
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Glob. Womens Health, 12 July 2024
Sec. Maternal Health
Volume 5 - 2024 | https://doi.org/10.3389/fgwh.2024.1397194
This article is part of the Research TopicInfluence of Intimate Partner Violence and Male Partner Involvement in Maternity Care in Low-and-Middle Income CountriesView all 8 articles
 Lukas Blumrich1*
Lukas Blumrich1* Braian Lucas Aguiar Sousa1Marco Antônio Barbieri2Vanda Maria Ferreira Simões3Antonio Augusto Moura da Silva3Heloisa Bettiol2
Braian Lucas Aguiar Sousa1Marco Antônio Barbieri2Vanda Maria Ferreira Simões3Antonio Augusto Moura da Silva3Heloisa Bettiol2 Alexandre Archanjo Ferraro1
Alexandre Archanjo Ferraro1
Introduction: Psychosocial stress during pregnancy has long-lasting and important consequences in the following generations, as it can affect intrauterine development. The impact on the developing immune system is notoriously important due to the associated morbidity and mortality in the first years of life. Little attention has been given to the role of violence during pregnancy (VDP), especially its impact on infant infectious morbidity.
Methods: We analyzed data from two Brazilian birth cohorts (n = 2,847) in two distinct cities (Ribeirão Preto and São Luís), collected during pregnancy and at the beginning of the second year of life. The association between VDP and infection in infancy was analyzed with structural equation modeling, using the WHO-VAW questionnaire as exposure and a latent variable for infection as the outcome.
Results: VDP was reported by 2.48% (sexual), 11.56% (physical), and 45.90% (psychological) of the mothers. The models presented an adequate fit. In the city of São Luís, VDP was significantly associated with the latent construct for infection (standardized beta = 0.182; p = 0.022), while that was not the case for the Ribeirão Preto sample (standardized beta = 0.113; p = 0.113). Further analyses showed a gradient effect for the different dimensions of the exposure, from psychological to physical and sexual violence.
Conclusion: Our results suggest an association of VDP with infant morbidity in a poorer socioeconomic setting, and highlight the importance of considering the different dimensions of intimate partner violence. These findings may have important implications for the comprehension of global health inequalities and of the effects of gender-based violence.
Maternal psychosocial stress during pregnancy has far-reaching effects on future generations, impacting both immediate and long-term health (1, 2). It affects approximately one-quarter of pregnant women globally (3) and is associated with a wide range of consequences for offspring's health, encompassing perinatal complications as well as long-term conditions including cardiovascular disease, metabolic syndrome, and neuropsychiatric disorders (4, 5).
Stress during pregnancy is a multifaceted concept that encompasses various factors, including depression or anxiety, perceived stress, natural disasters, heat stress, and experiences of discrimination. Although violence during pregnancy is a well-known global issue, it has received relatively less attention as a specific stressor. Given the variety of consequences of intimate partner violence, such as depression, higher perceived stress, and social isolation, it is imperative to investigate its distinct effects to fully comprehend the extent of the negative consequences associated with gender-based violence (6).
Studying violence during pregnancy presents numerous challenges, including obtaining reliable data and discerning its specific impacts. Additionally, the influence of environmental factors, such as socioeconomic status (3, 7) and culture (8, 9) (e.g., perceptions of intimate partner violence within relationship dynamics) remains unclear. Considering the complexity of a phenomenon such as intimate partner violence, it is likely that the impacts of violence vary across different populations (10, 11).
The wide-ranging consequences of maternal violence on offspring should not be underestimated. Extensive evidence indicates its association with maternal morbidity during (12–14) and after (14, 15) pregnancy, premature birth (16, 17), low birth weight (16–18), intrauterine growth restriction (19), undernutrition (20), infectious morbidity (21, 22), delayed neurodevelopment (23), and higher mortality (24). More recently, some studies have investigated the effects of prenatal violence on infectious morbidity in the offspring. Most of the studies that sought to clarify this relation used national surveys and evaluated the association between the lifetime occurrence of violence and specific morbid conditions in children at variable ages (22, 25–29).
To the best of our knowledge, the investigation of violence during pregnancy and its effects on infant morbidity of offspring in humans was done by only one study (30). Expanding these investigations is important to adequately comprehend the extent of the negative effects of violence, and to identify potential intervention targets for offspring morbidity and mortality.
There are a number of possible biological pathways for psychosocial stress and violence to impact on the development of the immune system, such as disruption of corticosteroid dynamics (31, 32), impaired transference of passive immunity, and changes in the gut microbiome (33). The first one could give rise to a suppressed immune response in the infant (34, 35) and disrupt thymus development (36), while changes in placental antibody transfer (37) could be deleterious at the beginning of the infant's life. Since the gut microbiota participates in the regulation of inflammatory processes, its disruption by stress could be detrimental, and stress during pregnancy may even influence the whole composition of the offspring's own intestinal microbiota (33, 37).
This study sought to investigate the association of violence during pregnancy with infant infectious morbidity in two Brazilian birth cohorts from cities with markedly different socioeconomic contexts.
This is an observational study using data from the cohort “Etiological Factors of Preterm Birth and Consequences of Perinatal Factors for Child Health: Brazilian Birth Cohort Study of Ribeirão Preto and São Luís (BRISA)” (38).
We analyzed the data from the birth cohorts of the cities Ribeirão Preto and São Luís, collected at three distinct waves (prenatal, perinatal, and postnatal, during the second year of infants’ life). The BRISA cohort study began data collection in 2010.
Ribeirão Preto is a wealthy and industrialized city in the State of São Paulo, with a Human Development Index (HDI) of 0.800, 604,682 inhabitants, of which 2.53% are below the poverty line, and a per capita income of USD 730.02 as of 201 0 (39). More than 99% of the residences receive piped water and more than 98% are equipped with sanitary sewage (40). São Luís is the capital of the State of Maranhão, in one of the poorest regions in the country, with a HDI of 0.768, 1.014.837 inhabitants, 13.81% below the poverty line, and a per capita income of USD 447.42 (39). 82% of residents have access to piped water, while only 45.7% were equipped with sanitary sewage as of 2010 (40).
