
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Genet. , 17 December 2021
Sec. Cancer Genetics and Oncogenomics
Volume 12 - 2021 | https://doi.org/10.3389/fgene.2021.750675
This article is part of the Research Topic Uncovering drug resistance during cancer therapy View all 7 articles
 Elaina J. Wang1
Elaina J. Wang1 Jia-Shu Chen1
Jia-Shu Chen1 Saket Jain2
Saket Jain2 Ramin A. Morshed2
Ramin A. Morshed2 Alexander F. Haddad2Sabraj Gill2Angad S. Beniwal2
Alexander F. Haddad2Sabraj Gill2Angad S. Beniwal2 Manish K. Aghi2*
Manish K. Aghi2*Glioblastoma is the most common malignant primary brain tumor in adults. Despite treatment consisting of surgical resection followed by radiotherapy and adjuvant chemotherapy, survival remains poor at a rate of 26.5% at 2 years. Recent successes in using immunotherapies to treat a number of solid and hematologic cancers have led to a growing interest in harnessing the immune system to target glioblastoma. Several studies have examined the efficacy of various immunotherapies, including checkpoint inhibitors, vaccines, adoptive transfer of lymphocytes, and oncolytic virotherapy in both pre-clinical and clinical settings. However, these therapies have yielded mixed results at best when applied to glioblastoma. While the initial failures of immunotherapy were thought to reflect the immunoprivileged environment of the brain, more recent studies have revealed immune escape mechanisms created by the tumor itself and adaptive resistance acquired in response to therapy. Several of these resistance mechanisms hijack key signaling pathways within the immune system to create a protumoral microenvironment. In this review, we discuss immunotherapies that have been trialed in glioblastoma, mechanisms of tumor resistance, and strategies to sensitize these tumors to immunotherapies. Insights gained from the studies summarized here may help pave the way for novel therapies to overcome barriers that have thus far limited the success of immunotherapy in glioblastoma.
Glioblastoma (GBM) is the most common cause of primary brain malignancy, accounting for 27% of all brain tumors and 80% of malignant brain tumors (Ostrom et al., 2015). The current standard of care (SOC) for primary GBM is maximally safe surgical resection followed by concurrent radiotherapy and temozolomide (TMZ) for 6 weeks and then adjuvant TMZ for 6 months (Fernandes et al., 2017). However, despite treatment, median survival remains low with a 2-year survival rate of under 30% (Stupp et al., 2005) and recurrence occurring in over 90% of high-grade glioma patients (Choucair et al., 1986).
The recent use of immunotherapies, such as immune checkpoint inhibitors and autologous T cells expressing chimeric antigen receptors (CAR), to successfully treat various solid and hematologic malignancies has led to growing interest in applying similar methods to GBM. Nivolumab, an anti-programmed death-1 (PD-1) antibody, and ipilimumab, an anti-cytotoxic T-lymphocyte associated-protein 4 (CTLA-4) antibody, have led to improvements in survival when used in stage III and IV melanoma patients (Wolchok et al., 2017). Autologous T cells genetically engineered to express CAR specific for CD19 on B cells have been used to treat hematologic malignancies (Kalos et al., 2011). Despite successes with other cancers, similar checkpoint inhibitor and T cell therapies applied to GBM have not seen the same level of success.
This review aims to delineate the multiple avenues of immunotherapy that have been tested in glioblastoma treatment, including checkpoint inhibitors, vaccines, adoptive transfer of effector lymphocytes, and oncolytic virotherapy to stimulate an anti-tumoral immune response. We will also address the mechanisms of primary and secondary resistance seen in the immunologically unique environment of the CNS. Finally, we will discuss strategies to overcome the immunosuppressive tumor microenvironment and subsequently sensitize tumors to the immune response.
Immune checkpoints are naturally occurring co-inhibitory receptors expressed on the surface of T cells that play an important role in down-modulating the immune response and promoting self-tolerance (Pardoll, 2012). While these receptors initially evolved to prevent the development of autoimmunity and maintain immune homeostasis, they have been found to be upregulated in various forms of cancer promoting immune tolerance to tumor cells (Pardoll, 2012). To this end, inhibitors targeting checkpoint molecules such as CTLA4 and PD1 have been used to successfully treat patients with solid tumors. In the following section, we will be covering well-known checkpoint inhibitors and their successes and pitfalls in treating various cancers (Table 1).
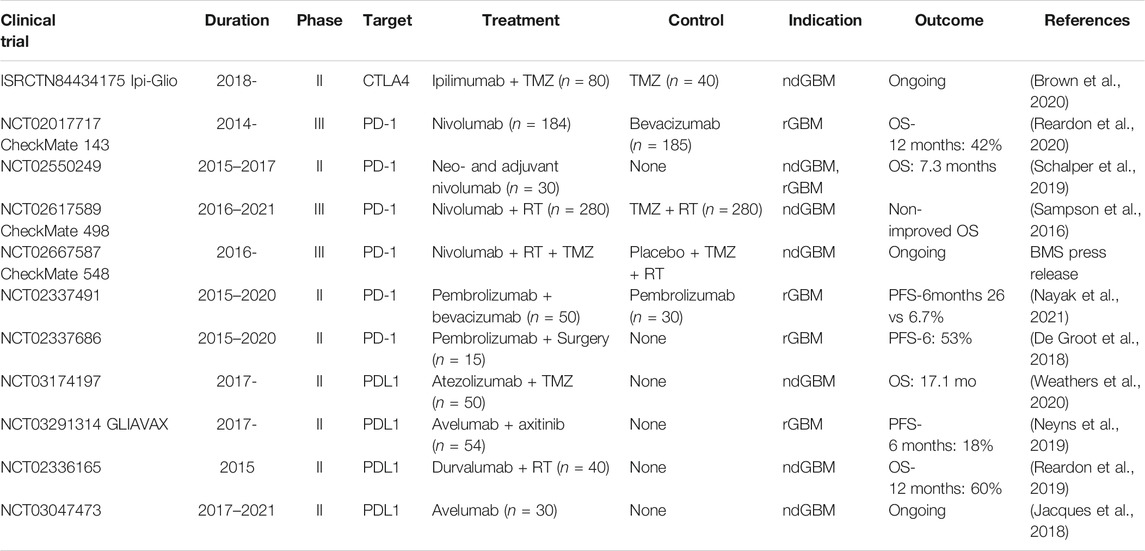
TABLE 1. Past and present phase II/III clinical trials with ICIs in glioblastoma.
The first checkpoint inhibitor approved for clinical use in cancer patients targeted CTLA4 (Hodi et al., 2003; Phan et al., 2003; Hodi et al., 2010; Hodi et al., 2003; Phan et al., 2003; Hodi et al., 2010), an inhibitory receptor expressed on regulatory T cells (Tregs), CD4, and CD8 T cells (Chan et al., 2014). Blockade of CTLA4 has been shown to increase the infiltrative T cell and decrease Treg response to tumor cells (Curran et al., 2010) by allowing the co-stimulatory receptor CD28 to bind CD80 (B7.1) and CD86 (B7.2) expressed on antigen-presenting cells (APC) (Linsley et al., 1994). Under homeostatic conditions, the interaction between CD28 and B7 provides a crucial second signal to activate T cells (Lenschow et al., 1996). This mechanism is well demonstrated by the rampant autoimmunity seen in CTLA4 knockout murine models (Tivol et al., 1995; Waterhouse et al., 1995).
Blockade of CTLA4 using the checkpoint inhibitor ipilimumab has been shown to improve survival in patients with unresectable stage III or IV melanoma when compared to use of a peptide vaccine alone (Hodi et al., 2010), and similar anti-CTLA4 therapies are currently being studied in clinical trials for cervical cancer, bladder cancer, and soft tissue sarcoma. In non-small cell lung cancer (NSCLC), the combination of anti-CTLA4 and anti-PD1 has been shown to delay time to deterioration compared to chemotherapy and resulted in an overall response rate of 30% in the CheckMate 568 study of 288 patients with stage IIIB/IV NSCLC (Ready et al., 2019; Reck et al., 2021). In preclinical murine models of GBM, CTLA4 blockade has been shown to decrease Treg populations and improve long-term survival (Fecci et al., 2007; Grauer et al., 2007). In patients with melanoma metastases to the brain, ipilimumab reaches a response rate of 18% in neurologically asymptomatic patients not on steroids and 5% in symptomatic patients taking steroids (Margolin et al., 2012). The use of ipilimumab with an anti-PD1 inhibitor in metastatic melanoma to the brain has also been shown to have improved intracranial efficacy than either monotherapy, likely via significant increase of CD8+ T cell migration to the brain (Taggart et al., 2018).
In GBM, the combination of ipilimumab and bevacizumab, a monoclonal antibody that inhibits vascular endothelial growth factor (VEGF), has been tested in 20 patients and demonstrated a 31% partial response rate with adverse events in 2 patients (Carter et al., 2016). While this suggests an overall benign safety profile for the combination of these two drugs to treat GBM, it has been noted in the literature that the mixture of newly diagnosed GBM (ndGBM) and recurrent GBM (rGBM) patients in the study, the use of radiographic response as a determinant of response rather than clinical status, and the higher rates of Grade 3 toxicity in combination therapy compared to bevacizumab alone (35 versus 11%) warrant closer investigation (Tini and Pirtoli, 2016). This has led to a formal phase I trial testing the maximally safe dose in three separate conditions: ipilimumab and TMZ, nivolumab and TMZ, and the combination of all three drugs in patients with gliosarcoma or ndGBM (National Cancer Institute (NCI), 2020).
Ipilimumab is also being tested as neoadjuvant treatment in combination with anti-PD1 inhibitor nivolumab for patients with surgically resectable GBM (MD PYW, 2021), and the same combination has been shown to be safe via intratumoural and intracavitary administration in a phase I trial for rGBM patients (Schwarze et al., 2020). In the ongoing Ipi-Glio trial, ipilimumab is being tested in combination with TMZ versus TMZ alone in rGBM patients with results pending (Brown et al., 2020).
The successes in targeting CTLA4 led to the development of similar antibodies against the checkpoint molecule PD1 and its ligand PDL1. PD1 is predominantly expressed on activated B and T cells, and it counters CD28-mediated stimulatory processes by binding its ligands PDL1 and PDL2 (Latchman et al., 2001; Keir et al., 2008). Much like the downstream consequences of CTLA and B7 binding, the interaction between PD1 and its ligands subsequently inhibits T cell activation and proliferation (Sharpe and Pauken, 2018), a mechanism highlighted by the presence of lymphoproliferation and spontaneous multi-organ autoimmunity in PD1 deficient murine models (Nishimura et al., 1998; Wang et al., 2005). PDL1 is not only expressed on immune cells but also on various tissues such as endothelial and epithelial cells, as well as classically ‘immune privileged’ sites such as the eye (Boussiotis, 2016). Its ubiquitous expression and upregulation on tumor cells suggest that PDL1 may play a role in immune evasion (Blank et al., 2005), making the PD1/PDL1 pathway an ideal target for checkpoint inhibition.
Two anti-PD1 inhibitors have been approved for clinical use: nivolumab and pembrolizumab. Initially tested in patients with melanoma, nivolumab was found to increase overall survival (72.9%) at 1 year in patients with metastatic melanoma compared to patients receiving dacarbazine (42.1%) (Robert et al., 2015). The combined use of nivolumab and ipilimumab (58%) was subsequently shown to increase rate of overall survival at 3 years compared to ipilimumab alone (34%) in a phase III trial from 2017 conducted in patients with advanced melanoma.345 However, similar findings have not been reproduced for nivolumab use in glioblastoma.
There have been three phase III trials testing the use of nivolumab in GBM: Checkmate 143, Checkmate 498, and Checkmate 548. Checkmate 143 tested use of nivolumab versus bevacizumab in patients with rGBM and found comparable overall survival (42%) in the two groups, with a higher objective response rate to bevacizumab (23.1%) than to nivolumab (7.8%) (Reardon et al., 2020). RNA sequencing of human glioma tissue after neoadjuvant nivolumab treatment did demonstrate increased immune cell infiltrate, T cell receptor clonal diversity, and expression of chemoattractant transcripts such as CCL4 and CCL3L1 compared to pre-treatment tissue (Schalper et al., 2019). However, despite the promotion of immune surveillance, nivolumab use did not significantly affect patient outcome.3738 Checkmate 498 tested nivolumab and radiation versus SOC TMZ and radiation in treatment-naïve, MGMT-unmethylated patients and found non-improved overall survival in the nivolumab-treated cohort (Sampson et al., 2016). Checkmate 548 tested the use of nivolumab and SOC to placebo and SOC in ndGBM patients with MGMT methylation but was unable to meet its primary endpoint of overall survival (Bristol-Myers Squibb, 2020a).
Pembrolizumab use has had a similar trajectory to that of nivolumab, finding limited success in GBM compared to melanoma. In a phase III trial testing pembrolizumab to ipilimumab for advanced melanoma patients (KEYNOTE-006), pembrolizumab use was associated with increased overall survival (Schachter et al., 2017). As adjuvant therapy in patients with resected stage III melanoma, pembrolizumab use (75.4%) continued to be associated with longer recurrence-free survival at 1 year than placebo (61%) (Eggermont et al., 2018). However, these findings did not translate to GBM, and a phase II trial using pembrolizumab alone versus with bevacizumab in patients with rGBM did not find a significant therapeutic benefit in either group (Nayak et al., 2021).
Atezolizumab, avelumab, and durvalumab are three anti-PDL1 inhibitors that have been approved for clinical use. Atezolizumab has seen promising results in both GBM and other cancers. In the IMvigor130 trial in urothelial cancer patients, the combination of atezolizumab and platinum-based chemotherapy was found to prolong progression-free survival compared to placebo and chemotherapy (Galsky et al., 2020). Atezolizumab was then found to be well-tolerated in rGBM patients, particularly in patients with a high peripheral CD4+ T cell count, (Lukas et al., 2018), and a phase II trial found the combination of atezolizumab TMZ, and radiation in ndGBM patients to be tolerable and efficacious with a median OS of 19 months and median PFS of 10.6 months (M.D. Anderson Cancer Center, 2021). However, avelumab has not seen a similar level of success in GBM, having failed to meet the threshold for justifying further investigation in the GLIAVAX trial testing axitinib and avelumab combination use in rGBM patients following SOC (Neyns et al., 2019). Durvalumab has been FDA approved for bladder cancer and non-small cell lung cancer (NSCLC) and is currently being tested in a phase II trial for newly diagnosed unmethylated GBM patients (Ludwig Institute for Cancer Research, 2021).
Lymphocyte activation gene-3 (LAG3) is a cell surface molecule that associates with the CD3/T cell receptor (TCR) complex to competitively bind MHC II molecules on antigen-presenting cells (APC), subsequently inhibiting immune cell proliferation (Long et al., 2018). Constant antigen exposure in the tumor microenvironment has been shown to upregulate LAG3 expression and contribute to immune cell exhaustion (Andrews et al., 2017). Its pervasive and aberrant expression in the tumor microenvironment has made it a target of interest in cancers that have seen limited success with established ICIs.
Preclinical data in murine GBM models has revealed improved survival in LAG3 knockout mice receiving anti-PD1 treatment compared to wild-type (WT) mice treated with anti-PD1, suggesting that LAG3 inhibition may potentiate the anti-tumoral effect of anti-PD1 (Harris-Bookman et al., 2018). The use of relatlimab, an anti-LAG3 monoclonal antibody, and nivolumab in combination is currently being tested in several clinical trials for GBM, hematologic malignancies, and other advanced solid tumors (Puhr and Ilhan-Mutlu, 2019). Of the anti-LAG3 drugs under development, relatlimab is the only to undergo phase III trials, currently for metastatic melanoma (Bristol-Myers Squibb, 2020b).
Peptide vaccines utilize in vitro-synthesized peptides to induce a lasting anti-tumor immune response (Kumai et al., 2017). The targets of peptide vaccines are either tumor-associated antigens (TAA) or tumor-specific antigens (TSA) (Calvo Tardón et al., 2019). TAAs are expressed in both non-malignant and malignant tissue but have higher expression in malignant tissue, while TSA are exclusively expressed in malignant tissue (Calvo Tardón et al., 2019). While TSAs are most often derived from non-synonymous single nucleotide variants (SNV), which are patient-specific, there has also been a push to use TSAs derived from alternative sources such as frameshift mutations, splice variants, fusion proteins, and endogenous retroelements, which have the benefit of being more likely to be shared among tumors and less likely to be patient-specific (Smith et al., 2019).
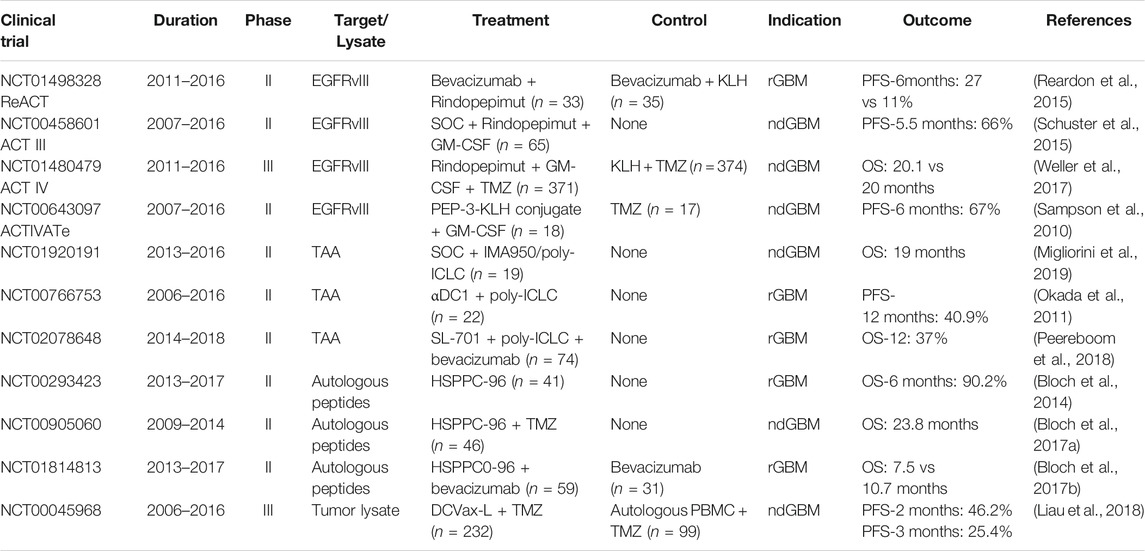
TABLE 2. Past and present phase II/III clinical trials with vaccines in glioblastoma.
Vaccines targeting TAAs have demonstrated non-improved overall survival in phase III trials for pancreatic cancer (Middleton et al., 2014) and renal cell carcinoma (Rini et al., 2016), but the use of a peptide vaccine against three TAAs (EphA2, IL13Rα2, and survivin) in children with recurrent high-grade gliomas was well tolerated and demonstrated a median PFS at 4.1 months and median OS at 12.9 months (Pollack et al., 2016). IMA950, a multi-peptide vaccine containing 11 tumor-associated peptides (Rampling et al., 2016), was well-tolerated in a phase I trial of ndGBM patients (Rampling et al., 2016) and shown to induce immunogenicity in the form of CD8+ T cell responses in 63.2% of ndGBM and grade III astrocytoma patients (Migliorini et al., 2019). However, unlike the synergy demonstrated between anti-LAG3 and anti-PD1 inhibitors, IMA950 vaccination did not improve response to bevacizumab in high grade glioma patients, and there were no significant differences in median PFS or OS between vaccinated and control patients (Boydell et al., 2019).
Epidermal growth factor receptor variant III deletion mutation (EGFRvIII) is the most well-studied TSA in GBM, and there have been several clinical trials conducted focusing on rindopepimut, a peptide vaccine targeting EGFRvIII (Swartz et al., 2014). The ReACT and ACT III are two phase II trials that have tested rindopepimut efficacy in targeting GBM. In the ReACT trial, combined treatment with rindopepimut and bevacizumab was tested against placebo in rGBM patients and found to have increased PFS at 6 months (27 vs 11%) (Reardon et al., 2015). The ACT III trial found promising PFS of 66% at 5.5 months and OS of 26% at 36 months in patients treated with rindopepimut and adjuvant TMZ after resection of EGFRvIII+ GBM (Schuster et al., 2015). However, the follow-up ACT IV phase III trial testing rindopepimut versus control did not find increased overall survival in ndGBM patients (Weller et al., 2017).
