 Daisy Afra Lumor1*
Daisy Afra Lumor1* Christian Obirikorang2
Christian Obirikorang2 Emmanuel Acheampong2,3,4
Emmanuel Acheampong2,3,4 Yaa Obirikorang5
Yaa Obirikorang5 Hubert Owusu2
Hubert Owusu2 Sam Newton6
Sam Newton6
- 1Department of Midwifery, St. Patrick's Nursing and Midwifery Training School, Offinso, Ghana
- 2Department of Molecular Medicine, School of Medicine and Dentistry, Kwame Nkrumah University of Science and Technology, Kumasi, Ghana
- 3Department of Genetic and Genome Biology, University of Leicester, Leicester, United Kingdom
- 4Centre for Precision Health, School of Medical and Health Sciences, Edith Cowan University, Joondalup, WA, Australia
- 5Department of Nursing, Garden City University College, Kumasi, Ghana
- 6Department of Global and International Health, School of Public Health, Kwame Nkrumah University of Science and Technology, Kumasi, Ghana
Background: Contraceptive use has many advantages for personal growth and societal advancement, but there is still the problem of unmet needs for women, which highlights the gap between women's reproductive intentions and contraceptive use. This study investigated knowledge, perceptions, and factors that influence contraceptive use among married women living in a military base in Ghana.
Methods: This cross-sectional study involved 350 married women between the ages of 20 and 58 years at the Uaddara Barracks, Kumasi. A structured questionnaire was used to collect information on the background, knowledge, perceptions on contraceptive use, and contraceptive methods used by participants. Data was entered into an Excel sheet and analysed using R version 4.2.1.
Results: Most of the participants were between the age range of 36 and 40 years (25.5%). Almost all study participants (97.4%), had heard about contraceptives with 80.6% showing a high level of knowledge on contraceptives. The majority of the women (84.6%) had previously used some form of contraceptives and 53.1% presently do. More than half of the participants (69.4%) had a positive perception of contraceptive use; 80.6% responded it was their own decision to use contraceptives, and 80.3% had the support of their husbands. Husbands' support of contraception resulted in a 5 times higher usage of contraceptives among women (aOR = 5.35; p < 0.001) while women who were married to military men were 45% (aOR = 0.45; p = 0.007) less likely to use contraceptive when compared to civilian wives. Demographic characteristics like being above 40 years (aOR = 0.25; p = 0.014), being a housewife (aOR = 0.42; p = 0.043) and working in the private sector (aOR = 0.33; p = 0.015) were significantly linked with less contraceptive use.
Conclusion: The study showed that women used contraceptives at a rate that was much higher than the national norm at the Uaddara Barracks, demonstrating the beneficial influence men had on women's contraceptive use. This thereby underscores the need for interventional policies that prioritized the male as much as women, while emphasizing the benefits of contraceptive use to the family and not just as an awareness program only.
1. Introduction
The global population is increasing more rapidly than the Earth can handle (1). The world's population is projected to reach 8.5 billion in 2030, 9.7 billion in 2050, and 11.2 billion by 2,100 (2). Much of this population growth is projected to be in the low-middle-income countries in Sub-Saharan Africa (3). Ghana's population increased by 30.4 percent from 18,912,079 in 2,000 to 24,658,823 in 2010 (4). This increase places an enormous burden on the country's ability to adequately provide for its citizens by putting a strain on essential social services such as education, health, water, and housing (1, 5). Thus, the promotion of family planning services such as modern conceptive use as a means of cutting down fertility rates, and empowering women in their childbearing age (3, 6). Not only that, family planning has enabled couples to choose the number and timing of childbirth while also serving to prevent unwanted pregnancies, and unsafe abortions, offering protection against sexually transmitted diseases such as HIV/AIDS through such methods as condom use (7, 8). In addition, family planning is widely regarded as an important way to achieve Millennium Development Goals (MGDs) 4 and 5 through the reduction of maternal and child mortality (8).
However, while the global use of family planning services was estimated to be 57.4% in 2015, it has rather remained low in many Sub-Saharan countries such as Ghana (7, 9, 10). Over the years, the prevalence of modern contraceptive use among married women in Africa rose from 23.9% in 2012 to 28.5% in 2017 with the West African subregion recording a low rate of 20.0% that same year (11). In other parts of the world, the prevalence of contraceptive use rose from 60.9% to 61.8% in Asia, while remaining steady at 66.7% in Latin America and the Caribbean (9, 12). Ghana's prevalence of contraceptive use stands at 27.1% with the country having missed its goal of reaching a 50.0% target rate in 2020 (11, 13).
It is estimated that about 225 million women in developing countries would like to delay or stop childbearing but are not using any contraceptive method, which is an unmet need for family planning (14). Women with an unmet need are those who are fecund and sexually active but are not using any method of contraception while reporting not wanting any more children or expressing a desire to delay the next child (14). The concept of unmet need points to the gap between women's reproductive intentions and their contraceptive behavior (15). Several factors have been associated with the low uptake of contraceptives. Some studies in Ghana have shown that knowledge of contraceptives, their availability, as well as easy access to contraception—particularly among young people, poorer segments of populations, or unmarried people—all have a positive influence on their use (6, 16, 17). Other factors include a limited choice of methods; fear of or experience of side effects; cultural or religious opposition; poor quality of available services; user and provider bias; and gender-based barriers (18–20).
