
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Gastroenterol., 01 August 2023
Sec. Hepatology
Volume 2 - 2023 | https://doi.org/10.3389/fgstr.2023.1209000
This article is part of the Research TopicRising Stars in Gastroenterology: 2023View all 8 articles
 Guilherme Grossi Lopes Cançado1*
Guilherme Grossi Lopes Cançado1* Aline Coelho Rocha Candolo2
Aline Coelho Rocha Candolo2 Mateus Jorge Nardelli1
Mateus Jorge Nardelli1 Patricia Momoyo Zitelli2Daniel Ferraz de Campos Mazo2,3
Patricia Momoyo Zitelli2Daniel Ferraz de Campos Mazo2,3 Claudia Pinto Oliveira2Marlone Cunha-Silva3Raquel Dias Greca3Roberta Chaves Araújo4Amanda Sacha Paulino Tolentino Alustau4Cláudia Alves Couto1Gabriel Rezende de Lima Roque2Alberto Queiroz Farias2Flair José Carrilho2Mário Guimarães Pessôa2
Claudia Pinto Oliveira2Marlone Cunha-Silva3Raquel Dias Greca3Roberta Chaves Araújo4Amanda Sacha Paulino Tolentino Alustau4Cláudia Alves Couto1Gabriel Rezende de Lima Roque2Alberto Queiroz Farias2Flair José Carrilho2Mário Guimarães Pessôa2Introduction: Cryptogenic chronic hepatitis is a growing cause of liver transplants, affecting 5%–15% of patients with chronic liver diseases. This study aimed to identify underlying causes of cryptogenic liver disease in a Brazilian cohort and propose a new diagnostic algorithm, including investigation for metabolic-dysfunction-associated fatty liver disease (MAFLD) and lysosomal acid lipase deficiency (LAL-D).
Methods: A retrospective analysis was conducted on 326 patients with presumed cryptogenic hepatitis.
Results: Using Czaja’s algorithm, non-alcoholic fatty liver disease was diagnosed in 21.3% of patients, while alpha-1 antitrypsin deficiency, alcoholic liver disease, autoimmune hepatitis, hemochromatosis, biliary-related hepatitis, viral hepatitis, Budd–Chiari syndrome, glycogenosis, drug-induced liver injury, and Wilson’s disease were diagnosed in smaller proportions (< 3.5% each). LAL-D was found in 1% of patients, and 53.6% of patients remained with cryptogenic hepatitis. The etiology of the liver disease in a subset of patients undergoing liver transplantation was updated post hoc based on explant histology, and non-alcoholic steatohepatitis was found in 52.5% of patients. By incorporating the concept of MAFLD, the new algorithm could diagnose 49.1% of patients, reducing the number of individuals without an etiological diagnosis by 11.4%.
Conclusion: One-third of patients with initially presumed cryptogenic liver disease were diagnosed with MAFLD. LAL-D should be considered in patients with chronic liver disease of unknown etiology. The updated diagnostic algorithm proposed in this study could improve diagnostic accuracy and aid in the management of patients with cryptogenic hepatitis.
Cryptogenic chronic hepatitis is a persistent inflammation of the liver that is unexplained by comprehensive clinical, laboratory, and histological investigations (1). It affects 5%–15% of patients with chronic liver disease (2). Cryptogenic cirrhosis is diagnosed in 5%–30% of patients with cirrhosis, and it is found in 3%–14% of adults awaiting liver transplantation (3–6). The diagnosis depends on the diligence, expertise, and rigor of the examiner, as well as on the laboratorial and anatomopathological resources available for a comprehensive investigation.
It is also important to mention that cryptogenic hepatitis may reflect a late phase of disease in which classical findings have been lost or obscured transiently (1). On the other hand, the new definition of metabolic-associated fatty liver disease has recently increased the potential for the etiological diagnosis of several patients previously labeled with cryptogenic hepatitis, especially among cirrhotics (7–10). Lysosomal acid lipase deficiency (LAL-D), silent autoimmune hepatitis, occult viral hepatitis, alcohol-related liver injury, and alpha-1 antitrypsin deficiency have also been linked to the cryptogenic liver disease spectrum and can histologically mimic non-alcoholic fatty liver disease. In this way, periodically re-evaluating these patients is vital for the perception of late-emerging diagnostic features, especially autoantibodies, metabolic variations, concurrent immune diseases, and liver biopsy findings.
