 Thérèse Delvaux
Thérèse Delvaux Vicky Jespers
Vicky Jespers Lenka Benova1
Lenka Benova1- 1Institute of Tropical Medicine, Antwerp, Belgium
- 2Belgian Health Care Knowledge Centre, Brussels, Belgium
- 3Julius Center for Health Sciences and Primary Care, University Medical Center Utrecht, Utrecht University, Utrecht, Netherlands
Introduction: Acceptability of and satisfaction with contraceptive methods are paramount for uptake and continuation. In the current context of multipurpose prevention of pregnancy and sexually transmitted diseases/HIV development, it is critical to have a better understanding of acceptability of and satisfaction with the contraceptive vaginal ring (CVR) including sexual satisfaction. The objective of this study was to review the evidence about acceptability of CVRs and general and sexual satisfaction of users.
Methods: We searched PubMed, CINAHL, and Web of Science (until December 31, 2020) and selected original studies documenting actual use of hormonal CVR and explicitly addressing any of the 3 outcomes.
Results: Of a total of 1,129 records screened, 46 studies were included. Most studies (n = 43, 93%) were prospective, conducted in high-income settings (n = 35), and reported on NuvaRing® use (n = 31). Overall, 27 (59%) studies included a comparison group, 38 (82%) studies used exclusively quantitative questionnaires, with qualitative only (n = 4, 9%), or mixed methods (n = 4, 9%) studies being less common. Ease of CVR insertion/removal/reinsertion was high in all the settings and improved with time of use, with qualitative studies supporting these findings. When mentioned, ring-related events were associated with discontinuation, and results on continuation of use were mixed. Among NuvaRing® studies, general satisfaction (being satisfied or very satisfied) was between 80 and 90% and tended to mirror continuation. Sexual satisfaction was less commonly reported and results were mixed. Overall, limited information was provided on actual CVR experiences of women (and men) and cultural norms that may affect sexuality and CVR use.
Conclusion: Positive aspects of acceptability of and satisfaction with CVRs were reported, but ring-related events and factors, which may affect long-term CVR use, deserve further study. More information is needed on actual experiences of women using CVRs, relationship aspects, male partner opinions, and contextual norms to better understand the acceptability of and satisfaction with CVRs.
Introduction
Contraceptive vaginal rings (CVRs) have been developed since 1970 and 3 CVRs are currently available: the etonogestrel and ethinyl estradiol ring (marketed as NuvaRing®), the progesterone ring for breastfeeding women (Progering®), and the recently approved segesterone acetate (previously called Nestorone) and ethinyl estradiol ring (Annovera™) (1, 2). Advantages of CVRs are multiple: they are user-initiated and controlled, independent of sexual acts, and can provide long-term effective protection (1). Moreover, vaginal rings could be designed to include several active ingredients that provide prevention for HIV, other sexually transmitted infections (STIs), and pregnancy (3).
Acceptability of and satisfaction with contraceptive methods impact uptake, adherence, and continuation and, therefore, contribute significantly to contraceptive effectiveness (4). In clinical studies, acceptability of contraceptive methods is often documented through the effect of the product on bleeding patterns/cycle control, its side effects, and the duration of use. Satisfaction tends to reflect the perceptions of the product of user and is assessed quantitatively through levels of satisfaction during actual use and/or indirectly assessed through willingness to use in the future or recommend the method (1). Both the concept of acceptability and satisfaction are in fact intertwined as illustrated by validated quantitative tools in which overall satisfaction is considered a dimension of acceptability (5, 6). Moreover, given vaginal administration, CVRs may affect sexual relationships. To this end, sexual satisfaction with CVR has been studied more specifically using sexual function assessment tools such as the Female Sexual Function Index (7). In reality, acceptability and satisfaction are complex concepts that are influenced by physical, behavioral, physiological, interpersonal, and structural factors. Recent studies documenting the effectiveness of vaginal products and devices in the field of HIV prevention have confirmed the key contribution of acceptability to adherence and theoretical frameworks presenting pathways from various acceptability dimensions toward satisfaction and then to adherence have been developed to aid further inquiry (8).
Given the current focus and importance of multipurpose technology for prevention of pregnancy and STIs/HIV, it is critical to have a better understanding of what is commonly considered as acceptability and satisfaction of CVR and main reported results with respect to these outcomes including sexual satisfaction. The objectives of this study were to review the overall evidence of acceptability of CVRs and general and sexual satisfaction of users.
Materials and Methods
Protocol and Registration
This study protocol was registered on the international prospective register of systematic reviews (PROSPERO) (CRD42017079157).
Literature Search
Databases searched were PubMed, cumulative index to nursing and allied health literature (CINAHL), and Web of Science with a cutoff date of December 31, 2020. The main search terms were “contraceptive vaginal ring” and “acceptability” or “satisfaction” or “sexual satisfaction” and synonyms of each of these terms were also included. Additional search terms included “qualitative methods,” “mixed methods,” and “trials.” The search strategies were adjusted according to the specifications of each database. Additional relevant publications from other sources (reference lists) were also included (Supplementary Material S1_Search strategy). The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) framework guidelines, flow diagram, and checklist were utilized to undertake this study.
Selection Criteria
Studies were eligible if they included actual CVR use by healthy women of reproductive age (15–49 years) and explicitly addressed acceptability, satisfaction, and/or sexual satisfaction. We did not use specific definitions of acceptability and satisfaction because we wanted to learn which definitions or concepts the various authors had used. Similarly, we did not select studies based on study methods used, but excluded reviews and opinion papers or commentaries, validation studies, studies that evaluated non-contraceptive vaginal ring use (such as rings for hormonal replacement therapy), or assessed acceptability or willingness to use hypothetically in the absence of actual user experiences. Studies that only enrolled women with a specific health condition (such as diabetes) and full texts in languages other than English, French, Dutch, Spanish, or Italian were also excluded (n = 3). In case of multiple articles presenting data from the same study with the same outcomes of interest, only the primary paper was included in this study (Excluded studies in Supplementary Material S2).
Study Selection
Each title and abstract were screened by two independent reviewers (TD and VJ) using the inclusion criteria described above. Full texts of all the papers selected in title and abstract screening were checked by both the reviewers before inclusion and any discrepancies were discussed until consensus was reached.
Study Quality Assessment and Data Synthesis
A standardized pretested form was used by TD to extract data from full texts on study characteristics: author names, year of publication, journal, study setting, study design, ring use and comparison group(s) (if any), research methods used and main findings related to acceptability, overall satisfaction and sexual satisfaction. Data on sample size, randomization process, and presence of a control group related to methodological quality assessment were also extracted, but were not considered a core component of this study, as we wanted to provide an overview of methods used to document acceptability and satisfaction.
