
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Genet. , 17 June 2021
Sec. RNA
Volume 12 - 2021 | https://doi.org/10.3389/fgene.2021.668324
 Baofu Wang1†
Baofu Wang1† Yang Li1†Xuezeng Hao1Jingjing Yang1Xiaowan Han1
Yang Li1†Xuezeng Hao1Jingjing Yang1Xiaowan Han1 Haiyan Li1
Haiyan Li1 Tong Li1
Tong Li1 Dayang Wang1Yu Teng1Liang Ma1Yao Li1
Dayang Wang1Yu Teng1Liang Ma1Yao Li1 Mingjing Zhao1*Xian Wang1,2*
Mingjing Zhao1*Xian Wang1,2*Background/Aims: This study aimed to compare the clinical value of the peak time point and area under the curve (AUC) of miRNAs and conventional biomarkers in acute myocardial infarction (AMI).
Methods: A literature search was carried out in PubMed, Web of Science, Embase, and Cochrane systematically. Screening studies, extracting data, and assessing article quality were performed independently by two researchers. Also, the names of miRNAs in the included studies were standardized by the miRBase database.
Results: A total of 40 studies, encompassing 6,960 participants, were included in this systematic review. The samples of circulating miRNAs were mainly from the plasma. The results of this systematic review displayed that miR-1-3p, miR-19b-3p, miR-22-5p, miR-122-5p, miR-124-3p, miR-133a/b, miR-134-5p, miR-150-5p, miR-186-5p, miR-208a, miR-223-3p, miR-483-5p, and miR-499a-5p reached peak time earlier and showed a shorter time window than the conventional biomarkers despite the different collection times of initial blood samples. miR-1-3p, miR-19b-3p, miR-133a/b, miR-208a/b, miR-223-3p, miR-483-5p, and miR-499a-5p were shown to be more valuable than classical biomarkers for the early diagnosis of AMI, and these miRNAs appeared to have the most potential biomarkers within 4 h of the onset of symptoms except miR-133a/b and miR-208b. Moreover, combined miRNAs or miRNAs combined with classical biomarkers could compensate for the deficiency of single miRNA and conventional biomarker in sensitivity or specificity for an optimal clinical value.
Conclusions: miR-1-3p, miR-19b-3p, miR-208a, miR-223-3p, miR-483-5p, and miR-499a-5p are promising biomarkers for AMI due to their satisfactory diagnostic accuracy and short time window (within 4 h of the onset of symptoms).
Acute myocardial infarction (AMI) accounted for the major proportion of morbidity and mortality in coronary heart disease (CHD) (White and Chew, 2008). Early diagnosis can prevent and alleviate cardiac cell death, improve heart function, and reduce cardiovascular adverse events. Conventional blood biomarkers, such as cardiac troponin (cTn), creatine kinase MB (CKMB), and high-sensitivity cTnT (hs-cTnT), are regarded as gold standards and widely used to diagnose AMI (Thygesen et al., 2018). However, circulating cTn is released slowly such that the concentration cannot be detected immediately in the early phase of AMI (Baker et al., 2011). In addition, these biomarkers have some limitations in specificity. Some non-AMI diseases, including myopericarditis, acute heart failure, stable chronic heart failure, acute pulmonary embolism, and chronic kidney disease, can falsely elevate cTn (Giannitsis and Katus, 2013; Thygesen et al., 2018). Thus, a novel diagnostic biomarker is necessary to meet the clinical demands.
MicroRNAs (miRNAs) are endogenous small non-coding RNAs that play a major role in various physiological and pathological processes (Lalem and Devaux, 2019). Due to their stability and tissue/cell specificity in peripheral circulation (Mitchell et al., 2008; D'Alessandra et al., 2010), a large number of circulating miRNAs have been reported as new potential biomarkers for diagnosing AMI (Zhao et al., 2019; Su J. et al., 2020; Wexler and Nussinovitch, 2020). However, whether miRNAs have a similar or equal clinical value with traditional biomarkers is yet to be elucidated. Therefore, this systematic review was conducted to compare the time window and area under the curve (AUC) of miRNAs and conventional biomarkers (cTnI/cTnT/CKMB/hs-cTnT).
Articles published before September 9, 2020, were searched comprehensively in electronic databases (PubMed, Web of Science, Embase and Cochrane) using the search terms “myocardial infarction” and “microRNAs” and their common synonyms.
The inclusion criteria of the studies were as follows: ① participants in the case group met the diagnostic criteria of AMI/ST-segment elevation myocardial infarction (STEMI)/non-ST-segment elevation myocardial infarction (NSTEMI) and the control group was non-AMI, including healthy volunteers or subjects without MI/AMI/cardiovascular disease; ② items were related to peak hour comparison of miRNAs and conventional biomarkers or AUC comparison of miRNAs and conventional biomarkers or peak hour and AUC comparison of miRNAs and conventional biomarkers; ③ the samples were from the plasma or serum. The exclusion criteria were as follows: ① non-clinical study; ② articles with incomplete information; ③ reviews, meta-analyses, and corresponding/conference abstracts.
Titles and abstracts of all included studies were assessed independently by two researchers (BW and YL) according to the inclusion and exclusion criteria. Data, including first author's name, year of publication, country, inclusion criteria, sample size, age, gender, medical history, miRNAs, classical biomarkers, detection method, detection time points, peak point, AUC, sensitivity, and specificity, were extracted from the included studies. The names of miRNAs were also standardized through the miRBase database. Any disagreement was resolved by discussing and consulting with the corresponding authors (MZ and XW).
The Newcastle–Ottawa scale (NOS) was used to assess the quality of studies based on three factors: the selection of the research population, compatibility of the study groups, and measurement of exposure factors. Each study scored 0–9 points.
A qualitative synthesis was adopted for this systematic review.
A total of 6,355 records were identified from four electronic databases, and 2,231 duplicate articles were removed. Subsequently, 4,017 studies were excluded after screening titles and abstracts, and 107 articles were subjected to full-text analysis. Finally, 40 studies that fulfilled the selection criteria were divided into three categories as follows, and the specific filtering process was illustrated in Figure 1.
① Peak hour comparison of miRNAs and conventional biomarkers (10 studies).
② AUC comparison of miRNAs and conventional biomarkers (26 studies).
③ Peak hour and AUC comparison of miRNAs and conventional biomarkers (4 studies).
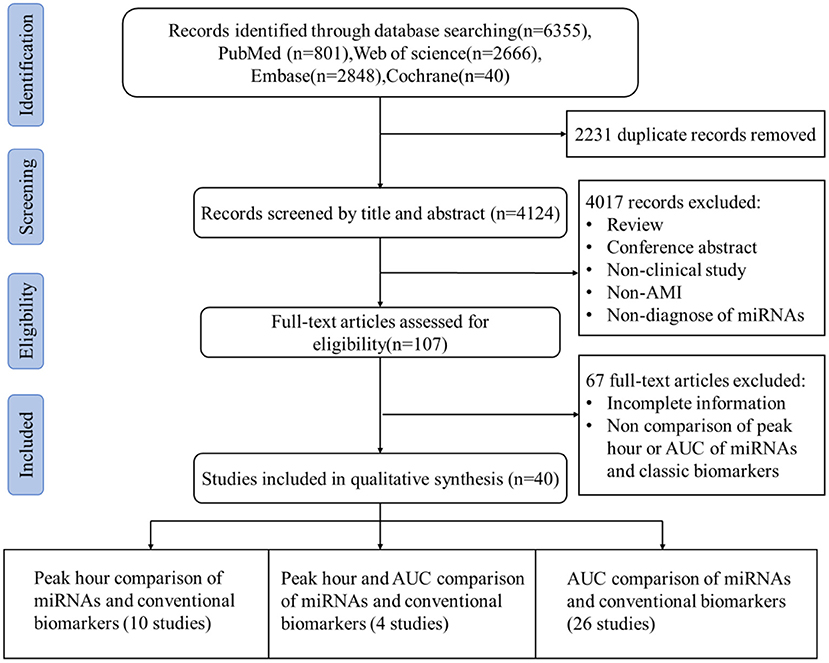
Figure 1. Flow diagram of the literature search.