Previously, Czaja had proposed a three-step algorithm to diagnose patients with cryptogenic chronic hepatitis, which has not been further validated in clinical practice (1). In this study, we aimed to investigate if patients with chronic hepatitis classified as cryptogenic by general practitioners may actually have a defined etiology if an appropriate diagnostic flowchart is followed, and to propose a new diagnostic approach incorporating metabolic-dysfunction-associated fatty liver disease (MAFLD) definition and LAL-D investigation.
The study population included adult (≥ 18 years old) patients diagnosed with cryptogenic chronic hepatitis by general practitioners and referred to four different Brazilian hepatology centers between 1 October 2016 and 30 November 2018 [Hospital das Clínicas of the University of São Paulo School of Medicine (HCFMUSP), Division of Gastroenterology (Gastrocentro) of the University of Campinas (UNICAMP), School of Medicine of Ribeirão Preto of the University of Sao Paulo (FMRP-USP), and Instituto Alfa de Gastroenterologia at Hospital das Clínicas of the Federal University of Minas Gerais (UFMG)]. All study procedures were conducted in accordance with the ethical standards of the Helsinki Declaration. The present study was approved by the Ethics Committee Boards of all institutions and individual informed consent was obtained from all participants at the time of blood collection for LAL-D enzyme activity measurement.
Demographic, clinical, and laboratory data, as well as liver histology and imaging findings, were retrospectively collected from electronic or paper-based medical records. Liver cirrhosis was defined according to clinical, imaging, and histological findings. Alcohol intake was assessed (less than <140 g/week for both genders) to exclude alcoholic liver disease. The body mass index (body weight [kg]/body height [m2]) was calculated in all patients. Overweight and obesity were assumed if the body mass index exceeded 25 kg/m2 and 30 kg/m2, respectively. Metabolic parameters, including serum fasting glucose, triglycerides, and cholesterol, as well as blood pressure and waist circumference, were reviewed for MAFLD diagnosis (7). The diagnosis of MAFLD was based on evidence of hepatic steatosis [histological, imaging, or blood biomarker evidence (fatty liver index ≥60) of fat accumulation in the liver] in addition to one of the following criteria: overweight/obesity, presence of type 2 diabetes mellitus, or evidence of metabolic dysregulation. MAFLD-related cirrhosis patients are patients with cirrhosis, historical documentation of steatosis by hepatic imaging or biopsy, and past or present evidence of metabolic risk factors that meet the criteria to diagnose MAFLD. The diagnosis of non-alcoholic fatty liver disease (NAFLD) was established by the evidence of hepatic steatosis by either imaging or histology, and lack of secondary causes of hepatic fat accumulation (11). Wilson’s disease and alpha-1 antitrypsin deficiency were tested by determination of ceruloplasmin/urinary copper, and alpha-1 antitrypsin levels (or alpha-1 fraction of protein electrophoresis, in cases where there were not dosages of alpha-1 antitrypsin available), respectively. Females with transferrin saturation of >45% and serum ferritin of >200 μg/L and males with transferrin saturation of >50% and ferritin of >300 μg/L were submitted to genotyping for p.C282Y in HFE and screened for hemochromatosis. All patients were also assessed for serum markers of hepatitis B and C (anti-HCV, HBsAg, anti-HBc, HBV DNA, and HCV RNA by polymerase chain reaction), HIV infection, serum anti-nuclear antibody, smooth muscle antibody, anti-liver kidney microsomal antibody type 1, and anti-mitochondrial antibodies. The international autoimmune hepatitis score was calculated for patients with clinically suspected autoimmune hepatitis. Additionally, liver imaging tests (ultrasound, computer tomography, and magnetic resonance, when available) were evaluated for the exclusion of MAFLD and biliary and vascular etiology. Histopathology was assessed in patients who underwent liver biopsy or liver transplantation. Finally, Czaja’s algorithm for cryptogenic chronic hepatitis diagnosis was retrospectively tested to assess its performance in a real-life cohort of patients with presumed chronic cryptogenic hepatitis referred by general practitioners to specialized centers (1). Individuals with incomplete investigations were excluded from the database.
