
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Gastroenterol., 01 November 2023
Sec. Gastrointestinal Infection
Volume 2 - 2023 | https://doi.org/10.3389/fgstr.2023.1270899
This article is part of the Research TopicGut Microbiota in Health and DiseaseView all 19 articles
 Rita Silva1,2
Rita Silva1,2 Liliana Dinis1,2,3Arnau Peris2Luís Novais4
Liliana Dinis1,2,3Arnau Peris2Luís Novais4 Conceição Calhau1Diogo Pestana1,2
Conceição Calhau1Diogo Pestana1,2 Cláudia Marques1,2*
Cláudia Marques1,2*Fecal microbiota transplantation (FMT) is indicated in many countries for patients with multiple recurrences of Clostridioides difficile infection (CDI) for whom appropriate antibiotic treatments have failed. Donor selection is a demanding and rigorous process in view of the implementation of FMT programs worldwide. One of the most noteworthy factors that has been shown to affect FMT outcomes is the microbial diversity of the stool donor. A detailed assessment of the donor’s microbiota is crucial, as the microbiota is complex, dynamic, and resilient, and a healthy microbiota has several dimensions in addition to the absence of pathogens. Diet is one of the most important factors that modulates the composition and function of the gut microbiome (GM) and has a critical role in orchestrating the host–microbiota crosstalk throughout life. The diversity of the human GM seems to be related to variations in dietary patterns. Currently, the dietary patterns of stool donors and receptors are not taken into consideration in any way for FMT. In this study, we reflect on the importance of including this type of assessment in the stool donor screening process and knowing the impact of diet on the GM, as well as the importance of monitoring receptors’ diet to ensure the engraftment of the transplanted microbiota.
The gut microbiome encodes over 3 million genes, whereas the human genome consists of approximately 23,000 genes (1). Therefore, the metabolic capacity of the gut microbiome greatly exceeds the metabolic capacity of human cells (2). The gut microbiota (GM) has a crucial role in the maintenance of health, with protective, structural, and metabolic functions (3). An imbalance in its composition and function (dysbiosis) has been associated with many disorders (4), including Clostridioides difficile infections (CDIs).
Fecal microbiota transplantation (FMT) was first described in the fourth century by the traditional Chinese medicine doctor Ge Hong (5), but it was only in 1983 that Schwan et al. published the first report of a successful treatment with FMT for CDI, through retention enema (6). Currently, FMT is an established treatment for recurrent CDI (7, 8), but it also seems promising as a therapy for many other disorders (9).