Overall, 6,960 participants were included based on the criteria of non-AMI (healthy volunteers or those without MI/AMI/cardiovascular disease) and AMI/STEMI/NSTEMI. A majority of studies focused on the miRNAs in the plasma, followed by the serum (Supplementary Tables 2–4), and qPCR was used to detect miRNAs. Also, the names of miRNAs were standardized by the miRBase database (Supplementary Table 1). The data of study ID, inclusive criteria, sample size, peak hour, and AUC of miRNAs and classical biomarkers were extracted for further evaluation.
1. Peak hour comparison of miRNAs and conventional biomarkers: As shown in Table 1, 561 participants from China, Portugal, Italy, and Poland were included. Notably, the time of collecting initial blood samples varied. The first samples were gained from the onset of symptoms/admission/cardiac catheterization, and the detection time interval was also different.
2. AUC comparison of miRNAs and conventional biomarkers: Participants who met the inclusive criteria were recruited in the study. The majority of the studies focused on the comparison between miR-1-3p/miR-133a/miR-208a/miR-208b/miR-499-5p and cTnT/cTnI, but only a few studies addressed the comparison of sensitivity and specificity (Table 2).
3. Peak hour and AUC comparison of miRNAs and conventional biomarkers: 349 participants diagnosed with AMI and 292 participants with non-AMI were enrolled in the studies (Table 3A). Three studies used plasma to detect miRNAs and classical biomarkers, while one study used plasma to detect miRNAs and serum for classical biomarkers. Although the first samples were obtained from the onset of symptoms, the detection time interval was also different. Furthermore, the comparison of AUC only referred to miRNAs and cTnI/CKMB (Table 3B).
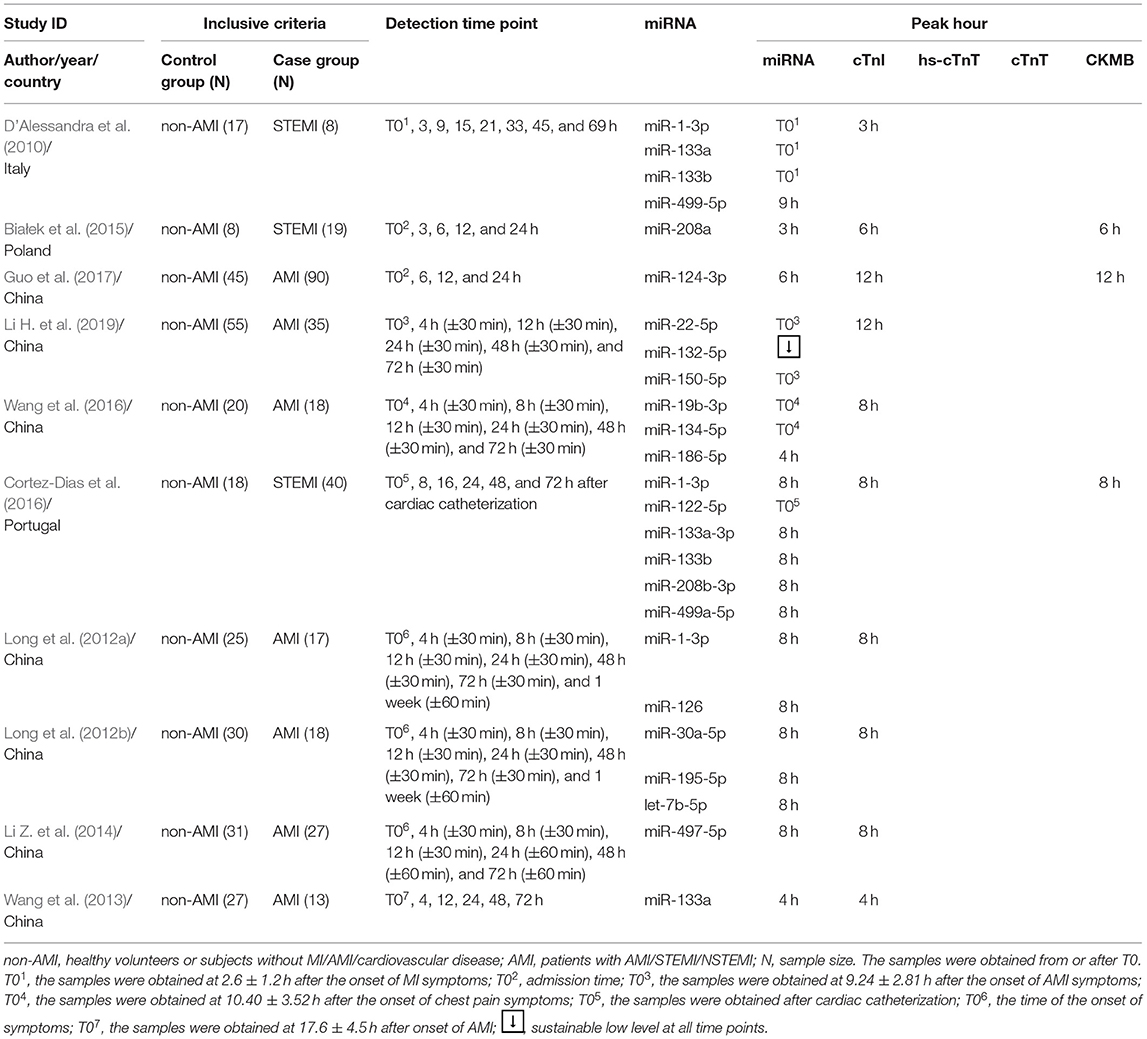
Table 1. Peak hour comparison of miRNAs and conventional biomarkers.
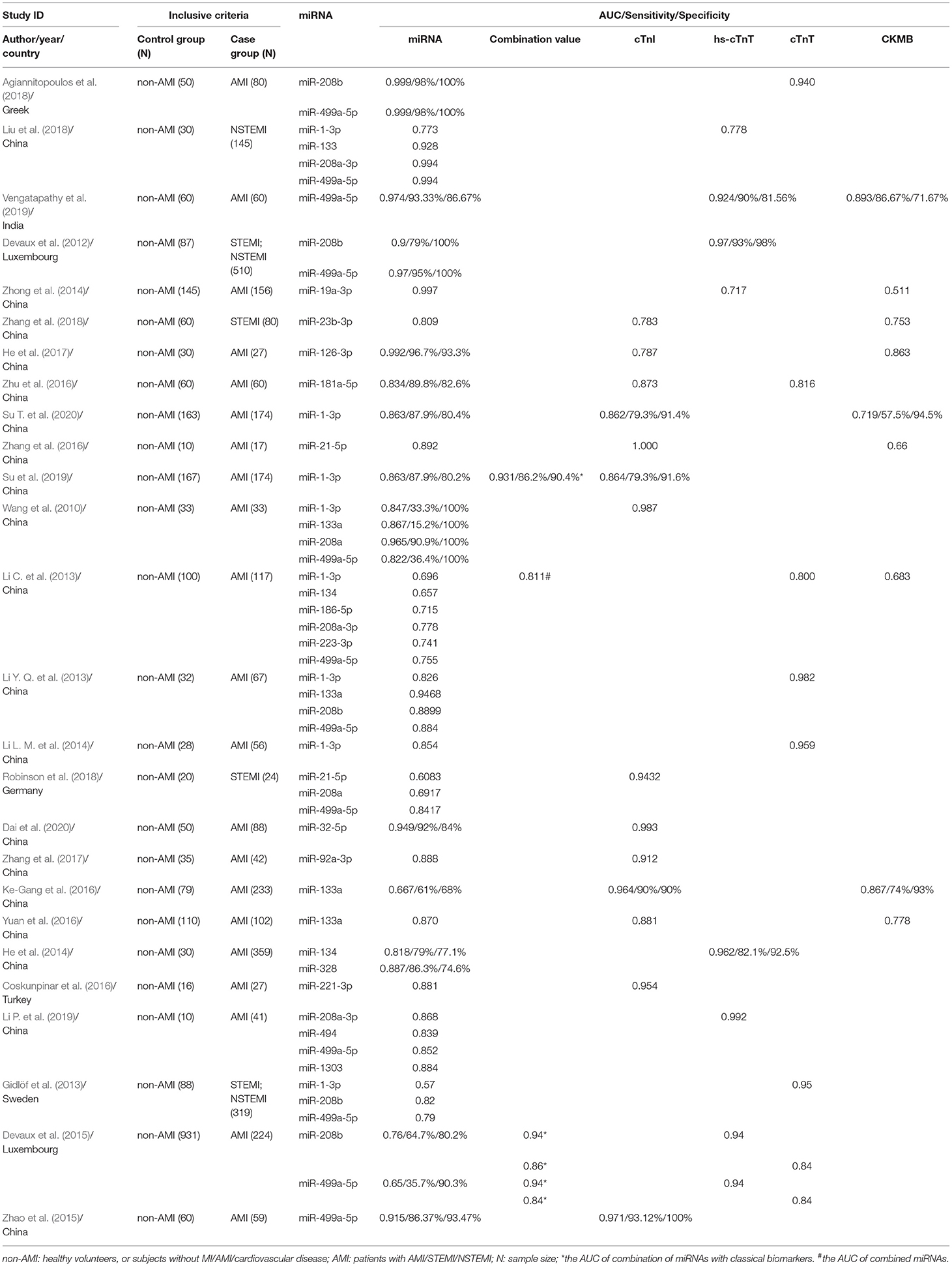
Table 2. AUC comparison of miRNAs and conventional biomarkers.
