 Robin Andrews
Robin Andrews Gabrielle Hale
Gabrielle Hale Bev John
Bev John Deborah Lancastle
Deborah Lancastle
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Glob. Womens Health, 03 December 2021
Sec. Women's Mental Health
Volume 2 - 2021 | https://doi.org/10.3389/fgwh.2021.757706
This article is part of the Research TopicThe Psychology of Menopause: Volume IView all 6 articles
Evidence suggests that monitoring and appraising symptoms can result in increased engagement in medical help-seeking, improved patient-doctor communication, and reductions in symptom prevalence and severity. To date, no systematic reviews have investigated whether symptom monitoring could be a useful intervention for menopausal women. This review explored whether symptom monitoring could improve menopausal symptoms and facilitate health-related behaviours. Results suggested that symptom monitoring was related to improvements in menopausal symptoms, patient-doctor communication and medical decision-making, heightened health awareness, and stronger engagement in setting treatment goals. Meta-analyses indicated large effects for the prolonged use of symptom diaries on hot flush frequencies. Between April 2019 and April 2021, PsychInfo, EMBASE, MEDLINE, CINAHL, Cochrane, ProQuest, PsychArticles, Scopus, and Web of Science were searched. Eighteen studies met the eligibility criteria and contributed data from 1,718 participants. Included studies quantitatively or qualitatively measured the impact of symptom monitoring on menopausal populations and symptoms. Research was narratively synthesised using thematic methods, 3 studies were examined via meta-analysis. Key themes suggest that symptom monitoring is related to improvements in menopausal symptoms, improved patient-doctor communication and medical decision-making, increased health awareness, and stronger engagement in goal-setting behaviours. Meta-analysis results indicated large effects for the prolonged use of symptom diaries on hot flush frequency: 0.73 [0.57, 0.90]. This review is limited due to the low number of studies eligible for inclusion, many of which lacked methodological quality. These results indicate that symptom monitoring has potential as an effective health intervention for women with menopausal symptoms. This intervention may be beneficial within healthcare settings, in order to improve patient-doctor relations and adherence to treatment regimes. However, findings are preliminary and quality assessments suggest high risk of bias. Thus, further research is needed to support these promising outcomes.
Systematic Review Registration Number: https://www.crd.york.ac.uk/prospero/display_record.php?, PROSPERO, identifier: CRD42019146270.
The menopause is diagnosed when over 12 months has passed since a woman last menstruated (1). Although cessation of menses is positively anticipated by some, the menopause, and the years prior, the perimenopause, can encompass a vast array of symptoms which can negatively impact quality of life (1, 2). These symptoms can be physiological in nature, including hot flushes and joint aches, whereas others impact psychological wellbeing, such as anxiety and low mood (1, 2).
Symptom monitoring has benefited numerous clinical populations, including patients with fibromyalgia, clinical depression, and cancer (3–5). Symptom monitoring involves recording symptoms using diaries, symptom questionnaires, or electronic health (e-health) instruments, including mobile apps or online symptom trackers; this can take place across time, or retrospectively at one or more given time points (6). Notable outcomes have included increased likelihood of accessing healthcare, heightened survival rates, and reductions in symptom prevalence and severity (3–5, 7, 8).
Despite broader literature demonstrating beneficial effects, symptom monitoring has not been formally evaluated as an intervention (3–5, 7, 8). According to the Medical Research Council's (MRC) framework for developing complex interventions, existing evidence for an intervention should ideally be collated into a systematic review to understand whether it is likely to be effective, whether it can be implemented into a research setting, and whether it can be widely implemented if the results are favourable (9). Should a review find evidence that an intervention is related to beneficial outcomes, the next evaluative phase should include an exploratory trial to measure the observed effects (9).
Thus, this review was designed according to three objectives: to assess whether symptom monitoring improves health outcomes relating to the menopause, e.g., changes in severity and reporting frequency of symptoms, or greater adherence to health-related behaviours; to evaluate mechanisms explaining why symptom monitoring influences health outcomes related to the menopause, e.g., whether it leads to greater health awareness or medical help-seeking; and, to categorise and compare the effects of different methods of symptom monitoring in order to inform best practise and intervention development.
The studies included in this review reported quantitative or qualitative data on the independent effects of symptom monitoring on menopausal symptoms, either as the intervention of interest or as a comparison or control intervention. Key outcomes included variances in symptom incidence or severity, and changes in health-related behaviour.
The methods used in this review are briefly summarised here, however it is recommended that the PROSPERO protocol be referred to for further details: registration number: CRD42019146270, available from: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42019146270. This review was developed in accordance with the PRISMA guidelines, and the Cochrane handbook for systematic reviews of interventions was consulted and the guidance followed (10).
Between April 2019 and August 2019, the following databases were searched PsycINFO, EMBASE, MEDLINE, CINAHL, Cochrane Library, ProQuest, PsycARTICLES, Scopus, and Web of Science. Updated searches took place in August 2020 and April 2021. Additional records were identified through forward and backward citation searches. Filters were used to focus the searches on English-language, female, adult-human participants. Date and geographical restrictions were not applied. Included studies had quantitatively or qualitatively assessed the independent effects of symptom monitoring on menopausal health outcomes.
Titles and abstracts were screened according to three preliminary criteria:
1. Participants included human adults, either mixed-gender or female-only. Mixed-gender research had to provide isolated data by gender.
2. The study collected data on the independent influence of symptom monitoring on health outcomes, either as the intervention of interest or as a comparison or control intervention, excluding research which instructed participants to monitor their symptoms in conjunction with a separate intervention.
3. The study explored common menopausal symptoms, excluding conditions which could impair an individual's ability to monitor their symptoms accurately, or could lead to fatality, hospitalisation, or were developed as a result of trauma.
