 Ava Oliaei1
Ava Oliaei1 Dean Elterman
Dean Elterman Eric Zimmerman
Eric Zimmerman Bilal Chughtai
Bilal Chughtai Hamid Sadri
Hamid Sadri
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Gastroenterol. , 03 September 2024
Sec. Therapy in Gastroenterology
Volume 3 - 2024 | https://doi.org/10.3389/fgstr.2024.1398102
Background and aim: Fecal incontinence (FI) is defined as the unintended loss of solid or liquid stool. FI adversely affects the patient’s quality of life. However, due to stigma, lack of awareness, and underdiagnosis, there is a notable gap in the knowledge regarding its prevalence. This study aimed to conduct a systematic review and meta-analysis of published literature reporting on FI prevalence and estimate the number of people afflicted by FI.
Methods: A systematic review was conducted following the PRISMA 2020 guidelines, using the Embase, MEDLINE, CINHAL, and PubMed databases to identify relevant publications in the English language. Two reviewers independently screened the articles and extracted data. The reference sections and content of the review papers were also evaluated. Thirty-two articles were selected and included. A meta-analysis of proportions was performed using RStudio software. A sub-analysis was conducted to account for the variation between sample population age groups to minimize heterogeneity. The pooled prevalence was extrapolated to the Canadian population and a sample of ten densely populated countries to estimate the number of people affected by FI.
Results: The Mean pooled FI prevalence in men and women was 7% (95% CI: 6-9%) and 10% (95% CI: 8-12%), respectively. The sub-analysis mean pooled prevalence of FI in men and women was 8% (95% CI: 6-10%) and 10% (95% CI: 8-12%), respectively. The authors estimate that between 1 and 1.5 million Canadians and 320 to 500 million people in the ten most populous countries suffer from FI.
Conclusion: Fecal incontinence is a prevalent underdiagnosed condition requiring appropriate and timely treatment to improve a patient’s quality of life.
Fecal incontinence (FI) is defined as the unintended loss of solid or liquid stool (1). FI substantially burdens an individual’s life, and patients often report lower quality of life (QoL) (2). Despite the significant burden, FI continues to be under-reported and undertreated, which stems from the stigma surrounding FI and the general lack of knowledge and awareness (3). This unawareness may impact the patient-physician interaction during the consultation, as many patients are embarrassed to discuss their symptoms with the healthcare provider or believe the symptoms are part of normal aging (4). Additionally, clinicians are often reluctant to ask about incontinence, thereby perhaps compounding the problem (5).
More than 50% of patients with FI are estimated not to seek treatment (6). A survey of individuals seeking gastroenterology consultations showed that 84% of FI patients did not proactively inform the specialist during the consultation (2). Furthermore, the diagnosis of FI is hindered by its heterogeneity and subjective nature. The differences in the etiology and pathophysiology of FI deter an objective assessment, wherein stigma and wording of the question can influence the results (7). As such, determining FI’s prevalence has proven challenging. Understandably, due to underreporting and underdiagnosis, no extensive population survey has been conducted on FI in Canada to date. This study aimed to conduct a systematic review and meta-analysis of published literature that reports on FI prevalence (primary outcomes)to better understand the prevalence of FI in Canada and estimate the number of people suffering from FI (secondary outcomes) to assist health policymakers in making informed decisions addressing FI.
We conducted a systematic review according to the “ Preferred Reporting Items for Systematic Reviews and Meta-Analyses “ (PRISMA) 2020 guidelines (Figure 1, Supplementary Table S1) (8).
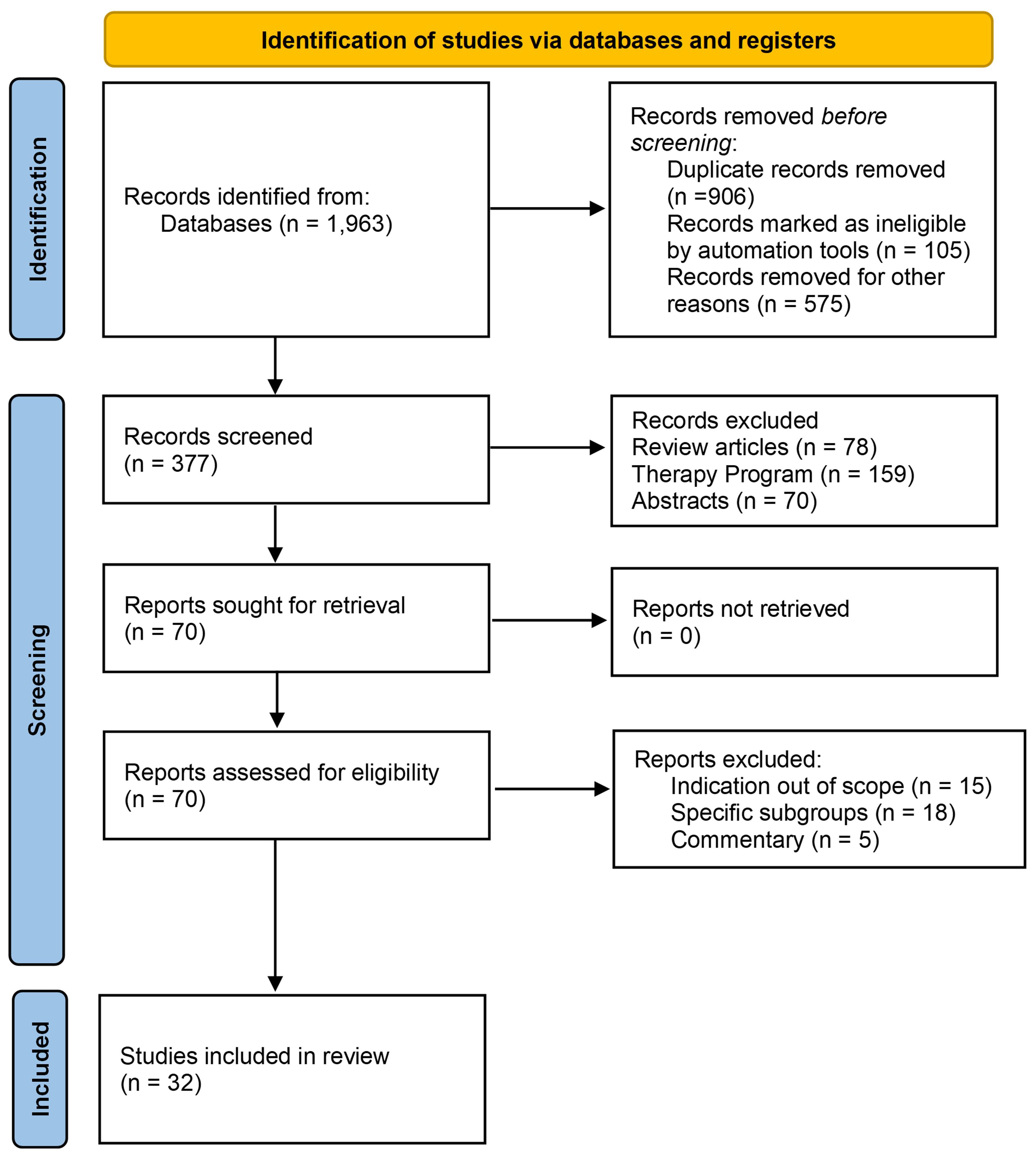
Figure 1. PRISMA literature search screening and selection flow-chart for fecal incontinence.