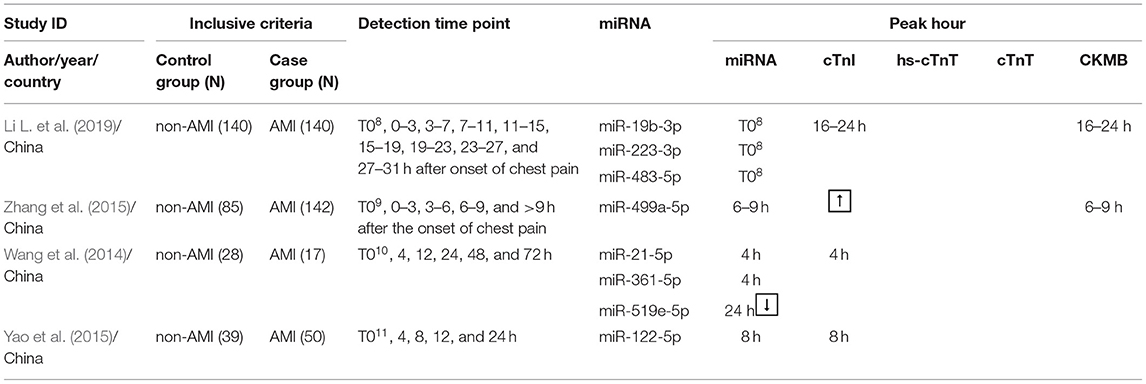
Table 3A. Peak hour and AUC comparison of miRNAs and conventional biomarkers.
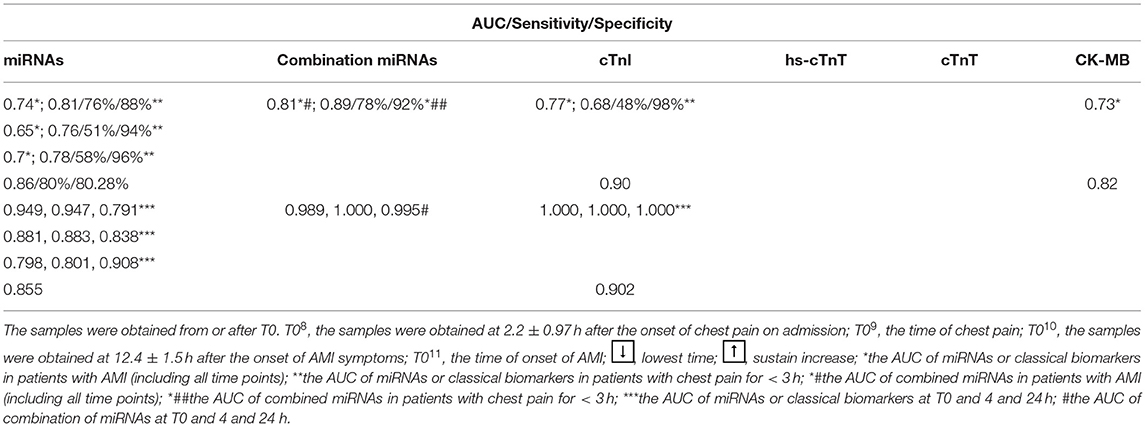
Table 3B. Peak hour and AUC comparison of miRNAs and conventional biomarkers.
The mean score of NOS in the included studies was 7.05. The quality assessment of the included studies was described in the Supplementary Table 5.
As shown in Table 1, most miRNAs showed a satisfactory time window for identifying the early phase of AMI despite different sampling and detecting time points. The level of miR-1-3p, miR-19b-3p, miR-22-5p, miR-122-5p, miR-124-3p, miR-133a, miR-133b, miR-134-5p, miR-150-5p, miR-186-5p, and miR-208a was dynamically detected from T0. miR-1-3p, miR-19b-3p, miR-22-5p, miR-122-5p, miR-133a, miR-133b, miR-134-5p, and miR-150-5p achieved peak immediately at T0 while miR-124-3p, miR-186-5p, and miR-208a expressions reached the peak levels at 6, 4, and 3 h, respectively. These miRNAs reached the peak expression 3–12 h earlier than cTnI/CKMB in the early phase of AMI (D'Alessandra et al., 2010; Białek et al., 2015; Cortez-Dias et al., 2016; Wang et al., 2016; Guo et al., 2017; Li H. et al., 2019).
Other publications revealed that miRNAs could be detected concurrently to, or later than, conventional biomarkers. Five studies showed that miRNAs, including let-7b-5p, miR-1-3p, miR-30a-5p, miR-126, miR-133a, miR-133a-3p, miR-133b, miR-195-5p, miR-208b-3p, miR-497-5p, and miR-499a-5p exhibited a similar trend to that of traditional biomarkers and achieved a peak at the same time points (Long et al., 2012a,b; Wang et al., 2013; Li L. M. et al., 2014; Cortez-Dias et al., 2016). Wang et al. (2013) collected blood samples at 4, 12, 24, 48, and 72 h after T0, and the results showed that circulating miR-133a and cTnI increased and achieved a peak at 4 h. Four other studies revealed that let-7b-5p, miR-1-3p, miR-30a-5p, miR-126, miR-133a-3p, miR-133b, miR-195-5p, miR-208b-3p, miR-497-5p, and miR-499a-5p were highly expressed in AMI compared to the control group and reached the peak expression at 8 h, which was similar to that of cTnI (Long et al., 2012a,b; Li Z. et al., 2014; Cortez-Dias et al., 2016) and CKMB (Cortez-Dias et al., 2016). In addition, miR-132-5p displayed a sustainable low level at all time points, and miR-499a-5p showed a peak level (9 h) later than that of cTnI (3 h) (D'Alessandra et al., 2010; Li H. et al., 2019).
As shown in Table 2, some studies reported that miRNAs had a better accuracy than the classical biomarkers. Agiannitopoulos et al. (2018) found that the AUC of both miR-208b and miR-499a-5p was 0.999, which was slightly higher than that of cTnT (0.94). Liu et al., Vengatapathy et al., and Devaux et al. showed that the diagnostic value of miR-208a-3p [0.994 (Liu et al., 2018)] and miR-499a-5p [0.994 (Liu et al., 2018), 0.974 (Vengatapathy et al., 2019), and 0.97 (Devaux et al., 2012)] was no less than that of hs-cTnT [0.778 (Liu et al., 2018), 0.924 (Vengatapathy et al., 2019), and 0.97 (Devaux et al., 2012)]. miR-133 and miR-19a-3p also showed a satisfactory diagnostic value, and the AUC of miR-133 and miR-19a-3p was 0.928 (Liu et al., 2018) and 0.997 (Zhong et al., 2014), respectively, compared to that of hs-cTnT [0.778 (Liu et al., 2018) and 0.717 (Zhong et al., 2014), respectively]. In addition, miR-23b-3p, miR-126-3p, and miR-181a-5p also showed a more accurate AUC. The AUC for miR-23b-3p, miR-126-3p, and miR-181a-5p was 0.809 (Zhang et al., 2018), 0.992 (He et al., 2017), and 0.834 (Zhu et al., 2016), respectively, which were higher than those of cTnI [0.783 (Zhang et al., 2018) and 0.787 (He et al., 2017)] and cTnT [0.816 (Zhu et al., 2016)]. Moreover, most of the studies revealed that the AUC of miRNAs was also superior to that of CKMB. As shown in Table 2, the AUC of miRNAs was 0.013–0.486 higher than that of CKMB, especially miR-1-3p, miR-19a-3p, miR-21-5p, and miR-126-3p, which were 0.144 (Su T. et al., 2020), 0.486 (Zhong et al., 2014), 0.232 (Zhang et al., 2016), and 0.129 (He et al., 2017) higher than that of CKMB.