Lysosomal acid lipase (LAL) enzyme activity was measured in all patients to assess the prevalence of LAL-D among patients with cryptogenic hepatitis. All individuals had collected a blood sample of about 5 mL from peripheral venous access, which was then pipetted (four drops) on filter paper for preparing dried blood spots. The material was randomly referred for analysis at Seattle Children’s Hospital, USA, or AFIP (Research Incentive Fund Association), Brazil. LAL activity was measured by a highly specific test using lalistat 2, a specific LAL inhibitor at both laboratories. In Seattle, in-house methodology was considered. In the AFIP laboratory, the methodology described by Hamilton et al. was used (12). The dosage of LAL activity was generously provided by Alexion Pharmaceuticals (New Haven, Connecticut, USA).
A statistical analysis was performed using SPSS 25.0 software (IBM, USA). Continuous variables distribution was assessed using the Shapiro–Wilk test, and those with Gaussian distribution were expressed as mean and standard deviation, or as median and interquartile range (IQR) if there was a skewed distribution. Categorical variables were expressed as absolute number and percentage. Comparison between both algorithms presented were made by chi-square statistics, and a p-value < 0.05 was considered significant.
Three hundred and twenty-six patients [mean age 60 (46–68) years, 42.9% male] were initially included, 35.7% with cirrhosis. Forty-five individuals were excluded due to incomplete etiological investigations. Clinical characteristics of the cohort are shown in Supplementary Table 1. Using Czaja’s algorithm, diagnosis of NAFLD could be established in 60 patients (21.3%), alpha-1-antitrypsin deficiency in nine (3.2%), alcoholic liver disease in seven (2.7%), autoimmune hepatitis in five (1.78%), hemochromatosis in five (1.78%), biliary-related hepatitis in four (1.4%), viral hepatitis in four (1.4%), Budd–Chiari