Patient and Public Involvement
No patient or public involvement took place in the design or conduct of this systematic review, which included 46 papers from many countries worldwide.
Results
Of 1,308 publications that were identified through database searching, after removal of duplicates, 1,129 titles/abstracts and 96 full texts were reviewed and 46 articles (primary studies) were included (Figure 1).
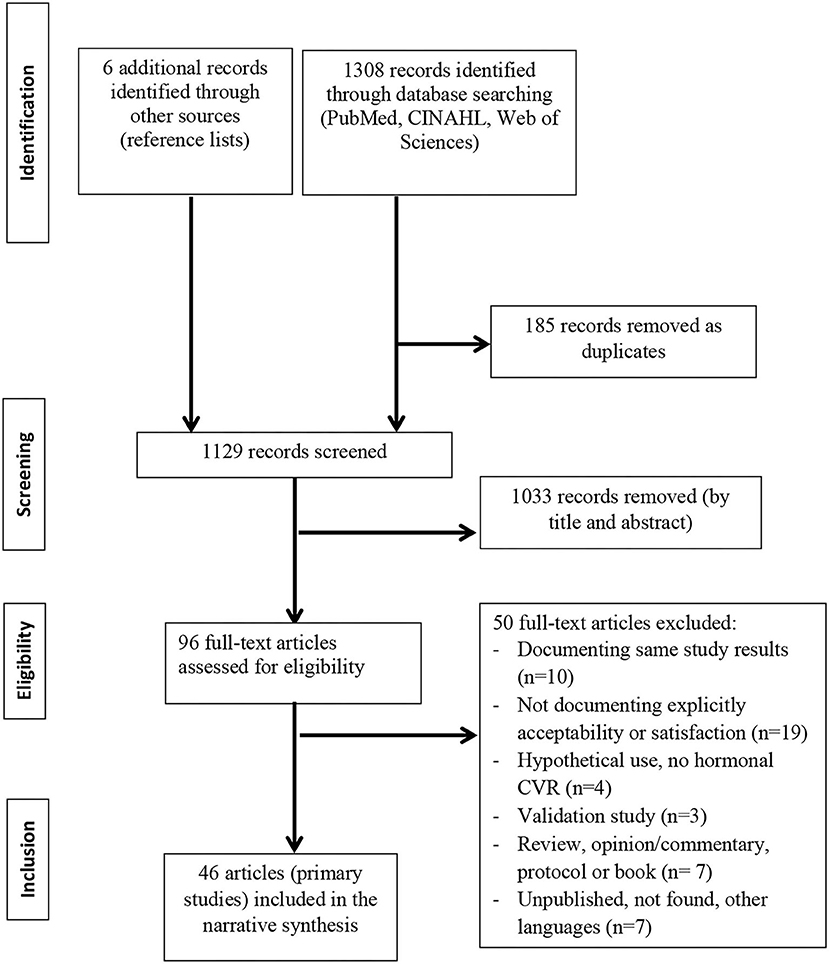
Figure 1. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart of the studies selection process for the review on contraceptive vaginal rings, acceptability, and general and sexual satisfaction.
Studies Design, Methods, Characteristics, and Settings
A total of 19 studies (41%) were randomized clinical trials (9–27), 24 studies were prospective non-randomized studies (28–51), and 3 studies were cross-sectional studies (52–54) (Table 1). A total of 27 studies (59%) used a controlled design, comparing CVR users to users of other hormonal methods [such as a combined oral contraceptive (COC) pill or patch] or to non-hormonal contraceptive methods (such as the copper intrauterine device) or comparing users of CVRs containing different hormonal dosages or the same CVR for different durations. The remaining 19 studies did not include a comparison group (Table 1).
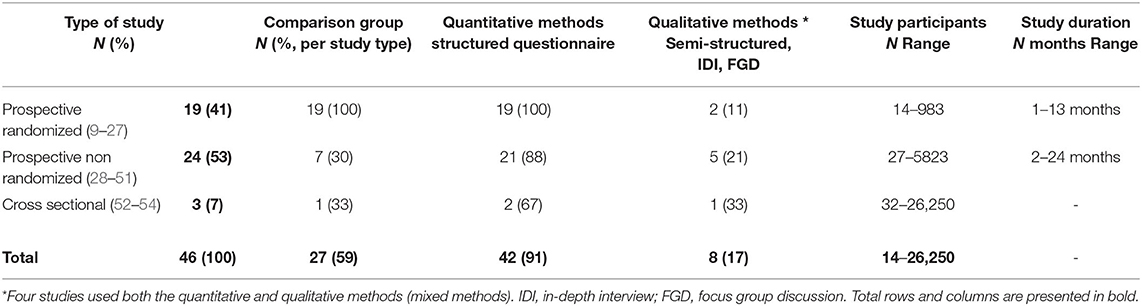
Table 1. Types of study design, methods, participants, and study duration.
Most studies (42/46, 91%) used quantitative structured questionnaires and 8 (17%) studies used qualitative semi-structured or in-depth interviews (IDIs) and/or focus group discussions (FGDs) (Table 1). Overall, 38 (82%) studies used exclusively quantitative structured questionnaires (25, 26, 30, 36, 41, 44, 49, 52), while 4 (9%) studies used only qualitative methods and 4 (9%) studies used both the quantitative and qualitative methods (25, 26, 36, 49). The number of participants in the prospective studies ranged from 14 to 5,823, with an average 50 to 200 participants. In total, 1 cross-sectional study was larger with up to 26,250 participants. The duration of use in the prospective studies ranged from 1 to 24 menstrual cycles, with about a third (n = 13) covering 12 cycles or more, another third (n = 13) covering 6 to 12 menstrual cycles, and the remaining studies covering 3 menstrual cycles or fewer (Table 1).
Studies were performed in 1 or more high-income settings, i.e., countries of Europe, USA, Canada, or Australia (n = 35/46 studies, 76%); Latin America (n = 5); Israel (n = 2); Asia (n = 5, of which 3 were in India); and Africa [n = 5, including 1 study each in Rwanda, Kenya, South Africa, and 2 studies in several (mostly sub-Saharan) African countries] (Table 2).
