
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Epidemiol. , 02 May 2023
Sec. Infectious Disease Epidemiology
Volume 3 - 2023 | https://doi.org/10.3389/fepid.2023.1068097
 Tubihemukama Methodius1*
Tubihemukama Methodius1* Angella Musewa2Bernadette Basuta Mirembe3Doreen Birungi2Sarah Nitumusiima2
Angella Musewa2Bernadette Basuta Mirembe3Doreen Birungi2Sarah Nitumusiima2 Irene Naigaga1,2John David Kabasa1William Bazeyo2
Irene Naigaga1,2John David Kabasa1William Bazeyo2
Introduction: COVID-19 is an infectious disease caused by severe acute respiratory syndrome coronavirus 2. There were no licensed vaccines or explicit medicines available for treatment at the time of conducting this study. Public health and social measures (PHSM) have been widely adopted to reduce the transmission of COVID-19. Hence, assessing people's knowledge, attitudes, and adherence/practices related to the management of COVID-19 is crucial for identifying the factors that may promote or hinder adherence to the implementation of PHSM.
Methods: We conducted a cross-sectional study in the Amuru, Kyotera, Wakiso, and Kampala districts of Uganda. We used a simple random sampling technique to select households and conducted face-to-face interviews in selected households. We administered questionnaires to respondents to assess the factors that promote or hinder adherence to and knowledge about PHSM implementation. We used a Likert scale to assess respondents’ attitudes toward COVID-19.
Results: Out of the 270 respondents, 54 (20%), 73 (27%), 42 (15.6%), and 101 (37.4%) were from the Kampala, Amuru, Wakiso, and Kyotera districts, respectively. Most of the respondents had adequate knowledge (72.2%), a high level of adherence (63.7%), and approximately 57.8% had good attitudes relating to COVID-19 and its prevention measures. An inferential analysis revealed that people from the Kampala district had higher chances (odds ratio = 4.668) of having a high level of knowledge compared to people from the Amuru district. It was also found that respondents who had a high level of (adequate) knowledge were twice as likely to have good attitudes compared to those with a low level of knowledge. In addition, people with good attitudes were 2.5 times as likely to adhere to the COVID-19 prevention measures compared to those with poor attitudes.
Conclusion: Most respondents had limited knowledge though the majority of them had adopted practices to prevent the spread of COVID-19. Respondents with low knowledge of COVID-19 need to be targeted, to improve their attitude toward the disease and their adherence to safe prevention practices.
COVID-19 is a contagious disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (1). The virus was first detected in Wuhan city, central China, in December 2019 (2). Cases were detected in other countries among international travelers who traveled from Wuhan to various countries (3). By February 2023, more than 6.8 million deaths worldwide and 3,628 cumulative deaths in Uganda had been recorded (4, 5). Currently, there are approved vaccines but no explicit medicines available for the treatment of COVID-19, and appropriate public health and social measures (PHSM) are key in preventing its transmission.
According to the WHO, PHSM are actions performed by individuals, institutions, communities, local and national governments, and international bodies to slow or stop the spread of COVID-19 (6). These measures can be individual and public, such as detecting and isolating cases, contact tracing and quarantine, and social and physical distancing (7). For PHSM to slow or stop the transmission of COVID-19, they must be implemented with the full engagement of the public. The extent to which the public adheres to the guidelines issued by the government is key.
COVID-19 is transmitted predominantly through respiratory droplets and, to a lesser extent, through contact with contaminated surfaces (8). A study conducted by Jones et al. highly indicated evidence of environmental contamination by patients with SARS-CoV-2 through respiratory droplets and fecal shedding, suggesting the environment is a potential medium of transmission; this supports the need for strict adherence to hand hygiene and other safety measures (9).
Uganda experienced the COVID-19 outbreak, with nearly 40,000 cases as of February 2021 (10). The government of Uganda imposed a total lockdown on most businesses and movements, both nationally and internationally, for easy containment of the disease, as was done in many other countries (11). The Ugandan Ministry of Health also invested heavily in community sensitization through media houses as well as mass testing, the equipping of healthcare units, and the recruitment of staff to increase the country's task force to fight the disease (12). By June 2020, it had been just 4 months since the confirmation of the first case in Uganda, and new cases were accumulating, with over four deaths, 1,154 accumulative cases, and over 1,000 recoveries (10). Community transmission was reported in various districts at the time of this study, given the intensive sensitization by the government. The Kampala and Wakiso districts recorded the highest number of community transmission cases whereas the Kyotera and Amuru districts were border districts at risk of continuous importation of the infection. The transmission of COVID-19 could be reduced by adhering to the standard operating procedure (SOP) (13). Therefore, the present study aimed to assess the knowledge, attitudes, and adherence among communities in high-risk districts and determine the possible drivers affecting adherence to PHSM for COVID-19. This study will add to the existing knowledge about the prevention and control of the spread of infectious diseases in low-income countries such as Uganda. The study helps to understand the different knowledge, practices, and attitudes about the PHSM regarding the border districts.
We conducted a cross-sectional study involving four districts: Amuru, Kyotera, Wakiso, and Kampala. These districts were selected because they registered the highest community and local transmission in Uganda at the time of writing the concept in June 2020. This was characterized by increased daily new cases within such communities, whose levels of knowledge, attitudes, and adherence to the prevention measures were unknown at the time. The Amuru district, in northern Uganda, hosts the Elegu border point, which is the major cross-border point to South Sudan. The Kyotera district, in southern Uganda, hosts two major cross-border points to Tanzania: Mutukula and Kasesero. The Kampala district, in the central region and home to the capital city of Uganda, hosts most national institutions. The Wakiso district, in the central region, surrounds Kampala and hosts the only international airport in Uganda, Entebbe. These areas have been illustrated on a map in Figure 1.
