 Chang Chen1†
Chang Chen1† Hui Jin
Hui Jin
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Genet. , 22 April 2021
Sec. Cancer Genetics
Volume 12 - 2021 | https://doi.org/10.3389/fgene.2021.666371
This article is part of the Research Topic RNA Modification in Human Cancers: Roles and Therapeutic Implications View all 48 articles
Tobacco smoking is an established risk factor for squamous cell carcinoma (SCC). We obtained smoking-related SCC, including cervical SCC (CSCC), esophageal SCC (ESCC), head and neck SCC (HNSC), and lung SCC (LUSC), from The Cancer Genome Atlas (TCGA) database to investigate the association between smoking status (reformed and current smoking) and prognosis. We found that reformed smokers had a better prognosis than current smokers in CSCC (p = 0.003), HNSC (p = 0.019), and LUSC (p < 0.01) cohorts. Then, we selected LUSC cohorts as the training cohort and other SCC cohorts as the test cohorts. Function analysis revealed that homologous recombination (HR) was the most significant pathway involved in smoking-induced LUSC. Moreover, the effect of cross-talk between the smoking status and HR deficiency (HRD) on the prognosis was further evaluated, revealing that quitting smoking with high HRD scores could significantly improve patients’ prognosis (p < 0.01). To improve prognosis prediction and more effectively screen suitable populations for platinum drugs and poly-ADP-ribose polymerase (PARP) inhibitors, we constructed a risk score model using smoking- and HRD-related genes in LUSC. The risk score model had high power for predicting 2-, 3-, and 5-year survival (p < 0.01, AUC = 0.67, 0.66, and 0.66). In addition, the risk scores were an independent risk factor for LUSC (HR = 2.34, 95%CI = 1.70–3.23). The practical nomogram was also built using the risk score, smoking status, and other clinical information with a good c-index (0.72, 95%CI = 0.70–0.74). Finally, we used other TCGA SCC cohorts to confirm the reliability and validity of the risk score model (p < 0.01 and AUC > 0.6 at 2, 3, and 5 years in CSCC and HNSC cohorts). In conclusion, the present study suggested that smoking cessation should be a part of smoking-related SCC treatment, and also provided a risk score model to predict prognosis and improve the effectiveness of screening the platinum/PARP population.
Squamous cell carcinomas (SCCs) originate from the epithelial tissues of the aerodigestive or genitourinary tracts. They often occur in the head and neck SCC (HNSC), esophageal SCC (ESCC), lung SCC (LUSC), and cervical SCC (CSCC), sharing common histological features and some risk factors. Among risk factors, tobacco smoking is an established risk factor for SCC, which can alter biological carcinogenesis pathways to promote cancer progression (Schuller, 2019; Sabbula and Anjum, 2020). Cigarette smoke contains many carcinogens that can cause genomic alteration and break immunologic homeostasis (Li et al., 2018). Many studies have reported that smoking cessation can eliminate the physiological driving force of cancer development and improve the prognosis of SCC patients (Dobson Amato et al., 2015; Yavorski and Blanck, 2016; Yang et al., 2020). However, the underlying mechanism of smoking-induced SCC remains unclear in smoking-related SCC.
Homologous recombination repair (HRR) is an important repair method for DNA double strand damage (Mackenroth and Alani, 2020). Cancer cells with homologous recombination deficiency (HRD) are sensitive to platinum drugs and poly-ADP-ribose polymerase (PARP) inhibitors. At present, BRCA1/2 mutation is the most comprehensive HRD biomarker (Hoppe et al., 2018). However, Turner and Ashworth proposed the concept of “BRCAness” to describe HRD without BRCA mutation but with a phenotype similar to BRCA mutation (Turner et al., 2004; Lord and Ashworth, 2016). Therefore, better biomarkers should be identified to screen a more effective platinum/PARP population. HRD scores, which are comprehensively calculated based on loss of heterozygosis (LOH), telomeric-allelic imbalance (TAI), and large-scale state transitions (LST), are considered as biomarkers of genomic instability with mutation (Takaya et al., 2020), which were applied in drug efficacy and tumor susceptibility evaluation (do Canto et al., 2019; Min et al., 2020).
In the present, we not only estimated the association between smoking cessation and smoking-related SCC prognosis but also investigated its potential mechanism. Importantly, we constructed a risk score model combining smoking and HRD, which could effectively screen suitable populations and improve prognostic prediction, especially for smoking-related SCC.
The data we used were from the public database. Level 3 data of gene expression profiles of LUSC, CSCC, ESCC, and HNSC patients were taken from the GDC Data Portal1. Clinical information, including age, gender, stage, tumor status, and survival outcome, were downloaded. The smoking exposure information of each patient was also obtained from The Cancer Genome Atlas (TCGA) database. The HRD scores were obtained from the TCGA Pan-Cancer dataset2. All data were extracted from TCGA, an open database, and followed the guidelines. Therefore, there was no requirement for ethics approval.
Smoking-related genes or HRD-related genes were obtained using the “limma” package in R software. Then, the Kyoto Encyclopedia of Genes and Genomes (KEGG) pathway and Gene Ontology (GO) analysis were performed using the “clusterProfiler” package in R.
Univariable Cox regression analysis was first used to identify survival genes. Then, multivariate Cox regression analysis was again employed to select candidates for building the risk score model. The corresponding coefficients from multivariate Cox analysis were used to calculate risk scores: .
Based on the risk scores, the patients were divided into the high-score group and low-score group. To estimate the prognostic ability of the risk score model, Kaplan-Meier (K-M) survival analysis and survival receiver operating characteristic (survival-ROC) curves were, respectively, applied.
Univariable and multivariable cox analyses were performed to evaluate the association between risk scores and prognosis. Then, a prognostic nomogram was applied as a quantitative tool to accurately predict each patient’s prognosis using risk scores and clinical information. Calibration curves were also plotted to evaluate the accuracy of the nomogram.
We calculated the risk score in CSCC, ESCC, and HNSC cohorts from the TCGA database based on the same formula. Then, K-M curves and survival-ROC curves were used to estimate the prognostic power and confirm the applicability and reliability of the risk score model in SCC cohorts.