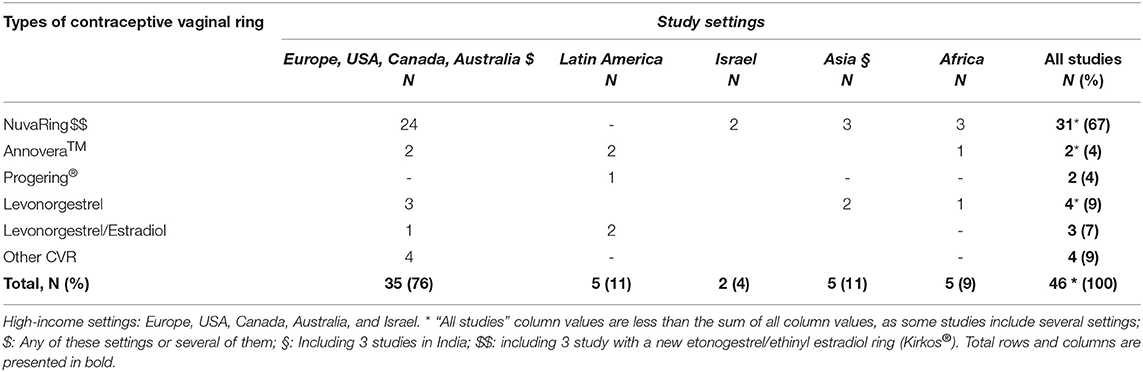
Table 2. Study settings and types of contraceptive vaginal rings.
NuvaRing® was the most studied CVR (31/46 studies, including 1 recent study testing a new etonogestrel/ethinyl estradiol—Kirkos®—against NuvaRing®), while 2 studies evaluated use of the Annovera™ ring and 2 other studies evaluated use of the Progering® among breastfeeding women. The remaining 11 studies investigated CVRs containing levonorgestrel (LNG) alone, combined with ethinyl estradiol or other progesterone regimens. These CVRs were not further developed and did not make it to the market (Table 2).
Main Findings on Acceptability, Satisfaction, and Sexual Satisfaction
Overall definitions of acceptability and satisfaction or how these outcomes were described, varied across studies, over time and according to the type of CVR. Therefore, we will present main results on these outcomes by type of CVR.
NuvaRing®
Studies documenting acceptability and/ or satisfaction of NuvaRing® commonly used structured questionnaires assessing the following similar dimensions: clarity of instructions; ease of use (including to insert/remove the ring); ease of package use; compliance or adherence (including removals and spontaneous expulsions); cycle-related characteristics (menstrual changes or pain); sexual comfort (whether the ring was felt by the woman or the male partner or whether the partner objected to the ring, without investigating sexual frequency, pleasure, or satisfaction); and overall satisfaction. These seven dimensions were included in a validated 21-item questionnaire by Novak et al. (5) and subsequently used in other studies (21, 31–33, 37, 38, 48). The IUD intra uterine device (ORTHO-BC-SAT) satisfaction questionnaire related to the use of hormonal contraception in general and including 8 dimensions similar to Novack et al. questionnaire that was used in 1 CVR study (19). Over 80% of NuvaRing® users in all the studies using the seven/eight dimensions showed that CVR instructions and packaging were clear and that the ring was easy to insert and remove (Table 3). In Kenya, a qualitative study showed that unease with vaginal insertion and ring placement issues (slippage and expulsion) created initial challenges requiring clinician assistance and practice for some participants (30). Similarly, an in-depth discussion with users in Rwanda showed that initial worries with respect to CVR insertion reduced over time with actual ring use and ring insertions and removals were, henceforth, described as easy (26). On the other hand, 2 studies reported that the previous use of tampons did not seem to influence satisfaction or successful ring use of CVR (14, 52). A number of studies reported spontaneous expulsions rates ranging from less than 2% (15, 17) to 5–20% (21, 36, 46, 51). A study in Switzerland showed that 17.5% of adverse events were ring related such as feeling the ring, vaginal discomfort, and vaginal expulsions (31). In a study in the Netherlands (38), women who felt the ring were more likely to remove it (sometimes, regularly, and always) during intercourse compared to those who did not feel it (22 vs. 6%) (Table 3). An in-depth study among adolescents in the US using NuvaRing® revealed that 5 of 32 participants discontinued because of ring-related events (52). In Kenya, minor side effects were described and concerns centered on ring efficacy, negative effect on a sexual desire of woman, future fertility issues, and non-suppression of menstruation, which were favored by most participants (30).
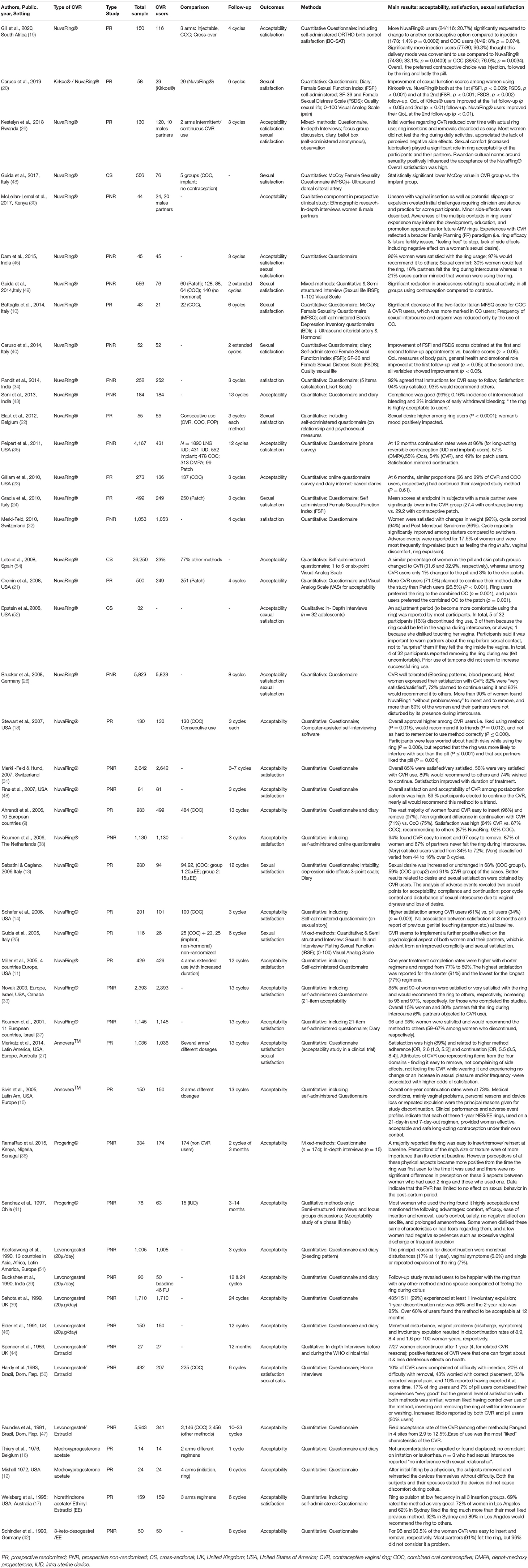
Table 3. Study characteristics, type of CVR and study, participants, comparison group, outcome(s), methods used, and main results, presented by type of CVR then chronologically.
