 Mathieu Nacher1,2,3*
Mathieu Nacher1,2,3* Julie Blanc1,2Sebastien Rabier2,4Aude Lucarelli2,4
Julie Blanc1,2Sebastien Rabier2,4Aude Lucarelli2,4 Antoine Adenis1,2,3Celia Basurko1,2,3Alphonse Louis5Dominique Dotou5Malika Leneuve5
Antoine Adenis1,2,3Celia Basurko1,2,3Alphonse Louis5Dominique Dotou5Malika Leneuve5 Lindsay Osei6
Lindsay Osei6 Narcisse Elenga2,7Najeh Hcini2,8
Narcisse Elenga2,7Najeh Hcini2,8
- 1Centre d'Investigation Clinique INSERM 1424, Centre Hospitalier de Cayenne, Cayenne, French Guiana
- 2Amazonian Infrastructures for Population Health, Centre Hospitalier de Cayenne, Cayenne, French Guiana
- 3Département Formation Recherche Santé, Université de Guyane, Cayenne, French Guiana
- 4COREVIH Guyane, Centre Hospitalier de Cayenne, Cayenne, French Guiana
- 5Service de Gynécologie Obstétrique, Centre Hospitalier de Cayenne, Cayenne, French Guiana
- 6Collectivité territoriale de Guyane, Protection Maternelle et Infantile, Cayenne, French Guiana
- 7Service de Pédiatrie, Centre Hospitalier de Cayenne, Cayenne, French Guiana
- 8Service de Gynécologie Obstétrique, Centre Hospitalier de l’Ouest Guyanais, Saint Laurent du Maroni, French Guiana
Introduction: In a context of high HIV prevalence, poor pregnancy follow-up, frequent poverty, preeclampsia, and preterm delivery, we aimed to describe the characteristics and outcomes of pregnancies among women living with HIV in French Guiana.
Methods: A retrospective cohort study was conducted on HIV-infected pregnancies enrolled between January 1st 1992 to 31st July 2022. Overall, there were 1,774 pregnancies in 881 women living with HIV.
Results: For 75.1% of pregnancies, the HIV diagnosis was already known before pregnancy and in 67.6% of women, HIV follow-up predated pregnancy. Nearly half of women, 49.6%, only had one pregnancy since having been diagnosed with HIV. Although most women received antiretroviral therapy during pregnancy, for those with the available information we found only 48.5% had an undetectable viral load at delivery. Overall, 15.3% of pregnancies ended with an abortion. There were a total of 110 newborns infected with HIV representing an overall transmission rate of 6.2% (110/1,771). Between 1993 and 2002, the transmission rate was 34%, between 2003 and 2012 it was 1.3%, and between 2013 and 2022 it was 0.7%. Overall, in Cayenne, since 2008, 106 of 581 HIV–infected pregnancies (18.2%) with available information were premature before 37 weeks of pregnancy; of these, 33 (5.7%) were very preterm deliveries and 73 (13.3%) were late preterm deliveries. Over time, in Cayenne, preterm delivery declined significantly.
Conclusions: The present study emphasizes that, despite spectacular progress in reducing mother to child transmission, pregnancy outcomes among women living with HIV are still preoccupying with high incidence of preterm delivery and low birth weight. Teasing out what fraction is linked to HIV and what fraction is linked to social precariousness and poor follow-up was not possible in this study. Despite the high incidence of very preterm delivery recent progress suggests that coordination efforts to improve follow-up may also have improved obstetrical outcomes.