syndrome in four (1.4%), glycogenosis in three (1%), drug-induced liver injury in two (0.7%), and Wilson’s disease in one (0.35%). In 158 patients, at least one liver biopsy had been performed. Etiological diagnosis was possible only by liver tissue evaluation in 21 individuals, most of them with NAFLD (57%). Finally, 175 out of 281 patients remained with cryptogenic hepatitis (62.3%). During follow-up, 40 of those patients were submitted for liver transplantation and 21 (52.5%) were retrospectively diagnosed with non-alcoholic steatohepatitis after a histopathological examination of the explanted liver (Figure 1A).
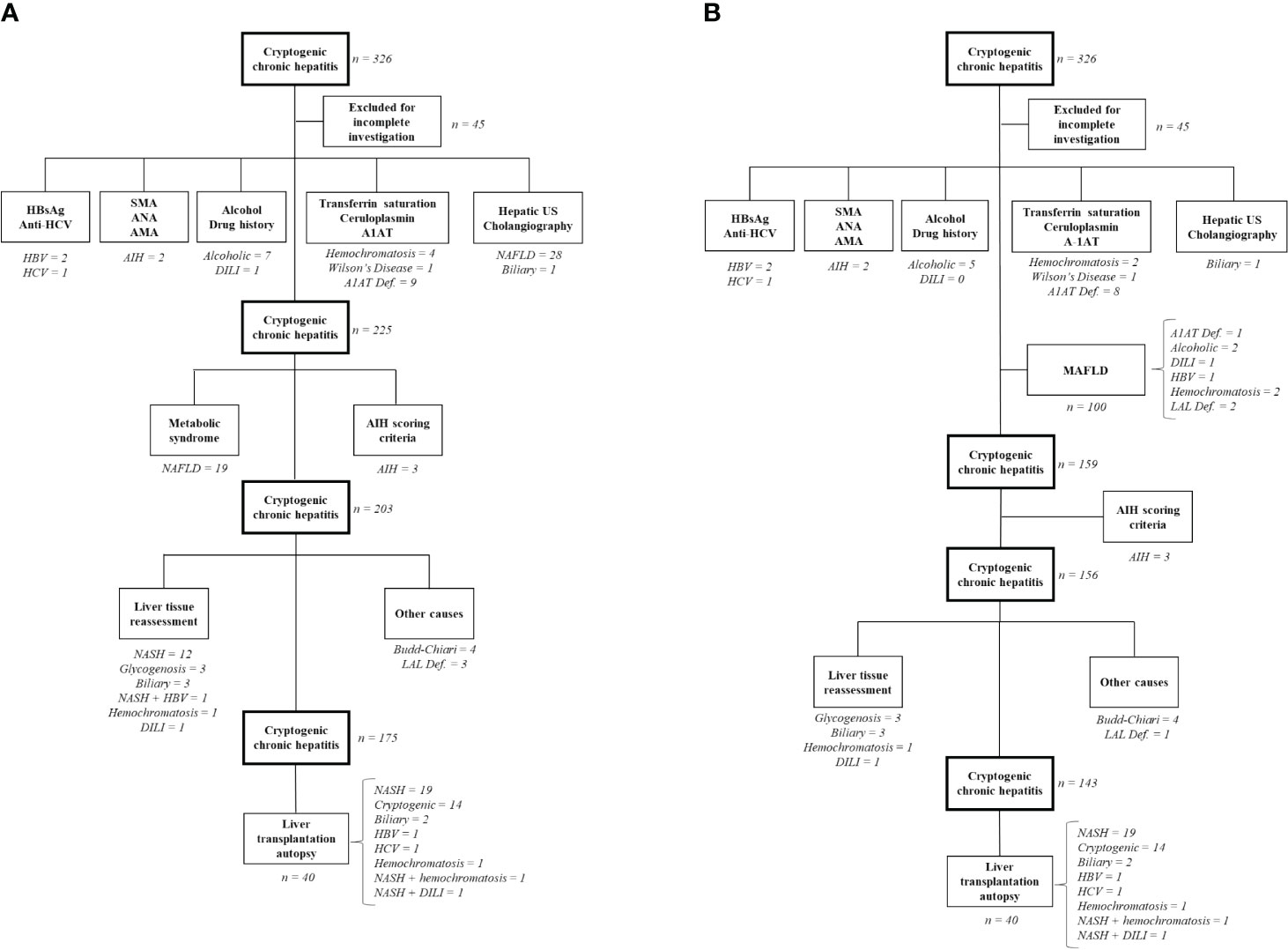
Figure 1 Algorithms for diagnosis of cryptogenic chronic hepatitis. (A) Original Czaja´s algorithm; (B) New proposed algorithm; After each etiology is presented the absolute number of patients diagnosed in each step. In brackets, it is described the number of patients with overlapping liver diseases and its respective etiologies. HCV, hepatitis C virus; HBV, hepatitis B virus; DILI, drug induced liver injury; US, ultrasound; A1AT, Alpha-1 antitrypsin deficiency; NAFLD, non-alcoholic fatty liver disease; NASH, non-alcoholic steatohepatitis; MAFLD, metabolic-dysfunction-associated fatty liver disease; AIH, autoimmune hepatitis; LAL def., lysosomal acid lipase deficiency.
By including MAFLD at the first step of the new algorithm, 100 patients would have been diagnosed (35.6%), reducing the number of individuals without a diagnosis by 11.4%. On the other hand, nine (9%) of those patients presented with another concomitant liver disease diagnosis besides MAFLD (Figure 1B). LAL-D was demonstrated in three individuals (1%). Finally, using the new algorithm, 143 patients out of 281 (50.9%) would remain cryptogenic.
Comparing both algorithms, chronic liver disease could have an etiological diagnosis in 37.7% by Czaja’s algorithm and 49.1% by the new algorithm (p = 0.006).
