 Oyeteju T. Odufuwa
Oyeteju T. Odufuwa
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Glob. Womens Health , 29 June 2022
Sec. Women's Mental Health
Volume 3 - 2022 | https://doi.org/10.3389/fgwh.2022.787263
This article is part of the Research Topic Reproductive Health and Mental Health in LMICS: Women’s Health View all 9 articles
The mental healthcare-seeking behavior of postpartum mothers has received little attention in Nigeria. Previous studies in the country have focused on determinants of physical health-seeking behavior, choice of maternal healthcare provider, prevalence, and determinants of maternal mental illness, yet, determinants of maternal mental health-seeking behavior among Nigerian women has been understudied. This study, therefore, examined the determinants of mental health-seeking behavior among postpartum women in Ibadan, Nigeria. Maternal mental illness, which was proxied using postpartum depression, was computed using the Edinburgh Postpartum Depression Scale. Data for the study were obtained through a survey method using a 9-page questionnaire. A 3-stage sampling technique was employed. The first stage was a stratified sampling to disaggregate the health facilities offering postnatal and immunization services on the basis of ownership of public and private healthcare providers. In the second stage, seven healthcare facilities comprising three (3) private and four (4) public healthcare were purposively selected based on the number of attendees. The final stage was a random selection of 390 postpartum mothers attending postnatal and immunization clinics across seven healthcare facilities. The prevalence of depression among the mothers was 20.8%. While only 39.5% of the depressed women sought care, 22.3% of the non-sufferers also sought mental healthcare. This revealed that both sufferers and non-sufferers sought mental healthcare. Also, a higher incidence of postpartum depression among the sufferers increased the likelihood of seeking mental healthcare. Age, family history of postpartum depression, and having the desired gender of child were determinants of mental health-seeking behavior. Among the sufferers of postpartum depression who failed to seek care, a low perceived need for mental healthcare, the perception that the depressive symptoms will go on their own, as well as fear of being stigmatized as a “weak mother”, were reasons for not seeking mental healthcare. Thus, to promote mental healthcare, the non-cost factors, like availability and accessibility to a mental healthcare facility should be addressed. To achieve this, mental healthcare sensitization programs should be integrated into maternal healthcare at all levels, and mothers attending antenatal clinics should be routinely screened for early symptoms of depression in the postpartum period.
Health is integral to the attainment of economic growth and sustainable development of any nation (1). The total health and well-being of an individual are ultimately dependent not only on the physical but also on the mental health status of its people (2). However, more attention has been paid on the physical health of the populace (1), while the mental aspect has often been neglected, especially in developing countries (Nigeria inclusive).
In Nigeria, an estimated 20 to 30% of its over 200 million population is believed to suffer from mental illness (3). Studies on mental health in the country had focused on the prevalence of mental illnesses (4–6), its risk factors (7, 8), and the perception and attitude of people to mental illnesses, especially stigmatization (9). The aspect of mental health-seeking behavior has been grossly understudied both in Nigeria and other parts of the world (10).
Specifically for women, the most common mental illnesses experienced in the postpartum period are postpartum blues, depression, anxiety, and psychosis (11, 12). Approximately 10 to 20% of pregnant and postpartum women experience any of these mental health problems; primarily depression and /or anxiety during pregnancy or after childbirth (13–15). This rate is often higher in developing countries where about 15.6 and 19.8% of pregnant and new mothers, respectively, experience psychiatric disorders. Norhayati (16) observed a postpartum period depression (PPD) prevalence ranging between 1.9 and 82.1% globally; 2.2 and 74% in developed and developing countries, respectively.
Postpartum period depression, which is one of the most common maternal mental illnesses, has been identified as a worldwide public health issue and the leading contributor to the disease burden in women of reproductive age (17). In Nigeria, a PPD prevalence rate of 14.6% has been observed in the South West (5); 22.9 and 34.6% in Enugu, South East (6, 8), and 21.8% in Jos, North Central (18). This high prevalence rate of PPD in the country, the accompanying consequences of this invisible illness on the mother and infant, coupled with the few neuropsychiatric healthcare facilities (eight) in the country, is a cause for concern (5, 6).
Globally, the provision of mental healthcare services to the citizenry has been identified as one of the responsibilities of government (19). Yet, the Nigerian government lags in this role despite its whopping number of cases. The current mental health system in Nigeria is characterized by grossly inadequate mental health facilities (only eight federal neuropsychiatric hospitals exist in the nation), human resource inadequacy, and failure to implement the existing Mental Health Policy (20).
There is a dearth of studies on mental health-seeking behavior in Nigeria. Most studies reveal that women experiencing mood disorders in the postpartum period rarely seek help (10, 12, 21–24). In addition, in most countries, Nigeria inclusive, women hardly attend the scheduled six (6) weeks postnatal check-up (25).
The peculiarity of mental healthcare can be seen in 3-folds: the first is the need for long-term consistent treatment of the affected women (26). The second is the human resource need for treating mental disorders which also require a different cohort of professionals to provide adequate care for the patient (20). The third is the stigma associated with people undergoing mental care (24, 27).
Age, marital status, education, household headship, size, and expenditure were identified as determinants of health-seeking behavior among Nigerians (1). It was also observed that members of the household preferred first to consult traditional, patent medicine vendors (PMVs), and religious bodies (churches/mosques) before consulting healthcare professionals (HCPs). In addition, Murithi (28) has identified gender, quality of service, information about this quality, user fees, and wealth as determinants of the demand for healthcare in a rural slum in Nairobi, Kenya. Olasehinde and Olaniyan (29) have also found that prime-age adults had lower chances to seek care than children and old-age. Hence, adults in their prime years, regardless of gender, are less likely to seek care.
Household size, distance, the total cost of healthcare, and the quality of access routes were found as determinants of healthcare services in Kogi State, Nigeria (30). Household headship and level of education were found to be vital determinants of seeking healthcare during illness in Kwara State, Nigeria (31). Gender was also observed to play an important role in the decision of individuals to seek care in Edo State, Nigeria, as older men were seen to have poor health literacy and health-seeking pattern (32).
Proximity to a facility, quality of care received, insurance coverage, income, health status, education, age, and gender were found to be predictive factors in seeking healthcare in rural China (33). These factors were also affirmed by Gotsadze, et al. (34) in Georgia who further revealed that personal status, means of payment, level of education, and religious beliefs were factors that could deter or encourage an individual to seek healthcare during illness.
Maternal mental health problems are often undiagnosed, untreated, or undertreated (15). Often, mothers, despite having access to healthcare practitioners, fail to seek healthcare, and even if they do, they do not receive the appropriate healthcare (24, 35). James and Blank (34) and Smith (36) also found stigmatizing attitudes toward mental health, unfamiliarity with the signs and symptoms of perinatal mental illness, and insufficient knowledge among healthcare providers, which all contributed to the delay to seek mental healthcare. Rural residence and being divorced or unmarried (marital status) were found to be associated with lower use of mental health services in a community in Northwestern China (37). The failure of people to seek healthcare in cases of mental illness over a lifetime increased the prevalence of mental disorders by 21%, while the lifetime use of mental health services reduced the prevalence to 2.45 and 4.67%.