FMT is a procedure in which the fecal microbial content from a healthy donor is administered into another patient’s intestinal tract, with the aim of treating a certain disease linked with the alteration of the GM (10). FMT can be performed through the upper gastrointestinal tract (GIT), via a duodenal tube or capsules taken orally, or through the lower GIT, via colonoscopy or an enema (9) (Figure 1).
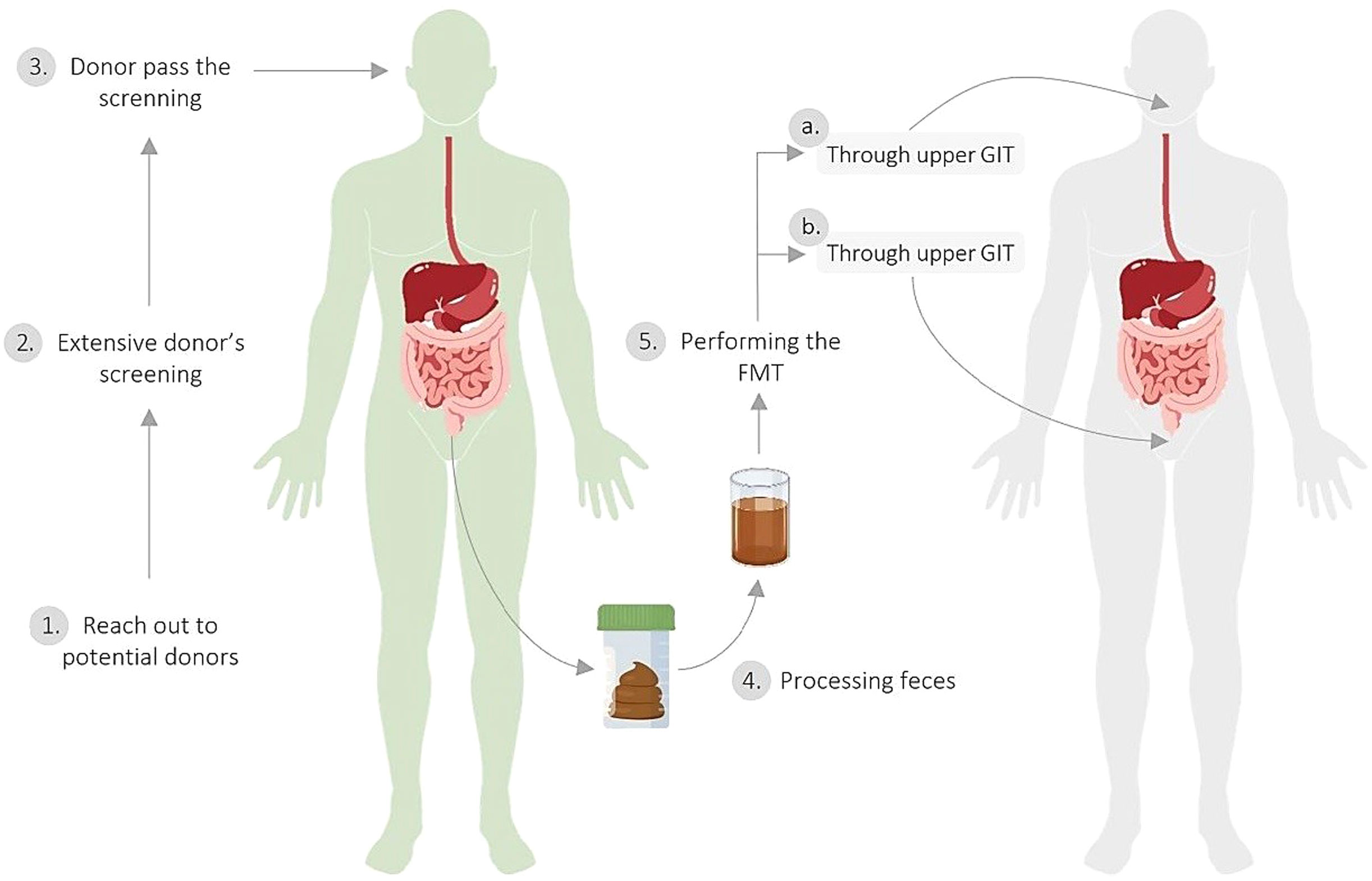
Figure 1 Fecal microbiota transplantation process. 1. Recruitment of potential healthy donors through media and advertising. 2. Extensive donor screening for medical history, infectious diseases, intestinal health, and risk behaviors; blood and stool testing; and screening of stool and stool donors for the presence of SARS-CoV-2 infection. 3. Donor passes the screening. 4. Processing feces through dilution (with 0.9% NaCl) and filtration to obtain microbiota. 5. Performing the FMT (A) through the upper GIT, through a duodenal tube or capsules taken orally or (B) through the lower GIT, through colonoscopy or an enema. The image is an adaptation of Bou Zerdan M. et al. (11), Alabdaljabar et al. (12), and Ooijevaar et al. (9).
FMT is indicated in many countries (7, 8) for patients with multiple recurrences of CDI for whom appropriate antibiotic treatments have failed (7), and it has cure rates of 80%–90% (13). In addition, it seems promising as a treatment for many other conditions (9). FMT has been studied in inflammatory bowel disease (14), obesity, and metabolic syndrome (15). FMT also seems promising in oncology (16), it might be useful in the prevention and treatment of psychiatric illnesses (17), and has the potential to treat Alzheimer’s and Parkinson’s diseases (18). More recently, it has been proposed as a potential treatment for COVID-19 (19).
Donor selection is a demanding and rigorous process in view of the implementation of FMT programs worldwide (20). In fact, choosing the right donor could be challenging in clinical practice because of the absence of a clear definition of a healthy GM, and because of the complexity of the host response (such as the immune response) and dietary habits (2).
Potential stool donors should undergo a detailed questionnaire including medical history, infectious diseases, intestinal health, and risk behaviors (21). They should also undergo blood and stool tests to prevent the direct transmission of infectious diseases and avoid transferring an adverse microbiota profile that could possibly increase the risk of the receptor developing other diseases related to an abnormal GM (21, 22).In addition, the US Food and Drug Administration (FDA) has recommended, since March 2020, the screening of stool and stool donors for the presence of SARS-CoV-2 infection (23).
In recent years, the debate about stool donor screening has become deeper. In fact, donors whose stool results in substantially more successful FMT outcomes than the stool of other donors have been described as “super-donors” (24). One of the most noteworthy factors that has been shown to affect FMT outcomes is the microbial diversity of the stool donor (25).
