 Daya K. Grewal1,2*
Daya K. Grewal1,2* Molly A. Patapoff3,4
Molly A. Patapoff3,4 Victoria Liou-Johnson2,5,6
Victoria Liou-Johnson2,5,6 Maheen M. Adamson1,5,7
Maheen M. Adamson1,5,7 Dylan J. Jester1
Dylan J. Jester1
- 1Women’s Operational Military Exposure Network Center of Excellence (WOMEN CoE), VA Palo Alto Health Care System, Palo Alto, CA, United States
- 2Department of Psychology, Palo Alto University, Palo Alto, CA, United States
- 3Sam and Rose Stein Institute for Research on Aging, University of California San Diego, La Jolla, CA, United States
- 4Department of Psychiatry, University of California San Diego, La Jolla, CA, United States
- 5Rehabilitation Service, VA Palo Alto Health Care System, Palo Alto, CA, United States
- 6Clinical Excellence Research Center, Stanford University School of Medicine, Stanford, CA, United States
- 7Department of Neurosurgery, Stanford University School of Medicine, Stanford, CA, United States
Objective: This study investigated the relationship between years of employment and cognitive health among older non-Latinx Black, Latinx, and non-Latinx White women. We hypothesized that women who had never been formally employed (i.e., zero years of formal work experience) would exhibit a pronounced cognitive decline.
Methods: Our study included 5,664 older adult women from the Health and Retirement Study (2010–2016) aged 65–101 (M = 75.41). Out of 5,664 participants, 850 identified as non-Latinx Black, 475 identified as Latinx, and 4,339 identified as non-Latinx White. Furthermore, 5,292 women indicated having a professional employment history of at least one year, whereas 372 women reported no formal work experience. The Telephone Interview for Cognitive Status-27 (TICS-27) was used to assess cognitive performance. Linear mixed effects models were conducted to assess whether employment history was associated with the rate of cognitive decline.
Results: In all three racial and ethnic groups, lower age, higher education, greater number of years worked, fewer chronic conditions, and greater household income were associated with better cognitive performance at baseline (p < .05). Additionally, women who had not worked in any formal capacity had a lower baseline cognitive performance (p < .001) and a more extreme decline in cognitive performance over time (p = .04).
Conclusion: In conclusion, we found that women without any formal work experience performed lower at baseline and experienced a steeper cognitive decline over time. These findings underscore the need to further explore the complex interrelationships between employment duration and cognitive trajectories, especially among older women and those from different racial and ethnic backgrounds.
Introduction
Cognitive decline remains one of the world's most burdensome chronic health conditions. Rates of Alzheimer's disease and related dementias (ADRD) have risen in recent years (1), and disproportionately across marginalized racial and ethnic groups. Non-Latinx Black and Latinx older adults have an increased risk of receiving an ADRD diagnosis when compared to their non-Latinx White counterparts (2–4), and this higher rate of ADRD is largely due to the effects of systemic racism on health and educational, occupational, and social opportunities. Additionally, women have an increased risk of developing ADRD (5). This greater risk may be linked to several factors: women are more likely than men to live into older age (6), there are sex differences in ADRD neuropathology and changes in hormones during menopause may affect risk (1, 5), and gender discrimination in education and work opportunities may result in lower cognitive reserve (CR) (7, 8).
Cognitive reserve
CR helps explain the discrepancies between neuropathology and clinical functioning. Individuals with high CR may not show symptoms of ADRD, despite significant brain atrophy and network disruption (9). CR has been linked to a 47% reduction in the risk of progressing to Mild Cognitive Impairment (MCI) or ADRD, independent of structural pathology and Alzheimer's biomarkers (10). CR enables alternative neuronal networks and cognitive strategies to maintain performance despite brain changes (11). However, operationalizing CR is complex due to varying definitions that influence the perceived risk of MCI or ADRD. Proxies like educational attainment, occupational complexity, and participation in intellectually enriching activities are often used as indirect measures of CR, assuming that higher levels indicate greater reserve (12). Another approach uses residual cognitive performance after adjusting for AD neuropathology to measure CR (10).
CR is significantly shaped by social determinants of health (SDoH), including education, occupational history, and socioeconomic status (SES). Education strengthens and creates neural networks (13–15) and serves as a proxy for higher SES. Those with higher educational attainment often secure better-paying jobs, leading to health-promoting behaviors, reduced social stressors, and a lower risk of cognitive decline (7, 16, 17). Occupation, as a core SES indicator, supports health maintenance by contributing to economic, cultural, or social capital (16, 18) and may directly influence cognitive outcomes (19).
The role of occupational history on cognitive reserve
Adulthood is largely occupied with work-related activities that demand significant time and energy (20). Jobs involving monotonous, low-skill tasks (low job complexity) and limited autonomy (low job control) are associated with poorer cognitive performance (21). In contrast, roles requiring higher cognitive engagement and complex social interactions are linked to better cognitive performance (22–27), reduced risk of ADRD (28), and a slower rate of cognitive decline post-retirement (29, 30), and roles with high autonomy correlate with increased hippocampal volume and a slower reduction in this volume over time (31, 32). Additionally, the cognitive benefits of job complexity appear to be moderated by leisure activity, especially social activities (22).