Factors affecting mental health-seeking behavior in the United Kingdom include expectations and experiences of mental healthcare professionals, the cultural needs, uncertainty of the role of professionals in providing the needed support, the perception that available healthcare was ineffective and inappropriate, hesitancy to approach professionals they were not familiar with, lack of continuity of care, and knowledge and experiences of healthcare during pregnancy (24). Bruffaerts, et al., (38) affirmed the case of “the worried well” who sought mental health treatment when they did not meet the criteria for a mental disorder. Hence, for PPD among mothers, most of the affected women do not seek care, while some who seek care are not diagnosed with mental illness.
In Nigeria, physical access to general and specialized mental healthcare, which is provided by the government, is limited to eight locations of the clinics, the few departments of psychiatry in the teaching hospitals and the privately-owned neuropsychiatric clinics, making it inequitable. This is quite worrisome. The limited access to mental health services impacts negatively on the decision of patients and their families to seek or not to seek mental healthcare.
This study was therefore aimed at examining the mental health-seeking behavior of postpartum women and the determinant factors of the decision to seek or not seek care. The hypothesis is that given a relatively high prevalence of PPD (as a proxy for mental illness during postpartum in Nigeria), the demand for mental healthcare is proportionally much less than it is expected to be. The objectives of this study are to (1) determine the factors making the sufferers of PPD seek or not seek mental healthcare, (2) determine the proportion of PPD sufferers and non-sufferers who seek mental healthcare, and (3) identify cost- and non-cost related factors preventing women suffering from PPD from seeking mental healthcare.
A facility-based survey was conducted among mothers with babies below 18 months, attending postnatal and immunization clinics in Ibadan, the capital of Oyo State, Nigeria. Ibadan, which is one of the highly populated metropolitan cities in Nigeria, has one of the highest postnatal attendances in the country (25). The choice of mothers with children below 18 months is due to the proposition that there are cases of PPD that present at birth and extend beyond the first year of birth (8, 23). Participants were contacted at the clinics and were invited to participate in the study by filling out the questionnaires with the aid of the research team.
A three-stage sampling technique was employed. The first stage was a stratified sampling to disaggregate the health facilities offering postnatal and immunization services, on the basis of ownership, into public and private healthcare providers. Free immunization services are provided in public healthcare facilities in the country, while private facilities provide paid immunization services that extend from birth to beyond 18 months. In the second stage, seven healthcare facilities comprising three (3) private and four (4) public healthcare facilities were purposively selected based on clinics with the highest number of attendees (patronage). The final stage was a random selection of 390 women whose children were between 2 weeks and 18 months, across the seven (6) healthcare facilities based on their willingness to participate in the study.
Ethical approval for this study was obtained from the Research and Ethical Committee of the University of Ibadan/University College Hospital Ethical Review Board (UI/UCH ERB) with the number NHREC/05/01/2008a in Ibadan, Oyo State, Nigeria. Consent was also obtained from the management of each hospital used in the study. The participation of the respondents was voluntary and based on verbal and written informed consent. They were also informed about their right to withdraw from participation if the need arose. The collected information was kept confidential and all data were anonymized, which minimized the risk of integrity infringement.
Data for the study were collected from mothers who brought their children for immunization services in the seven (6) healthcare facilities used. In this study, for the private healthcare providers, most of the immunizations were paid for, including the special vaccines. However, for the public clinics, all the vaccines were provided free of payment. As such, most rural mothers would rather visit the public healthcare facilities, while the mothers who were covered by the community-based or personal health insurance utilized the private facilities.
The administration of the research instruments was done in three phases. The first phase, which took place in June 2019, was to conduct a pilot study using the research instruments. The second phase was conducted for about 4 weeks in August 2019 after which a 12-week break was taken to ensure the availability of new cohorts of mothers at the immunization clinics. This was necessary because most immunizations were given at 4 weeks intervals. The final phase was conducted between December 2019 and January 2020. A five-man research team (comprising two student nurses, 2 field officers, and the Principal Investigator) who could speak Yoruba, the indigenous language fluently, was recruited to assist in the questionnaire administration. The response rate was about 75% across the seven (7) clinics. The clinical information of the mothers was not explored in this study because for most of the sampled mothers, the delivery location and choice of child immunization differed. The choice of child immunization clinics by mothers is often based on proximity to the mother's location.
Postpartum depression was measured using the Edinburgh Postpartum Depression Scale (EPDS). It is a widely used, standardized 10-item self-administered questionnaire with scores ranging from 0 to 3 for each of the ten items (39). The positively worded items were scored in reverse order before summing up. The responses provided on the EPDS scale are then summed up resulting in a total minimum of zero (0) and a maximum of 30. The incidence of PPD was identified using a cutoff of 12 on the EPDS scale. This cutoff has also been employed in similar studies (12, 18, 40–43). Women who had a score of 13 and above were classified as experiencing probable clinical depression, while those between 0 and 12 were identified to be void of depressive symptoms.
The choice of a cutoff of 12 to indicate probable signs of depression is because it maximizes sensitivity and specificity among postpartum women (44). The mental health index (EPDS) was tested for reliability using Cronbach's Alpha. The internal consistency of similar questions within the EPDS scale as estimated by the Cronbach's Alpha in the questionnaire study was 0.82 (Table 1). This finding is similar to a Cronbach's alpha of 0.89 by Adewuya, et al. (5). This shows the scale is highly reliable and valid for measuring depression in the postpartum period.
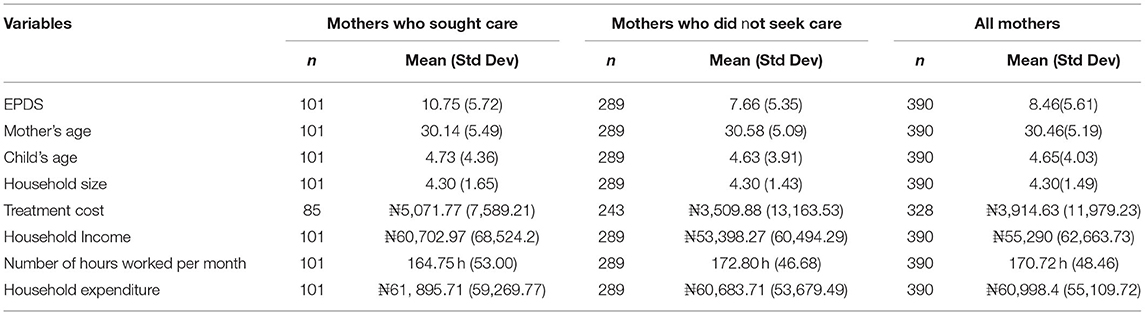
Table 1. Descriptive characteristics of continuous variables.
A probit regression was employed to estimate the determinants of mental health-seeking behavior. The probit model is one of the simplest forms of the qualitative response regression model in which the dependent variable is binary, taking the form of “1” if an attribute is present and the value of “0” if that attribute is absent. In this case, the presence of the attribute is the probability of seeking healthcare while its absence is the decision not to seek mental healthcare.