In addition, the stool receptors’ follow-up is focused on the side effects or complications of FMT in the short term (10, 21), and their long-term follow-up includes only the documentation of clinical details and relevant clinical results beyond the first 24 h (21). It does not take into consideration what the receptor should do to keep the transplanted microbiota in balance.
The gut microbiome is complex, dynamic, and resilient, as any biological system (26), and a healthy microbiota has several dimensions in addition to the absence of pathogens. So it is hard to define what a healthy human GM at an exact taxonomic level (27). However, a high level of taxa diversity, a high level of microbial gene richness, and stable microbiome functional cores indicate healthy GM communities (28).
It has been demonstrated that low levels of bacterial gene richness leads to increased adiposity, insulin resistance and dyslipidemia, and a further pronounced inflammatory phenotype (2), indicating the impact of GM on metabolic processes. Besides, an increasing number of diseases are linked with intestinal dysbiosis, such as metabolic, cardiovascular, and neurologic diseases (4), and pathologies such as inflammatory bowel (29) and autoimmune diseases (30). Individuals with these pathologies should not be stool donors, to prevent the transmission of a dysbiotic microbiota that could itself cause the disease in the receptor. Furthermore, donors are excluded based on disease, as we assume that because they have the disease they have an altered GM, but a question remains unanswered: what about those who already have an altered GM and do not have the pathology yet? We propose that the exclusion of these types of donors start to be considered.
Diet is one of the most important factors that modulates the composition and function of the GM and has a crucial role in orchestrating the host–microbiota crosstalk throughout life (31).
What we eat is a key factor in the composition of the GM, as diet is thought to explain about 20% of microbial structural variations in humans, indicating the ability of dietary approaches to aid in disease management through GM modulation (32). The integration between the GM, food groups, and short-chain fatty acid (SCFA)-producing bacteria is promising in the quest to further upgrade and transform dietary habits (33).
A diverse diet, especially in the number of different types of plant foods eaten, has been linked with greater microbial alpha-diversity, and is thought to enhance the diversity of substrates for the proliferation of numerous taxa (32). The interactions between diet and the GM are described in Figure 2.