We used the Embase, MEDLINE, CINHAL, and PubMed databases until December 2023. The search strategy focused on the terms “fecal incontinence” and “accidental bowel leakage” in conjunction with “prevalence” and “epidemiology.” The texts, tables, and graphs of the articles were thoroughly examined for data extraction. Additionally, the reference section and content of the review papers were evaluated. Two sets of reviewers (HS, AO and SS, EZ) independently screened and assessed the titles and abstracts of the identified articles, and studies were included in the analysis based on the following criteria:
Scope: Fecal incontinence prevalence and epidemiology study
Population: Adult patients with an FI diagnosis
Type of study: Epidemiology studies
Publications: Full article published in the English language
Out of scope: Other pathophysiology, such as post-surgical and post-partum retention
Publication type: Conference abstracts, review articles, letters, commentary, non-human studies, and non-English publications
Inconsistencies in identifying relevant studies were deliberated to reach an agreement. A pre-specified EXCEL sheet (Microsoft, Redmond, CA, USA) was used for data extraction, including the study year, country, reported prevalence data, number of patients, and age brackets.
Two sets of reviewers (HS & AO and SS & EZ) evaluated the risk of bias in the included studies using the Newcastle-Ottawa Scale (NOS). The NOS was designed to assess the quality of non-randomized studies in meta-analyses (9). The NOS uses a star system to assess various aspects of the study, including the selection of study groups, comparability between groups, and choosing the outcome of interest in cohort studies. Each criterion can be given one star within the “selection” and “outcome” categories, whereas comparability can receive up to two stars. Individual study quality and risk of bias were assessed using the approach described by Ribeiro et al. (10). Studies with a total score of ≥7, 6, or ≤5 were considered to have a low, medium, and high risk of bias, respectively.
A meta-analysis of proportions was conducted on the FI prevalence data from the included publications using the “Meta-prop” function in the RStudio software (Posit, Boston, MA, USA). Forest plots were created using the “forest” function of the software. Furthermore, to account for the variation in age ranges within the study sample populations and to minimize heterogeneity in the meta-analysis, subgroup analyses were performed for FI prevalence in men and women, excluding studies that did not report data for all ages above 20 years.
To determine the number of patients with FI in Canada, we applied the pooled prevalence derived from the meta-analysis to Canadian population data stratified by age, sex, and province using the current Statistics Canada demographic data (Supplementary Table S2) (11). Additionally, the pooled prevalence was applied to the latest population estimate in the ten most populous countries worldwide to estimate the number of people suffering from FI. The methodology and characteristics of the included studies are summarized in the Supplementary Material (Supplementary Table S3). All data are available in the text and Supplementary Material. Details are available upon request from the corresponding author.
Thirty-two studies were included in this analysis. Thirteen were from North America (12–24), one from South America (25), ten from Europe (2, 26–34), two from the Middle East (35, 36), three from Asia (37–39), and Australia (40–42). The sample size of included articles ranges from a minimum of 128 to a maximum of 42,796. The Median and Mean sample sizes were 749 and 3,398, respectively. Twenty studies provided data on both sexes, and 12 studies were only on females (Table 1). All studies were cross-sectional, and the surveys were administered online or in person. Only three studies were longitudinal surveys (22, 24, 25).