This study adopted the determinants of a health-seeking theory which specifies a model that identifies factors that influence the health-seeking pathway. The theory assumes that various factors determine the decision of an individual to seek (demand) healthcare and identifies broad determinants of this decision (genetics, behavioral, environmental and physical influences, medical care, and social and economic factors). In this study, the determinant factors are broadly characterized into four: individual woman, household, cost of treatment, maternal and child, and labor market characteristics.
The individual woman characteristics (IWCi) comprises the age (disaggregated into young mothers— <25 years; middle-aged mothers—between 25 and 40 years; and older mothers—above 40 years), religion (Christianity and Islam), and educational status of the woman which was classified into the four broad categories: no education, primary, secondary, and post-secondary education. The mental health index (MHIi) adopted the EPDS score to compute the presence (13–30) or absence (0–12) of depressive symptoms among the postpartum mothers. The household characteristics (HHi) include household size (numerical), family structure (polygamous or monogamous), and the presence or absence of a family history of PPD.
The cost of treatment (Log(CTii)) measures the cost of mental healthcare to include the cost of consultation, medication, admission, and other cost incurred during treatment; the value was however logged as it was skewed. Based on the theory of demand, mental healthcare is also perceived as good wherein there is an inverse relationship between price (care cost) and demand for mental healthcare. The labor market characteristics (LMCi) comprised the employment status of the woman and her spouse (being employed or not), the number of hours worked per month, and household income (sum of wage and non-wage income).
The data obtained were coded and analyzed using the IBM Statistical Package for Social Sciences SPSS version 21 and STATA 15, respectively. The probit regression analysis requires that one of the outcomes of the categorized variables be fixed as a reference category and the results would then be interpreted in relation to the reference category (45, 46).
Questionnaires were distributed to 520 mothers. Responses were received from 390 respondents (75% response rate) of whom 63 (16.15%) were below 25 years, 316 (81.03%) were between ages 25 and 40 years, and only 11 (2.82%) were above 40 years. On average, the mean age of the respondents was 30 years, while the mean age of the babies was about 5 months. Most of the respondents were married (91.28%). While 299 (76.67%) of the respondents had post-secondary education, only 91 (23.33%) of the women had at most secondary educational qualifications. Among the respondents, 283 (72.56%) of the women were Christians and 107 (27.44%) were Muslims. Most of the mothers were from a monogamous family structure (89.71%), though several of them still lived with extended family members, which is expected based on the cultural practice in Nigeria, especially where new mothers are expected to live with their in-laws.
Of the total women sampled, 209 (53.63%) of the mothers had a male child while 181 (46.41%) birthed male children. Based on the desirability of the gender birthed, 320 (82.05%) mothers had their desired gender of a child while 70 (17.95%) did not. The mode of delivery revealed that 63.33% of the mothers had their child through vagina delivery while 36.67% went through a cesarean section. Among the mothers, 42.3% were primiparous - first-time mothers, while 220 (56.4%) of the mothers were multiparous (had between 2 and 3 children), and only 5 (1.2%) had more than 5 children (grand-multiparous).
The labor market characteristics of the respondents revealed that 285 (73%) mothers were employed while 105 (26.7%) were unemployed. Most of the spouses (92.05%) of the mothers were employed while only 7.95% were unemployed. The mean household size was 4.3. The mothers worked for about 170 h per month. Most of the households earned less than their expenditure as the average household income was N55,290 naira while the mean household expenditure was about N61,000.
The descriptive statistics of the continuous and categorical variables are presented in Tables 1, 2. The results as presented in Table 2 show that 81 out of 390 women presented symptoms of depression in the postpartum period, revealing a PPD prevalence rate of 20.8%. However, only 39.5% (32 out of 81 sufferers) sought healthcare; 60.5% of the women, who suffered from PPD, did not seek mental healthcare. Ironically, among the 309 non-sufferers of PPD, 22.3% (69 out of 309 non-suffers) also sought healthcare. Thus, among all the 101 women who sought mental healthcare, only 31.7% had depressive symptoms in the postpartum period, while 68.3% had no evidence of suffering from PPD.
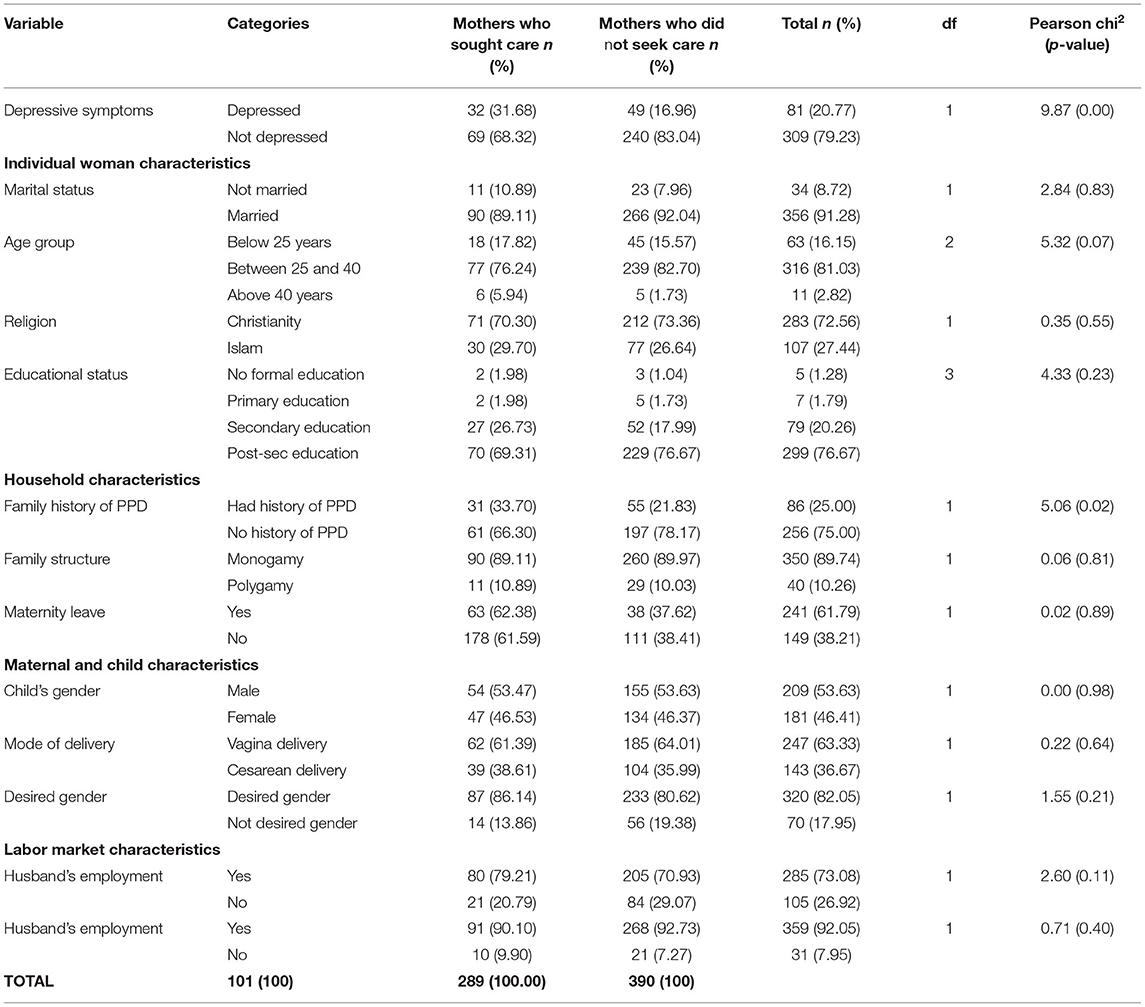
Table 2. Descriptive characteristics of categorical variables.