Racial discrimination's impact on occupation and cognitive reserve
Simons et al. (33) suggest a possible role of SES and discrimination on accelerated biological aging through the accrual of chronic illnesses. The impacts of racial discrimination and chronic stress due to socioeconomic hardship, substandard education quality, and neighborhood disadvantages are linked to cognitive impairment and an increased risk of ADRD (2–4). Differences in SDoH account for 39% of the non-Latinx Black- non-Latinx White disparity and 76% of the Latinx- non-Latinx White disparity in cognitive performance (34), with years worked explaining 6% and 10% of these disparities, respectively. However, the protective effects of higher education or occupational complexity on cognitive decline may not apply equally across non-Latinx Black, Latinx, and non-Latinx White adults (18, 35–38), in part due to poorer educational quality and limited opportunities for occupational mobility among marginalized groups (39).
Gender norms impact on occupation and cognitive performance
Gender disparities shape how occupational history impacts cognitive performance in older adulthood (40, 41). Occupational roles, often limited by historical gender norms, significantly influence cognitive health in later life (8, 42). Women, especially those from older birth cohorts, were subject to lower expectations for educational attainment and occupational status, often confined to roles with less cognitive complexity that could impact the rate of cognitive decline years later (22, 41). This effect is even more pronounced in women of color, who have faced compounded challenges due to intersecting sexism and racism, further limiting their educational and occupational opportunities and, thus, influencing their cognitive health (22, 43).
This study examined the impact of formal work experience on cognitive decline in older women, focusing on non-Latinx Black, Latinx, and non-Latinx White women to understand how years of formal employment affected cognitive trajectories. We hypothesized that having greater formal employment history would affect the rate of change on the TICS-27 over time (i.e., the interaction of employment duration by time) and that this effect would differ among non-Latinx Black, Latinx, and non-Latinx White women. Furthermore, we hypothesized that women who had never been formally employed (i.e., zero years of formal work experience) would exhibit a pronounced rate of cognitive decline.
Methods
Participants and study design
This is a retrospective cohort study examining a sample of older adult women (>65 years) from the Health and Retirement Study (HRS). The present study utilizes longitudinal data from the following four consecutive assessments: wave 10 (2010), wave 11 (2012), wave 12 (2014), and wave 13 (2016). The HRS is a collaboration between the National Institute of Aging (U01AG009740) and the University of Michigan, started in 1992. Managed by the University of Michigan's Survey Research Center, the study has maintained response rates between 81.7% and 89.1% since inception (49).
Inclusion criteria were: (1) aged ≥ 65 years at wave 10 and (2) identified as non-Latinx Black, Hispanic/Latinx, or non-Latinx White. Participants that identified as “other,” or were missing race and ethnicity data were excluded. Outcome: The Telephone Interview for Cognitive Status-27 (TICS-27) was used to assess cognitive performance. The TICS-27 is a 27-item measure of global cognition, scored using the Langa-Weir composite scoring approach (44). This method allocates 20 points to short-term and long-term memory and 7 points to processing speed and executive functions, with total scores ranging from 0 to 27.
Covariates
The following covariates were included to control for possible confounding contributors to cognitive decline: age (years), education (years), body mass index, annual household income (natural-logged U.S. dollars), and number of chronic health conditions, including high blood pressure, diabetes, cancer, lung disease, heart problems, stroke, psychological problems, and arthritis. All covariates were estimated at participants’ 2010 (wave 10) assessment which functioned as a baseline for our analyses.
Statistical analysis
Linear mixed effects models (LMMs) were conducted to assess the impact of employment duration on the rate of cognitive decline (i.e., change in cognitive performance over time). In this multilevel LMM framework, cognitive performance at each wave (Level 1) was nested within each participant (Level 2) to determine how women performed over time. Models were stratified by race and ethnicity (non-Latinx Black, Latinx, and non-Latinx White). The main independent variable of interest was employment duration (number of years worked), and the main outcome variable of interest was performance on the TICS-27 score measured consecutively over four waves. The coefficient for employment duration describes the average change in cognitive performance at baseline for each additional year of formal work experience. The coefficient for time describes the average change in cognitive performance over each wave (in roughly 2-year increments). An interaction term of time by employment duration describes the impact of each additional year of formal work experience on the average rate of change in cognitive performance. LMMs included a random intercept to capture interindividual differences at baseline. A random slope capturing intraindividual differences could not be estimated due to low within-person variance over time (i.e., the rate of change was largely homogeneous).
An additional LMM using the full sample (all three race and ethnicity groups) was constructed to examine cognitive decline in women with some vs. no formal work experience. In this model, employment duration was dummy coded as a categorical variable (zero years worked vs. one or more years work). An interaction term of time by the categorical employment duration variable assessed the impact of having no formal work experience on the average rate of change in cognitive performance. Due to significant differences in education between the two employment duration groups (i.e., a large effect size difference), models with education and without education are presented. As a sensitivity analysis, all models were reconducted with the TICS-20 memory component subscore (10 points immediate recall; 10 points delayed recall).
Results
The final sample included 5,664 women aged 65–101 (M = 75.41, SD = 7.22), of which 850 identified as non-Latinx Black, 475 identified as Latinx, and 4,339 participants identified as non-Latinx White. 5,292 women (93%) indicated having a professional employment history of at least one year, whereas 372 women (7%) reported no formal work experience. See Table 1 for baseline demographic information stratified by race and ethnicity.