In addition to the TCGA database, we also used other independent SCC cohorts from the GEO database to verify the risk score model, including the CSCC cohort (GSE44001), ESCC cohort (GSE53625), HNSC cohort (GSE65858), and LUSC cohort (GSE73403). We calculated the risk score of each patient using the same formula. Then, K-M curves and survival-ROC curves were also performed to confirm the prognostic power.
All data were expressed as mean ± SD (standard deviation). The K-M curves, univariable and multivariable cox analysis were performed using the “survival” package. Survival-ROC curves were applied with “timeROC” the package. The optimal cut-off values of risk scores were evaluated using the “survminer” package. The nomogram and calibration curves were plotted using the “rms” package. The analyses described above were conducted in R software 3.5 and Microsoft Excel 2016.
We selected smoking-related SCC patients for further study. A total of 95 CSCC patients (53 current smokers and 42 reformed smokers), 50 ESCC patients (26 current smokers and 24 reformed smokers), 393 HNSC patients (178 current smokers and 215 reformed smokers), and 471 LUSC patients (133 current smokers and 338 reformed smokers) were included in the study. As shown in Figure 1, patients who quit smoking had a longer survival time than those who kept smoking in CSCC (p = 0.003), HNSC (p = 0.019), and LUSC (p < 0.001). Among them, the number of LUSC patients was the largest and the results of survival analysis were the most significant. Therefore, we selected LUSC patients as the training cohort and other SCC cohorts as test cohorts for further study.
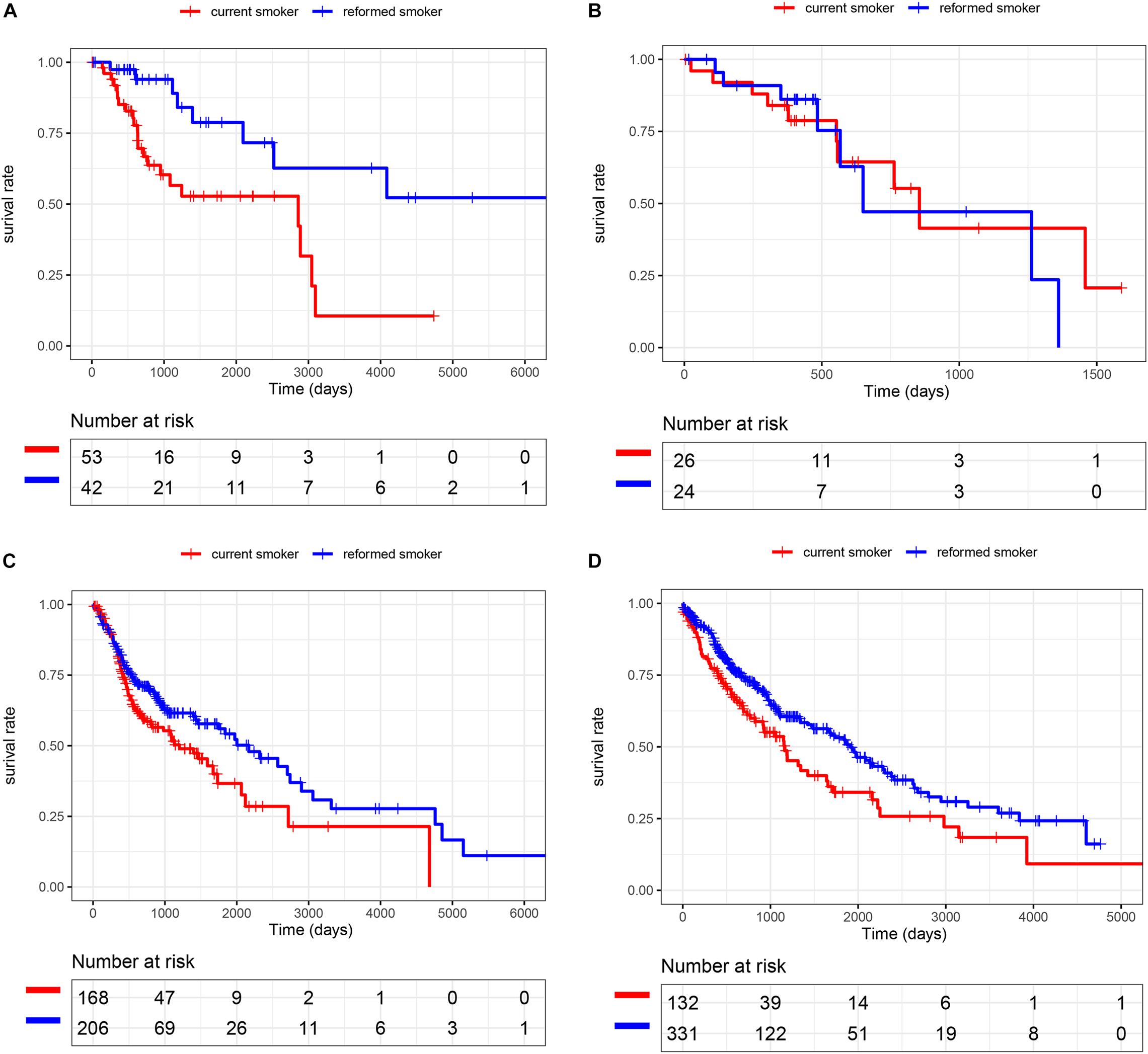
Figure 1. Smoking cessation could improve prognosis in SCC. (A) CSCC. (B) ESCC. (C) HNSC. (D) LUSC.
To understand the potential mechanism of the benefits of smoking cessation, we obtained smoking-related genes between current smokers and reformed smokers in LUSC patients (Figure 2A). Then, function analysis was performed. KEGG analysis found that homologous recombination (HR) was the most significant pathway in smoking-related LUSC (Figure 3A). GO analysis also found that HR-related GO terms, including double-strand break repair via HR, HR, regulation of double-strand break repair via HR, and negative regulation of double-strand break repair via HR, were significantly enriched (Figure 3B and Supplementary Table 1). Moreover, LUSC patients with higher HRD scores had better survival outcomes than those with lower HRD scores (Figure 3C, p = 0.043). We further investigated the effect of cross-talk between the smoking status and HR on the prognosis. LUSC patients were stratified in the combination of the smoking status and HRD scores, including current smoking and high HRD scores, current smoking and low HRD scores, reformed smoking and high HRD scores, and reformed smoking and low HRD scores. The survival analysis revealed that quitting smoking with high HRD scores could significantly improve LUSC patients’ prognosis (P < 0.01, Figure 3D).