Introduction
French Guiana is a French territory in South America that shares borders with Brazil and Suriname. For cultural reasons, it has the highest birth rate in Latin America (26.8 per 1,000 persons) (1). The HIV prevalence and incidence are the highest of all French territories. The prevalence of HIV in French Guiana in the 15–49 year-old age group is estimated at 1.6% and incidence has substantially declined since the advent of highly active antiretroviral therapy (2). The drivers of the epidemic are: frequent multiple sexual partnerships, transactional sex, and crack cocaine-related risky sex behaviors (3). These drivers are often related to social precariousness. Because French Guiana has the highest Gross Domestic Product (GDP) and health expenditure per capita in Latin America, it attracts numerous vulnerable immigrants who arrive in hope of better economic prospects. However, when they arrive, immigrants often live in great poverty. While 29% of the total population and nearly half of adults are foreigners, for persons living with the Human Immunodeficiency Virus (HIV), 80% are foreigners (3). Although many immigrants with HIV come from HIV endemic countries, we have shown that over half acquire the infection early after arrival in French Guiana, presumably because of enhanced sexual vulnerability linked to social precariousness (4, 5). In this context, the transmission mode of HIV is by far mostly heterosexual, with a balanced number of males and females. The health system is the French universal health care system, which provides mostly free health care to all (genotyping, viral load and CD4 lymphocyte measurements, and antiretrovirals, among others), including undocumented immigrants, most of whom benefit from residence permits for health reasons. However, for persons who have a difficult life, access to care is often complicated or secondary to the immediate pressing needs of survival. This is particularly obvious for pregnant women, over a third of whom have a poor pregnancy follow-up (6). Preterm delivery is double that of mainland France (13% vs. 6.9%, respectively) (7). Stillbirths and infant mortality are both 2–3 times greater than in France (8). The prevalence of HIV among pregnant women in French Guiana has exceeded 1% for over 3 decades. Since 2008, following the national French guidelines, all pregnant women receive a triple antiretroviral combination therapy. HIV during pregnancy has been associated with a number of adverse outcomes (9–12). The role of antiretrovirals has yielded contrasting results: some finding no difference in pregnancy outcomes (13) whereas others, notably a case control study in French Guiana, found antiretroviral treatment was associated with preterm delivery (12).
In this context of high HIV prevalence, frequent poverty, poor pregnancy follow-up, frequent preeclampsia, frequent preterm delivery, we hypothesized that describing pregnancy outcomes and their trends would provide precious information to optimize the care of women with HIV. We thus aimed to describe the characteristics and outcomes of 1,774 pregnancies among a historical hospital cohort of 881 women living with HIV in French Guiana. The Amazonian context of the study may provide useful information for other countries in the region.
Methods
The study was a retrospective cohort conducted on the French Guiana data included in the French Hospital Database for HIV (FHDH), a national cohort that prospectively records all events and characteristics of persons with HIV. HIV-infected pregnancies (confirmed infections by western blot analysis) enrolled between January 1st 1992 to 31st July 2022 were considered. While HIV was the exposure the main outcomes of interest were pregnancy outcome, transmission, obstetrical complications. Patient data are routinely entered in the database by physicians as they consult and trained research technicians who control for exhaustivity. The main study variables were age, country of birth, date of HIV discovery and reason for testing, initial CD4 count, CDC stage, viral load, antiretroviral treatment, opportunistic infections, and pregnancy outcomes (obstetrical complications, labor and delivery complications, early neonatal outcomes, complications related to puerperium). Because HIV records did not have precise information about term at delivery, between 2008 and 2022 research technicians compiled this information in Cayenne.
Statistical analysis
Descriptive analysis computed means and standard deviations for quantitative variables, and counts and percentages for qualitative and ordinal variables. Pregnancy complications were studied using International Classification of Diseases (ICD 10) codes O10–O16 (edema, proteinuria, and hypertensive disorders in pregnancy, childbirth, and the puerperium), O20–O29 (Other maternal disorders predominantly related to pregnancy), O40–O48 (Ectopic pregnancy, molar pregnancy, and other abnormal conceptions), O60–O75 (Complications of childbirth) and O98 (Other unspecified maternal conditions). The statistical analysis was performed using SAS 9.4 software (SAS Institute Inc., Cary, NC, USA).
Pregnancies with no event were censored at the date of delivery or termination. Only pregnancies with start and end dates were used.
Ethical and regulatory aspects
All patients included in the FHDH give informed consent for the use of their anonymized data, and for the publication of anonymized results from these data. This cohort has been approved by the Commission Nationale Informatique et Libertés (CNIL) since November 27th 1991, subsequently updated on March 30th 2021 (deliberation number 2021-044) and has led to several international publications.
Results
Overall, there were 1,774 pregnancies in 881 women living with HIV. The mean age at the time of pregnancy was 30.3 years (SD = 6.6). Most pregnant women were from Haiti (39.2%), Suriname (26%), and France (15.4%), as in the overall cohort.