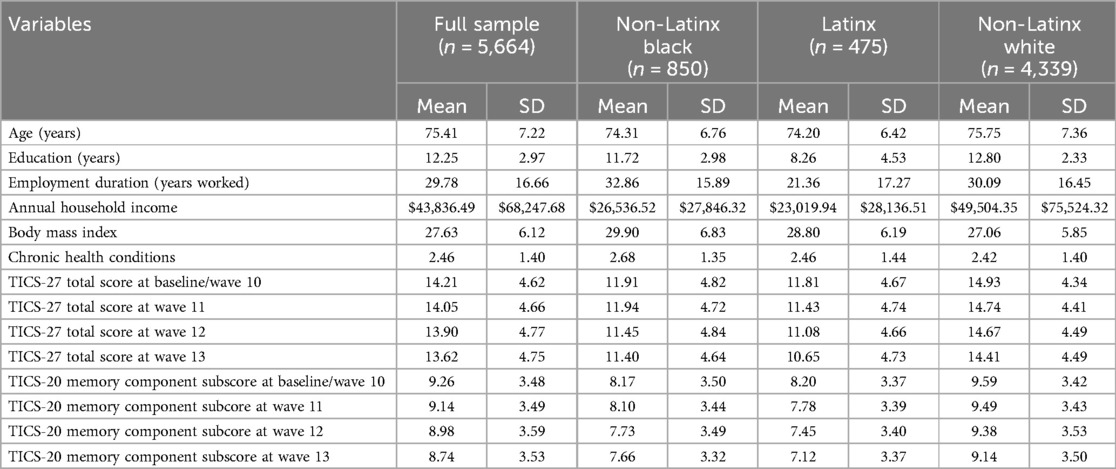
Table 1. Demographic characteristics by race and ethnicity group.SD, standard deviation; TICS-27, telephone interview for cognitive status–modified 27-item.
In all three racial and ethnic groups, lower age, higher education, greater number of years worked, fewer chronic conditions, and greater household income were significantly associated with higher TICS-27 scores (indicating better cognitive performance) at baseline (p < .05). In the non-Latinx Black and non-Latinx White groups, higher body mass index was also significantly associated with higher TICS-27 scores at baseline. No significant interactions were observed between duration of employment and slope of cognitive performance in any of the racial and ethnic groups (p > .05; Table 2). Removing educational attainment as a covariate from the race and ethnicity stratified analyses did not appreciably change the results.
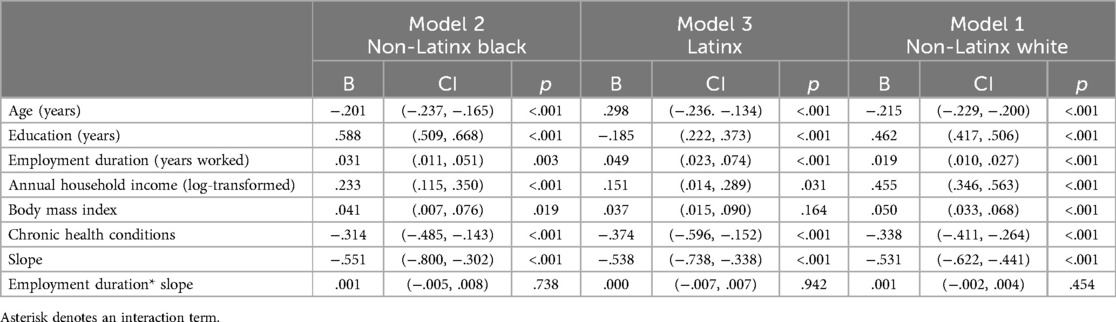
Table 2. Linear mixed effects models assessing the association of employment duration, covariates, and cognitive decline assessed via TICS-27 total score stratified by race and ethnicity.
In the full sample, women with some work experience (M = 12.41, SD = 2.84) compared to women with none (M = 10.08, SD = 3.73) had significantly higher levels of education, (p < .001, Cohen's d = −0.80). When excluding education as a covariate, having no formal work experience was significantly associated with lower TICS-27 scores at baseline (p < .001) and a greater rate of decline in cognitive performance over time (p = .04) compared to having one or more years of formal work experience. Compared to non-Latinx White women, non-Latinx Black and Latinx women performed lower at baseline (p < .001). When adjusting for education, differences between women with and without formal work experience were no longer significant, suggesting that disparities in educational attainment partially attenuated the relationship between formal work experience and cognitive decline. See Table 3 for full model details.