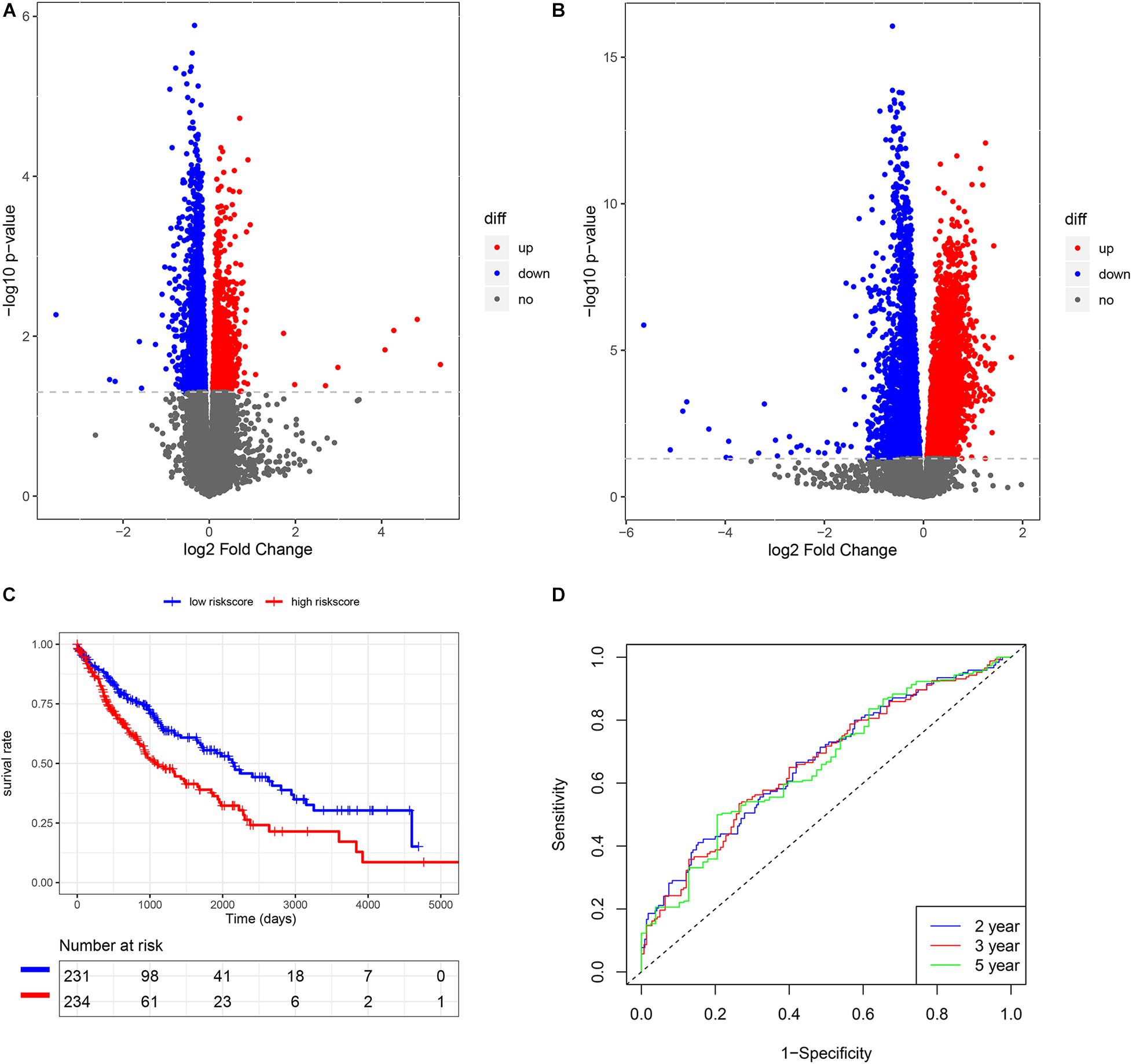
Figure 2. The construction of risk score model in LUSC. (A) The volcano plot of smoking-related genes. (B) The volcano plot of HRD-related genes. (C) K-M analysis of risk score model. (D) Survival ROC of risk score model.
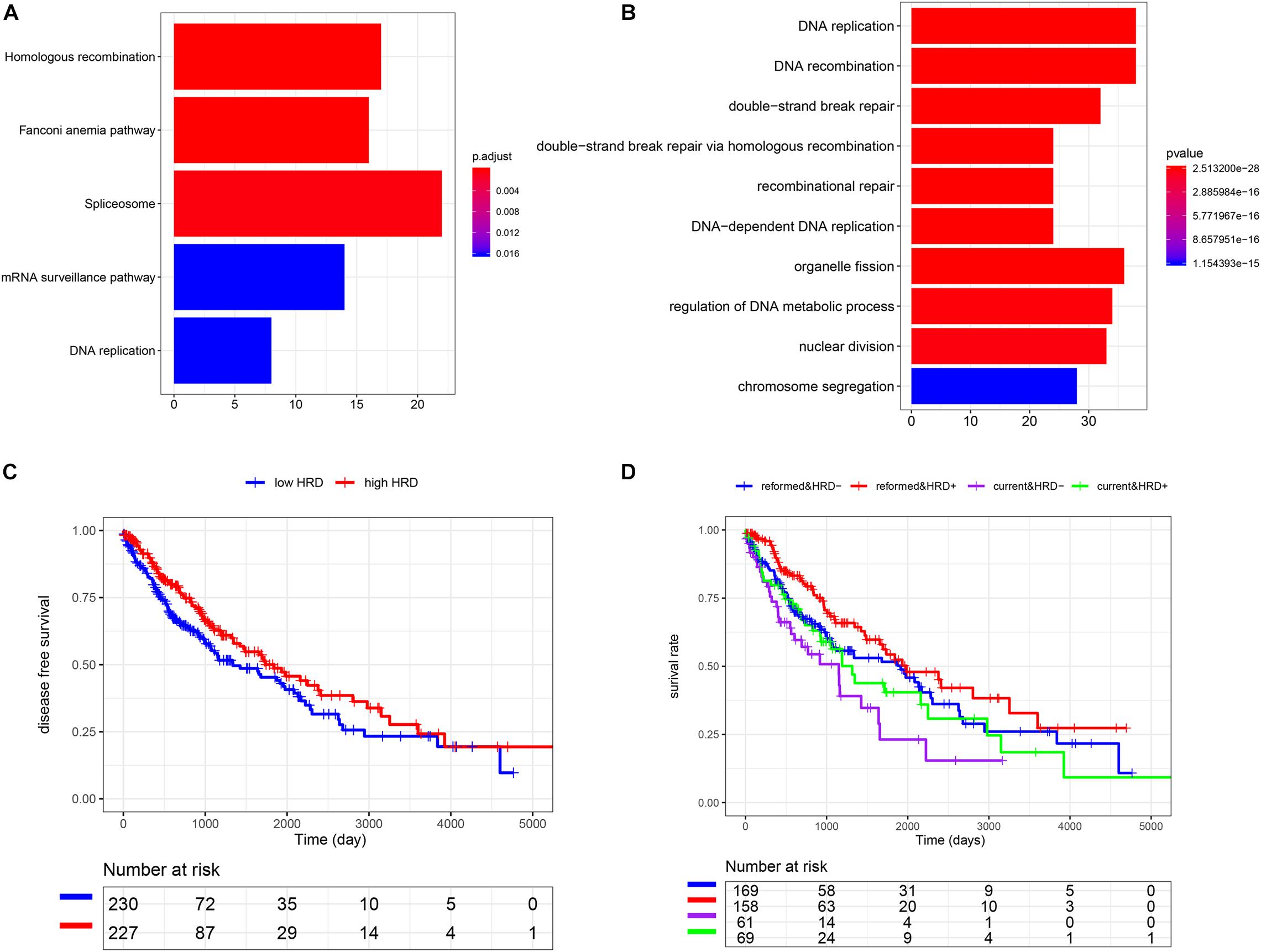
Figure 3. The association among smoking cessation, HRD, and prognosis in LUSC. (A) The KEGG analysis. (B) The GO analysis. (C) K-M analysis of high and low HRD scores. (D) The effect of cross-talk between the smoking status and homologous recombination on the prognosis.
We also subsequently identified the HRD-related genes between high- and low-HRD score patients (Figure 2B). There were 1218 same genes after taking an intersection for smoking-genes and HRD-genes (Supplementary Figure 1). Afterward, based on the univariate and multivariate Cox regression analysis (Supplementary Tables 2, 3), five eligible genes, including MAFK, LMBRD1, MESDC1, KLHL15, and E2F4, were selected to build a risk score model. Then, we divided the patients into high-risk and low-risk score groups and found that