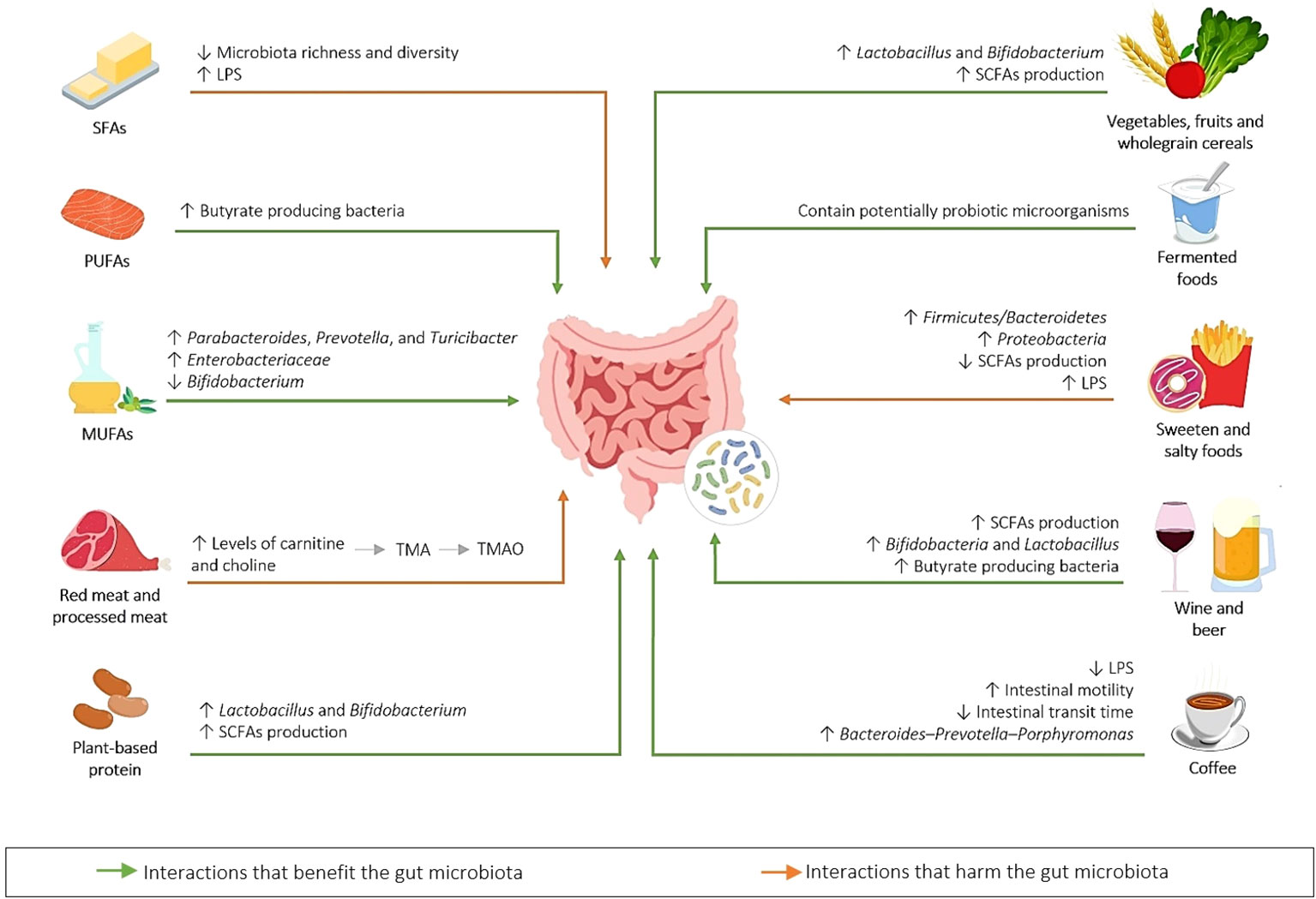
Figure 2 Gut microbiota–diet interactions. Common dietary components are metabolized by the GM to produce metabolites (for example, red and processed meat, containing high levels of carnitine and choline, both of which are precursors that the gut bacteria use to produce trimethylamine (TMA), which is converted by the enzyme flavin-containing monooxygenase 3 (FMO3) into trimethylamine N-oxide (TMAO) (34), that has been associated with atherosclerosis). A diet rich in saturated fatty acids (SFAs), sweet and salty foods modify the GM, causing elevated levels of lipopolysaccharides (LPSs) in the circulation, leading to a pro-inflammatory state (metabolic endotoxemia) (35). Some foods have a positive effect on the GM, for example, those that elevate short-chain fatty acid (SCFA) production and the abundance of Lactobacillus and Bifidobacterium (34), and those that are included in the Mediterranean diet, such as olive oil (35). Fermented foods (36), wine and beer (37), and coffee (38) consumption also have a positive effect on the GM composition. SFA, saturated fatty acid; MUFA, monounsaturated fatty acid; PUFA, polyunsaturated fatty acid; LPS, lipopolysaccharide; SCFA, short-chain fatty acid; TMA, trimethylamine; TMAO, trimethylamine N-oxide.
The diversity of the human GM seems to be related to variations in dietary patterns (39). In fact, several studies have demonstrated the ability of the Mediterranean diet (MD) to modulate the GM and host’s health (40–42). The MD is characterized by a high level of polyphenol-rich product content (extra-virgin olive oil, red wine, vegetables, grains, legumes, whole-grain cereals, and nuts), a positive fatty acid profile [high levels of monounsaturated fatty acids (MUFAs) and polyunsaturated fatty acids (PUFAs), and low levels of saturated fatty acids (SFAs)], and a low intake of processed meat and refined sugars (43). Adherence to the MD was found to be related to increased levels of SCFAs (acetate, propionate, butyrate, and lactate) (3, 42), Prevotella, and fiber-degrading Firmicutes (44, 45). It is worth mentioning that SCFAs are used as energy sources and participate in numerous metabolic pathways, including gluconeogenesis and lipogenesis, hence contributing to whole-body energy homeostasis (2). The MD has also been linked to improvements in the diversity and richness of the GM (35). Conversely, the Western diet, high in total fat, animal proteins, processed food, refined sugars, and food additives, leads to a dysbiosis in GM composition and is connected with obesity and other metabolic disorders (35).