The various factors that influence the use of modern contraceptive methods have been noted to differ across countries (16). In Ghana, both government and non-governmental organizations have employed various campaign programs to improve the use of modern contraceptives use across the country. While this has gained some success, specifically in improving awareness and knowledge of contraceptive methods across much of the country, women with unmet needs remain high (21). However, many studies exploring modern contraceptive use within the country have rather focused on the general population (6). This makes the current study important as it explores the factors that influence the use of modern contraceptive methods among women within the barracks, a place where military deployments routinely separate families over a long period of time. The information gathered would go a long way in formulating long-term campaign programs on how to effectively reach our military women and the wives of our military men with such unmet needs.
2. Materials and method
2.1. Study design and setting
This was a quantitative cross-sectional study conducted among 350 married women living in the barracks at the 4BN Uaddara Barracks, Kumasi. The barracks is about 10 min drive away from the city center, right beside the Komfo Anokye Teaching Hospital. It houses about 2,400 individuals which includes military personnel and their spouses, as well as civilian employees and their spouses who receive reproductive and other health services from the teaching hospital, nearby private clinics, and midwife-managed maternity homes.
2.2. Data collection
A structured questionnaire was used to obtain information from all study participants. The structured questionnaire was developed based on a review of published articles (22, 23) It was made up of four sections. Section A collected information on the sociodemographic characteristics of respondents. Section B was designed to collect information about contraceptive use. Section C constituted information on perceptions towards contraceptive methods. Section D consisted of questions about the involvement of their partners in contraceptive use. The study was pretested with 20 women of similar socio-cultural characteristics. Weaknesses identified during the pre-test were rectified before the final administration of the questionnaire. The independent variable of the study was contraceptive use among married women and the dependent variables of the study were knowledge, perceptions, compliance, and factors influencing contraceptive use. These are defined as a married woman's awareness and information on modern contraceptive methods, attitudes, adherence to modern contraceptive methods, and influencing factors of modern contraception uptake. To assess these, questions were asked about awareness of modern contraceptive methods; ever-used contraceptive methods (condoms, oral contraceptives, withdrawal, Intrauterine device, several methods, or abstinence); reasons for uptake or withdrawal, or the urge to continue usage.
2.3. Data handling and management
The knowledge of respondents about contraception scored a point for a correct answer and zero for a wrong answer. After adding the scores median split was used to define the respondents having low knowledge (those who were below the median) and high knowledge (those above the median mark). Similarly, for perception, using the point Likert scale, with agreed scoring one point and disagreed, and I don't know scoring zero for correctly answered questions, and vice versa for incorrectly answered questions. Scoring for attitude was done using a median split into dichotomous data; scores that are up to or more than the mean was regarded as a positive attitude and those below the median had a negative attitude.
2.4. Data analysis
Data was entered in an Excel spreadsheet for Windows and analyzed using R version 4.2.1. Data for continuous variables between two groups were presented as means ± SD standard deviation. Categorical variables were presented as frequency (n) and percentage (%). Women's contraceptive use were regressed on socio-demographic variables, knowledge level, perception of contraceptive use, partner's demographics, partner's support and use of the male condom, as well as on factors relating to marriage, fertility, and desire for more children. Significance was defined as a p-value of <0.05.
2.5. Ethical consideration
Ethical clearance was sought from the Committee on Human Research, Publications, and Ethics (CHRPE) (reference: CHRPE/AP/384/18) of KNUST and the Commanding Officer of the 4th Infantry Battalion, Uaddara Barracks, Kumasi. All respondents signed a written consent form, they were informed that taking part in the research was voluntary and that they can opt out at any time.
3. Results
3.1. Demographic characteristics of the study participants and their partners
Table 1 summarizes the socio-demographic characteristics of participants. The study involved 350 participants between the ages of 20 and 58 years, many of whom (25.5%) were within the 36–40 years bracket. The majority of participants (98.3%) have had secondary education, 83.4% were Christians, 40.9% were government employees, and almost half (49.7%) got married between the ages of 23 and 27 years. Most of the participants responded that their husbands got married between the ages of 28–32 years (43.4%), and 60.3% said their husbands have had an education to the tertiary level. A higher proportion of participants responded that their husbands were military personnel (77.4%) (Table 1).