There were also studies that revealed different results. The AUC of miRNAs was lower than that of cTnI, cTnT, and hs-cTnT, but yet satisfactory. In Table 2, the AUC of miR-1-3p was 0.773 (Liu et al., 2018), 0.863 (Su et al., 2019; Su T. et al., 2020), 0.847 (Wang et al., 2010), 0.696 (Li C. et al., 2013), 0.826 (Li Y. Q. et al., 2013), and 0.854 (Li L. M. et al., 2014), which resembled that of cTnI [0.862 (Su T. et al., 2020) and 0.864 (Su et al., 2019)] and hs-cTnT [0.778 (Liu et al., 2018)] or was lower than that of cTnI [0.987 (Wang et al., 2010)] and cTnT [0.800 (Li C. et al., 2013), 0.982 (Li Y. Q. et al., 2013), and 0.959 (Li L. M. et al., 2014)]. The results of the AUC comparison of miR-21-5p (Zhang et al., 2016; Robinson et al., 2018), miR-32-5p (Dai et al., 2020), miR-92a-3p (Zhang et al., 2017), miR-133a (Wang et al., 2010; Li Y. Q. et al., 2013; Ke-Gang et al., 2016; Yuan et al., 2016), miR-134 (Li C. et al., 2013; He et al., 2014), miR-181a-5p (Zhu et al., 2016), miR-186-5p (Li C. et al., 2013), miR-221-3p (Coskunpinar et al., 2016), miR-223-3p (Li C. et al., 2013), miR-208a-3p (Li C. et al., 2013; Li P. et al., 2019), miR-208a (Wang et al., 2010; Robinson et al., 2018), miR-208b (Devaux et al., 2012, 2015; Gidlöf et al., 2013; Li Y. Q. et al., 2013), miR-494 (Li P. et al., 2019), miR-499a-5p (Wang et al., 2010; Gidlöf et al., 2013; Li C. et al., 2013; Li Y. Q. et al., 2013; Devaux et al., 2015; Zhao et al., 2015; Robinson et al., 2018; Li P. et al., 2019), miR-328 (He et al., 2014), and miR-1303 (Li P. et al., 2019) with traditional biomarkers were similar to those with miR-1-3p.
Table 2 showed that the combination miRNAs or combination miRNAs with classical biomarkers increased the AUC of single miRNAs and traditional biomarkers. According to the publications, Li C. et al. (2013) demonstrated that the combination of miR-1-3p, miR-134, miR-186-5p, miR-208a-3p, miR-223-3p, and miR-499a-5p increased the AUC to 0.811, which was higher than that of the single miRNAs (miR-1-3p: 0.696; miR-134: 0.657; miR-186-5p: 0.715; miR-208a-3p: 0.778; miR-223-3p: 0.741; and miR-499a-5p: 0.755) and cTnT (0.800). Besides that, the diagnostic value of combined miRNAs and classical biomarkers was also increased. The AUC of the combination of miR-1-3p with cTnT, miR-208b with hs-cTnT, miR-208b with cTnT, miR-499a-5p with hs-cTnT, and miR-499a-5p with cTnT was 0.931, 0.94, 0.86, 0.94, and 0.84, respectively, which were significantly higher than that of single miRNA [miR-1-3p: 0.863 (Su et al., 2019); miR-208b: 0.76 (Devaux et al., 2015); and miR-499a-5p: 0.65 (Devaux et al., 2015)], cTnI [0.864 (Su et al., 2019)], and cTnT [0.84 (Devaux et al., 2015)], while the AUC of the combination of miR-208b with hs-cTnT (0.94) and miR-499a-5p with hs-cTnT (0.94) was identical to that of hs-cTnT (0.94) (Devaux et al., 2015).
A few studies compared the sensitivity and specificity of miRNAs and conventional biomarkers. In the study by Su et al., miR-1-3p had a better sensitivity but lower specificity [87.9 and 80.4% (Su T. et al., 2020); 87.9 and 80.2% (Su et al., 2019)] than cTnI [79.3 and 91.4% (Su T. et al., 2020); 79.3 and 91.6% (Su et al., 2019)] and CKMB [57.5 and 94.5% (Su T. et al., 2020)]. In the combination of miR-1-3p and cTnT, the specificity could be increased to 90.4% with a stable sensitivity (86.2%), higher than the specificity of miR-1-3p (80.2%) and the sensitivity of cTnI (79.3%) (Su et al., 2019). Furthermore, the study of Devaux et al. (2012) demonstrated that the specificity of miR-208b or miR-499a-5p could reach 100% while that of hs-cTnT was 98% and that the sensitivity of miR-499a-5p (95%) was also slightly higher than that of hs-cTnT (93%). Other studies also reported that the specificity of miR-1-3p, miR-133a, miR-208a, miR-208b, or miR-499a-5p could reach 100% with a satisfactory sensitivity, but there were no references of traditional biomarkers (Wang et al., 2010; Agiannitopoulos et al., 2018). Overall, 13 studies were involved, and the range of specificity of most miRNAs was 80–100%, and that of sensitivity was 79–100% (Table 2).
A total of four studies reported the peak hour and AUC of miRNAs and classical biomarkers simultaneously. As shown in Table 3, Li L. et al. (2019) reported that the levels of miR-19b-3p, miR-223-3p, and miR-483-5p were significantly increased in patients with AMI, and the highest concentration was at T0 while cTnI and CKMB reached the peak level at 16–24 h after T0. The AUC of miR-19b-3p, miR-223-3p, and miR-483-5p was 0.74, 0.65, and 0.7, respectively, lower than that of cTnI (0.77). However, the AUC of the combination of these three miRNAs could get an incremental value (0.81) for diagnosis of AMI (including subjects with chest pain for <3, 3–6, and ≥6 h), which was higher than that of cTnI (0.77) and CKMB (0.73). Furthermore, the present study demonstrated that these three miRNAs have an optimal AMI diagnostic value in patients with chest pain for <3 h. The data showed that the AUC for miR-19b-3p, miR-223-3p, miR-483-5p, and the miRNA panel (a combination of these three miRNAs) was 0.81, 0.76, 0.78, and 0.89, respectively, and each miRNA had better diagnostic accuracy compared with cTnI (0.68). Meanwhile, the sensitivity of miR-19b-3p, miR-223-3p, miR-483-5p, and the miRNA panel was 76, 51, 58, and 78%, respectively, higher than that of cTnI (48%). Also, the specificity of miR-19b-3p (88%), miR-223-3p (94%), miR-483-5p (96%), and miRNA panel (92%) was satisfactory. Notably, 76.1 and 77.5% of all AMI patients with chest pain for <3 h were detected positive by miR-19b-3P and the miRNA panel, respectively, which was significantly higher than the figure of cTnI (47.8%).
Other studies reported that the expression of circulating miR-21-5p, miR-122-5p, miR-361-5p, and miR-499a-5p was significantly increased while miR-519e-5p had a remarkably reduced expression and exhibited the lowest concentration at 24 h after T0 (Wang et al., 2014; Yao et al., 2015; Zhang et al., 2015). miR-21-5p, miR-122-5p, miR-361-5p, and miR-499a-5p reached their peak expression at 4, 8, 4, and 6–9 h, respectively, and the peak time of miR-21-5p, miR-122-5p, and miR-361-5p was similar to that of cTnI (Wang et al., 2014; Yao et al., 2015; Zhang et al., 2015). However, the AUC of these miRNAs (miR-21-5p, miR-122-5p, miR-361-5p, miR-519e-5p, and miR-499a-5p) was not superior to that of cTnI. As shown in Table 3B, the diagnostic value of these miRNAs was similar to that of cTnI and CKMB, whereas the AUC of miR-21-5p and miR-361-5p decreased with prolonged detection time. The optimal diagnostic value of the combination of miRNA-21-5p, miRNA-361-5p, and miRNA-519e-5p was at T4 (1.00), while cTnI showed a stable diagnostic value at T0 (1.00), T4 (1.00), and T24 (1.00) (Wang et al., 2014).