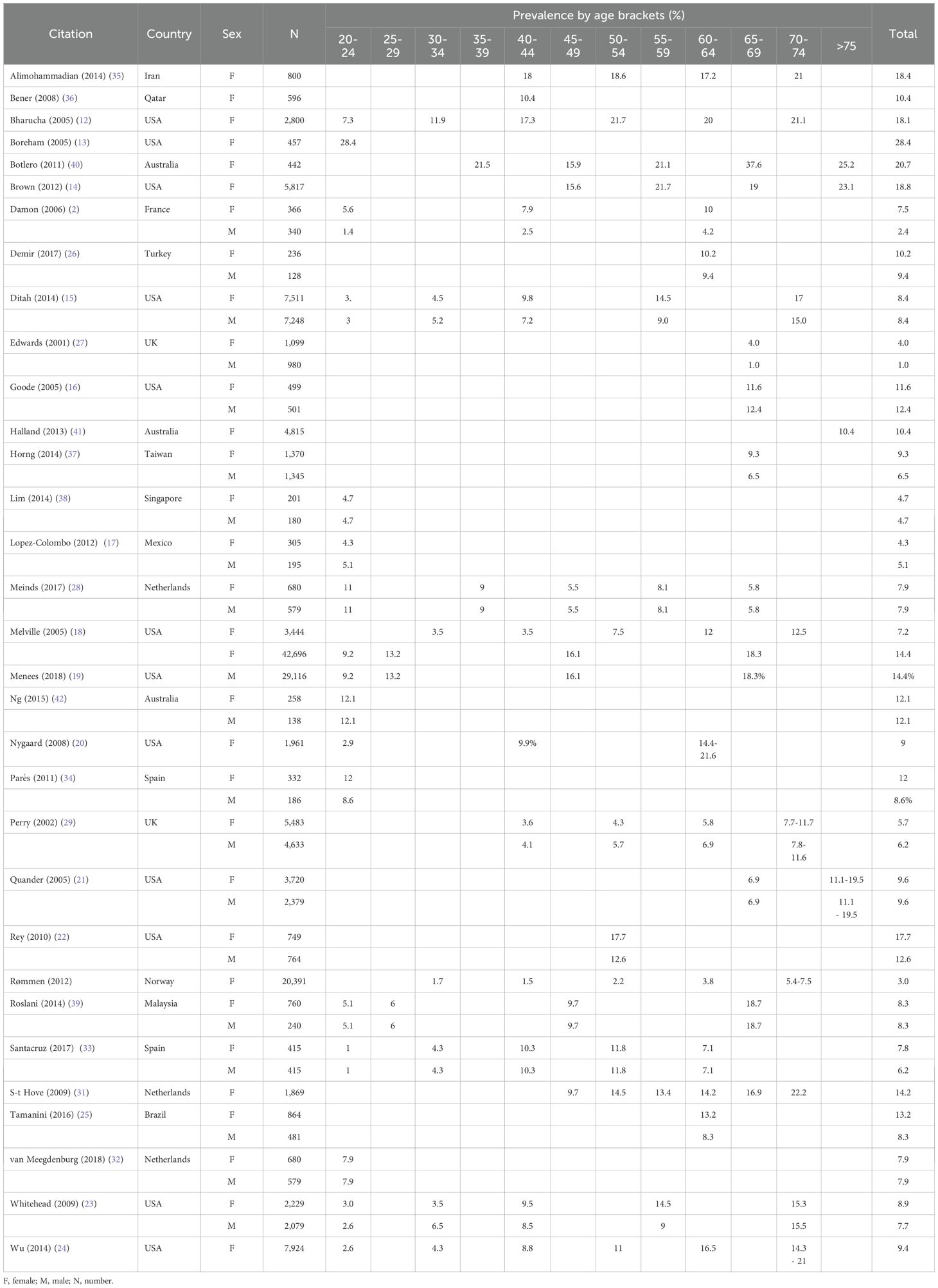
Table 1. Studies that reported the prevalence of fecal incontinence (percentage by age bracket).
The Mean pooled prevalence of FI in men and women was 7% (95% CI: 6–9%) and 10% (95% CI: 8–12%), respectively (Figure 2). The sub-analysis mean pooled prevalence for FI in men and women was 8% (95% CI: 6–10%) and 10% (95% CI: 8–12%), respectively (Supplementary Figure S1).
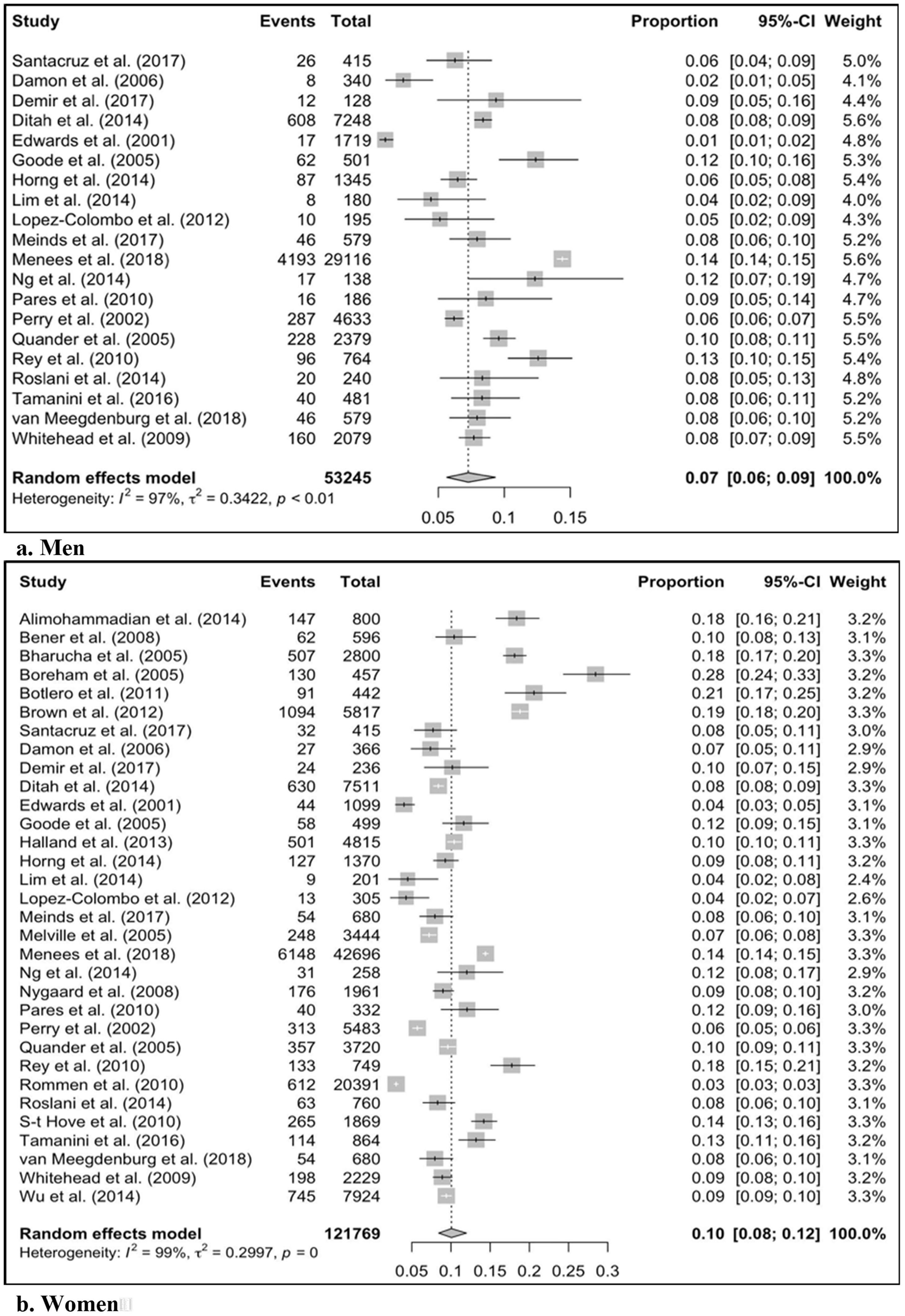
Figure 2. The pooled prevalence for fecal incontinence in men and women. CI, Confidence Interval.