Currently, the dietary patterns of stool donors and receptors are not taken into consideration in any guidance for FMT. In addition, no clinical practice recommendations are available to provide receptors or stool donors with dietary advice for FMT (46). Clancy et al. reported that, overall, health professionals and researchers who work with FMT reported that diet was a significant consideration for FMT receptors and donors, and that it would affect the outcomes of the FMT (46). Although they did not usually advise patients to see a dietitian/nutritionist before or after the FMT, and did not feel certain in giving dietary guidance, or that there was enough evidence to provide dietary counsel (46). Owing to the great contribution of diet to the composition and modulation of the GM (43), we consider it crucial to include this step in stool donor screening protocols, in order to guarantee the better quality of the transplanted microbiota and consequent benefits to the host. Moreover, the dietary follow-up of the stool receptors should also be taken into consideration, in order to guarantee the long-term efficiency of the FMT. This assumes a greater importance when FMT is intended to treat metabolic diseases. A study conducted by our group (data not published) showed—through the application of the Mediterranean Diet Adherence Screener (MEDAS) (47), a validated questionnaire to assess adherence to the MD—that only 55.6% (25 out of 45) of the potential stool donors had a level of high adherence (≥ 10) to the MD. These data suggest that the absence of chronic diseases may not be a suitable criterion for donor selection and that diet, as well as other lifestyle factors, should be evaluated to increase FMT efficiency and applicability in health. In addition, recent studies have demonstrated the importance of dietary habits, in particular fiber intake, in optimizing the success of FMT in the treatment of metabolic diseases (48–50). One study used autologous FMT to prolong the beneficial effect of a modified MD on weight regain. The findings of this study provided a provocative perspective where the co-supplementation of low-fermentable fiber may increase the potency of FMT (50). Mocanu et al. also provided a proof of concept for the use of a single-dose oral FMT combined with daily low-fermentable fiber supplementation to improve insulin sensitivity in patients with severe obesity and metabolic syndrome (49). Considering these data, would it not be important to evaluate and, if necessary, modify the dietary habits of the FMT receptor in future protocols?
Knowing the impact of diet on the GM, we propose that potential stool donors undergo dietary screening, to increase the probability of a beneficial and functional fecal microbiota being transplanted. We also believe that specific guidelines for stool receptors should be developed, mainly in the treatment of diseases other than CDI.
In addition, besides the inclusion of a dietary screening tool for the stool donor candidates it could be interesting to add nutrition counseling a few months prior to the stool donation in order to improve the quality of the stool donated, if necessary. Nutritionists could also enhance long-term FMT success by giving nutrition counseling services as part of multidisciplinary health care groups (51), as a healthy diet provides the commensal microbes with the substrates necessary for their proliferation and survival (24).
We hope to stimulate future research so that further information about dietary habits of FMT receptors and stool donors can be collected and thus make it possible to better understand the relationship between diet and FMT results. With this information, it would be possible to create a score for stool donors, where diet and other factors that modulate the GM are included. In fact, a validation study of a score of this kind would be interesting to assess whether or not those with the highest scores are, in fact, better donors.
The increased application of FMT in clinical practice will notably have a key impact on public health, as the prevalence of chronic diseases continues to increase. Therefore, the development of FMT protocols that honor this scientific evidence and promote the creation of more detailed screening and follow-up processes are of the utmost importance.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
RS: Writing – original draft. LD: Writing – review & editing. AP: Writing – review & editing. LN: Writing – review & editing. CC: Writing – review & editing. DP: Writing – review & editing. CM: Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work is supported by ERDF through the operation POCI-01–0145-ERDF-007746, funded by the Programa Operacional Competitividade e Internacionalização (COMPETE2020), and is financed by the Fundação para a Ciência e a Tecnologia, I.P. (FCT) through CINTESIS’s R&D Unit (UIDB/4255/2020).