AMI is one of the leading causes of death worldwide, and an early diagnostic marker is crucial and imperative for the efficient and timely therapy of AMI. cTn and CKMB are currently regarded as the critical biomarkers in diagnosing AMI. However, their clinical value for diagnosing early AMI and distinguishing it from non-AMI diseases remains limited (Feng et al., 2008; Moe and Wong, 2010; Thygesen et al., 2018). cTn and CKMB are released from cardiomyocytes when the myocardial cell membrane is damaged during ischemia, hypoxia, etc. The level of cTn in the plasma is elevated in 5–8 h after MI, and the high level could be sustained for 7–10 days, while CKMB is elevated in 4–8 h after MI, and the high level is sustained for 2–3 days (Feng et al., 2008; Yue et al., 2018). Nevertheless, the property of cTn and CKMB for early diagnosis of AMI is weak because the level of these biomarkers elevates late after MI. Thus, a biomarker that could be detected at the early stage of AMI with a better diagnostic value is needed to compensate for the deficiency of cTn and CKMB.
Recently, increasing studies demonstrated that miRNAs were a new era for the management of various diseases, and the role of miRNAs in the timely diagnosis of AMI was promising due to their stability and tissue/cell specificity in peripheral circulation (Mitchell et al., 2008; D'Alessandra et al., 2010; Rupaimoole and Slack, 2017; Li H. et al., 2019; Li P. et al., 2019). Therefore, a systematic review comparing the peak time point and AUC of miRNAs with conventional biomarkers in AMI was performed to clarify the potential diagnostic value of miRNAs in AMI. Among the included studies, most explored the peak time point or AUC of miRNAs, while only a few reported the peak time point and AUC of miRNAs with conventional biomarkers simultaneously.
This study presented that miRNAs might be superior for detection in the early phase of AMI. The consensus that passive leakage from ruptured cells and active secretion through extracellular vesicles derived from stimulated cells are two sources of circulating miRNAs was achieved (Zhang et al., 2013). The miRNAs can be packed in extracellular vesicles and released into the bloodstream when the myocardial cells undergo a microenvironment of ischemia–hypoxia, while cTn leaks into the blood when the myocardial membrane is damaged. Moreover, some miRNA compounds found in cells are more soluble and released into the bloodstream more easily than cTn (Akat et al., 2014). Therefore, miRNAs may be detected earlier than classical biomarkers. In this review, the miR-1-3p, miR-19b-3p, miR-22-5p, miR-122-5p, miR-124-3p, miR-133a, miR-133b, miR-134-5p, miR-150-5p, miR-186-5p, miR-208a, miR-223-3p, miR-483-5p, and miR-499a-5p reached a peak expression earlier than did cTnI/CKMB (D'Alessandra et al., 2010; Białek et al., 2015; Zhang et al., 2015; Cortez-Dias et al., 2016; Wang et al., 2016; Guo et al., 2017; Li H. et al., 2019; Li L. et al., 2019). Furthermore, miR-499a-5p presented as early as 1 h while cTnI and CK-MB were detected 2 h after chest pain in the study by Zhang et al. (2015) These studies indicate that the miRNAs have a short window and might compensate for the deficiency of cTnI/CKMB in the early phase of AMI. However, notably, the peak time of the same miRNAs was diverse in different studies. For example, miR-1-3p and miR-133a reached their peak earlier than cTnI in the study of D'Alessandra et al. (2010) while other studies suggested that the peak time points of miR-1-3p and miR-133a were the same as that of cTnI and CKMB. It is undeniable that the different collection times of the initial blood sample and the different detection time intervals in the included studies might be crucial factors for the peak time pints of miRNAs and the classical biomarkers. The onset time of chest pain symptom provided by patients might not be accurate, which is also a factor that could not be neglected.
Interestingly, this review also showed that most miRNAs possessed satisfactory AUC (0.75–0.99). Among the miRNAs mentioned, miR-1-3p, miR-133a/b, miR-208a/b, and miR-499a-5p got more attention. miR-1, miR-133a, miR-208a/b, and miR-499 are abundantly expressed in the myocardium and involved in various effects associated with heart wounding, arrhythmia, myocardial apoptosis, fibrosis, hypertrophy, and tissue remodeling. In cardiac pathology, including AMI, the expression of miR-1, miR-133a, miR-208a/b, and miR-499 is significantly elevated, and the level of increased cardiac miRNAs in circulation endows miRNAs with the ability of diagnosis for the early phase of AMI (Chistiakov et al., 2016). In this review, most studies reported that the AUC of miR-1, miR-133a/b, miR-208a/b, and miR-499a-5p showed a similar clinical value with that of the traditional biomarkers (Table 2) and that miR-1-3p, miR-133a/b, miR-208a, and miR-499a-5p also presented a short time window (Table 1). The AUC of miRNAs, such as miR-208b and miR-499a-5p, might be more accurate with prolonged detection time, and the diagnostic value is similar to that of hs-cTnT. Moreover, non-AMI diseases, including myopericarditis, acute/chronic heart failure, acute pulmonary embolism, chronic kidney disease, connective tissue disease, and skeletal muscle injury, could lead to a false increase in cTn and CKMB (Feng et al., 2008; Giannitsis and Katus, 2013; Thygesen et al., 2018). Some researches indicated that miR-1-3p, miR-133a, miR-208a/b, and miR-499a-5p might have better specificity than cTn and CKMB, and the specificity could even reach 100%. According to Wang et al. (2010) miR-499a-5p was mainly presented in the heart, and the expression was higher than that in skeletal muscle. Remarkably, miR-208a was only detected in the heart but not in the skeletal muscle. To further clarify the cardiac specificity of miR-208a, Wang et al. (2010) determined the levels of miR-208a in plasma from patients with AMI, acute kidney injury, chronic renal failure, stroke, and trauma. The results demonstrated that miR-208a could only be determined significantly with the highest sensitivity and specificity in AMI patients, but not acute kidney injury, chronic renal failure, stroke, and trauma. The expression level of serum miRNA-499a-5p in patients with stroke, acute and chronic kidney failure, or trauma was also significantly lower than that in patients with AMI (Zhao et al., 2015). Therefore, miRNAs might have optimal specificity to identify AMI from other non-AMI diseases. In addition, this review also showed that combined miRNAs or miRNAs combined with classical biomarkers could provide optimal sensitivity and specificity while enhancing the AUC of single miRNA or classical biomarker. Su et al. (2019) revealed that the combination of miR-1-3p with cTnI improved the sensitivity and the specificity to 86.2 and 90.5%, respectively, which were higher than the sensitivity of cTnI (79.3%) and the specificity of miR-1 (80.2%). These indicated that a combination of miRNAs with traditional biomarkers could compensate for the deficiency of single miRNA and conventional biomarker in sensitivity or specificity. In addition, miR-19a-3p, miR-21-5p, miR-23b-3p, miR-32-5p, miR-92a-3p, miR-134, miR-181a-5p, miR-221-3p, miR-328, miR-494, and miR-1303 also showed a dysregulated level in AMI (Table 2), but their diagnostic value still needs to be verified by a large simple size.