Accurate and timely diagnosis of a chronic hepatitis disease is fundamental to ensure patients receive appropriate treatment. Although there have been global improvements in analytical technology, developing nations such as Brazil face obstacles in enhancing their diagnostic abilities. These challenges stem from financial constraints, the concentration of resources in large urban centers, and a shortage of trained personnel (13). In our study, careful re-evaluation of all clinical, laboratory, imaging and histological data using Czaja’s algorithm could reduce the number of patients initially diagnosed with presumed cryptogenic hepatitis from 281 to 175 (–37.2%). Diagnostic yield could be improved by 11.4% by the inclusion of the new MALFD criteria and LAL-D investigation, although it is always a challenge to determine the best practical and feasible diagnostic strategy. The etiology of the liver disease was not defined in 50.9% of the cases using the new algorithm. Even in those who underwent liver transplantation, the histopathological examination of explanted liver could not define liver disease etiology in 35% of the cases.
The discovery of hepatitis B virus in the 1960s and hepatitis C virus in the 1990s have previously challenged the existence of cryptogenic chronic hepatitis (14, 15). Even after incorporating a viral hepatitis serological examination as part of the initial liver disease investigation, there can be still be cases of occult hepatitis C or B virus infection that can be perceived only after a direct liver tissue evaluation (16–18). In our study, two cases of occult viral hepatitis were observed in liver transplantation explants (5%), reinforcing the concept that viral hepatitis can still represent a small proportion of cryptogenic cirrhosis depending on the prevalence of the disease in the evaluated population. In fact, occult hepatitis C and B have been demonstrated in 8% (16) and 6.3% (18), respectively, of liver transplant patients with cryptogenic cirrhosis. Conversely, recent research indicates that the hepatitis B virus infection is responsible for a small percentage of cases (2%) of cryptogenic chronic hepatitis. Similarly, it is expected that hepatitis C virus infection also plays a minor role in this condition (19). Other viruses have also been investigated as etiological agents in the liver transplant population with cryptogenic cirrhosis, but with no definitive role, such as hepatitis G (20–22).
The obesity and metabolic syndrome epidemics in the last two decades have been dramatically associated with increasing occurrences of NAFLD. Interestingly, previous studies have shown that overweight and metabolic disorders are more likely to be found among cryptogenic chronic hepatitis subjects than in other causes of liver disease (8, 9, 23). Clark et al. have also demonstrated that patients with unexplained aminotransferase elevation present with significantly higher body mass index, waist circumference, triglycerides, and fasting insulin, and lower HDL—features associated with NAFLD (24). Furthermore, studies that evaluated histopathological findings in chronic cryptogenic hepatitis found a high frequency of fatty liver (28%–68%) (5, 25–28). Nevertheless, it is widely recognized that advanced hepatic fibrosis can alter, diminish, or even eliminate the histological characteristics of hepatic steatosis. This can result in the misidentification of individuals with NAFLD as having cryptogenic chronic liver disease. Previous studies have shown that cryptogenic cirrhosis presents more active fibrosis and a higher risk of liver-related clinical events than NAFLD-cirrhosis patients, highlighting the importance of differentiating both entities (29, 30). The new positive criteria for MAFLD minimizes this problem, especially for MAFLD-related cirrhosis, since histology is no longer required for diagnosis (7).
Histopathological examinations of the explanted liver after transplantation may significantly help to diagnose the cause of cirrhosis in patients with cryptogenic liver disease and guide specific post-transplantation therapies. NAFLD has been shown to be the most common cause of presumed cryptogenic liver disease diagnosed by histological evaluation of the explanted liver. In our cohort, non-alcoholic steatohepatitis was diagnosed in nearly 50% of the patients presenting for liver transplantation, which was similar to one other study evaluating liver explants (31). Conversely, Tardu et al. have shown a 25% rate of steatosis in the transplanted livers of patients with cryptogenic cirrhosis (6).