Table 1 shows HIV characteristics. Briefly, 69% of women had first been screened for HIV during pregnancy at the initiation of a physician. Only 14.9% of women had CD4 counts <200 per mm3 and 17% were at the Acquired Immuno Deficiency Syndrome (AIDS) stage. Between 1993 and 2002, the mean nadir CD4 count was 579 per mm3, between 2003 and 2012 it was 375 per mm3, and between 2013 and 2022 it was 509 per mm3.
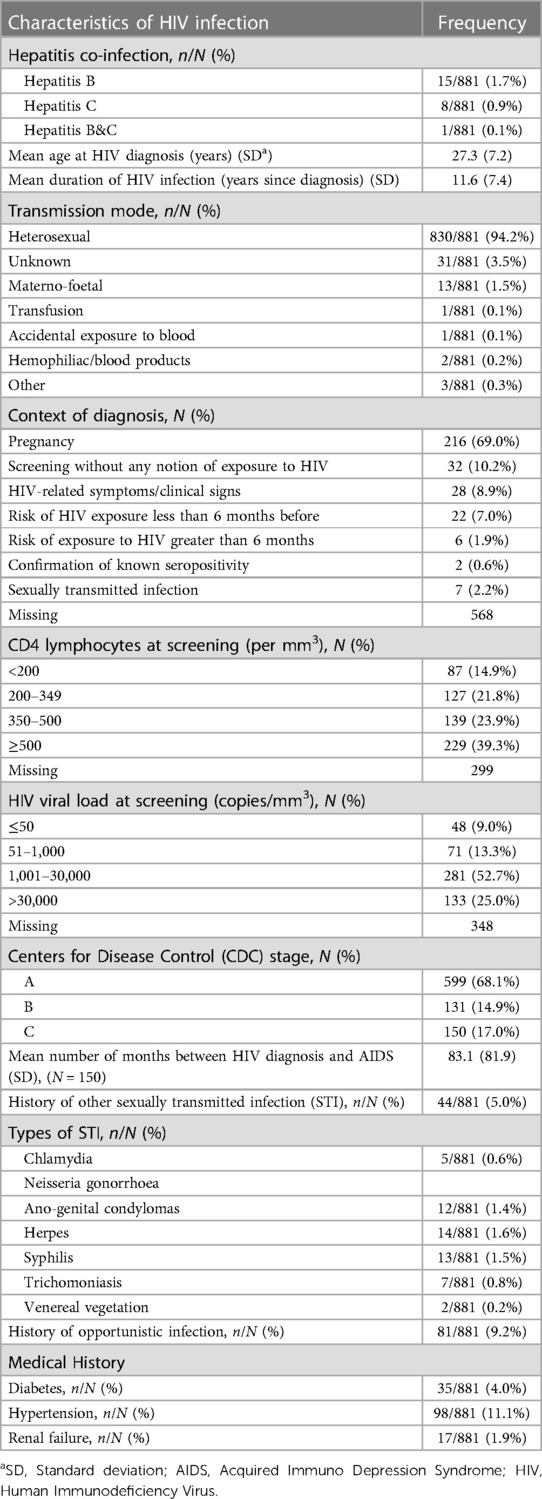
Table 1. Description of HIV characteristics among 881 pregnant women living in French Guiana with details on associated STI and comorbidities.
Table 2 shows that the HIV diagnosis was known in 75.1% of pregnancies and that, in 67.6% of women, HIV follow-up predated pregnancy. Nearly half of women, 49.4%, only had one pregnancy since having been diagnosed with HIV. Although most women received antiretroviral therapy during pregnancy, only 48.5% of those with the available information had an undetectable viral load at delivery. Between 2012 and 2022, 93% of pregnant women were on antiretroviral therapy.