The isocitrate dehydrogenase 1 (IDH1) mutation is another target of interest due to its expression in over two-thirds of all low-grade gliomas (Sun et al., 2013). Vaccines designed with peptides containing the R132H mutation have elicited mutation-specific CD4+ responses in mice expressing human MHC class I and II (Schumacher et al., 2014). A similar peptide vaccine against R132H was safely tested in a phase I trial of grade III and IV astrocytoma patients and demonstrated 82% PFS at 2 years in patients with immune responses (Platten et al., 2021).
Heat shock proteins (HSP) have also been utilized to stimulate anti-tumor immune responses due to their intrinsic ability as molecular chaperones to carry peptides that are subsequently cross-presented to the immune system (Shevtsov and Multhoff, 2016). Heat shock protein-peptide complexes (HSPPC) have been developed using tumor-derived HSP to successfully generate CD4+ and CD8+ responses in mouse models of mammary and lung tumors (Manjili et al., 2003) (p110), (Wang et al., 2003), In GBM, HSPPC-96 is one such vaccine designed with gp96, a multifunctional HSP capable of inducing both innate and tumor-specific adaptive immunity (Schild and Rammensee, 2000). A phase I trial in ndGBM patients demonstrated a higher median OS for patients with high tumor-specific immune responses (>40.5 months) after receiving HSPPC-96 compared to patients with low responses (14.6 months), as well as a PFS at 6 months of 89.5% (Ji et al., 2018). Patients with rGBM who received HSPPC-96 in a phase II trial were found to have a median OS of 42.6 weeks, with 90.2 and 29.3% of patients alive at 6 and 12 months respectively. (Bloch et al., 2014).
DC vaccines utilize the cell’s potent antigen presentation capabilities to elicit anti-tumor immune responses (Filley and Dey, 2017). Autologous DCs are harvested from the patient and stimulated with tumor antigens ex vivo before re-infusion (Tacken et al., 2007). DCs can be pulsed with one or multiple antigens – both approaches have been explored in clinical trials.
Two phase I trials that pulsed DCs with Wilms’ tumor 1 (WT1) and six GBM TAAs respectively have found these vaccines to be safe in rGBM and ndGBM patients (Phuphanich et al., 2013; Sakai et al., 2015). In the latter study utilizing multiple antigens, six patients remained tumor-free at 40 months follow-up (Phuphanich et al., 2013). A phase II trial testing α-type 1 polarized DCs also demonstrated a sustained response in one rGBM patient and PFS at 12 months in nine out of 22 patients (Okada et al., 2011). The use of cytomegalovirus phosphoprotein 65 RNA (CMV pp65) to prime DCs is also an active area of interest given the expression of pp65 in human glioma samples (Cobbs et al., 2002). DCs pulsed with cytomegalovirus phosphoprotein 65 RNA (CMV pp65) have been tested in ndGBM patients, achieving a median PFS and OS of 25.3 and 41.1 months respectively with four out of eleven patients staying progression-free at 59 months (Batich et al., 2017).
DCVax-L is another DC-based vaccine that pulses dendritic cells with autologous tumor lysate. A phase I and II trial testing autologous DC-tumor vaccine therapy in both recurrent and newly diagnosed GBM patients achieved a median survival of 525 days with lymphopenia and reversible elevations in AST/ALT as the only two reported adverse effects (Chang et al., 2011). As a result, a phase III trial was conducted that combined DCVax-L with SOC for 331 ndGBM patients, which revealed a median overall survival of 23.1 months from surgery and a 3-years survival of 46.4% (Liau et al., 2018).
The adoptive transfer of tumor infiltrative lymphocytes (TIL) has been extensively studied in GBM. Resected tumor specimen and lymphocytes are taken out of the patient and co-cultured in vitro, and lymphocytes reactive against TAAs are selected for as TILs and subsequently expanded prior to infusion back into the patient (Wang et al., 2020). The safety of this method was established in a study of six recurrent glioma patients who received autologous TILs that were expanded in vitro with recombinant IL-2. In this study, the only complications were low grade fevers, asymptomatic hydrocephalus, and asymptomatic cerebral swelling, and half of the patients had a partial response at 6 months while 1 patient had complete response at 45 months (Quattrocchi et al., 1999). Although TILs are not typically genetically modified at baseline in adoptive transfer, there is also an ongoing phase I trial evaluating the safety of using TILs transduced to express PD1 antibody in glioma patients (MD YY, 2021). Other than TILs, the adoptive transfer of lymphokine-activated killer (LAK) cells, which are peripheral mononuclear blood cells (PBMC) incubated with IL-2 in vitro, has revealed higher median survival rates for rGBM patients compared to those that undergo reoperation for recurrence (Dillman et al., 19972004). The use of LAKs to treat GBM is also currently being studied in a phase II trial (Hoag Memorial Hospital Presbyterian, 2013).

TABLE 3. Past and present phase I/II clinical trials with adoptive T cell transfer in glioblastoma.
Chimeric antigen receptor (CAR)-modified T cells have emerged in recent years as a promising avenue of individualized immunotherapy. Autologous T cells are taken from the patient and are engineered to express a synthetic chimeric receptor that can recognize target cells independent of antigen processing and MHC restriction (Maus et al., 2014). CAR T-cell therapy targeting CD19 has demonstrated efficacy in treating acute lymphoblastic leukemia (Maude et al., 2014), and it is currently being studied for use in GBM. HER2-specific CAR T cells have demonstrated antitumor activity in preclinical patient-derived xenografts (Ahmed et al., 2010) and shown to be safe in phase I trials using autologous HER2-specific CAR virus-specific T cells in CMV seropositive patients with HER2-positive rGBM (Ahmed et al., 2017). Other cell surface markers such as EGFRvIII and ephrin-A2 (EphA2) have been found to be efficacious targets for CAR T cells in xenograft models of GBM (Chow et al., 2013; Sampson et al., 2014; Johnson et al., 2015). In patients, CAR T cells targeting EGFRvIII in a phase I trial led to marked expansion of tumor-infiltrating T cells but also increased expression of inhibitory regulatory T cells and upregulation of immunosuppressive markers indoleamine 2,3-dioxygenase 1 (IDO1) and PDL1 (O’Rourke et al., 2017). CAR T cells targeting IL13Rα2 have been shown to be well tolerated via intracranial delivery in 3 patients with rGBM (Brown et al., 2015) and led to regression of multifocal rGBM in both brain and spine for 7.5 months in a patient who received both intracavitary and intraventricular infusions of CAR T cells targeting IL13Rα2 (Brown et al., 2016). To overcome the inherent heterogeneity in GBM, there has also been work studying the use of a trivalent CAR T cell that targets IL13Rα2, EphA2, and HER2 that has demonstrated increased and sustained response in patient-derived xenografts (Bielamowicz et al., 2016).
Oncolytic viruses (OV) have demonstrated much promise in eliciting therapeutic responses in several cancers including GBM. The premise of using OVs is twofold in their ability to selectively infect tumor cells and induce tumor cell lysis while also releasing tumor antigens that elicit an anti-tumor immune response. (Foreman et al., 2017).
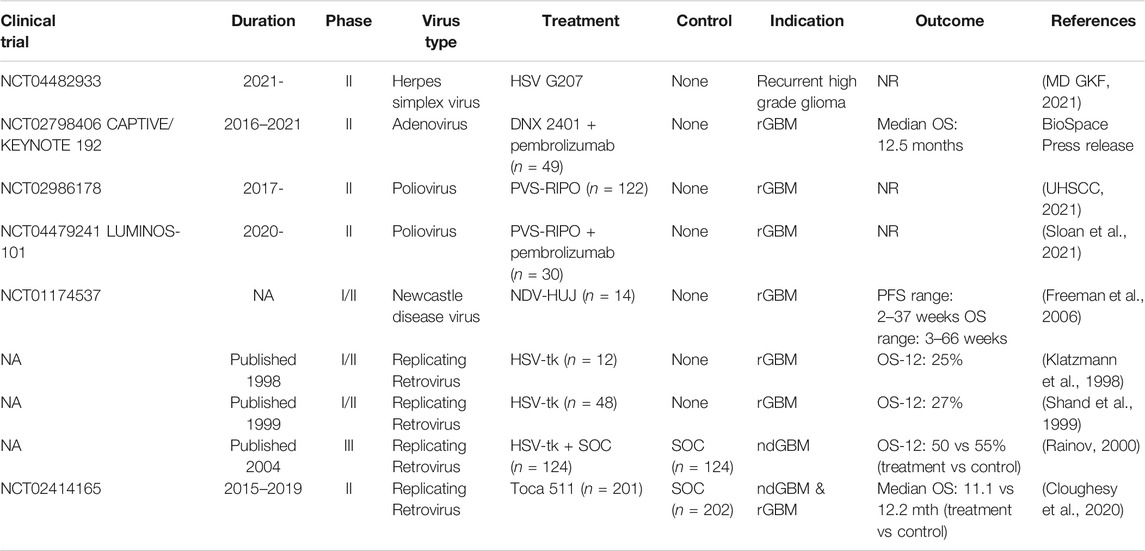
TABLE 4. Past and present phase II/III clinical trials with oncolytic virotherapy in glioblastoma.
The first OV therapy approved by the FDA in the United States was talimogene laherparepvec (tvec), an oncolytic herpesvirus, for advanced melanoma in 2015 (Conry et al., 2018), paving the way for the use of a host of mutated herpesviruses to treat GBM. Many of these mutated constructs are designed to allow preferential infection and lysis of tumor cells, allowing for viral propagation and stimulation of an immune response via release of tumor antigens (Yin et al., 2017). Two main HSV mutants tested in clinical trials for GBM are G207, capable of replicating in only dividing cells, and HSV1716, which can replicate in both dividing and nondividing cells (Immidisetti et al., 2021). There have been three phase I trials that demonstrated the safety and tolerability of G207 in rGBM and ndGBM patients (Markert et al., 2000; Markert et al., 2009; Markert et al., 2014), and similarly, three phase I trials have shown HSV1716 to be tolerable in ndGBM and rGBM patients (Rampling et al., 2000; Papanastassiou et al., 2002; Harrow et al., 2004). Additionally, there was a phase I trial testing intratumoral and peritumoral injection of HSV1716 after resection in pediatric patients with recurrent gliomas that was terminated due to low recruitment (Pediatric Brain Tumor Consortium, 2016). HSV1716 is currently undergoing testing in a phase II trial for children with recurrent high grade glioma (MD GKF, 2021). An alternate version of G207 named G47Δ is currently undergoing phase I and II studies in rGBM patients in Japan (JPRN-UMIN000002661). There is also a phase I trial currently underway testing M032, a genetically engineered HSV expressing IL12 transgene, in rGBM patients (MD JM, 2021).
Genetically manipulated adenovirus has also become a popular form of viral therapy in treating GBM. ONYX-015 is an adenovirus construct attenuated via deletion at the E1b locus that was one of the first such constructs to be tested in humans (Kirn, 2001). It was investigated in a 2004 phase I study of 24 rGBM patients who received intratumoral injections with a median survival of 6.2 months (Chiocca et al., 2004). However, attention ultimately shifted to other forms of adenovirus constructs for multiple reasons, including a lack of response to ONYX-015 as a single agent for solid tumors in multiple trials (Kirn, 2001).
There is now much work surrounding DNX-2401, a replication-competent adenovirus that is unable to bind healthy cells with intact retinoblastoma pathways and thus selectively binds tumor cells (Philbrick and Adamson, 2019) (p2401). A phase I trial for DNX-2401 tested dose escalation protocols via either single intratumoral injection or permanently implanted catheter followed by tumor resection for both groups and resulted in 5 (20%) patients with over 3 years of survival in the first group and 2 (17%) patients with over 2 years of survival in the second group (Lang et al., 2018). DNX-2401 has been demonstrated to promote a shift towards the M1 macrophage phenotype in the CSF of treated GBM patients compared with controls, suggesting a treatment-mediated protumoral shift in the immune landscape (Van den Bossche et al., 2018). A phase Ib trial has been completed testing the use of DNX-2401 alone versus in combination with interferon gamma (IFN-γ); while IFN-γ did not provide additional survival benefit, DNX-2401 alone appeared to provide an OS-12 of 33% across 27 patients (Lang et al., 2017). The recently completed phase II CAPTIVE/KEYNOTE 192 trial testing DNX-2401 in combination with pembrolizumab in rGBM patients has reported positive results with a median OS of 12.5 months (DNAtrix, 2021).
PVS-RIPO is a replication-competent polio-rhinovirus chimera that selectively infects cells expressing CD155 and demonstrates attenuated neurovirulence via substitution of the native internal ribosome entry site (IRES) for that of rhinovirus (Gromeier and Nair, 2018). Preclinical studies have demonstrated that PVS-RIPO infection may induce dendritic cell and neutrophilic recruitment to the tumor site in vivo (Gromeier and Nair, 2018; Mosaheb et al., 2020). A phase I trial testing intratumoral injection of PVS-RIPO in 61 rGBM patients demonstrated a higher OS rate of 21% at 36 months compared to historical controls, with 2 patients surviving for more than 70 months (Desjardins et al., 2018). The favorable results from phase I have led to two ongoing phase II trials testing PVS-RIPO alone in 122 rGBM patients (UHSCC, 2021) and testing PVS-RIPO in combination with pembrolizumab in 30 rGBM patients in the LUMINOS-101 trial. (Istari Oncology, 2021).
NDV, like much of the viruses discussed here, is capable of selectively infecting and inducing lysis in tumor cells from a variety of cancers (Matveeva et al., 2015). There have been three strains developed and tested in clinical trials over the years: MTH-68, NDV-HUJ, and Ulster. The first reported use of the MTH-68 strain to treat CNS tumors occurred in 1999 in pediatric patients with rGBM. This was followed up with a 2004 study that tested MTH-68 in four patients with high grade glioma that resulted in survival rates ranging from five to 9 years (Csatary and Bakács, 1999; Csatary et al., 2004). NDV-HUJ was tested in a 2006 phase I/II trial of 14 rGBM patients that had been refractory to treatment, with minimal Grade I and II toxicities only and three long-term survivors who all eventually progressed either clinically or radiologically (Freeman et al., 2006). In 2001, Schneider et al. tested autologous tumor cells infected with Ulster NDV and subsequently irradiated in 11 patients after surgical resection and found comparable survival compared to patients who received chemotherapy instead of virotherapy (Schneider et al., 2001). A similar approach was taken in 23 ndGBM patients who underwent maximal resection and received ATV-NDV, an anti-tumor vaccine infected with the Ulster NDV strain; the results demonstrated significantly increased rates of OS-1 (91 versus 45%) and OS-2 (39 versus 11%) compared to the control group (Steiner et al., 2004).
Reovirus is a double-stranded RNA virus that preferentially infects and lyses tumor cells in part via overactivated Ras signaling pathways that enhance proteolytic viral disassembly in malignant cells (Coffey et al., 1998; Norman et al., 2004; Alain et al., 2007). The application of reovirus for treating tumors was first accomplished via phase I studies on prostate cancer and cutaneous metastases from systemic cancer before eventually being tested on malignant gliomas by Forsyth et al. (2008) Nine of 12 patients were treated for GBM in a dose escalation protocol with no observable adverse events and survival ranging from 6 to 63 weeks (Forsyth et al., 2008). Similar findings were replicated by Kicielinski et al. when applying Reolysin, a wild-type reovirus, to malignant gliomas in a phase I study (Kicielinski et al., 2014). Results were promising, with survival ranging from 14 to 141 weeks, which prompted the designation of orphan drug status to Reolysin for the treatment of malignant glioma by the FDA in 2015 (Jaime-Ramirez et al., 2017). In vitro studies have demonstrated that reovirus administration induces DC maturation, stimulates proinflammatory cytokine production, including IFN-alpha, TNF-alpha, and IL-6, and increases NK cell cytolytic activity on tumor cells (Errington et al., 2008). Human studies have confirmed the capacity for reovirus to generate a pro-inflammatory environment, with intravenous delivery of reovirus to brain tumor patients being associated with increased CD8+ T cell tumor infiltration, likely attributed to the observed increase in CCL3, CCL4, and ICAM expression, which mediate migration to sites of inflammation (Samson et al., 2018). However, tumors from reovirus-treated patients were also noted to have greater expression of PD-1 and PD-L1 immune checkpoint proteins, highlighting a potential response mechanism by the tumor to counteract the stimulated immune system. While reovirus harbors significant therapeutic utility for the treatment of GBM, further characterization of the tumor’s response to infection is required, as well as consideration for combinatorial treatment with immune checkpoint blockades, such as anti-PD-1/PD-L1. As such, reovirus is no longer being investigated as a monotherapy, and further investigation with other treatment modalities is currently underway (Müller et al., 2020).
Parvovirus, specifically H-1 parvovirus (H-1PV), became the focus of many decades of cancer research after discovering that it possesses a natural tropism for human cancer cells in 1961 (Toolan, 1961). The rat is the natural host of H-1PV, and H-1PV has been shown to be nonpathogenic to humans by failing to produce new virus particles and induce cell lysis in normal, non-transformed cells (Angelova et al., 2015). However, it has been shown to infect and cause cell death in a wide range of cancers, including tumors of the bone, brain, breast, colon, lung, pancreas, and skin, as well as hematological disease such as Burkitt lymphoma, cutaneous T-cell lymphoma, and diffuse large B-cell lymphoma (Angelova et al., 2017; Bretscher and Marchini, 2019). The oncotropism of H-1PV involves a myriad of processes, including but not limited to factors essential for viral entry (PKCalpha, CDK1), replication (cyclin A/CDK2, E2F), and maturation (XPO1, PKB, PKC), as well as deficiency of mechanisms necessary to counter viral infection (type I IFN stress response), in tumor cells (Angelova et al., 2015). In vitro studies of H-1PV found selective killing of glioma cells via a cathepsin-mediated mechanism, which translated to prolonged survival in glioma-bearing rats treated with intratumoral, intravenous, and intranasal H-1PV inoculation, again via elevated cathepsin activation and activity (Di Piazza et al., 2007; Geletneky et al., 2010). The first clinical trial for GBM was then initiated by Geletneky et al., who found H-1PV (ParvOryx01) to be an immunogenic stimulus in patients with recurrent GBM (Geletneky et al., 2017). Treated patients were found to have strong leukocytic infiltration, predominantly CD8+ T cells and, to a lesser degree, CD4+ T cells. Additionally, a promising finding was that the increased CD8+ T cell population did not coincide with a responsive increase in tumor-invading Tregs that is typical of GBM. This is in line with in vitro studies that have found H-1PV to capable of suppressing the activity of Tregs (Moralès et al., 2012). Given these findings, in addition to a case series of patients successfully treated with a combination of NDV, parvovirus, and vaccinia virus, further characterization of the anti-tumor and immune sensitizing effects of H-1PV and investigation of its clinical effects in GBM through a randomized controlled trial is required (Gesundheit et al., 2020).
Replicating retroviral vectors have been harnessed for their ability to deliver ‘suicide genes,’ or genes that encode for proteins capable of converting non-toxic into toxic drugs upon delivery of a prodrug (Li et al., 2021). This was the basis of a retroviral vector encoding for HSV thymidine kinase (HSV-tk), which could convert ganciclovir (GCV) into GCV triphosphate, an inhibitor of DNA replication. HSV-tk was tested in 15 GBM patients who received intratumoral injection of HSV-tk followed by intravenous GCV administration, with 1 long-term survivor at 220 weeks (Ram et al., 1997). Twelve rGBM patients exhibited no serious adverse events in a phase I/II study after receiving intratumoral injection of HSV-tk cells intra-operatively, with 25% of patients living longer than 12 months (Klatzmann et al., 1998). A similar study in 13 ndGBM patients demonstrated significantly elevated soluble Fas ligand and IL-12 levels in serum of HSV-tk treated patients versus controls but did not find increased tumor-infiltrating lymphocytes at the resection cavity or activation of T or NK cells (Rainov et al., 2000). Another phase I/II clinical trial in 48 rGBM patients who received intracerebral injection of HSV-tk demonstrated no serious adverse events or evidence of virus in the serum or tissue at time of repeat resection (Shand et al., 1999). However, a phase III trial studying the effects of HSV-tk and GCV treatment in 248 ndGBM patients found no significant difference in PFS and median survival between treated and control patients, which was hypothesized to be due to poor transduction efficiency (Rainov, 2000).