A convenience sample was used in both cities. Pregnant women were identified in hospitals and health units on the occasion of a prenatal visit, and women with singleton pregnancies who had undergone an obstetrical ultrasound during the first trimester of gestation were invited to participate. The sample of São Luís consisted of 1.447 pregnant women, interviewed initially, from February 2010 to June 2011, while Ribeirão Preto had 1.400 subjects, interviewed between February 2010 and February 2011.
Interviews were held between the 22nd and the 25th week of pregnancy by a previously trained team to collect data on reproductive health, demographic and socioeconomic status, details of pregnancy, and life habits of the mothers. In Ribeirão Preto, data were collected at the Clinical Research Unit of the University Hospital, University of São Paulo, while in São Luís data were collected at the Clinical Research Center of the Mother-Child Unit of the University Hospital in São Luís.
Immediately after childbirth (i.e., in the period of 24 h after birth), interviews were conducted by teams of trained collaborators in maternity homes in both cities, collecting information about mothers and babies using standardized questionnaires. All team members were trained to perform data collection.
A new evaluation was conducted at the beginning of the second year of the infant's life, with age ranging from 12 to 36 months (median age was 18 months). Interviews were again conducted at University Hospitals in both cities, with standardized questionnaires about child's health and medical events, as described below.
All phases of the study were approved by the Research Ethics Committee of the University Hospital of the Ribeirão Preto Medical School/University of São Paulo (protocol 4116/2008) and the University Hospital of Federal University of Maranhão (protocol 4771/2008-30). All mothers who participated in the project signed the free and informed consent form after reading and understanding the project's aim and methods. Trained professionals helped to clarify information on the consent form when needed.
The sample size for the city of Ribeirão Preto was 1,400, while the sample size for São Luís was 1,447 dyads.
The chosen exposure was violence suffered during pregnancy, measured by the WHO Violence Against Women Questionnaire (41). We analyzed this data using a previously validated latent variable based on the first 13 questions of the questionnaire (42) (4 for the psychological, 6 for the physical, and 3 for the sexual dimension of violence).
The chosen outcome was built as a latent construct for the morbidity of the infant, derived from the following variables, obtained during the second-year interview with the mother: occurrence of fever in the last 2 weeks, occurrence of diarrhea in the last 2 weeks, and use of anti-inflammatory medication in the last 2 weeks, use of antibiotic medication in the last 2 weeks. The latent construct was analyzed as a continuous variable.
Additional variables, recognized as potential confounders, were also collected. These confounders were identified using a theoretical framework constructed using Direct Acyclic Graph Methodology (DAG) from the dagitty software (43). The identified confounders were: maternal age, marital situation, social support and support networks, maternal education, maternal occupation, and family income. The last three variables were used to build a latent construct for socioeconomic status, and added as a confounder in the model. Maternal age was analyzed as a continuous variable, while marital situation was categorized as married, living together, single or divorced/widowed. Social support and support networks were measured by the Medical Outcomes Study (MOS) Social Support survey (44), and analyzed as continuous (45). All of the instruments were administered in Brazilian Portuguese following transcultural adaptation, as reported in the original description of the birth cohort (38).
Categorical variables were described using absolute and relative frequencies. Continuous variables were described using mean and standard deviation.
Structural equation modelling was performed in MPlus Software (46) using the Weighted Least Square Mean and Variance (WLSMV) estimator and theta parameterization, in order to obtain adequate control for residual differences in variances. Models results were standardized. We expected the following results for model fit, based on previous research (47, 48): a value of RMSEA (Root Mean Square Error of Approximation) <0.08, CFI (Comparative Fit Index) >= 0.90 and TLI (Tucker-Lewis Index) >= 0.95; and a WRMR (Weighted Root Mean Squared Residual) value of <1.0. Ideally, p-value estimates for model fit should be above a value of 0.05. Considering our sample sizes, however, this metric is not expected to be attained and does not importantly impact model fit when other parameters are adequate.
Data was analyzed separately for each city, as we believe they constitute different populations and one of the study’s goals was to evaluate the relationship between exposure and outcome in different socioeconomic contexts.
The structural equations models constructed with the latent variables and the confounders fitted the data adequately, as shown in Table 1. The Weighted Root Mean Squared Residuals (WRMR) for both models were higher than 1.0, but, since this index is experimental and the other indexes indicate a very good fit, both models were considered adequate.
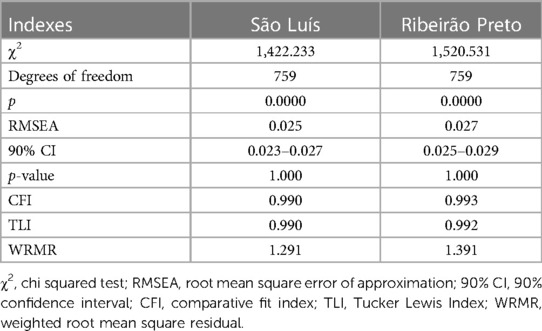
Table 1 Model fit for the structural equation models of association between violence during pregnancy and fever in the last 2 weeks in two birth cohorts in distinct cities (Ribeirão Preto and São Luís).
The descriptive statistics presented in Table 2 show important differences between the two cohorts. Maternal age was very similar for both cities, but the São Luís sample had almost two times as many non-skilled workers as Ribeirão Preto (19,70% vs. 10,40%, p < 0.001) and lower income (p < 0.001). Maternal educational level in São Luís saw more women completing the secondary level, but tertiary levels were very similar between the cities. As for marital status, Ribeirão Preto saw a higher rate of formally married women, but both cities had similar frequencies of single or divorced/widowed women.