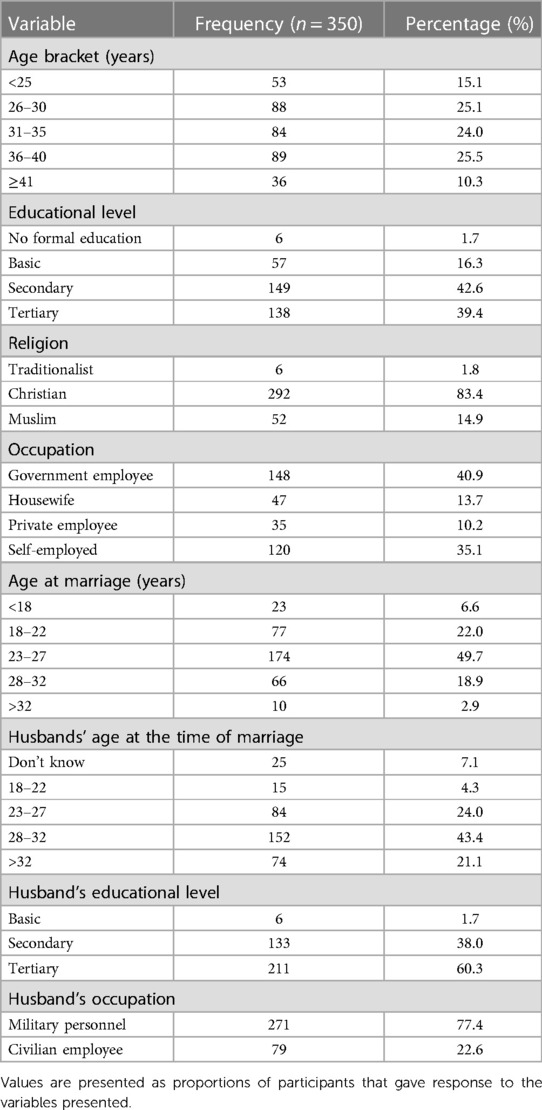
Table 1. Demographic characteristics of study participants.
3.2. Contraceptive use among the participants
Most of the participants (84.6%) have previously used some form of contraceptives, while 53.1% were currently doing so (Figures 1A,B). Injectable was the most used current contraceptive method (26.7%) (Supplementary Table S1). The majority of the participants (80.6%) indicated that they chose to use contraception on their own and 51.1% mentioned they had never had any side effects. In addition, 80.3% responded that their husbands supported them in using contraception, and 67.9% mentioned their husbands used the male condom respectively (Supplementary Table S1).
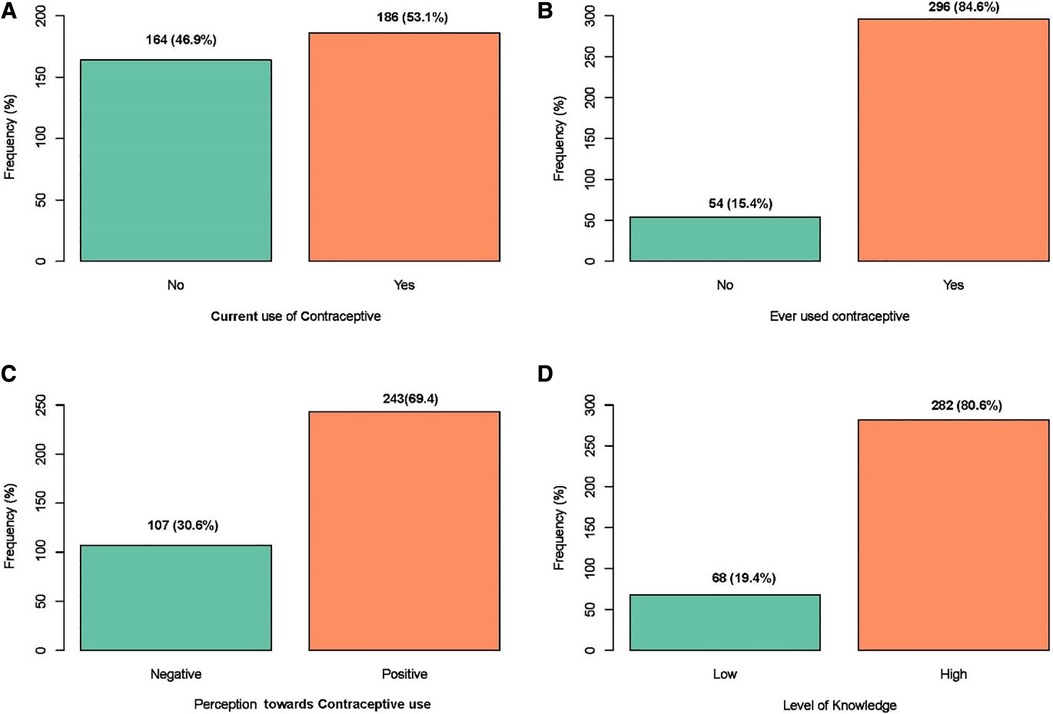
Figure 1. A graph showing the frequency distribution of women's: (A) current contraceptive use; (B) if they have ever used any contraceptive method; (C) their perception toward contraceptive use; (D) their level of knowledge on contraception.
3.3. Awareness and knowledge of contraceptive use among participants
Almost all study participants (97.4%), have heard about contraceptives and the principal source of information was the media/internet (64.5%) (Supplementary Table S2). Condoms (74.5%) were the most widely known contraceptive method. More than half (52.5%) of the participants knew withdrawal as a traditional contraceptive method. A major proportion of the participants (64.5%) knew about the sources of contraceptives with the family planning unit being the most frequently represented source (56.4%) (Supplementary Table S2). Overall, 80.6% of participants demonstrated a high level of knowledge of contraceptives (Figure 1D).
3.4. Perception of contraceptive use among participants
As shown in Supplementary Table S3, a majority of participants disagree with the fact that modern contraceptive services and commodities are inaccessible (69.7%), it is not easy to discuss sexual issues with a partner (62.0%), contraceptives are for females only (86.3%), and it is wrong to use contraceptives (82.9%) (Supplementary Table S3). On the other hand, more than half of the study participants agreed that contraceptives were acceptable at the barracks (63.7%) and that couple counselling could improve male involvement in contraceptive use (70.9%) (Supplementary Table S3). Altogether, 69.4% of participants showed positive perceptions towards contraceptive use (Figure 1C).