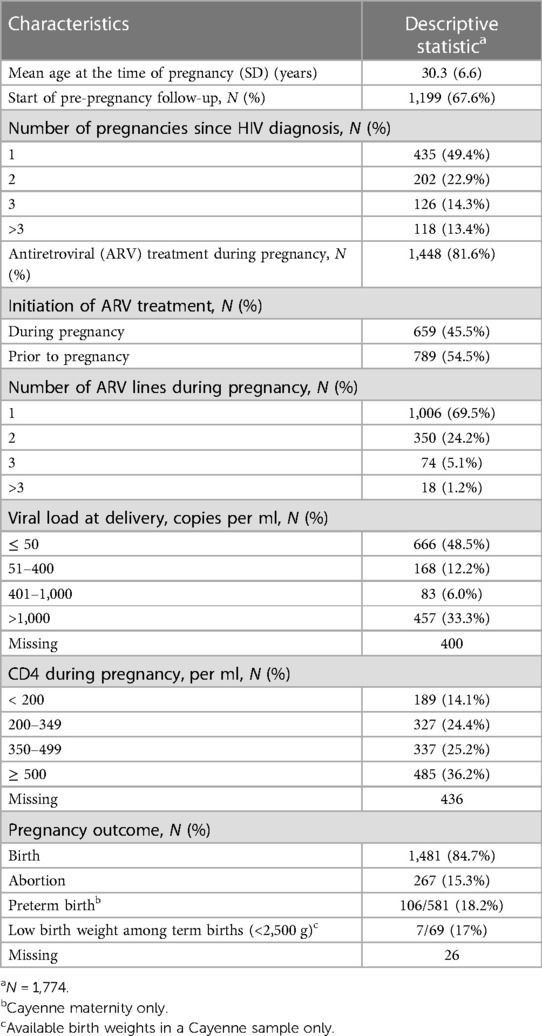
Table 2. Description of characteristics and outcomes among 1,774 pregnancies among 881 women living with HIV: French Guiana 1992–2022.
Overall, 15.3% of pregnancies ended with an abortion but between 2012 and 2022 it significantly declined to 10.4%. Overall, 99.8% of women gave exclusive artificial feeding to their newborn. Since the beginning of data collection, there were a total of 110 newborns infected with HIV representing an overall transmission rate of 6.2% (110/1,771). Between 1993 and 2002, the transmission rate was 34%, between 2003 and 2012 it was 1.3%, and between 2013 and 2022 it was 0.7%.
Figure 1 shows the gradual reduction of the viral load at delivery.
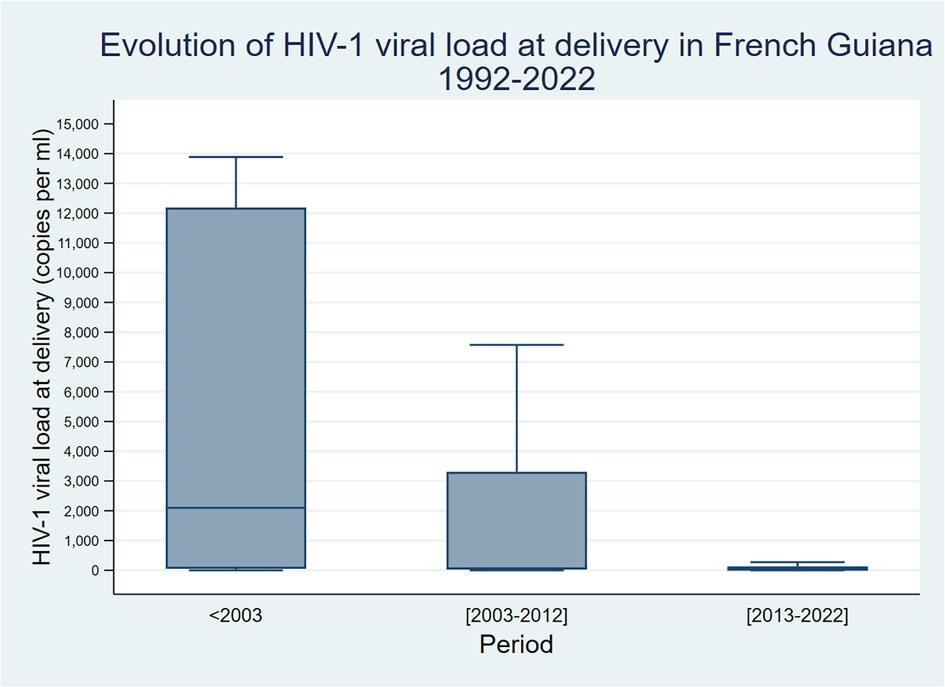
Figure 1. Evolution of HIV-1 viral load at delivery.