Full-text reports which appeared to meet the outlined criteria were screened independently by two authors. Prior to screening, authors engaged in a calibration process in order to enhance inter-reviewer consistency by screening 25 randomly selected studies. A Kappa statistic of: κ=0.757, ρ= 0.001 quantified agreement, indicating substantial inter-reviewer consistency (11). Any disagreements were discussed by authors. A PRISMA flowchart was produced to display the process of study selection, as well as reasons for exclusion (see Figure 1).
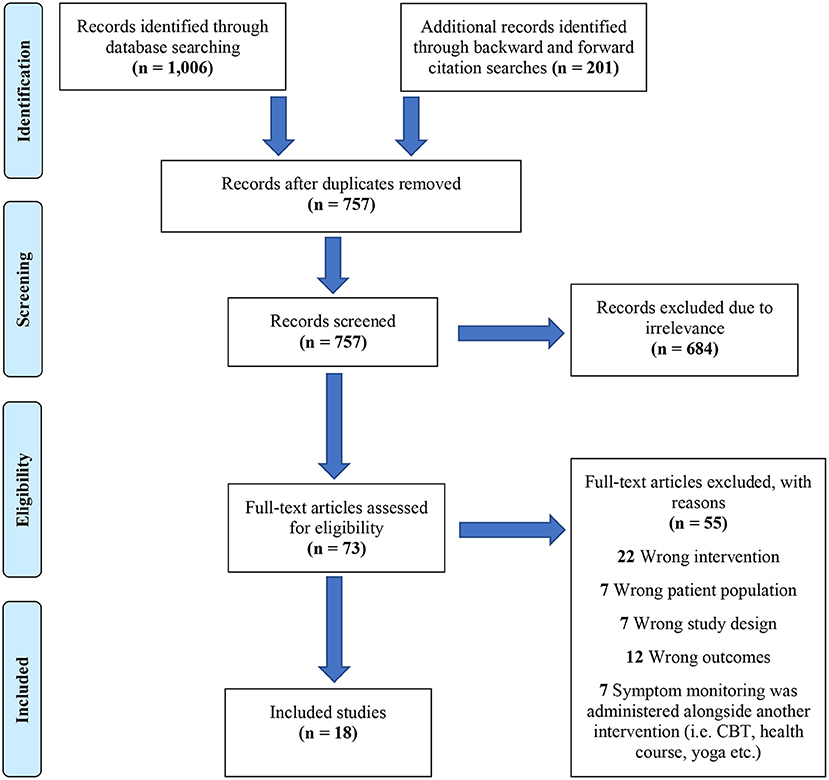
Figure 1. PRISMA flowchart of study selection process.
For quantitative research, the National Institute for Health and Care Excellence (12) developed a checklist based around the Graphical Appraisal Tool for Epidemiological studies [GATE; (13)]. NICE (12) appropriated this checklist for evaluating health intervention studies. This checklist was deemed suitable for this review as it can be used to appraise the internal and external validity of various research designs.
An appraisal tool for qualitative research was used to assess studies with these characteristics (14). This checklist is based around characteristics of qualitative research which may affect a study's internal validity, i.e. whether the links between the data, interpretations, and conclusions are clearly defined (14).
Both checklists were amended according to each study under review; in cases where randomisation did not occur (i.e. in observational studies) judgements were made based on whether confounding variables may have influenced findings. This method has been implemented into the Cochrane risk of bias tool, hence why it was deemed appropriate (10).
A thematic synthesis provided a means of combining qualitative and quantitative information in a succinct manner. This meant that findings from all included studies could be simultaneously evaluated and compared. Key themes were identified by summarising the extracted results of each study, with contributions being made by 2 authors.
RevMan 5.3 software was used to compute a meta-analysis of comparable studies which used continuous data. Three studies described comparable study designs and symptom monitoring methods, pre-treatment and post-treatment data were combined, and the standardised mean difference and 95% confidence intervals (CIs) were computed. A random-effects model was used to compensate for variations within the selected studies. The classification of effect sizes was determined from Cohen's (15) conventional values of effect size which indicate: 0.20 = small effect size, 0.40 = medium effect size, and 0.60 = large effect size. Significance was set at ρ < 0.05.
Heterogeneity was tested using the I2 value. The interpretation of the observed I2 value was determined by The Cochrane Handbook of Systematic Reviews guidance which indicated that I2 <30% was considered mild heterogeneity, I2 >30% as moderate heterogeneity, I2 >50% as substantial heterogeneity and I2 >75% as considerable heterogeneity (16).
Due to differences in menopausal symptoms and symptom monitoring methods, populations and interventions varied, therefore results were predominantly synthesised narratively. A meta-analysis was conducted on three studies which had provided data on the impact of symptom diaries on menopausal hot flushes.
Searches returned 18 studies which met the eligibility criteria and contributed data from 1,718 participants, see Figure 1 to view summary of study selection process.
Two studies involved the Women's Health Assessment Tool (WHAT), a symptom questionnaire relevant to midlife women (17, 18). Two studies included the Menopause Rating Scale (MRS), a questionnaire developed to evaluate menopausal symptom frequency, severity, and change (19, 20). Two studies explored The Computerised Symptom Capture Tool for Menopause [C-SCAT-M; (21, 22)]. The C-SCAT-M is a mobile app which features 54 menopausal symptoms, which were originally identified via the Seattle Women's Midlife Health Study (SWMHS). One study qualitatively explored the effects of daily self-weighing on perimenopausal weight changes (23). One study explored the MenoScores Questionnaire, the primary outcome was the hot flush scale (24). Four studies provided data on the effects of symptom diary use on perimenopausal symptoms, menopause-related headaches, sexual dysfunction, and incontinence (25–28). Six randomised controlled trails (RCTs) provided data on symptom-diary use and hot flush frequency (29–34). Three RCTs were evaluated via meta-analysis (30–32). See Table 1 to view a full summary of the characteristics of the included studies.