Our study has some limitations inherent to its retrospective design, such as some patients being lost due to missing data. A low incidence of autoimmune hepatitis in cryptogenic chronic hepatitis was observed, but it should be acknowledged that not all centers in Brazil have access to unconventional antibodies, such as anti-soluble liver antigen-liver/pancreas. Hepatic steatosis was detected by different methods—histological, imaging, or blood biomarker—which certainly present different accuracies. The high prevalence of cirrhotic patients may have been underestimated by the prevalence of fatty liver disease. Furthermore, liver biopsy was not performed in all patients. On the other hand, the large sample size and the multicenter data reflects real-life clinical practice. The implementation of the new algorithm would allow for an etiological diagnosis in 49.1% of the patients, reducing the necessity of tissue assessment in several patients.
In conclusion, a meticulous and consistent approach to patients with cryptogenic chronic hepatitis can result in an etiological diagnosis in almost 50% of cases. About one-third of patients initially diagnosed with cryptogenic liver disease were eventually found to have MAFLD. Although it is uncommon, testing for LAL-D should be considered for individuals with chronic liver disease of unknown origin. An updated diagnostic algorithm has been suggested for these individuals and should be tested in other groups to ensure its efficacy.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
The study was conducted in accordance with the Declaration of Helsinki, and approved by the following Institutional Review Boards [University of São Paulo School of Medicine (USP), University of Campinas (UNICAMP), Ribeirão Preto—University of Sao Paulo (FMRP-USP), and Federal University of Minas Gerais (UFMG)]. The patients/participants provided their written informed consent to participate in this study.
GC, AC, DM, CO, and MG: study concept and design, acquisition and interpretation of data, and analysis drafting of the manuscript. PZ: acquisition of data and exam collection. M-CS, RG, RA, AA, CC, and MN: acquisition of data. AF and FC: analysis drafting. MN: statistical analysis. All authors read and approved the final manuscript.
The dosage of lysosomal acid lipase was provided by Alexion Pharmaceuticals, which had no role in the study design, data evaluation, or manuscript writing.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fgstr.2023.1209000/full#supplementary-material
1. Czaja AJ. Cryptogenic chronic hepatitis and its changing guise in adults. Dig Dis Sci (2011) 56(12):3421–38. doi: 10.1007/s10620-011-1769-9
2. Kodali VP, Gordon SC, Silverman AL, McCray DG. Cryptogenic liver disease in the United States: further evidence for non-A, non-B, and non-C hepatitis. Am J Gastroenterol (1994) 89(10):1836–9.
3. Golabi P, Bush H, Stepanova M, Locklear CT, Jacobson IM, Mishra A, et al. Liver transplantation (LT) for cryptogenic cirrhosis (CC) and nonalcoholic steatohepatitis (NASH) cirrhosis data from the Scientific Registry of Transplant Recipients (SRTR): 1994 to 2016. Med (United States) (2018) 97(31):e11518. doi: 10.1097/MD.0000000000011518
4. Sanjeevi A, Lyden E, Sunderman B, Weseman R, Ashwathnarayan R, Mukherjee S. Outcomes of liver transplantation for cryptogenic cirrhosis: a single-center study of 71 patients. Transplant Proc (2003) 35(8):2977–80. doi: 10.1016/j.transproceed.2003.10.059
5. Marmur J, Bergquist A, Såtl P. Liver transplantation of patients with cryptogenic cirrhosis: Clinical characteristics and outcome. Scand J Gastroenterol (2010) 45(1):60–9. doi: 10.3109/00365520903384742