patients with high-risk scores had a worse outcome than those with low-risk scores (p < 0.01, Figure 2C). The survival ROC also indicated that the risk score model had good predicting power at 2, 3, and 5 years (AUC = 0.67, 0.67, and 0.66, Figure 2D).
In univariate Cox regression analysis, one risk score could increase the risk of death by 2.72 times (95% CI = 1.99–3.73, Figure 4A) for LUSC patients. A similar, significant increase in death risk was also observed by multivariate Cox analysis (hazard rate, HR = 2.34, 95%CI = 1.70–3.23, Figure 4B), indicating that the risk score model could serve as an independent prognostic indicator. We also provided a prognostic nomogram to predict each patient’s survival of 2, 3, and 5 years, whose calibration curve also suggested its good prediction (c-index = 0.72, 95%CI = 0.71–0.74) (Figures 4C,D).
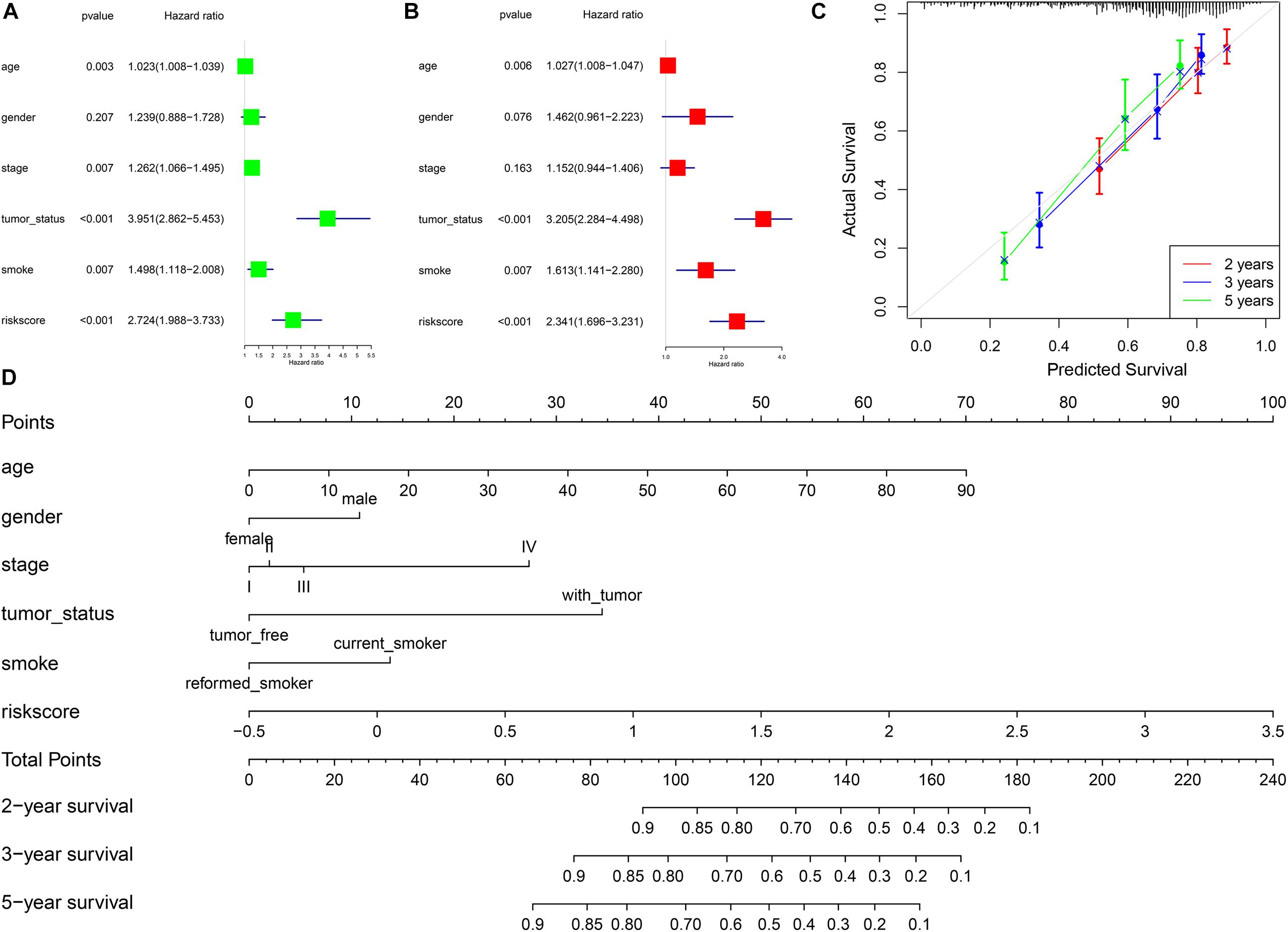
Figure 4. The association between risk scores and prognosis of LUSC. (A) Univariate Cox regression analysis. (B) Multivariate Cox regression analysis. (C) Calibration curve of nomogram. (D) Construction of nomogram.