This review further showed that the diagnostic value of miRNAs was associated with the onset time of chest pain, and the miRNAs might show a superior clinical value to traditional biomarkers in patients with AMI within 4 h of the onset of symptoms. In the study by Li L. et al. (2019) the AUC of miR-19b-3p (0.74), miR-223-3p (0.65), and miR-483-5p (0.7) was lower than that of cTnI (0.77) and CKMB (0.73) for diagnosis of AMI (including subjects with chest pain for <3, 3–6, and ≥6 h). Nevertheless, the diagnostic value of these three miRNAs was elevated in subjects with chest pain for <3 h. The AUC for miR-19b-3p, miR-223-3p, and miR-483-5p, and the miRNA panel (a combination of these three miRNAs) was 0.81, 0.76, 0.78, and 0.89, respectively, and each miRNA had better diagnostic accuracy than cTnI (0.68). Meanwhile, the sensitivity of the three miRNAs and the miRNA panel was higher than that of cTnI, and the specificity was also optimal. Furthermore, the positive detection rate of AMI of patients with chest pain for <3 h by miR-19b-3p (76.1%) and the miRNA panel (77.5%) was higher than that of cTnI (47.8%). In the study by Devaux et al. (2012), miR-499a-5p was positive in 93% of patients who presented <3 h after onset of pain while positive expression of hs-cTnT was in 88% of patients. Additionally, miR-1-3p also showed a satisfying diagnostic value compared to the classical biomarkers in subjects within 3 h of the onset of symptoms in the study by Su T. et al. (2020) and Su et al. (2019). Wang et al. (2010) also indicated that miR-208a might have a higher sensitivity than the classical biomarkers in the early AMI stage. All the patients with AMI within 4 h of the onset of symptoms could be detected by miR-208a, while 85% of the cases were detected by cTnI. These phenomena indicated that miRNAs might have better sensitivity than conventional biomarkers in patients with AMI within 4 h of the onset of symptoms. However, in the included studies, most did not record the exact onset time of chest pain or classified the patients according to the time of chest pain, which might be a critical factor for the different trend of diagnostic value of the same miRNAs.
Overall, miR-1-3p, miR-19b-3p, miR-133a/b, miR-208a/b, miR-223-3p, miR-483-5p, and miR-499a-5p may be more valuable than classical biomarkers for the early diagnosis of AMI, and these miRNAs show a short time window within 4 h of the onset of symptoms and satisfactory sensitivity and specificity, except miR-133a/b and miR-208b. Combined miRNAs or miRNAs combined with traditional biomarkers could also compensate for the deficiency of single miRNA or traditional biomarker with respect to sensitivity or specificity for an optimal clinal value. Nonetheless, some confounders and limitations of this review should be considered due to the restricted reports.
Subjects, sample size, the collecting time of samples, and quantitative methods of miRNAs not only were the main potential confounders and limitations of this systematic review but also influenced the inconsistency of the level, peak time, and statistical significance of the same miRNAs.
For the sample size of included studies, 27/40 studies enrolled subjects with a case group of <100. Ten and three studies had case group sample sizes of 100–300 and ≥300, respectively. miR-1-3p, miR-19b-3p, miR-133a/b, miR-208a/b, miR-223-3p, miR-483-5p, and miR-499a-5p were relatively reliable, powerful biomarkers based on multiple normalized researches and had larger sample sizes than other miRNAs. Although the number of subjects of the case group in the studies of miR-19a-3p, miR-23b-3p, miR-181a-5p, etc. was weak, the results of these studies still showed a meaningful clue that these miRNAs might be potential biomarkers but need to be verified by large samples in future studies.
The determination of miRNAs from different biological fluids remains controversial. Hermenegildo et al. (2017) reported that miRNA expressions varied according to the sample types from NSTEMI patients. Mompeón et al. (2020) indicated that samples from serum or plasma could be contaminated by red cells, white blood cells, platelets, and hemolysis and proposed that serum was preferable in circulating miRNA studies than plasma and that platelet-poor plasma would be rather appropriate when the miRNAs were highly expressed in the platelets. However, most of the studies selected plasma for miRNA determination but did not show whether the sample type influenced the levels of the selected miRNAs. Although the trends of the same miRNA results did not differ markedly between plasma and serum, it was still a potential factor for the inconsistency of the levels, peak time, and statistical significance of the same miRNAs. Moreover, the different initial sample collection time points and detection intervals were also major confounders that should not be neglected.
The majority of the included studies used qPCR to detect miRNAs while one study used droplet digital PCR (ddPCR) to detect miRNAs. The methods of qPCR are complex and time-consuming. Thus, a novel technology to reduce processing steps and improve the efficiency of detection needs to be addressed in the future. Besides that, ddPCR can absolutely quantitate nucleic acids with greater reproducibility and less inter- and intra-assay variability compared to qPCR (Hindson et al., 2011, 2013; Robinson et al., 2018). Robinson et al. (2018) indicated that the calculation method of the PCR value might influence the diagnostic accuracy of miRNAs and that ddPCR was superior in both technical proficiency and diagnostic potential compared to qPCR. Also, ddPCR was preferred for accurate and reproducible quantification of miRNAs in cardiovascular biology, which provided a reference for future research.
miR-1-3p, miR-19b-3p, miR-133a/b, miR-208a/b, miR-223-3p, miR-483-5p, and miR-499a-5p are shown to be more valuable than classical biomarkers for early diagnosis of AMI; particularly, miR-1-3p, miR-19b-3p, miR-208a, miR-223-3p, miR-483-5p, and miR-499a-5p appear to have the most potential as biomarkers in patients with AMI within 4 h of the onset of symptoms due to their short time window and optimal sensitivity and specificity. However, the diagnostic value of miRNAs and classical biomarkers in patients with AMI at different periods from the onset of chest pain needs further substantiation using large samples. A novel technology to improve the detection efficiency of miRNAs is also needed.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
BW, YL, and XHao: theme and design of the research. JY, YT, and LM: verification of data. XHan, DW, HL, JY, and TL: statistical analysis. BW and YL: writing of the manuscript. MZ and XW: critical revision of the manuscript for intellectual content and obtaining funding. All authors contributed to the article and approved the submitted version.
This study was supported by the National Natural Science Foundation Project of China (81774127 and 81774058) and the Young Teachers Fund of Beijing University of Chinese medicine (2018-JYBZZ-JS066).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fgene.2021.668324/full#supplementary-material
AMI, acute myocardial infarction; CHD, coronary heart disease; cTn, cardiac troponin; CKMB, creatine kinase MB; hs-cTnT, high-sensitivity cardiac troponin T; AUC, area under the curve; NSTEMI, non-ST segment elevation myocardial infarction; STEMI, ST-segment elevation myocardial infarction.
Agiannitopoulos, K., Pavlopoulou, P., Tsamis, K., Bampali, K., Samara, P., Nasioulas, G., et al. (2018). Expression of miR-208b and miR-499 in Greek patients with acute myocardial infarction. In Vivo 32, 313–318. doi: 10.21873/invivo.11239
Akat, K. M., Moore-McGriff, D., Morozov, P., Brown, M., Gogakos, T., Correa Da Rosa, J., et al. (2014). Comparative RNA-sequencing analysis of myocardial and circulating small RNAs in human heart failure and their utility as biomarkers. Proc. Natl. Acad. Sci. U.S.A. 111, 11151–11156. doi: 10.1073/pnas.1401724111
Baker, J. O., Reinhold, J., Redwood, S., and Marber, M. S. (2011). Troponins: redefining their limits. Heart 97, 447–452. doi: 10.1136/hrt.2010.205617
Białek, S., Górko, D., Zajkowska, A., Kołtowski, Ł., Grabowski, M., Stachurska, A., et al. (2015). Release kinetics of circulating miRNA-208a in the early phase of myocardial infarction. Kardiol. Pol. 73, 613–619. doi: 10.5603/KP.a2015.0067
Chistiakov, D. A., Orekhov, A. N., and Bobryshev, Y. V. (2016). Cardiac-specific miRNA in cardiogenesis, heart function, and cardiac pathology (with focus on myocardial infarction). J. Mol. Cell. Cardiol. 94, 107–121. doi: 10.1016/j.yjmcc.2016.03.015
Cortez-Dias, N., Costa, M. C., Carrilho-Ferreira, P., Silva, D., Jorge, C., Calisto, C., et al. (2016). Circulating miR-122-5p/miR-133b ratio is a specific early prognostic biomarker in acute myocardial infarction. Circ. J. 80, 2183–2191. doi: 10.1253/circj.CJ-16-0568
Coskunpinar, E., Cakmak, H. A., Kalkan, A. K., Tiryakioglu, N. O., Erturk, M., and Ongen, Z. (2016). Circulating miR-221-3p as a novel marker for early prediction of acute myocardial infarction. Gene 591, 90–96. doi: 10.1016/j.gene.2016.06.059
Dai, Y., Yan, T., and Gao, Y. (2020). Silence of miR-32-5p promotes endothelial cell viability by targeting KLF2 and serves as a diagnostic biomarker of acute myocardial infarction. Diagn. Pathol. 15:19. doi: 10.1186/s13000-020-00942-y
D'Alessandra, Y., Devanna, P., Limana, F., Straino, S., Di Carlo, A., Brambilla, P. G., et al. (2010). Circulating microRNAs are new and sensitive biomarkers of myocardial infarction. Eur. Heart J. 31, 2765–2773. doi: 10.1093/eurheartj/ehq167
Devaux, Y., Mueller, M., Haaf, P., Goretti, E., Twerenbold, R., Zangrando, J., et al. (2015). Diagnostic and prognostic value of circulating microRNAs in patients with acute chest pain. J. Intern. Med. 277, 260–271. doi: 10.1111/joim.12183
Devaux, Y., Vausort, M., Goretti, E., Nazarov, P. V., Azuaje, F., Gilson, G., et al. (2012). Use of circulating microRNAs to diagnose acute myocardial infarction. Clin. Chem. 58, 559–567. doi: 10.1373/clinchem.2011.173823
Feng, P. M., Liu, M., Cui, Y. P., Ye, M. M., Zhang, S. T., and Jiang, T. (2008). Comparison of the application value of cardiac troponin I (cTnI), cardiac troponin T (cTnT), and creatine kinase MB (CK-MB) for the diagnosis of acute myocardial infarction (AMI). Chin. Exp. Diagn. 2008, 1256–1258.