Overall satisfaction with NuvaRing®, measured on the 4–6-point Likert scale or using a dichotomous variable (Yes/No), ranged between 80 and 90%, with studies without a comparison group (other contraceptive method) more tending to report the highest satisfaction rates (Table 3). However, a high level of satisfaction (“being very satisfied”) varied across studies and ranged between 30 and 94% (the highest proportion reported in a study conducted in India) (14, 32, 34, 38). In Rwanda, general satisfaction with NuvaRing® was high (over 80%) and concurred with qualitative findings and a ballot box (anonymous) survey at the end of the trial (26). In South Africa, more injection users (96.3%) significantly thought that this delivery mode was convenient to use compared to NuvaRing® (83.1%; p = 0.0409) or COC (76.0%; p = 0.0034). Overall, the preferred contraceptive choice was injection, followed by the ring and lastly the pill (19). Willingness to recommend NuvaRing® to others ranged from 60 to over 90% in the studies documenting satisfaction. NuvaRing® can be used for 3 weeks, then removed for 1 week before reinsertion, or used for an extended period (or continuous use). In total, 3 studies documenting extended use of NuvaRing® showed fair satisfaction/sexual satisfaction rates (11, 40, 49); although, in 1 study, satisfaction rates tended to be higher among women using shorter regimens (11). In a randomized study controlling for intermittent vs. continuous NuvaRing® use in Rwanda, most women in both the groups reported similar acceptability and satisfaction and appreciated the absence of negative side effects (26).
A number of studies reported “sexual comfort” as whether NuvaRing® was felt by partners (up to 30%), whether a number of partners found it bothersome or did mind (5–20%) (28, 31, 37, 45), objected its use (6%) (33), or did prefer the pill (5–30%) instead of CVR (18). A multicenter NuvaRing® study in high-income settings pointed out that sexual comfort for the women who prematurely discontinued participation in the studies was only marginally lower than for those who completed them (33).
Sexual satisfaction while using NuvaRing® was reported in a total in 16 studies, exclusively (n = 9) or with acceptability and general satisfaction (n = 7). Through the use of female sexual function indexes, scales, or diaries, these studies showed mixed sexual satisfaction results with NuvaRing® use. In total, 2 studies (one without comparison group, another 1 comparing a new CVR Kirkos® to NuvaRing®) conducted in Italy reported an improvement of all the variables between baseline and follow-up (40). In total, 2 prospective controlled studies conducted by Guida et al. in Italy reported improved overall and sexual relationship (“complicity”) among couples (27) and reduced anxiousness compared to COC users (55). Increased sexual desire (compared to COC or progestin-only pill) was reported among NuvaRing® users in a small study in Belgium (22) and increased or unchanged sexual desire in another study comparing NuvaRing® to low estrogen dose COC (13). In Rwanda, most women reported that ring use stimulated conversations with their partners about increased lubrication and sexual desire, but also about family planning and more general relationship topics. Most women (81%) reported at least once during ring use that the ring made sex feel better and this increased to 87% at the last study visit. Qualitative data confirmed this finding “this ring should be promoted as a sex enhancer” (26). The authors highlighted that Rwandan cultural norms around sexuality positively influenced the acceptance of the NuvaRing®. On the other hand, a randomized trial found that the McCoy Female Sexuality Questionnaire decreased significantly over treatment among COC and CVR users (10). A recent cross-sectional study reported significantly lower median values of female sexuality indexes in the CVR group compared to implant (53). In total, 2 studies found significantly decreased libido (3.3 vs. 0.8%) or mean female sexual function indexes with the ring compared to COC or patch users, respectively (21, 31).
Results with respect to continuation rates reported in our acceptability/satisfaction studies were mixed. Some NuvaRing® studies showed a higher willingness to continue the use of the method (71% for CVR vs. 26.5% for skin patch users) (21) or a higher continuation rate (1% CVR users changed to pill or patch vs. 32–33% COC and skin patch users who changed to CVR) (21, 54). Other studies showed similar (high or low) continuation rates compared to COC [71 CVR vs. 75% COC (9, 23); 26 CVR vs. 29% COC (10)]. In total, 12 months continuation rates were lower (54%) for CVR users compared to 86% among long-acting reversible contraception [intra uterine device (IUD) and implant], 57% for depot-medroxyprogesterone acetate (DMPA), and 55% for COC, but higher than for skin patch users (49%) in a study conducted in the US. A recent study conducted among adolescents in South Africa showed that more NuvaRing® users (24/116; 21%) significantly requested to change to another contraceptive option compared to injection (1/73; 1.4% p = 0.0002) and COC users (4/49; 8% p = 0.074) (19). Finally, 1 year treatment completion rates were higher (77%) with the shorter NuvaRing® treatment regimens compared to 1-year extended regimen use (59%) (11).
Finally, opinions of male partner about NuvaRing® were usually indirectly assessed by asking women about perception of the CVR of their partners (dimension and sexual comfort). Only 2 studies interviewed (qualitatively) the male partners themselves on perceptions and experiences with the ring (26, 30): In Kenya, experiences with CVR reflected a broader family planning (FP) paradigm: FP intentions and disclosure practices were influenced by partner support, socioeconomic factors, religion, cultural beliefs, and societal norms, including female sexuality (30). In Rwanda, finding from a limited number of interviews of male partners was in line with high acceptability and satisfaction reported by women (26).
Annovera™ and Progering®
Acceptability of Annovera™ was reported as high in 2 studies. Similar acceptability dimensions than in NuvaRing® studies were used in an Annovera™ trial in Europe, USA, and Latin America and included in a theoretical framework presenting a pathway from acceptability to satisfaction then further to adherence and continuation (27). In the same study, satisfaction with Annovera™ was rated high (89%) and was associated to adherence and continuation (p < 0.001). Not feeling the ring while wearing it and experiencing no change or an increase in sexual pleasure and/or frequency was associated with higher odds of satisfaction (Table 3) (27). An earlier study showed an overall 1-year continuation rates at 73%. Medical conditions, mainly vaginal problems, personal reasons, and device loss or repeated expulsion, were the principal reasons given for study discontinuation (15).
Acceptability of the progesterone vaginal ring was rated high including ease to insert/remove/reinsert in African and Latin American settings and perceptions positively improved between the time the ring was first seen and the time it was used (36, 41) (Table 3). Perceptions of the size or texture of ring were reported of more importance than its color at baseline in African settings (36). In Latin America, 5–30% of women reported negative experiences (vaginal symptoms—excessive discharge or expulsion) (41), while in African settings expulsion reported rate was 5%. The study in sub-Saharan Africa included “family support” as an additional dimension of acceptability (36) and reported using a theoretical framework including other stakeholders such as healthcare providers, program managers, and policymakers, although the framework was not presented. In this study, data indicated that the CVR had limited to no effect on sexual behavior in the postpartum period (36).