We also analyzed the expression level of these five genes in other SCC cohorts and found that most of them were also related to smoking cessation (Supplementary Table 4). Importantly, we estimated the prognostic value of the risk score model in SCC cohorts. K-M and survival-ROC analysis showed that high-score patients had higher hazard rates than low-score patients in CSCC (p < 0.01, AUC = 0.60, 0.62, and 0.73 at 2, 3, and 5 years, Figures 5A,B), in HNSC (p < 0.01, AUC = 0.62, 0.60, and 0.61 at 2, 3, and 5 years, Figures 5E,F). There was no statistical significance in ESCC patients, but low-score patients tended to live longer than high-score patients (p = 0.12, AUC = 0.63 and 0.61 at 2 and 3 years, Figures 5C,D).
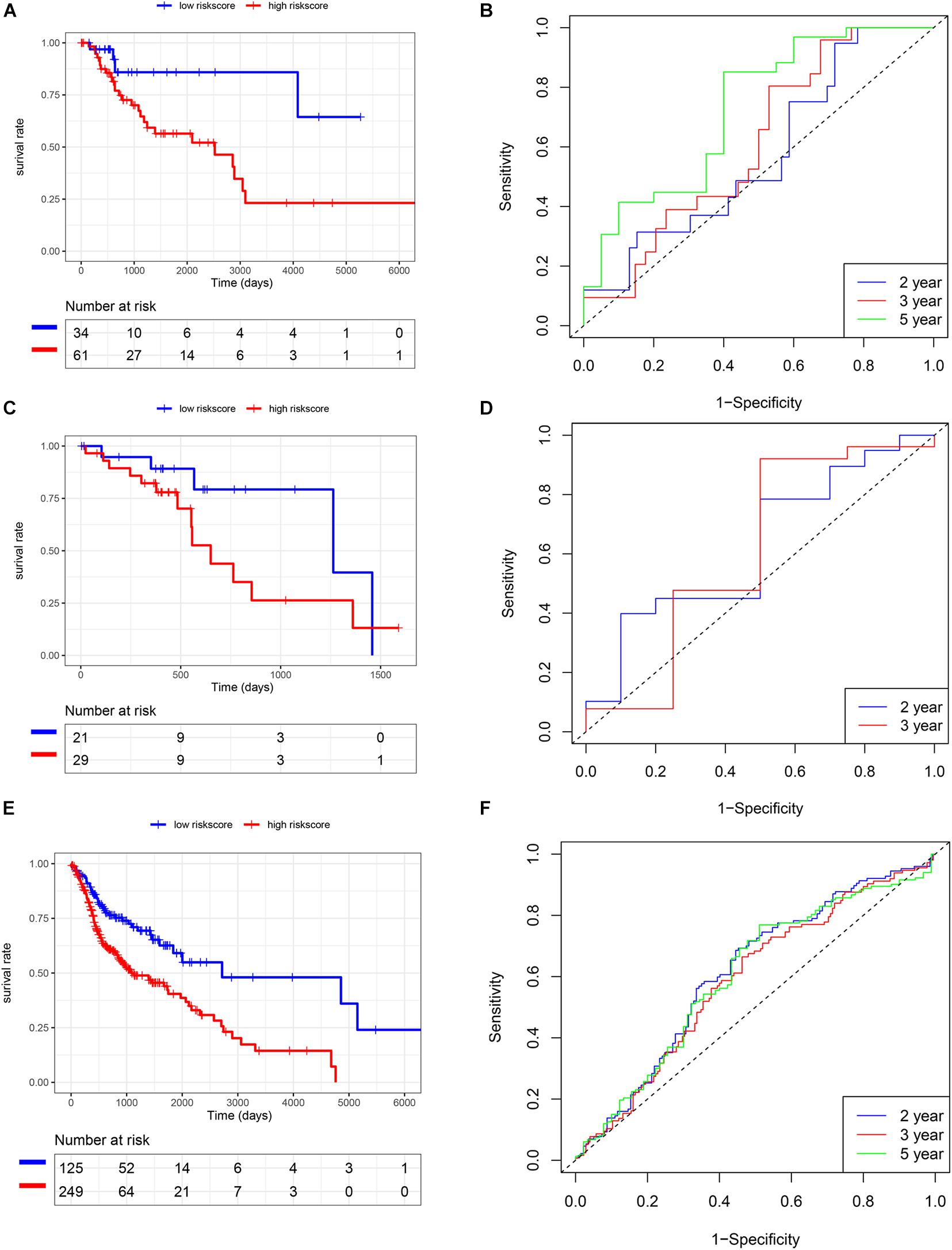
Figure 5. Validation of the risk score model in TCGA SCC cohorts. (A,B) CSCC. (C,D) ESCC. (E,F) HNSC.
