 Susanne B. Haga
Susanne B. Haga
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Genet. , 01 October 2021
Sec. Pharmacogenetics and Pharmacogenomics
Volume 12 - 2021 | https://doi.org/10.3389/fgene.2021.741395
This article is part of the Research Topic Pharmacogenomics: From Bench to Bedside and Back Again View all 8 articles
Incidental or secondary findings have been a major part of the discussion of genomic medicine research and clinical applications. For pharmacogenetic (PGx) testing, secondary findings arise due to the pleiotropic effects of pharmacogenes, often related to their endogenous functions. Unlike the guidelines that have been developed for whole exome or genome sequencing applications for management of secondary findings (though slightly different from PGx testing in that these refer to detection of variants in multiple genes, some with clinical significance and actionability), no corresponding guidelines have been developed for PGx clinical laboratories. Nonetheless, patient and provider education will remain key components of any PGx testing program to minimize adverse responses related to secondary findings.
Pharmacogenetic (PGx) testing has been implemented in a variety of clinical settings, including inpatient and outpatient settings (Cavallari et al., 2016; Schuh and Crosby, 2019; Smith et al., 2020; Dong et al., 2021), community pharmacies (Ferreri et al., 2014), academic medical centers (Hicks et al., 2012), executive health programs (Liko et al., 2021), and nursing homes (Dorfman et al., 2020). Despite the excitement for the field to improve therapeutic decision-making, the early adopters of PGx testing have highlighted some barriers, demonstrating the complexity of initiating a new type of testing with multiple types of delivery approaches, and limited provider awareness and clinical decision support (Klein et al., 2017; Moyer and Caraballo, 2017; Lanting et al., 2020; Omer, 2020; Chang et al., 2021; Luczak et al., 2021). The debate about the value of PGx testing continues as more evidence is gathered (Davis et al., 2021; Hicks et al., 2021), impacted by when and where testing is delivered, the type of test, and cost-effectiveness (Janssens and Deverka, 2014; Plumpton et al., 2019). In contrast to disease-based genetic testing, PGx tests are perceived to raise fewer ethical and psychosocial concerns (Peterson-Iyer, 2008; Gershon et al., 2014; Haga, 2009; Meli et al., 2021) than disease-based testing and do not typically require the involvement of genetic specialists or intensive patient education and counseling. However, one of the ethical concerns about PGx testing is the potential for additional information to be revealed, known as incidental or secondary findings, (Henrikson et al., 2008; Westbrook et al., 2013). Secondary findings may be welcome for some patients and undesired by others, but regardless of preference, their management warrants consideration by clinical testing laboratories and health providers to optimize patient and provider comprehension and respect for patient preferences.
Secondary findings are not unique to PGx testing and differ slightly from other types of clinical testing. For example, asymptomatic masses detected on imaging are referred to as “incidentalomas.” The frequency of incidentalomas varies by tissue (Vernooij et al., 2007; Secchi et al., 2017; Lu et al., 2021).
In pathology, and specifically with respect to whole genome sequencing (WGS) or exome genome sequencing (WES) (analogous to a whole body scan in radiology), secondary findings occur with the detection of genetic variants throughout the genome or exome that are unrelated to the clinical indication for testing (Amendola et al., 2015). Secondary findings have also been reported with other types of comprehensive genetic and genomic applications including non-invasive prenatal testing (Bianchi et al., 2015; Mastromoro et al., 2021) and chromosomal microarray testing (Rosina et al., 2021). Although much of the literature has focused on secondary findings in the germline, it is also possible to detect secondary findings present in somatic tissues in germline testing due to mixed cell populations in the patient specimen (Weitzel et al., 2018; Chao et al., 2021). Likewise, tumor-based testing can reveal secondary germline findings (Cushman-Vokoun et al., 2021). In some cases, disease-related genes are also associated with medication responses (Hosoya and Miyagawa, 2021).
In contrast, for PGx testing, secondary findings occur due to the pleiotropic effects of some pharmacogenes, where a gene associated with a given medication response for which testing is ordered is also linked to another phenotype, either response to other medications and/or disease risks, both unrelated to the current clinical indication (therefore, same gene but multiple phenotypes). ApoE is often cited as an example of a secondary finding for PGx testing, due to its association with both statin response and risk of Alzheimer’s disease (Bainbridge et al., 2011). Furthermore, PGx testing differs from other tests in that the scope of testing is limited to the analysis of one or more genes associated with a given medication response, and therefore, the potential for discovery of a genetic variant in a gene not related to drug metabolism or other function is not possible. Thus, due to the nature of the test, certain genes like ApoE can be excluded in a PGx test, a gene which is not typically included in PGx test panels (Haga and Kantor, 2018).
These examples highlight the complexity and range of information revealed by secondary findings and the dilemmas presented with respect to the appropriate reporting, management and follow-up. Several clinical guidelines have been developed in radiology for the management of incidental findings for different tissues (Fassnacht et al., 2016; Patel et al., 2020).