Giannitsis, E., and Katus, H. A. (2013). Cardiac troponin level elevations not related to acute coronary syndromes. Nat. Rev. Cardiol. 10, 623–634. doi: 10.1038/nrcardio.2013.129
Gidlöf, O., Smith, J. G., Miyazu, K., Gilje, P., Spencer, A., Blomquist, S., et al. (2013). Circulating cardio-enriched microRNAs are associated with long-term prognosis following myocardial infarction. BMC Cardiovasc. Disord. 13:12. doi: 10.1186/1471-2261-13-12
Guo, M. L., Guo, L. L., and Weng, Y. Q. (2017). Implication of peripheral blood miRNA-124 in predicting acute myocardial infarction. Eur. Rev. Med. Pharmacol. Sci. 21, 1054–1059. doi: 10.1016/j.jacc.2017.07.071
He, F., Lv, P., Zhao, X., Wang, X., Ma, X., Meng, W., et al. (2014). Predictive value of circulating miR-328 and miR-134 for acute myocardial infarction. Mol. Cell. Biochem. 394, 137–144. doi: 10.1007/s11010-014-2089-0
He, Y., Zhong, J., Huang, S., Shui, X., Kong, D., Chen, C., et al. (2017). Elevated circulating miR-126-3p expression in patients with acute myocardial infarction: its diagnostic value. Int. J. Clin. Exp. Pathol. 10, 11051–11056.
Hermenegildo, C., Mompeon, A., Januario, T., Vidal-Gomez, X., Pujol, M., Perez-Cremades, D., et al. (2017). Comparative analysis of miRNA expression in serum and plasma of patients with acute myocardial infarction. J. Hypertens. 35:e204. doi: 10.1097/01.hjh.0000523575.94981.9b
Hindson, B. J., Ness, K. D., Masquelier, D. A., Belgrader, P., Heredia, N. J., Makarewicz, A. J., et al. (2011). High-throughput droplet digital PCR system for absolute quantitation of DNA copy number. Anal. Chem. 83, 8604–8610. doi: 10.1021/ac202028g
Hindson, C. M., Chevillet, Jr., Briggs, H. A., Gallichotte, E. N., Ruf, I. K., Hindson, B. J., et al. (2013). Absolute quantification by droplet digital PCR versus analog real-time PCR. Nat. Methods 10, 1003–1005. doi: 10.1038/nmeth.2633
Ke-Gang, J., Zhi-Wei, L., Xin, Z., Jing, W., Ping, S., Xue-Jing, H., et al. (2016). Evaluating diagnostic and prognostic value of plasma miRNA133a in acute chest pain patients undergoing coronary angiography. Medicine 95:e3412. doi: 10.1097/MD.0000000000003412
Lalem, T., and Devaux, Y. (2019). Circulating microRNAs to predict heart failure after acute myocardial infarction in women. Clin. Biochem. 70, 1–7. doi: 10.1016/j.clinbiochem.2019.05.011
Li, C., Fang, Z., Jiang, T., Zhang, Q., Liu, C., Zhang, C., et al. (2013). Serum microRNAs profile from genome-wide serves as a fingerprint for diagnosis of acute myocardial infarction and angina pectoris. BMC Med. Genomics 6:16. doi: 10.1186/1755-8794-6-16
Li, H., Zhang, P., Li, F., Yuan, G., Wang, X., Zhang, A., et al. (2019). Plasma miR-22-5p, miR-132-5p, and miR-150-3p are associated with acute myocardial infarction. Biomed. Res. Int. 2019:5012648. doi: 10.1155/2019/5012648
Li, L., Li, S., Wu, M., Chi, C., Hu, D., Cui, Y., et al. (2019). Early diagnostic value of circulating microRNAs in patients with suspected acute myocardial infarction. J. Cell. Physiol. 234, 13649–13658. doi: 10.1002/jcp.28045
Li, L. M., Cai, W. B., Ye, Q., Liu, J. M., Li, X., and Liao, X. X. (2014). Comparison of plasma microRNA-1 and cardiac troponin T in early diagnosis of patients with acute myocardial infarction. World J. Emerg. Med. 5, 182–186. doi: 10.5847/wjem.j.issn.1920-8642.2014.03.004
Li, P., Li, S. Y., Liu, M., Ruan, J. W., Wang, Z. D., and Xie, W. C. (2019). Value of the expression of miR-208, miR-494, miR-499 and miR-1303 in early diagnosis of acute myocardial infarction. Life Sci. 232:116547. doi: 10.1016/j.lfs.2019.116547
Li, Y. Q., Zhang, M. F., Wen, H. Y., Hu, C. L., Liu, R., Wei, H. Y., et al. (2013). Comparing the diagnostic values of circulating microRNAs and cardiac troponin T in patients with acute myocardial infarction. Clinics 68, 75–80. doi: 10.6061/clinics/2013(01)OA12
Li, Z., Lu, J., Luo, Y., Li, S., and Chen, M. (2014). High association between human circulating microRNA-497 and acute myocardial infarction. Sci. World J. 2014:931845. doi: 10.1155/2014/931845
Liu, G., Niu, X., Meng, X., and Zhang, Z. (2018). Sensitive miRNA markers for the detection and management of NSTEMI acute myocardial infarction patients. J. Thorac. Dis. 10, 3206–3215. doi: 10.21037/jtd.2018.05.141
Long, G., Wang, F., Duan, Q., Chen, F., Yang, S., Gong, W., et al. (2012a). Human circulating microRNA-1 and microRNA-126 as potential novel indicators for acute myocardial infarction. Int. J. Biol. Sci. 8, 811–818. doi: 10.7150/ijbs.4439
Long, G., Wang, F., Duan, Q., Yang, S., Chen, F., Gong, W., et al. (2012b). Circulating miR-30a, miR-195 and let-7b associated with acute myocardial infarction. PLoS ONE 7:e50926. doi: 10.1371/journal.pone.0050926
Mitchell, P. S., Parkin, R. K., Kroh, E. M., Fritz, B. R., Wyman, S. K., Pogosova-Agadjanyan, E. L., et al. (2008). Circulating microRNAs as stable blood-based markers for cancer detection. Proc. Natl. Acad. Sci. U.S.A. 105, 10513–10518. doi: 10.1073/pnas.0804549105
Moe, K. T., and Wong, P. (2010). Current trends in diagnostic biomarkers of acute coronary syndrome. Ann. Acad. Med. Singap. 39, 210–215.