It is evident from this study that both sufferers and non-sufferers of PPD sought mental healthcare. A possible reason for this is that the symptoms of PPD and other emotional symptoms experienced by mothers after delivery (such as baby blues) are quite similar. The difference is often in the duration of PPD compared to other symptoms. Symptoms of maternity blues often occur from birth to 14 days postpartum while PPD extends to a year postpartum and beyond in some cases.
In terms of the mental healthcare provider, the study revealed that most of the women (62.38%) sought healthcare through self-treatment, while 13.9 and 18.8% sought treatment from religious bodies and general hospitals, respectively. Only 5% sought healthcare from specialized neuropsychiatric hospitals. Self-treatment, in this case, included treatment from self-medication and consultation with friends and family. Reasons provided by the 60.5% of mothers who though suffered from PPD but did not seek mental healthcare included fear of dying, being stigmatized, perceived non-severity of the illness, belief that the symptoms will fade away, the perception that prayers and faith in God will sort the feeling, and fear of being tagged “a weak mother”.
The average treatment cost of PPD was about N3,914.63 as presented in Table 1. Women who sought care worked for fewer hours per month (164.8 h) compared to women who did not seek care (172.8 h). The reverse is observed for the household income. Women who sought care had an average household income of N60,702.97, compared to N53,398.27 of their counterparts who did not seek care. Furthermore, the bivariate analysis using the chi-square showed that being depressed (p = 0.00), women's age (p = 0.07), and family history of PPD (p = 0.05) were significantly related to the likelihood of seeking mental healthcare.
Table 3 presents the probit regression estimates of the determinants of the mental health-seeking behavior model to identify whether mothers who had experienced postpartum depression were more or less likely to seek mental healthcare. The relationship among the outcome variables (probability of seeking mental healthcare), presence of postpartum depressive symptoms (PPD), and the potential mediating variables was first estimated using the individual woman and household characteristics comprising age, marital status, religion, education, household size, and family history of PPD (Column 1), then adjusted for treatment cost and maternity leave (Column 2), maternal and child characteristics (Column 3), and then labor market characteristics (Column 4).
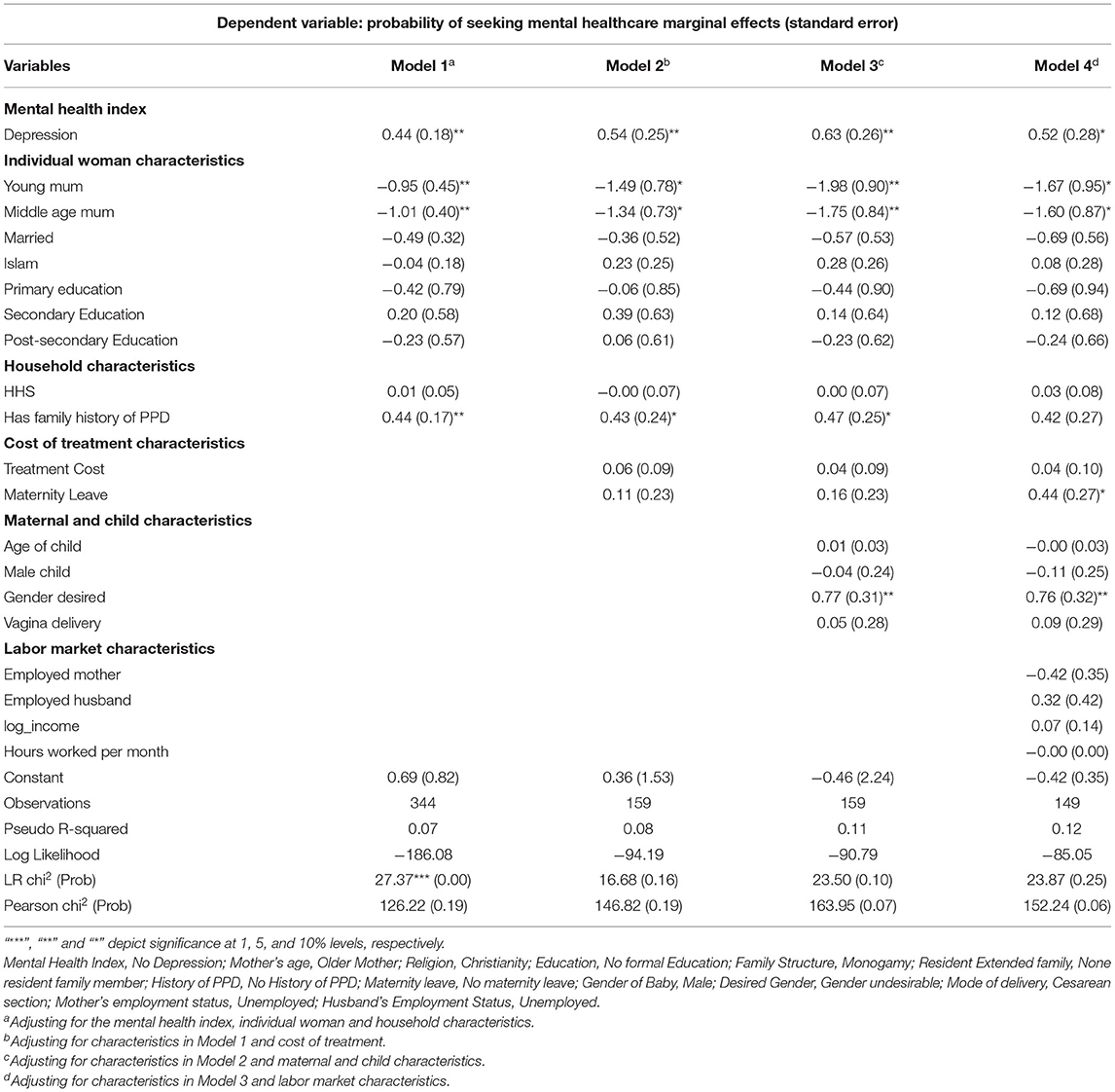
Table 3. Probit regression results of determinants of probability of seeking mental healthcare.
The results of the estimation as shown in Table 3 reveal that a higher incidence of PPD significantly predicts a higher probability of seeking mental healthcare among sufferers of PPD relative to non-sufferers. This effect is positive and significant across all four columns. However, the probability increases from 0.44 in the baseline estimates to 0.54 with the introduction of treatment costs and maternity leave. This likelihood further rose to 0.63 when maternal and child characteristics were incorporated into the model. The probability of seeking mental healthcare however decreased to 0.52 when labor market characteristics were integrated into the model. More severe cases of PPD might be disabling enough to propel the sufferers to seek mental healthcare.