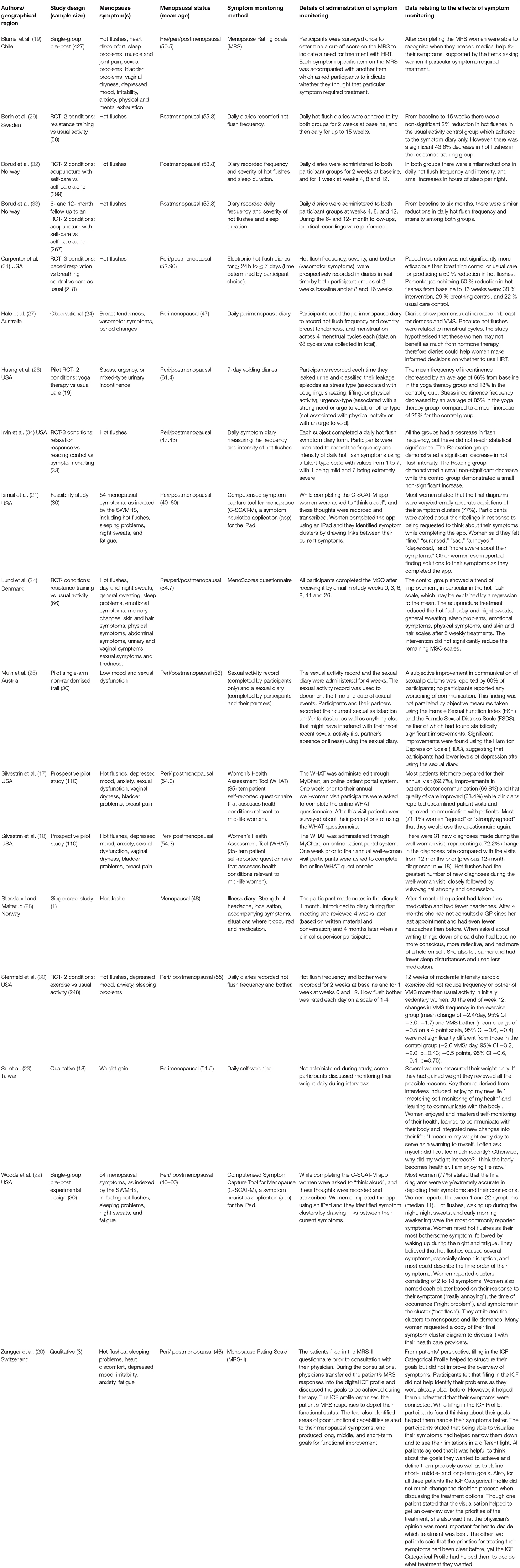
Table 1. Visual summary of study characteristics.
Few studies were judged to have adequate validity, with all but 4 being considered unsatisfactory (30–33). See Table 2 to view quality assessment summary ranked from lowest to highest quality.
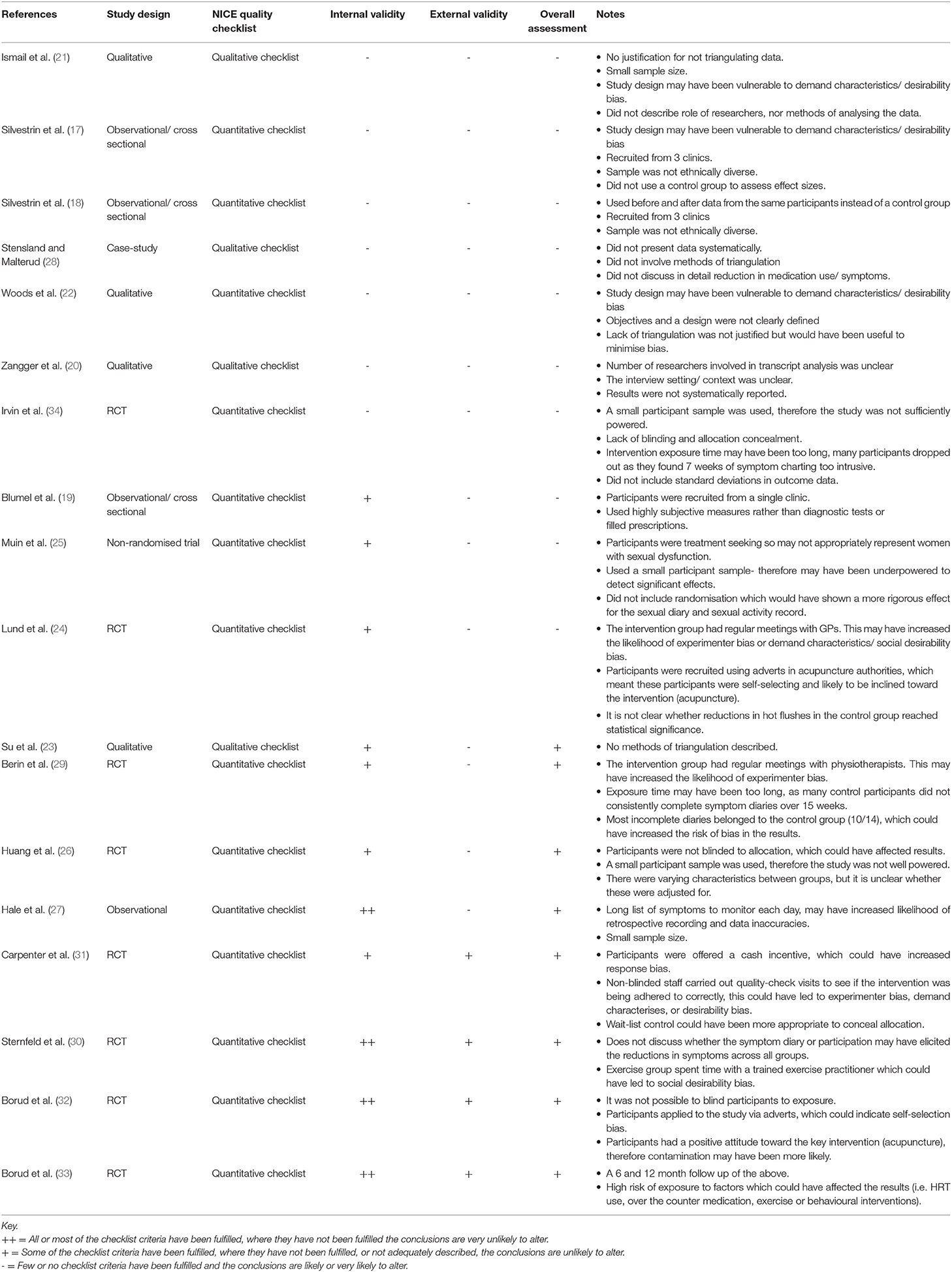
Table 2. Quality assessment summary.