Mompeón, A., Ortega-Paz, L., Vidal-Gómez, X., Costa, T. J., Pérez-Cremades, D., Garcia-Blas, S., et al. (2020). Disparate miRNA expression in serum and plasma of patients with acute myocardial infarction: a systematic and paired comparative analysis. Sci. Rep. 10:5373. doi: 10.1038/s41598-020-61507-z
Robinson, S., Follo, M., Haenel, D., Mauler, M., Stallmann, D., Tewari, M., et al. (2018). Droplet digital PCR as a novel detection method for quantifying microRNAs in acute myocardial infarction. Int. J. Cardiol. 257, 247–254. doi: 10.1016/j.ijcard.2017.10.111
Rupaimoole, R., and Slack, F. J. (2017). MicroRNA therapeutics: towards a new era for the management of cancer and other diseases. Nat. Rev. Drug Discov. 16, 203–222. doi: 10.1038/nrd.2016.246
Su, J., Li, J., Yu, Q., Wang, J., Li, X., Yang, J., et al. (2020). Exosomal miRNAs as potential biomarkers for acute myocardial infarction. IUBMB Life 72, 384–400. doi: 10.1002/iub.2189
Su, T., Shao, X., Zhang, X., Han, Z., Yang, C., and Li, X. (2019). Circulating microRNA-1 in the diagnosis and predicting prognosis of patients with chest pain: a prospective cohort study. BMC Cardiovasc. Disord. 19:5. doi: 10.1186/s12872-018-0987-x
Su, T., Shao, X., Zhang, X., Yang, C., and Shao, X. (2020). Value of circulating miRNA-1 detected within 3 h after the onset of acute chest pain in the diagnosis and prognosis of acute myocardial infarction. Int. J. Cardiol. 307, 146–151. doi: 10.1016/j.ijcard.2019.09.050
Thygesen, K., Alpert, J. S., Jaffe, A. S., Chaitman, B. R., Bax, J. J., Morrow, D. A., et al. (2018). Fourth universal definition of myocardial infarction. J. Am. Coll. Cardiol. 72, 2231–2264. doi: 10.1016/j.jacc.2018.08.1038
Vengatapathy, K. V., Ramesh, R., Rajappa, M., Kulkarni, S., and Hanifa, M. (2019). Role of serum microRNA-499 as a diagnostic marker in acute myocardial infarction. Cor. Vasa. 61, 272–276. doi: 10.1016/j.crvasa.2018.03.008
Wang, F., Long, G., Zhao, C., Li, H., Chaugai, S., Wang, Y., et al. (2013). Plasma microRNA-133a is a new marker for both acute myocardial infarction and underlying coronary artery stenosis. J. Transl. Med. 11:222. doi: 10.1186/1479-5876-11-222
Wang, F., Long, G., Zhao, C., Li, H., Chaugai, S., Wang, Y., et al. (2014). Atherosclerosis-related circulating miRNAs as novel and sensitive predictors for acute myocardial infarction. PLoS ONE 9:e105734. doi: 10.1371/journal.pone.0105734
Wang, G. K., Zhu, J. Q., Zhang, J. T., Li, Q., Li, Y., He, J., et al. (2010). Circulating microRNA: a novel potential biomarker for early diagnosis of acute myocardial infarction in humans. Eur. Heart J. 31, 659–666. doi: 10.1093/eurheartj/ehq013
Wang, K. J., Zhao, X., Liu, Y. Z., Zeng, Q. T., Mao, X. B., Li, S. N., et al. (2016). Circulating MiR-19b-3p, MiR-134-5p and MiR-186-5p are promising novel biomarkers for early diagnosis of acute myocardial infarction. Cell Physiol. Biochem. 38, 1015–1029. doi: 10.1159/000443053
Wexler, Y., and Nussinovitch, U. (2020). The diagnostic value of Mir-133a in ST elevation and non-ST elevation myocardial infarction: a meta-analysis. Cells 9:793. doi: 10.3390/cells9040793
White, H. D., and Chew, D. P. (2008). Acute myocardial infarction. Lancet 372, 570–584. doi: 10.1016/S0140-6736(08)61237-4
Yao, X. L., Lu, X. L., Yan, C. Y., Wan, Q. L., Cheng, G. C., and Li, Y. M. (2015). Circulating miR-122-5p as a potential novel biomarker for diagnosis of acute myocardial infarction. Int. J. Clin. Exp. Pathol. 8, 16014–16019.
Yuan, L., Liu, X., Chen, F., Zhang, L., Chen, X., Huang, Q., et al. (2016). Diagnostic and prognostic value of circulating MicroRNA-133a in patients with acute myocardial infarction. Clin. Lab. 62, 1233–1241. doi: 10.7754/Clin.Lab.2015.151023
Yue, M. X., Tong, M. Q., Li, D. F., Geng, B., Hu, W. B., and Li, J. (2018). Expert consensus on the application of combined detection of myeloperoxidase, cardiac fatty acid binding protein and cardiac troponin I in acute coronary syndrome. Chin. J. Health Emerg. 4, 223–235.
Zhang, J., Li, Y., and Zhao, Q. (2018). Circulating miR-23b as a novel biomarker for early risk stratification after ST-elevation myocardial infarction. Med. Sci. Monit. 24, 1517–1523. doi: 10.12659/MSM.908060
Zhang, L., Chen, X., Su, T., Li, H., Huang, Q., Wu, D., et al. (2015). Circulating miR-499 are novel and sensitive biomarker of acute myocardial infarction. J. Thorac. Dis. 7, 303–308. doi: 10.1016/j.jacc.2015.06.318
Zhang, S. Y., Xie, J. Y., Liang, H. W., Chen, X., and Zhang, C. Y. (2013). The origin, function and diagnostic potential of extracellular microRNA in human body fluids. Prog. Biochem. Biophys. 40, 603–616. doi: 10.3724/SP.J.1206.2013.00260
Zhang, Y., Cheng, J., Chen, F., Wu, C., Zhang, J., Ren, X., et al. (2017). Circulating endothelial microparticles and miR-92a in acute myocardial infarction. Biosci Rep. 37:BSR20170047. doi: 10.1042/BSR20170047
Zhang, Y., Liu, Y. J., Liu, T., Zhang, H., and Yang, S. J. (2016). Plasma microRNA-21 is a potential diagnostic biomarker of acute myocardial infarction. Eur. Rev. Med. Pharmacol. Sci. 20, 323–329.
Zhao, C. H., Cheng, G. C., He, R. L., Hong, Y., Wan, Q. L., Wang, Z. Z., et al. (2015). Analysis and clinical significance of microRNA-499 expression levels in serum of patients with acute myocardial infarction. Genet. Mol. Res. 14, 4027–4034. doi: 10.4238/2015.April.27.17
Zhao, J., Yu, H., Yan, P., Zhou, X., Wang, Y., and Yao, Y. (2019). Circulating MicroRNA-499 as a diagnostic biomarker for acute myocardial infarction: a meta-analysis. Dis. Markers. 2019:6121696. doi: 10.1155/2019/6121696
Zhong, J., He, Y., Chen, W., Shui, X., Chen, C., and Lei, W. (2014). Circulating microRNA-19a as a potential novel biomarker for diagnosis of acute myocardial infarction. Int. J. Mol. Sci. 15, 20355–20364. doi: 10.3390/ijms151120355
Keywords: miRNAs, conventional biomarkers, acute myocardial infarction, peak time, AUC
Citation: Wang B, Li Y, Hao X, Yang J, Han X, Li H, Li T, Wang D, Teng Y, Ma L, Li Y, Zhao M and Wang X (2021) Comparison of the Clinical Value of miRNAs and Conventional Biomarkers in AMI: A Systematic Review. Front. Genet. 12:668324. doi: 10.3389/fgene.2021.668324
Received: 17 February 2021; Accepted: 04 May 2021;
Published: 17 June 2021.
Edited by:
Peter Igaz, Semmelweis University, HungaryReviewed by:
Emanuela Bostjancic, University of Ljubljana, SloveniaCopyright © 2021 Wang, Li, Hao, Yang, Han, Li, Li, Wang, Teng, Ma, Li, Zhao and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mingjing Zhao, bWpneDIwMDRAMTYzLmNvbQ==; Xian Wang, d3g2NTA1MTVAMTYzLmNvbQ==
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.