With regards to age, the estimates show that younger (below 25 years) and middle age (between 25 and 40 years) mothers were less likely to seek mental healthcare relative to older mothers (above 40 years). Being a younger and middle-aged mother reduced the likelihood of seeking mental care by 0.95 and 1.01, respectively, relative to being an older mother. This likelihood increased to 1.49 for the younger mothers and 1.34 for middle-aged mothers when adjusted for treatment cost, 1.98 and 1.75 when adjusted for maternal and child characteristics while it reduced to 1.67 and 1.60 when labor market characteristics were introduced. The same trend, with a lower probability, is observed with middle-aged mothers in comparison with older mothers. This might be closely related to the ability of older mothers to better differentiate between PPD and the normal baby blues associated with recent childbirth, based on their experience as compared to the experience of younger mothers. Other individual woman characteristics (marital status, religion, education, and household size) were not significant determinants of MHSB.
Having a family history of PPD was significant. Mothers who had a family history of postpartum depression had a higher probability (0.44) of seeking mental healthcare. This effect remains almost the same even after controlling for the cost of treatment and maternal and child characteristics. However, having a family history of PPD became insignificant after controlling for labor market characteristics. The significance of a history of PPD in the woman's family can be because the sufferer will be encouraged to seek prompt healthcare as the invisible illness will not be misconstrued as any other illness. In addition, family members will most likely understand the symptoms and be aware of places where to seek healthcare.
The cost of treatment and maternity leave were both not significant as determinants of women seeking healthcare in the second and third columns. Across all the models, care cost was not a determinant of the decision of seeking mental healthcare. Its non-significance might reveal that regardless of the cost of treatment, women with severe cases of PPD will still seek care.
Women who had maternity leave from work had a higher likelihood of seeking mental healthcare (0.44) compared to their counterparts who did not have maternity leave. It is important to note here that maternity leave is given to women who work in formal employment, thus they can recuperate before returning to their paid employment. However, the self-employed might find it difficult to have a structured maternity leave. Having a maternity leave provides ample time for the mother to seek care before the resumption of work.
Women who desired a particular gender for their child (preferably male due to the patriarchal nature of Nigeria) were more likely to seek care (0.77) relative to those who did not have that desire. This effect was almost the same (0.76) even when labor market characteristics were included in the model. This could be due to the feeling of security of the woman, owing to the belief that if she has a male child, she has secured the love and attention of her spouse.
This study confirms some similarities in determinants of mental health-seeking behavior in Nigeria as compared with other countries. But there are also significant peculiarities and surprises in the behavior pattern.
The most prominent reason identified for failing to seek mental healthcare was a lack of knowledge of the symptoms of the illness, as most of them argue that they did not recognize the symptoms as requiring health-seeking behavior. Childbirth and child care immediately after birth are demanding both physically and mentally. Most women appear not to be able to differentiate between the challenges of childcare after birth and mental health issues. This is an outcome of low and weak mental health education. This is supported by the findings of Whitton (21) who opined that although most women suffering from PPD recognized there was something wrong, more than 80% of them did not report their symptoms to any health professional. This might be due to a lack of experience in differentiating between the demands of childcare after childbirth and mental health conditions.
In addition, mental health is associated with stigmatization. In the Nigerian case, stigmatization work in two ways. First, a new mother is expected to be strong without showing signs of weakness while taking care of the baby. Most women are therefore unwilling to seek care because of the stigmatization of being labeled “a weak or incapable mother” (11, 12). The second level has to do with the stigmatization of mental illness itself whether it is caused by childbirth or not.
Furthermore, many women do not seek healthcare when there is a perception of non-severity of the symptoms. The perceptions that “the symptoms will go by itself ”, and that “there is no need to seek for healthcare” were dominant among the mothers. In an extreme case, a respondent stated she did not want to die as her reason for not seeking care. A few mothers stated that it was a personal issue that could be handled personally “by myself ”. While there is a lot of support system from older family members, especially the in-laws during the period of childbirth, the mother is also careful to be seen as strong and capable of caring for her new child, especially before her in-laws. The perception of the non-severity of the symptoms felt by these mothers can be attributed to the lack of physical visible symptoms of mental illness as compared to visible symptoms of physical illnesses. This is also a reflection of the lack of awareness of mothers about PPD, its symptoms, and associated dangers. This calls for public education with a focus on mothers.
Of particular interest is the fact that while only 39.5% of depressed women sought care, 22.3% of non-sufferers also sought mental healthcare. This shows that both sufferers and non-sufferers sought mental healthcare. It also affirms the notion of “the worried well” by Button, et al. (24) who opined that those who seek care for mental illness were not diagnosed with the illness. The communal nature of the Nigerian society might be a reason for this where the more experienced and older members of the family are to have the capacity to diagnose an illness whether visible or not. This further indicates that regardless of the nature of the symptoms felt, there is a lot of uncertainty and difficulty in recognizing PPD and indeed other mental disorder symptoms, despite the notion by Gaynes et al. (13), Bowen, et al. (14), and Li, et al. (15) who affirm that ~10–20% of pregnant and postpartum women experience depression and /or anxiety during pregnancy or after childbirth.
In addition, it was observed that most of the women who sought care, did so informally; through self-medication which included being treated by themselves and/or consulting with friends and family. This was also observed by Goyal, et al. (12) who concluded that some of the mothers who had symptoms of PPD were unaware and did not perceive it as a psychological illness. The more experienced family members in Nigerian society are also more likely to proffer the expected nature, prospect, and possible solution to such illnesses. Furthermore, the nature of the healthcare system in the country is such that over 70% of healthcare expenditure is out-of-pocket. The economic condition of the country, which features a high level of poverty and income inequality, further worsened by the COVID-19 pandemic, makes it difficult to devote the financial resources required for the intensive and long-term nature of mental health treatment.
Only 5% of the women sought healthcare from a specialized neuropsychiatric hospital. This might be closely linked to the absence of a neuropsychiatric hospital in Oyo State (the study area), even though a department of psychiatry exists in the University College Hospital located in the state. This finding is affirmed by Whitton (21), whose study revealed that 54% of the women who sought care spoke to friends and family and only 4% spoke to a health practitioner.
A higher incidence of postpartum depression among the sufferers increased the likelihood of seeking mental healthcare. This is supported by the finding of Andrade, et al. (47), Kessler, et al. (48), Tegegne and Legese (49), and Grissette, (50) who opined that the severity of illness, not the cost of treatment, motivated the demand for mental healthcare. Severe PPD necessitating seeking healthcare could be attributed to the disabling nature of severe cases of PPD, where the woman is unable to cope with the normal stresses of life, thereby leaving the patient with no choice but to seek healthcare.
Women whose family members have had a history of PPD were more likely to seek care. This is substantiated by Bina (51) who opined that predictors of women with PPD seeking healthcare had a history of depression. Also, since most of the women sought healthcare from family and friends, having a family history of PPD could be attributed to the family member's knowledge of the symptoms and nature of PPD and not stigmatizing the affected women about PPD being a sign of weakness. Also, family intervention and support are perceived to play strategic roles in healthcare-seeking as they increase health literacy as observed by Odaman and Ibiezugbe (32) and Smith (36). A sufferer whose family member had experienced PPD has higher chances of seeking care since such family members will be able to distinguish between symptoms of the expected maternity blues and PPD and encourage the new mother to seek mental healthcare. This is affirmed by Button, et al. (24) who opined that informal consultation with another person with whom the woman is familiar influences her decision to seek healthcare.