Other Types of CVRs
Earlier studies on other types of CVRs reported on acceptability often referring to clinical features and tolerability. Vaginal symptoms, expulsions, and menstrual disturbances led to discontinuation among LNG 20 μg ring users (46, 51). Similarly, results from a qualitative study with the same ring conducted in the UK (parallel to the WHO randomized trial) showed that overall 7 of 27 women discontinued after a year and 4 of them for ring-related reasons (44). In a study conducted in the early 80s in Latin America with a LNG/estradiol ring, 43% of women reported being worried about correct ring placement/insertion (50) (Table 3).
Discussion
Many studies using mostly quantitative structured questionnaires have documented acceptability and satisfaction of hormonal CVR, particularly NuvaRing®. The majority of these studies were conducted in high- or middle-income settings. Overall, CVR studies show that easiness to insert/remove/reinsert CVRs was high. Continuation rates, when reported, showed mixed results. Among NuvaRing® studies, general satisfaction (being satisfied or very satisfied) was between 80 and 90%, although limited information was provided on actual experiences of women while using CVR; relationship attributes (such as couple communication and decision to use CVR); and contextual elements such as community perceptions of contraception and the CVR, gender/sexual norms, and experience.
Ease of insertion/removal/reinsertion of CVRs was reported in most included studies and rated high including in Latin American or African settings. Among the included studies, qualitative data on actual experiences of women while using the ring showed that initial worries related to CVR itself or its use, such as aspect, insertion, removal, and feeling the ring inside the vagina, improved over time (26, 30, 52), as it is also reported in 1 qualitative systematic review of CVR and 1 systematic review of vaginal rings (55, 56). Initial concerns sometimes required additional support from the provider or practice from the user (30, 55) or benefited of an adjustment period as reported among adolescents and younger users in the US (52). In addition, 2 other CVR studies have shown that “ease of use” was a major reason reported by participants for either selecting or using CVR in Spain (57, 58).
Perception of the ring of user was sparsely documented and data on ring expulsions were limited in the identified studies. However, when documented, ring-related reasons (slippage, expulsion, vaginal problems, or discomfort) contributed for a proportion of women to discontinuation of all the types of CVRs and confirmed findings from previous studies (55, 59). Expulsions and mechanical properties of the ring were included as a specific dimension in acceptability theoretical frameworks that were used in 2 included studies (26, 27) and in vaginal ring HIV prevention studies (8) and deserve to be further addressed in future studies.
Among NuvaRing® studies, general satisfaction (being satisfied or very satisfied) was reported between 80 and 90%. However, as highlighted in our results, a comparison group (i.e., including the use of another contraceptive method or another regimen) was not present in about 40% of studies. Data triangulation between quantitative and qualitative data contributed to confirm or provide more information on satisfaction and factors, such as increased lubrication, leading to satisfaction and adherence (26, 36, 55).
Standard clinical trials in the field of CVRs mostly used structured questionnaires to assess acceptability, satisfaction, and/or sexual satisfaction. Mixed methods approaches combining quantitative and qualitative data collection were less commonly encountered. Clinical trial teams may be less familiar or reluctant to use qualitative approaches because this requires additional resources, time, and expertise over-and-above those required to carry out a clinical trial. Furthermore, qualitative study designs often use a purposive sampling strategy enrolling small numbers of participants, which is different from clinical trial designs based on representative sampling and statistical power calculations. Unlike CVR studies, HIV prevention vaginal rings studies often used mixed and qualitative methods and have documented acceptability of vaginal rings in low-income (high HIV prevalence) settings. These studies (8, 60) have highlighted the importance of using or incorporating qualitative study into clinical trial designs and the contribution of theoretical frameworks to better understand acceptability and satisfaction, as also shown in several studies of this study (25–27, 30, 36, 41, 44, 49, 52).
“Sexual comfort” usually referred to whether the ring was (reported) as felt either by women or partners during sexual intercourse or if the male partner “minded” the ring or its physical effects during intercourse (33). This issue raised concerns among less than a third of women in all the contexts studied. The regular set of acceptability dimensions used and information collected in NuvaRing® acceptability studies did not include measures of frequency of sexual encounters or sexual satisfaction. Sexual satisfaction investigated most of the time in separate studies using female sexuality indexes or other similar measures that showed mixed results. According to a study by Sabatini and Cagliano, they pointed out that the analysis of adverse events revealed that disturbance of sexual intercourse was a crucial point for acceptability, compliance, and continuation (13). This is in line with other studies documenting the relationship between contraception and sexuality (61). Some authors believe that sexual side effects are the best predictors of discontinuation of oral contraceptives among heterosexual adult women (62). Actually, contraceptives can affect sexuality of women in a wide variety of ways beyond sexual functioning alone, for example, they can affect communication between sexual partners and empowerment of women (63). Interestingly, as qualitative data showed in Rwanda, enhanced communication of couples (for instance because of CVR use and potential increased lubrication) contributed to the acceptability of the NuvaRing®. The use of female sexual function indexes and aspects related to sexual relationship may help to improve our understanding of the relationships between contraception and sexuality including for CVRs.
When reported as it was not the focus of this study, willingness to continue CVR use or continuation rates showed mixed results compared to contraceptive pill users and skin patch. Some evidence suggests that long-acting contraceptives (implants or IUD) have higher continuation rates compared to short-acting contraceptives such as COC, but also CVR and skin patch. In South Africa, injectables showed the highest continuation rates and satisfaction.
Overall, limited information was provided on actual experiences of women using CVR and cultural context, which may affect CVR use (55). Further documenting actual experiences of women using the CVR and male partner opinions (including with respect to relationship and sexuality) can contribute to a better understanding of acceptability of and satisfaction with CVR (55). Awareness of the multiple contexts in experience of ring users and giving a strong voice to women with respect to their perception of contraceptive methods may inform the development and promotion approaches for CVR and more broadly vaginal rings (30, 64, 65).
This study has several limitations. First, given the lack of standardized definitions of acceptability and satisfaction, we may have missed articles documenting CVR acceptability or satisfaction that were not explicitly using this terminology and instead referred to continuation or adherence, which was not a specific outcome of interest in this study. Second, we could not always deduct from the methods sections of included studies whether interviews included open-ended questions. This may have led to under-recording of the use of semi-structured interviews. However in-depth qualitative techniques, such as IDIs or FGDs, were always clearly described in studies.