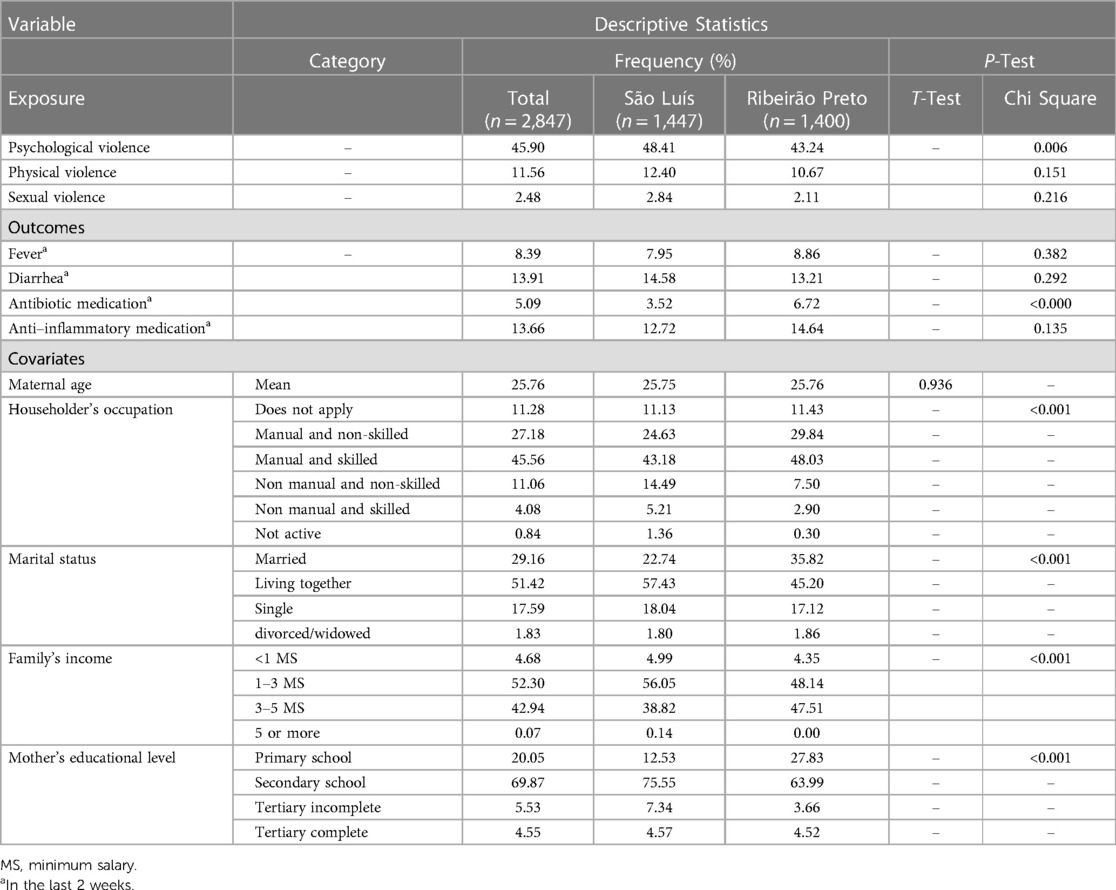
Table 2 Description of the sample characteristics of two birth cohorts from Brazilian cities [São Luís (n = 1,447) and Ribeirão Preto (n = 1,400)] in 2010.
As for the violence exposure during pregnancy, mothers in São Luís reported psychological violence (as understood as any affirmative response in the items related to psychological violence in the WHO questionnaire) more frequently than mothers in Ribeirão Preto (48.41% vs. 43.24%, p = 0.006). Fever in the last 2 weeks has a similar frequency in both cities, of 7.95% and 8.86%, (p = 0.382), respectively. Diarrhea saw a similar distribution (p = 0.292). While in São Luís 3.52% of the mothers reported at the use of antibiotic medication two weeks prior to the interview, in Ribeirão Preto this rate was 6.72% (p < 0.001), and the use of anti-inflammatory medication was similar in both cities.
Our analysis show (Table 3) that violence during pregnancy was associated with infant morbidity in the city of São Luís (standardized beta = 0.182, p = 0.022) but not in the city of Ribeirão Preto (stardardized beta = 0.113, p = 0.113). In the city of São Luís, given the results found, we conducted a post-hoc analysis for each dimension of violence (psychological, physical, and sexual) separately as the exposure (Table 4). Effect sizes tended to increase as it would be expected in the case of a gradient effect (psychological violence beta = 0.053, p = 0.405; physical violence beta = 0.115, p = 0.220; sexual violence beta = 0.428, p < 0.001), but only the sexual violence was found to be statistically significantly associated with infant morbidity.
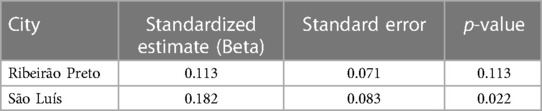
Table 3 Standardized model results (STDYX) for the latent variable for infection on latent variable for violence.
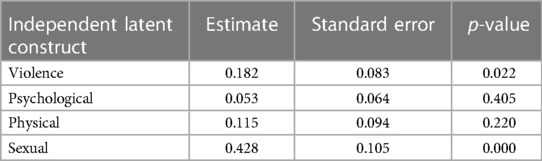
Table 4 Standardized model results for the regression of the latent variable for infection different levels of the latent variable for violence in the city of São luis.
Our results suggest a context-specific effect for violence during pregnancy on infant morbidity, as measured by fever, diarrhea, or use of antibiotic or anti-inflammatory medication in the last two weeks. This association was present in the city of São Luís, but could not be detected in the city of Ribeirão Preto, and saw a gradient effect with increasing effect sizes when considering the psychological, physical, and sexual dimensions of violence.