With the increasing use of WGS/WES in the 2010s, several professional organizations have recognized the potential for secondary findings and/or developed guidance on how to manage these variants (van El et al., 2013; Boycott et al., 2015; Matthijs et al., 2016). In 2013, the American College of Medical Genetics and Genomics (ACMG) issued its first guideline regarding the reporting of secondary findings detected in WES/WGS testing (Green et al., 2013). A total of 56 genes were selected for which the evidence linked to a given phenotype is strong and the ability to intervene exists (i.e., “actionable”). Clinical testing laboratories can include an addendum to the WES/WGS test report of the additional genes if patients consent to receive the secondary report. The list has been revised twice: in 2017, the list was updated to include 59 genes (Kalia et al., 2017) and in 2021, 14 more genes were added to bring the total to 73 genes (Miller et al., 2021). Several papers have reported the identification of pathogenic/actionable PGx variants from WES/WGS datasets (Lee et al., 2016; Thauvin-Robinet et al., 2019; Eghbali et al., 2020). The 2017 ACMG guidelines indicated that PGx variants were being considered for inclusion in the future but none were considered for the 2021 guidance. Both RYR1 and CACNA1S are already included on the ACMG list (for malignant hyperthermia susceptibility) for which a pharmacogenetic guideline has been developed (Gonsalves et al., 2019). In patients undergoing WES/WGS, the detection of variants from the ACMG gene list in non-high-risk patients and PGx variants has raised the possibility of population health screening for some of these genes (Levy-Lahad et al., 2015; Rego et al., 2018; Chaudhari et al., 2020), though they have not been validated for this purpose (ACMG Board of Directors, 2019).
Since PGx testing is limited to a relatively small set of genes associated with metabolism, transport and other pathways important to medication response (Haga and Kantor, 2018), the potential for (and quantity of) secondary information is obviously less than WGS/WES or other broad-based testing platforms, though not insignificant. In a 2013 publication, Westbrook at el. conducted an extensive literature review to define the extent of PGx incidental findings. Based on a 34-gene PGx test panel, they identified 26 genes with a reported secondary finding and eight of these genes had secondary findings replicated (Westbrook et al., 2013). Each gene had an average of 11 reported associated phenotypes of statistical significance, but only 0.4 associated phenotypes were validated. For example, ABC1 has been associated with breast cancer, colorectal cancer, and inflammatory bowel disease. Furthermore, they reported extensive variability in the number of studies with respect to racial and ethnic diversity, with substantially fewer replicated studies for non-European groups. In 2016, Oetjens et al. analyzed 184 functional variants in 34 pharmacogenes and reported five replicated genotype-phenotype associations and identified an additional eight novel associations (Oetjens et al., 2016).
The Clinical Pharmacogenetics Implementation Consortium (CPIC) has developed 25 guidelines on the interpretation and recommendations for use of PGx test results. In each guideline, there is a section entitled “Incidental Findings” for either the gene and/or drug (or both). A review of the 25 current CPIC guidelines finds eight guidelines that mention a disease risk or phenotype (not counting CFTR for the medication ivacaftor since it is a diagnostic test for cystic fibrosis) (Table 1). Of the six guidelines on or that include CYP2D6 (Hicks et al., 2015; Bell et al., 2017; Hicks et al., 2017; Goetz et al., 2018; Brown et al., 2019; Crews et al., 2021) aside from implications for other therapies, only one noted incidental findings related to a disease risk (suicide and depression).
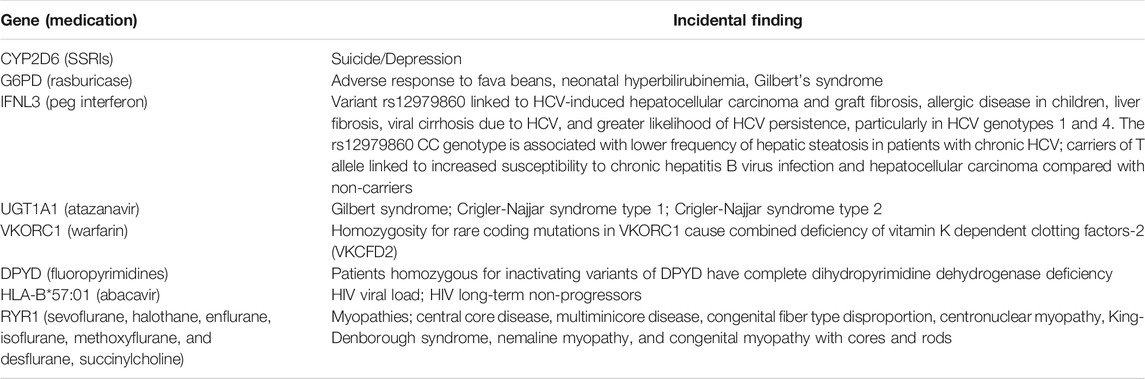
TABLE 1. Incidental findings in CPIC guidelines.
As clinical evidence continues to accumulate, the number of associations of PGx variants (and non-PGx variants) with responses to multiple medications as well as disease risk linked to their endogenous roles (Nebert and Dalton, 2006) will likely expand as presaged by the growing ACMG list. Although secondary findings have been known for some time, reports of different group’s experiences with implementing PGx testing do not mention challenges related to management of secondary findings (Pasternak et al., 2020; Luczak et al., 2021). This lack of mention may be due to inadequate evidence of many PGx secondary findings, the limited number of validated secondary findings, or a lack of reporting by clinical PGx testing laboratories (due to absence of standards on reporting).