3.5. Married life of study participants
Most of the participants (40.3%) have been married for 1–5 years, and 45% of them had 1–2 children. One hundred and sixty-seven of the participants (47.7%) desired a male child and 40.9% desired a female child. More than half (69.1%) of the study subjects anticipated having 3–4 children while only 5.1% projected to have 7–8 children. Higher proportions of the participants had no problems taking decisions in marriage (61.1%) and the remaining 38.9% noted to have problems taking decisions in marriage (Supplementary Table S4).
3.6. Factors associated with contraceptive use among participants
Multivariate logistic regression analysis showed that participants who were above 40 years were 25% less likely to use contraceptives when compared to women who were 25 years old or younger (aOR = 0.25; p = 0.014), where women who were housewives (aOR = 0.42; p = 0.043) or those who worked in the private sector (aOR = 0.13; p = 0.015) were associated with a 25% and 42% less likelihood to use any form of contraceptives when compared, and those who were government employees (Figure 2). No significant relationship was observed between participants likelihood to use contraceptives and their educational level, religion, and age of marriage. Nonetheless, participants with a higher knowledge of contraceptives were 4 times more likely to use them than those who did not have much knowledge on contraceptives (OR = 4.38; p < 0.001).
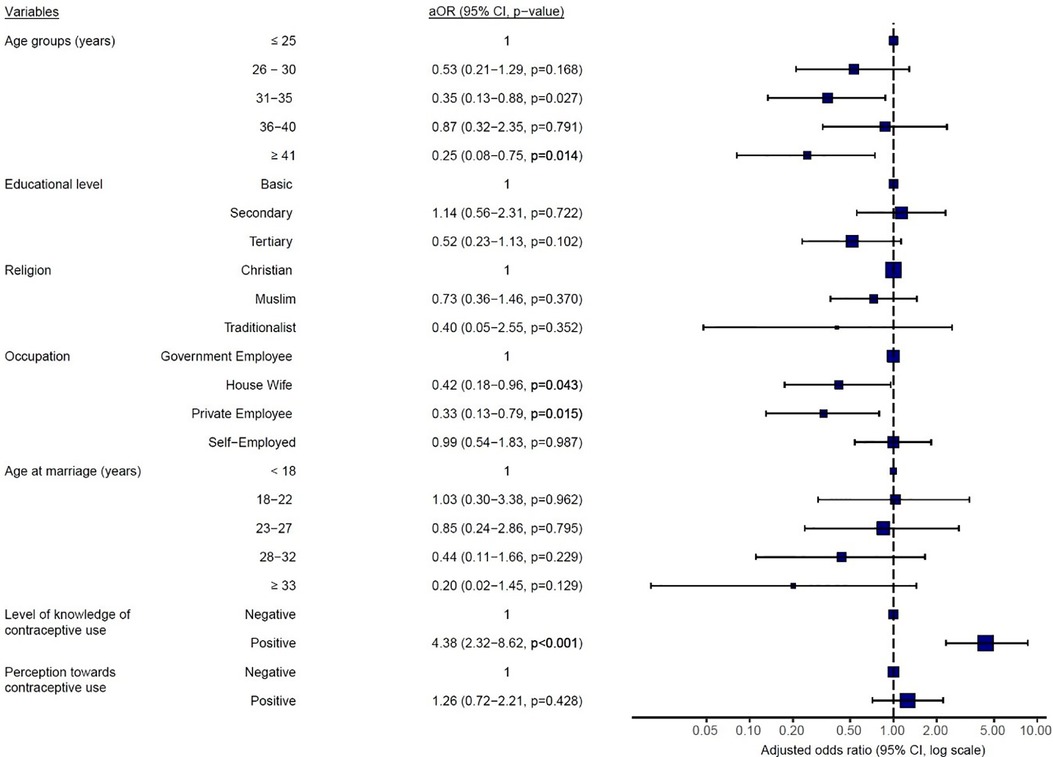
Figure 2. Multivariate logistic regression analysis of women's current contraceptive use on socio-demographic variables, knowledge level, and perception of contraceptive use. aOR, adjusted odds ratio, CI, confidence interval, p < 0.05 is statistically significant.
As depicted in Figure 3, participants whose husbands were 33 years or older at the time of marriage were significantly less likely to use contraceptives (aOR = 0.29; p = 0.043) when compared to those whose husbands got married between 18 and 22 years. Moreover, participants with husbands who have attained a tertiary level of education (aOR = 0.43; p = 0.001) or were married to Military Personnels (aOR = 0.45; p = 0.007) were at reduced odds of using contraceptives when compared to those whose husbands have only attained a secondary school level of education or were civil servants respectively (Figure 3). However, participants whose husbands support contraception were 5 times more likely to use contraceptives (aOR = 5.35; p < 0.001) than those whose husbands were not in support of contraceptive use (Figure 3).