Considering the distinct socioeconomic characteristics of the two cities, the impact of violence during pregnancy was observed exclusively within the population living in the city with lower socioeconomic status. São Luís, in comparison to Ribeirão Preto, displayed significantly lower levels of human development, as evidenced by a notably lower Human Development Index (HDI) score (0.768, ranking 249th in Brazil) compared to Ribeirão Preto's higher HDI score (0.800, ranking 40th). Additionally, São Luís exhibited lower per capita income (USD 447.42) (39) compared to Ribeirão Preto (USD 730.02) (40) at the time of data collection.
Albeit some statistically significant differences could be noted between the two samples (Table 1), the samples share very similar characteristics overall and the São Luis sample presented higher levels of maternal education. This holds substantial implications, as it suggests a systemic or contextual effect for socioeconomic status (SES). Considering the similarities in the SES of both samples, the finding limited to the city of São Luís can be plausibly explained by the differences in health service quality and access to adequate healthcare and education between the two cities. The suggestion that some negative effects of pregnancy exposures may only be detected in harsher systemic socioeconomic conditions can contribute to a better understanding of health disparities and challenges, both prevalent in the Global South.
This context-specific effect may explain the results of Manzolli et al. (30), that found no association between prenatal exposure to violence and diarrhea or respiratory infection in infancy. This study, the only other one to evaluate the effects of violence during pregnancy on infant morbidity, was conducted in the southern region of Brazil. The socioeconomic conditions in the cities where data was collected for their study are much more similar to Ribeirão Preto than to São Luís, and thus are in line with our findings.
The presence of a gradient effect observed across various dimensions of violence, as assessed using the WHO instrument, provides compelling evidence supporting the association under investigation. While no statistically significant association was found when considering psychological and physical violence individually, the statistically significant findings obtained when considering all dimensions collectively may suggest insufficient statistical power due to the inclusion of many confounding variables with complex interrelationships in our structural equation models.
Notably, a substantial standardized effect size was observed for sexual violence, emphasizing the significance of incorporating this dimension of violence in analyses. To the best of our knowledge, no prior studies have specifically examined the effects of sexual violence during pregnancy on longer term offspring heath (i.e., later than the neonatal period). Considering how common forced intercourse is worldwide (49) and how sexual violence is a sexual manifestation of gender-based violence (50), our findings underscore the importance of including this dimension in future research to comprehensively understand the complete range of detrimental effects resulting from violence.
The biological mechanisms possibly responsible for this association are not completely understood. A well-stablished hypothesis concerns the importance of cortisol in fetal development (31, 32). The 11β-HSD2 enzyme in the placenta has a protective function, converting most of the maternal cortisol that reaches fetal circulation into the inactive cortisone (51). Stressed mothers, however, in addition to presenting higher levels of circulating cortisol, may have impaired function of this enzyme, leading to a higher exposure of the fetus to cortisol during development (32, 37). This exposure in turn may modulate immune system development and function, mainly through programming of the hypothalamic-pituitary-adrenocortical axis of the fetus (32, 51). It was also previously suggested that the diminished function of the mother's immune system due to exposure to higher levels of glucocorticoids may impair the transplacental transfer of passive immunity (32). Another proposed mechanism suggests the role of the microbial gut on the development of the immune function of the offspring, since altered patterns of colonization are related to maternal stress during pregnancy and these may have a range of consequences (33, 52).
It is also important to consider how the experience of violence can be an obstacle for access to adequate healthcare (53). Women who experience intimate partner violence are less likely to attend adequate prenatal care, and may be less prone to search for healthcare in case of illness (53, 54). Households with the experience of violence, for this reason, may be chronically at a higher risk for morbidity. The first observation may induce a selection bias in our study, since mothers were recruited at a prenatal care appointment. Since in the Brazilian healthcare system there is an active strategy for screening and following up pregnant women, however, we believe this possible bias does not significantly impact our findings. Having less access to healthcare in general, however, is another potential explanation for increased offspring morbidity. Mothers who experience high levels of stress may also have impaired ability to perceive children's worsened health conditions, and, since our outcomes were based on mothers’ recall ability, this could underestimate the effect size we found. There is no available research on this phenomenon, and it remains an assumption.
Considering the theoretical model constructed for this analysis (Figure 1), we believe there is also the possibility of a behavioral pathway that may be partially responsible for the association here analyzed. The violence during pregnancy may impair a woman's ability to adequately care for herself as manifested in, for example, not attending healthcare appointments or searching for help when in need (54, 55). Violence during pregnancy may also impair the quality of the bond between mother and offspring, and it is reported that breastfeeding may be importantly affected by the experience of violence (56–58). The same applies for maternal mental health during and after pregnancy and substance use (58–61). All these factors may be directly related to child's health, and thus may act as mediators (62) of this relationship.