Toca 511 is a replication-competent retroviral vector that delivers cytosine deaminase (CD) to convert prodrug 5-fluorocytosine (5-FC) to antineoplastic agent 5-fluorouracil (5-FU) (Huang et al., 2013). Toca 511 was tested in 45 high grade glioma patients in a phase I trial that demonstrated a significantly longer OS of 13.6 months compared to control (Cloughesy et al., 2016). These favorable results led to a phase II trial testing Toca 511 to SOC in GBM patients and demonstrated no significant difference in median survival between the two groups (Cloughesy et al., 2020).
Despite the successes seen with immunotherapy against GBM in preclinical models, these results have not translated well in the clinical setting, as fewer than 10% of GBM patients have been shown to respond to immunotherapy (McGranahan et al., 2019) (p2401). As such, it is important to understand the intrinsic and adaptive forms of resistance exhibited in GBM (Table 5).
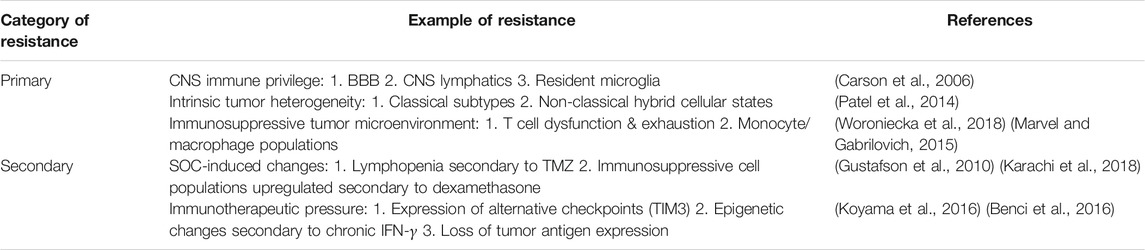
TABLE 5. Mechanisms of immunotherapy resistance in glioblastoma.
Several factors contribute to immune evasion in GBM. Unlike other cancers, GBM has been known to display extensive intratumoral heterogeneity (Patel et al., 2014), which confounds efforts to identify high-quality clonal neoantigens regardless of the form of immunotherapy trialed. While GBM has traditionally been classified into proneural, classical, mesenchymal, and neural subsets, single cell RNA-sequencing has revealed cross-over among the subtypes within the same tumor and the presence of hybrid cellular states (Patel et al., 2014). Genomic studies of GBM heterogeneity have revealed the presence of a CD133+ chemo- and radio-resistant cancer stem cell (CSC) population responsible for tumor initiation and found to have higher expression in recurrent tumors (Bao et al., 2006; Liu et al., 2006; Tamura et al., 2013; Qazi et al., 2017), but even then, CD133+ has failed to be a universal marker of CSCs given the discovery of similarly functioning CD133- cell populations (Chen et al., 2010).
In addition to the extensive phenotypic heterogeneity of cells within a tumor, there is a strong immunosuppressive microenviroment within GBM tumors that remains a major barrier to immunotherapy efficacy (Moserle and Casanovas, 2013). At baseline, GBM patients exhibit a lower number of circulating T cells despite being treatment-naïve (Chongsathidkiet et al., 2018). This phenomenon has been attributed to T cell sequestration in the bone marrow in the setting of GBM as well as other intracranial tumors, due to tumor-mediated internalization of G-protein coupled receptor sphingosine-1-phosphate receptor 1 (S1P1) (Chongsathidkiet et al., 2018). The same study demonstrated reversal of T cell sequestration in murine models of GBM upon inhibiting S1P1 internalization (Chongsathidkiet et al., 2018).
The circulating T cells that are available in the setting of GBM often display dysfunctional phenotypes including but not limited to tolerance and exhaustion (Brooks et al., 1977; Woroniecka et al., 2018). The exhausted phenotype is commonly seen in chronic viral infections and various cancers and has recently been suggested to be irreversible in spite of antigen clearance due to a novel concept referred to as ‘epigenetic scarring’ (Abdel-Hakeem et al., 2021). Persistent proliferation in the setting of chronic antigenic exposure can also lead to shortening of telomeres resulting in T cell senescence (Woroniecka et al., 2018). Importantly, GBM utilizes naturally occurring mechanisms of immune tolerance to promote FasL-mediated peripheral deletion of T cells and recruitment of Tregs via expression of IDO1 on dendritic cells and T cell immunoglobulin- and mucin domain-containing molecule 4 (TIM4) on macrophages (Xu et al., 2011; Choi et al., 2012; Woroniecka et al., 2018). Beyond lymphocytes, the presence of myeloid-derived suppressor cells (MDSC) in both peripheral blood and intracranially has been shown to contribute to immune suppression and tumor progression via expression of arginase, inducible nitric oxide synthase, and reactive oxygen or nitrogen species (Bronte and Zanovello, 2005; Gabrilovich and Nagaraj, 2009; Marvel and Gabrilovich, 2015). Tumor-associated macrophages (TAM) have been similarly implicated via secretion of immunosuppressive cytokines IL10 and TGFβ secondary to induction by CSCs. (Wu et al., 2010; Zhou et al., 2016).
While the central nervous system (CNS) is known to be a site of immune privilege secondary to naturally occurring mechanisms of immune homeostasis such as the blood brain barrier (BBB) and resident microglia (Desland and Hormigo, 2020), the immunosuppression intrinsic to GBM and independent of location in the CNS is clear when comparing the microenvironment and immunotherapeutic results of GBM to that of brain metastases (Friebel et al., 2020). Single cell analysis has revealed that the GBM microenvironment has higher expression of tissue-resident microglia while the metastatic tumor environment has higher expression of tissue-invading leukocytes (Friebel et al., 2020). At the same time, 80% of the leukocytes expressed in the GBM microenvironment were found to be classically immunosuppressive TAMs while most leukocytes found in the metastatic tumor environment were T cells (Friebel et al., 2020). These dichotomous immune findings may help explain why ICIs have seen more success in treating patients with brain metastases from melanoma or NSCLC compared to those with GBM (Goldberg et al., 2016; Tawbi et al., 2018; Kluger et al., 2019).
GBM has been shown to acquire forms of secondary resistance in the setting of recurrence and treatment. Patients with rGBM who initially responded to anti-PD1 immunotherapy have been found to have loss of neo-epitopes and delayed upregulation of immunosuppressive genes upon recurrence (Zhao et al., 2019). Despite the expression of EGFRvIII in 19% of ndGBM, a vaccine trial targeting EGFR found that 82% of tumors had lost EGFRvIII expression upon recurrence (Sampson et al., 2010; Brennan et al., 2013).
The current standard of care for GBM can also further exacerbate immune evasion. Dexamethasone, which is commonly used to reduce peri-tumoral edema and temporarily improve neurological symptoms, has been shown to upregulate expression of CTLA-4 on T cells and subsequently dampen patient response to checkpoint blockade (Giles et al., 2018). A unique phenotype of altered monocytes (CD14+ HLA-DR-) has also been identified to represent an immunosuppressive population whose levels increase in response to dexamethasone treatment (Gustafson et al., 2010). TMZ treatment may also result in profound lymphopenia, and in GBM patients, TMZ-induced lymphopenia is worsened by both the absence of a compensatory increase in proliferation-inducing cytokines and the failure of adoptive transfer to increase T cell counts (Karachi et al., 2018). Radiotherapy alone promotes secretion of classically immunosuppressive cytokines IL-6, IL-8, IL10 (Tabatabaei et al., 2017; Authier et al., 2015) but when combined with chemotherapy as in the current SOC, the combination has been shown to severely deplete CD4+ and CD8+ T cells and increase the proportion of Tregs (Fadul et al., 2011). In a study of 96 patients with high grade gliomas, patients with CD4+ counts under 200 at 2 months after therapeutic initiation were found to have significantly shorter survival than those with higher counts (13.1 vs 19.7 months), highlighting the importance of understanding the effects of treatment in contributing to drug resistance in GBM (Grossman et al., 2011).
The use of immunotherapeutic agents discussed here may also contribute to secondary resistance. In melanoma patients treated with anti-PD1 blockade who subsequently relapsed, genomic analysis of paired primary and recurrent tumor revealed alterations in β2 microglobulin and JAK1/2 genes that were the main drivers of acquired PD1 resistance (Shin et al., 2017). It has also been shown in lung cancer that downregulation of one checkpoint may lead to subsequent upregulation of other checkpoint molecules, such as the upregulation of TIM3 in the setting of anti-PD1 blockade (Koyama et al., 2016). In glioblastoma, the use of CAR T cells targeting EGFRvIII has been linked to a compensatory influx of immunosuppressive Tregs into the tumor microenvironment as well as loss of EGFRvIII expression in surgically resected tumors post-treatment (O’Rourke et al., 2017). Similarly, the use of CAR T cells targeting IL13Rα2 was shown to lead to improved survival in preclinical murine models, but recurrent gliomas post-treatment experienced downregulation of the target antigen, suggesting that the use of CAR T cells targeting a singular antigen may select for GBM cells that lack expression and subsequently allow for disease progression (Krenciute et al., 2017).
The limited clinical success seen in the use of immunotherapeutic agents against GBM is likely due to a multifactorial process of immunosuppression, local immune cell dysfunction, and tumor cell heterogeneity, as highlighted by the aforementioned mechanisms of tumor resistance. As a result, adjuvant approaches that prime the tumor microenvironment for a robust, antitumor immune response have been the focus of active investigation (Lim et al., 2018). In this final section, we will highlight strategies that remodel the tumor microenvironment for immunotherapy by downregulating its immunosuppressive qualities and upregulating its cytolytic potential, as well as their potential and/or observed adverse effects.
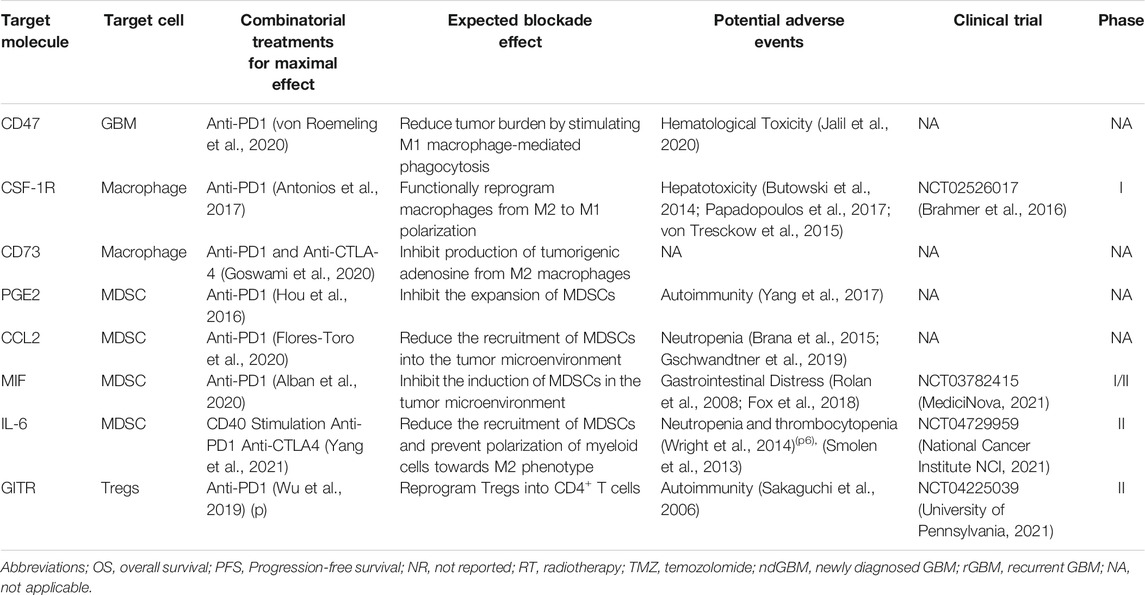
TABLE 6. Immunotherapy sensitization strategies in glioblastoma.
Many efforts have been directed towards targeting the myeloid compartment, specifically M2-type TAMs and MDSCs, given their wide variety of immunosuppressive functions and dense abundance in the tumor mass (Glass and Synowitz, 2014). CD47, a ubiquitously expressed protein on the surface of GBM cells, interacts with signal-regulatory protein alpha (SIRP
CD47 inhibitors have been tested in several phase I/II clinical trials for hematological and advanced solid malignancies (Jalil et al., 2020). While preclinical studies in mice have shown good tolerance with minimal signs of toxicity, clinical trials have encountered issues regarding hematological toxicity including anemia, leukopenia, and thrombocytopenia (Gholamin et al., 2017; Li et al., 2018). CD47 is ubiquitously expressed by non-cancerous cells of the hematopoietic system, which makes them an alternative binding site for systemically delivered anti-CD47 antibodies (Ishikawa-Sekigami et al., 2006; Hu et al., 2020). Consequently, non-tumor binding of antibodies was found to induce unintentional FcR-mediated phagocytosis of red blood cells leading to toxic anemia (Zhang et al., 2020). Studies have experienced success in mitigating hematological toxicity by delivering a low, priming dose of anti-CD47 antibodies to induce a predictable, transient anemia and compensatory reticulocytosis for non-Hodgkin’s lymphoma (Advani et al., 2018). However, future investigations of applying anti-CD47 treatment to GBM must still consider the possibility of hematological toxicity and develop effective strategies to bypass it.
Similar to CD47, colony stimulating factor-1 receptor (CSF-1R), a member of the receptor protein tyrosine kinase (rPTK) family, has also been implicated in the differentiation of myeloid cells into M2 macrophages (Dai et al., 2002). In GBM xenograft models, CSF-1R inhibition decreases M2 markers on TAMs but does not deplete the cell population due to tumor-secreted factors, notably GM-CSF and IFN-
In addition to targeting the polarization of M2 macrophages, potential adjuvant treatments have also aimed to target the function of M2-type macrophages. Specifically, CD73, an ectonucleotidase preferentially expressed on M2 polarized macrophages, interacts with its upstream signaling molecule CD39 to facilitate the production of adenosine from extracellular ATP (Zanin et al., 2012; Antonioli et al., 2013). Adenosine is a known promoter of tumor proliferation and angiogenesis, and in the case of GBM, it has been implicated in the development of TMZ chemoresistance and CD8+ T cell dysfunction via the A2B adenosine receptor (Takenaka et al., 2019; Yan et al., 2019). CD73 expression on myeloid cells has also been correlated with higher co-expression of the immunosuppressive and protumorigenic CCR2, CCR5, ITGAV, and CSF-1R chemokine receptors (Goswami et al., 2020). Clinical trials targeting these chemokine receptors are underway, but CD73 may be a more relevant target given its high co-expression and the limited success observed thus far. A preliminary study that induced prolonged survival in CD73 knockout models of GBM treated with dual blockade of PD-1 and CTLA-4 highlights the potential of CD73 for combination therapy and need for further investigation (Goswami et al., 2020). Given that clinical trials focusing on targeting CD73 in GBM have yet to commence or are ongoing in other malignances, there is limited awareness of its associated adverse events beyond results from animal studies (Jin et al., 2021). While studies in mice have shown that CD73 plays a role in platelet aggregation and protection of the heart, kidney, and lungs from ischemia, animal studies have shown good tolerability to CD73 blockade (Stagg, 2012; Antonioli et al., 2016; Azambuja et al., 2020). However, these results should not be used to extrapolate responses in humans, and a better understanding of the safety of targeting CD73 will be had following the conclusion of ongoing clinical trials.
Myeloid-derived suppressor cells (MDSC), a heterogenous population of CD11b+ CD33+ HLA-DR- myeloid cells found in the peripheral blood and tumor mass of GBM patients, have also emerged as a potential target for sensitizing the tumor microenvironment to immunotherapy given their myriad immunosuppressive functions associated with poor prognosis (Almand et al., 2001; Alban et al., 2018). MDSCs have been implicated in GBM tumor progression through the inhibition of T cells, NK cells, dendritic cells, and macrophages, the expansion and differentiation of T regulatory cells, and the promotion of immunosuppressive B cells (Raychaudhuri et al., 2011; Mi et al., 2020). To control their tumorigenic activity, approaches have attempted to target the infiltration, expansion, and activation of MDSCs. Prostaglandin E2 (PGE2) and C-C motif chemokine ligand 2 (CCL2) have both been associated with the recruitment of MDSCs to tumor tissue, while macrophage migration inhibitory factor (MIF) signaling through the chemokine ligand 2 (CXCL2) and MIF/C-X-C motif chemokine receptor 2 (CXCR2) axis has been linked to the differentiation of myeloid cells into MDSCs (Simpson et al., 2012; Chang et al., 2016).
In preclinical models, inhibition of PGE2 production through COX2 inhibitors, specifically acetylsalicylic acid and celecoxib, led to both the suppression of gliomagenesis and reduction of MDSCs in the tumor microenvironment through a decrease in CCL2 (Fujita et al., 2011; Shono et al., 2020). Furthermore, COX2 inhibition in GBM has also garnered interest for its radiosensitizing effects in vivo (Ma et al., 2011). While the enthusiasm for COX2 as a therapeutic target has stagnated due to multiple cohort studies and clinical trials that inversely correlated COX2 inhibitors with survival, its efficacy as an immunotherapeutic adjuvant has yet to be thoroughly investigated and warrants further study (Qiu et al., 2017). Alternatively, it may also be appropriate to shift focus towards PGE2 as a therapeutic target rather than COX2 itself, especially given the broad range of well-known adverse effects associated with COX2 inhibition such as hypertension, congestive heart failure exacerbation, renal impairment, and other cardiovascular events (Mukherjee et al., 2001; Wright, 2002). There are currently no clinical trials focused on targeting PGE2. However, an oncolytic vaccina virus was recently designed to inactivate PGE2 and successfully reduce the number of MDSCs and T regulatory cells in a mouse tumor model as well as potentiate the response to anti-PD1 therapy (Hou et al., 2016). Thus, the safety associated with targeting PGE2 is currently unknown beyond those associated with COX2 inhibition, however, downregulating MDSCs will pose the risk of autoimmune side-effects such as autoreactive T-cells, more so than traditional immunotherapies given the wider spectrum of activity in MDSCs than targeted immune checkpoint inhibitors (Yang et al., 2017).
CCL2 inhibition through anti-CCL2 monoclonal antibodies (mAb) has also experienced success in reducing the population of MDSCs and improving survival in GBM xenograft models (Zhu et al., 2011). Additionally, inhibition of the CCL2 receptor (CCR2) in conjunction with PD-1 checkpoint inhibition extended survival in GBM-bearing mice, highlighting its ability to augment immunotherapy (Flores-Toro et al., 2020). Clinical trial using carlumab monotherapy, a human IgG1k monoclonal antibody against CCL2, had little success in patients with advanced solid tumors and metastatic prostate cancer, however, results from CCL2 blockade with immune checkpoint blockade have yet to be reported (Pienta et al., 2013; Sandhu et al., 2013). While carlumab clinical trials were well-tolerated with mild-to-moderate adverse events, neutropenia occurred commonly in a multicenter phase 1b study, which may be due to the elimination of CCL2’s anti-apoptotic effect in neutrophils and increase the risk of infection in patients (Brana et al., 2015; Gschwandtner et al., 2019).
The MIF signaling axis has also recently garnered interest as a target given the high levels of the MIF non-cognate receptor CXCR2 expressed on MDSCs and the enhanced CD8+ T cell activity observed in the tumor microenvironment following treatment with ibudilast, an inhibitor of MIF-CD74 interactions (Alban et al., 2020). Ibudilast is currently being investigated in clinical trials as an adjuvant to TMZ, given its ability to sensitize GBM cells to TMZ, safely penetrate the BBB, and confer minimal adverse events, with phase 1 studies and clinical trials for other neurological diseases such as multiple sclerosis reporting gastrointestinal side effects, headaches, and depression as the most concerning (Rolan et al., 2008; Fox et al., 2018). However, given the preliminary findings of increased lymphocyte activation, additional clinical trials pairing ibudilast with immune checkpoint inhibitors like anti-PD-1 to maximize cytolytic activity against tumor cells should also be considered.