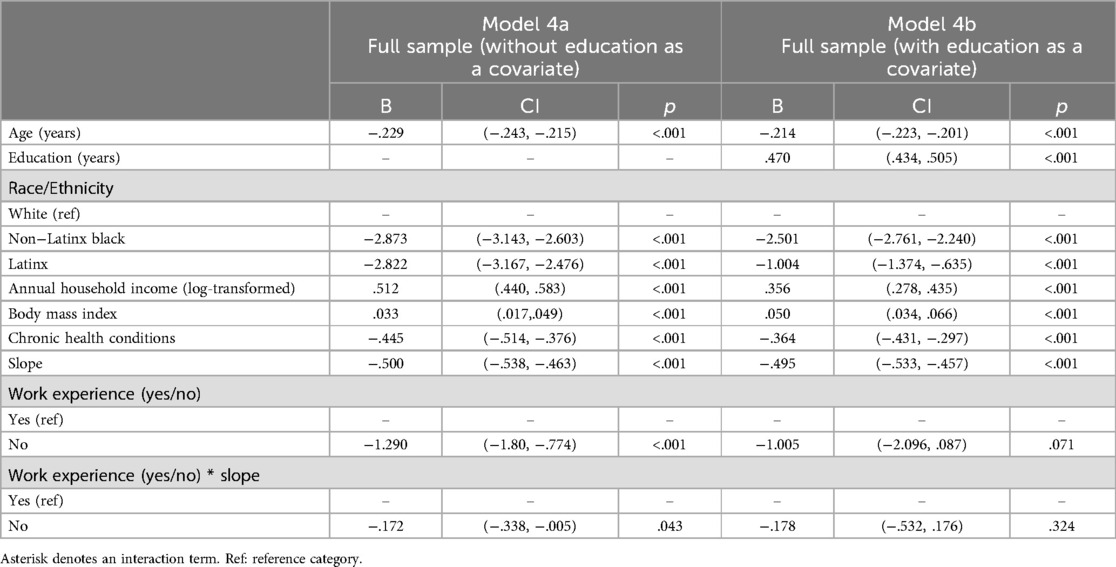
Table 3. Linear mixed effects models assessing the association of categorical employment duration, covariates, and cognitive decline assessed via TICS-27 total score in the full sample.
When repeating the above analyses with the TICS-20 memory component subscore as the outcome variable, results largely remained the same. However, in the full sample, having no formal work experience was associated with lower performance on the TICS-20 memory component scores at baseline, and this effect persisted after adjusting for education (p = .04). See Tables 4, 5 for full details.
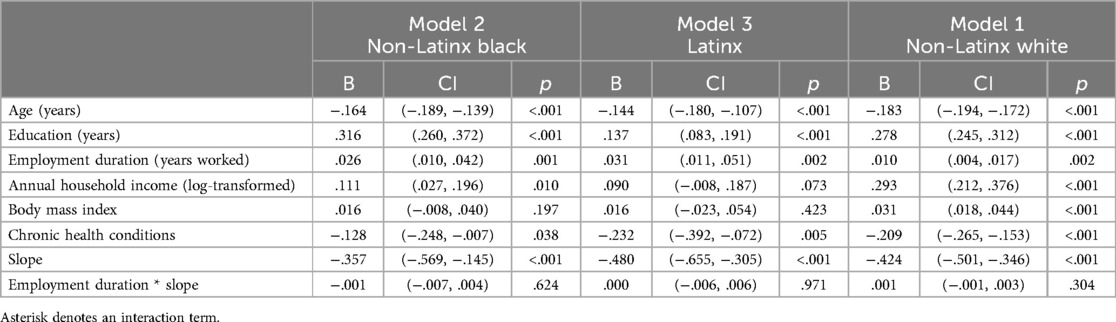
Table 4. Linear mixed effects models assessing the association of employment duration, covariates, and cognitive decline assessed via TICS−20 memory component subscore stratified by race and ethnicity.

Table 5. Linear mixed effects models assessing the association of categorical employment duration, covariates, and cognitive decline assessed via TICS-20 memory component subscore in the full sample.
Discussion
This study was primarily focused on elucidating the impact of formal work experience on the cognitive trajectories of older women (≥65), with a particular emphasis on historically marginalized groups, including non-Latinx Black, Latinx, and non-Latinx White women. We examined the impact of employment duration on cognitive decline over time, considering potential variations across different racial and ethnic backgrounds. Our results did not substantiate the first hypothesis. The number of years of employment did not affect the rate of cognitive decline, nor was there a differential impact by race and ethnicity among the women in our study. However, years worked did positively impact baseline performance, with each of the racial and ethnic groups having better TICS-27 and TICS-20 performance with greater employment history.
Discrimination based on race and ethnicity significantly influences employment opportunities and cognitive health trajectories. For non-Latinx Black Americans, the effects of institutional racism result in reduced access to high quality education, lower job attainment, and diminished income compared to other racial and ethnic groups (33). non-Latinx Black Americans disproportionately experience socioeconomic stressors, including financial precarity, lower-status jobs, periods of unemployment, inadequate housing, and the compounded challenges of food deserts and elevated crime rates (45). These factors hinder professional advancement and may negatively affect cognitive reserve. Additionally, it is well-known that chronic conditions may cluster among racial, ethnic, geographic, or cultural groups due to differences in health behaviors, access to healthcare, systemic inequities, and the numerous impacts of social determinants of health. Future work should consider whether specific chronic conditions uniquely affect the rate of cognitive decline in older women from different backgrounds and identities.
Educational attainment was included and excluded from certain models to determine whether the effect of years worked on cognitive performance was fully or partially explained by educational attainment. Given that educational attainment can confound the relationship between years worked and cognitive performance, it was essential to assess its attenuating effect. Although women without formal work experience performed worse at baseline and over time, these findings were attenuated by the inclusion of educational attainment. A larger sample would be needed to determine if educational attainment and formal work experience independently affect cognitive performance at baseline and over time or if these factors are interdependent.