Conclusion
Many studies using mostly quantitative structured questionnaires have documented acceptability and satisfaction of hormonal CVRs, particularly NuvaRing®. Despite the use of similar dimensions in a number of studies, there was a lack of standardized definitions of acceptability and satisfaction. Sexual satisfaction or pleasure was not typically included in acceptability dimensions and findings were not very informative in terms of actual experiences of women using CVRs and the cultural context that may affect sexuality and contribute to shape acceptability of CVRs. The use of mixed methods or qualitative approaches, including information on experiences of women using CVRs, relationship aspects, male partner opinions, and contextual sexual norms may lead to a better understanding of acceptability and satisfaction of CVRs. In addition, the use of theoretical acceptability frameworks highlighting the actual pathway from acceptability to satisfaction and adherence might also be useful.
Author Contributions
TD, VJ, LB, and JW conceived and designed the study and wrote manuscript. TD, VJ, and LB conducted data-based searches. TD and VJ conducted data screening, selected the studies, performed data analysis, and presentation of results. TD conducted data extraction. All the authors provided input in manuscript writing and approved the final manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fgwh.2021.799963/full#supplementary-material
References
1. Brache V, Faundes A. Contraceptive vaginal rings: a review. Contraception. (2010) 82:418–27. doi: 10.1016/j.contraception.2010.04.012
2. Monteiro I, Guazzelli C BL. Advances in contraceptive vaginal rings: what does the future hold? Expert Opin Pharmacother. (2018) 19:1685–91. doi: 10.1080/14656566.2018.1519549
3. World Health Organisation: WHO recommends the dapivirine vaginal ring as a new choice for HIV prevention for women at substantial risk of HIV infection [Internet]. Available online at: https://www.who.int/news/item/26-01-2021-who-recommends-the-dapivirine-vaginal-ring-as-a-new-choice-for-hiv-prevention-for-women-at-substantial-risk-of-hiv-infection. (accessed Nov 8, 2021)
4. Trussell J. Contraceptive failure in the United States. Contraception. (2011) 83:397–404. doi: 10.1016/j.contraception.2011.01.021
5. Novak A, de la Loge C, Abetz L. Development and validation of an acceptability and satisfaction questionnaire for a contraceptive vaginal ring, NuvaRing. Pharmacoeconomics. (2004) 22:245–56. doi: 10.2165/00019053-200422040-00003
6. Colwell HH, Mathias SD, Cimms TA, Rothman M, Friedman AJ, Patrick DL. The ORTHO BC-SAT–a satisfaction questionnaire for women using hormonal contraceptives. QualLife Res. (2006) 15:1621–31. doi: 10.1007/s11136-006-0026-8
7. Rosen R, Brown C, Heiman J, Leiblum S, Meston C, Shabsigh R, et al. The female sexual function index (FSFI): a multidimensional self-report instrument for the assessment of female sexual function. J Sex Marital Ther. (2011) 26:191–208. doi: 10.1080/009262300278597
8. Van Der Straten A, Montgomery ET, Cheng H, Wegner L, Masenga G, Von Mollendorf C, et al. High acceptability of a vaginal ring intended as a microbicide delivery method for HIV prevention in African women. AIDS Behav. (2012) 16:1775–86. doi: 10.1007/s10461-012-0215-0
9. Ahrendt H-JJ, Nisand I, Bastianelli C, Gomez MA, Gemzell-Danielsson K, Urdl W, et al. Efficacy, acceptability and tolerability of the combined contraceptive ring, NuvaRing, compared with an oral contraceptive containing 30 micrograms of ethinyl estradiol and 3 micrograms of drospirenone. Contraception. (2006) 74:451–7. doi: 10.1016/j.contraception.2006.07.004
10. Battaglia C, Morotti E, Persico N, Battaglia B, Busacchi P, Casadio P, et al. Clitoral vascularization and sexual behavior in young patients treated with drospirenone-ethinyl estradiol or contraceptive vaginal ring: a prospective, randomized, pilot study. J Sex Med. (2014) 11:471–80. doi: 10.1111/jsm.12392
11. Miller L, Verhoeven CHJ, Hout J. Extended regimens of the contraceptive vaginal ring: a randomized trial. Obs Gynecol. (2005) 106:473–82. doi: 10.1097/01.AOG.0000175144.08035.74
12. Mishell DR, Lumkin M, Stone S, Mishell DR. Inhibition of ovulation with cyclic use of progestogen-impregnated intravaginal devices. Am J Obstet Gynecol. (1972) 113:927–32. doi: 10.1016/0002-9378(72)90658-8
13. Sabatini R, Cagiano R. Comparison profiles of cycle control, side effects and sexual satisfaction of three hormonal contraceptives. Contraception. (2006) 74:220–3. doi: 10.1016/j.contraception.2006.03.022
14. Schafer JE, Osborne LM, Davis AR, Westhoff C. Acceptability and satisfaction using Quick Start with the contraceptive vaginal ring versus an oral contraceptive. Contraception. (2006) 73:488–92. doi: 10.1016/j.contraception.2005.11.003
15. Sivin I, Mishell DR, Alvarez F, Brache V, Elomaa K, Lahteenmaki P, et al. Contraceptive vaginal rings releasing Nestorone and ethinylestradiol: a 1-year dose-finding trial. Contraception. (2005) 71:122–9. doi: 10.1016/j.contraception.2004.08.010
16. Thiery M, Vandekerckhove D, Dhont M, Vermeulen A, Decoster JM. The medroxyprogesterone acetate intravaginal silastic ring as a contraceptive device. Contraception. (1976) 13:605–17. doi: 10.1016/0010-7824(76)90016-0
17. Weisberg E, Fraser IS, Mishell DRJ, Lacarra M, Bardin CW. The acceptability of a combined oestrogen/progestogen contraceptive vaginal ring. Contraception. (1995) 51:39–44. doi: 10.1016/0010-7824(94)00005-H
18. Stewart FH, Brown BA, Raine TR, Weitz TA, Harper CC. Adolescent and young women's experience with the vaginal ring and oral contraceptive pills. J Pediatr Adolesc Gynecol. (2007) 20:345–51. doi: 10.1016/j.jpag.2007.06.001