IL-6 drives myeloid-based immunosuppressive activity through the induction of PD-L1 expression on MDSCs (Lamano et al., 2019). While IL-6 neutralization has been shown to enhance T cell tumor infiltration, it alone does not sensitize the tumor to immune checkpoint blockade via anti-PD-1 or anti-CTLA-4 (Yang et al., 2021). However, CD40 stimulation in conjunction with IL-6 inhibition and PD-1 and CTLA-4 immune checkpoint blockade did produce clinically relevant responses in syngeneic GBM models, notably the reversal of macrophage-mediated immune suppression and extended survival Yang et al., 2021. This finding supporting dual-targeting of IL-6, CD40, and multiple immune checkpoints emphasizes the paradigm shift towards strategically selecting multiple interrelated targets that increase the possibility of a successful response to immunotherapy. An ongoing clinical trial investigating the addition of tocilizumab, a monoclonal antibody against IL-6, alongside atezolizumab and fractionated stereotactic radiation therapy in recurrent GBM will shed more light on the clinical efficacy of concurrent IL-6 and PD-L1 blockade in GBM. Given the use of tocilizumab for other conditions such as rheumatoid arthritis, adverse effects are minimal, acceptable, and promising for utilization in GBM treatment. Complications mainly consist of neutropenia and rare thrombocytopenia given IL-6 receptors on neutrophils that may bind monoclonal antibodies and lead to opsonization and neutrophil phagocytosis (Wright et al., 2014) (p6), (Smolen et al., 2013).
In addition to cells from the myeloid compartments, cells derived from the lymphoid lineage also possess immunosuppressive functions and serve as potential therapeutic targets, most notable of which are Tregs. Tregs are characterized as a CD25+ FOXP3+ subset of CD4+ cells that divert immune responses away from cytotoxic Th1-mediated responses and towards Th2-mediated responses in part through increasing the expression of CTLA-4 and decreasing the secretion of IL-2 and IFN-
Despite its immunosuppressive mechanisms documented earlier, radiotherapy can also sensitize the immune response via its ability to increase MHC-1 expression on the surface of tumor cells, leading to better antigen presentation and recognition by cytotoxic T cells (Rajani et al., 2019; Sevenich, 2019). Antiangiogenic therapies have also been considered as a treatment option for overcoming resistance to immune checkpoint therapies in GBM. Dual blockade of VEGF and Ang-2 with concurrent anti-PD-1 treatment has been shown to extend survival, increase cytotoxic T lymphocyte infiltration, and decrease MDSC and Treg abundance (Fukumura et al., 2018; Di Tacchio et al., 2019).
Overall, clinical trials investigating multimodal therapies in GBM that integrate conventional treatments, such as radiotherapy and anti-angiogenic therapy, with novel immunotherapies and strategies for bypassing tumor resistance are currently underway. This combinatorial approach to treatment exemplifies the new frontier of GBM immunotherapy that leverages strategic combinations of multiple treatments to reverse immunosuppression within the microenvironment and maximize the potential of immunotherapy.
Much progress has been made in the landscape of immunotherapies designed to treat glioblastoma. Several immune checkpoint inhibitors have been adopted from other cancer trials for use in glioblastoma, and although the uniquely resistant environment of glioblastoma has prevented similar successes seen in other cancers, several advances have been made in introducing new vaccine, adoptive T cell, and oncolytic virotherapies to induce both tumor lysis and an anti-tumor immune response. New forms of sensitization to overcome primary and adaptive resistance include myeloid and lymphoid-targeting strategies, as well as the introduction of multimodal treatments integrated with conventional standard of care. Looking forward, it is important to recognize the intrinsic differences between glioblastoma and other cancers that the aforementioned therapies have been trialed in, in order to design more targeted treatments that can overcome the uniquely immunosuppressive environment of GBM.
Conceptualization: MA, RM and EW; Writing - Original draft: EW, J-SC and SJ; Visualization: EW, SG and AB; Writing - Review & editing: MA, RM and AH; Supervision: MA.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abdel-Hakeem, M. S., Manne, S., Beltra, J.-C., Stelekati, E., Chen, Z., Nzingha, K., et al. (2021). Epigenetic Scarring of Exhausted T Cells Hinders Memory Differentiation upon Eliminating Chronic Antigenic Stimulation. Nat. Immunol. 22 (8), 1008–1019. doi:10.1038/s41590-021-00975-5
Advani, R., Flinn, I., Popplewell, L., Forero, A., Bartlett, N. L., Ghosh, N., et al. (2018). CD47 Blockade by Hu5F9-G4 and Rituximab in Non-hodgkin's Lymphoma. N. Engl. J. Med. 379 (18), 1711–1721. doi:10.1056/NEJMoa1807315
Ahmed, N., Brawley, V., Hegde, M., Bielamowicz, K., Kalra, M., Landi, D., et al. (2017). HER2-Specific Chimeric Antigen Receptor-Modified Virus-specific T Cells for Progressive Glioblastoma. JAMA Oncol. 3 (8), 1094. doi:10.1001/jamaoncol.2017.0184
Ahmed, N., Salsman, V. S., Kew, Y., Shaffer, D., Powell, S., Zhang, Y. J., et al. (2010). HER2-specific T Cells Target Primary Glioblastoma Stem Cells and Induce Regression of Autologous Experimental Tumors. Clin. Cancer Res. 16 (2), 474–485. doi:10.1158/1078-0432.CCR-09-1322
Alain, T., Kim, T. S., Lun, X., Liacini, A., Schiff, L. A., Senger, D. L., et al. (2007). Proteolytic Disassembly Is a Critical Determinant for Reovirus Oncolysis. Mol. Ther. 15 (8), 1512–1521. doi:10.1038/sj.mt.6300207
Alban, T. J., Alvarado, A. G., Sorensen, M. D., Bayik, D., Volovetz, J., Serbinowski, E., et al. (2018). Global Immune Fingerprinting in Glioblastoma Patient Peripheral Blood Reveals Immune-Suppression Signatures Associated with Prognosis. JCI Insight 3 (21), 122264. doi:10.1172/jci.insight.122264
Alban, T. J., Bayik, D., Otvos, B., Rabljenovic, A., Leng, L., Jia-Shiun, L., et al. (2020). Glioblastoma Myeloid-Derived Suppressor Cell Subsets Express Differential Macrophage Migration Inhibitory Factor Receptor Profiles that Can Be Targeted to Reduce Immune Suppression. Front. Immunol. 11, 1191. doi:10.3389/fimmu.2020.01191
Almand, B., Clark, J. I., Nikitina, E., van Beynen, J., English, N. R., Knight, S. C., et al. (2001). Increased Production of Immature Myeloid Cells in Cancer Patients: a Mechanism of Immunosuppression in Cancer. J. Immunol. 166 (1), 678–689. doi:10.4049/jimmunol.166.1.678
Amoozgar, Z., Kloepper, J., Ren, J., Tay, R. E., Kazer, S. W., Kiner, E., et al. (2021). Targeting Treg Cells with GITR Activation Alleviates Resistance to Immunotherapy in Murine Glioblastomas. Nat. Commun. 12 (1), 2582. doi:10.1038/s41467-021-22885-8
Andrews, L. P., Marciscano, A. E., Drake, C. G., and Vignali, D. A. A. (2017). LAG3 (CD223) as a Cancer Immunotherapy Target. Immunol. Rev. 276 (1), 80–96. doi:10.1111/imr.12519
Angelova, A. L., Geletneky, K., Nüesch, J. P. F., and Rommelaere, J. (2015). Tumor Selectivity of Oncolytic Parvoviruses: From In Vitro and Animal Models to Cancer Patients. Front. Bioeng. Biotechnol. 3, 55. doi:10.3389/fbioe.2015.00055
Angelova, A. L., Witzens-Harig, M., Galabov, A. S., and Rommelaere, J. (2017). The Oncolytic Virotherapy Era in Cancer Management: Prospects of Applying H-1 Parvovirus to Treat Blood and Solid Cancers. Front. Oncol. 7, 93. doi:10.3389/fonc.2017.00093
Antonioli, L., Pacher, P., Vizi, E. S., and Haskó, G. (2013). CD39 and CD73 in Immunity and Inflammation. Trends Mol. Med. 19 (6), 355–367. doi:10.1016/j.molmed.2013.03.005
Antonioli, L., Yegutkin, G. G., Pacher, P., Blandizzi, C., and Haskó, G. (2016). Anti-CD73 in Cancer Immunotherapy: Awakening New Opportunities. Trends Cancer 2 (2), 95–109. doi:10.1016/j.trecan.2016.01.003
Antonios, J. P., Soto, H., Everson, R. G., Moughon, D., Orpilla, J. R., Shin, N. P., et al. (2017). Immunosuppressive Tumor-Infiltrating Myeloid Cells Mediate Adaptive Immune Resistance via a PD-1/pd-L1 Mechanism in Glioblastoma. Neuonc 19 (6), now287–807. doi:10.1093/neuonc/now287
Authier, A., Farrand, K. J., Broadley, K. W. R., Ancelet, L. R., Hunn, M. K., Stone, S., et al. (2015). Enhanced Immunosuppression by Therapy-Exposed Glioblastoma Multiforme Tumor Cells. Int. J. Cancer 136 (11), 2566–2578. doi:10.1002/ijc.29309
Azambuja, J. H., Schuh, R. S., Michels, L. R., Gelsleichter, N. E., Beckenkamp, L. R., Iser, I. C., et al. (2020). Nasal Administration of Cationic Nanoemulsions as CD73-siRNA Delivery System for Glioblastoma Treatment: a New Therapeutical Approach. Mol. Neurobiol. 57 (2), 635–649. doi:10.1007/s12035-019-01730-6
Bao, S., Wu, Q., McLendon, R. E., Hao, Y., Shi, Q., Hjelmeland, A. B., et al. (2006). Glioma Stem Cells Promote Radioresistance by Preferential Activation of the DNA Damage Response. Nature 444 (7120), 756–760. doi:10.1038/nature05236
Batich, K. A., Reap, E. A., Archer, G. E., Sanchez-Perez, L., Nair, S. K., Schmittling, R. J., et al. (2017). Long-term Survival in Glioblastoma with Cytomegalovirus Pp65-Targeted Vaccination. Clin. Cancer Res. 23 (8), 1898–1909. doi:10.1158/1078-0432.ccr-16-2057
Benci, J. L., Xu, B., Qiu, Y., Wu, T. J., Dada, H., Twyman-Saint Victor, C., et al. (2016). Tumor Interferon Signaling Regulates a Multigenic Resistance Program to Immune Checkpoint Blockade. Cell 167 (6), 1540–1554. doi:10.1016/j.cell.2016.11.022
Bielamowicz, K., Fousek, K., Byrd, T. T., Samaha, H., Mukherjee, M., Aware, N., et al. (2016). Trivalent CAR T Cells Overcome Interpatient Antigenic Variability in Glioblastoma. Neuro-Oncol 20 (4), 506–518. doi:10.1093/neuonc/nox182
Blank, C., Gajewski, T. F., and Mackensen, A. (2005). Interaction of PD-L1 on Tumor Cells with PD-1 on Tumor-specific T Cells as a Mechanism of Immune Evasion: Implications for Tumor Immunotherapy. Cancer Immunol. Immunother. 54 (4), 307–314. doi:10.1007/s00262-004-0593-x
Bloch, O., Crane, C. A., Fuks, Y., Kaur, R., Aghi, M. K., Berger, M. S., et al. (2014). Heat-shock Protein Peptide Complex-96 Vaccination for Recurrent Glioblastoma: a Phase II, Single-Arm Trial. Neuro-Oncol. 16 (2), 274–279. doi:10.1093/neuonc/not203
Bloch, O., Lim, M., Sughrue, M. E., Komotar, R. J., Abrahams, J. M., O'Rourke, D. M., et al. (2017). Autologous Heat Shock Protein Peptide Vaccination for Newly Diagnosed Glioblastoma: Impact of Peripheral PD-L1 Expression on Response to Therapy. Clin. Cancer Res. 23 (14), 3575–3584. doi:10.1158/1078-0432.CCR-16-1369
Bloch, O., Shi, Q., Anderson, S. K., Knopp, M., Raizer, J., Clarke, J., et al. (2017). Atim-14. Alliance a071101: a Phase ii Randomized Trial Comparing the Efficacy of heat Shock Protein Peptide Complex-96 (hsppc-96) Vaccine Given with Bevacizumab Versus Bevacizumab Alone in the Treatment of Surgically Resectable Recurrent Glioblastoma. Neuro-Oncol. 19 (Suppl. 6), vi29. doi:10.1093/neuonc/nox168.110
Boussiotis, V. A. (2016). Molecular and Biochemical Aspects of the PD-1 Checkpoint Pathway. N. Engl. J. Med. 375 (18), 1767–1778. doi:10.1056/NEJMra1514296
Boydell, E., Marinari, E., Migliorini, D., Dietrich, P.-Y., Patrikidou, A., and Dutoit, V. (2019). Exploratory Study of the Effect of IMA950/Poly-ICLC Vaccination on Response to Bevacizumab in Relapsing High-Grade Glioma Patients. Cancers 11 (4), 464. doi:10.3390/cancers11040464
Brahmer, J., Rasco, D., Chen, M., Masteller, E., Qazi, I., Rogers, S., et al. (2016). Abstract B143: A Phase 1a/1b Study of FPA008 in Combination with Nivolumab in Patients with Selected Advanced Cancers. Cancer Immunol. Res. 4 (1 Suppl. ment), B143. doi:10.1158/2326-6074.CRICIMTEATIAACR15-B143
Brana, I., Calles, A., LoRusso, P. M., Yee, L. K., Puchalski, T. A., Seetharam, S., et al. (2015). Carlumab, an Anti-C-C Chemokine Ligand 2 Monoclonal Antibody, in Combination with Four Chemotherapy Regimens for the Treatment of Patients with Solid Tumors: an Open-Label, Multicenter Phase 1b Study. Targ Oncol. 10 (1), 111–123. doi:10.1007/s11523-014-0320-2
Brennan, C. W., Verhaak, R. G., McKenna, A., Campos, B., Noushmehr, H., Salama, S. R., et al. (2013). The Somatic Genomic Landscape of Glioblastoma. Cell 155 (2), 462–477. doi:10.1016/j.cell.2013.09.034
Bretscher, C., and Marchini, A. (2019). H-1 Parvovirus as a Cancer-Killing Agent: Past, Present, and Future. Viruses 11 (6), 562. doi:10.3390/v11060562
Bristol-Myers Squibb, (2020). A Randomized Phase 3 Single Blind Study of Temozolomide Plus Radiation Therapy Combined with Nivolumab or Placebo in Newly Diagnosed Adult Subjects with MGMT-Methylated (Tumor O6-Methylguanine DNA Methyltransferase) Glioblastoma. New York: clinicaltrials.gov. Availableat: https://clinicaltrials.gov/ct2/show/NCT02667587 (Accessed June 21, 2021).
Bristol-Myers Squibb, (2020). A Randomized, Double-Blind Phase 2/3 Study of Relatlimab Combined with Nivolumab versus Nivolumab in Participants with Previously Untreated Metastatic or Unresectable Melanoma. New York: clinicaltrials.gov. Availableat: https://clinicaltrials.gov/ct2/show/NCT03470922 (Accessed June 22, 2021).
Bronte, V., and Zanovello, P. (2005). Regulation of Immune Responses by L-Arginine Metabolism. Nat. Rev. Immunol. 5 (8), 641–654. doi:10.1038/nri1668
Brooks, W. H., Roszman, T. L., Mahaley, M. S., and Woosley, R. E. (1977). Immunobiology of Primary Intracranial Tumours. II. Analysis of Lymphocyte Subpopulations in Patients with Primary Brain Tumours. Clin. Exp. Immunol. 29 (1), 61–66.
Brown, C. E., Alizadeh, D., Starr, R., Weng, L., Wagner, R., and Naranjo, A. (2016). Regression of Glioblastoma after Chimeric Antigen Receptor T-Cell Therapy. N. Engl. J. Med. 376, 2561–2569. doi:10.1056/NEJMoa1610497
Brown, C. E., Badie, B., Barish, M. E., Weng, L., Ostberg, J. R., Chang, W.-C., et al. (2015). Bioactivity and Safety of IL13Rα2-Redirected Chimeric Antigen Receptor CD8+ T Cells in Patients with Recurrent Glioblastoma. Clin. Cancer Res. 21 (18), 4062–4072. doi:10.1158/1078-0432.CCR-15-0428
Brown, N. F., Ng, S. M., Brooks, C., Coutts, T., Holmes, J., Roberts, C., et al. (2020). A Phase II Open Label, Randomised Study of Ipilimumab with Temozolomide versus Temozolomide Alone after Surgery and Chemoradiotherapy in Patients with Recently Diagnosed Glioblastoma: the Ipi-Glio Trial Protocol. BMC Cancer 20 (1), 198. doi:10.1186/s12885-020-6624-y
Butowski, N. A., Colman, H., De Groot, J. F., Omuro, A. M. P., Nayak, L., Cloughesy, T. F., et al. (2014). A Phase 2 Study of Orally Administered PLX3397 in Patients with Recurrent Glioblastoma. Jco 32 (15_Suppl. l), 2023. doi:10.1200/jco.2014.32.15_suppl.2023
Calvo Tardón, M., Allard, M., Dutoit, V., Dietrich, P.-Y., and Walker, P. R. (2019). Peptides as Cancer Vaccines. Curr. Opin. Pharmacol. 47, 20–26. doi:10.1016/j.coph.2019.01.007
Cannarile, M. A., Weisser, M., Jacob, W., Jegg, A.-M., Ries, C. H., and Rüttinger, D. (2017). Colony-stimulating Factor 1 Receptor (CSF1R) Inhibitors in Cancer Therapy. J. Immunotherapy Cancer 5 (1), 53. doi:10.1186/s40425-017-0257-y
Carson, M. J., Doose, J. M., Melchior, B., Schmid, C. D., and Ploix, C. C. (2006). CNS Immune Privilege: Hiding in plain Sight. Immunol. Rev. 213, 48–65. doi:10.1111/j.1600-065X.2006.00441.x
Carter, T., Shaw, H., Cohn-Brown, D., Chester, K., and Mulholland, P. (2016). Ipilimumab and Bevacizumab in Glioblastoma. Clin. Oncol. 28 (10), 622–626. doi:10.1016/j.clon.2016.04.042
Chan, D. V., Gibson, H. M., Aufiero, B. M., Wilson, A. J., Hafner, M. S., Mi, Q.-S., et al. (2014). Differential CTLA-4 Expression in Human CD4+ versus CD8+ T Cells Is Associated with Increased NFAT1 and Inhibition of CD4+ Proliferation. Genes Immun. 15 (1), 25–32. doi:10.1038/gene.2013.57
Chang, A. L., Miska, J., Wainwright, D. A., Dey, M., Rivetta, C. V., Yu, D., et al. (2016). CCL2 Produced by the Glioma Microenvironment Is Essential for the Recruitment of Regulatory T Cells and Myeloid-Derived Suppressor Cells. Cancer Res. 76 (19), 5671–5682. doi:10.1158/0008-5472.CAN-16-0144
Chang, C.-N., Huang, Y.-C., Yang, D.-M., Kikuta, K., Wei, K.-J., Kubota, T., et al. (2011). A Phase I/II Clinical Trial Investigating the Adverse and Therapeutic Effects of a Postoperative Autologous Dendritic Cell Tumor Vaccine in Patients with Malignant Glioma. J. Clin. Neurosci. 18 (8), 1048–1054. doi:10.1016/j.jocn.2010.11.034
Chen, R., Nishimura, M. C., Bumbaca, S. M., Kharbanda, S., Forrest, W. F., Kasman, I. M., et al. (2010). A Hierarchy of Self-Renewing Tumor-Initiating Cell Types in Glioblastoma. Cancer Cell 17 (4), 362–375. doi:10.1016/j.ccr.2009.12.049
Chiocca, E. A., Abbed, K. M., Tatter, S., Louis, D. N., Hochberg, F. H., Barker, F., et al. (2004). A Phase I Open-Label, Dose-Escalation, Multi-Institutional Trial of Injection with an E1B-Attenuated Adenovirus, ONYX-015, into the Peritumoral Region of Recurrent Malignant Gliomas, in the Adjuvant Setting. Mol. Ther. 10 (5), 958–966. doi:10.1016/j.ymthe.2004.07.021
Choi, B. D., Fecci, P. E., and Sampson, J. H. (2012). Regulatory T Cells Move in when Gliomas Say "I Do". Clin. Cancer Res. 18 (22), 6086–6088. doi:10.1158/1078-0432.CCR-12-2801
Chongsathidkiet, P., Jackson, C., Koyama, S., Loebel, F., Cui, X., Farber, S. H., et al. (2018). Sequestration of T Cells in Bone Marrow in the Setting of Glioblastoma and Other Intracranial Tumors. Nat. Med. 24 (9), 1459–1468. doi:10.1038/s41591-018-0135-2
Choucair, A. K., Levin, V. A., Gutin, P. H., Davis, R. L., Silver, P., Edwards, M. S. B., et al. (1986). Development of Multiple Lesions during Radiation Therapy and Chemotherapy in Patients with Gliomas. J. Neurosurg. 65 (5), 654–658. doi:10.3171/jns.1986.65.5.0654
Chow, K. K., Naik, S., Kakarla, S., Brawley, V. S., Shaffer, D. R., Yi, Z., et al. (2013). T Cells Redirected to EphA2 for the Immunotherapy of Glioblastoma. Mol. Ther. 21 (3), 629–637. doi:10.1038/mt.2012.210
Cloughesy, T. F., Landolfi, J., Hogan, D. J., Bloomfield, S., Carter, B., Chen, C. C., et al. (2016). Phase 1 Trial of Vocimagene Amiretrorepvec and 5-fluorocytosine for Recurrent High-Grade Glioma. Sci. Transl. Med. 8 (341), 341ra75. doi:10.1126/scitranslmed.aad9784
Cloughesy, T. F., Petrecca, K., Walbert, T., Butowski, N., Salacz, M., Perry, J., et al. (2020). Effect of Vocimagene Amiretrorepvec in Combination with Flucytosine vs Standard of Care on Survival Following Tumor Resection in Patients with Recurrent High-Grade Glioma. JAMA Oncol. 6 (12), 1939–1946. doi:10.1001/jamaoncol.2020.3161
Cobbs, C. S., Harkins, L., Samanta, M., Gillespie, G. Y., Bharara, S., King, P. H., et al. (2002). Human Cytomegalovirus Infection and Expression in Human Malignant Glioma. Cancer Res. 62 (12), 3347–3350.