Five themes were identified, one was related to physiological changes following adherence to symptom monitoring and encompassed variations in symptom frequency and severity regarding hot flushes, urinary incontinence, migraines, sexual dysfunction, and depression; the other four themes encompassed health-related behavioural changes and included improvements in patient-doctor communication, shared decision-making, health and symptom awareness, and goal setting.
Reductions in hot flush frequency were present among studies which involved the use of symptom diaries (24, 30–33). Four randomised trials included before and after data on the effects of symptom diaries on vasomotor symptoms (VMS) and reported significant reductions in hot flush frequency scores (30–33). Diary studies with smaller sample sizes also reported reductions in VMS, although these findings were non-significant (29, 34).
Huang et al. (26)used voiding diaries to research symptom change and frequency among 19 menopausal women with urinary incontinence partaking in a yoga therapy intervention. All participants kept 7-day voiding diaries where they recorded each time they leaked urine. After 6 weeks, total incontinence frequency had reduced by 13% in the control group which used the voiding diary alone.
tensland and Malterud (S28) described a perimenopausal patient presenting with worsening migraine and muscle pain. This patient was advised to compile an illness diary for 4 weeks, detailing the strength of her headache, its localisation, accompanying symptoms, situations where it had occurred, and medications used (28). After 4 weeks of diary use the patient reported using half as much medication as she had the month prior (28). At four-month follow-up the patient stated that her symptoms had improved even more so, and attributed these improvements to her becoming more aware and reflective of her health through the symptom-diary (28).
Muin et al. (25) studied 30 menopausal participants diagnosed with sexual dysfunction, who were asked to keep a sexual diary for 4 weeks. Sixty percent of participants reported subjective improvements in sex life and sexual communication and significant improvements were found using the Hamilton Depression Scale (HDS).
Two studies explored the WHAT menopause symptom questionnaire among menopausal patients attending a well woman clinic (17, 18). These studies reported that the WHAT had improved patient-doctor communication from both the clinicians' and patients' perspectives, which led to a rise in the number of diagnoses made, especially for sensitive conditions including vaginal dryness, sexual dysfunction and depression (17, 18).
Ismail and colleagues (21) evaluated the C-SCAT-M app, which enables users to appraise their menopause symptoms and generate a report. Participants were asked to voice their thoughts and experiences whilst completing the app, and many requested a copy of their symptom report to share with their physician, commenting that it would be a useful communication aid (21).
Two studies evaluating the MRS found it improved patients' efficacy in making medical treatment decisions (19, 20).
Hale et al. (27) employed symptom-diaries to explore whether menopausal symptoms were related to the menstrual cycle. Diaries showed premenstrual increases in breast tenderness and VMS, therefore authors hypothesised that symptom diaries could help women identify when cyclical HRT or non-hormonal treatments might be more beneficial than continuous HRT (27).
During Zangger et al.'s (20) study, one participant stated that being able to see her symptoms visually represented on the MRS had enabled her to recognise that they were connected. In Ismail and colleagues (21) study, participants found solutions to their symptoms as they completed the C-SCAT-M app. The researchers proposed that heightened symptom awareness had prompted participants to reflect upon strategies to alleviate their symptoms.
Su et al. (23) evaluated the weight loss experiences of 18 obese perimenopausal women who had been diagnosed with metabolic syndrome. Findings demonstrated that awareness of weight gain was a factor that motivated perimenopausal women to change their lifestyle habits (23). Participants expressed that they had become more aware of their health via daily self-weighing, which made them feel better able to “communicate with their body's voice” (23).
Another finding to emerge from Zangger et al.'s (20) study was related to goal setting. After completing the MRS, women were able to restructure their symptom scores into short-, middle, and long-term health goals. Another study conducted by Woods and colleagues (22) evaluated the C-SCAT-M. This research focused on the app's ability to allow women to communicate their heuristics related to menopausal symptom attributions (22). By using the C-SCAT-M, women reported their symptoms, grouped them into clusters, specified the order of occurrence, gave the clusters meaningful names, and identified relationships between symptoms. The authors speculated that by appraising, naming, prioritising, and grouping their symptoms, participants gleaned a greater understanding of what they were hoping to achieve in terms of treatment.