We hypothesized that older women with no formal employment history would demonstrate a more pronounced rate of cognitive decline, supported by existing literature that highlights the role of job complexity in mitigating cognitive decline and reducing the risk of ADRD (22–28). Historically, women in the United States were restricted from fully participating in the formal workforce due to gender norms and legal discrimination until the Civil Rights Act of 1964. As a result, older cohorts of women (e.g., Silent Generation, Greatest Generation) often assumed demanding, unpaid roles as homemakers and caregivers, while their daughters (e.g., Baby Boomers) were encouraged to pursue “feminine” roles in the economy, such as teachers, nurses, administrative assistants, wait staff, and beauticians. These generational gender norms and legal segregation led to disparities in educational attainment, occupational status, and work complexity for women, which may have influenced their cognitive functioning and trajectory in later life (8, 42). This hypothesis aligns with the broader narrative that women are at an elevated risk for ADRD, a disparity that may be partly attributable to gender-based differences in CR stemming from historical discrimination in educational and occupational opportunities (5, 7, 8).
The Latinx cohort performed similarly at baseline to the non-Latinx Black cohort, despite having worked fewer years (21.36 vs. 32.68) and having lower educational attainment (8.26 vs. 11.72) on average. Age does not appear to be a confound, as these two groups were similar (74.20 vs. 74.31). If educational attainment was fully attenuating the relationship between formal work experience and cognitive performance, we might expect a significantly lower performance from our Latinx cohort. Because we do not see this (TICS-27: 11.81 vs. 11.91), it suggests that other factors such as education quality, cognitive reserve, test-wiseness, or a variety of other factors may be preserving our Latinx cohort's performance, at least on a univariate level.
Educational attainment is not solely a measure of knowledge or skill acquisition; it is often indicative of a broader spectrum of socioeconomic advantages. Higher education is correlated with higher-paying occupations, which may be a reflection of or a pathway to generational wealth. Such economic stability can afford an individual the luxury of engaging in health-promoting activities, accessing superior healthcare services, or reducing exposure to chronic social stressors—all of which are linked with preserving cognitive function (7, 16, 17). Moreover, prior literature has highlighted that education can enhance the brain's resilience to neuropathological damage by strengthening existing neural networks and facilitating the development of new ones (14). This reserve allows individuals to better cope with the structural changes associated with aging and potentially delays the onset of clinical manifestations of ADRD. However, older women with no formal work experience had fewer years of education on average in our study. It is possible that educational attainment and formal work experience impact cognitive health through similar processes for some women (e.g., cognitive reserve), but this is not likely to be true for all women. There may be a variety of reasons why a woman chooses to or is forced to abstain from the workforce (e.g., preference and economic ability to do so; health concerns; experiences of discrimination; gender roles and expectations), and each of these groups may have a different level of education and risk for cognitive decline in later life. Clearly, more work needs to be conducted along these lines.
Furthermore, despite our initial hypotheses, we did not observe an effect of employment duration on cognitive decline across non-Latinx Black, Latinx, or non-Latinx White older women. Several SDoH are known to impact cognitive health and risk of ADRD (46, 47), yet determinants especially prominent among historically underserved groups remain understudied (e.g., experiences of discrimination, exclusion from the formal workforce, nativity status; disparities in education quality) (34, 48). In our study, formal work experience affected cognitive performance and the rate of decline uniformly across non-Latinx Black, Latinx, or non-Latinx White women, which differs from the previous findings by Jester et al. (34) in which the number of years worked explained a sizeable proportion of the non-Latinx Black- non-Latinx White (6%) and Latinx- non-Latinx White (10%) disparities in cognitive performance at baseline. It is important to consider the possibility that a SDoH like work experience may influence performance at baseline, but not necessarily differences in longitudinal trajectories. Alternatively, it may be that when measuring cognitive trajectories by race and ethnicity, education simply explains more of the variance, thus attenuating the relationship. Although our findings paint an unclear image of the relationship between the number of years worked and cognitive decline across racial and ethnic groups, it highlights the need for ongoing research into the SDoHs that impact cognitive health.
Our findings are subject to methodological limitations, primarily stemming from the structure and availability of variables within the HRS. The HRS's classification of racial and ethnic groups is limited, which may not capture the full diversity within each category. It does not include individuals who do not fit into the predefined classifications or have missing race and ethnicity data. This categorization limitation could lead to a lack of representation and an incomplete understanding of the cognitive trajectories across a more diverse population. Furthermore, the variables available in the HRS allowed us to consider the quantity of education, but not the quality. The quality of education is a critical factor that can influence cognitive outcomes and varies based on several factors, such as socioeconomic status, school resources, and geographic location. The absence of data on the quality of education means that our analysis may only partially reflect the nuanced ways in which educational experiences impact cognitive health. Unfortunately, the reason for being absent from the formal workplace was not registered in the HRS dataset. Work is needed to understand how education and formal work experience influence each other, and how/whether they explain the same or different aspects of cognitive performance and cognitive decline. Furthermore, residual confounding may exist in our models despite our attempts at controlling for a variety of demographic, social, and health factors. Finally, this study's outcome variable was limited to the TICS-27. While TICS-27 is a widely used and validated measure for assessing global cognitive performance in the HRS, it does not capture the various domains of cognition in sufficient detail. Given that our sensitivity analysis utilizing the TICS-20 memory component subscore yielded slightly differing results, future work should include a full cognitive battery when possible.