Coffey, M. C., Strong, J. E., Forsyth, P. A., and Lee, P. W. K. (1998). Reovirus Therapy of Tumors with Activated Ras Pathway. Science 282 (5392), 1332–1334. doi:10.1126/science.282.5392.1332
Conry, R. M., Westbrook, B., McKee, S., and Norwood, T. G. (2018). Talimogene Laherparepvec: First in Class Oncolytic Virotherapy. Hum. Vaccin. Immunother. 14 (4), 839–846. doi:10.1080/21645515.2017.1412896
Cosmi, L., Liotta, F., Angeli, R., Mazzinghi, B., Santarlasci, V., Manetti, R., et al. (2004). Th2 Cells Are Less Susceptible Than Th1 Cells to the Suppressive Activity of CD25+ Regulatory Thymocytes Because of Their Responsiveness to Different Cytokines. Blood 103 (8), 3117–3121. doi:10.1182/blood-2003-09-3302
Csatary, L. K., and Bakács, T. (1999). Use of Newcastle Disease Virus Vaccine (MTH-68/H) in a Patient with High-Grade Glioblastoma. JAMA 281 (17), 1588–a. doi:10.1001/jama.281.17.1588-a
Csatary, L. K., Gosztonyi, G., Szeberenyi, J., Fabian, Z., Liszka, V., Bodey, B., et al. (2004). MTH-68/H Oncolytic Viral Treatment in Human High-Grade Gliomas. J. Neurooncol. 67 (1-2), 83–93. doi:10.1023/b:neon.0000021735.85511.05
Curran, M. A., Montalvo, W., Yagita, H., and Allison, J. P. (2010). PD-1 and CTLA-4 Combination Blockade Expands Infiltrating T Cells and Reduces Regulatory T and Myeloid Cells within B16 Melanoma Tumors. Proc. Natl. Acad. Sci. 107 (9), 4275–4280. doi:10.1073/pnas.0915174107
Dai, X.-M., Ryan, G. R., Hapel, A. J., Dominguez, M. G., Russell, R. G., Kapp, S., et al. (2002). Targeted Disruption of the Mouse colony-stimulating Factor 1 Receptor Gene Results in Osteopetrosis, Mononuclear Phagocyte Deficiency, Increased Primitive Progenitor Cell Frequencies, and Reproductive Defects. Blood 99 (1), 111–120. doi:10.1182/blood.v99.1.111
De Groot, J. F., Penas-Prado, M., Mandel, J. J., O'Brien, B. J., Weathers, S.-P. S., Zhou, S., et al. (2018). Window-of-opportunity Clinical Trial of a PD-1 Inhibitor in Patients with Recurrent Glioblastoma. Jco 36 (15_Suppl. l), 2008. doi:10.1200/JCO.2018.36.15_suppl.2008
Desjardins, A., Gromeier, M., Herndon, J. E., Beaubier, N., Bolognesi, D. P., Friedman, A. H., et al. (2018). Recurrent Glioblastoma Treated with Recombinant Poliovirus. N. Engl. J. Med. 379, 150–161. doi:10.1056/NEJMoa1716435
Desland, F. A., and Hormigo, A. (2020). The CNS and the Brain Tumor Microenvironment: Implications for Glioblastoma Immunotherapy. Ijms 21 (19), 7358. doi:10.3390/ijms21197358
Di Piazza, M., Mader, C., Geletneky, K., Herrero y Calle, M., Weber, E., Schlehofer, J., et al. (2007). Cytosolic Activation of Cathepsins Mediates Parvovirus H-1-Induced Killing of Cisplatin and TRAIL-Resistant Glioma Cells. J. Virol. 81 (8), 4186–4198. doi:10.1128/JVI.02601-06
Di Tacchio, M., Macas, J., Weissenberger, J., Sommer, K., Bähr, O., Steinbach, J. P., et al. (2019). Tumor Vessel Normalization, Immunostimulatory Reprogramming, and Improved Survival in Glioblastoma with Combined Inhibition of PD-1, Angiopoietin-2, and VEGF. Cancer Immunol. Res. 7 (12), 1910–1927. doi:10.1158/2326-6066.CIR-18-0865
Dillman, R. O., Duma, C. M., Ellis, R. A., Cornforth, A. N., Schiltz, P. M., Sharp, S. L., et al. (2009). Intralesional Lymphokine-Activated Killer Cells as Adjuvant Therapy for Primary Glioblastoma. J. Immunother. 32 (9), 914–919. doi:10.1097/CJI.0b013e3181b2910f
Dillman, R. O., Duma, C. M., Schiltz, P. M., DePriest, C., Ellis, R. A., Okamoto, K., et al. (19972004). Intracavitary Placement of Autologous Lymphokine-Activated Killer (LAK) Cells after Resection of Recurrent Glioblastoma. J. Immunother. 27 (5), 398–404. doi:10.1097/00002371-200409000-00009
DNAtrix, Announces Positive Data from Phase 2 CAPTIVE (KEYNOTE-192) Study with DNX-2401 in Patients with Recurrent Glioblastoma Highlighted in an Oral Late-Breaking Presentation during Society for Neuro-Oncology (SNO) Annual Meeting. BioSpace; 2021. Accessed October 18, 2021. Availableat: https://www.biospace.com/article/dnatrix-announces-positive-data-from-phase-2-captive-keynote-192-study-with-dnx-2401-in-patients-with-recurrent-glioblastoma-highlighted-in-an-oral-late-breaking-presentation-during-society-for-neuro-oncology-sno-annual-meeting/
Eggermont, A. M. M., Blank, C. U., Mandala, M., Long, G. V., Atkinson, V., Dalle, S., et al. (2018). Adjuvant Pembrolizumab versus Placebo in Resected Stage III Melanoma. N. Engl. J. Med. 378, 1789–1801. doi:10.1056/NEJMoa1802357
Errington, F., Steele, L., Prestwich, R., Harrington, K. J., Pandha, H. S., Vidal, L., et al. (2008). Reovirus Activates Human Dendritic Cells to Promote Innate Antitumor Immunity. J. Immunol. 180 (9), 6018–6026. doi:10.4049/jimmunol.180.9.6018
Fadul, C. E., Fisher, J. L., Gui, J., Hampton, T. H., Côté, A. L., and Ernstoff, M. S. (2011). Immune Modulation Effects of Concomitant Temozolomide and Radiation Therapy on Peripheral Blood Mononuclear Cells in Patients with Glioblastoma Multiforme. Neuro-Oncology 13 (4), 393–400. doi:10.1093/neuonc/noq204
Fecci, P. E., Ochiai, H., Mitchell, D. A., Grossi, P. M., Sweeney, A. E., Archer, G. E., et al. (2007). Systemic CTLA-4 Blockade Ameliorates Glioma-Induced Changes to the CD4+ T Cell Compartment without Affecting Regulatory T-Cell Function. Clin. Cancer Res. 13 (7), 2158–2167. doi:10.1158/1078-0432.CCR-06-2070
Fernandes, C., Costa, A., Osório, L., Lago, R. C., Linhares, P., Carvalho, B., et al. (2017). “Current Standards of Care in Glioblastoma Therapy,” in Glioblastoma. Editor S. De Vleeschouwer (Brisbane, Queensla: Codon Publications). doi:10.15586/codon.glioblastoma.2017.ch11
Filley, A. C., and Dey, M. (2017). Dendritic Cell Based Vaccination Strategy: an Evolving Paradigm. J. Neurooncol. 133 (2), 223–235. doi:10.1007/s11060-017-2446-4
Flores-Toro, J. A., Luo, D., Gopinath, A., Sarkisian, M. R., Campbell, J. J., Charo, I. F., et al. (2020). CCR2 Inhibition Reduces Tumor Myeloid Cells and Unmasks a Checkpoint Inhibitor Effect to Slow Progression of Resistant Murine Gliomas. Proc. Natl. Acad. Sci. USA 117 (2), 1129–1138. doi:10.1073/pnas.1910856117
Foreman, P. M., Friedman, G. K., Cassady, K. A., and Markert, J. M. (2017). Oncolytic Virotherapy for the Treatment of Malignant Glioma. Neurotherapeutics 14 (2), 333–344. doi:10.1007/s13311-017-0516-0
Forsyth, P., Roldán, G., George, D., Wallace, C., Palmer, C. A., Morris, D., et al. (2008). A Phase I Trial of Intratumoral Administration of Reovirus in Patients with Histologically Confirmed Recurrent Malignant Gliomas. Mol. Ther. 16 (3), 627–632. doi:10.1038/sj.mt.6300403
Fox, R. J., Coffey, C. S., Conwit, R., Cudkowicz, M. E., Gleason, T., Goodman, A., et al. (2018). Phase 2 Trial of Ibudilast in Progressive Multiple Sclerosis. N. Engl. J. Med. 379 (9), 846–855. doi:10.1056/NEJMoa1803583
Freeman, A. I., Zakay-Rones, Z., Gomori, J. M., Linetsky, E., Rasooly, L., Greenbaum, E., et al. (2006). Phase I/II Trial of Intravenous NDV-HUJ Oncolytic Virus in Recurrent Glioblastoma Multiforme. Mol. Ther. 13 (1), 221–228. doi:10.1016/j.ymthe.2005.08.016
Friebel, E., Kapolou, K., Unger, S., Núñez, N. G., Utz, S., Rushing, E. J., et al. (2020). Single-Cell Mapping of Human Brain Cancer Reveals Tumor-specific Instruction of Tissue-Invading Leukocytes. Cell 181 (7), 1626–1642. doi:10.1016/j.cell.2020.04.055
Fujita, M., Kohanbash, G., Fellows-Mayle, W., Hamilton, R. L., Komohara, Y., Decker, S. A., et al. (2011). COX-2 Blockade Suppresses Gliomagenesis by Inhibiting Myeloid-Derived Suppressor Cells. Cancer Res. 71 (7), 2664–2674. doi:10.1158/0008-5472.CAN-10-3055
Fukumura, D., Kloepper, J., Amoozgar, Z., Duda, D. G., and Jain, R. K. (2018). Enhancing Cancer Immunotherapy Using Antiangiogenics: Opportunities and Challenges. Nat. Rev. Clin. Oncol. 15 (5), 325–340. doi:10.1038/nrclinonc.2018.29
Gabrilovich, D. I., and Nagaraj, S. (2009). Myeloid-derived Suppressor Cells as Regulators of the Immune System. Nat. Rev. Immunol. 9 (3), 162–174. doi:10.1038/nri2506
Galsky, M. D., Arija, J. Á. A., Bamias, A., Davis, I. D., De Santis, M., Kikuchi, E., et al. (2020). Atezolizumab with or without Chemotherapy in Metastatic Urothelial Cancer (IMvigor130): a Multicentre, Randomised, Placebo-Controlled Phase 3 Trial. The Lancet 395 (10236), 1547–1557. doi:10.1016/S0140-6736(20)30230-0
Geletneky, K., Hajda, J., Angelova, A. L., Leuchs, B., Capper, D., Bartsch, A. J., et al. (2017). Oncolytic H-1 Parvovirus Shows Safety and Signs of Immunogenic Activity in a First Phase I/IIa Glioblastoma Trial. Mol. Ther. 25 (12), 2620–2634. doi:10.1016/j.ymthe.2017.08.016
Geletneky, K., Kiprianova, I., Ayache, A., Koch, R., Herrero y Calle, M., Deleu, L., et al. (2010). Regression of Advanced Rat and Human Gliomas by Local or Systemic Treatment with Oncolytic Parvovirus H-1 in Rat Models. Neuro-Oncology 12 (8), 804–814. doi:10.1093/neuonc/noq023
Gesundheit, B., Ben-David, E., Posen, Y., Ellis, R., Wollmann, G., Schneider, E. M., et al. (2020). Effective Treatment of Glioblastoma Multiforme with Oncolytic Virotherapy: A Case-Series. Front. Oncol. 10, 702. doi:10.3389/fonc.2020.00702
Gholamin, S., Mitra, S. S., Feroze, A. H., Liu, J., Kahn, S. A., Zhang, M., et al. (2017). Disrupting the CD47-Sirpα Anti-phagocytic axis by a Humanized Anti-CD47 Antibody Is an Efficacious Treatment for Malignant Pediatric Brain Tumors. Sci. Transl. Med. 9 (381), eaaf2968. doi:10.1126/scitranslmed.aaf2968
Giles, A. J., Hutchinson, M.-K. N. D., Sonnemann, H. M., Jung, J., Fecci, P. E., Ratnam, N. M., et al. (2018). Dexamethasone-induced Immunosuppression: Mechanisms and Implications for Immunotherapy. J. Immunotherapy Cancer 6 (1), 51. doi:10.1186/s40425-018-0371-5
Glass, R., and Synowitz, M. (2014). CNS Macrophages and Peripheral Myeloid Cells in Brain Tumours. Acta Neuropathol. 128 (3), 347–362. doi:10.1007/s00401-014-1274-2
Goldberg, S. B., Gettinger, S. N., Mahajan, A., Chiang, A. C., Herbst, R. S., Sznol, M., et al. (2016). Pembrolizumab for Patients with Melanoma or Non-small-cell Lung Cancer and Untreated Brain Metastases: Early Analysis of a Non-randomised, Open-Label, Phase 2 Trial. Lancet Oncol. 17 (7), 976–983. doi:10.1016/S1470-2045(16)30053-5
Goswami, S., Walle, T., Cornish, A. E., Basu, S., Anandhan, S., Fernandez, I., et al. (2020). Immune Profiling of Human Tumors Identifies CD73 as a Combinatorial Target in Glioblastoma. Nat. Med. 26 (1), 39–46. doi:10.1038/s41591-019-0694-x
Grauer, O. M., Nierkens, S., Bennink, E., Toonen, L. W. J., Boon, L., Wesseling, P., et al. (2007). CD4+FoxP3+ Regulatory T Cells Gradually Accumulate in Gliomas during Tumor Growth and Efficiently Suppress Antiglioma Immune Responsesin Vivo. Int. J. Cancer 121 (1), 95–105. doi:10.1002/ijc.22607
Gromeier, M., and Nair, S. K. (2018). Recombinant Poliovirus for Cancer Immunotherapy. Annu. Rev. Med. 69 (1), 289–299. doi:10.1146/annurev-med-050715-104655
Grossman, S. A., Ye, X., Lesser, G., Sloan, A., Carraway, H., Desideri, S., et al. (2011). Immunosuppression in Patients with High-Grade Gliomas Treated with Radiation and Temozolomide. Clin. Cancer Res. 17 (16), 5473–5480. doi:10.1158/1078-0432.CCR-11-0774
Gschwandtner, M., Derler, R., and Midwood, K. S. (2019). More Than Just Attractive: How CCL2 Influences Myeloid Cell Behavior beyond Chemotaxis. Front. Immunol. 10, 2759. doi:10.3389/fimmu.2019.02759
Gustafson, M. P., Lin, Y., New, K. C., Bulur, P. A., O'Neill, B. P., Gastineau, D. A., et al. (2010). Systemic Immune Suppression in Glioblastoma: the Interplay between CD14+HLA-DRlo/neg Monocytes, Tumor Factors, and Dexamethasone. Neuro-Oncol. 12 (7), 631–644. doi:10.1093/neuonc/noq001
Harris-Bookman, S., Mathios, D., Martin, A. M., Xia, Y., Kim, E., Xu, H., et al. (2018). Expression of LAG-3 and Efficacy of Combination Treatment with Anti-LAG-3 and Anti-PD-1 Monoclonal Antibodies in Glioblastoma. Int. J. Cancer 143 (12), 3201–3208. doi:10.1002/ijc.31661
Harrow, S., Papanastassiou, V., Harland, J., Mabbs, R., Petty, R., Fraser, M., et al. (2004). HSV1716 Injection into the Brain Adjacent to Tumour Following Surgical Resection of High-Grade Glioma: Safety Data and Long-Term Survival. Gene Ther. 11 (22), 1648–1658. doi:10.1038/sj.gt.3302289
Hoag Memorial Hospital Presbyterian, (2013). Phase II Trial of Intralesional Adoptive Cellular Therapy of Glioblastoma with Interleukin-2-Stimulated Lymphocytes. Newport Beach, CA: clinicaltrials.gov. Availableat: https://clinicaltrials.gov/ct2/show/NCT00331526 (Accessed July 25, 2021).