Preterm deliveries
Overall, in Cayenne, since 2008, 106 of 581 (18.2%) pregnancies among women living with HIV with available information were premature before 37 weeks of pregnancy; of these, 33 (5.7%) were very preterm deliveries (28 to less than 32 weeks) and 73 (13.3%) were late preterm deliveries (<37 weeks and >32 weeks). In a sample from Cayenne maternity, the median birthweight was 3,050 g and 17% were considered to have low birth weight (<2,500 g). Among term births, 7/69 (10%) had low birth weight.
Over time, in Cayenne, preterm delivery declined significantly (Figure 2, χ2 for trend P < 0. 019). Overall, 48 cases of preeclampsia (2.7%) were reported.
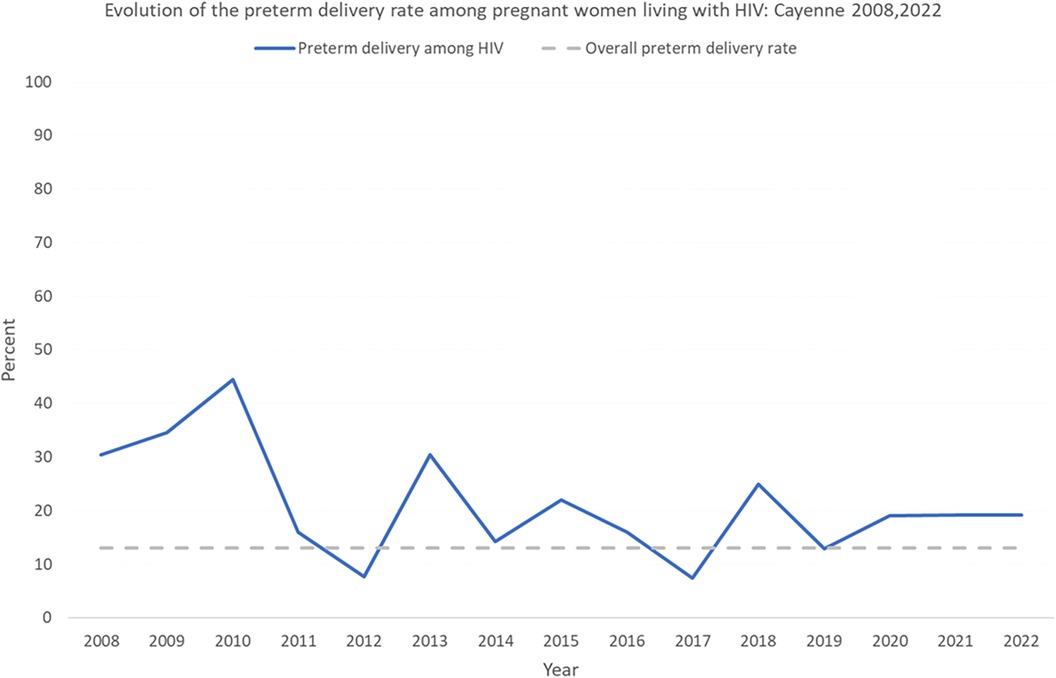
Figure 2. Evolution of the preterm delivery rate among pregnant women living with HIV in Cayenne.
Supplementary Table S1 details the number of obstetrical events corresponding to the following ICD 10 codes: O10–O16, O20–O29, O40–O48, O60–O75 and O98.
Discussion
Here, in a territory combining the highest HIV prevalence of all French territories, the highest fertility rate in Latin America, we provide the first epidemiologic overview of HIV-positive pregnancies. Among pregnant women living with HIV, we show that the preterm delivery rate remained particularly high: in 2022 it was 19.2% vs. 13% in the general population of French Guiana, and 6.9% in the general population of mainland France. The proportion of low birth weight births was also very high: 17% vs. 11.9% in the general population of French Guiana, and 7.5% in the general population of mainland France, and 14.6% in the world (14).
Over half (53%) of the general population of French Guiana lives below the poverty threshold, 29% lives in great poverty (15), and persons living with HIV are an even more precarious subpopulation. The link between poor follow-up, psychosocial stressors, and preterm delivery has been previously shown and presumably explain much of this difference (6). However, HIV itself may also contribute to this very high rate of preterm delivery (12). Other analytic studies in territories with widespread poverty have yielded contrasting conclusions: some did not demonstrate significant differences (13) whereas others did (12). Although the present study was only descriptive, the levels of preterm delivery or low birth weight were substantially greater than in the general population of French Guiana and it is likely that there are indeed worse pregnancy outcomes among women living with HIV than in the general female population of French Guiana. Given the progress in testing and treating women, we hypothesize that the remaining challenges regarding preterm delivery and low birth weight would most benefit from optimal obstetrical follow-up.