The discovery or reporting of secondary findings may cause some patient anxiety, confusion, additional expenses, and burden on the healthcare system, if it follows the experiences of some other genetic and genomic secondary findings. Compared to a clinical sequencing test for diagnosis, PGx testing may be viewed more as an elective test and the benefits and risks of the primary and secondary findings will be weighed differently. Thus, understanding the impact of secondary findings on PGx test utilization and patient interest in secondary findings will help inform implementation strategies. A number of studies have explored patient’s (Gray et al., 2016; Mackley et al., 2017; Hicks et al., 2018; Delanne et al., 2019; Houdayer et al., 2019) and research participants’ (Bollinger et al., 2012) interest in secondary findings related to clinical sequencing, reporting mixed interest in secondary findings, though generally favorable for those that are considered to be clinically actionable. While attitudes about PGx testing overall are generally favorable, much less exploration of secondary findings has been conducted (Haga et al., 2011).
So, where are we left with respect to secondary findings and PGx testing as it stands now? Medication response is a complex phenotype impacted by both host genetics, environmental factors and the gut microbiome. A growing body of literature highlights the important role of the gut microbiome on drug response (Zhang et al., 2018; Clarke et al., 2019) as well as disease risk (Andrews et al., 2021; Zhang et al., 2021). Thus, we should not confine the definition of secondary findings to host genetic variants. Future PGx testing that includes testing of both the host genome and the gut microbiome will likely produce more secondary findings. Further adding to the complexity of data interpretation are the interactions with diet and co-medications, leading to investigations into the potential use of artificial intelligence-based prediction tools (Lin et al., 2020; de Jong et al., 2021).
To date, no standards for the reporting of secondary findings for clinical PGx testing have been developed. The path taken by the clinical sequencing community and experiences to date can inform the development of a similar approach by the PGx community. For clinical sequencing, the ACMG guideline recommends offering secondary findings to all patients irrespective of age as an opt-out (Miller et al., 2021).
A first step would be to develop a consensus list of secondary findings of pharmacogenes to avoid disparities in what information is offered or reported between laboratories (Bombard et al., 2020; Reble et al., 2021). Then, clinical PGx testing labs that include genes in their test panels with secondary findings could offer patients the option of receiving a separate report on secondary findings (Brothers et al., 2017).
However, the clinical setting in which PGx testing is offered is likely to be quite different from that in which clinical sequencing is offered with respect to the types of providers, their knowledge of genetics, and time to discuss testing with patients. Specifically, genetic specialists are not typically involved in the delivery of PGx testing and thus, the delivery of information for PGx testing (and primary and secondary test results) will be quite different. Development of patient educational materials are essential, including information about secondary findings in the informed consent forms, though at the time of our review of informed consent documents, we did not find any mention of secondary findings (Haga and Mills, 2016). Efforts should be directed toward novel patient communication strategies such as through videos or step-by-step navigational tools to explain testing or how to understand the lab report for both primary and secondary findings (if requested).
Education of providers will remain a critical component to promoting informed decision-making about testing and preferences for secondary findings. Educational support is needed for not only authorized prescribers, but other health professionals such as nurses and pharmacists. While clinical decision supports provide an important component in the appropriate use of PGx testing (Nishimura et al., 2015; Liu et al., 2021), they may not be widely accessible or as helpful with respect to secondary findings. In some cases, the PGx test-ordering provider may not be the appropriate person to communicate secondary findings and referral to a pharmacist or a genetic counselor for secondary information related to other medications or disease risk, respectively, may be warranted (Callard et al., 2012; Zierhut et al., 2017; Chart et al., 2021). Patients may be directed to access their secondary results through their primary care provider, and with the patient’s consent, copies of the test results may be sent to both the test-ordering provider and a primary care provider. Alternatively, team-based genetics groups may be established to provide immediate support for a range of secondary findings revealed by all types of genetic and genomic testing including PGx testing to both patients and their providers (Thauvin-Robinet et al., 2019).
Furthermore, with the reported benefit of re-analysis and re-interpretation of variant data to reflect new evidence (Connell et al., 2019; Liu et al., 2019; Salfati et al., 2019; Neubauer et al., 2021), updated test reports may include new information regarding primary or secondary findings. Thus, in addition to obtaining patient preferences regarding current secondary findings, laboratories may consider soliciting patient preferences about receiving updated reports for both primary and secondary findings. In time, this may become standard practice for genetic and genomic testing.
In conclusion, the identification of disease-related secondary information of PGx variants presents a more complicated scenario for PGx testing, albeit still potentially beneficial.
Whether it is an incidental finding or not has almost become incidental in the debate about the management of these findings, eclipsed by whether the results are clinically actionable or show clinical utility. Though portrayed more as a risk of testing (or any other clinical tests), secondary findings may or may not be perceived as such by patients and informing patients in advance of the possibility is the best strategy. PGx testing represents a microcosm of the larger issue of secondary findings for WGS/WES and other comprehensive genomic analysis (e.g., NIPT). Though the scale differs, the major concerns overlap, notably how best to manage secondary results and standards for identification and reporting. In time, providers and patients may begin to view genetic and genomic testing as they might with radiology and the unavoidable detection of variants outside of the clinical indication—a “side effect” of PGx testing. But until that time, provider and patient preparation are key to minimizing adverse responses to secondary findings.
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
The author is solely responsible for the outline, data, and draft of the manuscript.
