Creanga AA, Gillespie DG, Tsui AO. Economic status, education and empowerment: implications for maternal health service utilization in developing countries. PLoS One. (2010) 5(6):e11190. doi: 10.1371/journal.pone.0011190
12. Do M, Kurimoto N. Women’s empowerment and choice of contraceptive methods in selected African countries. Int Perspect Sex Rreprod Hhealth. (2012) 38(1):23–33. doi: 10.1363/3802312
13. Cinar K, Kose T. The determinants of women’s empowerment in Turkey: a multilevel analysis. S Eur Soc Polit. (2018) 23(3):365–86. doi: 10.1080/13608746.2018.1511077
14. Kwagala B, Wandera SO, Ndugga P, Kabagenyi A. Empowerment, partner’s behaviours and intimate partner physical violence among married women in Uganda. BMC public Hhealth. (2013) 13(1):1112. doi: 10.1186/1471-2458-13-1112
15. Raudeliuniene J, Dzemyda I, Kimpah J. Factors for assessment of women empowerment: theoretical approach’. 8th International Scientific Conference on Business and Management (2014) 2014. p. 15–6
16. Sen KK, Nilima S. Women’s empowerment and its determinants in Bangladesh: evidence from a national survey. Dhaka Univ J Sci. (2018) 66(2):129–34. doi: 10.3329/dujs.v66i2.54557
17. Tabassum M, Begum N, Rana MS, Faruk MO, Miah MM. Factors influencing women’s empowerment in Bangladesh. Sci Technol Public Policy. (2019) 3(1):1. doi: 10.11648/j.stpp.20190301.11
18. Constitution of the Federal Democratic Republic of Ethiopia. (1994). Available online at: https://www.wipo.int/edocs/lexdocs/laws/en/et/et007en.pdf (accessed July 04, 2024).
19. National Policy on Women. (2020). Available online at: https://www.abyssinialaw.com/online-resources/policies-and-strategies?download=1374:national-policy-on-ethiopian-women (accessed July 04, 2024).
20. Growth and Transformation Plan (GTP I). (2010). Available online at: http://et.china-embassy.org/eng/asebyxx/P020150429599764253764.pdf (accessed July 05, 2024).
21. Growth and Transformation Plan (GTP II). (2019). Available online at: https://europa.eu/capacity4dev/file/30510/download?token=efsF8UiP (accessed July 05, 2024).
22. Central Statistical Agency (CSA) [Ethiopia] and ICF. Ethiopia Demographic and Health Survey 2016. Addis Ababa, Ethiopia, and Rockville, Maryland, USA: CSA and ICF (2016).
23. Ebrahim NB, Atteraya MS. Women’s decision-making autonomy and their attitude towards wife-beating: findings from the 2011 Ethiopia’s demographic and health survey. J Immigr Minor Health. (2018) 20(3):603–11. doi: 10.1007/s10903-017-0592-6
24. World Bank. The World Bank in Ethiopia. (2024). Available online at: http://www.worldbank.org/en/country/ethiopia/overview (accessed July 08, 2024)
25. Central Statistical Agency (CSA) I. Ethiopian Demographic and Health Survey. Addis Abeba: Addis Ababa, Ethiopia, and Rockville, Maryland, USA: CSA and ICF (2016).
26. Health FDRoEMo. Federal Democratic Republic of Ethiopia Ministry of Health. Annual Performance Report. Addis Ababa: Ethiopian Federal Ministry of Health (2018).
27. Health FDRoEMo. HSTP: Health Sector Transformation Plan: 2015/16-2019/20 (2008-2012 EFY). Addis Ababa: Federal Democratic Republic of Ethiopia Ministry of Health (2015).
28. Croft TN, Marshall AM, Allen CK, Arnold F, Assaf S, Balian S. Guide to DHS Statistics. Rockville: ICF (2018).
29. Central Statistical Agency—CSA/Ethiopia, ICF. Ethiopia Demographic and Health Survey 2016. Addis Ababa, Ethiopia: CSA and ICF (2017).