In French Guiana, health professionals and non-government organizations have been proactive in reaching vulnerable populations. These treatment and prevention efforts have now led to most women delivering with viral loads beneath transmission thresholds and very low residual transmission, usually in cases of women tested late in their pregnancy or lost to follow-up. Between 2012 and 2022, 93% of pregnant women had received ARV treatment, a figure that is only slightly above that of what is reported globally (13). This emphasizes the residual challenges that remain to follow the most vulnerable women, a fraction of whom escape the reach of the health system.
The present study has a number of limitations. The absence of a proper control group in the present study was a notable limitation. The crude comparisons relied on different data sources for the general population of French Guiana. Our analysis was purely descriptive and spans over 3 decades of multiple gradual changes, in terms of social conditions, of HIV care and more generally of the organization of the health system. It is therefore difficult to pinpoint any single factor involved in the positive trends but rather a convergence of proactive efforts to reach and test pregnant women, improvements of the coordination of health care workers, improvement in treatment strategies, improvements in the tolerance and effectiveness of antiretrovirals being a potent combination to reduce vertical transmission of HIV. Another important limitation is that social factors are probably the major determinant of the studied health outcomes, yet we had no direct measurement of precariousness in our data, so we can only assume –not prove—that much of what is shown is detrimentally influenced by precariousness. The information about preterm delivery rests on a subsample from Cayenne's level 3 maternity which may bias preterm delivery estimates upwards. Furthermore, the data on birthweight was also a subsample from Cayenne maternity so results should be taken with caution. Despite the above limitations, the present study has some merits as it is the first study to provide real life data on historical trends and remaining challenges in French Guiana; it also provides important information on various standard aspects of HIV infection and their temporal evolution.
In summary, the present study shows that with time the system has been successful in reducing mother to child transmission and preterm births. However, challenges remain because incidence of preterm delivery and low birth weight are still substantially higher than in the general population of pregnant women in French Guiana. Teasing out what fraction is linked to HIV and what fraction is linked to social precariousness and poor follow-up was not possible in this study but, in practice, it seems crucial to implement to continue early and careful obstetrical follow-up for pregnant women living with HIV. Reducing maternal-fetal transmission of HIV necessarily implies efforts to improve access to care for fragile populations.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions. According to French Law data cannot be sent to other structures without prior authorization by the Commission Nationale Informatique et Libertés. Upon resonable request and with permission from the CNIL anonymized data may be shared. Requests to access these datasets should be directed toY29yZXZpaEBjaC1jYXllbm5lLmZy.
Ethics statement
The studies involving humans were approved by Commission Nationale Informatique et Libertés (CNIL). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
MN: Conceptualization, Formal analysis, Supervision, Writing – original draft, Writing – review & editing. JB: Data curation, Formal analysis, Writing – review & editing. SR: Data curation, Writing – review & editing. AL: Investigation, Writing – review & editing. AA: Project administration, Writing – review & editing. CB: Writing – review & editing. AL: Writing – review & editing. DD: Writing – review & editing. ML: Writing – review & editing. LO: Writing – review & editing. NE: Writing – review & editing. NH: Investigation, Validation, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fgwh.2023.1264837/full#supplementary-material
References
1. Nacher M, Basurko C, Douine M, Lambert Y, Hcini N, Elenga N, et al. The epidemiologic transition in French Guiana: secular trends and setbacks, and comparisons with continental France and South American countries. Trop Med Infect Dis. (2023) 8:219. doi: 10.3390/tropicalmed8040219
2. Nacher M, Adriouch L, Huber F, Vantilcke V, Djossou F, Elenga N, et al. Modeling of the HIV epidemic and continuum of care in French Guiana. PloS One. (2018) 13:e0197990. doi: 10.1258/ijsa.2010.009570
3. Nacher M, Vantilcke V, Parriault MC, Van Melle A, Hanf M, Labadie G, et al. What is driving the HIV epidemic in French Guiana? Int J STD AIDS. (2010) 21:359–61. doi: 10.1258/ijsa.2010.009570
4. Arantes I, Bello G, Darcissac E, Lacoste V, Nacher M. Using phylogenetic surveillance and epidemiological data to understand the HIV-1 transmission dynamics in French Guiana. AIDS. (2021) 35:979–84. doi: 10.1097/QAD.0000000000002817
5. Nacher M, Adriouch L, Melle AV, Parriault M-C, Adenis A, Couppié P. Country of infection among HIV-infected patients born abroad living in French Guiana. PLoS One. (2018) 13:e0192564. doi: 10.1371/journal.pone.0192564
6. Leneuve-Dorilas M, Favre A, Carles G, Louis A, Nacher M. Risk factors for premature birth in French Guiana: the importance of reducing health inequalities. J Matern Fetal Neonatal Med. (2019) 32:1388–96. doi: 10.1080/14767058.2017.1403578
7. Interroger les données de mortalité | CépiDc. Available online at: https://www.cepidc.inserm.fr/donnees-et-publications/interroger-les-donnees-de-mortalite (accessed July 21, 2023).