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
ACMG Board of Directors (2019). The use of ACMG secondary findings recommendations for general population screening: a policy statement of the American College of Medical Genetics and Genomics (ACMG). Genet. Med. 21, 1467–1468. doi:10.1038/s41436-019-0502-5
Amendola, L. M. (2015). Chapitre IV. L'Angle Solide. Genome Res. 25, 305–438. doi:10.1101/gr.183483.11410.1515/9781501502385-005
Andrews, M. C. (2021). Gut microbiota signatures are associated with toxicity to combined CTLA-4 and PD-1 blockade. Nat. Med. 27, 1432–1441. doi:10.1038/s41591-021-01406-6
Bainbridge, M. N., Wiszniewski, W., Murdock, D. R., Friedman, J., Gonzaga-Jauregui, C., Newsham, I., et al. (2011). Whole-genome sequencing for optimized patient management. Sci. Translational Med. 3, 87re3. doi:10.1126/scitranslmed.3002243
Bell, G., Caudle, K., Whirl-Carrillo, M., Gordon, R., Hikino, K., Prows, C., et al. (2017). Clinical Pharmacogenetics Implementation Consortium (CPIC) guideline for CYP2D6 genotype and use of ondansetron and tropisetron. Clin. Pharmacol. Ther. 102, 213–218. doi:10.1002/cpt.598
Bianchi, D. W., Chudova, D., Sehnert, A. J., Bhatt, S., Murray, K., Prosen, T. L., et al. (2015). Noninvasive Prenatal Testing and Incidental Detection of Occult Maternal Malignancies. JAMA 314, 162–169. doi:10.1001/jama.2015.7120
Bollinger, J. M., Scott, J., Dvoskin, R., and Kaufman, D. (2012). Public preferences regarding the return of individual genetic research results: findings from a qualitative focus group study. Genet. Med. 14, 451–457. doi:10.1038/gim.2011.66
Bombard, Y., au, fnm., Clausen, M., Shickh, S., Mighton, C., Casalino, S., et al. (2020). Effectiveness of the Genomics ADvISER decision aid for the selection of secondary findings from genomic sequencing: a randomized clinical trial. Genet. Med. 22, 727–735. doi:10.1038/s41436-019-0702-z
Boycott, K., Hartley, T., Adam, S., Bernier, F., Chong, K., Fernandez, B. A., et al. (2015). The clinical application of genome-wide sequencing for monogenic diseases in Canada: Position Statement of the Canadian College of Medical Geneticists. J. Med. Genet. 52, 431–437. doi:10.1136/jmedgenet-2015-103144
Brothers, K. B., East, K. M., Kelley, W. V., Wright, M. F., Westbrook, M. J., Rich, C. A., et al. (2017). Eliciting preferences on secondary findings: the Preferences Instrument for Genomic Secondary Results. Genet. Med. 19, 337–344. doi:10.1038/gim.2016.110
Brown, J. T., Bishop, J. R., Sangkuhl, K., Nurmi, E. L., Mueller, D. J., Dinh, J. C., et al. (2019). Clinical Pharmacogenetics Implementation Consortium Guideline for Cytochrome P450 ( CYP ) 2D6 Genotype and Atomoxetine Therapy. Clin. Pharmacol. Ther. 106, 94–102. doi:10.1002/cpt.1409
Callard, A., Newman, W., and Payne, K. (2012). Delivering a pharmacogenetic service: is there a role for genetic counselors. J. Genet. Counsel 21, 527–535. doi:10.1007/s10897-011-9415-4
Cavallari, L. H., Lee, C. R., Duarte, J. D., Nutescu, E. A., Weitzel, K. W., Stouffer, G. A., et al. (2016). Implementation of inpatient models of pharmacogenetics programs. Am. J. Health Syst. Pharm. 73, 1944–1954. doi:10.2146/ajhp150946
Chang, W.-C., Tanoshima, R., Ross, C. J. D., and Carleton, B. C. (2021). Challenges and Opportunities in Implementing Pharmacogenetic Testing in Clinical Settings. Annu. Rev. Pharmacol. Toxicol. 61, 65–84. doi:10.1146/annurev-pharmtox-030920-025745
Chao, E. C., au, fnm., Astbury, C., Deignan, J. L., Pronold, M., Reddi, H. V., et al. (2021). Incidental detection of acquired variants in germline genetic and genomic testing: a points to consider statement of the American College of Medical Genetics and Genomics (ACMG). Genet. Med. 23, 1179–1184. doi:10.1038/s41436-021-01138-5
Chart, N. A., Kisor, D. F., and Farrell, C. L. (2021). Defining the role of pharmacists in medication-related genetic counseling. Personalized Med. 18, 509–522. doi:10.2217/pme-2021-0005
Chaudhari, B. P., Manickam, K., and McBride, K. L. (2020). A pediatric perspective on genomics and prevention in the twenty-first century. Pediatr. Res. 87, 338–344. doi:10.1038/s41390-019-0597-z
Clarke, G., Sandhu, K. V., Griffin, B. T., Dinan, T. G., Cryan, J. F., and Hyland, N. P. (2019). Gut Reactions: Breaking Down Xenobiotic-Microbiome Interactions. Pharmacol. Rev. 71, 198–224. doi:10.1124/pr.118.015768