CM, DP, CC, and LN are co-founders of YourBiome®, a spin-off of Universidade NOVA de Lisboa. LD and AP were YourBiome® employees under the project ALT20-03-02B7-FEDER-069744.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Valdes AM, Walter J, Segal E, Spector TD. Role of the gut microbiota in nutrition and health. Bmj (2018) 361:k2179. doi: 10.1136/bmj.k2179
2. Cani PD, Van Hul M, Lefort C, Depommier C, Rastelli M, Everard A. Microbial regulation of organismal energy homeostasis. Nat Metab (2019) 1(1):34–46. doi: 10.1038/s42255-018-0017-4
3. Prakash S, Rodes L, Coussa-Charley M, Tomaro-Duchesneau C. Gut microbiota: next frontier in understanding human health and development of biotherapeutics. Biologics (2011) 5:71–86. doi: 10.2147/BTT.S19099
4. Gebrayel P, Nicco C, Al Khodor S, Bilinski J, Caselli E, Comelli EM, et al. Microbiota medicine: towards clinical revolution. J Trans Med (2022) 20(1):111. doi: 10.1186/s12967-022-03296-9
5. Zhang F, Luo W, Shi Y, Fan Z, Ji G. Should we standardize the 1,700-year-old fecal microbiota transplantation? Am J Gastroenterol (2012) 107(11):1755. doi: 10.1038/ajg.2012.251
6. Schwan A, Sjölin S, Trottestam U, Aronsson B. Relapsing clostridium difficile enterocolitis cured by rectal infusion of homologous faeces. Lancet (1983) 2(8354):845. doi: 10.1016/S0140-6736(83)90753-5
7. McDonald LC, Gerding DN, Johnson S, Bakken JS, Carroll KC, Coffin SE, et al. Clinical practice guidelines for clostridium difficile infection in adults and children: 2017 update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). Clin Infect Dis (2018) 66(7):987–94. doi: 10.1093/cid/ciy149
8. Debast SB, Bauer MP, Kuijper EJ. European Society of Clinical Microbiology and Infectious Diseases: update of the treatment guidance document for Clostridium difficile infection. Clin Microbiol Infect (2014) 20 Suppl 2:1–26. doi: 10.1111/1469-0691.12418
9. Ooijevaar RE, Terveer EM, Verspaget HW, Kuijper EJ, Keller JJ. Clinical application and potential of fecal microbiota transplantation. Annu Rev Med (2019) 70:335–51. doi: 10.1146/annurev-med-111717-122956
10. Cammarota G, Ianiro G, Tilg H, Rajilić-Stojanović M, Kump P, Satokari R, et al. European consensus conference on faecal microbiota transplantation in clinical practice. Gut (2017) 66(4):569–80. doi: 10.1136/gutjnl-2016-313017
11. Bou Zerdan M, Niforatos S, Nasr S, Nasr D, Ombada M, John S, et al. Fecal microbiota transplant for hematologic and oncologic diseases: principle and practice. Cancers (2022) 14(3):691. doi: 10.3390/cancers14030691
12. Alabdaljabar MS, Aslam HM, Veeraballi S, Faizee FA, Husain BH, Iqbal SM, et al. Restoration of the original inhabitants: A systematic review on fecal microbiota transplantation for graft-versus-host disease. Cureus (2022) 14(4):e23873. doi: 10.7759/cureus.23873
13. Quraishi MN, Widlak M, Bhala N, Moore D, Price M, Sharma N, et al. Systematic review with meta-analysis: the efficacy of faecal microbiota transplantation for the treatment of recurrent and refractory Clostridium difficile infection. Aliment Pharmacol Ther (2017) 46(5):479–93. doi: 10.1111/apt.14201
14. Stojek M, Jabłońska A, Adrych K. The role of fecal microbiota transplantation in the treatment of inflammatory bowel disease. J Clin Med (2021) 10(18):4055. doi: 10.3390/jcm10184055
15. Zhang Z, Mocanu V, Cai C, Dang J, Slater L, Deehan EC, et al. Impact of fecal microbiota transplantation on obesity and metabolic syndrome-A systematic review. Nutrients (2019) 11(10):2291. doi: 10.3390/nu11102291
16. Lythgoe MP, Ghani R, Mullish BH, Marchesi JR, Krell J. The potential of fecal microbiota transplantation in oncology. Trends Microbiol (2022) 30(1):10–2. doi: 10.1016/j.tim.2021.10.003
17. Chinna Meyyappan A, Forth E, Wallace CJK, Milev R. Effect of fecal microbiota transplant on symptoms of psychiatric disorders: a systematic review. BMC Psychiatry (2020) 20(1):299. doi: 10.21203/rs.3.rs-16542/v1