30. Snijders TAB. Multilevel Aanalysis: An Introduction to Basic and Applied Multilevel Analysis (2012).
31. Rodriguez G, Elo I. Intra-class correlation in random-effects models for binary data. Stata J. (2003) 3(1):32–46. doi: 10.1177/1536867X0300300102
32. Woldemicael G, Tenkorang EY: Women’s autonomy and maternal health-seeking behavior in Ethiopia. Matern Child Health J. (2010) 14(6):988–98. doi: 10.1007/s10995-009-0535-5
33. Soni M, Ireen S, Siddique A. Factors influencing empowerment level of women: a case study of Kushtia, Bangladesh. Int Adv Res J Sci Eng Tech. (2016) 3(2):93–7.
34. Akram N. Women’s empowerment in Pakistan: its dimensions and determinants. Soc Indic Res. (2018) 140(2):755–75. doi: 10.1007/s11205-017-1793-z
35. Bloom SS, Wypij D, Das Gupta M: Dimensions of women’s autonomy and the influence on maternal health care utilization in a North Indian city. Demography. (2001) 38(1):67–78. doi: 10.1353/dem.2001.0001
36. Pandey S, Lama G, Lee H. Effect of women’s empowerment on their utilization of health services: a case of Nepal. Int Soc Work. (2012) 55:554–73. doi: 10.1177/0020872811408575
37. Seidu A-A, Dzantor S, Sambah F, Ahinkorah BO, Ameyaw EK. Participation in household decision making and justification of wife beating: evidence from the 2018 Mali demographic and health survey. Int Health. (2022) 14(1):74–83. doi: 10.1093/inthealth/ihab008
38. Butler MG, Walker M, Pablo LA. Bartels SA: Relationship between women’s decision-making power over their own health care and use of modern contraception in the Democratic Republic of the Congo: a cross-sectional secondary data analysis. BMC Womens Hhealth. (2021) 21(1):309. doi: 10.1186/s12905-021-01450-x
39. Abshoko AD, Terye ND, Shamenna AT. Determinants of socio-economic empowerment of married women: evidence from Ethiopia. Human Soc Sci. (2016) 4(3):66. doi: 10.11648/j.hss.20160403.11
40. Sell M, Minot N. What factors explain women’s empowerment? Decision-making among small-scale farmers in Uganda. In: Stan L, editor. Women’s Studies International Forum: 2018. Amsterdam: Elsevier (2018). p. 46–55.
41. Asaolu IO, Alaofè H, Gunn JK, Adu AK, Monroy AJ, Ehiri JE, et al. Measuring women’s empowerment in sub-Saharan Africa: exploratory and confirmatory factor analyses of the demographic and health surveys. Front Psychol. (2018) 9:994. doi: 10.3389/fpsyg.2018.00994
42. Nwogwugwu N. Women's empowerment and women's health in Africa. In: Yacob-Haliso O, Falola T, editors. The Palgrave Handbook of African Women's Studies. Cham: Palgrave Macmillan. (2020). doi: 10.1007/978-3-319-77030-7_160-1
43. Obayelu OA, Chime AC. Dimensions and drivers of women’s empowerment in rural Nigeria. Int J Soc Econ. (2020) 47(3):315–33.
44. Musonera A, Heshmati A. Measuring women’s empowerment in Rwanda. In: Heshmati A, editor. Studies on Economic Development and Growth in Selected African Countries. Cham: Springer (2017). p. 11–39.
45. Musonera A, Heshmati A. Measuring women's empowerment in Rwanda. In: East Africa Research Papers in Economics and Finance. EARP-EF no. 2016: 02 Jönköping International Business School (JIBS). Jönköping: Jönköping University (2016).
46. Bushra A, Wajiha N. Assessing the socio-economic determinants of women empowerment in Pakistan. Proc Soc Behav Sci. (2015) 177:3–8. doi: 10.1016/j.sbspro.2015.02.321
47. Sharma GD, Sanchita. Determinants and indicators of women empowerment: a walk through psychological patterns and behavioural implications. Res J Bus Manag. (2016) 11(1):15–27. doi: 10.3923/rjbm.2017.15.27
48. Habibov N, Barrett BJ, Chernyak E. Understanding women’s empowerment and its determinants in post-communist countries: results of Azerbaijan national survey. In: Stan L, editor. Women’s Studies International Forum: 2017. Vol. 62. Amsterdam: Elsevier (2017). p. 125–35.
49. Power C. SDG 10 reducing inequalities. In: Franco IB, editor. Actioning the Global Goals for Local Impact. Cham: Springer (2020). p. 153–72.