All the included studies had a low risk of bias. The mean NOS score of the studies was 7.7 out of 9, with a range of 7.5 - 9 (Supplementary Table S4).
The pooled meta-analysis data indicated that 6–10% of men and 8–12% of women over 20 years of age have experienced FI. Thus, we estimate that between 1 and 1.5 million people suffer from FI in Canada (Table 2).
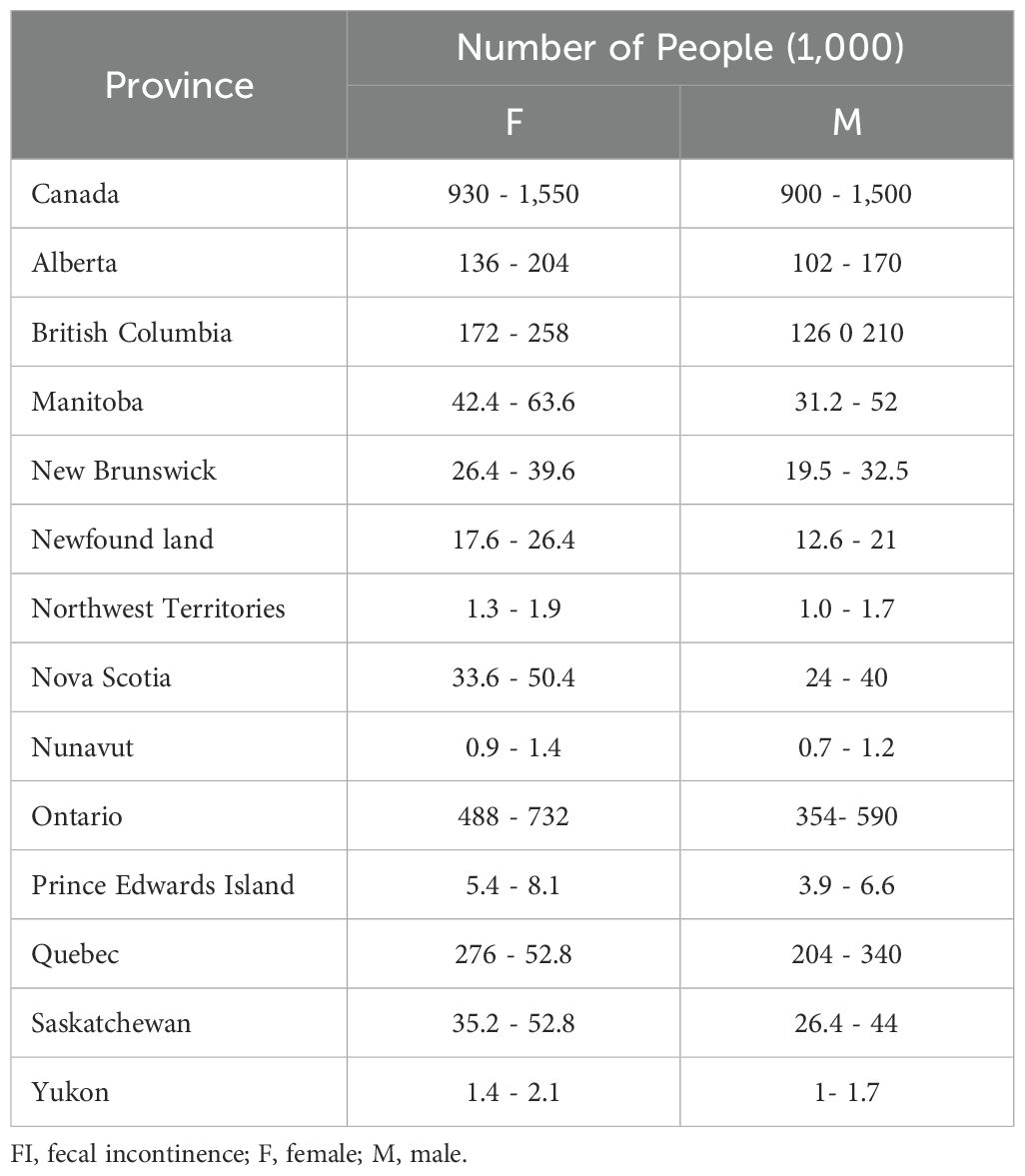
Table 2. Estimated number of people in Canada with fecal incontinence by province.
Moreover, we extrapolated the pooled prevalence of FI to the ten most populous countries worldwide to assess FI’s global impact of FI. We estimated that between 320 million and 500 million people suffer from FI in these countries (Table 3).
