
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Genet. , 09 April 2021
Sec. Genomic Medicine
Volume 12 - 2021 | https://doi.org/10.3389/fgene.2021.616392
 Xinyao Zhou1†
Xinyao Zhou1† Jia Zhou1†
Jia Zhou1† Xing Wei1Ruen Yao2Yingjun Yang1
Xing Wei1Ruen Yao2Yingjun Yang1 Linbei Deng1Gang Zou1Xietong Wang3
Linbei Deng1Gang Zou1Xietong Wang3 Yaping Yang4,5Tao Duan1
Yaping Yang4,5Tao Duan1 Jian Wang2*
Jian Wang2* Luming Sun1*
Luming Sun1*The purpose of the study was to use exome sequencing (ES) to study the contribution of single-gene disorders to recurrent non-immune hydrops fetalis (NIHF) and retrospectively evaluate the value of genetic diagnosis on prenatal management and pregnancy outcome. From January 2012 to October 2018, a cohort of 28 fetuses with recurrent NIHF was analyzed by trio ES. Fetuses with immune hydrops, non-genetic factors (including infection, etc.), karyotype, or CNV abnormalities were excluded. Variants were interpreted based on ACMG/AMP guidelines. Fetal therapy was performed on seven fetuses. Of the 28 fetuses, 10 (36%) were found to carry causal genetic variants (pathogenic or likely pathogenic) in eight genes (GBA, GUSB, GBE1, RAPSN, FOXC2, PIEZO1, LZTR1, and FOXP3). Five (18%) fetuses had variant(s) of uncertain significance (VUS). Of the 10 fetuses with definitive molecular diagnosis, five (50%) were diagnosed with inborn errors of metabolism. Among the seven fetuses who received fetal therapy, two had definitive molecular diagnosis and resulted in neonatal death. Among the remaining five fetuses with negative results, four had newborn survival and one had intrauterine fetal death. Trio ES could facilitate genetic diagnosis of recurrent NIHF and improve the prenatal management and pregnancy outcome.
Hydrops fetalis is a condition of excessively pathological fluid accumulation in more than two fetal tissues and body cavities. It affects 1 in 1,700–3,000 pregnancies and is a life-threatening fetal situation. Non-immune hydrops fetalis (NIHF) was described as fetal hydrops not caused by red cell alloimmunization. NIHF accounts for around 90% of cases of hydrops fetalis (Society for Maternal-Fetal Medicine, Norton et al., 2015).
NIHF should be thought of as a symptom or an end-stage status of a variety of diseases. The etiologies of NIHF include genetic disorders, structural abnormalities, hematologic diseases, infections, twin-twin transfusion syndrome, extrathoracic tumors, and other causes. Genetic disorders, including chromosomal abnormalities, copy number variations (CNV), and single-gene disorders, have been reported to account for one-third of NIHF cases (Moreno et al., 2013; Society for Maternal-Fetal Medicine, Norton et al., 2015).
Traditional karyotyping and chromosomal microarray analysis (CMA) have been suggested as a routine genetic testing offered to NIHF cases according to the AJOG guideline (Santo et al., 2011; Bellini et al., 2015; Society for Maternal-Fetal Medicine, Norton et al., 2015; Mardy et al., 2019, 2020; Sparks et al., 2019). According to recently published study, in which underlying genetic etiology were investigated in a total of 65 NIHF cases, CMA and/or karyotype testing were offered on 67.7% (44/65) of cases, and 25.0% (11/44) were confirmed to have chromosomal abnormalities and pathogenic/likely pathogenic CNV (Sparks et al., 2019). As we have known, a number of single-gene disorders were also associated with NIHF according to previous limited case reports and small series focusing on some specific genetic disorders. For example, lysosomal storage disorders (LSDs) have been reported to contribute to approximately 1% of non-immune hydrops cases by specific enzymatic analyses according to previous studies from 1979 to 2013 (Burin et al., 2004; Bellini et al., 2015). With exome sequencing (ES) widely used in recent years, more rare genetic diseases related to NIHF, such as generalized lymphatic dysplasia, Cornelia de Lange syndrome, Kabuki syndrome, and RASopathies, can also be identified with diagnostic yield of 9% and 29% for NIHF with normal karyotyping and CMA given the results from the PAGE study and the recent publication (Fotiou et al., 2015; Datkhaeva et al., 2018; Lord et al., 2019; Sparks et al., 2020). However, the PAGE study was not designed specific for NIHF cases, and the population studied in the recent publication was of different racial or ethnic backgrounds.