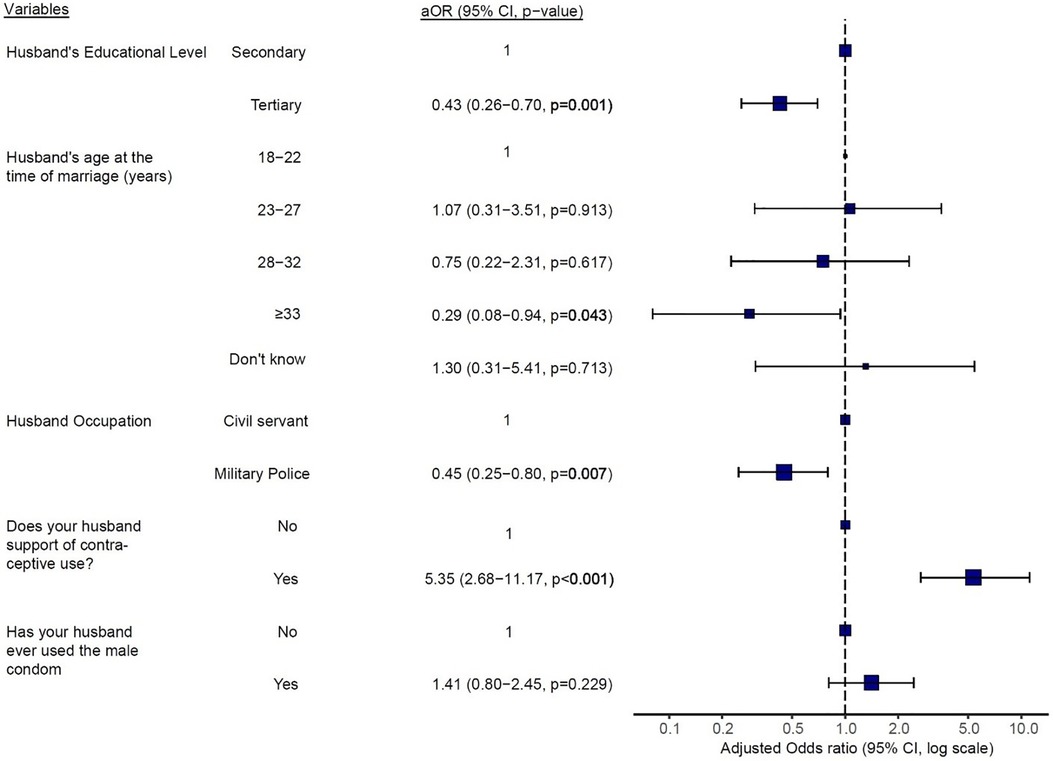
Figure 3. Multivariate logistic regression analysis of women's current contraceptive use on partner's demographics and partner's support and use of the male condom. aOR, adjusted odds ratio, CI, confidence interval, p < 0.05 is statistically significant.
In addition, married women who had 3–4 children (aOR = 14.91; p < 0.0001) or ≥5 children alive (aOR = 11.79; p = 0.004) were 14 and 11 times respectively more likely to use contraceptives than women with 1–2 children alive (Figure 4). On the other hand, women who wanted male children were 25% less likely to currently use any form of contraceptives (aOR = 0.25; p < 0.0001) when compared to women who had no such desire. The length of participant's married life, desire for a female child, and participant's difficulties in taking decisions were all not significantly associated with their current use of contraceptives (Figure 4).
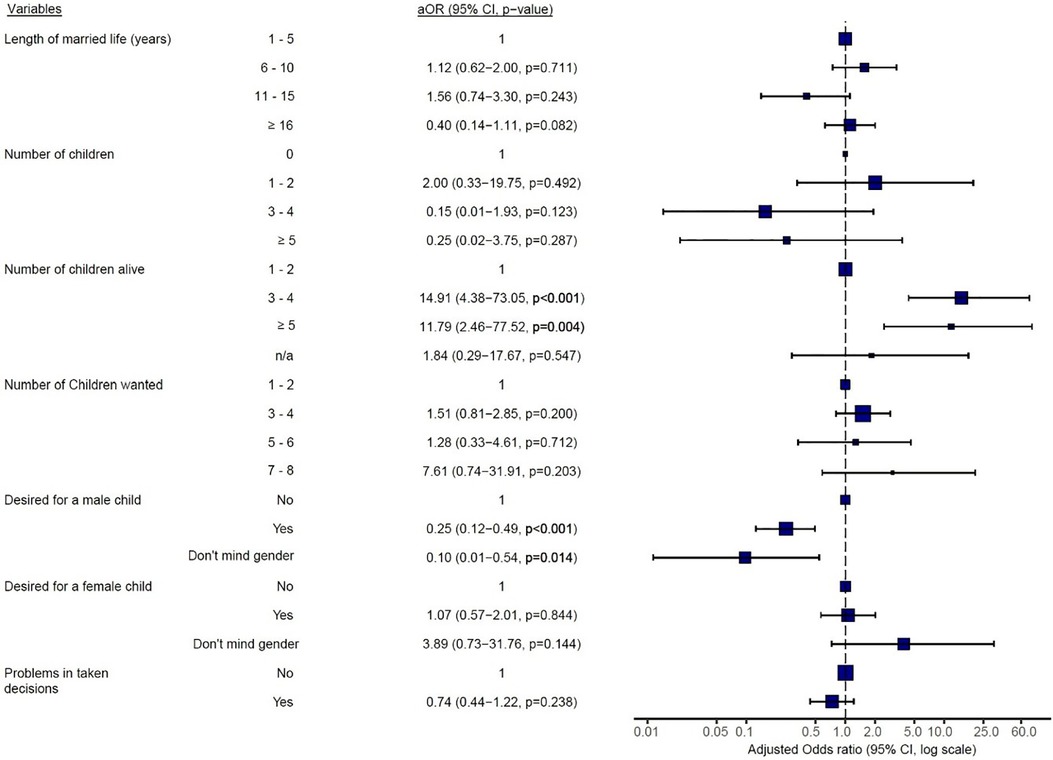
Figure 4. Multivariate logistic regression analysis of women's current contraceptive use on factors relating to marriage, fertility, and desire for more children. aOR, adjusted odds ratio, CI, confidence interval, p < 0.05 is statistically significant.