In addition to its limitations, this study has several strengths. One of the main strengths is the substantial sample size of older women, which allows for more robust and generalizable findings. The richness of the HRS data is another significant strength, providing comprehensive information on a wide range of variables, including demographic, socioeconomic, and health-related factors. Furthermore, the longitudinal design of the HRS allows for examining changes over time, adding depth to our understanding of cognitive decline.
In conclusion, the relationship between formal work experience, education, race and ethnicity, and cognitive decline in older women is complex and multifaceted. Our study adds to the growing body of literature recognizing educational disparities’ crucial role in cognitive health outcomes. While our study points to educational disparities as a significant factor in cognitive decline, we recognize that education is intertwined with broader social issues, including gendered expectations and roles. The historical underrepresentation of women in higher education and the workforce, often due to caregiving responsibilities or cultural norms, especially in developing countries, merits further investigation to determine its impact on cognitive health. Moreover, gender discrimination and societal expectations have differentially shaped the educational and occupational opportunities available to women. As such, future studies should examine how these gendered experiences intersect with race and occupation to influence cognitive outcomes.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found here: https://hrsdata.isr.umich.edu/data-products.
Ethics statement
Ethical approval was not required for the studies involving humans because publicly available data sets were analyzed in this study. The studies were conducted in accordance with the local legislation and institutional requirements.
Author contributions
DG: Conceptualization, Writing – original draft, Writing – review & editing. MP: Formal Analysis, Methodology, Writing – review & editing. VL-J: Conceptualization, Supervision, Writing – review & editing. MA: Supervision, Writing – review & editing. DJ: Conceptualization, Methodology, Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The National Institute on Aging (U01-AG009740) funded the HRS, with supplemental funding from the Social Security Administration. This work was supported by the WOMEN CoE.
Acknowledgments
This study was not preregistered. The contents do not represent the views of the U.S. Department of Veterans Affairs or the United States Government, Stanford University School of Medicine, or Palo Alto University.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Mielke MM, Aggarwal NT, Vila-Castelar C, Agarwal P, Arenaza-Urquijo EM, Brett B, et al. Consideration of sex and gender in Alzheimer’s disease and related disorders from a global perspective. Alzheimer’s Dement. (2022) 18(12):2707–24. doi: 10.1002/alz.12662
2. Coogan P, Schon K, Li S, Cozier Y, Bethea T, Rosenberg L. Experiences of racism and subjective cognitive function in African American women. Alzheimers Dement Diag, Assess Dis Monitor. (2020) 12(1):e12067. doi: 10.1002/dad2.12067
3. Letang SK, Lin SS-H, Parmelee PA, McDonough IM. Ethnoracial disparities in cognition are associated with multiple socioeconomic status-stress pathways. Cogn Res Princ Implic. (2021) 6(1):64. doi: 10.1186/s41235-021-00329-7
4. Zuelsdorff M, Larson JL, Hunt JFV, Kim AJ, Koscik RL, Buckingham WR, et al. The area deprivation Index: a novel tool for harmonizable risk assessment in Alzheimer’s disease research. Alzheimers Dement Transl Res Clin Interv. (2020) 6(1):e12039. doi: 10.1002/trc2.1203
5. Scheyer O, Rahman A, Hristov H, Berkowitz C, Isaacson RS, Diaz Brinton R, et al. Female sex and Alzheimer’s risk: the menopause connection. J Prevent Alzheimers Dis. (2018) 5(4):225–30. doi: 10.14283/jpad.2018.34
6. Gordon EH, Peel NM, Samanta M, Theou O, Howlett SE, Hubbard RE. Sex differences in frailty: a systematic review and meta-analysis. Exp Gerontol. (2017) 89:30–40. doi: 10.1016/j.exger.2016.12.021
7. Lyu J, Burr JA. Socioeconomic status across the life course and cognitive function among older adults: an examination of the latency, pathways, and accumulation hypotheses. J Aging Health. (2016) 28(1):40–67. doi: 10.1177/0898264315585504
8. Rocca WA, Grossardt BR, Shuster LT. Oophorectomy, estrogen, and dementia: a 2014 update. Mol Cell Endocrinol. (2014) 389(1–2):7–12. doi: 10.1016/j.mce.2014.01.020
9. Mortimer JA, Snowdon DA, Markesbery WR. Head circumference, education and risk of dementia: findings from the nun study. J Clin Exp Neuropsychol. (2003) 25(5):671–9. doi: 10.1076/jcen.25.5.671.14584