Hodi, F. S., Mihm, M. C., Soiffer, R. J., Haluska, F. G., Butler, M., Seiden, M. V., et al. (2003). Biologic Activity of Cytotoxic T Lymphocyte-Associated Antigen 4 Antibody Blockade in Previously Vaccinated Metastatic Melanoma and Ovarian Carcinoma Patients. Proc. Natl. Acad. Sci. 100 (8), 4712–4717. doi:10.1073/pnas.0830997100
Hodi, F. S., O'Day, S. J., McDermott, D. F., Weber, R. W., Sosman, J. A., Haanen, J. B., et al. (2010). Improved Survival with Ipilimumab in Patients with Metastatic Melanoma. N. Engl. J. Med. 363 (8), 711–723. doi:10.1056/NEJMoa1003466
Hou, W., Sampath, P., Rojas, J. J., and Thorne, S. H. (2016). Oncolytic Virus-Mediated Targeting of PGE 2 in the Tumor Alters the Immune Status and Sensitizes Established and Resistant Tumors to Immunotherapy. Cancer Cell 30 (1), 108–119. doi:10.1016/j.ccell.2016.05.012
Hu, J., Xiao, Q., Dong, M., Guo, D., Wu, X., and Wang, B. (2020). Glioblastoma Immunotherapy Targeting the Innate Immune Checkpoint CD47-Sirpα Axis. Front. Immunol. 11, 593219. doi:10.3389/fimmu.2020.593219
Huang, T. T., Hlavaty, J., Ostertag, D., Espinoza, F. L., Martin, B., Petznek, H., et al. (2013). Toca 511 Gene Transfer and 5-fluorocytosine in Combination with Temozolomide Demonstrates Synergistic Therapeutic Efficacy in a Temozolomide-Sensitive Glioblastoma Model. Cancer Gene Ther. 20 (10), 544–551. doi:10.1038/cgt.2013.51
Immidisetti, A. V., Nwagwu, C. D., Adamson, D. C., Patel, N. V., and Carbonell, A.-M. (2021). Clinically Explored Virus-Based Therapies for the Treatment of Recurrent High-Grade Glioma in Adults. Biomedicines 9 (2), 138. doi:10.3390/biomedicines9020138
Ishikawa-Sekigami, T., Kaneko, Y., Saito, Y., Murata, Y., Okazawa, H., Ohnishi, H., et al. (2006). Enhanced Phagocytosis of CD47-Deficient Red Blood Cells by Splenic Macrophages Requires SHPS-1. Biochem. Biophysical Res. Commun. 343 (4), 1197–1200. doi:10.1016/j.bbrc.2006.03.094
Istari Oncology (2021). Inc. A Multicenter Phase 2 Study of Oncolytic Polio/Rhinovirus Recombinant (PVSRIPO) in Recurrent WHO Grade IV Malignant Glioma Patients. Morrisville, NC: clinicaltrials.gov. Availableat: https://clinicaltrials.gov/ct2/show/NCT02986178 (Accessed October 18, 2021).
Jacques, F. H., Nicholas, G., and Lorimer, I. (2018). Avelumab in Newly Diagnosed Glioblastoma Multiforme: The SEJ Study. Ann. Oncol. 29, viii131. doi:10.1093/annonc/mdy273.393
Jaime-Ramirez, A. C., Yu, J.-G., Caserta, E., Yoo, J. Y., Zhang, J., Lee, T. J., et al. (2017). Reolysin and Histone Deacetylase Inhibition in the Treatment of Head and Neck Squamous Cell Carcinoma. Mol. Ther. - Oncolytics 5, 87–96. doi:10.1016/j.omto.2017.05.002
Jalil, A. R., Andrechak, J. C., and Discher, D. E. (2020). Macrophage Checkpoint Blockade: Results from Initial Clinical Trials, Binding Analyses, and CD47-Sirpα Structure-Function. Antib Ther. 3 (2), 80–94. doi:10.1093/abt/tbaa006
Ji, N., Zhang, Y., Liu, Y., Xie, J., Wang, Y., Hao, S., et al. (2018). Heat Shock Protein Peptide Complex-96 Vaccination for Newly Diagnosed Glioblastoma: a Phase I, Single-Arm Trial. JCI Insight 3 (10), e99145. doi:10.1172/jci.insight.99145
Jin, K., Mao, C., Chen, L., Wang, L., Liu, Y., and Yuan, J. (2021). Adenosinergic Pathway: A Hope in the Immunotherapy of Glioblastoma. Cancers 13 (2), 229. doi:10.3390/cancers13020229
Johnson, L. A., Scholler, J., Ohkuri, T., Kosaka, A., Patel, P. R., McGettigan, S. E., et al. (2015). Rational Development and Characterization of Humanized Anti-EGFR Variant III Chimeric Antigen Receptor T Cells for Glioblastoma. Sci. Transl. Med. 7 (275), 275ra22. doi:10.1126/scitranslmed.aaa4963
Jonuleit, H., Schmitt, E., Stassen, M., Tuettenberg, A., Knop, J., and Enk, A. H. (2001). Identification and Functional Characterization of Human Cd4+Cd25+ T Cells with Regulatory Properties Isolated from Peripheral Blood. J. Exp. Med. 193 (11), 1285–1294. doi:10.1084/jem.193.11.1285
Kalos, M., Levine, B. L., Porter, D. L., Katz, S., Grupp, S. A., Bagg, A., et al. (2011). T Cells with Chimeric Antigen Receptors Have Potent Antitumor Effects and Can Establish Memory in Patients with Advanced Leukemia. Sci. Transl. Med. 3 (95), 95ra73. doi:10.1126/scitranslmed.3002842
Karachi, A., Dastmalchi, F., Mitchell, D. A., and Rahman, M. (2018). Temozolomide for Immunomodulation in the Treatment of Glioblastoma. Neuro-Oncol 20 (12), 1566–1572. doi:10.1093/neuonc/noy072
Keir, M. E., Butte, M. J., Freeman, G. J., and Sharpe, A. H. (2008). PD-1 and its Ligands in Tolerance and Immunity. Annu. Rev. Immunol. 26 (1), 677–704. doi:10.1146/annurev.immunol.26.021607.090331
Kicielinski, K. P., Chiocca, E. A., Yu, J. S., Gill, G. M., Coffey, M., and Markert, J. M. (2014). Phase 1 Clinical Trial of Intratumoral Reovirus Infusion for the Treatment of Recurrent Malignant Gliomas in Adults. Mol. Ther. 22 (5), 1056–1062. doi:10.1038/mt.2014.21
Kirn, D. (2001). Clinical Research Results with Dl1520 (Onyx-015), a Replication-Selective Adenovirus for the Treatment of Cancer: what Have We Learned? Gene Ther. 8 (2), 89–98. doi:10.1038/sj.gt.3301377
Klatzmann, D., Valéry, C. A., Bensimon, G., Marro, B., Boyer, O., Mokhtari, K., et al. (1998). A Phase I/II Study of Herpes Simplex Virus Type 1 Thymidine Kinase "Suicide" Gene Therapy for Recurrent Glioblastoma. Hum. Gene Ther. 9 (17), 2595–2604. doi:10.1089/hum.1998.9.17-259510.1089/10430349850019436
Kluger, H. M., Chiang, V., Mahajan, A., Zito, C. R., Sznol, M., Tran, T., et al. (2019). Long-Term Survival of Patients with Melanoma with Active Brain Metastases Treated with Pembrolizumab on a Phase II Trial. Jco 37 (1), 52–60. doi:10.1200/JCO.18.00204
Koyama, S., Akbay, E. A., Li, Y. Y., Herter-Sprie, G. S., Buczkowski, K. A., Richards, W. G., et al. (2016). Adaptive Resistance to Therapeutic PD-1 Blockade Is Associated with Upregulation of Alternative Immune Checkpoints. Nat. Commun. 7, 10501. doi:10.1038/ncomms10501
Krenciute, G., Prinzing, B. L., Yi, Z., Wu, M.-F., Liu, H., Dotti, G., et al. (2017). Transgenic Expression of IL15 Improves Antiglioma Activity of IL13Rα2-CAR T Cells but Results in Antigen Loss Variants. Cancer Immunol. Res. 5 (7), 571–581. doi:10.1158/2326-6066.CIR-16-0376
Kumai, T., Fan, A., Harabuchi, Y., and Celis, E. (2017). Cancer Immunotherapy: Moving Forward with Peptide T Cell Vaccines. Curr. Opin. Immunol. 47, 57–63. doi:10.1016/j.coi.2017.07.003
Lamano, J. B., Lamano, J. B., Li, Y. D., DiDomenico, J. D., Choy, W., Veliceasa, D., et al. (2019). Glioblastoma-Derived IL6 Induces Immunosuppressive Peripheral Myeloid Cell PD-L1 and Promotes Tumor Growth. Clin. Cancer Res. 25 (12), 3643–3657. doi:10.1158/1078-0432.CCR-18-2402
Lang, F. F., Conrad, C., Gomez-Manzano, C., Yung, W. K. A., Sawaya, R., Weinberg, J. S., et al. (2018). Phase I Study of DNX-2401 (Delta-24-RGD) Oncolytic Adenovirus: Replication and Immunotherapeutic Effects in Recurrent Malignant Glioma. Jco 36 (14), 1419–1427. doi:10.1200/JCO.2017.75.8219
Lang, F. F., Tran, N. D., Puduvalli, V. K., Elder, J. B., Fink, K. L., Conrad, C. A., et al. (2017). Phase 1b Open-Label Randomized Study of the Oncolytic Adenovirus DNX-2401 Administered with or without Interferon Gamma for Recurrent Glioblastoma. Jco 35 (15_Suppl. l), 2002. doi:10.1200/JCO.2017.35.15_suppl.2002
Latchman, Y., Wood, C. R., Chernova, T., Chaudhary, D., Borde, M., Chernova, I., et al. (2001). PD-L2 Is a Second Ligand for PD-1 and Inhibits T Cell Activation. Nat. Immunol. 2 (3), 261–268. doi:10.1038/85330
Lenschow, D. J., Walunas, T. L., and Bluestone, J. A. (1996). CD28/B7 System of T Cell Costimulation. Annu. Rev. Immunol. 14, 233–258. doi:10.1146/annurev.immunol.14.1.233
Li, F., Lv, B., Liu, Y., Hua, T., Han, J., Sun, C., et al. (2018). Blocking the CD47-Sirpα axis by Delivery of Anti-CD47 Antibody Induces Antitumor Effects in Glioma and Glioma Stem Cells. Oncoimmunology 7 (2), e1391973. doi:10.1080/2162402X.2017.1391973
Li, J., Wang, W., Wang, J., Cao, Y., Wang, S., and Zhao, J. (2021). Viral Gene Therapy for Glioblastoma Multiforme: A Promising Hope for the Current Dilemma. Front. Oncol. 11, 1819. doi:10.3389/fonc.2021.678226
Liau, L. M., Ashkan, K., Tran, D. D., Campian, J. L., Trusheim, J. E., Cobbs, C. S., et al. (2018). First Results on Survival from a Large Phase 3 Clinical Trial of an Autologous Dendritic Cell Vaccine in Newly Diagnosed Glioblastoma. J. Transl Med. 16 (1), 142. doi:10.1186/s12967-018-1507-6
Lim, M., Xia, Y., Bettegowda, C., and Weller, M. (2018). Current State of Immunotherapy for Glioblastoma. Nat. Rev. Clin. Oncol. 15 (7), 422–442. doi:10.1038/s41571-018-0003-5
Lin, Y., Zhao, J.-L., Zheng, Q.-J., Jiang, X., Tian, J., Liang, S.-Q., et al. (2018). Notch Signaling Modulates Macrophage Polarization and Phagocytosis through Direct Suppression of Signal Regulatory Protein α Expression. Front. Immunol. 9, 1744. doi:10.3389/fimmu.2018.01744
Linsley, P. S., Greene, J. L., Brady, W., Bajorath, J., Ledbetter, J. A., and Peach, R. (1994). Human B7-1 (CD80) and B7-2 (CD86) Bind with Similar Avidities but Distinct Kinetics to CD28 and CTLA-4 Receptors. Immunity 1 (9), 793–801. doi:10.1016/s1074-7613(94)80021-9
Liu, G., Yuan, X., Zeng, Z., Tunici, P., Ng, H., Abdulkadir, I. R., et al. (2006). Analysis of Gene Expression and Chemoresistance of CD133+ Cancer Stem Cells in Glioblastoma. Mol. Cancer 5 (1), 67. doi:10.1186/1476-4598-5-67
Liu, Y., Chang, Y., He, X., Cai, Y., Jiang, H., Jia, R., et al. (2020). CD47 Enhances Cell Viability and Migration Ability but Inhibits Apoptosis in Endometrial Carcinoma Cells via the PI3K/Akt/mTOR Signaling Pathway. Front. Oncol. 10. doi:10.3389/fonc.2020.01525
Long, L., Zhang, X., Chen, F., Pan, Q., Phiphatwatchara, P., Zeng, Y., et al. (2018). The Promising Immune Checkpoint LAG-3: from Tumor Microenvironment to Cancer Immunotherapy. Genes Cancer 9 (5-6), 176–189. doi:10.18632/genesandcancer.180
Ludwig Institute for Cancer Research, (2021). Phase 2 Study to Evaluate the Clinical Efficacy and Safety of MEDI4736 in Patients with Glioblastoma (GBM). Gaithersburg, MD: clinicaltrials.gov. Availableat: https://clinicaltrials.gov/ct2/show/NCT02336165 (Accessed June 21, 2021).
Lukas, R. V., Rodon, J., Becker, K., Wong, E. T., Shih, K., Touat, M., et al. (2018). Clinical Activity and Safety of Atezolizumab in Patients with Recurrent Glioblastoma. J. Neurooncol. 140 (2), 317–328. doi:10.1007/s11060-018-2955-9
Ma, H.-I., Chiou, S.-H., Hueng, D.-Y., Tai, L.-K., Huang, P.-I., Kao, C.-L., et al. (2011). Celecoxib and Radioresistant Glioblastoma-Derived CD133+ Cells: Improvement in Radiotherapeutic Effects. Jns 114 (3), 651–662. doi:10.3171/2009.11.JNS091396
Manjili, M. H., Wang, X.-Y., Chen, X., Martin, T., Repasky, E. A., Henderson, R., et al. (2003). HSP110-HER2/neu Chaperone Complex Vaccine Induces Protective Immunity against Spontaneous Mammary Tumors in HER-2/neu Transgenic Mice. J. Immunol. 171 (8), 4054–4061. doi:10.4049/jimmunol.171.8.4054
Margolin, K., Ernstoff, M. S., Hamid, O., Lawrence, D., McDermott, D., Puzanov, I., et al. (2012). Ipilimumab in Patients with Melanoma and Brain Metastases: an Open-Label, Phase 2 Trial. Lancet Oncol. 13 (5), 459–465. doi:10.1016/S1470-2045(12)70090-6
Markert, J. M., Liechty, P. G., Wang, W., Gaston, S., Braz, E., Karrasch, M., et al. (2009). Phase Ib Trial of Mutant Herpes Simplex Virus G207 Inoculated Pre-and post-tumor Resection for Recurrent GBM. Mol. Ther. 17 (1), 199–207. doi:10.1038/mt.2008.228
Markert, J. M., Medlock, M. D., Rabkin, S. D., Gillespie, G. Y., Todo, T., Hunter, W. D., et al. (2000). Conditionally Replicating Herpes Simplex Virus Mutant, G207 for the Treatment of Malignant Glioma: Results of a Phase I Trial. Gene Ther. 7 (10), 867–874. doi:10.1038/sj.gt.3301205
Markert, J. M., Razdan, S. N., Kuo, H.-C., Cantor, A., Knoll, A., Karrasch, M., et al. (2014). A Phase 1 Trial of Oncolytic HSV-1, G207, Given in Combination with Radiation for Recurrent GBM Demonstrates Safety and Radiographic Responses. Mol. Ther. 22 (5), 1048–1055. doi:10.1038/mt.2014.22
Marvel, D., and Gabrilovich, D. I. (2015). Myeloid-derived Suppressor Cells in the Tumor Microenvironment: Expect the Unexpected. J. Clin. Invest. 125 (9), 3356–3364. doi:10.1172/jci80005
Matveeva, O. V., Guo, Z. S., Senin, V. M., Senina, A. V., Shabalina, S. A., and Chumakov, P. M. (2015). Oncolysis by Paramyxoviruses: Preclinical and Clinical Studies. Mol. Ther. - Oncolytics 2, 15017. doi:10.1038/mto.2015.17
Maude, S. L., Frey, N., Shaw, P. A., Aplenc, R., Barrett, D. M., Bunin, N. J., et al. (2014). Chimeric Antigen Receptor T Cells for Sustained Remissions in Leukemia. N. Engl. J. Med. 371 (16), 1507–1517. doi:10.1056/NEJMoa1407222
Maus, M. V., Grupp, S. A., Porter, D. L., and June, C. H. (2014). Antibody-modified T Cells: CARs Take the Front Seat for Hematologic Malignancies. Blood 123 (17), 2625–2635. doi:10.1182/blood-2013-11-492231
McGranahan, T., Therkelsen, K. E., Ahmad, S., and Nagpal, S. (2019). Current State of Immunotherapy for Treatment of Glioblastoma. Curr. Treat. Options. Oncol. 20 (3), 24. doi:10.1007/s11864-019-0619-4
Md Gkf, (2021). Phase II Clinical Trial of HSV G207 with a Single 5 Gy Radiation Dose in Children with Recurrent High-Grade Glioma. Birmingham, AL: clinicaltrials.gov. Availableat: https://clinicaltrials.gov/ct2/show/NCT04482933 (Accessed October 19, 2021).
Md Jm, (2021). A Phase 1 Study of M032 (NSC 733972), a Genetically Engineered HSV-1 Expressing IL-12, in Patients with Recurrent/Progressive Glioblastoma Multiforme, Anaplastic Astrocytoma, or Gliosarcoma. Birmingham, AL: clinicaltrials.gov. Availableat: https://clinicaltrials.gov/ct2/show/NCT02062827 (Accessed October 18, 2021).
Md Pyw, (2021). A Phase Ib Clinical Trial to Evaluate Early Immunologic Pharmacodynamic Parameters Following Neoadjuvant Anti-PD-1 (Nivolumab), or the Combination of Anti-PD-1 Plus Anti-CTLA-4 (Nivolumab Plus Ipilimumab) in Patients with Surgically Accessible Glioblastoma. Boston, MA: clinicaltrials.gov. Availableat: https://clinicaltrials.gov/ct2/show/NCT04606316 (Accessed October 17, 2021).
Md Yy, (2021). The Safety and Efficacy Study of Autologous Tumor-Infiltrating T LymphocyteTILnd Transgenic Modified TIL Cells Adoptive Therapies for Patients with Glioblastoma Multiforme. Shanghai, China: clinicaltrials.gov. Availableat: https://clinicaltrials.gov/ct2/show/NCT03347097 (Accessed July 25, 2021).
M.D. Anderson Cancer Center, (2021). Phase I/II Study to Evaluate the Safety and Clinical Efficacy of Atezolizumab (APDL1) in Combination with Temozolomide and Radiation in Patients with Newly Diagnosed Glioblastoma (GBM). Houston, TX: clinicaltrials.gov. Availableat: https://clinicaltrials.gov/ct2/show/NCT03174197 (Accessed June 21, 2021).
MediciNova, (2021). Phase 1b/2a Single-Center, Open-Label, Dose Escalation Study to Evaluate the Safety, Tolerability, and Efficacy of MN-166 (Ibudilast) and Temozolomide Combination Treatment in Patients with Newly Diagnosed or Recurrent Glioblastoma. San Diego, CA: clinicaltrials.gov. Availableat: https://clinicaltrials.gov/ct2/show/NCT03782415 (Accessed October 19, 2021).