4. Discussion
Contraceptive use has many advantages, including, control of fertility and, as a result, population growth (21) and letting people decide how many and when to have children (24). There is an unmet need for women, despite prioritizing its acceptance (15). This study determined the knowledge, perceptions, and factors that influence contraceptive use among married women living in Uaddara Barracks, a military base in Kumasi, Ashanti Region.
In this study, a high degree of knowledge and awareness of contraceptives was observed among the study participants, which was consistent with the findings by Marrone et al, who reported that the Ghanaian population had a sufficient level of awareness level of contraceptive use (both modern and traditional) (21). Our results revealed that nearly all respondents could indicate at least one modern method of contraception, which is consistent with findings from other recent studies which showed a near-to-total universality of women's knowledge of contraceptive methods (6, 18, 25). The three modern contraceptives that the study participants most frequently reported using—both currently and in the past—were pills, injections, and condoms. Our results further reveal that injectables were the most used current contraceptive method. Similar findings have been reported by the Ghana Statistical Service (26). Aryeetey et al. (18), reported that estrogen/progesterone pills, male condoms, and injectables were the most commonly used contraceptive methods because they are the most frequently provided methods in many Ghanaian family planning centers. Nevertheless, due to wide media publicity in the fight against HIV/AIDS, many women were already familiar with condoms as a method of contraception (27). Moreover, other studies have also reported that a majority of reproductive-age women gravitate toward the use of injectables (23, 25). Eliason et al. reported that injectables are a preferred option, especially for new contraceptive users because certain communities associated the use of modern contraceptives with promiscuity. Similarly, Kamangu also notes that due to their high accuracy in pregnancy prevention and a reduction in the number of clinic visits for the service, injectables were a popular choice among Tanzanian women (25, 28).
In Ghana, modern contraceptive methods are available through the public health system as well as commercial outlets such as chemical stores, pharmacies, and other social marketing organizations (18). This was consistent with the present study where most women considered pharmacies and family planning units as their source for contraceptives. This reflects favorably on the national effort of making contraceptive methods more easily available and accessible. Nonetheless, participants’ ability to access contraceptive methods could also be a product of the urban setting in which they find themselves, which has been shown to provide more easily accessible avenues to obtain contraceptive methods than in rural areas (29).
We observed that a considerable proportion of the participants reported having ever used one or more contraceptive methods while more than half were currently still using contraceptives. These figures were much higher than the national contraceptive prevalence rate of 25% (26), or those of specific geographic areas within the country such as 36.9% in Ashaiman (6), or in other developing countries such as Nigeria (38%) (30), Pakistan (49%) (31), and India (45%) (32). The study also reported participants’ socio-demographic factors such as age, occupation, and age at marriage as factors that significantly influenced a person's decision to use modern contraceptives. These findings are consistent with those reported by Apanga and Adam in the Talensi District of Ghana (8) where age and occupation were associated with modern contraceptive use. Likewise, some other factors that influenced contraceptive use among married women in Uaddara Barracks included the number of children alive and a desire for a male child, with those in favor of having more than two children being less likely to use contraceptives. In addition, women above the age of 40 years reported a less likelihood to use contraceptives, which reflects a time when many would begin menopause. However, another fact that needs stressing is the role husbands play in their wives’ decision to use contraceptives.
Whereas 80.6% of married women currently using any form of contraceptive reported it was their own decision to use contraceptives, this was however possible with 80.3% of them having the support of their husbands. This was a far higher percentage rate than that observed in other studies in Ghana or Uganda where although a majority of women were aware of contraceptives, only a small percentage of them were able to access contraceptives due to opposition from their husbands (6, 8, 18). Thus, the reason for a higher rate of husband support observed in this study could be attributed to the occupational status and educational level of husbands, factors which were significantly associated with contraceptive use among women in this study. Again, this could also be a matter of rural-urban differences where rural residents are less likely to use contraceptive methods compared to urban residents (21). Nevertheless, women who were married to military men were also observed to be significantly less likely to use contraceptives when compared to women with civil employee husbands. This could reflect fact that wives whose military husbands are always away on deployment could be disincentivized or apathetic to the use of contraceptives when compared to civilian wives whose husbands are mostly present with them at home. In the same vein, this study also observed that participants whose husbands were above 32 years at the time of marriage were less likely to support the use of contraceptives, which could reflect a greater desire to give birth at that age.