The non-significance of religion in this study contradicts the results of Gotsadze, et al. (34) who identified religion or religious beliefs as a supporting factor to seek healthcare. This finding differs from the conventional belief that religion provides support for the people. The case of mental illness is peculiar, as the cultural belief of stigmatization and the choice of the victims to seek self-treatment is likely to undermine the expected supportive roles played by religion. This finding also contradicts Olasehinde (1) who found that household members prefer to consult traditional healers, patent medicine vendors (PMVs), and religious bodies (churches/mosques) before consulting healthcare professionals (HCPs). In this study, this could be explained by the fact that as self-selected participants already at a health facility, they had overcome any potential religion-related barriers.
Contrary to the findings of Tegegne and Legese (49), marital status was not found to be a significant determinant of PPD health-seeking behavior. This suggests that the presence or absence of a spouse is inconsequential for the choice to seek care. In Northwestern China, being divorced or unmarried (non-marital status) was found to be associated with lower use of mental health services (37). Perhaps this disparity highlights the differences in cultural attitudes and contexts of marriage in Nigeria (Africa) and China. It could mean in China, the core family (husband and children) constitutes the main support to a mother. However, in Africa, there are many informal and extended family relations, which play a significant role in supporting mothers. This might be attributed to the fact that in the choice to seek mental healthcare in Nigeria, the extended family plays a more influential role than the nuclear family. Hence, being married or not, does not greatly impact the decision to seek care.
The non-significance of the treatment cost in the decision to seek mental healthcare contradicts the findings of Hjortsberg (52), Jameson (53), Muriithi (28), Olasehinde (1), and Hossain et al. (23) who observed that user costs were a major deterrent of seeking care. This finding would be intriguing if it was a community-based study, given that treatment always comes at a cost and is the commonest deterrent of demand for healthcare in general. However, this was a study of self-selected mothers who were already in a health facility; that is, they were mothers who could afford to pay for healthcare. Therefore, treatment cost was not an issue. Furthermore, against the perception of many, the treatment of mental illness, though long term, is often not as expensive as assumed. Unlike physical illness, mental illness requires the consistent creation of an enabling environment for the sufferers to thrive and do away with the triggers of the mental illness.
The study shows that based on age, young (below 25 years) and middle-aged (between 25 and 40 years) mothers were less likely to seek mental healthcare relative to older mothers (above 40 years). This is supported by the studies of Muriithi (28), Olasehinde (1) who also found that the probability of seeking professional healthcare increases with age. Thus, being a younger or middle-aged mother reduced the likelihood of seeking mental healthcare. The finding that only older mothers were likely to seek mental healthcare could be due to the previous experience of such mothers who might be likely to be able to understand the peculiarity of the symptoms they might be experiencing. This is also confirmed by Olasehinde and Olaniyan (29) who found that the adults in prime age, regardless of gender, are less likely to seek healthcare (54). This is in line with a general perception about the human life cycle: those who are in their prime years are healthier and less likely to get serious health conditions, and therefore less likely to seek healthcare.
The finding of the non-significance of income and employment status of both the woman and her spouse contradicts evidence from the study of Gotsadze et al. (34) in China and Bina (51) and Hansotte, (11). In contrast to the findings of Olasehinde (1) and Muriithi, (28), income did not affect a mother's decision to seek mental healthcare. This finding is expected since user cost was also observed as a non-determinant. Again, this is not surprising, given that the study participants were self-selected by already being at a health facility, meaning they were able to afford healthcare. Those who could not afford to pay for healthcare would not be found at a health facility. The mothers who sought healthcare possibly all came from a higher income bracket supported by employment or other forms of getting income. Thus, labor market outcomes in Nigeria are not essential factors in determining the health-seeking behaviors of sick individuals.
The long-term nature of the treatment (drugs and therapy) dissuaded some mothers from seeking healthcare as they stated they would rather pray about the symptoms. This could be perceived as an attitudinal barrier to not only seeking but also staying in treatment, as affirmed by Andrade et al. (47). The extended period of treating mental illness is often perceived to be accompanied by the stigmatization of continual hospital visits. This calls for the sensitization and education of mothers and the public about PPD.
It is evident from the low proportion of women who sought healthcare that there is low mental health literacy in the study area as evidenced by women with PPD who gave the reason “It will go away on its own”. This belief by the affected women of their experiences being part of their “destiny” is affirmed by Bruffaerts et al. (38) and Small et al. (55). It is important to promote mental health awareness among postpartum mothers. To this end, PPD should be routinely screened during postnatal and immunization clinics. In addition, there is a high level of stigmatization and discrimination associated with mothers experiencing depression in the postpartum period. This can discourage sufferers from seeking healthcare for mental illness, as affirmed by Button et al. (24), Adjorlolo et al. (56) and Goyal et al. (12). It is therefore vital to engage the community, religious, and traditional leaders to promote community sensitization efforts on mental health issues in the country.
The study has several limitations. First is the high non-response rate because most of the mothers were playing a dual role of filling the questionnaire and caring for the baby, as most of the respondents were from the immunization rather than postnatal clinics. This is because of the very low postnatal attendance in Nigeria. Also, most of the sampled women hardly knew the exact time of onset and duration of the depressive symptoms. Another limitation of this study that may have affected the detection rates of postpartum depression is the use of only a self-administered questionnaire to measure depression, without combining it with the clinical records of the respondents.
The study was facility-based, and as such women who did not attend either postnatal or immunization services were excluded from the study. The strengths of this study include its large sample size and the diversity of the study sample in terms of the use of private and public healthcare providers which can indicate various socioeconomic statuses.
Most depressed women are unaware that they are experiencing a treatable mood disorder. The severity of mental illness, age, and family history of PPD are the main determinants of demand for mental healthcare in the study area. While having a family history of postpartum depression, the desired gender of the child and experience of severe depression increased the likelihood of seeking mental healthcare, being a younger mother reduced this possibility. Also, this study has revealed that the cost of treatment, labor market factors, and marital status did not determine the decision to seek mental healthcare.
More studies are recommended to identify determinants of the choice of mental healthcare for sufferers of postpartum depression. This study can also be replicated in the post-COVID-19 era to identify the impact of the pandemic. Furthermore, a community-based study can be conducted using combined clinical diagnosis and self-administered questionnaires.
Non-cost strategies can be implemented to encourage mothers to seek mental healthcare, as the cost of treatment is not a deterring factor. Women attending antenatal clinics should be routinely screened for possible signs of PPD to encourage prompt demand for healthcare rather than till its severity becomes disabling. Mental healthcare should be made available and integrated into maternal healthcare services provided at all levels of provision. Screening of mothers for PPD should be done during routine immunization and postnatal visits. Increasing the availability of mental healthcare facilities in the country can promote higher patronage of formal mental healthcare services.