Monitoring symptoms across time appeared to be useful for reducing symptom frequencies, as well as medication usage, and this effect may be explained by heightened health and symptom awareness (24–26, 28–34). Patient-doctor communication was facilitated by tools which allowed users to define the totality of their symptoms from an exhaustive inventory (17, 18, 21). Medical decision-making was facilitated by utilising symptom appraisal tools in conjunction with items assessing medication need, or digital ICF profiles, thus suggesting that input from medical systems is vital for unlocking the tool's decision-making capabilities (19, 20). Medical decision-making may also be improved by menstrual diaries, as they can allow patients and practitioners to understand whether VMS are related to the menstrual cycle or menopause (27). An illness diary, symptom appraisal tools, and daily self-weighing were related to improvements in health and symptom awareness, and this increased awareness was related to symptom improvements and changes in health-related behaviours (20, 21, 23, 28). Finally, symptom appraisal tools which allowed the user to compare their symptoms and corresponding severities supported setting treatment goals (20, 22).
Three RCTs were deemed appropriate for evaluation via quantitative synthesis. These studies included continuous data measuring the independent effects of prolonged symptom diary use on VMS frequency (30–32). Using a random effects model, the standardised mean difference and statistical heterogeneity with Chi2 and I2 figures were calculated.
Three other studies measured the independent effects of prolonged symptom diary use on VMS (29, 33, 34). One was excluded because it used a small participant sample (N = 11) in the symptom diary arm and failed to provide standard deviations for mean frequency of VMS following symptom diary use (34).
Berin et al.'s (29) study was excluded from the main meta-analysis because a disproportionate amount of missing data was attributed to the control group. The control group provided before and after data from participants who had been using VMS diaries for 15 weeks, however 35% of these participants did not consistently complete diaries. This meant the analysis likely underestimated reductions in VMS (29). To understand the impact of excluding this study on the overall effect of symptom monitoring, a meta-analysis was conducted with Berin et al.'s (29) data included and it suggested a large effect size (0.61, 95% CI 0.34 to 0.88) with the difference being significant in favour of post symptom-diary use (Z = 4.45, p = 0.001). However, heterogeneity was substantial (I2 = 60%).
A third study was excluded which depicted a 6- and 12-month follow-up of a study which is included in the present meta-analysis (33). The later study increased the heterogeneity statistic (I2 = 78%), therefore the earlier study by Borud et al. (32) was chosen for inclusion.
The three included studies involved a total of 303 participants at baseline, and 296 participants post-intervention. Each study reported continuous data for VMS frequencies. Two studies included mean differences in VMS frequency following symptom diary use therefore mean VMS frequency following symptom-diary use was calculated by subtracting the post-intervention mean difference from the pre-intervention mean (30, 32). Borud et al. (32)reported mean frequency of VMS at baseline and the standard deviation (13.1, 4.9) and mean change in VMS frequency following symptom diary use and the standard deviation (9.4, 3.7). Sternfeld et al. (30) reported confidence intervals instead of standard deviations for baseline VMS frequency (8.0 [7.3, 8.7]) and mean change in VMS frequency following symptom diary use (−2.6 [−3.2, −2.0]), therefore confidence intervals for baseline and post-intervention measures were recalculated into standard deviations (4.26, 3.56). Carpenter et al. (31) reported mean frequency of VMS and standard deviations pre (7.31, 4.04) and post prolonged symptom-diary use (4.76, 3.5).
The standardised mean difference for symptom frequency suggested a large effect size (0.73, 95% CI 0.57 to 0.90) and the difference was significant in favour of post symptom-diary use (Z = 8.68, p = 0.001). Heterogeneity was absent (I2 = 0%). See Figure 2 to view a forest plot detailing the effects of symptom diaries on hot flush frequency scores.
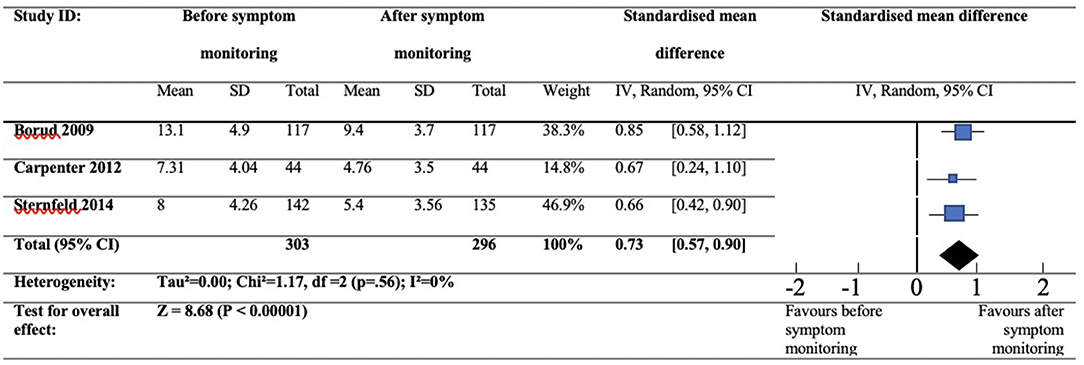
Figure 2. Forest plot showing hot flush frequency at baseline and post-symptom diary use.
This review investigated whether symptom monitoring could yield improvements in menopausal symptoms and health-related behaviours. This suggests that symptom monitoring has potential as an effective intervention. Systematic searches returned 18 studies which contributed data from 1,718 participants. Methods which allowed patients to track their symptoms across time were related to symptom improvements and heightened health awareness, whereas tools which enabled patients to appraise their symptoms at any given time point enhanced health awareness, treatment goal setting, patient-doctor communication, and shared decision-making. A meta-analysis suggested large effects for the prolonged use of symptom diaries on VMS frequencies: 0.73 [0.57, 0.90]. In regard to the MRC framework, these results suggest that the effects of prolonged symptom monitoring be further measured via an exploratory trial; and should symptom monitoring be implemented within the wider community, it is recommended that symptom monitoring and appraisal methods should include an exhaustive array of symptoms and be used in conjunction with organised health systems in order to reap potential benefits in patient doctor communication, medical decision-making, and treatment goal setting (9).