Connell, P. S., Jeewa, A., Kearney, D. L., Tunuguntla, H., Denfield, S. W., Allen, H. D., et al. (2019). A 14‐year‐old in heart failure with multiple cardiomyopathy variants illustrates a role for signal‐to‐noise analysis in gene test re‐interpretation. Clin. Case Rep. 7, 211–217. doi:10.1002/ccr3.1920
Crews, K. R., Monte, A. A., Huddart, R., Caudle, K. E., Kharasch, E. D., Gaedigk, A., et al. (2021). Clinical Pharmacogenetics Implementation Consortium Guideline for CYP2D6 , OPRM1 , and COMT Genotypes and Select Opioid Therapy. Clin. Pharmacol. Ther. 2. doi:10.1002/cpt.2149
Cushman-Vokoun, A., Lauring, J., Pfeifer, J., Olson, D. R., Berry, A., Thorson, J., et al. (2021). Laboratory and Clinical Implications of Incidental and Secondary Germline Findings during Tumor Testing. Arch. Pathol. Lab. Med. doi:10.5858/arpa.2020-0025-CP
Davis, B. H., Williams, K., Absher, D., Korf, B., and Limdi, N. A. (2021). Evaluation of population‐level pharmacogenetic actionability in Alabama. Clin. Transl Sci. doi:10.1111/cts.13097
de Jong, J., Cutcutache, I., Page, M., Elmoufti, S., Dilley, C., Fröhlich, H., et al. (2021). Towards realizing the vision of precision medicine: AI based prediction of clinical drug response. Brain 144, 1738–1750. doi:10.1093/brain/awab108
Delanne, J., Nambot, S., Chassagne, A., Putois, O., Pelissier, A., Peyron, C., et al. (2019). Secondary findings from whole-exome/genome sequencing evaluating stakeholder perspectives. A review of the literature. Eur. J. Med. Genet. 62, 103529. doi:10.1016/j.ejmg.2018.08.010
Dong, O. M., Bates, J., Chanfreau-Coffinier, C., Naglich, M., Kelley, M. J., Meyer, L. J., et al. (2021). Veterans Affairs Pharmacogenomic Testing for Veterans (PHASER) clinical program. Pharmacogenomics 22, 137–144. doi:10.2217/pgs-2020-0173
Dorfman, R., London, Z., Metias, M., Kabakchiev, B., Mukerjee, G., and Moser, A. (2020). Individualized Medication Management in Ontario Long-Term Care Clinical Impact on Management of Depression, Pain, and Dementia. J. Am. Med. Directors Assoc. 21, 823–829. e5. doi:10.1016/j.jamda.2020.04.009
Eghbali, M., Fatemi, K. S., Salehpour, S., Abiri, M., Saei, H., Talebi, S., et al. (2020). Whole-Exome Sequencing Uncovers Novel Causative Variants and Additional Findings in Three Patients Affected by Glycogen Storage Disease Type VI and Fanconi−Bickel Syndrome. Front. Genet. 11, 601566. doi:10.3389/fgene.2020.601566
Fassnacht, M., Arlt, W., Bancos, I., Dralle, H., Newell-Price, J., Sahdev, A., et al. (2016). Management of adrenal incidentalomas: European Society of Endocrinology Clinical Practice Guideline in collaboration with the European Network for the Study of Adrenal Tumors. Eur. J. Endocrinol. 175, G1–g34. doi:10.1530/eje-16-0467
Ferreri, S. P., Greco, A. J., Michaels, N. M., O’Connor, S. K., Chater, R. W., Viera, A. J., et al. (2014). Implementation of a pharmacogenomics service in a community pharmacy. J. Am. Pharm. Assoc. 54, 172–180. doi:10.1331/JAPhA.2014.13033
Gershon, E. S., Alliey-Rodriguez, N., and Grennan, K. (2014). Ethical and public policy challenges for pharmacogenomics. Dialogues Clin. Neurosci. 16, 567–574. doi:10.31887/DCNS.2014.16.4/egershon
Goetz, M. P., Sangkuhl, K., Guchelaar, H.-J., Schwab, M., Province, M., Whirl-Carrillo, M., et al. (2018). Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2D6 and Tamoxifen Therapy. Clin. Pharmacol. Ther. 103, 770–777. doi:10.1002/cpt.1007
Gonsalves, S. G., Dirksen, R. T., Sangkuhl, K., Pulk, R., Alvarellos, M., Vo, T., et al. (2019). Clinical Pharmacogenetics Implementation Consortium ( CPIC ) Guideline for the Use of Potent Volatile Anesthetic Agents and Succinylcholine in the Context of RYR 1 or CACNA 1S Genotypes. Clin. Pharmacol. Ther. 105, 1338–1344. doi:10.1002/cpt.1319
Gray, S. W., Park, E. R., Najita, J., Martins, Y., Traeger, L., Bair, E., et al. (2016). Oncologist's and cancer patient's views on whole-exome sequencing and incidental findings: results from the CanSeq study. Genet. Med. 18, 1011–1019. doi:10.1038/gim.2015.207
Green, R. C., Berg, J. S., Grody, W. W., Kalia, S. S., Korf, B. R., Martin, C. L., et al. (2013). ACMG recommendations for reporting of incidental findings in clinical exome and genome sequencing. Genet. Med. 15, 565–574. doi:10.1038/gim.2013.73
Haga, S. B. (2009). Pharmacogenomics: Applications to Patient Care. In Ethical, Legal, Social Challenges to Applied Pharmacogenomics (Lenexa, KS: American College of Clinical Pharmacology), Chapter 16, 2007.