The purpose of the study was to investigate the detection rate and classification of single-gene disorder for recurrent NIHF cases presenting at our Fetal Medicine Unit of Shanghai First Maternity and Infant Hospital for possible fetal therapy by prenatal ES to help prenatal counseling, which were more likely associated with single-gene disorder.
We performed a retrospective study of 49 cases with recurrent fetal hydrops at the Fetal Medicine Unit and Prenatal Diagnosis Center of Shanghai First Maternity and Infant Hospital from January 2012 to October 2018.
Routine prenatal work-up was followed to explore the etiology of fetal hydrops according to AJOG and Chinese NIHF national guideline (Medicine CSOP, 2017; Mardy et al., 2019). ES was offered to the cases prenatally or postnatally as follows: (1) Immune fetal hydrops were ruled out by antibody screening test. (2) Normal karyotyping and CNV results. (3) There was no evidence of intrauterine cytomegalovirus (CMV), toxoplasmosis, and parvovirus infection by serum screening or diagnostic test by polymerase chain reaction (PCR) on amniotic fluid. (4) Thalassemia was ruled out by carrier screening and DNA testing following invasive diagnostic procedures. All the cases had detailed ultrasound and fetal echocardiography. Nuchal translucency or cystic hygroma in the first trimester, fetal structural abnormalities (including skeletal, cardiac, renal, intracranial, genital, face profile, etc.), and growth disorders were recorded.
Pretest counseling for prenatal ES was delivered in an intelligible fashion to the parents by trained genetic professionals. Parents were informed to receive disease-causing variants (pathogenic or likely pathogenic). They were also informed to be aware of the possibility of receiving variants of uncertain significance and choose whether to receive an extended analysis report for the fetus as well as for the parents, which included incidental and secondary findings. Results were reported to the parents when a multidisciplinary team of clinical and laboratory geneticists, obstetricians, and genetic counselors reviewed all the variants in relation to the ultrasound scan findings during pregnancy, or after delivery/termination.
This study was approved by the Ethical Committee of Shanghai First Maternity and Infant Hospital. Written informed consents were obtained from all patients who received genetic tests.
ES and variant evaluation were performed according to experimental procedures described previously (Hu et al., 2018). Genomic DNA was isolated from all samples by using the QIAamp DNA Blood Midi Kit (Qiagen, Hilden, Germany) according to the manufacturer’s protocol. Targeted regions were captured by the SureSelectXT Human All Exon V6 (Cat. No. 5190–8864, Agilent Technologies, Santa Clara, CA) kit. NGS was performed on the HiSeq X Ten platform (Illumina, San Diego, CA) according to the manufacturer’s protocol. Paired-end reads were aligned to the GRCh37/hg19 human reference sequence. BAM and VCF files were generated by NextGENe software (SoftGenetics, State College, PA).
Variants were annotated and filtered by Ingenuity Variant Analysis1. Common variants were filtered based on their frequencies in the databases of the Genome Aggregation Database (gnomAD)2, the Exome Sequencing Project3, the 1000 Genomes Project4, and an internal database. Forty genes associated with HPO, termed “Non-immune hydrops fetalis HP:0001790,” were first analyzed. If no candidate variant was found, we further analyzed all genes for putative disease-causing variants. Genes associated with inborn errors of metabolism, generalized lymphatic dysplasia, skeletal dysplasia, neurodevelopment disorders, cardiomyopathies, congenital nephritis, mitochondrial mutations, RASopathies, etc., were carefully analyzed. Rare phenotype-related variants were classified according to the American College of Medical Genetics and Genomics/Association for Molecular Pathology (ACMG/AMP) guidelines (Richards et al., 2015). All putative disease-causing variants detected by ES were confirmed by Sanger sequencing. Family members were also examined by PCR and Sanger sequencing to test the origin of the variants. A multidisciplinary team of clinical and laboratory geneticists, obstetricians, and genetic counselors reviewed all the variants in relation to the ultrasound scan findings to make a final decision about the seven variant classifications (e.g., positive-definitive, positive-probable, positive-possible, uncertain-VUS, uncertain-Autosomal Recessive, Single heterozygous variant, uncertain-contributory, and uncertain-other) according to the classification scheme of case-level results by Vora et al. (2017).
A total of 49 recurrent hydrops fetalis cases were identified from January 2012 through October 2018 in our center (Figure 1). Among these, 10 were immune fetal hydrops cases. One case was CNV anomalies with 5p15.33p14.3 duplication and 13q32.2q34 deletion from paternal balanced translocation. Two cases were confirmed with alpha-thalassemia by carrier screening and DNA testing by invasive diagnostic procedures. There were 28 pregnant women who agreed to have further ES evaluation for hydropic fetuses, and eight women refused. The demographics of the overall cohort are described in Table 1. The turnaround time of ES is 4–6 weeks.