In addition to the TCGA database, we also use other independent SCC cohorts from the GEO database to verify the risk score model. K-M and survival-ROC analysis showed that high-score patients had higher hazard rates than low-score patients in CSCC (p = 0.01, AUC = 0.62, 0.58, and 0.52 at 2, 3, and 5 years, Figures 6A,B), in HNSC (p = 0.03, AUC = 0.52, 0.53, and 0.58 at 2, 3, and 5 years, Figures 6E,F), and in LUSC (p = 0.02, AUC = 0.61, 0.56, and 0.57 at 2, 3, and 5 years, Figures 6G,H). However, there was no statistical significance in ESCC patients (p = 0.86, AUC = 0.59, 0.54, and 0.59 at 2, 3, and 5 years, Figures 6C,D).
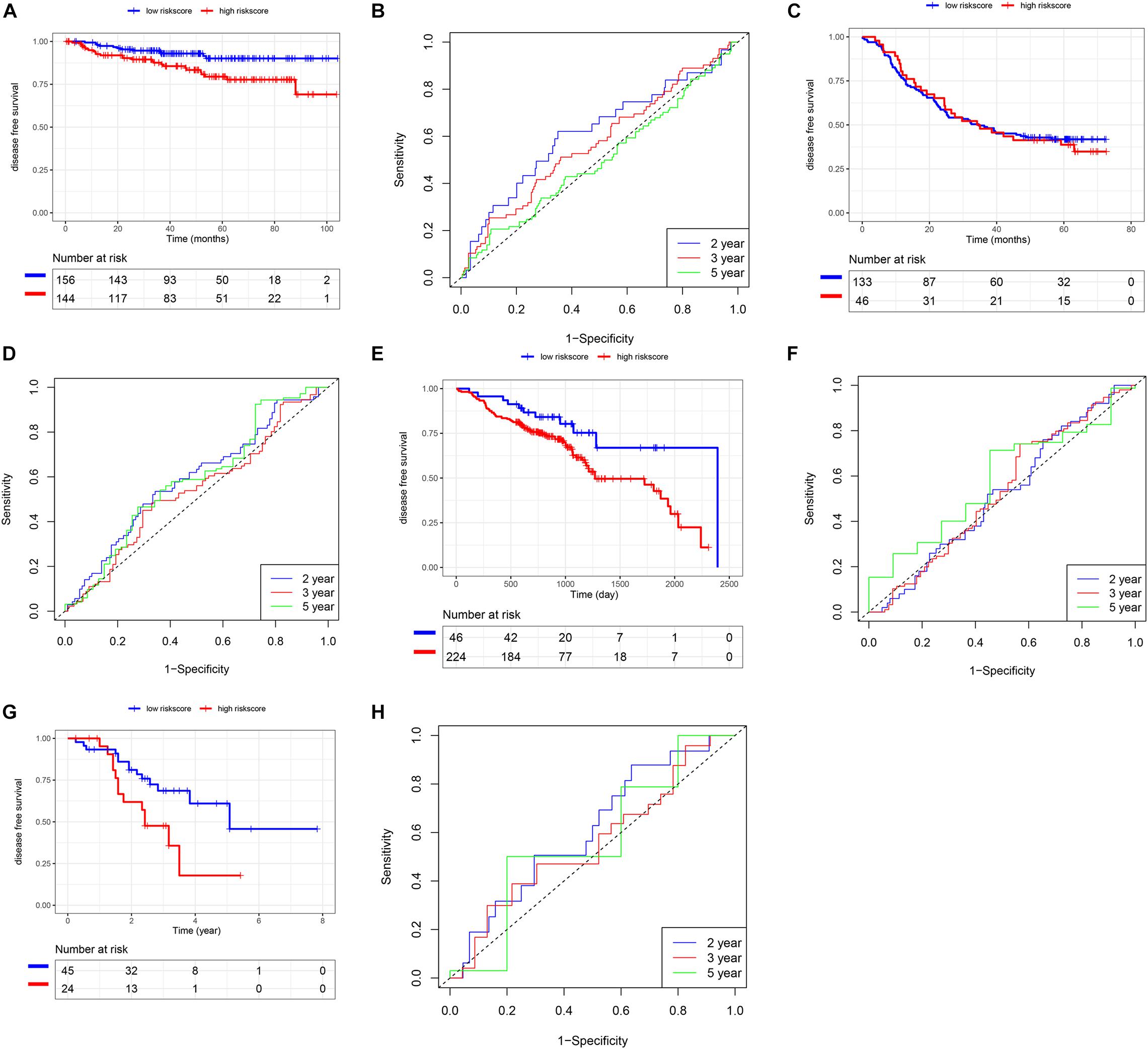
Figure 6. Validation of the risk score model using SCC cohorts from the GEO database. (A,B) CSCC. (C,D) ESCC. (E,F) HNSC. (G,H) LUSC.
Tobacco smoking has been confirmed to be a critical risk factor for SCC development, and smoking cessation can increase overall survival after diagnosis (Dobson Amato et al., 2015; Yavorski and Blanck, 2016). To further understand the benefits of quitting smoking for patients’ prognosis, we selected smoking-related SCC patients from the TCGA database.
By plotting K-M curves, we found that current smokers had a worse prognosis than reformed smokers in most SCC cohorts, which was consistent with other studies (Li et al., 2020; Yang et al., 2020). Then, we found smoking-related genes and performed function analysis in LUSC, pointing out that HR was an important pathway of smoking to aggravate cancer. It is known that DNA double-strand breaks induced by cigarette smoke can be repaired mainly through HR repair (Helleday, 2003; Albino et al., 2004). Many genes involved in HR repair are significantly associated with smoking to influence the risk of lung cancer (Ryk et al., 2006; Nogueira et al., 2010). Hammouz et al. (2020) also constructed a gene co-expression network and found that smoking significantly affected HR to induce lung adenocarcinoma. In addition, many scholars have used HRD scores in cancer studies. Takaya et al. (2020) analyzed the association between HRD score and high-grade serous ovarian carcinoma and suggested that patients could be classified into different prognostic subtypes for personalized treatment. Kraya et al. (2019) investigated the molecular features of BRCA1/2 alterations in breast cancer patients and found that HRD scores and hormone receptor subtypes could predict the immunogenicity of BRCA1/2 breast cancer, and provided the basis for formulating the best immunotherapy strategy. In the present study, we also found that high HRD scores could increase survival time, suggesting that the cross-talk between smoking cessation and high HRD scores might help treatment and improve overall survival.