19. Gill K, Happel AU, Pidwell T, Mendelsohn A, Duyver M, Johnson L, et al. An open-label, randomized crossover study to evaluate the acceptability and preference for contraceptive options in female adolescents, 15 to 19 years of age in Cape Town, as a proxy for HIV prevention methods (UChoose). J Int AIDS Soc. (2020) 23:1–10. doi: 10.1002/jia2.25626
20. Caruso S, Cianci S, Panella M, Giunta G, Matarazzo MG, Cianci A. Comparative randomized study on the sexual function and quality of life of women on contraceptive vaginal ring containing ethinylestradiol/etonogestrel 347/1100mg or 27/117mg. Gynecol Endocrinol. (2019) 35:1–5. doi: 10.1080/09513590.2019.1603290
21. Creinin MD, Meyn LA, Borgatta L, Barnhart K, Jensen J, Burke AE, et al. Multicenter comparison of the contraceptive ring and patch: a randomized controlled trial. Obstet Gynecol. (2008) 111:267–77. doi: 10.1097/01.AOG.0000298338.58511.d1
22. Elaut E, Buysse A, De SP De CG, Gerris J, Deschepper E, et al. Relation of androgen receptor sensitivity and mood to sexual desire in hormonal contraception users. Contraception. (2012) 85:470–9. doi: 10.1016/j.contraception.2011.10.007
23. Gilliam ML, Neustadt A, Kozloski M, Mistretta S, Tilmon S, Godfrey E. Adherence and acceptability of the contraceptive ring compared with the pill among students: a randomized controlled trial. Obstet Gynecol. (2010) 115:503–10. doi: 10.1097/AOG.0b013e3181cf45dc
24. Gracia CR, Sammel MD, Charlesworth S, Lin H, Barnhart KT, Creinin MD. Sexual function in first-time contraceptive ring and contraceptive patch users. Fertil Steril. (2010) 93:21–8. doi: 10.1016/j.fertnstert.2008.09.066
25. Guida M, Sardo AD, Bramante S, Sparice S, Acunzo G, Tommaselli GA, et al. Effects of two types of hormonal contraception - oral versus intravaginal - on the sexual life of women and their partners. Hum Reprod. (2005) 20:1100–6. doi: 10.1093/humrep/deh686
26. Kestelyn E, Van Nuil JI, Umulisa MM, Umutoni G, Uwingabire A, Mwambarangwe L, et al. High acceptability of a contraceptive vaginal ring among women in Kigali, Rwanda. PLoS ONE. (2018) 13:e0199096. doi: 10.1371/journal.pone.0199096
27. Merkatz RB, Plagianos M, Hoskin E, Cooney M, Hewett PC, Mensch BS. Acceptability of the nestorone(R)/ethinyl estradiol contraceptive vaginal ring: development of a model implications for introduction. Contraception. (2014) 90:514–21. doi: 10.1016/j.contraception.2014.05.015
28. Brucker C, Karck U, Merkle E. Cycle control, tolerability, efficacy and acceptability of the vaginal contraceptive ring, NuvaRing®: results of clinical experience in Germany. Eur J Contracept Reprod Heal Care. (2008) 13:31–8. doi: 10.1080/13625180701577122
29. Buckshee K, Kumar S, Saraya L. Contraceptive vaginal ring–a rising star on the contraceptive horizon. Adv Contracept. (1990) 6:177–83. doi: 10.1007/BF01849492
30. McLellan-Lemal E, Ondeng'e K, Gust DA, Desai M, Otieno FO, Madiega PA, et al. Contraceptive vaginal ring experiences among women and men in Kisumu, Kenya: a qualitative study. Front Womens Heal. (2017) 2. doi: 10.15761/FWH.1000122
31. Merki-Feld GS, Hund M. Clinical experience with NuvaRing® in daily practice in Switzerland: Cycle control and acceptability among women of all reproductive ages. Eur J Contracept Reprod Heal Care. (2007) 12:240–7. doi: 10.1080/13625180701440180
32. Merki-Feld GS, Hund M. Clinical experience with the combined contraceptive vaginal ring in Switzerland, including a subgroup analysis of previous hormonal contraceptive use. Eur J Contracept Reprod Heal Care. (2010) 15:413–22. doi: 10.3109/13625187.2010.524717
33. Novák A, de la Loge C, Abetz L, van der Meulen EA, Novak A, de la Loge C, et al. The combined contraceptive vaginal ring, NuvaRing®: An international study of user acceptability. Contraception. (2003) 67:187–94. doi: 10.1016/S0010-7824(02)00514-0
34. Pandit SN, Chauhan AR, Anagani M, Reddy S, Birla A, Ray SK. Multicenter study of contraceptive vaginal ring (NuvaRing®) in normal daily practice in Indian women. J Obstet Gynecol India. (2014) 64:409–16. doi: 10.1007/s13224-014-0559-7
35. Peipert JF, Zhao Q, Allsworth JE, Petrosky E, Madden T, Eisenberg D, et al. Continuation and satisfaction of reversible contraception. Obstet Gynecol. (2011) 117:1105–13. doi: 10.1097/AOG.0b013e31821188ad
36. RamaRao S, Clark H, Rajamani D, Ishaku S, Mané B, Obaré F, et al. Progesterone Vaginal Ring: Results of a Three-Country Acceptability Study. New York, NY: Population Council (2015). doi: 10.31899/rh9.1063
37. Roumen FJ, Apter D, Mulders TMT, Dieben TOM. Efficacy, tolerability and acceptability of a novel contraceptive vaginal ring releasing etonogestrel and ethinyl oestradiol. HumReprod. (2001) 16:469–75. doi: 10.1093/humrep/16.3.469
38. Roumen FJME, Op Ten Berg MMT, Hoomans EHM. The combined contraceptive vaginal ring (NuvaRing®): first experience in daily clinical practice in The Netherlands. Eur J Contracept Reprod Heal Care. (2006) 11:14–22. doi: 10.1080/13625180500389547
39. Sahota J, Barnes PMFF, Mansfield E, Bradley JL, Kirkman RJEE. Initial UK experience of the levonorgestrel-releasing contraceptive intravaginal ring. Adv Contracept. (1999) 15:313–24. doi: 10.1023/A:1006748626008
40. Caruso S, Cianci S, Malandrino C, Cicero C, Lo Presti L, Cianci A, et al. Quality of sexual life of women using the contraceptive vaginal ring in extended cycles: preliminary report. EurJContraceptReprodHealth Care. (2014) 19:307–14. doi: 10.3109/13625187.2014.914488
41. Sanchez S, Araya, Araya C, Tijero M, Diaz S. Women's perceptions and experience with the progesterone vaginal ring for contraception during breastfeeding. In: London, England, Reproductive Health Matters, (1997). p. 49–57.