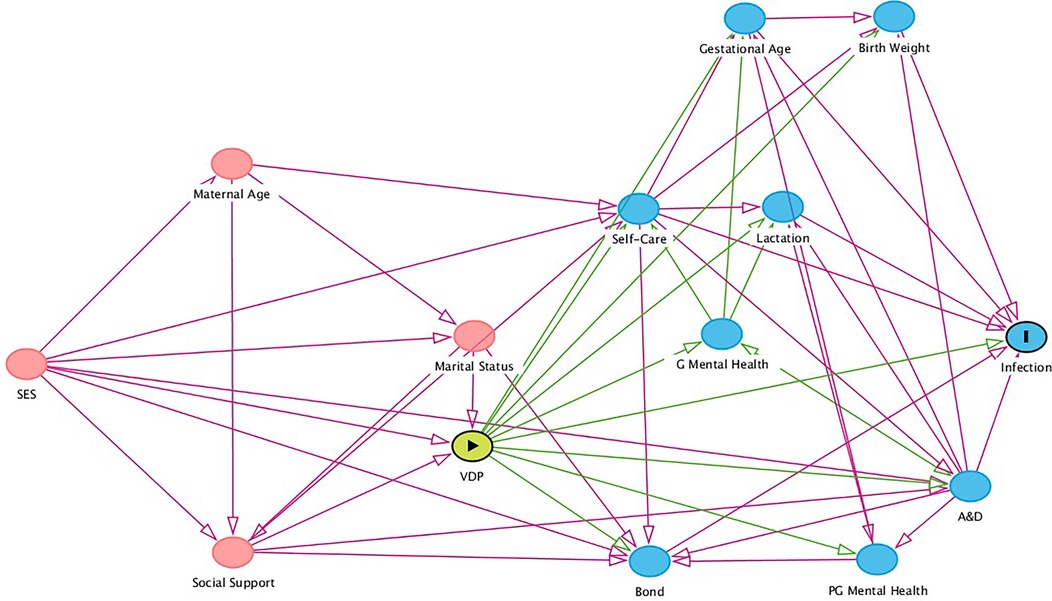
Figure 1 Directed acyclic graph (DAG) depicting the epidemiological model for the association between violence during pregnancy and fever in infancy. SES, Socioeconomic Status; VDP, Violence During Pregnancy; G Mental Health, Mother's Mental Health during Pregnancy; A&D, Alcohol and Drugs use during Pregnancy; Bond, Maternal-infant Bonding; PG Mental Health, Mother's Mental Health Post Pregnancy. Variables in red are ancestral variables of both exposure and outcome, and thus are recognized as confounders in the theoretical model. Variables in blue are recognized as mediators of the relationship between exposure and outcome in the model.
Our findings highlight the importance of thorough screening for violence against pregnant women and the importance of a gender and equity-based perspective in prenatal care. The impact of VDP for the infants’ health has already been established (6), but our findings may shed light on outcomes previously ignored. It may also add more weight to the benefits of violence screening recommendations (5, 63, 64). Efforts to mitigate the impact of violence should be made, such as devoting more time to understand each patient's context and discussing which are the possibilities for social and legal support (65, 66). The pathways through which it acts shall be the object of future studies, but as we understand it as a psychosocial stressor, already established strategies may be useful, such as group therapy, referral to social service professionals, empowering women to recognize and seek their rights and resources available to face situations of violence (66).
The strengths of our study include the use of the DAG methodology and the inclusion of a diversity of confounders in our models. Considering the array of confounders identified with the DAG methodology and included in the model, there is hardly an unmeasured confounder that could explain away this association. All the data was collected using validated instruments and using a standardized methodology. Our sample included populations from markedly different socioeconomic and cultural backgrounds, but who share the same language and political system, and thus comparisons are possible.
Some limitations should be noted. The first and most important is the underestimation of the violence suffered by the subjects included, mostly due to fear of retaliation or judgment. To minimize this possibility, all the interviewers were received previous training directed at collecting information about violence. The second is the memory bias present in the data here analyzed, as the sole source of information for each variable was the interviewed mother. For this reason, we chose to use a latent variable as the outcome for this analysis, since the variables used for its construction present complementary information on child morbidity. Lastly, the methodology used for sampling does not allow the generalization of results, but provides very strong internal validity for the study of the mechanisms of disease.
The results here presented suggest an important association of violence during pregnancy and infant morbidity in the second year of life in a harsher socioeconomic setting. Moreover, a gradient effect for the different dimensions of violence was observed. Considering the ubiquity of violence against women, these findings may have important implications for public health and for the comprehension of global health inequalities. Furthermore, they underscore the pressing need for comprehensive efforts to address gender-based violence on a global scale.
The datasets presented in this article are not readily available because the data here analyzed is the property of the RPS Consortium, and questions or requests can be directed to the corresponding author for the correct referral. Requests to access the datasets should be directed to Lukas Blumrich,bHVrYXMuYmx1bXJpY2hAZm0udXNwLmJy.
This study was approved by the Research Ethics Committee of the University Hospital of the Ribeirão Preto Medical School/University of São Paulo (protocol 4116/2008) and the Research Ethics Committee of University Hospital of Federal University of Maranhão (protocol 4771/2008-30). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
LB: Conceptualization, Formal Analysis, Methodology, Writing – original draft, Writing – review & editing. BS: Conceptualization, Writing – review & editing. MB: Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Writing – review & editing. VS: Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Writing – review & editing. AS: Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Writing – review & editing. HB: Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Writing – review & editing. AF: Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
This project received the financial support from the Brazilian funding agencies Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq, process 471923/2011-7; 561058/2015-5; Finance Code 001), Fundação de Amparo à Pesquisa do Estado do Maranhão (FAPEMA, process 0035/2008), and Fundação de Pesquisa de São Paulo (FAPESP; process 2008-53593-0; 2020/12265-2) through the BRISA project.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Bleker LS, de Rooij SR, Roseboom TJ. Prenatal psychological stress exposure and neurodevelopment and health of children. Int J Environ Res Public Health. (2019) 16(19):3657. doi: 10.3390/ijerph16193657