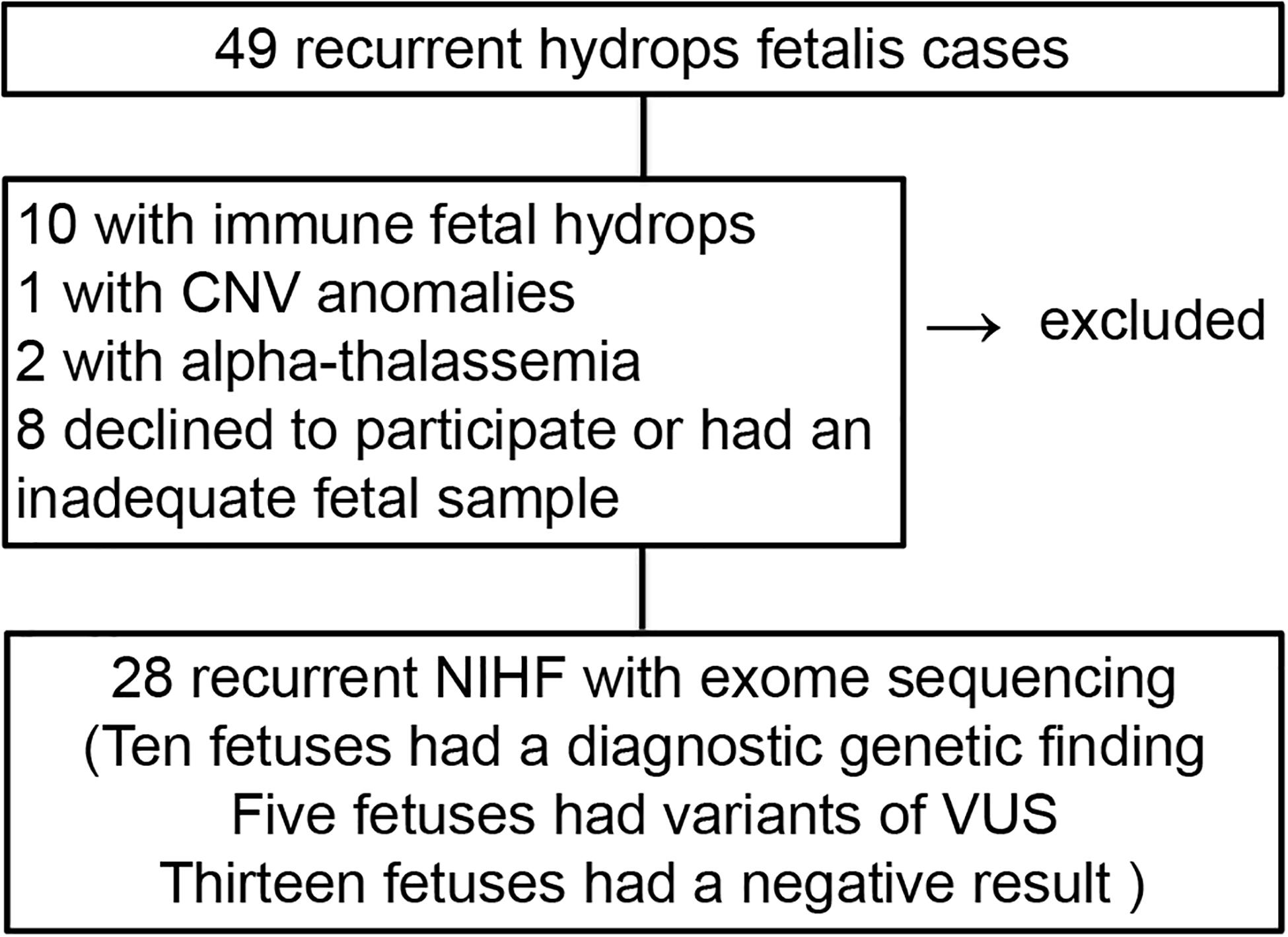
Figure 1. The flow diagram of the cohort and outcomes.