Although the findings of this study are consistent with other findings, the cross-sectional methodology and small sample size utilized in this present study made it difficult to determine the causal effect of the relationship between demographic characteristics, knowledge and marital factors, and contraceptive usage.
5. Conclusion
A large majority of married women at the Uaddara Barracks were adequately informed about contraceptives, with a higher percentage having ever used and continuing to use them than the national average. Women married to military men were found to be less likely to use contraceptives when compared to spouses of civilian employees living in the barracks. Likewise, the support of husbands for their wives' usage of contraceptives played a significant role in the women's ability to access and use them. As such, this underscores the need for interventional policies that prioritized the male as much as women, while also emphasizing the benefits of contraceptive use to military wives and men who could be apathetic toward contraceptive use due to the prolonged absence of military men from the home.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Committee on Human Research, Publications and Ethics (CHRPE) (reference: CHRPE/AP/384/18) of KNUST. The patients/participants provided their written informed consent to participate in this study.
Author contributions
DL, CO, and SN designed the study. Collection of research data and laboratory investigations were done by DL and YO. CO, EA, and HO performed data analysis and interpretation. DL, EA, and HO wrote the manuscript. CO, SN, and YO reviewed the manuscript. All authors contributed to the article and approved the submitted version.
Acknowledgments
The authors wish to express their profound gratitude to all the staff of the 4 Infantry Battalion (4BN) and participants at the Uaddara Barracks, who voluntarily participated in the research. Gratitude also goes to workers at the Department of Midwifery, St. Patrick's Nursing and Midwifery Training School, Offinso, and Department of Molecular Medicine, KNUST, Kumasi–Ghana.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fgwh.2023.1110024/full#supplementary-material
References
1. Lutz W, Kc S. Dimensions of global population projections: what do we know about future population trends and structures? Philos Trans R Soc B. (2010) 365(1554):2779–91. doi: 10.1098/rstb.2010.0133
2. DeSa UN. World population prospects: the 2012 revision. Population division of the department of economic and social affairs of the United Nations Secretariat, New York. (2013) 18p.
3. Speidel JJ, Weiss DC, Ethelston SA, Gilbert SM. Population policies, programmes and the environment. Philos Trans R Soc Lond B Biol Sci. (2009) 364(1532):3049–65. doi: 10.1098/rstb.2009.0162
4. Agyemang J, Newton S, Nkrumah I, Tsoka-Gwegweni JM, Cumber SN. Contraceptive use and associated factors among sexually active female adolescents in Atwima Kwanwoma district, Ashanti region-Ghana. Pan Afr Med J. (2019) 32:182. doi: 10.11604/pamj.2019.32.182.15344
5. Anasel MG, Mlinga UJ. Determinants of contraceptive use among married women in Tanzania: Policy implication. Afr Popul Stud. (2014). 28:976–88. doi: 10.11564/28-0-550
6. Asiedu A, Asare BY-A, Dwumfour-Asare B, Baafi D, Adam A-R, Aryee SE, et al. Determinants of modern contraceptive use: a cross-sectional study among market women in the Ashiaman municipality of Ghana. Int J Africa Nurs Sci. (2020) 12:100184. doi: 10.1016/j.ijans.2019.100184
7. Eliason S, Baiden F, Quansah-Asare G, Graham-Hayfron Y, Bonsu D, Phillips J, et al. Factors influencing the intention of women in rural Ghana to adopt postpartum family planning. Reprod Health. (2013) 10:34. doi: 10.1186/1742-4755-10-34
8. Apanga PA, Adam MA. Factors influencing the uptake of family planning services in the Talensi district, Ghana. Pan Afr Med J. (2015) 20(1):10. doi: 10.11604/pamj.2015.20.10.5301
9. Betran AP, Torloni MR, Zhang JJ, Gülmezoglu AM. WHO Working group on caesarean section. WHO statement on caesarean section rates. BJOG. (2016) 123(5):667–70. doi: 10.1111/1471-0528.13526
10. Stephenson R, Baschieri A, Clements S, Hennink M, Madise N. Contextual influences on modern contraceptive use in Sub-Saharan Africa. Am J Public Health. (2007) 97(7):1233–40. doi: 10.2105/AJPH.2005.071522
11. Cahill N, Sonneveldt E, Stover J, Weinberger M, Williamson J, Wei C, et al. Modern contraceptive use, unmet need, and demand satisfied among women of reproductive age who are married or in a union in the focus countries of the family planning 2020 initiative: a systematic analysis using the family planning estimation tool. Lancet. (2018) 391(10123):870–82. doi: 10.1016/S0140-6736(17)33104-5
12. Hong R, Fronczak N, Chinbuah A, Miller R. Ghana Trend analysis for family planning services, 1993, 1996, and 2002. Calverton, Maryland, USA: ORC Macro (2005).
13. Adjei KK, Laar AK, Narh CT, Abdulai MA, Newton S, Owusu-Agyei S, et al. A comparative study on the availability of modern contraceptives in public and private health facilities in a Peri-Urban community in Ghana. Reprod Health. (2015) 12:68. doi: 10.1186/s12978-015-0058-z
14. Machiyama K, Cleland J. Unmet need for Family planning in Ghana: Trends and Determinants. Strengthening Evidence for Programming on Unintended Pregnancy; Population Council; African Institute for Development policy (Ed.), Is access enough, (2013): 25p.