6. Tardu A, Karagul S, Yagci MA, Ertugrul I, Sumer F, Kirmizi S, et al. Histopathological examination of explanted liver after transplantation in patients with cryptogenic cirrhosis. Transplant Proc (2015) 47(5):1450–2. doi: 10.1016/j.transproceed.2015.04.020
7. Eslam M, Newsome PN, Sarin SK, Anstee QM, Targher G, Romero-Gomez M, et al. A new definition for metabolic dysfunction-associated fatty liver disease: An international expert consensus statement. J Hepatol (2020) 73(1):202–9. doi: 10.1016/j.jhep.2020.03.039
8. Idilman R, Aydogan M, Oruncu MB, Kartal A, Elhan AH, Ellik Z, et al. Natural history of cirrhosis: changing trends in etiology over the years. Dig Dis (2021) 39(4):358–65. doi: 10.1159/000512746
9. Bharath Kumar C, Goel A, Jaleel R, David D, Zachariah U, Ramachandran J, et al. Prevalence of risk factors for nonalcoholic fatty liver disease in middle-aged and elderly patients with cryptogenic cirrhosis. J Clin Exp Hepatol (2022) 12(2):492–502. doi: 10.1016/j.jceh.2021.05.008
10. Huang DQ, Terrault NA, Tacke F, Gluud LL, Arrese M, Bugianesi E, et al. Global epidemiology of cirrhosis — aetiology, trends and predictions. Nat Rev Gastroenterol Hepatol (2023) 20(6):388–98. doi: 10.1038/s41575-023-00759-2
11. Chalasani N, Younossi Z, Lavine JE, Charlton M, Cusi K, Rinella M, et al. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology (2018) 67(1):328–57. doi: 10.1002/hep.29367
12. Hamilton J, Jones I, Srivastava R, Galloway P. A new method for the measurement of lysosomal acid lipase in dried blood spots using the inhibitor Lalistat 2. Clin Chim Acta (2012) 413(15–16):1207–10. doi: 10.1016/j.cca.2012.03.019
13. Cançado GGL, de Abreu ES, Nardelli MJ, Serwa P, Brachmann M. A cost of illness comparison for toxigenic Clostridioides difficile diagnosis algorithms in developing countries. Anaerobe (2021) 70:102390. doi: 10.1016/j.anaerobe.2021.102390
14. Schmidt WN, Wu P, Cederna J, Mitros FA, LaBrecque DR, Stapleton JT. Surreptitious Hepatitis C Virus (HCV) infection detected in the majority of patients with cryptogenic chronic hepatitis and negative HCV antibody tests. J Infect Dis (1997) 176(1):27–33. doi: 10.1086/514033
15. Berasain C. Pathological and virological findings in patients with persistent hypertransaminasaemia of unknown aetiology. Gut (2000) 47(3):429–35. doi: 10.1136/gut.47.3.429
16. Yaghobi R, Kazemi MJ, Geramizadeh B, Malek Hosseini SA, Moayedi J. Significance of occult Hepatitis C virus infection in liver transplant patients with cryptogenic cirrhosis. Exp Clin Transplant (2020) 18(2):206–9. doi: 10.6002/ect.2017.0332
17. Rendon JC, Cortes-Mancera F, Restrepo-Gutierrez JC, Hoyos S, Navas MC. Molecular characterization of occult hepatitis B virus infection in patients with end-stage liver disease in Colombia. PloS One (2017) 12(7):e0180447. doi: 10.1371/journal.pone.0180447
18. Ferrari TCA, Xavier MAP, Vidigal PVT, Amaral NS, Diniz PA, Resende AP, et al. Occult hepatitis B virus infection in liver transplant patients in a Brazilian referral center. Braz J Med Biol Res (2014) 47(11):990–4. doi: 10.1590/1414-431X20143782
19. Kaviani MJ. Occult hepatitis B virus infection and cryptogenic chronic hepatitis in an area with intermediate prevalence of HBV infection. World J Gastroenterol (2006) 12(31):5048. doi: 10.3748/wjg.v12.i31.5048
20. Pessoa MG, Terrault NA, Ferrell LD, Kim JP, Kolberg J, Detmer J, et al. Hepatitis G virus in patients with cryptogenic liver disease undergoing liver transplantation. Hepatology (1997) 25(5):1266–70. doi: 10.1002/hep.510250535