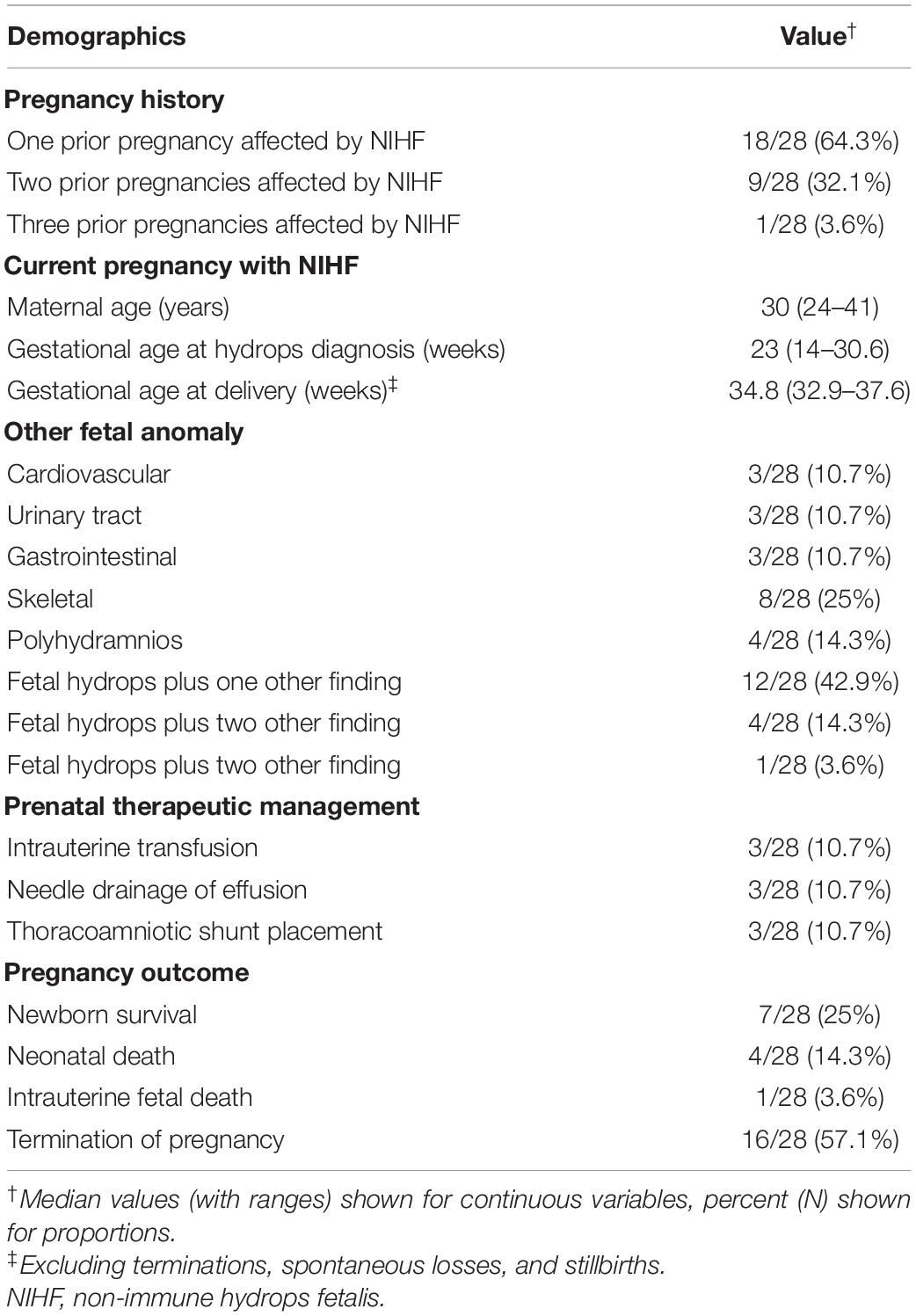
Table 1. Demographics of the overall cohort.
The genotype and phenotype data of our cohort are listed in Table 2 and Supplementary Table 1. Ten (36%) fetuses had a diagnostic genetic finding (i.e., the variant was considered pathogenic or likely pathogenic and causative of the fetal phenotype). These diagnostic variants included eight missense mutations, two in-frame deletion mutations, two frameshift mutations, one canonical + one splice site mutation, one stop-gain mutation, and one initiation codon mutation. Five (18%) fetuses showed genetic variants that were classified as clinically relevant variants of uncertain clinical significance (VUS). Thirteen fetuses (46%) had a negative result.