After the univariate and multivariate Cox regression analysis, the risk score model was established using five smoking- and HRD-related genes in the LUSC cohort, including LMBRD1, MAFK, MESDC1, KLHL15, and E2F4. LMBR1 domain containing 1 (LMBRD1) encodes a lysosomal membrane protein that may be involved in the transport and metabolism of cobalamin. Mutations of LMBRD1 are also associated with vitamin B12 metabolism disorder (Fettelschoss et al., 2017). MAF bZIP transcription factor K (MAFK), an important transcription factor of the MAF family, is associated with epithelial–mesenchymal transition and malignant progression in different cancers (Wang et al., 2015; Okita et al., 2017). Mesoderm development candidate 1 (MESDC1), also known as TLNRD1, is confirmed as an oncogenic function in bladder cancer and hepatocellular carcinoma (Tatarano et al., 2012; Wu et al., 2017). The kelch-like family member 15 (KLHL15) can encode a member of the kelch-like family of proteins and is involved in protein ubiquitination and cytoskeletal organization (Ferretti et al., 2016; Zhou et al., 2019), but few studies focus on cancers. E2F transcription factor 4 (E2F4), a member of the E2F family of transcription factors, plays an important role in inhibiting proliferation-associated genes, and its gene mutation and increased expression are related to different cancers (Gong et al., 2020; Zhuang et al., 2020). In the future, these genes should be deeply investigated roles in SCC. Afterward, we performed K-M and survival-ROC analysis to estimate the predictive value of the risk score model, suggesting that the model was a predictor with good sensitivity and specificity in LUSC patients.
To better predict the prognosis of each patient, we constructed a nomogram integrating risk scores, smoking status, and clinical information. As a practical tool to improve predictive accuracy, these methods have been applied in many studies on different cancers (Sun et al., 2020; Yang et al., 2020). The nomogram with different aspects of markers, including risk scores, smoking status, age, gender, and tumor stage, had high clinical application value, which might be a promising way to change clinical management (Birkhahn et al., 2007).
Lastly, we validated the risk score model in other SCC cohorts from TCGA and GEO databases, indicating that the application of risk scores could be extrapolated to CSCC and HNSC patients.
The present study is of great significance in theory and application. First, we demonstrated that keeping smoking after diagnosis could increase the risk of SCC death, suggesting that smoking cessation should be a part of cancer treatment. Second, the risk score model was constructed using smoking- and HRD-related genes, which could make up for the deficiency of HRD based on BRCA (Turner et al., 2004; Lord and Ashworth, 2016), more effective in screening the population suitable for targeted therapy. In the future, we should further verify the application of the risk score model in different SCC cohorts, especially in Asian or Chinese populations.
The present study provided comprehensive insights into the association among smoking status, HRD, and prognosis in SCC. Moreover, a risk score model integrating smoking and HRD was constructed to serve as the potential predictive biomarker and add effectiveness in screening the suitable population for targeted therapy.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
CC, XC, and SL conceived and designed the study, performed the bioinformatic analysis, and wrote the manuscript. HC, MC, LB, and HJ contributed to the revision of the manuscript draft. All authors read and approved the final manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fgene.2021.666371/full#supplementary-material
Albino, A. P., Huang, X., Jorgensen, E., Yang, J., Gietl, D., Traganos, F., et al. (2004). Induction of H2AX phosphorylation in pulmonary cells by tobacco smoke: a new assay for carcinogens. Cell Cycle 3, 1062–1068.
Birkhahn, M., Mitra, A. P., and Cote, R. J. (2007). Molecular markers for bladder cancer: the road to a multimarker approach. Expert Rev. Anticancer Ther. 7, 1717–1727. doi: 10.1586/14737140.7.12.1717
do Canto, L. M., Larsen, S. J., Catin Kupper, B. E., Begnami, M., Scapulatempo-Neto, C., Petersen, A. H., et al. (2019). Increased levels of genomic instability and mutations in homologous recombination genes in locally advanced rectal carcinomas. Front. Oncol. 9:395. doi: 10.3389/fonc.2019.00395
Dobson Amato, K. A., Hyland, A., Reed, R., Mahoney, M. C., Marshall, J., Giovino, G., et al. (2015). Tobacco cessation may improve lung cancer patient survival. J. Thorac. Oncol. 10, 1014–1019. doi: 10.1097/JTO.0000000000000578
Ferretti, L. P., Himmels, S. F., Trenner, A., Walker, C., von Aesch, C., Eggenschwiler, A., et al. (2016). Cullin3-KLHL15 ubiquitin ligase mediates CtIP protein turnover to fine-tune DNA-end resection. Nat. Commun. 7:12628. doi: 10.1038/ncomms12628
Fettelschoss, V., Burda, P., Sagne, C., Coelho, D., De Laet, C., Lutz, S., et al. (2017). Clinical or ATPase domain mutations in ABCD4 disrupt the interaction between the vitamin B12-trafficking proteins ABCD4 and LMBD1. J. Biol. Chem. 292, 11980–11991. doi: 10.1074/jbc.M117.784819
Gong, J., Fan, H., Deng, J., and Zhang, Q. (2020). LncRNA HAND2-AS1 represses cervical cancer progression by interaction with transcription factor E2F4 at the promoter of C16orf74. J. Cell. Mol. Med. 24, 6015–6027. doi: 10.1111/jcmm.15117