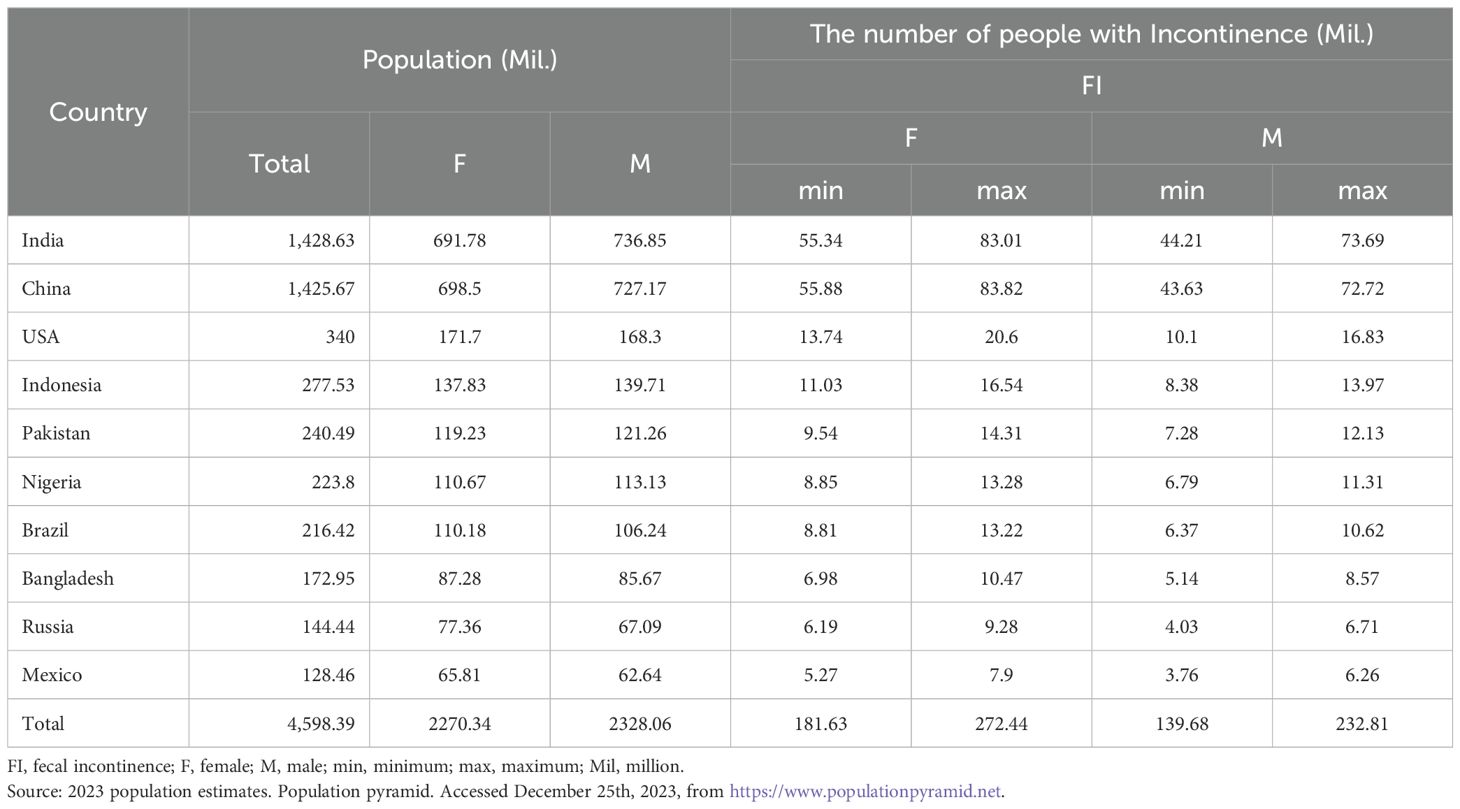
Table 3. Estimates of fecal incontinence in the ten most populous countries.
Considering the grave impact of FI on a patient’s QoL, treatment with FI can profoundly affect a patient’s well-being. Various pharmacological and non-pharmacological treatments are available for FI, including behavioral therapies (e.g., dietary modifications and bowel retraining), physical therapies (e.g., biofeedback), anti-diarrheal medications, padding, and mechanical inserts (e.g., plugs) (43). Surgical options (e.g., artificial bowel sphincter) are considered for unresponsive patients who lack long-term success (7).
Another viable option is sacral neuromodulation (SNM), a minimally invasive procedure that restores neural communication between the brain and bowel, making it an effective therapy for FI. This therapy uses a small lead surgically implanted adjacent to the sacral nerve and stimulates the nerve using electrical currents originating from an implanted pulse generator. Initially, patients undergo a peripheral nerve evaluation (PNE), an indicator of treatment response. In responsive patients who receive a permanent implant, 92% achieve significant symptom remission after six months (43–45). The aforementioned surgical treatments for FI have up to 40% morbidity, while SNM complications occur in up to 20% of patients and primarily involve localized pain at the site of the PNE or implant (7, 43).
This systematic review and meta-analysis pooled international data to estimate fecal incontinence prevalence. Our results demonstrated a 7% and 10% pooled prevalence of FI in men and women, respectively. To our knowledge, this is the first study attempting to infer sex-stratified FI based on prevalence data of FI in individuals aged > 20 years in Canada. The Canadian FI prevalence by sex and province was estimated by overlaying the pooled prevalence in the Canadian provincial population data.
Our results are comparable with those of Whitehead et al., who reported that 17.6% of Canadians had experienced at least one FI symptom, although they did not specify the symptom or differentiate the prevalence between the sexes (23). The Canadian Incontinence Foundation estimates that 5% of the non-hospitalized population, 1% of those under 65 years, and 4%–7% of those over 65 years are afflicted by FI, while the data from international surveys on FI range from 7% to 12% (28). Our study results were aligned with other studies that reported a prevalence of 9.1% and 7.6% for women and men, respectively (19).
Some of the data differences can be attributed to the variations among clinical definitions of FI (e.g., frequency and elapsed time of involuntary stool) and questionnaires on FI. Whitehead found that, while 16% of their sample reported at least one FI symptom, 7% and 3.3% met the Rome III and Rome IV criteria, respectively (23). Another variation between studies was the time intervals, spanning from a week to a lifetime, which could result in different prevalence. The 2015 US National Gastrointestinal Survey found that 14.4% of the respondents had lifetime experience with FI. However, only 4.7% of the patients had FI within the last seven days (19).
In this study, we did not conduct an age-adjusted meta-analysis because comprehensive data for each age group were unavailable. However, consistent with previous studies, we observed a trend of increasing FI rate with age (19).
Furthermore, sub-analyses using published data for individuals over 20 years of age demonstrated no change in the FI rate. We expected a lower pooled proportion value because studies with the same sample populations and greater risk for such conditions were excluded. Menees et al. reported a higher lifetime prevalence for those over 20 years of age, and Horng et al. reported a lower one-year prevalence for those over 65 (19, 37).