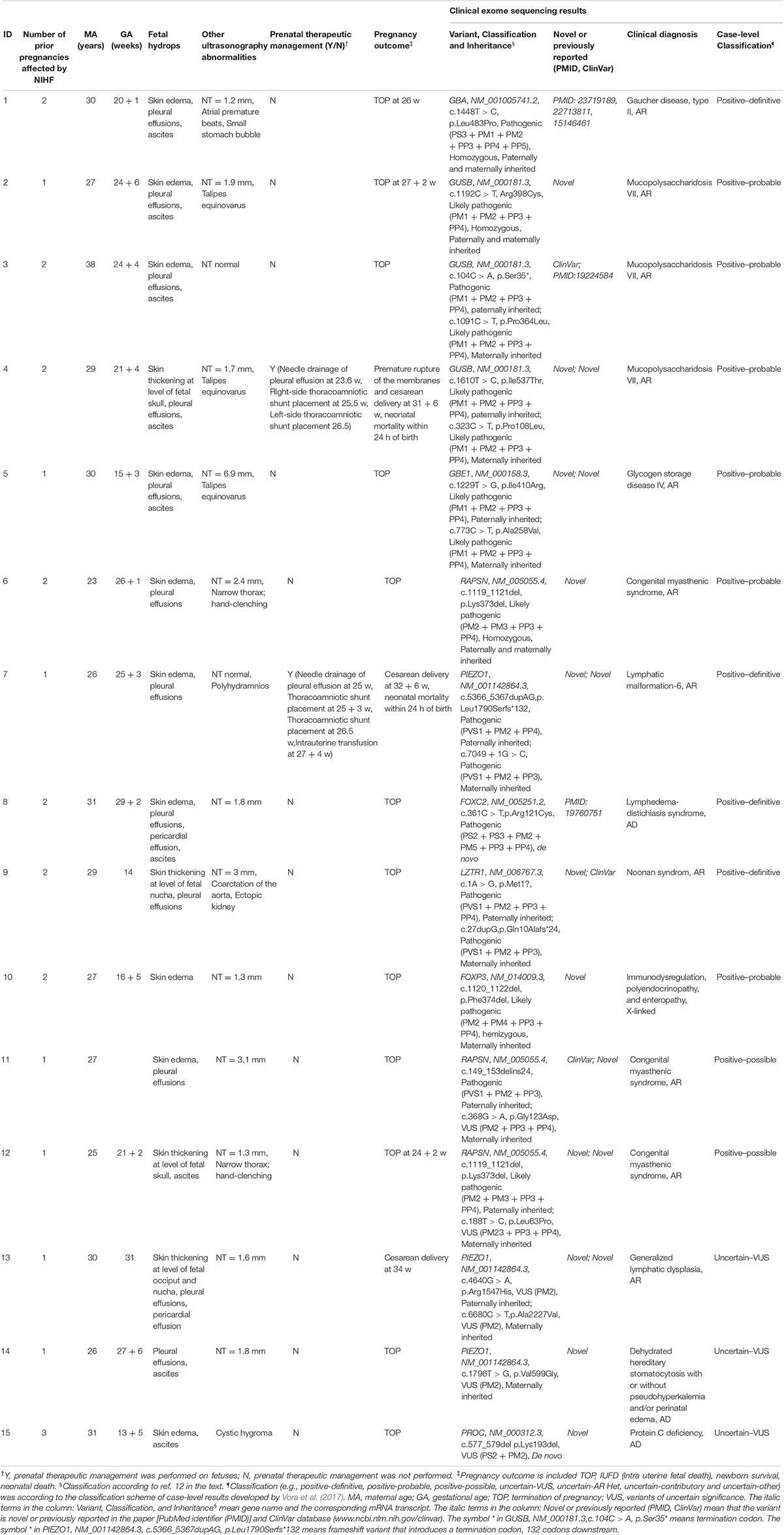
Table 2. The phenotype and genotype information of the cohort.
Of 10 diagnostic cases, nine fetuses had inherited the relevant mutations from their parents (one fetus with diagnosis of Gaucher disease, type II, GBA; three with mucopolysaccharidosis VII, GUSB; one with glycogen storage disease IV, GBE1; one with congenital myasthenic syndrome, RAPSN; one with lymphatic malformation-6, PIEZO1; one with Noonan syndrome LZTR1, and one with immunodysregulation, polyendocrinopathy, and enteropathy, FOXP3). The one with FOXP3 hemizygous mutation was X-linked recessive inherited disorders. One had a de novo mutation (lymphedema–distichiasis syndrome, FOXC2). For the de novo case given the history of recurrent NIHF, although there was no sample available for the previous pregnancy to confirm the same etiology with current pregnancy, germline mosaicism was highly suspected from parents. Among the 28 fetuses, 15 fetuses had additional abnormal ultrasound findings besides hydrops (including abnormal cardiovascular findings by echocardiogram, urinary tract abnormalities, gastrointestinal anomalies, skeletal abnormalities, and with 14% of the cases (4 of 28) had increased nuchal translucency (3 mm) or cystic hygroma). Among these, 6 (40%) of 15 cases had diagnostic genetic finding from ES results. Thirteen fetuses were isolated NIHF and 4 (31%) of 13 had diagnostic genetic finding. There was no significant difference in the detection rate of single-gene disorders between hydropic fetuses with or without other abnormal ultrasound findings.