18. Wang H, Yang F, Zhang S, Xin R, Sun Y. Genetic and environmental factors in Alzheimer's and Parkinson's diseases and promising therapeutic intervention via fecal microbiota transplantation. NPJ Parkinsons Dis (2021) 7(1):70. doi: 10.1038/s41531-021-00213-7
19. Nejadghaderi SA, Nazemalhosseini-Mojarad E, Asadzadeh Aghdaei H. Fecal microbiota transplantation for COVID-19; a potential emerging treatment strategy. Med Hypotheses (2021) 147:110476. doi: 10.1016/j.mehy.2020.110476
20. Bibbò S, Settanni CR, Porcari S, Bocchino E, Ianiro G, Cammarota G, et al. Fecal microbiota transplantation: screening and selection to choose the optimal donor. J Clin Med (2020) 9(6):1757. doi: 10.3390/jcm9061757
21. Keller JJ, Ooijevaar RE, Hvas CL, Terveer EM, Lieberknecht SC, Högenauer C, et al. A standardised model for stool banking for faecal microbiota transplantation: a consensus report from a multidisciplinary UEG working group. United Eur Gastroenterol J (2020) 2:2050640620967898. doi: 10.1177/2050640620967898
22. Cammarota G, Ianiro G, Kelly CR, Mullish BH, Allegretti JR, Kassam Z, et al. International consensus conference on stool banking for faecal microbiota transplantation in clinical practice. Gut (2019) 68(12):2111–21. doi: 10.1136/gutjnl-2019-319548
23. Coryell MP, kiviak M, Pereira N, Murugkar PP, Rippe J, Williams DB, et al. A method for detection of SARS-CoV-2 RNA in healthy human stool: a validation study. Lancet Microbe (2021) 2(6):e259–66. doi: 10.1016/S2666-5247(21)00059-8
24. Wilson BC, Vatanen T, Cutfield WS, O'Sullivan JM. The super-donor phenomenon in fecal microbiota transplantation. Front Cell Infect Microbiol (2019) 9:2. doi: 10.3389/fcimb.2019.00002
25. Kump P, Wurm P, Gröchenig HP, Wenzl H, Petritsch W, Halwachs B, et al. The taxonomic composition of the donor intestinal microbiota is a major factor influencing the efficacy of faecal microbiota transplantation in therapy refractory ulcerative colitis. Aliment Pharmacol Ther (2018) 47(1):67–77. doi: 10.1111/apt.14387
26. Martínez JE, Vargas A, Pérez-Sánchez T, Encío IJ, Cabello-Olmo M, Barajas M. Human microbiota network: unveiling potential crosstalk between the different microbiota ecosystems and their role in health and disease. Nutrients (2021) 13(9)2905. doi: 10.3390/nu13092905
27. Fan Y, Pedersen O. Gut microbiota in human metabolic health and disease. Nat Rev Microbiol (2021) 19(1):55–71. doi: 10.1038/s41579-020-0433-9
28. Consortium HMP. Structure, function and diversity of the healthy human microbiome. Nature (2012) 486(7402):207–14. doi: 10.1038/nature11234
29. Nishida A, Inoue R, Inatomi O, Bamba S, Naito Y, Andoh A. Gut microbiota in the pathogenesis of inflammatory bowel disease. Clin J Gastroenterol (2018) 11(1):1–10. doi: 10.1007/s12328-017-0813-5
30. Tsai YW, Dong JL, Jian YJ, Fu SH, Chien MW, Liu YW, et al. Gut microbiota-modulated metabolomic profiling shapes the etiology and pathogenesis of autoimmune diseases. Microorganisms (2021) 9(9):1930. doi: 10.3390/microorganisms9091930
31. Zmora N, Suez J, Elinav E. You are what you eat: diet, health and the gut microbiota. Nat Rev Gastroenterol Hepatol (2019) 16(1):35–56. doi: 10.1038/s41575-018-0061-2
32. Leeming ER, Johnson AJ, Spector TD, Le Roy CI. Effect of diet on the gut microbiota: rethinking intervention duration. Nutrients (2019) 11(12):2862. doi: 10.3390/nu11122862
33. Magro DO, Rossoni C, Saad-Hossne R, Santos A. INTERACTION BETWEEN FOOD PYRAMID AND GUT MICROBIOTA. A NEW NUTRITIONAL APPROACH. Arq Gastroenterol (2023) 60(1):132–6. doi: 10.1590/s0004-2803.202301000-15
34. Kolodziejczyk AA, Zheng D, Elinav E. Diet-microbiota interactions and personalized nutrition. Nat Rev Microbiol (2019) 17(12):742–53. doi: 10.1038/s41579-019-0256-8
35. Rinninella E, Cintoni M, Raoul P, Lopetuso LR, Scaldaferri F, Pulcini G, et al. Food components and dietary habits: keys for a healthy gut microbiota composition. Nutrients (2019) 11(10):2393. doi: 10.3390/nu11102393
36. Bell V, Ferrão J, Pimentel L, Pintado M, Fernandes T. Fermented foods, and gut microbiota. Foods (2018) 7(12):195. doi: 10.3390/foods7120195