Haga, S. B., and Kantor, A. (2018). Horizon Scan Of Clinical Laboratories Offering Pharmacogenetic Testing. Health Aff. 37, 717–723. doi:10.1377/hlthaff.2017.1564
Haga, S. B., and Mills, R. (2016). A review of consent practices and perspectives for pharmacogenetic testing. Pharmacogenomics 17, 1595–1605. doi:10.2217/pgs-2016-0039
Haga, S. B., OʼDaniel, J. M., Tindall, G. M., Lipkus, I. R., and Agans, R. (2011). Public attitudes toward ancillary information revealed by pharmacogenetic testing under limited information conditions. Genet. Med. 13, 723–728. doi:10.1097/GIM.0b013e31821afcc0
Henrikson, N. B., Burke, W., and Veenstra, D. L. (2008). Ancillary risk information and pharmacogenetic tests: social and policy implications. Pharmacogenomics J. 8, 85–89. doi:10.1038/sj.tpj.6500457
Hicks, J., Bishop, J., Sangkuhl, K., Müller, D., Ji, Y., Leckband, S., et al. (2015). Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline forCYP2D6 and CYP2C19 Genotypes and Dosing of Selective Serotonin Reuptake Inhibitors. Clin. Pharmacol. Ther. 98, 127–134. doi:10.1002/cpt.147
Hicks, J. K., Crews, K. R., Hoffman, J. M., Kornegay, N. M., Wilkinson, M. R., Lorier, R., et al. (2012). A clinician-driven automated system for integration of pharmacogenetic interpretations into an electronic medical record. Clin. Pharmacol. Ther. 92, 563–566. doi:10.1038/clpt.2012.140
Hicks, J. K., El Rouby, N., Ong, H. H., Schildcrout, J. S., Ramsey, L. B., Shi, Y., et al. (2021). Opportunity for Genotype‐Guided Prescribing Among Adult Patients in 11 US Health Systems. Clin. Pharmacol. Ther. 110, 179–188. doi:10.1002/cpt.2161
Hicks, J. K., Shealy, A., Schreiber, A., Coleridge, M., Noss, R., Natowicz, M., et al. (2018). Patient Decisions to Receive Secondary Pharmacogenomic Findings and Development of a Multidisciplinary Practice Model to Integrate Results Into Patient Care. Clin. Translational Sci. 11, 71–76. doi:10.1111/cts.12493
Hicks, J., Sangkuhl, K., Swen, J., Ellingrod, V., Müller, D., Shimoda, K., et al. (2017). Clinical pharmacogenetics implementation consortium guideline (CPIC) for CYP2D6 and CYP2C19 genotypes and dosing of tricyclic antidepressants: 2016 update. Clin. Pharmacol. Ther. 102, 37–44. doi:10.1002/cpt.597
Hosoya, N., and Miyagawa, K. (2021). Implications of the germline variants of DNA damage response genes detected by cancer precision medicine for radiological risk communication and cancer therapy decisions. J. Radiat. Res. 62, i44–i52. doi:10.1093/jrr/rrab009
Houdayer, F., Putois, O., Babonneau, M. L., Chaumet, H., Joly, L., Juif, C., et al. (2019). Secondary findings from next generation sequencing: Psychological and ethical issues. Family and patient perspectives. Eur. J. Med. Genet. 62, 103711. doi:10.1016/j.ejmg.2019.103711
Janssens, A. C. J. W., and Deverka, P. A. (2014). Useless until proven effective: the clinical utility of preemptive pharmacogenetic testing. Clin. Pharmacol. Ther. 96, 652–654. doi:10.1038/clpt.2014.186
Kalia, S. S., au, fnm., Adelman, K., Bale, S. J., Chung, W. K., Eng, C., et al. (2017). Recommendations for reporting of secondary findings in clinical exome and genome sequencing, 2016 update (ACMG SF v2.0): a policy statement of the American College of Medical Genetics and Genomics. Genet. Med. 19, 249–255. doi:10.1038/gim.2016.190
Karen Peterson-Iyer, K. (2008). Pharmacogenomics, ethics, and public policy. Kennedy Inst. Ethics J. 18, 35–56. doi:10.1353/ken.0.0004
Klein, M. E., Parvez, M. M., and Shin, J.-G. (2017). Clinical Implementation of Pharmacogenomics for Personalized Precision Medicine: Barriers and Solutions. J. Pharm. Sci. 106, 2368–2379. doi:10.1016/j.xphs.2017.04.051
Lanting, P., Drenth, E., Boven, L., van Hoek, A., Hijlkema, A., Poot, E., et al. (2020). Practical Barriers and Facilitators Experienced by Patients, Pharmacists and Physicians to the Implementation of Pharmacogenomic Screening in Dutch Outpatient Hospital Care-An Explorative Pilot Study. Jpm 10, 293. doi:10.3390/jpm10040293
Lee, E. M. J., Xu, K., Mosbrook, E., Links, A., Guzman, J., Adams, D. R., et al. (2016). Pharmacogenomic incidental findings in 308 families: The NIH Undiagnosed Diseases Program experience. Genet. Med. 18, 1303–1307. doi:10.1038/gim.2016.47
Levy-Lahad, E., Lahad, A., and King, M.-C. (2014). Precision medicine meets public health: population screening for BRCA1 and BRCA2. JNCI J. Natl. Cancer Inst. 107, dju420. doi:10.1093/jnci/dju420
Liko, I., Corbin, L., Tobin, E., Aquilante, C. L., and Lee, Y. M. (2021). Implementation of a pharmacist-provided pharmacogenomics service in an executive health program. Am. J. Health Syst. Pharm. 10, 1093. doi:10.1093/ajhp/zxab137