The current study focused on sex-specific FI prevalence to increase physicians’ and patients’ awareness. The results of this study showed a slightly higher prevalence of FI in women than in men. In contrast, other studies have not found a significant difference between the sexes (23). Women are likely to be more susceptible to FI because of factors such as childbirth trauma and being prone to irritable bowel syndrome (44). It is also possible that our results have been skewed due to the higher willingness of women to report FI symptoms compared to men (46).
Due to the stigma and unawareness, FI is underreported and underdiagnosed. Additionally, the subjective nature of assessment tools used for FI diagnosis would cause substantial variability in diagnosis, making assessing the actual prevalence of FI through a large-scale nationwide study impractical (4).
The ramifications of FI underreporting and a lack of awareness in clinical practice are multifold. First, eligible patients may not have received timely and appropriate care. In addition, many patients with FI may not be referred to specialized centers for more advanced and cost-effective therapies (e.g., SNM) (47). The high prevalence of FI emphasizes the need to diagnose patients using standardized criteria proactively. Particularly in Canada, with a growing aging population, we expect an increase in FI prevalence, an increasing financial burden, and a declining QoL (19).
Additionally, this study considered data from the English language publications. Although this might be considered a limitation and potentially skew the data, studies have shown the impact of social constructs, beliefs, language, and wording in the diagnosis and scoring tools. Consequently, we believe these inclusion criteria are justified and aligned with the study goal.
This study estimated the number of patients with FI by sex in Canada. Based on the quintuple healthcare framework, achieving optimal outcomes at a reasonable cost with flexibility for professional judgment requires appropriate and timely planning that reflects demographic changes (48). These data are critical for FI, an underreported and stigmatized disease (49).
Patients with unmonitored FI are likely to suffer from comorbidities, increasing the burden on the individual and the healthcare system (50). Thus, interventions with effective treatments and strategies can help reduce the burden of healthcare resource utilization. Furthermore, measures that improve efficiency by reducing healthcare and hospital resources or long-term complications may be implemented to help leaders and hospital managers optimize their offerings within budget constraints. In this study, we provide an example of an opportunity in which the prevalence of the disease in the general population is presented. Similar opportunities may aid healthcare leaders and decision-makers in optimizing care delivery based on patient outcomes and values. Collectively, and over time, such policies can improve the efficiency of healthcare delivery more comprehensively for different therapy areas (51).
The results of this study should be considered within the limitations. First, the methodology for data collection, sampling, clinical measures, and timelines varied across studies. The heterogeneity of the data required a random-effects meta-analysis model in our study. The varied methodology might account for some of the reported differences in the prevalence data. Varying clinical measures between studies led to different item scores, wording, and response formats.
Rømmen et al. employed a more stringent criterion, considering an FI diagnosis only if participants reported experiencing at least one occurrence of FI per week over the past month, resulting in an overall prevalence of 3% (30). In contrast, the study by Lim et al., which utilized in-person interviews for data collection, reported an overall prevalence of 4.7%, while the study by Bharucha et al., which employed a mailed questionnaire, found an overall prevalence of 18.1% (12, 38). This divergence in findings may be attributed to individuals experiencing embarrassment or hesitation to discuss their symptoms during face-to-face interviews.
The analyzed studies were also heterogeneous in data collection using self-administered questionnaires, in-person reviews, remote (online and telephone) surveys, and variable settings (e.g., clinics, hospitals, or private residences). The sampling methods and populations differed (e.g., random sampling or the general population). Further research on the current prevalence of FI in the Canadian population is warranted. Widespread population-based surveys that utilize consistent diagnostic criteria and sampling methodologies, as well as electronic health record data to estimate the number of patients with FI, could substantiate our findings, better estimate SNM candidates, and raise awareness of the importance of this treatment.
Fecal incontinence is prevalent among men and women, but it is underdiagnosed and underreported, and requires more attention to improve patient quality of life.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
AO: Data curation, Investigation, Software, Validation, Writing – original draft, Writing – review & editing, Formal Analysis. DE: Conceptualization, Writing – review & editing. SS: Investigation, Writing – review & editing. EZ: Data curation, Investigation, Writing – review & editing. PP: Writing – review & editing. BC: Investigation, Writing – review & editing. HS: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Software, Supervision, Validation, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial was received for the research, authorship, and/or publication of this article.
HS and PP are employees of Medtronic, the manufacturer of sacral neuromodulation technology. DE has conducted research and received speaker and consultant honoraria from Medtronic.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fgstr.2024.1398102/full#supplementary-material
1. Whitehead WE, Simren M, Busby-Whitehead J, Heymen S, van Tilburg MAL, Sperber AD, et al. Fecal incontinence diagnosed by the Rome IV criteria in the United States, Canada, and the United Kingdom. Clin Gastroenterol Hepatol. (2020) 18:385–91. doi: 10.1016/j.cgh.2019.05.040
2. Damon H, Guye O, Seigneurin A, Long F, Sonko A, Faucheron J-L, et al. Prevalence of anal incontinence in adults and impact on quality-of-life. Gastroentérologie Clinique Biologique. (2006) 30:37–43. doi: 10.1016/S0399-8320(06)73076-7
3. Rosato-Scott C, Barrington DJ, Bhakta A, House SJ, Mactaggart I, Wilbur J. How to Talk About Incontinence: A Checklist. Brighton, UK: Institute of Development Studies (IDS) (2020). doi: 10.19088/SLH.2020.006
4. Whitehead WE, Palsson OS, Simren M. Treating fecal incontinence: an unmet need in primary care medicine. N C Med J. (2016) 77:211–5. doi: 10.18043/ncm.77.3.211
5. Meyer I, Richter HE. Impact of fecal incontinence and its treatment on quality of life in women. Womens Health (Lond). (2015) 11:225–38. doi: 10.2217/whe.14.66
6. Corcos J, Schick E. Prevalence of overactive bladder and incontinence in Canada. Can J Urol. (2004) 11:2278–84.
7. Thaha MA, Abukar AA, Thin NN, Ramsanahie A, Knowles CH. Sacral nerve stimulation for faecal incontinence and constipation in adults. Cochrane Database Systematic Rev. (2015) 2015. doi: 10.1002/14651858.CD004464.pub3. Cochrane Incontinence Group, editor.
8. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021), 10(1):n71. doi: 10.1136/bmj.n71
9. Wells G, Shea B, O’Connell D, Peterson J, Welch V, Losos M, et al. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Ottawa, Canada: The Ottawa Hospital Research Institute. Available at: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp.
10. Ribeiro CM, Beserra BTS, Silva NG, Lima CL, Rocha PRS, Coelho MS, et al. Exposure to endocrine-disrupting chemicals and anthropometric measures of obesity: a systematic review and meta-analysis. BMJ Open. (2020) 10:e033509. doi: 10.1136/bmjopen-2019-033509
11. Statistics Canada. (2023). Population estimates on July 1st, by age and sex. Ottawa, Canada: Government of Canada. doi: 10.25318/1710000501-ENG
12. Bharucha AE. Relationship between symptoms and disordered continence mechanisms in women with idiopathic faecal incontinence. Gut. (2005) 54:546–55. doi: 10.1136/gut.2004.047696
13. Boreham MK, Richter HE, Kenton KS, Nager CW, Gregory WT, Aronson MP, et al. Anal incontinence in women presenting for gynecologic care: Prevalence, risk factors, and impact upon quality of life. Am J Obstetrics Gynecology. (2005) 192:1637–42. doi: 10.1016/j.ajog.2004.11.030
14. Brown HW, Wexner SD, Segall MM, Brezoczky KL, Lukacz ES. Accidental bowel leakage in the mature women’s health study: prevalence and predictors: Accidental bowel leakage: prevalence and predictors. Int J Clin Practice. (2012) 66:1101–8. doi: 10.1111/ijcp.12018
15. Ditah I, Devaki P, Luma HN, Ditah C, Njei B, Jaiyeoba C, et al. Prevalence, trends, and risk factors for fecal incontinence in United States adults, 2005–2010. Clin Gastroenterol Hepatology. (2014) 12:636–43.e2. doi: 10.1016/j.cgh.2013.07.020
16. Goode PS, Burgio KL, Halli AD, Jones RW, Richter HE, Redden DT, et al. Prevalence and correlates of fecal incontinence in community-dwelling older adults: FECAL INCONTINENCE IN OLDER ADULTS. J Am Geriatrics Society. (2005) 53:629–35. doi: 10.1111/j.1532-5415.2005.53211.x
17. López-Colombo A, Morgan D, Bravo-González D, Montiel-Jarquín A, Méndez-Martínez S, Schmulson M. The epidemiology of functional gastrointestinal disorders in Mexico: A population-based study. Gastroenterol Res Practice. (2012) 2012:1–8. doi: 10.1155/2012/606174
18. Melville JL, Fan M-Y, Newton K, Fenner D. Fecal incontinence in US women: A population-based study. Am J Obstetrics Gynecology. (2005) 193:2071–6. doi: 10.1016/j.ajog.2005.07.018
19. Menees SB, Almario CV, Spiegel BMR, Chey WD. Prevalence of and factors associated with fecal incontinence: results from a population-based survey. Gastroenterology. (2018) 154:1672–81.e3. doi: 10.1053/j.gastro.2018.01.062
20. Nygaard I. Prevalence of symptomatic pelvic floor disorders in US women. JAMA. (2008) 300:1311. doi: 10.1001/jama.300.11.1311
21. Quander CR, Morris MC, Melson J, Bienias JL, Evans DA. Prevalence of and factors associated with fecal incontinence in a large community study of older individuals. Am J Gastroenterology. (2005) 100:905–9. doi: 10.1111/j.1572-0241.2005.30511.x
22. Rey E, Choung RS, Schleck CD, Zinsmeister AR, Locke RG, Talley NJ. Onset and risk factors for fecal incontinence in a US community. Am J Gastroenterology. (2010) 105:412–9. doi: 10.1038/ajg.2009.594
23. Whitehead WE, Borrud L, Goode PS, Meikle S, Mueller ER, Tuteja A, et al. Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology. (2009) 137:512–17.e2. doi: 10.1053/j.gastro.2009.04.054
24. Wu JM, Vaughan CP, Goode PS, Redden DT, Burgio KL, Richter HE, et al. Prevalence and trends of symptomatic pelvic floor disorders in U.S. Women. Obstetrics Gynecology. (2014) 123:141–8. doi: 10.1097/AOG.0000000000000057
25. Tamanini JTN, de Jesus FA, Castro RA, Ferreira Sartori MG, Castello Girão MJB, dos Santos JLF, et al. The prevalence of fecal incontinence and associated risk factors in older adults participating in the SABE study: The Prevalence of Fecal Incontinence Among Older Adults: The SABE Study. Neurourol Urodynam. (2016) 35:959–64. doi: 10.1002/nau.22836
26. Demir N, Yuruyen M, Atay K, Yavuzer H, Hatemi I, Doventas A, et al. Prevalence of fecal incontinence and associated risk factors in elderly outpatients: a cross-sectional study. Aging Clin Exp Res. (2017) 29:1165–71. doi: 10.1007/s40520-017-0723-x
27. Edwards NI. The prevalence of faecal incontinence in older people living at home. Age Ageing. (2001) 30:503–7. doi: 10.1093/ageing/30.6.503
28. Meinds RJ, van Meegdenburg MM, Trzpis M, Broens PMA. On the prevalence of constipation and fecal incontinence, and their co-occurrence, in the Netherlands. Int J Colorectal Dis. (2017) 32:475–83. doi: 10.1007/s00384-016-2722-3
29. Perry S. Prevalence of faecal incontinence in adults aged 40 years or more living in the community. Gut. (2002) 50:480–4. doi: 10.1136/gut.50.4.480
30. Rømmen K, Schei B, Rydning A, H Sultan A, Mørkved S. Prevalence of anal incontinence among Norwegian women: a cross-sectional study. BMJ Open. (2012) 2:e001257. doi: 10.1136/bmjopen-2012-001257