Mi, Y., Guo, N., Luan, J., Cheng, J., Hu, Z., Jiang, P., et al. (2020). The Emerging Role of Myeloid-Derived Suppressor Cells in the Glioma Immune Suppressive Microenvironment. Front. Immunol. 11, 737. doi:10.3389/fimmu.2020.00737
Middleton, G., Silcocks, P., Cox, T., Valle, J., Wadsley, J., Propper, D., et al. (2014). Gemcitabine and Capecitabine with or without Telomerase Peptide Vaccine GV1001 in Patients with Locally Advanced or Metastatic Pancreatic Cancer (TeloVac): an Open-Label, Randomised, Phase 3 Trial. Lancet Oncol. 15 (8), 829–840. doi:10.1016/S1470-2045(14)70236-0
Migliorini, D., Dutoit, V., Allard, M., Grandjean Hallez, N., Marinari, E., Widmer, V., et al. (2019). Phase I/II Trial Testing Safety and Immunogenicity of the Multipeptide IMA950/poly-ICLC Vaccine in Newly Diagnosed Adult Malignant Astrocytoma Patients. Neuro-Oncol. 21 (7), 923–933. doi:10.1093/neuonc/noz040
Miska, J., Rashidi, A., Chang, A. L., Muroski, M. E., Han, Y., Zhang, L., et al. (2016). Anti-GITR Therapy Promotes Immunity against Malignant Glioma in a Murine Model. Cancer Immunol. Immunother. 65 (12), 1555–1567. doi:10.1007/s00262-016-1912-8
Mok, S., Koya, R. C., Tsui, C., Xu, J., Robert, L., Wu, L., et al. (2014). Inhibition of CSF-1 Receptor Improves the Antitumor Efficacy of Adoptive Cell Transfer Immunotherapy. Cancer Res. 74 (1), 153–161. doi:10.1158/0008-5472.CAN-13-1816
Moralès, O., Richard, A., Martin, N., Mrizak, D., Sénéchal, M., Miroux, C., et al. (2012). Activation of a Helper and Not Regulatory Human CD4+ T Cell Response by Oncolytic H-1 Parvovirus. PLOS ONE 7 (2), e32197. doi:10.1371/journal.pone.0032197
Mosaheb, M. M., Dobrikova, E. Y., Brown, M. C., Yang, Y., Cable, J., Okada, H., et al. (2020). Genetically Stable Poliovirus Vectors Activate Dendritic Cells and Prime Antitumor CD8 T Cell Immunity. Nat. Commun. 11 (1), 524. doi:10.1038/s41467-019-13939-z
Moserle, L., and Casanovas, O. (2013). Anti-angiogenesis and Metastasis: a Tumour and Stromal Cell alliance. J. Intern. Med. 273 (2), 128–137. doi:10.1111/joim.12018
Mukherjee, D., Nissen, S. E., and Topol, E. J. (2001). Risk of Cardiovascular Events Associated with Selective COX-2 Inhibitors. JAMA 286 (8), 954–959. doi:10.1001/jama.286.8.954
Müller, L., Berkeley, R., Barr, T., Ilett, E., and Errington-Mais, F. (2020). Past, Present and Future of Oncolytic Reovirus. Cancers 12 (11), 3219. doi:10.3390/cancers12113219
National Cancer Institute Nci, (2021). A Safety Run-In and Phase II Study Evaluating the Efficacy, Safety, and Impact on the Tumor Microenvironment of the Combination of Tocilizumab, Atezolizumab, and Fractionated Stereotactic Radiotherapy in Recurrent Glioblastoma. clinicaltrials.gov. Availableat: https://clinicaltrials.gov/ct2/show/NCT04729959 (Accessed October 19, 2021).
National Cancer Institute (Nci), (2020). Phase I Study of Ipilimumab, Nivolumab, and the Combination in Patients with Newly Diagnosed Glioblastoma. clinicaltrials.gov. Availableat: https://clinicaltrials.gov/ct2/show/NCT02311920 (Accessed October 17, 2021).
Nayak, L., Molinaro, A. M., Peters, K., Clarke, J. L., Jordan, J. T., de Groot, J., et al. (2021). Randomized Phase II and Biomarker Study of Pembrolizumab Plus Bevacizumab versus Pembrolizumab Alone for Patients with Recurrent Glioblastoma. Clin. Cancer Res. 27 (4), 1048–1057. doi:10.1158/1078-0432.ccr-20-2500
Neyns, B., Ben Salama, L., Awada, G., De Cremer, J., Schwarze, J. K., Seynaeve, L., et al. (2019). GLIAVAX: A Stratified Phase II Clinical Trial of Avelumab and Axitinib in Patients with Recurrent Glioblastoma. Jco 37 (15_Suppl. l), 2034. doi:10.1200/JCO.2019.37.15_suppl.2034
Nishimura, H., Minato, N., Nakano, T., and Honjo, T. (1998). Immunological Studies on PD-1 Deficient Mice: Implication of PD-1 as a Negative Regulator for B Cell Responses. Int. Immunol. 10 (10), 1563–1572. doi:10.1093/intimm/10.10.1563
Norman, K. L., Hirasawa, K., Yang, A.-D., Shields, M. A., and Lee, P. W. K. (2004). Reovirus Oncolysis: the Ras/RalGEF/p38 Pathway Dictates Host Cell Permissiveness to Reovirus Infection. Proc. Natl. Acad. Sci. 101 (30), 11099–11104. doi:10.1073/pnas.0404310101
Okada, H., Kalinski, P., Ueda, R., Hoji, A., Kohanbash, G., Donegan, T. E., et al. (2011). Induction of CD8+ T-Cell Responses against Novel Glioma-Associated Antigen Peptides and Clinical Activity by Vaccinations with α-Type 1 Polarized Dendritic Cells and Polyinosinic-Polycytidylic Acid Stabilized by Lysine and Carboxymethylcellulose in Patients with Recurrent Malignant Glioma. Jco 29 (3), 330–336. doi:10.1200/JCO.2010.30.7744
O’Rourke, D. M., Nasrallah, M. P., Desai, A., Melenhorst, J. J., Mansfield, K., Morrissette, J. J. D., et al. (2017). A Single Dose of Peripherally Infused EGFRvIII-Directed CAR T Cells Mediates Antigen Loss and Induces Adaptive Resistance in Patients with Recurrent Glioblastoma. Sci. Transl. Med. 9 (399). doi:10.1126/scitranslmed.aaa0984
Ostrom, Q. T., Gittleman, H., Fulop, J., Liu, M., Blanda, R., Kromer, C., et al. (2015). CBTRUS Statistical Report: Primary Brain and Central Nervous System Tumors Diagnosed in the United States in 2008-2012. Neuro Oncol. 17 (Suppl. l_4), iv1–iv62. doi:10.1093/neuonc/nov189
Papadopoulos, K. P., Gluck, L., Martin, L. P., Olszanski, A. J., Tolcher, A. W., Ngarmchamnanrith, G., et al. (2017). First-in-Human Study of AMG 820, a Monoclonal Anti-Colony-Stimulating Factor 1 Receptor Antibody, in Patients with Advanced Solid Tumors. Clin. Cancer Res. 23 (19), 5703–5710. doi:10.1158/1078-0432.CCR-16-3261
Papanastassiou, V., Rampling, R., Fraser, M., Petty, R., Hadley, D., Nicoll, J., et al. (2002). The Potential for Efficacy of the Modified (ICP 34.5−) Herpes Simplex Virus HSV1716 Following Intratumoural Injection into Human Malignant Glioma: a Proof of Principle Study. Gene Ther. 9 (6), 398–406. doi:10.1038/sj.gt.3301664
Pardoll, D. M. (2012). The Blockade of Immune Checkpoints in Cancer Immunotherapy. Nat. Rev. Cancer 12 (4), 252–264. doi:10.1038/nrc3239
Patel, A. P., Tirosh, I., Trombetta, J. J., Shalek, A. K., Gillespie, S. M., Wakimoto, H., et al. (2014). Single-cell RNA-Seq Highlights Intratumoral Heterogeneity in Primary Glioblastoma. Science 344 (6190), 1396–1401. doi:10.1126/science.1254257
Patel, M. A., Kim, J. E., Theodros, D., Tam, A., Velarde, E., Kochel, C. M., et al. (2016). Agonist Anti-GITR Monoclonal Antibody and Stereotactic Radiation Induce Immune-Mediated Survival Advantage in Murine Intracranial Glioma. J. Immunotherapy Cancer 4, 28. doi:10.1186/s40425-016-0132-2
Pediatric Brain Tumor Consortium, (2016). A Phase I Study of Intratumoral/Peritumoral Herpes Simplex Virus-1 Mutant HSV1716 in Patients with Refractory or Recurrent High Grade Gliomas (HGG). clinicaltrials.gov. Availableat: https://clinicaltrials.gov/ct2/show/NCT02031965 (Accessed October 18, 2021).
Peereboom, D. M., Nabors, L. B., Kumthekar, P., Badruddoja, M. A., Fink, K. L., Lieberman, F. S., et al. (2018). Phase 2 Trial of SL-701 in Relapsed/refractory (R/r) Glioblastoma (GBM): Correlation of Immune Response with Longer-Term Survival. Jco 36 (15_Suppl. l), 2058. doi:10.1200/JCO.2018.36.15_suppl.2058
Phan, G. Q., Yang, J. C., Sherry, R. M., Hwu, P., Topalian, S. L., Schwartzentruber, D. J., et al. (2003). Cancer Regression and Autoimmunity Induced by Cytotoxic T Lymphocyte-Associated Antigen 4 Blockade in Patients with Metastatic Melanoma. Pnas 100 (14), 8372–8377. doi:10.1073/pnas.1533209100
Philbrick, B., and Adamson, D. C. (2019). DNX-2401: an Investigational Drug for the Treatment of Recurrent Glioblastoma. Expert Opin. Investig. Drugs 28 (12), 1041–1049. doi:10.1080/13543784.2019.1694000
Phuphanich, S., Wheeler, C. J., Rudnick, J. D., Mazer, M., Wang, H., Nuño, M. A., et al. (2013). Phase I Trial of a Multi-Epitope-Pulsed Dendritic Cell Vaccine for Patients with Newly Diagnosed Glioblastoma. Cancer Immunol. Immunother. 62 (1), 125–135. doi:10.1007/s00262-012-1319-0
Pienta, K. J., Machiels, J.-P., Schrijvers, D., Alekseev, B., Shkolnik, M., Crabb, S. J., et al. (2013). Phase 2 Study of Carlumab (CNTO 888), a Human Monoclonal Antibody against CC-Chemokine Ligand 2 (CCL2), in Metastatic Castration-Resistant Prostate Cancer. Invest. New Drugs 31 (3), 760–768. doi:10.1007/s10637-012-9869-8
Platten, M., Bunse, L., Wick, A., Bunse, T., Le Cornet, L., Harting, I., et al. (2021). A Vaccine Targeting Mutant IDH1 in Newly Diagnosed Glioma. Nature 592 (7854), 463–468. doi:10.1038/s41586-021-03363-z
Pollack, I. F., Jakacki, R. I., Butterfield, L. H., Hamilton, R. L., Panigrahy, A., Normolle, D. P., et al. (2016). Antigen-specific Immunoreactivity and Clinical Outcome Following Vaccination with Glioma-Associated Antigen Peptides in Children with Recurrent High-Grade Gliomas: Results of a Pilot Study. J. Neurooncol. 130 (3), 517–527. doi:10.1007/s11060-016-2245-3
Puhr, H. C., and Ilhan-Mutlu, A. (2019). New Emerging Targets in Cancer Immunotherapy: the Role of LAG3. ESMO Open 4 (2), e000482. doi:10.1136/esmoopen-2018-000482
Pyonteck, S. M., Akkari, L., Schuhmacher, A. J., Bowman, R. L., Sevenich, L., Quail, D. F., et al. (2013). CSF-1R Inhibition Alters Macrophage Polarization and Blocks Glioma Progression. Nat. Med. 19 (10), 1264–1272. doi:10.1038/nm.3337
Qazi, M. A., Vora, P., Venugopal, C., Sidhu, S. S., Moffat, J., Swanton, C., et al. (2017). Intratumoral Heterogeneity: Pathways to Treatment Resistance and Relapse in Human Glioblastoma. Ann. Oncol. 28 (7), 1448–1456. doi:10.1093/annonc/mdx169
Qiu, J., Shi, Z., and Jiang, J. (2017). Cyclooxygenase-2 in Glioblastoma Multiforme. Drug Discov. Today 22 (1), 148–156. doi:10.1016/j.drudis.2016.09.017
Quattrocchi, K. B., Miller, C. H., Cush, S., Bernard, S. A., Dull, S. T., Smith, M., et al. (1999). Pilot Study of Local Autologous Tumor Infiltrating Lymphocytes for the Treatment of Recurrent Malignant Gliomas. J. Neurooncol. 45 (2), 141–157. doi:10.1023/a:1006293606710
Rainov, N. G. (2000). A Phase III Clinical Evaluation of Herpes Simplex Virus Type 1 Thymidine Kinase and Ganciclovir Gene Therapy as an Adjuvant to Surgical Resection and Radiation in Adults with Previously Untreated Glioblastoma Multiforme. Hum. Gene Ther. 11 (17), 2389–2401. doi:10.1089/104303400750038499
Rainov, N. G., Kramm, C. M., Banning, U., Riemann, D., Holzhausen, H.-J., Heidecke, V., et al. (2000). Immune Response Induced by Retrovirus-Mediated HSV-Tk/GCV Pharmacogene Therapy in Patients with Glioblastoma Multiforme. Gene Ther. 7 (21), 1853–1858. doi:10.1038/sj.gt.3301311
Rajani, K. R., Carlstrom, L. P., Parney, I. F., Johnson, A. J., Warrington, A. E., and Burns, T. C. (2019). Harnessing Radiation Biology to Augment Immunotherapy for Glioblastoma. Front. Oncol. 8, 656. doi:10.3389/fonc.2018.00656
Ram, Z., Culver, K. W., Oshiro, E. M., Viola, J. J., DeVroom, H. L., Otto, E., et al. (1997). Therapy of Malignant Brain Tumors by Intratumoral Implantation of Retroviral Vector-Producing Cells. Nat. Med. 3 (12), 1354–1361. doi:10.1038/nm1297-1354
Rampling, R., Cruickshank, G., Papanastassiou, V., Nicoll, J., Hadley, D., Brennan, D., et al. (2000). Toxicity Evaluation of Replication-Competent Herpes Simplex Virus (ICP 34.5 Null Mutant 1716) in Patients with Recurrent Malignant Glioma. Gene Ther. 7 (10), 859–866. doi:10.1038/sj.gt.3301184
Rampling, R., Peoples, S., Mulholland, P. J., James, A., Al-Salihi, O., Twelves, C. J., et al. (2016). A Cancer Research UK First Time in Human Phase I Trial of IMA950 (Novel Multipeptide Therapeutic Vaccine) in Patients with Newly Diagnosed Glioblastoma. Clin. Cancer Res. 22 (19), 4776–4785. doi:10.1158/1078-0432.CCR-16-0506
Raychaudhuri, B., Rayman, P., Ireland, J., Ko, J., Rini, B., Borden, E. C., et al. (2011). Myeloid-derived Suppressor Cell Accumulation and Function in Patients with Newly Diagnosed Glioblastoma. Neuro-Oncology 13 (6), 591–599. doi:10.1093/neuonc/nor042
Ready, N., Hellmann, M. D., Awad, M. M., Otterson, G. A., Gutierrez, M., Gainor, J. F., et al. (2019). First-Line Nivolumab Plus Ipilimumab in Advanced Non-small-cell Lung Cancer (CheckMate 568): Outcomes by Programmed Death Ligand 1 and Tumor Mutational Burden as Biomarkers. Jco 37 (12), 992–1000. doi:10.1200/JCO.18.01042
Reardon, D. A., Brandes, A. A., Omuro, A., Mulholland, P., Lim, M., Wick, A., et al. (2020). Effect of Nivolumab vs Bevacizumab in Patients with Recurrent Glioblastoma. JAMA Oncol. 6 (7), 1003–1010. doi:10.1001/jamaoncol.2020.1024
Reardon, D. A., Kaley, T. J., Dietrich, J., Clarke, J. L., Dunn, G., Lim, M., et al. (2019). Phase II Study to Evaluate Safety and Efficacy of MEDI4736 (Durvalumab) + Radiotherapy in Patients with Newly Diagnosed Unmethylated MGMT Glioblastoma (New Unmeth GBM). Jco 37 (15_Suppl. l), 2032. doi:10.1200/JCO.2019.37.15_suppl.2032
Reardon, D. A., Schuster, J., Tran, D. D., Fink, K. L., Nabors, L. B., Li, G., et al. (2015). ReACT: Overall Survival from a Randomized Phase II Study of Rindopepimut (CDX-110) Plus Bevacizumab in Relapsed Glioblastoma. Jco 33 (15_Suppl. l), 2009. doi:10.1200/jco.2015.33.15_suppl.2009
Reck, M., Ciuleanu, T-E., and Lee, J-S. (2021). First-Line Nivolumab Plus Ipilimumab versus Chemotherapy in Advanced NSCLC with 1% or Greater Tumor PD-L1 Expression: Patient-Reported Outcomes from CheckMate 227 Part 1. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 16 (4), 665–676. doi:10.1016/j.jtho.2020.12.019
Ries, C. H., Cannarile, M. A., Hoves, S., Benz, J., Wartha, K., Runza, V., et al. (2014). Targeting Tumor-Associated Macrophages with Anti-CSF-1r Antibody Reveals a Strategy for Cancer Therapy. Cancer Cell 25 (6), 846–859. doi:10.1016/j.ccr.2014.05.016
Rini, B. I., Stenzl, A., Zdrojowy, R., Kogan, M., Shkolnik, M., Oudard, S., et al. (2016). IMA901, a Multipeptide Cancer Vaccine, Plus Sunitinib versus Sunitinib Alone, as First-Line Therapy for Advanced or Metastatic Renal Cell Carcinoma (IMPRINT): a Multicentre, Open-Label, Randomised, Controlled, Phase 3 Trial. Lancet Oncol. 17 (11), 1599–1611. doi:10.1016/S1470-2045(16)30408-9
Robert, C., Long, G. V., Brady, B., Dutriaux, C., Maio, M., Mortier, L., et al. (2015). Nivolumab in Previously Untreated Melanoma withoutBRAFMutation. N. Engl. J. Med. 372 (4), 320–330. doi:10.1056/NEJMoa1412082
Rolan, P., Gibbons, J. A., He, L., Chang, E., Jones, D., Gross, M. I., et al. (2008). Ibudilast in Healthy Volunteers: Safety, Tolerability and Pharmacokinetics with Single and Multiple Doses. Br. J. Clin. Pharmacol. 66 (6), 792–801. doi:10.1111/j.1365-2125.2008.03270.x
Sakaguchi, S., Ono, M., Setoguchi, R., Yagi, H., Hori, S., Fehervari, Z., et al. (2006). Foxp3+CD25+CD4+ Natural Regulatory T Cells in Dominant Self-Tolerance and Autoimmune Disease. Immunol. Rev. 212, 8–27. doi:10.1111/j.0105-2896.2006.00427.x
Sakai, K., Shimodaira, S., Maejima, S., Udagawa, N., Sano, K., Higuchi, Y., et al. (2015). Dendritic Cell-Based Immunotherapy Targeting Wilms' Tumor 1 in Patients with Recurrent Malignant Glioma. Jns 123 (4), 989–997. doi:10.3171/2015.1.JNS141554
Sampson, J. H., Choi, B. D., Sanchez-Perez, L., Suryadevara, C. M., Snyder, D. J., Flores, C. T., et al. (2014). EGFRvIII mCAR-Modified T-Cell Therapy Cures Mice with Established Intracerebral Glioma and Generates Host Immunity against Tumor-Antigen Loss. Clin. Cancer Res. 20 (4), 972–984. doi:10.1158/1078-0432.CCR-13-0709
Sampson, J. H., Heimberger, A. B., Archer, G. E., Aldape, K. D., Friedman, A. H., Friedman, H. S., et al. (2010). Immunologic Escape after Prolonged Progression-free Survival with Epidermal Growth Factor Receptor Variant III Peptide Vaccination in Patients with Newly Diagnosed Glioblastoma. Jco 28 (31), 4722–4729. doi:10.1200/JCO.2010.28.6963
Sampson, J. H., Omuro, A. M. P., Preusser, M., Lim, M., Butowski, N. A., Cloughesy, T. F., et al. (2016). A Randomized, Phase 3, Open-Label Study of Nivolumab versus Temozolomide (TMZ) in Combination with Radiotherapy (RT) in Adult Patients (Pts) with Newly Diagnosed, O-6-Methylguanine DNA Methyltransferase (MGMT)-unmethylated Glioblastoma (GBM): CheckMate-498. Jco 34 (15_Suppl. l), TPS2079. doi:10.1200/JCO.2016.34.15_suppl.TPS2079