Lin, E., Lin, C.-H., and Lane, H.-Y. (2020). Precision Psychiatry Applications with Pharmacogenomics: Artificial Intelligence and Machine Learning Approaches. Ijms 21, 969. doi:10.3390/ijms21030969
Liu, M., Vnencak‐Jones, C. L., Roland, B. P., Gatto, C. L., Mathe, J. L., Just, S. L., et al. (2021). A Tutorial for Pharmacogenomics Implementation through End‐to‐End Clinical Decision Support Based on Ten Years of Experience from PREDICT. Clin. Pharmacol. Ther. 109, 101–115. doi:10.1002/cpt.2079
Liu, P., Meng, L., Normand, E. A., Xia, F., Song, X., Ghazi, A., et al. (2019). Reanalysis of Clinical Exome Sequencing Data. N. Engl. J. Med. 380, 2478–2480. doi:10.1056/NEJMc1812033
Lu, S. M., Waldman, L. E., Boudiab, E. M., Lopez, C. D., Bassiri-Tehrani, B., DelMauro, M. A., et al. (2021). Incidence, Impact, and Management of Incidentalomas on Preoperative Computed Tomographic Angiograms for Breast Cancer Patients with and without Genetic Mutations. Plast. Reconstr. Surg. 147, 1259–1269. doi:10.1097/prs.0000000000007941
Luczak, T., Brown, S. J., Armbruster, D., Hundertmark, M., Brown, J., and Stenehjem, D. (2021). Strategies and settings of clinical pharmacogenetic implementation: a scoping review of pharmacogenetics programs. Pharmacogenomics 22, 345–364. doi:10.2217/pgs-2020-0181
Mackley, M. P., Fletcher, B., Parker, M., Watkins, H., and Ormondroyd, E. (2017). Stakeholder views on secondary findings in whole-genome and whole-exome sequencing: a systematic review of quantitative and qualitative studies. Genet. Med. 19, 283–293. doi:10.1038/gim.2016.109
Mastromoro, G., Guadagnolo, D., Marchionni, E., Di Palma, F., Gigante, L., Versacci, P., et al. (2021). Incidental SOS1 variant identified by non-invasive prenatal screening: Prenatal diagnosis and family clinical reassessment. Eur. J. Obstet. Gynecol. Reprod. Biol. 256, 518–520. doi:10.1016/j.ejogrb.2020.11.003
Matthijs, G., Souche, E., Alders, M., Corveleyn, A., Eck, S., Feenstra, I., et al. (2016). Erratum: Guidelines for diagnostic next-generation sequencing. Eur. J. Hum. Genet. 24, 1515. doi:10.1038/ejhg.2016.63
Meli, B. A., Fenech, A. G., Cordina, M., and Agius, E. (2021). Ethical aspects pertaining to the use of pharmacogenetic tests. Res. Soc. Administrative Pharm. 17, 799–804. doi:10.1016/j.sapharm.2020.06.013
Miller, D. T., Lee, K., Chung, W. K., Gordon, A. S., Herman, G. E., Klein, T. E., et al. (2021). ACMG SF v3.0 list for reporting of secondary findings in clinical exome and genome sequencing: a policy statement of the American College of Medical Genetics and Genomics (ACMG). Genet. Med. 23, 1381–1390. doi:10.1038/s41436-021-01172-3
Miller, D. T., Lee, K., Gordon, A. S., Amendola, L. M., Adelman, K., Bale, S. J., et al. (2021). Recommendations for reporting of secondary findings in clinical exome and genome sequencing, 2021 update: a policy statement of the American College of Medical Genetics and Genomics (ACMG). Genet. Med. 23, 1391–1398. doi:10.1038/s41436-021-01171-4
Moyer, A. M., and Caraballo, P. J. (2017). The challenges of implementing pharmacogenomic testing in the clinic. Expert Rev. Pharmacoeconomics Outcomes Res. 17, 567–577. doi:10.1080/14737167.2017.1385395
Nebert, D. W., and Dalton, T. P. (2006). The role of cytochrome P450 enzymes in endogenous signalling pathways and environmental carcinogenesis. Nat. Rev. Cancer 6, 947–960. doi:10.1038/nrc2015
Neubauer, J., Wang, S., Russo, G., and Haas, C. (2021). Re-evaluation of single nucleotide variants and identification of structural variants in a cohort of 45 sudden unexplained death cases. Int. J. Leg. Med 135, 1341–1349. doi:10.1007/s00414-021-02580-5
Nishimura, A. A., Shirts, B. H., Dorschner, M. O., Amendola, L. M., Smith, J. W., Jarvik, G. P., et al. (2015). Development of clinical decision support alerts for pharmacogenomic incidental findings from exome sequencing. Genet. Med. 17, 939–942. doi:10.1038/gim.2015.5
Oetjens, M. T., Bush, W. S., Denny, J. C., Birdwell, K., Kodaman, N., Verma, A., et al. (2016). Evidence for extensive pleiotropy among pharmacogenes. Pharmacogenomics 17, 853–866. doi:10.2217/pgs-2015-0007
Omer, M. S. (2020). Literature Review Concerning the Challenges of Implementing Pharmacogenetics in Primary Care Practice. Cureus 12, e9616. doi:10.7759/cureus.9616
Pasternak, A. L., Ward, K. M., Ateya, M. B., Choe, H. M., Thompson, A. N., Clark, J. S., et al. (2020). Establishment of a Pharmacogenetics Service Focused on Optimizing Existing Pharmacogenetic Testing at a Large Academic Health Center. Jpm 10, 154. doi:10.3390/jpm10040154