42. Schindler AE. The 3-keto-desogestrel / ethinylestradiol ring: a new parenteral form of hormonal contraception. Eur J Obstet Gynecol Reprod Biol. (1993) 49:13–4. doi: 10.1016/0028-2243(93)90101-H
43. Soni A, Garg S, Bangar R. Efficacy, user acceptability, tolerability, and cycle control of a combined contraceptive vaginal ring: the indian perspective. J Obstet Gynecol India. (2013) 63:337–41. doi: 10.1007/s13224-013-0391-5
44. Spencer BE, Jones V, Elstein M. The acceptability of the contraceptive vaginal ring. Br J Fam Plann. (1986) 12:82–7.
45. Dam P, Paul J, Banerjee I, Sorkhel A, Chakravorty PS. To study the acceptability and efficacy of combined contraceptive vaginal ring amidst Indian women. J Evol Med Dent Sci. (2015) 4:6602–12. doi: 10.14260/jemds/2015/956
46. Elder MG, Lawson JP, Elstein M, Nuttall ID. The efficacy and acceptability of a low-dose levonorgestrel intravaginal ring for contraception in a UK cohort. Contraception. (1991) 43:129–37. doi: 10.1016/0010-7824(91)90040-M
47. Faundes A, Hardy E, Reyes Q, Pastene L, Portes-Carrasco R. Acceptability of the contraceptive vaginal ring by rural and urban population in two Latin American Countries. Contraception. (1981) 24:393–414. doi: 10.1016/0010-7824(81)90006-8
48. Fine PM, Tryggestad J, Meyers NJ, Sangi-Haghpeykar H. Safety and acceptability with the use of a contraceptive vaginal ring after surgical or medical abortion. Contraception. (2007) 75:367–71. doi: 10.1016/j.contraception.2007.01.009
49. Guida M, Cibarelli F, Troisi J, Gallo A, Palumbo AR, Di Spiezio SA. Sexual life impact evaluation of different hormonal contraceptives on the basis of their methods of administration. Arch Gynecol Obstet. (2014) 290:1239–47. doi: 10.1007/s00404-014-3323-4
50. Hardy EE, Reyes Q, Gomez F, Portes-Carrasco R, Faundes A. User's perception of the contraceptive vaginal ring: a field study in Brazil and the Dominican Republic. Stud Fam Plann. (1983) 14:284–90. doi: 10.2307/1965397
51. Koetsawang S, Gao J, Krishna U, Cuadros A, Dhall GI, Wyss R, et al. Microdose intravaginal levonorgestrel contraception: a multicentre clinical trial II Expulsions and removals. Contraception. (1990) 41:125–41. doi: 10.1016/0010-7824(90)90142-I
52. Epstein LB, Sokal-Gutierrez K, Ivey SL, Raine T, Auerswald C. Adolescent experiences with the vaginal ring. J Adolesc Heal. (2008) 43:64–70. doi: 10.1016/j.jadohealth.2007.12.007
53. Guida M, Di Carlo C, Troisi J, Gallo A, Cibarelli F, Martini E, et al. The sexuological impact of hormonal contraceptives based on their route of administration. Gynecol Endocrinol. (2016) 2:1–5. doi: 10.1080/09513590.2016.1249841
54. Lete I, Doval JL, Perez-Campos E, Lertxundi R, Correa M, de V la, et al. Self-described impact of noncompliance among users of a combined hormonal contraceptive method. Contraception. (2008) 77:276–82. doi: 10.1016/j.contraception.2007.11.009
55. Vargas SE, Midoun MM, Guillen M, Getz ML, Underhill K, Kuo C, et al. A Qualitative systematic review of women's experiences using contraceptive vaginal rings: implications for new technologies. Perspect Sex Reprod Health. (2019) 51:71–80. doi: 10.1363/psrh.12103
56. Griffin JB, Ridgeway K, Montgomery E, Torjesen K, Clark R, Peterson J, et al. Vaginal ring acceptability and related preferences among women in low- and middle-income countries: a systematic review and narrative synthesis. PLoS ONE. (2019) 14:e0224898. doi: 10.1371/journal.pone.0224898
57. Lete I, Doval JL, Perez-Campos E, Sanchez-Borrego R, Correa M, de la Viuda E, et al. Factors affecting women's selection of a combined hormonal contraceptive method: the TEAM-06 Spanish cross-sectional study. Contraception. (2007) 76:77–83. doi: 10.1016/j.contraception.2007.04.014
58. Lete I, Pérez-Campos E. Differences in contraceptive use between Spanish female healthcare providers and Spanish women in the general population aged 23 to 49 years: the HABITS Study. Eur J Contracept Reprod Heal Care. (2014) 19:161–8. doi: 10.3109/13625187.2014.893424
59. Roumen FJME, Mishell DRJ. The contraceptive vaginal ring, NuvaRing ®, a decade after its introduction. Eur J Contracept Reprod Heal Care. (2012) 17:415–27. doi: 10.3109/13625187.2012.713535
60. Morrow KM, Rosen RK, Salomon L, Woodsong C, Severy L, Fava JL, et al. Using integrated mixed methods to develop behavioral measures of factors associated with microbicide acceptability. Qual Health Res. (2011) 21:987–99. doi: 10.1177/1049732311404245
61. Trussell J, Westoff CF. Contraceptive practice and trends in coital frequency. Fam Plann Perspect. (1980) 12:246–9. doi: 10.2307/2134867
62. Sanders SA, Graham CA, Bass JL, Bancroft J. A. prospective study of the effects of oral contraceptives on sexuality and well-being and their relationship to discontinuation. Contraception. (2001) 64:51–8. doi: 10.1016/S0010-7824(01)00218-9
63. Higgins JA, Smith NK. The Sexual Acceptability of Contraception: Reviewing the Literature and Building a New Concept. J Sex Res. (2016) 53:417–56. doi: 10.1080/00224499.2015.1134425
64. Hardon A. The development of contraceptive technologies: a feminist critique. Gend Dev. (1994) 2:40–4. doi: 10.1080/09682869308520010
65. Woodsong C, Musara P, Chandipwisa A, Montgomery E, Alleman P, Chirenje M, et al. Interest in multipurpose prevention of HIV and pregnancy: perspectives of women, men, health professionals and community stakeholders in two vaginal gel studies in southern Africa. BJOG. (2014) 121:45–52. doi: 10.1111/1471-0528.12875
Keywords: contraceptive vaginal ring, hormonal contraception, acceptability, satisfaction, sexual satisfaction
Citation: Delvaux T, Jespers V, Benova L and van de Wijgert J (2021) Acceptability and Satisfaction of Contraceptive Vaginal Rings in Clinical Studies: A Systematic Review and Narrative Synthesis. Front. Glob. Womens Health 2:799963. doi: 10.3389/fgwh.2021.799963
Received: 22 October 2021; Accepted: 11 November 2021;
Published: 14 December 2021.
Edited by:
Deborah Ann Constant, University of Cape Town, South AfricaReviewed by:
Malgorzata Beksinska, University of the Witwatersrand, South AfricaIñaki Lete, Basque Biobank, Spain
Copyright © 2021 Delvaux, Jespers, Benova and van de Wijgert. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Thérèse Delvaux, dGRlbHZhdXhAaXRnLmJl