Samson, A., Scott, K. J., Taggart, D., West, E. J., Wilson, E., Nuovo, G. J., et al. (2018). Intravenous Delivery of Oncolytic Reovirus to Brain Tumor Patients Immunologically Primes for Subsequent Checkpoint Blockade. Sci. Transl. Med. 10 (422), eaam7577. doi:10.1126/scitranslmed.aam7577
Sandhu, S. K., Papadopoulos, K., Fong, P. C., Patnaik, A., Messiou, C., Olmos, D., et al. (2013). A First-In-Human, First-In-Class, Phase I Study of Carlumab (CNTO 888), a Human Monoclonal Antibody against CC-Chemokine Ligand 2 in Patients with Solid Tumors. Cancer Chemother. Pharmacol. 71 (4), 1041–1050. doi:10.1007/s00280-013-2099-8
Schachter, J., Ribas, A., Long, G. V., Arance, A., Grob, J.-J., Mortier, L., et al. (2017). Pembrolizumab versus Ipilimumab for Advanced Melanoma: Final Overall Survival Results of a Multicentre, Randomised, Open-Label Phase 3 Study (KEYNOTE-006). The Lancet 390 (10105), 1853–1862. doi:10.1016/S0140-6736(17)31601-X
Schalper, K. A., Rodriguez-Ruiz, M. E., Diez-Valle, R., López-Janeiro, A., Porciuncula, A., Idoate, M. A., et al. (2019). Neoadjuvant Nivolumab Modifies the Tumor Immune Microenvironment in Resectable Glioblastoma. Nat. Med. 25 (3), 470–476. doi:10.1038/s41591-018-0339-5
Schild, H., and Rammensee, H.-G. (2000). gp96-The Immune System's Swiss Army Knife. Nat. Immunol. 1 (2), 100–101. doi:10.1038/77770
Schneider, T., Gerhards, R., Kirches, E., and Firsching, R. (2001). Preliminary Results of Active Specific Immunization with Modified Tumor Cell Vaccine in Glioblastoma Multiforme. J. Neurooncol. 53 (1), 39–46. doi:10.1023/A:1011856406683
Schumacher, T., Bunse, L., Pusch, S., Sahm, F., Wiestler, B., Quandt, J., et al. (2014). A Vaccine Targeting Mutant IDH1 Induces Antitumour Immunity. Nature 512 (7514), 324–327. doi:10.1038/nature13387
Schuster, J., Lai, R. K., Recht, L. D., Reardon, D. A., Paleologos, N. A., Groves, M. D., et al. (2015). A Phase II, Multicenter Trial of Rindopepimut (CDX-110) in Newly Diagnosed Glioblastoma: the ACT III Study. Neuro-Oncology 17 (6), 854–861. doi:10.1093/neuonc/nou348
Schwarze, J. K., Bertels, C., Awada, G., Tijtgat, J., Tuyaerts, S., Cras, L., et al. (2020). 65MO A Phase I Clinical Trial on Intratumoural (IT) Administration of Ipilimumab (IPI) Plus Nivolumab (NIVO) Followed by Intracavitary (IC) Administration of Nivolumab in Patients with Recurrent Glioblastoma. Ann. Oncol. 31, S1443. doi:10.1016/j.annonc.2020.10.553
Sevenich, L. (2019). Turning "Cold" into "Hot" Tumors-Opportunities and Challenges for Radio-Immunotherapy against Primary and Metastatic Brain Cancers. Front. Oncol. 9, 163. doi:10.3389/fonc.2019.00163
Shand, N., Weber, F., Mariani, L., Bernstein, M., Gianella-Borradori, A., Long, Z., et al. (1999). A Phase 1-2 Clinical Trial of Gene Therapy for Recurrent Glioblastoma Multiforme by Tumor Transduction with the Herpes Simplex Thymidine Kinase Gene Followed by Ganciclovir. Hum. Gene Ther. 10 (14), 2325–2335. doi:10.1089/10430349950016979
Sharpe, A. H., and Pauken, K. E. (2018). The Diverse Functions of the PD1 Inhibitory Pathway. Nat. Rev. Immunol. 18 (3), 153–167. doi:10.1038/nri.2017.108
Shevtsov, M., and Multhoff, G. (2016). Heat Shock Protein-Peptide and HSP-Based Immunotherapies for the Treatment of Cancer. Front. Immunol. 7, 171. doi:10.3389/fimmu.2016.00171
Shin, D. S., Zaretsky, J. M., Escuin-Ordinas, H., Garcia-Diaz, A., Hu-Lieskovan, S., Kalbasi, A., et al. (2017). Primary Resistance to PD-1 Blockade Mediated by JAK1/2 Mutations. Cancer Discov. 7 (2), 188–201. doi:10.1158/2159-8290.CD-16-1223
Shono, K., Yamaguchi, I., Mizobuchi, Y., Kagusa, H., Sumi, A., Fujihara, T., et al. (2020). Downregulation of the CCL2/CCR2 and CXCL10/CXCR3 Axes Contributes to Antitumor Effects in a Mouse Model of Malignant Glioma. Sci. Rep. 10 (1), 15286. doi:10.1038/s41598-020-71857-3
Simpson, K. D., Templeton, D. J., and Cross, J. V. (2012). Macrophage Migration Inhibitory Factor Promotes Tumor Growth and Metastasis by Inducing Myeloid-Derived Suppressor Cells in the Tumor Microenvironment. J.I. 189 (12), 5533–5540. doi:10.4049/jimmunol.1201161
Sloan, A. E., Buerki, R. A., Murphy, C., Kelly, A. T., Ambady, P., Brown, M., et al. (2021). LUMINOS-101: Phase 2 Study of PVSRIPO with Pembrolizumab in Recurrent Glioblastoma. Jco 39 (15_Suppl. l), TPS2065. doi:10.1200/JCO.2021.39.15_suppl.TPS2065
Smith, C. C., Selitsky, S. R., Chai, S., Armistead, P. M., Vincent, B. G., and Serody, J. S. (2019). Alternative Tumour-specific Antigens. Nat. Rev. Cancer 19 (8), 465–478. doi:10.1038/s41568-019-0162-4
Smolen, J. S., Schoels, M. M., Nishimoto, N., Breedveld, F. C., Burmester, G. R., Dougados, M., et al. (2013). Consensus Statement on Blocking the Effects of Interleukin-6 and in Particular by Interleukin-6 Receptor Inhibition in Rheumatoid Arthritis and Other Inflammatory Conditions. Ann. Rheum. Dis. 72 (4), 482–492. doi:10.1136/annrheumdis-2012-202469
Stagg, J. (2012). The Double-Edge Sword Effect of Anti-CD73 Cancer Therapy. Oncoimmunology 1 (2), 217–218. doi:10.4161/onci.1.2.18101
Steiner, H. H., Bonsanto, M. M., Beckhove, P., Brysch, M., Geletneky, K., Ahmadi, R., et al. (2004). Antitumor Vaccination of Patients with Glioblastoma Multiforme: A Pilot Study to Assess Feasibility, Safety, and Clinical Benefit. Jco 22 (21), 4272–4281. doi:10.1200/JCO.2004.09.038
Stupp, R., Mason, W. P., van den Bent, M. J., Weller, M., Fisher, B., Taphoorn, M. J. B., et al. (2005). Radiotherapy Plus Concomitant and Adjuvant Temozolomide for Glioblastoma. N. Engl. J. Med. 352 (10), 987–996. doi:10.1056/NEJMoa043330
Sun, H., Yin, L., Li, S., Han, S., Song, G., Liu, N., et al. (2013). Prognostic Significance of IDH Mutation in Adult Low-Grade Gliomas: a Meta-Analysis. J. Neurooncol. 113 (2), 277–284. doi:10.1007/s11060-013-1107-5
Swartz, A. M., Li, Q.-J., and Sampson, J. H. (2014). Rindopepimut: a Promising Immunotherapeutic for the Treatment of Glioblastoma Multiforme. Immunotherapy 6 (6), 679–690. doi:10.2217/imt.14.21
Tabatabaei, P., Visse, E., Bergström, P., Brännström, T., Siesjö, P., and Bergenheim, A. T. (2017). Radiotherapy Induces an Immediate Inflammatory Reaction in Malignant Glioma: a Clinical Microdialysis Study. J. Neurooncol. 131 (1), 83–92. doi:10.1007/s11060-016-2271-1
Tacken, P. J., de Vries, I. J. M., Torensma, R., and Figdor, C. G. (2007). Dendritic-cell Immunotherapy: from Ex Vivo Loading to In Vivo Targeting. Nat. Rev. Immunol. 7 (10), 790–802. doi:10.1038/nri2173
Taggart, D., Andreou, T., Scott, K. J., Williams, J., Rippaus, N., Brownlie, R. J., et al. (2018). Anti-PD-1/anti-CTLA-4 Efficacy in Melanoma Brain Metastases Depends on Extracranial Disease and Augmentation of CD8+ T Cell Trafficking. Proc. Natl. Acad. Sci. USA 115 (7), E1540–E1549. doi:10.1073/pnas.1714089115
Takenaka, M. C., Gabriely, G., Rothhammer, V., Mascanfroni, I. D., Wheeler, M. A., Chao, C.-C., et al. (2019). Control of Tumor-Associated Macrophages and T Cells in Glioblastoma via AHR and CD39. Nat. Neurosci. 22 (5), 729–740. doi:10.1038/s41593-019-0370-y
Tamura, K., Aoyagi, M., Ando, N., Ogishima, T., Wakimoto, H., Yamamoto, M., et al. (2013). Expansion of CD133-Positive Glioma Cells in Recurrent De Novo Glioblastomas after Radiotherapy and Chemotherapy. Jns 119 (5), 1145–1155. doi:10.3171/2013.7.JNS122417
Tawbi, H. A., Forsyth, P. A., Algazi, A., Hamid, O., Hodi, F. S., Moschos, S. J., et al. (2018). Combined Nivolumab and Ipilimumab in Melanoma Metastatic to the Brain. N. Engl. J. Med. 379 (8), 722–730. doi:10.1056/NEJMoa1805453
Tini, P., and Pirtoli, L. (2016). Combining Ipilimumab and Bevacizumab in Glioblastoma Is Really Safe and Effective? Clin. Oncol. 28 (10), 663. doi:10.1016/j.clon.2016.06.003
Tivol, E. A., Borriello, F., Schweitzer, A. N., Lynch, W. P., Bluestone, J. A., and Sharpe, A. H. (1995). Loss of CTLA-4 Leads to Massive Lymphoproliferation and Fatal Multiorgan Tissue Destruction, Revealing a Critical Negative Regulatory Role of CTLA-4. Immunity 3 (5), 541–547. doi:10.1016/1074-7613(95)90125-6
Toolan, H. W. (1961). A Virus Associated with Transplantable Human Tumors. Bull. N. Y Acad. Med. 37 (5), 305–310.
Uhscc, (2021). Opens New Trial with PVSRIPO a Viralbased Immunotherapy in Combination with Pembrolizumab. Shaker Heights, OH: clinicaltrials.gov. Availableat: https://www.uhhospitals.org/for-clinicians/articles-and-news/articles/2020/11/uhscc-opens-new-trial-with-pvsripo-a-viralbased-immunotherapy-in-combination-with-pembrolizumab (Accessed October 20, 2021).
University of Pennsylvania, (2021). A Phase II Study of the Anti-GITR Agonist INCAGN1876 and the PD-1 Inhibitor INCMGA00012 in Combination with Stereotactic Radiosurgery in Recurrent Glioblastoma. Philadelphia: clinicaltrials.gov. Availableat: https://clinicaltrials.gov/ct2/show/NCT04225039 (Accessed October 19, 2021).
Van den Bossche, W. B. L., Kleijn, A., Teunissen, C. E., Voerman, J. S. A., Teodosio, C., Noske, D. P., et al. (2018). Oncolytic Virotherapy in Glioblastoma Patients Induces a Tumor Macrophage Phenotypic Shift Leading to an Altered Glioblastoma Microenvironment. Neuro-Oncol. 20 (11), 1494–1504. doi:10.1093/neuonc/noy082
von Roemeling, C. A., Wang, Y., Qie, Y., Yuan, H., Zhao, H., Liu, X., et al. (2020). Therapeutic Modulation of Phagocytosis in Glioblastoma Can Activate Both Innate and Adaptive Antitumour Immunity. Nat. Commun. 11 (1), 1508. doi:10.1038/s41467-020-15129-8
von Tresckow, B., Morschhauser, F., Ribrag, V., Topp, M. S., Chien, C., Seetharam, S., et al. (2015). An Open-Label, Multicenter, Phase I/II Study of JNJ-40346527, a CSF-1R Inhibitor, in Patients with Relapsed or Refractory Hodgkin Lymphoma. Clin. Cancer Res. 21 (8), 1843–1850. doi:10.1158/1078-0432.CCR-14-1845
Wang, J., Shen, F., Yao, Y., Wang, L.-l., Zhu, Y., and Hu, J. (2020). Adoptive Cell Therapy: A Novel and Potential Immunotherapy for Glioblastoma. Front. Oncol. 10, 59. doi:10.3389/fonc.2020.00059
Wang, J., Yoshida, T., Nakaki, F., Hiai, H., Okazaki, T., and Honjo, T. (2005). Establishment of NOD-Pdcd1-/- Mice as an Efficient Animal Model of Type I Diabetes. Proc. Natl. Acad. Sci. 102 (33), 11823–11828. doi:10.1073/pnas.0505497102
Wang, X.-Y., Kazim, L., Repasky, E. A., and Subjeck, J. R. (2003). Immunization with Tumor-Derived ER Chaperone Grp170 Elicits Tumor-specific CD8+ T-Cell Responses and Reduces Pulmonary Metastatic Disease. Int. J. Cancer 105 (2), 226–231. doi:10.1002/ijc.11058
Waterhouse, P., Penninger, J. M., Timms, E., Wakeham, A., Shahinian, A., Lee, K. P., et al. (1995). Lymphoproliferative Disorders with Early Lethality in Mice Deficient in Ctla-4. Science 270 (5238), 985–988. doi:10.1126/science.270.5238.985
Weathers, S.-P. S., Kamiya-Matsuoka, C., Harrison, R. A., Liu, D. D., Dervin, S., Yun, C., et al. (2020). Phase I/II Study to Evaluate the Safety and Clinical Efficacy of Atezolizumab (Atezo; aPDL1) in Combination with Temozolomide (TMZ) and Radiation in Patients with Newly Diagnosed Glioblastoma (GBM). Jco 38 (15_Suppl. l), 2511. doi:10.1200/JCO.2020.38.15_suppl.2511
Weiss, S. A., Djureinovic, D., Jessel, S., Krykbaeva, I., Zhang, L., Jilaveanu, L., et al. (2021). A Phase I Study of APX005M and Cabiralizumab with or without Nivolumab in Patients with Melanoma, Kidney Cancer, or Non-small Cell Lung Cancer Resistant to Anti-PD-1/pd-L1. Clin. Cancer Res. 27, 4757–4767. doi:10.1158/1078-0432.CCR-21-0903
Weller, M., Butowski, N., Tran, D. D., Recht, L. D., Lim, M., Hirte, H., et al. (2017). Rindopepimut with Temozolomide for Patients with Newly Diagnosed, EGFRvIII-Expressing Glioblastoma (ACT IV): a Randomised, Double-Blind, International Phase 3 Trial. Lancet Oncol. 18 (10), 1373–1385. doi:10.1016/S1470-2045(17)30517-X
Wolchok, J. D., Chiarion-Sileni, V., Gonzalez, R., Rutkowski, P., Grob, J.-J., Cowey, C. L., et al. (2017). Overall Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 377 (14), 1345–1356. doi:10.1056/NEJMoa1709684
Woroniecka, K. I., Rhodin, K. E., Chongsathidkiet, P., Keith, K. A., and Fecci, P. E. (2018). T-cell Dysfunction in Glioblastoma: Applying a New Framework. Clin. Cancer Res. 24 (16), 3792–3802. doi:10.1158/1078-0432.CCR-18-0047
Wright, H. L., Cross, A. L., Edwards, S. W., and Moots, R. J. (2014). Effects of IL-6 and IL-6 Blockade on Neutrophil Function In Vitro and In Vivo. Rheumatol. Oxf Engl. 53 (7), 1321–1331. doi:10.1093/rheumatology/keu035
Wu, A., Maxwell, R., Xia, Y., Cardarelli, P., Oyasu, M., Belcaid, Z., et al. (2019). Combination Anti-CXCR4 and Anti-PD-1 Immunotherapy Provides Survival Benefit in Glioblastoma through Immune Cell Modulation of Tumor Microenvironment. J. Neurooncol. 143 (2), 241–249. doi:10.1007/s11060-019-03172-5
Wu, A., Wei, J., Kong, L.-Y., Wang, Y., Priebe, W., Qiao, W., et al. (2010). Glioma Cancer Stem Cells Induce Immunosuppressive Macrophages/microglia. Neuro-Oncol. 12 (11), 1113–1125. doi:10.1093/neuonc/noq082
Xu, L., Xiao, H., Xu, M., Zhou, C., Yi, L., and Liang, H. (2011). Glioma-derived T Cell Immunoglobulin- and Mucin Domain-Containing Molecule-4 (TIM4) Contributes to Tumor Tolerance. J. Biol. Chem. 286 (42), 36694–36699. doi:10.1074/jbc.M111.292540
Yan, A., Joachims, M. L., Thompson, L. F., Miller, A. D., Canoll, P. D., and Bynoe, M. S. (2019). CD73 Promotes Glioblastoma Pathogenesis and Enhances its Chemoresistance via A2B Adenosine Receptor Signaling. J. Neurosci. 39 (22), 4387–4402. doi:10.1523/JNEUROSCI.1118-18.2019
Yang, F., He, Z., Duan, H., Zhang, D., Li, J., Yang, H., et al. (2021). Synergistic Immunotherapy of Glioblastoma by Dual Targeting of IL-6 and CD40. Nat. Commun. 12 (1), 3424. doi:10.1038/s41467-021-23832-3
Yang, L., Yu, H., Dong, S., Zhong, Y., and Hu, S. (2017). Recognizing and Managing on Toxicities in Cancer Immunotherapy. Tumour Biol. 39 (3), 101042831769454. doi:10.1177/1010428317694542
Yin, J., Markert, J. M., and Leavenworth, J. W. (2017). Modulation of the Intratumoral Immune Landscape by Oncolytic Herpes Simplex Virus Virotherapy. Front. Oncol. 7, 136. doi:10.3389/fonc.2017.00136
Zanin, R. F., Braganhol, E., Bergamin, L. S., Campesato, L. F. I., Filho, A. Z., Moreira, J. C. F., et al. (2012). Differential Macrophage Activation Alters the Expression Profile of NTPDase and Ecto-5′-Nucleotidase. PLOS ONE 7 (2), e31205. doi:10.1371/journal.pone.0031205
Zhang, M., Hutter, G., Kahn, S. A., Azad, T. D., Gholamin, S., Xu, C. Y., et al. (2016). Anti-CD47 Treatment Stimulates Phagocytosis of Glioblastoma by M1 and M2 Polarized Macrophages and Promotes M1 Polarized Macrophages In Vivo. PLoS One 11 (4), e0153550. doi:10.1371/journal.pone.0153550
Zhang, W., Huang, Q., Xiao, W., Zhao, Y., Pi, J., Xu, H., et al. (2020). Advances in Anti-tumor Treatments Targeting the CD47/SIRPα Axis. Front. Immunol. 11, 18. doi:10.3389/fimmu.2020.00018
Zhao, J., Chen, A. X., Gartrell, R. D., Silverman, A. M., Aparicio, L., Chu, T., et al. (2019). Immune and Genomic Correlates of Response to Anti-PD-1 Immunotherapy in Glioblastoma. Nat. Med. 25 (3), 462–469. doi:10.1038/s41591-019-0349-y
Zhou, W., and Bao, S. (2016). “Cancer Stem Cells and Tumor-Associated Macrophages,” in Cancer Stem Cells. Editors H. Liu, and J. D Lathia (Academic Press), 367–394. doi:10.1016/B978-0-12-803892-5.00014-0
Keywords: glioblastoma, immunotherapy, resistance, immunoprivilege, checkpoint inhibitors, vaccine, CAR (chimeric antigen receptor) T cells, virotherapy
Citation: Wang EJ, Chen J-S, Jain S, Morshed RA, Haddad AF, Gill S, Beniwal AS and Aghi MK (2021) Immunotherapy Resistance in Glioblastoma. Front. Genet. 12:750675. doi: 10.3389/fgene.2021.750675
Received: 31 August 2021; Accepted: 27 October 2021;
Published: 17 December 2021.
Edited by:
Jian-Guo Zhou, University of Erlangen Nuremberg, GermanyReviewed by:
Jozsef Dudas, Innsbruck Medical University, AustriaCopyright © 2021 Wang, Chen, Jain, Morshed, Haddad, Gill, Beniwal and Aghi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Manish K. Aghi, bWFuaXNoLmFnaGlAdWNzZi5lZHU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.