15. Casterline JB, Sinding SW. Unmet need for family planning in developing countries and implications for population policy. Popul Dev Rev. (2000) 26(4):691–723. doi: 10.1111/j.1728-4457.2000.00691.x
16. Nketiah-Amponsah E, Arthur E, Abuosi A. Correlates of contraceptive use among Ghanaian women of reproductive age (15-49 years). Afr J Reprod Health. (2012) 16(3):154–69.
17. Lauria L, Donati S, Spinelli A, Bonciani M, Grandolfo ME. The effect of contraceptive counselling in the pre and post-natal period on contraceptive use at three months after delivery among Italian and immigrant women. Ann Ist Super Sanita. (2014) 50(1):54–61. doi: 10.4415/ANN_14_01_09
18. Aryeetey R, Kotoh AM, Hindin MJ. Knowledge, perceptions and ever use of modern contraception among women in the Ga east district, Ghana. Afr J Reprod Health. (2010) 14(4):26–30. 23437509.21812195
19. Bhattathiry MM, Ethirajan N. Unmet need for family planning among married women of reproductive age group in Urban Tamil Nadu. J Fam Community Med. (2014) 21(1):53. doi: 10.4103/2230-8229.128786
20. Kabagenyi A, Jennings L, Reid A, Nalwadda G, Ntozi J, Atuyambe L. Barriers to male involvement in contraceptive uptake and reproductive health services: a qualitative study of men and women’s perceptions in two rural districts in Uganda. Reprod Health. (2014) 11(1):21. doi: 10.1186/1742-4755-11-21
21. Marrone G, Abdul-Rahman L, De Coninck Z, Johansson A. Predictors of contraceptive use among female adolescents in Ghana. Afr J Reprod Health. (2014) 18(1):102–9. 24796174.24796174
22. Obwoya JG, Wulifan JK, Kalolo A. Factors influencing contraceptives use among women in the Juba city of South Sudan. Int J Popul Res. (2018) 2018:1–7. doi: 10.1155/2018/6381842
23. Beson P, Appiah R, Adomah-Afari A. Modern contraceptive use among reproductive-aged women in Ghana: prevalence, predictors, and policy implications. BMC Women’s Health. (2018) 18(1):1–8. doi: 10.1186/s12905-018-0649-2
24. Sonfield A, Hasstedt K, Gold RB. Moving forward: family planning in the era of health reform. (2014).
25. Eliason S, Awoonor-Williams JK, Eliason C, Novignon J, Nonvignon J, Aikins M. Determinants of modern family planning use among women of reproductive age in the Nkwanta district of Ghana: a case-control study. Reprod Health. (2014) 11(1):65. doi: 10.1186/1742-4755-11-65
26. Ghana Statistical Service (GSS). Ghana Malaria Indicator Survey, 2016. Ghana Health Service (GHS), and ICF. (2017).
27. Wade DM, Hankins M, Smyth DA, Rhone EE, Mythen MG, Howell DC, et al. Detecting acute distress and risk of future psychological morbidity in critically ill patients: validation of the intensive care psychological assessment tool. Crit Care. (2014) 18(5):519. doi: 10.1186/s13054-014-0519-8
28. Kamangu AA. Perceptions on the availability, accessibility and use of modern contraceptive methods among women in iringa municipality, Tanzania. Int J Humanit Soc Sci. (2016) 6(9):123–7.
29. Nakirijja DS, Xuili X, Kayiso MI. Socio-economic determinants of access to and utilization of contraception among rural women in Uganda: the case of wakiso district. Health Sci J. (2018) 12(6):1–20. doi: 10.21767/1791-809X.1000608
30. Osaro BO, Tobin-West CI, Mezie-Okoye MM. Knowledge of modern contraceptives and their use among rural women of childbearing age in rivers state Nigeria. Ann Trop Med Publi Health. (2017) 10(4):1043. doi: 10.4103/ATMPH.ATMPH_762_16
31. Khan A, Hashmi HA, Naqvi Z. Awareness and practice of contraception among child bearing age women. J Surg Pak (Int). (2011) 16(4):179–82.
Keywords: contraceptive use, condom, women, Ghana, Africa
Citation: Lumor DA, Obirikorang C, Acheampong E, Obirikorang Y, Owusu H and Newton S (2023) The relevance of knowledge, perception, and factors that influence contraceptive use among married women living in Uaddara Barracks, Ghana. Front. Glob. Womens Health 4:1110024. doi: 10.3389/fgwh.2023.1110024
Received: 28 November 2022; Accepted: 2 August 2023;
Published: 15 August 2023.
Edited by:
Stephen Kennedy, University of Oxford, United KingdomReviewed by:
Adu Appiah-kubi, University of Health and Allied Sciences, GhanaAndrea Jimenez-Zambrano, University of Colorado, United States
Loretta Bass, University of Oklahoma, United States
Seth Feinberg, Western Washington University, United States
© 2023 Lumor, Obirikorang, Acheampong, Obirikorang, Owusu and Newton. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Daisy Afra Lumor ZGFnZGFpc3lnQHlhaG9vLmNvLnVr