31. Hove MCPh S-t, AL P-G, Eijkemans MJC, Steegers-Theunissen RPM, CW B, Vierhout ME. The prevalence of pelvic organ prolapse symptoms and signs and their relation with bladder and bowel disorders in a general female population. Int Urogynecol J. (2009) 20:1037–45. doi: 10.1007/s00192-009-0902-1
32. Meegdenburg MM, Trzpis M, Broens PM. Fecal incontinence and parity in the Dutch population: A cross-sectional analysis. United Eur Gastroenterol J. (2018) 6:781–90. doi: 10.1177/2050640618760386
33. Cerdán Santacruz C, Santos Rancaño R, Vigara García M, Fernández Pérez C, Ortega López M, Cerdán Miguel J. Prevalence of anal incontinence in a working population within a healthcare environment. Scandinavian J Gastroenterology. (2017) 52:1340–7. doi: 10.1080/00365521.2017.1378713
34. Parés D, Vial M, Bohle B, Maestre Y, Pera M, Roura M, et al. Prevalence of faecal incontinence and analysis of its impact on quality of life and mental health: Faecal incontinence in primary care. Colorectal Disease. (2011) 13:899–905. doi: 10.1111/j.1463-1318.2010.02281.x
35. Alimohammadian M, Ahmadi B, Janani L, Mahjubi B. Suffering in silence: a community-based study of fecal incontinence in women. Int J Colorectal Dis. (2014) 29:401–6. doi: 10.1007/s00384-013-1809-3
36. Bener A, Saleh N, Burgut FT. Prevalence and determinants of fecal incontinence in premenopausal women in an Arabian community. Climacteric. (2008) 11:429–35. doi: 10.1080/13697130802241519
37. Horng S-S, Chou Y-J, Huang N, Fang Y-T, Chou P. Fecal incontinence epidemiology and help seeking among older people in Taiwan: FI Epidemiology and Help Seeking. Neurourol Urodynam. (2014) 33:1153–8. doi: 10.1002/nau.22462
38. Lim W, Heng C, Wong M, Tang C. Prevalence of faecal incontinence in the community: a cross-sectional study in Singapore. smedj. (2014) 55:640–3. doi: 10.11622/smedj.2014177
39. Roslani AC, Ramakrishnan R, Azmi S, Arapoc DJ, Goh A. Prevalence of faecal incontinence and its related factors among patients in a Malaysian academic setting. BMC Gastroenterol. (2014) 14:95. doi: 10.1186/1471-230X-14-95
40. Botlero R, Bell RJ, Urquhart DM, Davis SR. Prevalence of fecal incontinence and its relationship with urinary incontinence in women living in the community. Menopause. (2011) 18:685–9. doi: 10.1097/gme.0b013e3181fee03b
41. Halland M, Koloski NA, Jones M, Byles J, Chiarelli P, Forder P, et al. Prevalence correlates and impact of fecal incontinence among older women. Dis Colon Rectum. (2013) 56:1080–6. doi: 10.1097/DCR.0b013e31829203a9
42. Ng K -S, Nassar N, Hamd K, Nagarajah A, Gladman MA. Prevalence of functional bowel disorders and faecal incontinence: an Australian primary care survey. Colorectal Dis. (2015) 17:150–9. doi: 10.1111/codi.12808
43. Hetzer FH. Quality of life and morbidity after permanent sacral nerve stimulation for fecal incontinence. Arch Surg. (2007) 142:8. doi: 10.1001/archsurg.142.1.8
44. Desprez C, Damon H, Meurette G, Mege D, Faucheron J-L, Brochard C, et al. Ten-year evaluation of a large retrospective cohort treated by sacral nerve modulation for fecal incontinence: results of a French multicenter study. Ann Surgery. (2022) 275:735–42. doi: 10.1097/SLA.0000000000004251
45. Tjandra JJ, Chan MKY, Yeh CH, Murray-Green C. Sacral Nerve Stimulation is more Effective than Optimal Medical Therapy for Severe Fecal Incontinence: A Randomized, Controlled Study. Dis Colon Rectum. (2008) 51:494–502. doi: 10.1007/s10350-007-9103-5
46. Pretlove SJ, Radley S, Toozs-Hobson PM, Thompson PJ, Coomarasamy A, Khan KS. Prevalence of anal incontinence according to age and gender: a systematic review and meta-regression analysis. Int Urogynecol J. (2006) 17:407–17. doi: 10.1007/s00192-005-0014-5
47. Hassouna MM, Sadri H. Economic evaluation of sacral neuromodulation in overactive bladder: A Canadian perspective. CUAJ. (2015) 9:242. doi: 10.5489/cuaj.2711
48. Nundy S, Cooper LA, Mate KS. The quintuple aim for health care improvement: A new imperative to advance health equity. JAMA. (2022) 327:521. doi: 10.1001/jama.2021.25181
49. Turan JM, Elafros MA, Logie CH, Banik S, Turan B, Crockett KB, et al. Challenges and opportunities in examining and addressing intersectional stigma and health. BMC Med. (2019) 17:7. doi: 10.1186/s12916-018-1246-9
50. Von Gontard A, Baeyens D, Van Hoecke E, Warzak WJ, Bachmann C. Psychological and psychiatric issues in urinary and fecal incontinence. J Urology. (2011) 185:1432–7. doi: 10.1016/j.juro.2010.11.051
Keywords: systematic review, fecal incontinence, prevalence, meta-analysis, population estimate
Citation: Oliaei A, Elterman D, Sadri S, Zimmerman E, Pezeshki P, Chughtai B and Sadri H (2024) Estimating the number of Canadians suffering from fecal incontinence using pooled prevalence data from meta-analysis. Front. Gastroenterol. 3:1398102. doi: 10.3389/fgstr.2024.1398102
Received: 08 March 2024; Accepted: 12 August 2024;
Published: 03 September 2024.
Edited by:
Danny Con, University of Melbourne, AustraliaReviewed by:
Diego Sánchez Muñoz, Instituto Digestivo, SpainCopyright © 2024 Oliaei, Elterman, Sadri, Zimmerman, Pezeshki, Chughtai and Sadri. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hamid Sadri, SGFtaWQuc2FkcmlAbWFpbC51dG9yb250by5jYQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.