The key finding from this review was that tracking symptoms could facilitate improvements (24–26, 28, 30–34). This is supported by the meta-analysis which assessed VMS frequency scores at baseline and after prolonged symptom diary use; results favoured post-diary use and showed large effects for reducing VMS (30–32). This result has been demonstrated by prior studies which have shown symptom reductions within alternative patient populations, suggesting that the beneficial effects of symptom monitoring are transferable across multiple ailments (5, 7, 8).
Symptom monitoring was also associated with improvements in health-related behaviours, including heightened awareness (21–23, 28). Ismail et al. (21) reported that women found solutions to their menopausal symptoms as they completed the C-SCAT-M, suggesting that symptom appraisal had brought the participant's health to the forefront of their minds, which prompted them to reflect, consider remedies, and invoke behavioural changes (21). A similar result was reported in a case-study whereby a patient reported reductions in medication use and headache symptoms following use of a symptom diary; the patient attributed these improvements to the symptom diary heightening her awareness, which prompted her to amend her health behaviours accordingly (28).
The MRS and the C-SCAT-M were related to treatment goal setting (20, 22). Goal setting is a facet of Chewning and Sleath's (35) client-centred model of medical decision-making and management. This model depicts how the patient and physician could work together to carry out the following practises: identify treatment goals, choose treatment options, monitor symptoms and evaluate treatments, and revise treatments if problems occur.
Symptom monitoring methods could support this model, tools such as the MRS and the C-SCAT-M can help patients prioritise symptoms and identify the improvements they expect to see in the future, and this process can facilitate decision-making and patient-doctor communication. This theory corresponds with additional themes from this review, which found evidence that symptom monitoring could be useful for improving patient-doctor communication and facilitating decisions to use HRT and seek timely medical help (17–21, 27).
This review is limited by the low number of studies identified for inclusion, many of which were lacking methodological quality. Moreover, only three studies were integrated into the meta-analysis, meaning a funnel plot was not computed and risk of bias could not reliably be ascertained (36). Meta-analyses with low study inclusions are notorious for overestimating effect sizes (37).
To the author's knowledge, no other meta-analyses of this type have been conducted before, therefore this review provides a foundation for subsequent estimations of the effects of symptom diaries in symptom reduction. Numerous studies have given evidence that symptom monitoring could yield symptom improvements for a number of conditions (5, 7, 8). Therefore, future reviews should assess prolonged symptom monitoring on alternative conditions and symptoms.
An unexpected observation was that authors appeared to consider symptom monitoring as a benign “control” activity (29–32). Only two RCTs acknowledged the symptom reductions observed within the control groups, and neither considered whether symptom monitoring contributed to these reductions, despite symptom monitoring being the only activity control participants had been instructed to adhere to (24, 33). While Borud et al. (33) speculated that the improvements were due to “the therapeutic effects of research participation”, Lund et al. (24) posited that the reductions could be attributed to a regression toward the mean. This might be plausible given the non-significant reductions seen in studies with smaller sample sizes (29, 34). Although it is worth noting that all RCTs included in this review reported some degree of improvement within the control groups, and the majority reported significant effects. Furthermore, data from Berin et al.'s (29) research were excluded from the meta-analysis, as this study reported that 35% of participants did not consistently complete symptom diaries, suggesting reductions in VMS were likely to be underestimated (29). However, to understand whether this exclusion impacted the main review findings, a meta-analysis was conducted including Berin et al.'s (29) data and it continued to support the key result demonstrating large effects for the prolonged use of symptom diaries on VMS frequencies (0.61, 95% CI 0.34 to 0.88). These observations indicate that symptom monitoring can induce clinical benefits, which authors neither expect nor acknowledge, suggesting that there is an unrealised potential for monitoring to be implemented as a useful health intervention.
Further to this, in the included RCTs symptom monitoring was not intended as an intervention and therefore do not include non-symptom monitoring arms. Thus, it is not possible to discern whether any observed reduction in symptoms were an effect of symptom monitoring via diaries or due to alternative mechanisms (e.g., passage of time), although it would be anticipated that such mechanisms would also be in play in any intervention group. The MRC framework proposes that should reviewed literature suggest an intervention has potential benefits, the next phase to evaluate it should involve an exploratory trial (9). Therefore, future research should explore the effects of symptom monitoring as a standalone intervention for menopausal symptoms against a control intervention in which monitoring is not included. Such a design has previously been used in fertility research, which notably demonstrated that symptom monitoring was associated with improvements in anxiety and depression ratings (38).
However, evidence from the reviewed studies suggest that monitoring might be associated with increased attrition rates; Irvin et al. (34) reported that participants allocated into the monitoring group found symptom charting intrusive, whereas Berin et al. (29) mentions incomplete diaries in the control group. These factors may be indictive of negative consequences and could have an impact on the outcomes measured; therefore, further research should aim to understand the harms associated with symptom monitoring, as well as the benefits.
This review suggests that symptom monitoring and appraisal methods are effective for reducing menopausal symptoms, and improving health awareness, shared decision-making, patient-doctor communication, and treatment goal setting. In line with the MRC framework, this suggests that symptom monitoring is likely to be an effective intervention (9). However, these findings are preliminary, and few studies were identified for inclusion, many of which lacked methodological quality, suggesting more research is needed to establish symptom monitoring as a useful intervention. A key finding was that prolonged symptom monitoring is effective for symptom reduction, a result which should further be investigated via an exploratory trial, in accordance with the methods established by the MRC framework (9). In terms of implementing symptom monitoring within the wider community, these results support that symptom appraisal tools should be used in conjunction with organised health systems to unlock potential improvements in decision-making, goal setting, and patient-doctor communication. Ultimately, the findings described here could provide foundational data to researchers wishing to unravel the effects of symptom monitoring, or develop a simple, cost-effective intervention which may have significant implications on menopausal health outcomes.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
RA was responsible for conceptualising this review's design, collecting, analysing, and interpreting the data, and drafting the final article. GH contributed to the acquisition, analysis and interpretation of data, and critically revised and approved the article for publication. BJ and DL were responsible for conceptualising the study design, critically appraising the article for important intellectual content, and final approval for publication. All authors contributed to the article and approved the submitted version.