Among the cohort, 16 chose termination of pregnancy (TOP) directly and 12 families chose to continue pregnancy. Seven fetuses received therapy, including intrauterine transfusion(s) for anemia and centesis and/or shunt insertion for pleural effusion (Tables 1, 2). With ES performed prenatally and postnatally. Five fetal interventions were done in isolated cases. Two were associated with other abnormal ultrasound findings, which were considered as secondary findings related to fetal hydrops: One was associated with talipes equinovarus and one with tricuspid regurgitation. Four of them survived with good outcomes and negative ES results. Three of them had perinatal death. One had fetal demise mostly like due to the complication from blood transfusion with negative ES result. The other two had neonatal death with positive ES results.
Trio-ES could deliver a diagnostic yield of 36% (10/28) in recurrent NIHF fetuses with no aneuploidy and causative CNVs detected and negative screening for alpha-thalassemia and beta-thalassemia.
A higher diagnostic rate (36%) was noticed in our study compared with other studies (Moreno et al., 2013; Sheth et al., 2017; Sudrie-Arnaud et al., 2018; Lord et al., 2019; Sparks et al., 2019, 2020). One reason was that recurrent fetal hydrops in the study represented a highly selected study group, which indicated that a higher incidence of single-gene disorders and non-genetic reasons contributing to NIHF has been ruled out as much as possible in the study following systematic work-up for NIHF. To our knowledge, only one study showed higher diagnostic rate (58%) by prenatal ES than our study. However, the study only included 12 NIHF cases, and 5 of 12 were found to carry the same homozygous variant in the AARS2 gene based on a founder effect (Bruwer et al., 2018). In our study, thalassemia, which can be contributed to NIHF with a higher prevalence in Southern China was ruled out through screening and targeted gene panel. Our data showed two cases (2/39, 5%) with alpha-thalassemia. The diagnostic rate of single-gene disorder by ES for recurrent NIHF in our study would be higher if thalassemia was also taken into account. Nearly half of the cases in our study still remain underdiagnosed. Most the known phenotypes are from postnatal data, making phenotype correlation for prenatal cases difficult. Systematic prenatal and postnatal examination should be evaluated for these NIHF cases. Moreover, undetected variants in critical functional regions of the known genes associated with NIHF beyond the exons or those that were not captured at sufficient depth for panel sequencing and CNVs below the resolution of chromosomal microarray still cannot be excluded. Additional WGS or Bionano optical mapping (BOM) may be beneficial in this situation while considering recurrent NIHF.
Among the cases with positive ES results, 80% of the cases (8 of 10) were autosomal recessive. One was X-linked recessive. One was autosomal dominant. Those major causes of fetal hydrops such as RASopathies, which composed the largest proportion in the recent publication (Sparks et al., 2020), are likely to be de novo and therefore would not have been identified in our recurrent cohort, which might skew results toward the autosome recessive inherited disorders. The results also indicated that inborn errors of metabolism accounted for 50% of the single-gene disorders for NIHF detected by ES, and they all confirmed to diagnosed with lysosomal storage disorders (LSD). A previous study from the Indian study group also indicated that lysosomal storage disorders (LSD) accounted for 21% (7/33) of NIHF cases. These indicated biochemical screening (HPLC-MS/MS) and/or lysosomal enzyme testing as a first-line test, which may help to improve the diagnostic strategy for NIHF.
It has been a big challenge to counsel with patients with recurrent fetal hydrops prenatally regarding whether genetic testing, including karyotype, CMA, and ES, should be offered to all the patients with NIHF or not. The study demonstrated that there was no significant difference in the detection rate of single-gene disorders between hydropic fetuses with or without structural abnormalities and suggested that ES should be offered to NIHF, especially recurrent NIHF cases, no matter whether the hydrops was isolated or not.