37. Quesada-Molina M, Muñoz-Garach A, Tinahones FJ, Moreno-Indias I. A new perspective on the health benefits of moderate beer consumption: involvement of the gut microbiota. Metabolites (2019) 9(11):272. doi: 10.3390/metabo9110272
38. González S, Salazar N, Ruiz-Saavedra S, Gómez-Martín M, de Los Reyes-Gavilán CG, Gueimonde M. Long-term coffee consumption is associated with fecal microbial composition in humans. Nutrients (2020) 12(5):1287. doi: 10.3390/nu12051287
39. Wong JM. Gut microbiota and cardiometabolic outcomes: influence of dietary patterns and their associated components. Am J Clin Nutr (2014) 100 Suppl 1:369s–77s. doi: 10.3945/ajcn.113.071639
40. De Filippis F, Pellegrini N, Vannini L, Jeffery IB, La Storia A, Laghi L, et al. High-level adherence to a Mediterranean diet beneficially impacts the gut microbiota and associated metabolome. Gut (2016) 65(11):1812–21. doi: 10.1136/gutjnl-2015-309957
41. Del Chierico F, Vernocchi P, Dallapiccola B, Putignani L. Mediterranean diet and health: food effects on gut microbiota and disease control. Int J Mol Sci (2014) 15(7):11678–99. doi: 10.3390/ijms150711678
42. Nagpal R, Shively CA, Register TC, Craft S, Yadav H. Gut microbiome-Mediterranean diet interactions in improving host health. F1000Res (2019) 8:699. doi: 10.12688/f1000research.18992.1
43. Moszak M, Szulińska M, Bogdański P. You are what you eat-the relationship between diet, microbiota, and metabolic disorders-A review. Nutrients (2020) 12(4):1096. doi: 10.3390/nu12041096
44. Ismael S, Silvestre MP, Vasques M, Araújo JR, Morais J, Duarte MI, et al. A pilot study on the metabolic impact of mediterranean diet in type 2 diabetes: is gut microbiota the key? Nutrients (2021) 13(4):1228. doi: 10.3390/nu13041228
45. Beam A, Clinger E, Hao L. Effect of diet and dietary components on the composition of the gut microbiota. Nutrients (2021) 13(8):2795. doi: 10.3390/nu13082795
46. Clancy AK, Gunaratne AW, Borody TJ. Dietary management for faecal microbiota transplant: an international survey of clinical and research practice, knowledge and attitudes. Front Nutr (2021) 8:653653. doi: 10.3389/fnut.2021.653653
47. Zazpe I, Sanchez-Tainta A, Estruch R, Lamuela-Raventos RM, Schröder H, Salas-Salvado J, et al. A large randomized individual and group intervention conducted by registered dietitians increased adherence to Mediterranean-type diets: the PREDIMED study. J Am Diet Assoc (2008) 108(7):1134–44. doi: 10.1016/j.jada.2008.04.011
48. Hanssen NMJ, Nieuwdorp M. Fecal microbiota transplantation and fiber supplementation, better together? Cell Rep Med (2021) 2(9):100403. doi: 10.1016/j.xcrm.2021.100403
49. Mocanu V, Zhang Z, Deehan EC, Kao DH, Hotte N, Karmali S, et al. Fecal microbial transplantation and fiber supplementation in patients with severe obesity and metabolic syndrome: a randomized double-blind, placebo-controlled phase 2 trial. Nat Med (2021) 27(7):1272–9. doi: 10.1038/s41591-021-01399-2
50. Rinott E, Youngster I, Yaskolka Meir A, Tsaban G, Zelicha H, Kaplan A, et al. Effects of diet-modulated autologous fecal microbiota transplantation on weight regain. Gastroenterology (2021) 160(1):158–173.e10. doi: 10.1053/j.gastro.2020.08.041
Keywords: diet, fecal microbiota transplantation, FMT receptors, gut microbiota, stool donors
Citation: Silva R, Dinis L, Peris A, Novais L, Calhau C, Pestana D and Marques C (2023) Fecal microbiota transplantation—could stool donors’ and receptors’ diet be the key to future success?. Front. Gastroenterol. 2:1270899. doi: 10.3389/fgstr.2023.1270899
Received: 01 August 2023; Accepted: 16 October 2023;
Published: 01 November 2023.
Edited by:
Rui Manuel Ferreira, Universidade do Porto, PortugalReviewed by:
Andrey Santos, State University of Campinas, BrazilCopyright © 2023 Silva, Dinis, Peris, Novais, Calhau, Pestana and Marques. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cláudia Marques, Y2xhdWRpYS5zb2ZpYS5tYXJxdWVzQG5tcy51bmwucHQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.