Hammouz, R. Y., Kostanek, J. K., Dudzisz, A., Witas, P., Orzechowska, M., and Bednarek, A. K. (2020). Differential expression of lung adenocarcinoma transcriptome with signature of tobacco exposure. J. Appl. Genet. 61, 421–437. doi: 10.1007/s13353-020-00569-1
Helleday, T. (2003). Pathways for mitotic homologous recombination in mammalian cells. Mutat. Res. 532, 103–115. doi: 10.1016/j.mrfmmm.2003.08.013
Hoppe, M. M., Sundar, R., Tan, D. S. P., and Jeyasekharan, A. D. (2018). Biomarkers for homologous recombination deficiency in cancer. J. Natl. Cancer Inst. 110, 704–713. doi: 10.1093/jnci/djy085
Kraya, A. A., Maxwell, K. N., Wubbenhorst, B., Wenz, B. M., Pluta, J., Rech, A. J., et al. (2019). Genomic signatures predict the immunogenicity of BRCA-deficient breast cancer. Clin. Cancer Res. 25, 4363–4374. doi: 10.1158/1078-0432.CCR-18-0468
Li, J., Li, H., Zhang, C., Zhang, C., and Wang, H. (2020). Integrative analysis of genomic alteration, immune cells infiltration and prognosis of lung squamous cell carcinoma (LUSC) to identify smoking-related biomarkers. Int. Immunopharmacol. 89(Pt A):107053. doi: 10.1016/j.intimp.2020.107053
Li, X., Li, J., Wu, P., Zhou, L., Lu, B., Ying, K., et al. (2018). Smoker and non-smoker lung adenocarcinoma is characterized by distinct tumor immune microenvironments. Oncoimmunology 7:e1494677. doi: 10.1080/2162402X.2018.1494677
Lord, C. J., and Ashworth, A. (2016). BRCAness revisited. Nat. Rev. Cancer 16, 110–120. doi: 10.1038/nrc.2015.21
Mackenroth, B., and Alani, E. (2020). Collaborations between chromatin and nuclear architecture to optimize DNA repair fidelity. DNA Repair 97:103018. doi: 10.1016/j.dnarep.2020.103018
Min, A., Kim, K., Jeong, K., Choi, S., Kim, S., Suh, K. J., et al. (2020). Homologous repair deficiency score for identifying breast cancers with defective DNA damage response. Sci. Rep. 10:12506. doi: 10.1038/s41598-020-68176-y
Nogueira, A., Catarino, R., Coelho, A., Araujo, A., Gomes, M., and Medeiros, R. (2010). Influence of DNA repair RAD51 gene variants in overall survival of non-small cell lung cancer patients treated with first line chemotherapy. Cancer Chemother. Pharmacol. 66, 501–506. doi: 10.1007/s00280-009-1187-2
Okita, Y., Kimura, M., Xie, R., Chen, C., Shen, L. T., Kojima, Y., et al. (2017). The transcription factor MAFK induces EMT and malignant progression of triple-negative breast cancer cells through its target GPNMB. Sci. Signal. 10:eaak9397. doi: 10.1126/scisignal.aak9397
Ryk, C., Kumar, R., Thirumaran, R. K., and Hou, S. M. (2006). Polymorphisms in the DNA repair genes XRCC1, APEX1, XRCC3 and NBS1, and the risk for lung cancer in never- and ever-smokers. Lung Cancer 54, 285–292. doi: 10.1016/j.lungcan.2006.08.004
Schuller, H. M. (2019). The impact of smoking and the influence of other factors on lung cancer. Expert Rev. Respir. Med. 13, 761–769. doi: 10.1080/17476348.2019.1645010
Sun, L., Guan, A., Jin, Y., Liu, M., Xiao, Y., Xu, H., et al. (2020). Comparison of prognostic value of red cell-related parameters of biliary tract cancer after surgical resection and integration of a prognostic nomogram: a retrospective study. Adv. Ther. 38, 1227–1244. doi: 10.1007/s12325-020-01595-5
Takaya, H., Nakai, H., Takamatsu, S., Mandai, M., and Matsumura, N. (2020). Homologous recombination deficiency status-based classification of high-grade serous ovarian carcinoma. Sci. Rep. 10:2757. doi: 10.1038/s41598-020-59671-3
Tatarano, S., Chiyomaru, T., Kawakami, K., Enokida, H., Yoshino, H., Hidaka, H., et al. (2012). Novel oncogenic function of mesoderm development candidate 1 and its regulation by MiR-574-3p in bladder cancer cell lines. Int. J. Oncol. 40, 951–959. doi: 10.3892/ijo.2011.1294
Turner, N., Tutt, A., and Ashworth, A. (2004). Hallmarks of ‘BRCAness’ in sporadic cancers. Nat. Rev. Cancer 4, 814–819. doi: 10.1038/nrc1457
Wang, R., Zheng, J., Zhang, D. S., Yang, Y. H., and Zhao, Z. F. (2015). Wnt1-induced MAFK expression promotes osteosarcoma cell proliferation. Genet. Mol. Res. GMR 14, 7315–7325. doi: 10.4238/2015.July.3.7
Wu, S. G., Huang, Y. J., Bao, B., Wu, L. M., Dong, J., Liu, X. H., et al. (2017). miR-508-5p acts as an anti-oncogene by targeting MESDC1 in hepatocellular carcinoma. Neoplasma 64, 40–47. doi: 10.4149/neo_2017_105
Yang, S., Liu, T., and Liang, G. (2020). The benefits of smoking cessation on survival in cancer patients by integrative analysis of multi-omics data. Mol. Oncol. 14, 2069–2080. doi: 10.1002/1878-0261.12755
Yavorski, J. M., and Blanck, G. (2016). Smoking correlates with increased cytoskeletal protein-related coding region mutations in the lung and head and neck datasets of the cancer genome atlas. Physiol. Rep. 4:e13045. doi: 10.14814/phy2.13045
Zhou, Y., He, L., Liu, X. D., Guan, H., Li, Y., Huang, R. X., et al. (2019). Integrated analysis of lncrna and mrna transcriptomes reveals new regulators of ubiquitination and the immune response in silica-induced pulmonary fibrosis. BioMed. Res. Int. 2019:6305065. doi: 10.1155/2019/6305065
Keywords: smoking cessation, homologous recombination deficiency, prognosis, SCC, risk score model
Citation: Chen C, Cheng X, Li S, Chen H, Cui M, Bian L and Jin H (2021) A Novel Signature for Predicting Prognosis of Smoking-Related Squamous Cell Carcinoma. Front. Genet. 12:666371. doi: 10.3389/fgene.2021.666371
Received: 10 February 2021; Accepted: 23 March 2021;
Published: 22 April 2021.
Edited by:
Tianbao Li, Geneis (Beijing) Co. Ltd., ChinaReviewed by:
Jiheng Xu, New York University, United StatesCopyright © 2021 Chen, Cheng, Li, Chen, Cui, Bian and Jin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Linlin Bian, MzA3ODgxMzgzQHFxLmNvbQ==; Hui Jin, MTg3NTE5NjI4MjZAMTYzLmNt
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.