To explore the value of WES in the fetal therapy, prenatal and postnatal WES results from seven cases following fetal therapy for NIHF were reviewed, and perinatal outcomes were followed up. Four cases survived with good outcomes, which all had negative ES results. Three cases had perinatal death, two of which had positive ES results diagnosed by postnatal samples. Our study indicated that developing rapid or even express ES would be helpful to prioritize workflow for prenatal management for improving the perinatal outcomes.
Our study is not without limitations. The turnaround time (4–6 weeks) is relatively long for a prenatal application, and the sample size in our study is too small to systematically evaluate the profile and frequency of each single-gene disorder in NIHF. A large prospective study of the NIHF cohort will be expected in the future study.
In conclusion, trio-ES can deliver a high diagnostic yield in recurrent NIHF condition. Inborn errors of metabolism were the major causes of the single-gene disorders for recurrent NIHF and accounts for half of our diagnosed cases. The identification of a single-gene disorder may optimize the workflow for prenatal management for NIHF.
The data that support the findings of this study are available on request from the corresponding author.
The studies involving human participants were reviewed and approved by the Ethical Committee of Shanghai First Maternity and Infant Hospital. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin. Written informed consent was obtained from the individual(s), and minor(s)’ legal guardian/next of kin, for the publication of any potentially identifiable images or data included in this article.
LS conceived and designed the workflow. XZ performed the experiments, analyzed the data, and wrote the manuscript. JZ, XWe, YiY, LD, and GZ collected the samples. RY and JW analyzed the data and created the figures. XWa, YaY, TD, and JW revised the manuscript. All authors approved the final manuscript.
This work was supported by the National Key Research and Development Program of China (Grant No. 2018YFC1002900), National Natural Science Foundation of China (Grant Nos. 81601312, 82071656, and 81871174), Foundation of Shanghai Municipal Commission of Health and Family Planning (Grant No. 201540195), Shanghai Hospital Development Center (Grant No. SHDC12016117), Science and Technology Commission of Shanghai Municipality (Grant No. 16411963100), Shanghai Municipal Medical and Health Discipline Construction Projects (Grant No. 2017ZZ02015), and the Shanghai “Rising Stars of Medical Talent” Youth Development Program.
YaY was employed by the company AiLife Diagnostics.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationship that could be construed as a potential conflict of interest.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fgene.2021.616392/full#supplementary-material
Bellini, C., Donarini, G., Paladini, D., Calevo, M. G., Bellini, T., Ramenghi, L. A., et al. (2015). Etiology of non-immune hydrops fetalis: an update. Am. J. Med. Genet. A 167A, 1082–1088. doi: 10.1002/ajmg.a.36988
Bruwer, Z., Al Riyami, N., Al Dughaishi, T., Al Murshedi, F., Al Sayegh, A., Al Kindy, A., et al. (2018). Inborn errors of metabolism in a cohort of pregnancies with non-immune hydrops fetalis: a single center experience. J. Perinat. Med. 46, 968–974. doi: 10.1515/jpm-2017-0124
Burin, M. G., Scholz, A. P., Gus, R., Sanseverino, M. T., Fritsh, A., Magalhaes, J. A., et al. (2004). Investigation of lysosomal storage diseases in nonimmune hydrops fetalis. Prenat. Diagn. 24, 653–657. doi: 10.1002/pd.967
Datkhaeva, I., Arboleda, V. A., Senaratne, T. N., Nikpour, G., Meyerson, C., Geng, Y., et al. (2018). Identification of novel PIEZO1 variants using prenatal exome sequencing and correlation to ultrasound and autopsy findings of recurrent hydrops fetalis. Am. J. Med. Genet. A 176, 2829–2834. doi: 10.1002/ajmg.a.40533
Fotiou, E., Martin-Almedina, S., Simpson, M. A., Lin, S., Gordon, K., Brice, G., et al. (2015). Novel mutations in PIEZO1 cause an autosomal recessive generalized lymphatic dysplasia with non-immune hydrops fetalis. Nat. Commun. 6:8085. doi: 10.1038/ncomms9085