2. Fitzgerald E, Hor K, Drake AJ. Maternal influences on fetal brain development: the role of nutrition, infection and stress, and the potential for intergenerational consequences. Early Hum Dev. (2020) 150:105190. doi: 10.1016/j.earlhumdev.2020.105190
3. Román-Gálvez RM, Martín-Peláez S, Fernández-Félix BM, Zamora J, Khan KS, Bueno-Cavanillas A. Worldwide prevalence of intimate partner violence in pregnancy. A systematic review and meta-analysis. Front Public Health. (2021) 9:738459. doi: 10.3389/fpubh.2021.738459
4. Román-Gálvez RM, Martín-Peláez S, Martínez-Galiano JM, Khan KS, Bueno-Cavanillas A. Prevalence of intimate partner violence in pregnancy: an umbrella review. Int J Environ Res Public Health. (2021) 18(2):707. doi: 10.3390/ijerph18020707
5. Chisholm CA, Bullock L, Ferguson JEJ. Intimate partner violence and pregnancy: epidemiology and impact. Am J Obstet Gynecol. (2017) 217(2):141–4. doi: 10.1016/j.ajog.2017.05.042
6. Agarwal S, Prasad R, Mantri S, Chandrakar R, Gupta S, Babhulkar V, et al. A comprehensive review of intimate partner violence during pregnancy and its adverse effects on maternal and fetal health. Cureus. (2023) 15(5):e39262. doi: 10.7759/cureus.39262
7. Zhao Q, Huang Y, Sun M, Li Y, Lommel LL. Risk factors associated with intimate partner violence against Chinese women: a systematic review. Int J Environ Res Public Health. (2022) 19(23):16258. doi: 10.3390/ijerph192316258
8. Shaw B, Stevanovic-Fenn N, Gibson L, Davin C, Chipanta NSK, Lubin AB, et al. Shifting norms in faith communities to reduce intimate partner violence: results from a cluster randomized controlled trial in Nigeria. J Interpers Violence. (2023) 16:8862605231176799. doi: 10.1177/08862605231176799
9. Li Y, Dong F, Bullock LFC, Bloom T. “Get stuck and can’t walk out”: exploring the needs for support among Chinese immigrant women experiencing intimate partner violence in the United States. Violence Vict. (2023) 38(1):95–110. doi: 10.1891/VV-2022-0011
10. Prasad SS, Bidwell JT, Murray-García JL. Impacts of culture on perceptions of intimate partner violence among Fijian Indian women in the United States. J Forensic Nurs. (2023) 19(2):122–30. doi: 10.1097/JFN.0000000000000440
11. Mj L, Mh S RC, T M DR, B P. A comparative analysis of gender discrepancy stress, attitudes toward intimate partner violence, and perpetration among young adults in the USA and Uganda. Int J Environ Res Public Health. (2022) 19(20):13373. doi: 10.3390/ijerph192013373
12. Moraes CL, Amorim AR, Reichenheim ME. Gestational weight gain differentials in the presence of intimate partner violence. Int J Gynaecol Obstet Off Organ Int Fed Gynaecol Obstet. (2006) 95(3):254–60. doi: 10.1016/j.ijgo.2006.08.015
13. Rao N, Norris Turner A, Harrington B, Nampandeni P, Banda V, Norris A. Correlations between intimate partner violence and spontaneous abortion, stillbirth, and neonatal death in Rural Malawi. Int J Gynaecol Obstet Off Organ Int Fed Gynaecol Obstet. (2017) 138(1):74–8. doi: 10.1002/ijgo.12173
14. Alhusen JL, Ray E, Sharps P, Bullock L. Intimate partner violence during pregnancy: maternal and neonatal outcomes. J Womens Health. (2015) 24(1):100–6. doi: 10.1089/jwh.2014.4872
15. Ankerstjerne LBS, Laizer SN, Andreasen K, Normann AK, Wu C, Linde DS, et al. Landscaping the evidence of intimate partner violence and postpartum depression: a systematic review. BMJ Open. (2022) 12(5):e051426. doi: 10.1136/bmjopen-2021-051426
16. Belay HG, Debebe GA, Ayele AD, Kassa BG, Mihretie GN, Bezabih LM, et al. Intimate partner violence during pregnancy and adverse birth outcomes in Ethiopia: a systematic review and meta-analysis. PLoS One. (2022) 17(12):e0275836. doi: 10.1371/journal.pone.0275836
17. Hill A, Pallitto C, McCleary-Sills J, Garcia-Moreno C. A systematic review and meta-analysis of intimate partner violence during pregnancy and selected birth outcomes. Int J Gynaecol Obstet Off Organ Int Fed Gynaecol Obstet. (2016) 133(3):269–76. doi: 10.1016/j.ijgo.2015.10.023
18. Lin CH, Lin WS, Chang HY, Wu SI. Domestic violence against pregnant women is a potential risk factor for low birthweight in full-term neonates: a population-based retrospective cohort study. PLoS One. (2022) 17(12):e0279469. doi: 10.1371/journal.pone.0279469
19. Lobato G, Reichenheim ME, Moraes CL, Peixoto-Filho FM, Migowski LS. Psychologic intimate partner violence and the risk of intrauterine growth restriction in rio de janeiro. Int J Gynaecol Obstet Off Organ Int Fed Gynaecol Obstet. (2018) 143(1):77–83. doi: 10.1002/ijgo.12393
20. Rahman M, Poudel KC, Yasuoka J, Otsuka K, Yoshikawa K, Jimba M. Maternal exposure to intimate partner violence and the risk of undernutrition among children younger than 5 years in Bangladesh. Am J Public Health. (2012) 102(7):1336–45. doi: 10.2105/AJPH.2011.300396
21. MacGinty R, Lesosky M, Barnett W, Nduru PM, Vanker A, Stein DJ, et al. Maternal psychosocial risk factors and lower respiratory tract infection (LRTI) during infancy in a South African birth cohort. PLoS One. (2019) 14(12):e0226144. doi: 10.1371/journal.pone.0226144
22. Bintabara D, Kibusi SM. Intimate partner violence victimization increases the risk of under-five morbidity: a stratified multilevel analysis of pooled Tanzania demographic health surveys, 2010–2016. PLoS One. (2018) 13(8):e0201814. doi: 10.1371/journal.pone.0201814