10. Nelson ME, Jester DJ, Petkus AJ, Andel R. Cognitive reserve, Alzheimer’s neuropathology, and risk of dementia: a systematic review and meta-analysis. Neuropsychol Rev. (2021) 31(2):233–50. doi: 10.1007/s11065-021-09478-4
11. Stern Y. What is cognitive reserve? Theory and research application of the reserve concept. J Int Neuropsychol Soc. (2002) 8(3):448–60. doi: 10.1017/S1355617702813248
12. Opdebeeck C, Martyr A, Clare L. Cognitive reserve and cognitive function in healthy older people: a meta-analysis. Aging Neuropsychol Cogn. (2016) 23(1):40–60. doi: 10.1080/13825585.2015.1041450
13. Avila JF, Rentería MA, Jones RN, Vonk JMJ, Turney I, Sol K, et al. Education differentially contributes to cognitive reserve across racial/ethnic groups. Alzheimers Dement. (2021) 17(1):70–80. doi: 10.1002/alz.12176
14. Stern Y. Cognitive reserve⋆. Neuropsychologia. (2009) 47(10):2015–28. doi: 10.1016/j.neuropsychologia.2009.03.004
15. Wilson RS, Yu L, Lamar M, Schneider JA, Boyle PA, Bennett DA. Education and cognitive reserve in old age. Neurology. (2019) 92(10):e1041–50. doi: 10.1212/WNL.0000000000007036
16. Phelan JC, Link BG, Tehranifar P. Social conditions as fundamental causes of health inequalities: theory, evidence, and policy implications. J Health Soc Behav. (2010) 51(1_suppl):S28–40. doi: 10.1177/0022146510383498
17. Thoits PA. Stress and health: major findings and policy implications. J Health Soc Behav. (2010) 51(1_suppl):S41–53. doi: 10.1177/0022146510383499
18. Fujishiro K, MacDonald LA, Crowe M, McClure LA, Howard VJ, Wadley VG. The role of occupation in explaining cognitive functioning in later life: education and occupational complexity in a U.S. National sample of black and white men and women. J Gerontol Series B. (2019) 74(7):1189–99. doi: 10.1093/geronb/gbx112
19. Stebbins RC, Yang YC, Reason M, Aiello AE, Belsky DW, Harris KM, et al. Occupational cognitive stimulation, socioeconomic status, and cognitive functioning in young adulthood. SSM Popul Health. (2022) 17:101024. doi: 10.1016/j.ssmph.2022.101024
20. Calatayud E, Lozano-Berges G, Peralta-Marrupe P, Latorre E, Gomez-Soria I. Job demands may determine cognitive and physical aging after retirement. J Appl Gerontol. (2022) 41(12):2435–46. doi: 10.1177/07334648221120080
21. Gajewski PD, Wild-Wall N, Schapkin SA, Erdmann U, Freude G, Falkenstein M. Effects of aging and job demands on cognitive flexibility assessed by task switching. Biol Psychol. (2010) 85(2):187–99. doi: 10.1016/j.biopsycho.2010.06.009
22. Andel R, Silverstein M, Kåreholt I. The role of midlife occupational complexity and leisure activity in late-life cognition. The J Gerontol B Psychol Sci Soc Sci. (2015) 70(2):314–21. doi: 10.1093/geronb/gbu110
23. Hussenoeder FS, Riedel-Heller SG, Conrad I, Rodriguez FS. Concepts of mental demands at work that protect against cognitive decline and dementia: a systematic review. Am J Health Promot. (2019) 33(8):1200–8. doi: 10.1177/0890117119861309
24. Karp A, Andel R, Parker MG, Wang H-X, Winblad B, Fratiglioni L. Mentally stimulating activities at work during midlife and dementia risk after age 75: follow-up study from the kungsholmen project. Am J Geriatr Psychiatry. (2009) 17(3):227–36. doi: 10.1097/JGP.0b013e318190b691
25. Marquié JC, Duarte LR, Bessières P, Dalm C, Gentil C, Ruidavets JB. Higher mental stimulation at work is associated with improved cognitive functioning in both young and older workers. Ergonomics. (2010) 53(11):1287–301. doi: 10.1080/00140139.2010.519125
26. Nexø MA, Meng A, Borg V. Can psychosocial work conditions protect against age-related cognitive decline? Results from a systematic review. Occup Environ Med. (2016) 73(7):487–96. doi: 10.1136/oemed-2016-103550
27. Vemuri P, Lesnick TG, Przybelski SA, Machulda M, Knopman DS, Mielke MM, et al. Association of lifetime intellectual enrichment with cognitive decline in the older population. JAMA Neurol. (2014) 71(8):1017. doi: 10.1001/jamaneurol.2014.963
28. Fay D, Kamps A. Work characteristics and the emergence of a sustainable workforce: do job design principles matter? Gedrag & Organisatie. (2006) 19(2):184. doi: 10.5117/2006.019.002.006
29. Fisher GG, Stachowski A, Infurna FJ, Faul JD, Grosch J, Tetrick LE. Mental work demands, retirement, and longitudinal trajectories of cognitive functioning. J Occup Health Psychol. (2014) 19(2):231–42. doi: 10.1037/a0035724
30. Pool E, Brosch T, Delplanque S, Sander D. Attentional bias for positive emotional stimuli: a meta-analytic investigation. Psychol Bull. (2016) 142(1):79–106. doi: 10.1037/bul0000026
31. Boots EA, Schultz SA, Oh JM, Larson J, Edwards D, Cook D, et al. Cardiorespiratory fitness is associated with brain structure, cognition, and mood in a middle-aged cohort at risk for Alzheimer’s disease. Brain Imaging Behav. (2015) 9(3):639–49. doi: 10.1007/s11682-014-9325-9