The introduction of the National Health Insurance Scheme (NHIS) at the National level, and its adoption in individual states of the country, Nigeria, is expected to make healthcare more affordable and accessible. In addition to this scheme, access to mental health services can be achieved by increasing the health budget and specifically the proportion of the budget allocated to mental health.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by University of Ibadan/University College Hospital Ethical Review Board (UI/UCH ERB) with Number NHREC/05/01/2008a in Ibadan, Oyo State, Nigeria. The patients/participants provided their written informed consent to participate in this study.
OOd prepared the research instruments, compiled the literature review, computed the theoretical framework, conducted the data collection, analysis, discussion, and interpretation of results. OOl prepared the introduction, formalized the research questions, conceptualized the study, and prepared the conclusion. SO contributed to the literature review, discussion sections, and provided technical support in the entire manuscript. All authors contributed to the preparation of the submitted version. All authors contributed to the article and approved the submitted version.
The authors acknowledge the financial support provided by the African Economic Research Consortium (AERC), Nairobi, Kenya, the African Health Economics and Policy Association (AfHEA), and the World Health Organization Africa Region Office (WHO-AFRO).
SO was employed by African Centre for Global Health and Social Transformation.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Olasehinde N. Healthcare seeking behaviour in Nigeria. J Popul Soc Stud. (2018) 26:207–18. doi: 10.25133/JPSSv26n3.015
2. Kolappa K, Henderson DC, Kishore SP. No physical health without mental health: Lessons unlearned? Editorials. Bull World Health Organ. (2013) 91:3–3A. doi: 10.2471/BLT.12.115063
3. Onyemelukwe C. Stigma and mental health in Nigeria: some suggestions for law reform. J Law Policy Glob. (2016) 55:63–68.
4. Abiodun OA. Postnatal depression in primary care populations in Nigeria. Gen Hosp Psychiatry. (2006) 28:133–6. doi: 10.1016/j.genhosppsych.2005.11.002
5. Adewuya AO, Eegunranti AB, Lawal AM. Prevalence of postnatal depression in Western Nigerian Women: a controlled study. Int J Psychiatry Clin Pract. (2005) 9:60–64. doi: 10.1080/13651500510018211
6. Agbaje OS, Anyanwu JI, Umoke PIC, Iwuagwu TE, Iweama CN, Ozoemena EL, et al. Depressive and anxiety symptoms associated factors among postnatal women in Enugu-North Senatorial District, South-East Nigeria: a cross-sectional study. Arch Pub Health. (2019) 77:1. doi: 10.1186/s13690-018-0329-6
7. Kakyo TA, Muliira JK, Mbalinda JK, Kizza IB, Muliira RS. Factors associated with depressive symptoms among postpartum mothers a rural district in Uganda. Midwifery. (2012) 28:374–9. doi: 10.1016/j.midw.2011.05.001
8. Chinawa JM, Odetunde OI, Ndu IK, Ezugwu EC, Aniwada EC, Chinawa AT, et al. Postpartum depression among mothers as seen in hospitals in Enugu, South-East Nigeria: an undocumented issue. Pan Afr Med J. (2016) 23:180–6. doi: 10.11604/pamj.2016.23.180.8244
9. Gureje O, Lasebikan VO, Ephraim-Oluwanuga O, Olley BO, Kola L. Community study of knowledge of and attitude to mental illness in Nigeria. Br J Psychiatry. (2005) 186:436–441. doi: 10.1192/bjp.186.5.436
10. Coates AO, Schaefer CA, Alexander JL. Detection of postpartum depression and anxiety in a large health plan. J Behav Health Serv Res. (2004) 31:117–33. doi: 10.1007/BF02287376
11. Hansotte E, Payne SI, Babich SM. Positive postpartum depression screening practices and subsequent mental health treatment for low-income women in Western countries: a systematic literature review. Public Health Rev. (2017) 38:1–17. doi: 10.1186/s40985-017-0050-y
12. Goyal S, Gupta B, Sharma E, Dalal PK, Pradeep Y. Psychiatric morbidity, cultural factors, and health-seeking behaviour in perinatal women: a cross-sectional study from a tertiary care centre of North India. Indian J Psychol Med. (2020) 42:52–60. doi: 10.4103/IJPSYM.IJPSYM_96_19
13. Gaynes BN, Gavin N, Meltzer-Brody S, Lohr KN, Swinson T, et al. Perinatal depression: prevalence, screening accuracy and screening outcomes. Evid Rep Technol Assess. (2005) 119:1–8. doi: 10.1037/e439372005-001
14. Bowen A, Bowen R, Butt P, Rahman K, Muhajarine N. Patterns of depression and treatment in pregnant and postpartum women. Can J Psychiatry. (2012) 57:161–7. doi: 10.1177/070674371205700305
15. Li H, Bowen A, Szafron M, Moraros J, Muhajarine N. Maternal mental health: a shared care approach. Prim Health Care Res Dev. (2016) 17:175–83. doi: 10.1017/S146342361500033X
16. Norhayati MN, Nik-Hazlina NH, Asrenee AR, Wan-Emilin WMA. Magnitude and risk factors for postpartum symptoms: a literature review. J Affect Disord. (2015) 175:34–52. doi: 10.1016/j.jad.2014.12.041
17. World Health Organization. Mental Health and Substance Use. Maternal mental health (2021). Available online at: https://www.who.int/teams/mental-health-and-substance-use/maternal-mental-health
18. Tungchama FP, Obindo JT, Armiya'u AY, Maigari YT, Davou FJ, Goar SG, et al. Prevalence and sociodemographic correlates of postpartum depression among women attending Postnatal and/or Children's Welfare Clinics in a Tertiary Hospital, Jos, Nigeria. Sahel Med J. (2018) 21:23–30. doi: 10.4103/smj.smj_39_16
19. Craigwell R, Bynoe D, Lowe S. The effectiveness of government expenditure on education and healthcare in the Caribbean. Int J Dev Issues. (2012) 11:4–18. doi: 10.1108/14468951211213831
20. World Health Organization (WHO-AIMS Report). Ministry of Health, WHO. WHO-AIMS Report on Mental Health System in Nigeria. Ibadan: Ministry of Health and WHO (2006).
21. Whitton A, Warner R, Appleby L. The pathway to care in post-natal depression: women's attitudes to post-natal depression and its treatment. Br J Gen Pract. (1996) 46:427–8.
22. Viinamäki H, Rastas S, Tukeva L, Kuha S, Niskanen L, et al. Postpartum mental health. J Psychosom Obstet Gynecol. (1994) 15:141–6. doi: 10.3109/01674829409025639
23. Hossain SJ, Roy BR, Hossain AT, Mehrin F, Tipu SMMU, Tofail F, et al. Prevalence of maternal postpartum depression, health-seeking behavior and out of pocket payment for physical illness and cost coping mechanism of the poor families in Bangladesh: a rural community-based study. Int J Environ Res Public Health. (2020) 13:4727. doi: 10.3390/ijerph17134727
24. Button S, Thornton A, Lee S, Shakespeare J, Ayers S. Seeking healthcare for perinatal psychological distress: a meta-synthesis of women's experiences. Br J Gen Pract. (2017) 67:e692–9. doi: 10.3399/bjgp17X692549
25. National Population Commission (NPopC) [Nigeria] and ICF International. Nigeria Demographic and Health Survey. Abuja: NDHS (2018).