8. Mathieu M, Lambert V, Carles G, Picone O, Carod J-F, Pomar L, et al. Incidence, causes, and risk factors of stillbirth in an Amazonian context: saint laurent du Maroni maternity ward 2016–2021. Eur J Obstet Gynecol Reprod Biol X. (2023) 18:100190. doi: 10.1016/j.eurox.2023.100190
9. Xiao P-L, Zhou Y-B, Chen Y, Yang M-X, Song X-X, Shi Y, et al. Association between maternal HIV infection and low birth weight and prematurity: a meta-analysis of cohort studies. BMC Pregnancy Childbirth. (2015) 15:246. doi: 10.1186/s12884-015-0684-z
10. Silva Cd, Alves RdS, Santos TSD, Bragagnollo GR, Tavares CM, Santos AAPD. Epidemiological overview of HIV/AIDS in pregnant women from a state of northeastern Brazil. Rev Bras Enferm. (2018) 71:568–76. doi: 10.1590/0034-7167-2017-0495
11. Lopez M, Figueras F, Hernandez S, Lonca M, Garcia R, Palacio M, et al. Association of HIV infection with spontaneous and iatrogenic preterm delivery: effect of HAART. AIDS. (2012) 26:37–43. doi: 10.1097/QAD.0b013e32834db300
12. Elenga N, Djossou Fl, Nacher M. Association between maternal human immunodeficiency virus infection and preterm birth. Medicine (Baltimore). (2021) 100:e22670. doi: 10.1097/MD.0000000000022670
13. Mugo C, Nduati R, Osoro E, Nyawanda BO, Mirieri H, Hunsperger E, et al. Comparable pregnancy outcomes for HIV-uninfected and HIV-infected women on antiretroviral treatment in Kenya. J Infect Dis. (2022) 226:678–86. doi: 10.1093/infdis/jiac128
14. Low birthweight—UNICEF DATA. Available online at: https://data.unicef.org/topic/nutrition/low-birthweight/ (accessed July 4, 2023).
15. 29% des Guyanais en situation de grande pauvreté en 2018—Insee Analyses Guyane—59. Available online at: https://www.insee.fr/fr/statistiques/6468775 (accessed January 6, 2023).
Keywords: HIV, pregnancy, vertical transmission, preterm delivery, French Guiana
Citation: Nacher M, Blanc J, Rabier S, Lucarelli A, Adenis A, Basurko C, Louis A, Dotou D, Leneuve M, Osei L, Elenga N and Hcini N (2024) Thirty years of HIV pregnancies in French Guiana: prevention successes and remaining obstetrical challenges. Front. Glob. Womens Health 4:1264837. doi: 10.3389/fgwh.2023.1264837
Received: 21 July 2023; Accepted: 13 December 2023;
Published: 3 January 2024.
Edited by:
May Maloba, Global innovation Kenya, KenyaReviewed by:
Marta Lopez, Hospital Clinic of Barcelona, SpainPatrick Kaonga, University of Zambia, Zambia
© 2024 Nacher, Blanc, Rabier, Lucarelli, Adenis, Basurko, Louis, Dotou, Leneuve, Osei, Elenga and Hcini. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mathieu Nacher bWF0aGlldS5uYWNoZXI2NkBnbWFpbC5jb20=