32. Valenzuela MJ, Sachdev P, Wen W, Chen X, Brodaty H. Lifespan mental activity predicts diminished rate of hippocampal atrophy. PLoS One. (2008) 3(7):e2598. doi: 10.1371/journal.pone.0002598
33. Simons RL, Ong ML, Beach SRH, Lei M-K, Philibert R, Mielke MM. Direct and indirect effects of socioeconomic Status and discrimination on subjective cognitive decline: a longitudinal study of African American women. The Journals of Gerontology: Series B. (2023) 78(5):799–808. doi: 10.1093/geronb/gbad029
34. Jester DJ, Kohn JN, Tibiriçá L, Thomas ML, Brown LL, Murphy JD, et al. Differences in social determinants of health underlie racial/ethnic disparities in psychological health and well-being: study of 11,143 older adults. Am J Psychiatry. (2023) 180(7):483–94. doi: 10.1176/appi.ajp.20220158
35. Jester DJ, Palmer BW, Thomas ML, Brown LL, Tibiriçá L, Jeste DV, et al. Impact of educational attainment on time to cognitive decline among marginalized older adults: cohort study of 20,311 adults. J Am Geriatr Soc. (2023) 71(9):2913–23. doi: 10.1111/jgs.18340
36. Pager D, Western B, Sugie N. Sequencing disadvantage: barriers to employment facing young black and white men with criminal records. Ann Am Acad Pol Soc Sci. (2009) 623(1):195–213. doi: 10.1177/0002716208330793
37. Tomaskovic-Devey D, Thomas M, Johnson K. Race and the accumulation of human capital across the career: a theoretical model and fixed-effects application. Am J Sociol. (2005) 111(1):58–89. doi: 10.1086/431779
38. Vaisey S. Education and its discontents: overqualification in America, 1972–2002. Soc Forces. (2006) 85(2):835–64. doi: 10.1353/sof.2007.0028
39. Bailey ZD, Krieger N, Agénor M, Graves J, Linos N, Bassett MT. Structural racism and health inequities in the USA: evidence and interventions. Lancet. (2017) 389(10077):1453–63. doi: 10.1016/S0140-6736(17)30569-X
40. Busch F. Gender segregation, occupational sorting, and growth of wage disparities between women. Demography. (2020) 57(3):1063–88. doi: 10.1007/s13524-020-00887-3
41. Buchmann C, DiPrete TA, McDaniel A. Gender inequalities in education. Annu Rev Sociol. (2008) 34(1):319–37. doi: 10.1146/annurev.soc.34.040507.134719
42. Gerstorf D, Herlitz A, Smith J. Stability of sex differences in cognition in advanced old age: the role of education and attrition. J Gerontol B. (2006) 61(4):245–P249. doi: 10.1093/geronb/61.4.P245
43. Velez BL, Cox R, Polihronakis CJ, Moradi B. Discrimination, work outcomes, and mental health among women of color: the protective role of womanist attitudes. J Couns Psychol. (2018) 65(2):178–93. doi: 10.1037/cou0000274
44. Langa KM. Langa-Weir classification of cognitive function (1995 Onward). Survey Research Center Institute for Social Research, University of Michigan. (2020)).
45. Massey DS. Categorically Unequal: The American Stratification System. New York, NY: Russell Sage Foundation (2007).
46. Adkins-Jackson PB, George KM, Besser LM, Hyun J, Lamar M, Hill-Jarrett TG, et al. The structural and social determinants of Alzheimer’s disease related dementias. Alzheimers Dement. (2023) 19(7):3171–85. doi: 10.1002/alz.13027
47. Joshi P, Hendrie K, Jester DJ, Dasarathy D, Lavretsky H, Ku BS, et al. Social connections as determinants of cognitive health and as targets for social interventions in persons with or at risk of Alzheimer’s disease and related disorders: a scoping review. Int Psychogeriatr. (2024) 36(2):92–118. doi: 10.1017/S1041610223000923
48. Tibiriçá L, Jester DJ, Kohn JN, Williams AP, McEvoy LK, Palmer BW. Perceived discrimination and nativity status: risk of cognitive impairment among Latin American older adults. Int Psychogeriatr. (2023):1–13. doi: 10.1017/S1041610223004374. [Epub ahead of print].
49. The Health and Retirement Study (HRS). (2011). Available online at: https://hrs.isr.umich.edu/
Keywords: cognitive reserve, occupation, gender norms, socioeconomic factors, ethnic minority, aging
Citation: Grewal DK, Patapoff MA, Liou-Johnson V, Adamson MM and Jester DJ (2024) The absence of formal work experience may affect the rate of cognitive decline in older adult women: findings from the health and retirement study. Front. Glob. Womens Health 5:1458553. doi: 10.3389/fgwh.2024.1458553
Received: 2 July 2024; Accepted: 3 September 2024;
Published: 16 September 2024.
Edited by:
Esther Bui, University of Toronto, CanadaReviewed by:
Gabrielle Britton, Instituto de Investigaciones Científicas y Servicios de Alta Tecnología,Panama P. Emanuela Voinescu, Brigham and Women's Hospital and Harvard Medical School, United States
Copyright: © 2024 Grewal, Patapoff, Liou-Johnson, Adamson and Jester. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Daya K. Grewal, ZGdyZXdhbEBwYWxvYWx0b3UuZWR1