26. Cronin C, Forsstrom M, Papageorge NW. Mental health, human capital and labor market outcomes. Hum Cap Labor Mark Outcomes. (2017). doi: 10.2139/ssrn.2896946
27. Jones A. Healthcare seeking in the perinatal period: a review of barriers and facilitators. Soc Work Public Health. (2019) 34:596–605. doi: 10.1080/19371918.2019.1635947
28. Muriithi MK. The determinants of health-seeking behaviour in a Nairobi Slum, Kenya. Eur Sci J. (2013) 9:151–64
29. Olasehinde N, Olaniyan O. Determinants of household health expenditure in Nigeria. Int J Soc Econ. (2017) 44:1694–709. doi: 10.1108/IJSE-12-2015-0324
30. Awoyemi T, Obayelu O, Opaluwa H. Effect of distance on utilization of health care services in rural Kogi State, Nigeria. J Hum Ecol. (2011) 35:1–9. doi: 10.1080/09709274.2011.11906385
31. Musah K, Kayode O. Preliminary assessment of healthcare seeking behaviour among users of primary healthcare facilities in Ilorin Metropolis, Kwara State, Nigeria. IOSR J Nurs Health Sci. (2014) 3:31–5. doi: 10.9790/1959-03413135
32. Odaman O, Ibiezugbe M. Health seeking behavior among the elderly in Edo Central Nigeria. Int Rev Soc Sci Hum. (2014) 7:201–10.
33. Yip WC, Wang H, Liu Y. Determinants of patient choice of medical provider: a case study in rural China. Health Policy Plan. (1998) 13:311–22. doi: 10.1093/heapol/13.3.311
34. Gotsadze G, Bennett S, Ranson K, Gzirishvili D. Healthcare-seeking behaviour and out-of-pocket payments in Tbilisi, Georgia. Health Policy Plan. (2005) 20:232–42. doi: 10.1093/heapol/czi029
35. Pearlstein T, Howard M, Salisbury A, Zlotnick C. Postpartum depression. Am J Obstet Gynecol. (2009) 200:357–69. doi: 10.1016/j.ajog.2008.11.033
36. Smith MS, Lawrence V, Sadler E, Easter A. Barriers to accessing mental health services for women with perinatal mental illness: systematic review meta-synthesis of qualitative studies in the UK. BMJ Open. (2019) 9:e024803. doi: 10.1136/bmjopen-2018-024803
37. Liu L, Xiao-li C, Chun-ping N, Ping Y, Yue-qin H, Liu ZR, et al. Survey on the use of mental health services and healthcare-seeking behaviors in a community population in Northwestern China. Psychiatry Res. (2018) 262:135–40. doi: 10.1016/j.psychres.2018.02.010
38. Bruffaerts R, Posada-Villa J, Al-Hamzawi AO, Gureje O, Huang Y, Hu C, et al. Proportion of patients without mental disorders being treated in mental health services worldwide. Br J Psychiatry. (2015) 206:101–9. doi: 10.1192/bjp.bp.113.141424
39. Cox JL, Holden JM, Sagovsky R. Development of the 10-item Edinburgh Postnatal Depression Scale. Br J Psychiatry. (1987) 15:782–6. doi: 10.1192/bjp.150.6.782
40. Owoeye AO, Aina OF, Morakinyo O. Risk factors of postpartum depression and EPDS scores in a group of Nigerian women. Trop Doct. (2006) 36:100–3. doi: 10.1258/004947506776593341
41. Abdollahi F, Lye MS, Zarghami M. Perspective of postpartum depression theories: a narrative literature review. N Am J Med Sci. (2016) 8:232. doi: 10.4103/1947-2714.185027
42. Vaezi A, Soojoodi F, Banihashemi AT, Nojomi M. The association between social support and postpartum depression in women: a cross sectional study. Women Birth. (2018) 32:e238–42. doi: 10.1016/j.wombi.2018.07.014
43. Palumbo G, Mirabella F, Gigantesco A. Positive screening and risk factors for postpartum depression. Eur Psychiatry. (2017) 42:77–85. doi: 10.1016/j.eurpsy.2016.11.009
44. Levis B, Negeri Z, Sun Y, Benedetti A, Thombs BD, Depression Screening Data (DEPRESSD) EPDS Group. Accuracy of the Edinburgh Postnatal Depression Scale (EPDS) for screening to detect major depression among pregnant and postpartum women: systematic review and meta-analysis of individual participant data. BMJ. (2020) 371:m4022. doi: 10.1136/bmj.m4022
47. Andrade LH, Alonso J, Mneimneh Z, Wells JE, Al-Hamzawi A, Borges G, et al. Barriers to mental health treatment: results from the WHO World Mental Health surveys. Psychol Med. (2013) 44:1303–17. doi: 10.1017/S0033291713001943
48. Kessler R, Aguilar-Gaxiola S, Alonso J, Chatterji S, Lee S, et al. The global burden of mental disorder: an update from the WHO World Mental Health (WMH) Survey. Epidemiol Psichiatr Soc. (2009) 18:23–33. doi: 10.1017/S1121189X00001421
49. Tegegne A, Legese M. The urban poor and healthseeking behaviour: the healthcare seeking behaviour of the ‘poorest of the poor' in Addis Ababa, Ethiopia. Glob J Hum Soc Sci. (2014) 14.
50. Grissette BG, Spratling R, Aycock DM. Barriers to healthcare-seeking behaviour among women with postpartum depression. JOGNN. (2018). doi: 10.1016/j.jogn.2018.09.006
51. Bina R. Seeking Healthcare for Postpartum Depression: the Behavioural Model of Health Service Use as a Framework for Predicting Treatment Utilization for Postpartum Depression. UMB Digital Archive downloaded 05.03.2019. (2011).
52. Hjortserg C. Why do the sick not utilize healthcare? The case of Zamia. Health Econ. (2003) 12:55–50. doi: 10.1002/hec.839
53. Jameson JP, Blank MB. Diagnosis and treatment of depression and anxiety in rural and non-rural primary care: national survey results. Psychiatric Serv. (2010) 61:624–7. doi: 10.1176/ps.2010.61.6.624
55. Small R, Brown S, Lumley J, Astbury J. Missing voices: what women say and do about depression after childbirth. J Reprod Infant Psychol. (1994) 12:89–103. doi: 10.1080/02646839408408872
Keywords: Edinburgh postnatal depression scale, maternal mental health, women, healthcare-seeking behaviors, postpartum depression (PPD)
Citation: Odufuwa OT, Olaniyan O and Okuonzi SA (2022) Determinants of Mental Healthcare-Seeking Behavior of Postpartum Women in Ibadan, Nigeria. Front. Glob. Womens Health 3:787263. doi: 10.3389/fgwh.2022.787263
Received: 30 September 2021; Accepted: 12 May 2022;
Published: 29 June 2022.
Edited by:
Caroline Gurvich, Monash University, AustraliaReviewed by:
Sandra Nakić Radoš, Catholic University of Croatia, CroatiaCopyright © 2022 Odufuwa, Olaniyan and Okuonzi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Oyeteju T. Odufuwa, toluwaniteju04@yahoo.com
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.