This research is part of a PhD thesis which is funded by the University of South Wales, Knowledge Economy Skills Scholarships [KESS 2, a pan-Wales operation supported by European Social Funds (ESF) through the Welsh Government], and Health & Her. KESS-2 (grant number: c80815 KESS 2).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors would like to thank our faculty librarian, Gill Edwardes for her role in consulting with the development of the search expressions, search strategy, and best use of resources.
1. Dalal PK, Agarwal M. Postmenopausal syndrome. Indian J Psychiatry. (2015) 6:S222. doi: 10.4103/0019-5545.161483
2. Constantine GD, Graham S, Clerinx C, Bernick BA, Krassan M, Mirkin S, et al. Behaviours and attitudes influencing treatment decisions for menopausal symptoms in five European countries. Post Reproductive Health. (2016) 3:112–22. doi: 10.1177/2053369116632439
3. Shafran R, Gyani A, Rostron J, Allen S, Myles-Hooton P, Allcott-Watson H, et al. Translating the intention to seek treatment into action: does symptom monitoring make a difference? results from a randomized controlled trial. Behav Cogn Psychother. (2019) 47:114–28. doi: 10.1017/S1352465818000498
4. Basch E, Deal AM, Kris MG, Scher HI, Hudis CA, Sabbatini P, et al. Symptom monitoring with patient-reported outcomes during routine cancer treatment: a randomized controlled trial. J Clin Oncol. (2016) 3:557–65. doi: 10.1200/JCO.2015.63.0830
5. Collinge W, Yarnold P, Soltysik R. Fibromyalgia symptom reduction by online behavioral self-monitoring, longitudinal single subject analysis and automated delivery of individualized guidance. N Am J Med Sci. (2013) 9:546. doi: 10.4103/1947-2714.118920
6. Ben-Zeev D, McHugo GJ, Xie H, Dobbins K, Young MA. Comparing retrospective reports to real-time/real-place mobile assessments in individuals with schizophrenia and a nonclinical comparison group. Schizophr Bull. (2012) 3:396–404. doi: 10.1093/schbul/sbr171
7. Khakbazan Z, Taghipour A, Roudsari RL, Mohammadi E. Help seeking behavior of women with self-discovered breast cancer symptoms: a meta-ethnographic synthesis of patient delay. PLoS ONE. (2014) 12:e110262. doi: 10.1371/journal.pone.0110262
8. Devineni T, Blanchard EB. A randomized controlled trial of an internet-based treatment for chronic headache. Behav Res Ther. (2005) 43:277–92. doi: 10.1016/j.brat.2004.01.008
9. O'Cathain A, Croot L, Duncan N N, Rousseau Sworn K, Turner KM, et al. Guidance on how to develop complex interventions to improve health and healthcare. BMJ open. (2019) 9:e029954. doi: 10.1136/bmjopen-2019-029954
10. Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. (2019) Cochrane handbook for systematic reviews of interventions, second ed. Chichester (UK): John Wiley and Sons. doi: 10.1002/9781119536604
11. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. (1977) 1:159–74. doi: 10.2307/2529310
12. National Institute for Health and Care Excellence (NICE). Quality Appraisal Checklist: Quantitative Intervention Studies, Methods for the Development of NICE Public Health Guidance (3rd edition). (2019). Available online at: https://www.nice.org.uk/process/pmg4/chapter/appendix-f-quality-appraisal-checklist-quantitative-intervention-studies, 2012 (accessed 13 August 2019).
13. Jackson R, Ameratunga S, Broad J, Connor J, Lethaby A, Robb G, et al. The GATE frame: critical appraisal with pictures. BMJ Evid Based Med. (2006) 2:35–8. doi: 10.1136/ebm.11.2.35
14. National Institute for Health and Care Excellence (NICE). Quality Appraisal Checklist: Qualitative Studies, Methods for the Development of NICE Public Health Guidance (3rd edition). (2019). Available online at: https://www.nice.org.uk/process/pmg4/chapter/appendix-h-quality-appraisal-checklist-qualitative-studies, 2012 (accessed 13 August 2019).