21. Pessoa MG, Terrault NA, Detmer J, Kolberg J, Collins M, Hassoba HM, et al. Quantitation of hepatitis G and C viruses in the liver: evidence that hepatitis G virus is not hepatotropic. Hepatology (1998) 27(3):877–80. doi: 10.1002/hep.510270335
22. Pessoa MG, Terrault NA, Ferrell LD, Detmer J, Kolberg J, Collins ML, et al. Hepatitis after liver transplantation: The role of the known and unknown viruses. Liver Transplant Surg (1998) 4(6):461–8. doi: 10.1002/lt.500040603
23. Caldwell SH, Oelsner DH, Iezzoni JC, Hespenheide EE, Battle EH, Driscoll CJ. Cryptogenic cirrhosis: Clinical characterization and risk factors for underlying disease. Hepatology (1999) 29(3):664–9. doi: 10.1002/hep.510290347
24. Clark JM, Brancati FL, Diehl AM. The prevalence and etiology of elevated aminotransferase levels in the United States. Am J Gastroenterol (2003) 98(5):960–7. doi: 10.1111/j.1572-0241.2003.07486.x
25. Tanaka N, Tanaka E, Sheena Y, Komatsu M, Okiyama W, Misawa N, et al. Useful parameters for distinguishing nonalcoholic steatohepatitis with mild steatosis from cryptogenic chronic hepatitis in the Japanese population. Liver Int (2006) 26(8):956–63. doi: 10.1111/j.1478-3231.2006.01338.x
26. Mathiesen UL, Franzén A LE. The clinical significance of slightly to moderately increased liver transaminase values in asymptomatic patients. Scand J Gastroenterol (1999) 34(1):85–91. doi: 10.1080/00365529950172880
27. Skelly MM, James PD, Ryder SD. Findings on liver biopsy to investigate abnormal liver function tests in the absence of diagnostic serology. J Hepatol (2001) 35(2):195–9. doi: 10.1016/S0168-8278(01)00094-0
28. Ayata G, Gordon FD, Lewis WD, Pomfret E, Pomposelli JJ, Jenkins RL, et al. Cryptogenic cirrhosis: Clinicopathologic findings at and after liver transplantation. Hum Pathol (2002) 33(11):1098–104. doi: 10.1053/hupa.2002.129419
29. Younossi Z, Stepanova M, Sanyal AJ, Harrison SA, Ratziu V, Abdelmalek MF, et al. The conundrum of cryptogenic cirrhosis: Adverse outcomes without treatment options. J Hepatol (2018) 69(6):1365–70. doi: 10.1016/j.jhep.2018.08.013
30. Thuluvath PJ, Kantsevoy S, Thuluvath AJ, Savva Y. Is cryptogenic cirrhosis different from NASH cirrhosis? J Hepatol (2018) 68(3):519–25. doi: 10.1016/j.jhep.2017.11.018
31. Nayak NC, Vasdev N, Saigal S, Soin AS. End-stage nonalcoholic fatty liver disease: evaluation of pathomorphologic features and relationship to cryptogenic cirrhosis from study of explant livers in a living donor liver transplant program. Hum Pathol (2010) 41(3):425–30. doi: 10.1016/j.humpath.2009.06.021
Keywords: cryptogenic hepatitis, cryptogenic cirrhosis, metabolic associated fatty liver disease, non-alcoholic fatty liver disease, diagnosis, algorithm
Citation: Cançado GGL, Candolo ACR, Nardelli MJ, Zitelli PM, Mazo DFdC, Oliveira CP, Cunha-Silva M, Greca RD, Araújo RC, Alustau ASPT, Couto CA, Roque GRdL, Farias AQ, Carrilho FJ and Pessôa MG (2023) Cryptogenic chronic hepatitis: looking for an ideal diagnostic algorithm. Front. Gastroenterol. 2:1209000. doi: 10.3389/fgstr.2023.1209000
Received: 20 April 2023; Accepted: 14 July 2023;
Published: 01 August 2023.
Edited by:
Terry Cheuk-Fung Yip, The Chinese University of Hong Kong, Hong Kong SAR, ChinaReviewed by:
Martin Janičko, University of Pavol Jozef Šafárik, SlovakiaCopyright © 2023 Cançado, Candolo, Nardelli, Zitelli, Mazo, Oliveira, Cunha-Silva, Greca, Araújo, Alustau, Couto, Roque, Farias, Carrilho and Pessôa. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Guilherme Grossi Lopes Cançado, Z3VpbGhlcm1lZ3Jvc3NpQHRlcnJhLmNvbS5icg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.