23. Toso K, de Cock P, Leavey G. Maternal exposure to violence and offspring neurodevelopment: a systematic review. Paediatr Perinat Epidemiol. (2020) 34(2):190–203. doi: 10.1111/ppe.12651
24. Yaya S, Odusina EK, Adjei NK, Uthman OA. Association between intimate partner violence during pregnancy and risk of preterm birth. BMC Public Health. (2021) 21(1):1610. doi: 10.1186/s12889-021-11625-8
25. Nakphong MK, von Ehrenstein OS. Intimate partner violence and childhood illnesses in Cambodia: a cross-sectional study. Arch Dis Child. (2020) 105(3):223–8. doi: 10.1136/archdischild-2019-317663
26. Paul P, Mondal D. Maternal experience of intimate partner violence and its association with morbidity and mortality of children: evidence from India. PLoS One. (2020) 15(4):e0232454. doi: 10.1371/journal.pone.0232454
27. Silverman JG, Decker MR, Gupta J, Kapur N, Raj A, Naved RT. Maternal experiences of intimate partner violence and child morbidity in Bangladesh: evidence from a national Bangladeshi sample. Arch Pediatr Adolesc Med. (2009) 163(8):700–5. doi: 10.1001/archpediatrics.2009.115
28. Ferdousy EZ, Matin MA. Association between intimate partner violence and child morbidity in south Asia. J Health Popul Nutr. (2015) 33(1):16. doi: 10.1186/s41043-015-0016-y
29. Chilanga E, Collin-Vézina D, MacIntosh H, Mitchell C, Cherney K. Prevalence and determinants of malaria infection among children of local farmers in Central Malawi. Malar J. (2020) 19(1):308. doi: 10.1186/s12936-020-03382-7
30. Manzolli P, Nunes MA, Schmidt MI, Ferri CP. Abuse against women, depression, and infant morbidity: a primary care cohort study in Brazil. Am J Prev Med. (2012) 43(2):188–95. doi: 10.1016/j.amepre.2012.04.013
31. Marques AH, Bjørke-Monsen AL, Teixeira AL, Silverman MN. Maternal stress, nutrition and physical activity: impact on immune function, CNS development and psychopathology. Brain Res. (2015) 1617:28–46. doi: 10.1016/j.brainres.2014.10.051
32. Reynolds RM. Glucocorticoid excess and the developmental origins of disease: two decades of testing the hypothesis–2012 curt richter award winner. Psychoneuroendocrinology. (2013) 38(1):1–11. doi: 10.1016/j.psyneuen.2012.08.012
33. Yeramilli V, Cheddadi R, Shah J, Brawner K, Martin C. A review of the impact of maternal prenatal stress on offspring microbiota and metabolites. Metabolites. (2023) 13(4):535. doi: 10.3390/metabo13040535
34. O'Connor TG, Winter MA, Hunn J, Carnahan J, Pressman EK, Glover V, et al. Prenatal maternal anxiety predicts reduced adaptive immunity in infants. Brain Behav Immun. (2013) 32:21–8. doi: 10.1016/j.bbi.2013.02.002
35. Riis JL, Granger DA, Woo H, Voegtline K, DiPietro JA, Johnson SB. Long-term associations between prenatal maternal cortisol and child neuroendocrine-immune regulation. Int J Behav Med. (2020) 27(3):267–81. doi: 10.1007/s12529-019-09814-2
36. Marques AH, O’Connor TG, Roth C, Susser E, Bjørke-Monsen AL. The influence of maternal prenatal and early childhood nutrition and maternal prenatal stress on offspring immune system development and neurodevelopmental disorders. Front Neurosci. (2013) 7:120. doi: 10.3389/fnins.2013.00120
37. Beijers R, Buitelaar JK, de Weerth C. Mechanisms underlying the effects of prenatal psychosocial stress on child outcomes: beyond the HPA axis. Eur Child Adolesc Psychiatry. (2014) 23(10):943–56. doi: 10.1007/s00787-014-0566-3
38. da Silva AAM, Simões VMF, Barbieri MA, Cardoso VC, Alves CMC, Thomaz EBAF, et al. A protocol to identify non-classical risk factors for preterm births: the Brazilian ribeirão preto and são luís prenatal cohort (BRISA). Reprod Health. (2014) 11(1):79. doi: 10.1186/1742-4755-11-79
39. Atlas Brasil. Available online at: http://www.atlasbrasil.org.br/consulta/planilha (Accessed August 7, 2021).
40. SNIS - Diagnóstico dos Serviços de Água e Esgotos. (2010). (Accessed July 20, 2023). Available online at: http://antigo.snis.gov.br/diagnostico-anual-agua-e-esgotos/diagnostico-ae-2010
41. García-Moreno C, Jansen HA, Ellsberg M, Heise L, Watts C. WHO Multi-Country Study on Women's Wealth and Domestic Violence Against Women: Summary Report. Geneva, Switzerland: World Health Organization (2005). Available online at: https://www.who.int/publications/i/item/9241593512 (Accessed July 08, 2024).
42. Ribeiro MRC, de Britto e Alves MTSS, Batista RFL, Ribeiro CCC, Schraiber LB, Barbieri MA, et al. Confirmatory factor analysis of the WHO violence against women instrument in pregnant women: results from the BRISA prenatal cohort. PLoS One. (2014) 9(12):e115382. doi: 10.1371/journal.pone.0115382
43. Textor J, van der Zander B, Gilthorpe MS, Liśkiewicz M, Ellison GT. Robust causal inference using directed acyclic graphs: the R package ‘dagitty.’. Int J Epidemiol. (2016) 45(6):1887–94. doi: 10.1093/ije/dyw341
44. Sherbourne CD, Stewart AL. The MOS social support survey. Soc Sci Med 1982. (1991) 32(6):705–14. doi: 10.1016/0277-9536(91)90150-b
45. Ribeiro MRC, da Silva AAM, de Britto e Alves MTSS, Batista RFL, Ribeiro CCC, Schraiber LB, et al. Effects of socioeconomic status and social support on violence against pregnant women: a structural equation modeling analysis. PLoS One. (2017) 12(1):e0170469. doi: 10.1371/journal.pone.0170469
47. Hooper D, Coughlan J, Mullen M. Structural equation modeling: guidelines for determining model fit. Electron J Bus Res Methods. (2008) 6(1):53–60. doi: 10.21427/D7CF7R