15. Cohen J. (1962) The statistical power of abnormal-social psychological research: a review. J Abnorm Psychol. 65:145. doi: 10.1037/h0045186
16. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. (2002) 11:1539–58. doi: 10.1002/sim.1186
17. Silvestrin TM, Steenrod AW, Coyne KS, Gross DE, Esinduy CB, Kodsi AB, et al. An approach to improve the care of mid-life women through the implementation of a Women's Health Assessment Tool/Clinical Decision Support toolkit. Women's Health. (2016) 5:456–64. doi: 10.1177/1745505716664742
18. Silvestrin TM, Steenrod AW, Coyne KS, Gross D, Esinduy C, Kodsi A, et al. Outcomes of Implementing the Women's Health Assessment. Tool, and Clinical Decision Support Tool Kit Women's Health. (2016) 3:313–23. doi: 10.2217/whe.16.3
19. Blumel JE, Arteaga E, Parra J, Monsalve C, Reyes V, Vallejo MS, et al. Decision-making for the treatment of climacteric symptoms using the Menopause Rating Scale. Maturitas. (2018) 111:15–9. doi: 10.1016/j.maturitas.2018.02.010
20. Zangger M, Poethig D F, Meissner, von Wolff M, Stute P. Linking the menopause rating scale to the International classification of functioning, disability and health–A first step towards the implementation of the EMAS menopause health care model. Maturitas. (2018) 118:15–9. doi: 10.1016/j.maturitas.2018.10.003
21. Ismail R, Linder LA, MacPherson CF, Woods NF. Feasibility of an iPad application for studying menopause-related symptom clusters and women's heuristics. Inform Health Soc Care. 3:247–66. doi: 10.3109/17538157.2015.1008489
22. Woods NF, Ismail R, Linder LA, Macpherson CF. Midlife women's symptom cluster heuristics: evaluation of an iPad application for data collection. Menopause. (2015) 10:1058. doi: 10.1097/GME.0000000000000429
23. Su MC, Lin HR, Chu NF, Huang CH, Tsao LI. Weight loss experiences of obese perimenopausal women with metabolic syndrome. J Clini Nurs. (2015) 24:1849–59. doi: 10.1111/jocn.12806
24. Lund KS, Siersma V, Brodersen J, Waldorff FB. Efficacy of a standardised acupuncture approach for women with bothersome menopausal symptoms: a pragmatic randomised study in primary care (the ACOM study). BMJ Open. (2019) 1:e023637. doi: 10.1136/bmjopen-2018-023637
25. Muin DA, Wolzt M, Rezaei SS, Tremmel-Scheinost M, Salama M, Fuchs C, et al. Effect of sexual diary keeping and self-evaluation on female sexual function and depression: a pilot study, Eur J Contracept Reprod Health Care. (2016) 2:141–9. doi: 10.3109/13625187.2015.1074676
26. Huang AJ, Jenny HE, Chesney MA, Schembri M, Subak LL. A group-based yoga therapy intervention for urinary incontinence in women: a pilot randomized trial. Female Pelvic Med Reconstr Surg. (2014) 3:147–54. doi: 10.1097/SPV.0000000000000072
27. Hale GE, Hitchcock CL, Williams LA, Vigna YM, Prior JC. Cyclicity of breast tenderness and night-time vasomotor symptoms in mid-life women: information collected using the Daily Perimenopause Diary. Climacteric. (2003) 2:128–39. doi: 10.1080/cmt.6.2.128.139
28. Stensland P, Malterud K. Unravelling empowering internal voices- a case study on the interactive use of illness diaries. Fam Pract. (2001) 4:425–9. doi: 10.1093/fampra/18.4.425
29. Berin E, Hammar M, Lindblom H, Lindh-Åstrand L, Rubér M, Holm AC. Resistance training for hot flushes in postmenopausal women: A randomised controlled trial. Maturitas. (2019) 126:55–60. doi: 10.1016/j.maturitas.2019.05.005
30. Sternfeld B, Guthrie KA, Ensrud KE, LaCroix AZ, Larson JC, Dunn AL, et al. Efficacy of exercise for menopausal symptoms: a randomized controlled trial. Menopause. (2014) 4 330. doi: 10.1097/GME.0b013e31829e4089
31. Carpenter JS, Burns DS, Wu J, Otte JL, Schneider B, Ryker K, et al. Paced respiration for vasomotor and other menopausal symptoms: a randomized, controlled trial. Journal of general internal medicine. (2013) 2:193–200. doi: 10.1007/s11606-012-2202-6
32. Borud EK, Alraek T, White A, Fonnebo V, Eggen AE, Hammar M, et al. The acupuncture on hot flushes among menopausal women (ACUFLASH) study, a randomized controlled trial. Menopause. (2009) 3:484–93. doi: 10.1097/gme.0b013e31818c02ad
33. Borud EK, Alraek T, White A, Grimsgaard S. The Acupuncture on Hot Flashes Among Menopausal Women study: observational follow-up results at 6 and 12 months. Menopause. (2010) 2:262–8. doi: 10.1097/gme.0b013e3181c07275
34. Irvin JH, Domar AD, Clark C, Zuttermeister PC, Friedman R. The effects of relaxation response training on menopausal symptoms. J Psychosom Obstet Gynaecol 4. (1996) 202–7. doi: 10.3109/01674829609025684
35. Chewning B, Sleath B. Medication decision-making and management: a client-centered model, Social science and medicine. (1996) 3:389–98. doi: 10.1016/0277-9536(95)00156-5
36. Lau J, Ioannidis JP, Terrin N, Schmid CH, Olkin I. The case of the misleading funnel plot. BMJ. (2006) 7568:597–600. doi: 10.1136/bmj.333.7568.597
37. Seide SE, Röver C, Friede T. Likelihood-based random-effects meta-analysis with few studies: empirical and simulation studies. BMC Med Res Methodol. (2019) 1:16. doi: 10.1186/s12874-018-0618-3
Keywords: symptom monitoring, menopause, midlife, menopausal symptoms, MRC framework, health behaviour, e-health, women's health
Citation: Andrews R, Hale G, John B and Lancastle D (2021) Evaluating the Effects of Symptom Monitoring on Menopausal Health Outcomes: A Systematic Review and Meta-Analysis. Front. Glob. Womens Health 2:757706. doi: 10.3389/fgwh.2021.757706
Received: 12 August 2021; Accepted: 09 November 2021;
Published: 03 December 2021.
Edited by:
Caroline Gurvich, Monash University, AustraliaReviewed by:
Vera Mateus, Mackenzie Presbyterian University, BrazilCopyright © 2021 Andrews, Hale, John and Lancastle. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Robin Andrews, cm9iaW4uYW5kcmV3c0Bzb3V0aHdhbGVzLmFjLnVr; orcid.org/0000-0002-5149-7649
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.