Hu, X., Li, N., Xu, Y., Li, G., Yu, T., Yao, R. E., et al. (2018). Proband-only medical exome sequencing as a cost-effective first-tier genetic diagnostic test for patients without prior molecular tests and clinical diagnosis in a developing country: the China experience. Genet. Med. 20, 1045–1053. doi: 10.1038/gim.2017.195
Lord, J., McMullan, D. J., Eberhardt, R. Y., Rinck, G., Hamilton, S. J., Quinlan-Jones, E., et al. (2019). Prenatal exome sequencing analysis in fetal structural anomalies detected by ultrasonography (PAGE): a cohort study. Lancet 393, 747–757. doi: 10.1016/S0140-6736(18)31940-8
Mardy, A. H., Chetty, S. P., Norton, M. E., and Sparks, T. N. (2019). A system-based approach to the genetic etiologies of non-immune hydrops fetalis. Prenat. Diagn. 39, 732–750. doi: 10.1002/pd.5479
Mardy, A. H., Rangwala, N., Hernandez-Cruz, Y., Gosnell, K. A., Gonzalez, J. M., Norton, M. E., et al. (2020). Utility of chromosomal microarray for diagnosis in cases of nonimmune hydrops fetalis. Prenat. Diagn. 40, 492–496. doi: 10.1002/pd.5617
Medicine CSOP (2017). Clinical guideline: nonimmune hydrops fetalis. Chin. J. Perinat. Med. 20, 769–775. (Chinese Journal),Google Scholar
Moreno, C. A., Kanazawa, T., Barini, R., Nomura, M. L., Andrade, K. C., Gomes, C. P., et al. (2013). Non-immune hydrops fetalis: a prospective study of 53 cases. Am. J. Med. Genet. A 161A, 3078–3086. doi: 10.1002/ajmg.a.36171
Richards, S., Aziz, N., Bale, S., Bick, D., Das, S., Gastier-Foster, J., et al. (2015). Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American college of medical genetics and genomics and the association for molecular pathology. Genet. Med. 17, 405–424. doi: 10.1038/gim.2015.30
Santo, S., Mansour, S., Thilaganathan, B., Homfray, T., Papageorghiou, A., Calvert, S., et al. (2011). Prenatal diagnosis of non-immune hydrops fetalis: what do we tell the parents? Prenat. Diagn. 31, 186–195. doi: 10.1002/pd.2677
Sheth, J., Mistri, M., Shah, K., Chaudhary, M., Godbole, K., and Sheth, F. (2017). Lysosomal storage disorders in nonimmune hydrops fetalis (NIHF): an Indian experience. JIMD Rep. 35, 47–52. doi: 10.1007/8904_2016_24
Society for Maternal-Fetal Medicine, Norton, M. E., Chauhan, S. P., and Dashe, J. S. (2015). Society for maternal-fetal medicine (SMFM) clinical guideline #7: nonimmune hydrops fetalis. Am. J. Obstet. Gynecol. 212, 127–139. doi: 10.1016/j.ajog.2014.12.018
Sparks, T. N., Lianoglou, B. R., Adami, R. R., Pluym, I. D., Holliman, K., Duffy, J., et al. (2020). Exome sequencing for prenatal diagnosis in nonimmune hydrops fetalis. N. Engl. J. Med. 383, 1746–1756. doi: 10.1056/NEJMoa2023643
Sparks, T. N., Thao, K., Lianoglou, B. R., Boe, N. M., Bruce, K. G., Datkhaeva, I., et al. (2019). Nonimmune hydrops fetalis: identifying the underlying genetic etiology. Genet. Med. 21, 1339–1344. doi: 10.1038/s41436-018-0352-6
Sudrie-Arnaud, B., Marguet, F., Patrier, S., Martinovic, J., Louillet, F., Broux, F., et al. (2018). Metabolic causes of nonimmune hydrops fetalis: a next-generation sequencing panel as a first-line investigation. Clin. Chim. Acta 481, 1–8. doi: 10.1016/j.cca.2018.02.023
Keywords: exome sequencing, single gene disorders, prenatal diagnose, non-immune hydrops fetalis NIHF, prenatal management
Citation: Zhou X, Zhou J, Wei X, Yao R, Yang Y, Deng L, Zou G, Wang X, Yang Y, Duan T, Wang J and Sun L (2021) Value of Exome Sequencing in Diagnosis and Management of Recurrent Non-immune Hydrops Fetalis: A Retrospective Analysis. Front. Genet. 12:616392. doi: 10.3389/fgene.2021.616392
Received: 13 October 2020; Accepted: 26 February 2021;
Published: 09 April 2021.
Edited by:
Mark Kilby, University of Birmingham, United KingdomReviewed by:
Mary Norton, University of California, San Francisco, United StatesCopyright © 2021 Zhou, Zhou, Wei, Yao, Yang, Deng, Zou, Wang, Yang, Duan, Wang and Sun. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jian Wang, TGFid2FuZ2ppYW5Ac2hzbXUuZWR1LmNu; Luming Sun, bHVtaW5nX3N1bkAxNjMuY29t
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.