48. Kline RB. Principles and Practice of Structural Equation Modeling. 2nd edn. New York: Guilford Publications (2005).
49. Sardinha L, Maheu-Giroux M, Stöckl H, Meyer SR, García-Moreno C. Global, regional, and national prevalence estimates of physical or sexual, or both, intimate partner violence against women in 2018. Lancet. (2022) 399(10327):803–13. doi: 10.1016/S0140-6736(21)02664-7
50. Giugliani C, Ruschel AE, Patuzzi GC, da Silva MCB. Violência Sexual e Direito ao Aborto Legal no Brasil: Fatos e Reflexões. Rio de Janeiro: SciELO-Editora FIOCRUZ (2021). doi: 10.7476/9786557081099
51. Zijlmans MAC, Beijers R, Riksen-Walraven MJ, de Weerth C. Maternal late pregnancy anxiety and stress is associated with children’s health: a longitudinal study. Stress. (2017) 20(5):495–504. doi: 10.1080/10253890.2017.1348497
52. Jašarević E, Bale TL. Prenatal and postnatal contributions of the maternal microbiome on offspring programming. Front Neuroendocrinol. (2019) 55:100797. doi: 10.1016/j.yfrne.2019.100797
53. Papas L, Hollingdrake O, Currie J. Social determinant factors and access to health care for women experiencing domestic and family violence: qualitative synthesis. J Adv Nurs. (2023) 79(5):1633–49. doi: 10.1111/jan.15565
54. Robinson L, Spilsbury K. Systematic review of the perceptions and experiences of accessing health services by adult victims of domestic violence. Health Soc Care Community. (2008) 16(1):16–30. doi: 10.1111/j.1365-2524.2007.00721.x
55. Hollingdrake O, Saadi N, Alban Cruz A, Currie J. Qualitative study of the perspectives of women with lived experience of domestic and family violence on accessing healthcare. J Adv Nurs. (2023) 79(4):1353–66. doi: 10.1111/jan.15316
56. Moraes CL, de Oliveira AS, Reichenheim ME, Lobato G. Severe physical violence between intimate partners during pregnancy: a risk factor for early cessation of exclusive breast-feeding. Public Health Nutr. (2011) 14(12):2148–55. doi: 10.1017/S1368980011000802
57. Chaves K, Eastwood J, Ogbo FA, Hendry A, Jalaludin B, Khanlari S, et al. Intimate partner violence identified through routine antenatal screening and maternal and perinatal health outcomes. BMC Pregnancy Childbirth. (2019) 19(1):357. doi: 10.1186/s12884-019-2527-9
58. Tran LM, Nguyen PH, Naved RT, Menon P. Intimate partner violence is associated with poorer maternal mental health and breastfeeding practices in Bangladesh. Health Policy Plan. (2020) 35(Supplement_1):i19–29. doi: 10.1093/heapol/czaa106
59. Zhang S, Wang L, Yang T, Chen L, Qiu X, Wang T, et al. Maternal violence experiences and risk of postpartum depression: a meta-analysis of cohort studies. Eur Psychiatry. (2019) 55:90–101. doi: 10.1016/j.eurpsy.2018.10.005
60. Barcelona de Mendoza V, Harville EW, Savage J, Giarratano G. Experiences of intimate partner and neighborhood violence and their association with mental health in pregnant women. J Interpers Violence. (2018) 33(6):938–59. doi: 10.1177/0886260515613346
61. Almeida CP, Cunha FF, Pires EP, Sá E. Common mental disorders in pregnancy in the context of interpartner violence. J Psychiatr Ment Health Nurs. (2013) 20(5):419–25. doi: 10.1111/j.1365-2850.2012.01937.x
62. Farland LV, Correia KFB, Dodge LE, Modest AM, Williams PL, Smith LH, et al. The importance of mediation in reproductive health studies. Hum Reprod Oxf Engl. (2020) 35(6):1262–6. doi: 10.1093/humrep/deaa064
63. O’Doherty L, Hegarty K, Ramsay J, Davidson LL, Feder G, Taft A. Screening women for intimate partner violence in healthcare settings. Cochrane Database Syst Rev. (2015) 7:CD007007. doi: 10.1002/14651858.CD007007.pub3
64. World Health Organization. Responding to Intimate Partner Violence and Sexual Violence Against Women: WHO Clinical and Policy Guidelines. Geneva: World Health Organization (2013). Available online at: http://www.ncbi.nlm.nih.gov/books/NBK174250/ (Accessed July 24, 2023).
65. Sapkota D, Baird K, Saito A, Anderson D. Interventions for reducing and/or controlling domestic violence among pregnant women in low- and middle-income countries: a systematic review. Syst Rev. (2019) 8(1):79. doi: 10.1186/s13643-019-0998-4
Keywords: domestic violence, intimate partner violence, gender-based violence, infection, infancy
Citation: Blumrich L, Sousa BLA, Barbieri MA, Simões VMF, da Silva AAM, Bettiol H and Ferraro AA (2024) Intergenerational consequences of violence: violence during pregnancy as a risk factor for infection in infancy. Front. Glob. Womens Health 5:1397194. doi: 10.3389/fgwh.2024.1397194
Received: 7 March 2024; Accepted: 27 June 2024;
Published: 12 July 2024.
Edited by:
Guy-Lucien Whembolua, University of Cincinnati, United StatesReviewed by:
Muswamba Mwamba, Stephen F. Austin State University, United States© 2024 Blumrich, Sousa, Barbieri, Simões, da Silva, Bettiol and Ferraro. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lukas Blumrich, bHVrYXMuYmx1bXJpY2hAZm0udXNwLmJy
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.