50. Phan L. Measuring women’s empowerment at household level using DHS data of four Southeast Asian countries. Soc Indic Res. (2016) 126(1):359–78. doi: 10.1007/s11205-015-0876-y
51. Shetty S, Hans V. Role of Education in Women Empowerment and Development: Issues and Impact. Role of Education in Women Empowerment and Development: Issues and Impact (2015).
53. Nussbaum M. Women and Human Development: The Capabilities Approach. Cambridge University Press (2000).
54. Sen A. Human rights and capabilities. J Hum Dev. (2005) 6(2):151–66. doi: 10.1080/14649880500120491
55. Palamuleni ME, Adebowale AS. Women empowerment and the current use of long acting and permanent contraceptive: evidence from 2010 Malawi demographic and health survey. Malawi Med J. (2014) 26(3):63–70.27529015
56. Kirigiti PJ, Fulment A, Matunga B. Determinants and attitudes of women on empowerment through MFIs. Bus Econ Res. (2018) 8(4):80. doi: 10.5296/ber.v8i4.13521
57. Njoh AJ, Akiwumi FA. The impact of religion on women empowerment as a millennium development goal in Africa. Soc Indic Res. (2012) 107(1):1–18. doi: 10.1007/s11205-011-9827-4
58. Klingorova K, Havlíček T. Religion and gender inequality: the status of women in the societies of world religions. Morav Geogr Rep. (2015) 23(2):2–11. doi: 10.1515/mgr-2015-0006
59. Chattopadhyay S, Roy Chowdhury J. Does religion affect women’s agency? Empirical evidence from India. J Econ Race Policy. (2024):1–18. doi: 10.1007/s41996-024-00141-7
60. Singer P. The Life you can Save: How to do Your Part to End World Poverty: Random House Incorporated (2010).
61. Dormekpor E. Poverty and gender inequality in developing countries. Dev Country Stud. (2015) 5(10):76–102.
62. Alkire S, Robles G. Multidimensional Poverty Index Summer 2017: Brief Methodological Note and Results. OPHI Methodological Notes. (2017) 45.
63. Smith N. Economic inequality and poverty: where do we go from here? Int J Sociol Soc Policy. (2010) 30:127–39. doi: 10.1108/01443331011033328
64. Dalal K. Causes and Consequences of Violence against Child Labour and Women in Developing Countries. Institutionen för folkhälsovetenskap/Department of Public Health Sciences (2008) 30(3/4):127–39. doi: 10.1108/01443331011033328
65. Costa JC, Saad GE, Hellwig F, Maia MFS, Barros AJ. Measures of women’s empowerment based on individual-level data: a literature review with a focus on the methodological approaches. Front Sociol. (2023) 8:1231790. doi: 10.3389/fsoc.2023.1231790
66. Kabeer N, Mahmud S, Tasneem S. The contested relationship between paid work and women’s empowerment: empirical analysis from Bangladesh. Eur J Dev Res. (2018) 30:235–51. doi: 10.1057/s41287-017-0119-y
Keywords: justified wife-beating, multilevel analysis, Ethiopia, decision making, women's empowerment
Citation: Dellie E, Tiruneh MG, Jejaw M, Demissie KA, Getnet M, Belachew TB, Teshale G, Addis B, Geberu DM, Yazachew L, Tafere TZ and Worku N (2024) What factors influence women's empowerment in Ethiopia? A multilevel analysis of Ethiopia's demographic and health survey data. Front. Glob. Womens Health 5:1463157. doi: 10.3389/fgwh.2024.1463157
Received: 11 July 2024; Accepted: 14 October 2024;
Published: 31 October 2024.
Edited by:
Jay S. Mishra, University of Wisconsin-Madison, United StatesReviewed by:
Nosakhare Orobaton, Bill and Melinda Gates Foundation, United StatesPankaj Yadav, University of Wisconsin-Madison, United States
Copyright: © 2024 Dellie, Tiruneh, Jejaw, Demissie, Getnet, Belachew, Teshale, Addis, Geberu, Yazachew, Tafere and Worku. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Endalkachew Dellie, ZW5kYWxrZC4wN0BnbWFpbC5jb20=
†These authors have contributed equally to this work