Patel, M. D., Ascher, S. M., Horrow, M. M., Pickhardt, P. J., Poder, L., Goldman, M., et al. (2020). Management of Incidental Adnexal Findings on CT and MRI: A White Paper of the ACR Incidental Findings Committee. J. Am. Coll. Radiol. 17, 248–254. doi:10.1016/j.jacr.2019.10.008
Plumpton, C. O., Pirmohamed, M., and Hughes, D. A. (2019). Cost‐Effectiveness of Panel Tests for Multiple Pharmacogenes Associated with Adverse Drug Reactions: An Evaluation Framework. Clin. Pharmacol. Ther. 105, 1429–1438. doi:10.1002/cpt.1312
Reble, E., Gutierrez Salazar, M., Zakoor, K.-R., Khalouei, S., Clausen, M., Kodida, R., et al. (2021). Beyond medically actionable results: an analytical pipeline for decreasing the burden of returning all clinically significant secondary findings. Hum. Genet. 140, 493–504. doi:10.1007/s00439-020-02220-9
Rego, S., Dagan-Rosenfeld, O., Zhou, W., Sailani, M. R., Limcaoco, P., Colbert, E., et al. (2018). High-frequency actionable pathogenic exome variants in an average-risk cohort. Cold Spring Harb Mol. Case Stud. 4, a003178. doi:10.1101/mcs.a003178
Rosina, E., Rinaldi, B., Silipigni, R., Bergamaschi, L., Gattuso, G., Signoroni, S., et al. (2021). Incidental finding of APC deletion in a child: double trouble or double chance? - a case report. Ital. J. Pediatr. 47, 31. doi:10.1186/s13052-021-00969-x
Salfati, E. L., Spencer, E. G., Topol, S. E., Muse, E. D., Rueda, M., Lucas, J. R., et al. (2019). Re-analysis of whole-exome sequencing data uncovers novel diagnostic variants and improves molecular diagnostic yields for sudden death and idiopathic diseases. Genome Med. 11, 83. doi:10.1186/s13073-019-0702-2
Schuh, M. J., and Crosby, S. (2019). Description of an Established, Fee-for-Service, Office-Based, Pharmacist-Managed Pharmacogenomics Practice. The Senior Care Pharmacist 34, 660–668. doi:10.4140/TCP.n.2019.660
Secchi, F., Di Leo, G., Zanardo, M., Alì, M., Cannaò, P. M., and Sardanelli, F. (2017). Detection of incidental cardiac findings in noncardiac chest computed tomography. Medicine (Baltimore) 96, e7531. doi:10.1097/md.0000000000007531
Smith, D. M., Peshkin, B. N., Springfield, T. B., Brown, R. P., Hwang, E., Kmiecik, S., et al. (2020). Pharmacogenetics in Practice: Estimating the Clinical Actionability of Pharmacogenetic Testing in Perioperative and Ambulatory Settings. Clin. Transl Sci. 13, 618–627. doi:10.1111/cts.12748
Thauvin-Robinet, C., Thevenon, J., Nambot, S., Delanne, J., Kuentz, P., Bruel, A.-L., et al. (2019). Secondary actionable findings identified by exome sequencing: expected impact on the organisation of care from the study of 700 consecutive tests. Eur. J. Hum. Genet. 27, 1197–1214. doi:10.1038/s41431-019-0384-7
van El, C. G., au, fnm., Cornel, M. C., Borry, P., Hastings, R. J., Fellmann, F., et al. (2013). Whole-genome sequencing in health care. Eur. J. Hum. Genet. 21, 580–584. doi:10.1038/ejhg.2013.46
Vernooij, M. W., Ikram, M. A., Tanghe, H. L., Vincent, A. J. P. E., Hofman, A., Krestin, G. P., et al. (2007). Incidental findings on brain MRI in the general population. N. Engl. J. Med. 357, 1821–1828. doi:10.1056/NEJMoa070972
Weitzel, J. N., Chao, E. C., Nehoray, B., Van Tongeren, L. R., LaDuca, H., Blazer, K. R., et al. (2018). Somatic TP53 variants frequently confound germ-line testing results. Genet. Med. 20, 809–816. doi:10.1038/gim.2017.196
Westbrook, M. J., Wright, M. F., Van Driest, S. L., McGregor, T. L., Denny, J. C., Zuvich, R. L., et al. (2013). Mapping the incidentalome: estimating incidental findings generated through clinical pharmacogenomics testing. Genet. Med. 15, 325–331. doi:10.1038/gim.2012.147
Zhang, J., Zhang, J., and Wang, R. (2018). Gut microbiota modulates drug pharmacokinetics. Drug Metab. Rev. 50, 357–368. doi:10.1080/03602532.2018.1497647
Zhang, Q., Yun, Y., An, H., Zhao, W., Ma, T., Wang, Z., et al. (2021). Gut Microbiome Composition Associated with Major Depressive Disorder and Sleep Quality. Front. Psychiatry 12, 645045. doi:10.3389/fpsyt.2021.645045
Keywords: standards, patient consent, education, incidental (secondary) findings, clinical reporting
Citation: Haga SB (2021) Revisiting Secondary Information Related to Pharmacogenetic Testing. Front. Genet. 12:741395. doi: 10.3389/fgene.2021.741395
Received: 14 July 2021; Accepted: 13 September 2021;
Published: 01 October 2021.
Edited by:
Jeffrey A. Shaman, Coriell Life Sciences (CLS), United StatesReviewed by:
Jai Narendra Patel, Levine Cancer Institute, United StatesCopyright © 2021 Haga. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Susanne B. Haga, c3VzYW5uZS5oYWdhQGR1a2UuZWR1
†ORCID: Susanne B. Haga, orcid.org/0000-0001-8817-7406
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.