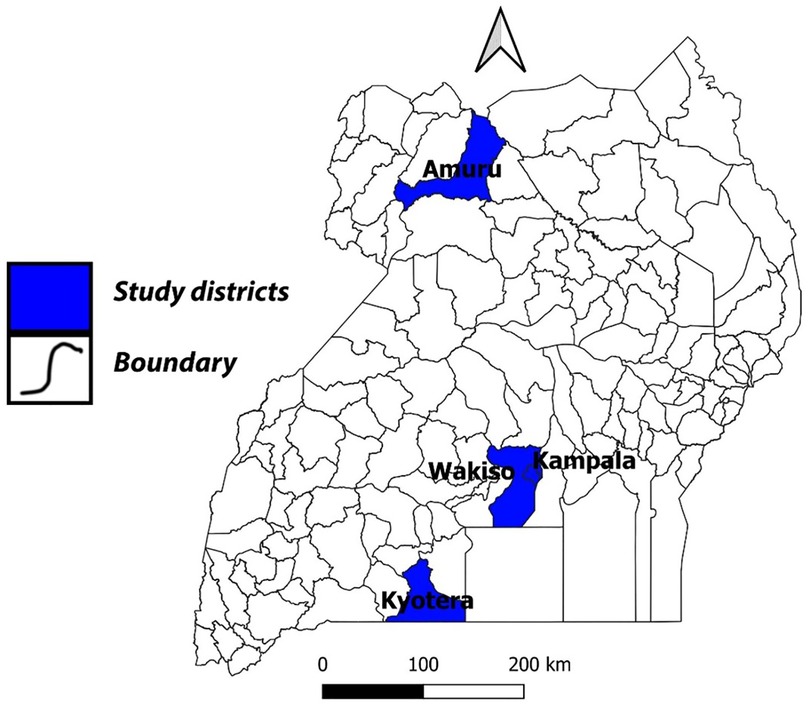
Figure 1. Map of Uganda showing the Amuru, Kyotera, Wakiso, and Kampala districts.
The present study was conducted among individuals in households within selected high-risk districts with community transmission. Emphasis was made to ensure that the head of the household responded to the questions since they were assumed to have sufficient knowledge about those living in the same household. We used households as our study unit to ensure different respondents were interviewed. The total number of people (population) in all the study districts was approximately 5,072,800 (https://www.citypopulation.de/en/uganda/admin/). Using the Taro Yamane formula, a total of 280 households was estimated to be selected from the four districts of study. We used a simple random sampling method to select households. Using information from the district health officers (DHOs) and village health teams (VHTs), high-risk sub-counties (with a high likelihood of human concentration, such as trading centers) were considered for the selection of households.
We conducted face-to-face interviews guided by a structured questionnaire administered to respondents of these selected households during the month of November 2020, when lockdown restrictions were partly loosened to all movement of extra public health workers. We collected data on demographic characteristics, including sex, age, level of education, exposure factors, and sources of information on COVID-19. Knowledge of COVID-19 was assessed with different questions and each plausible answer considered to be correct scored 1 point; incorrect responses scored 0 points. We assessed the attitudes of respondents using a 5-point Likert scale with questions modified appropriately for COVID-19. The responses were as follows: strongly disagree, disagree, neutral, agree, and strongly agree, with each scoring 1–5, respectively. We categorized responses using a 4-point Likert scale for practices toward COVID-19; these were scored 1 to 4 as always, sometimes, rarely, and never, respectively.
Data were entered into an Excel spreadsheet and cleaned for inconsistencies and missing values. The cleaned data were then imported into SPSS version 23 for statistical analysis. Numerical data were presented as means and standard deviations. Categorical data were presented as frequencies and proportions. The variables that were used to evaluate each of the components (knowledge, attitude, and adherence) were first averaged for each respondent (row-wise) to generate a continuous column of means for each component. For each component, a mean of the means was computed. In addition, for each component, values above the mean of the means were categorized as adequate/good/high and those below the mean of the means as inadequate/poor/low, for knowledge, attitude, and adherence, respectively. The association between knowledge, attitude, and adherence with predisposing factors was determined using a chi-square test, and associations with related p-values <0.05 were considered to be significant (bivariate analysis level). The significant factors were then combined to run logistic regression models (multivariate analysis level).
The present study aimed to assess the knowledge, attitude, and adherence relating to COVID-19 prevention measures. It was conducted in four districts in Uganda: Amuru (73/270, 27%), Kyotera (101/270, 37.4%), Wakiso (42/270, 14.6%), and Kampala (54/270, 20.0%). Most (165/270, 61.1%) of the respondents were women, whereas 105 (38.9%) were men. The mean age of the respondents was 39 ± 13 years, and most of the respondents (114/270, 42.2%) were aged 30–44 years. The majority of the respondents had attained a primary education level (34.8%), whereas fewer (15.2%) of them did not have any formal education. Their major source of COVID-19 information was the media, including radio, television, and social media platforms such as WhatsApp and Facebook. Friends as a source of information included relatives, peer members, and any other person involved in the conveying of information without involving any media means (Table 1).

Table 1. Demographic characteristics of the respondents.
The majority (72.2%) of the respondents had adequate knowledge of COVID-19 and its prevention measures. This could be attributed to efforts by the Ministry of Health in educating the public about prevention and control measures. People from the districts of Wakiso (100%), Kyotera (63.5%), Kampala (100%), and Amuru (78.1%) registered adequate knowledge about COVID-19 and its prevention measures, except for Amuru (42.5%) (Table 2).
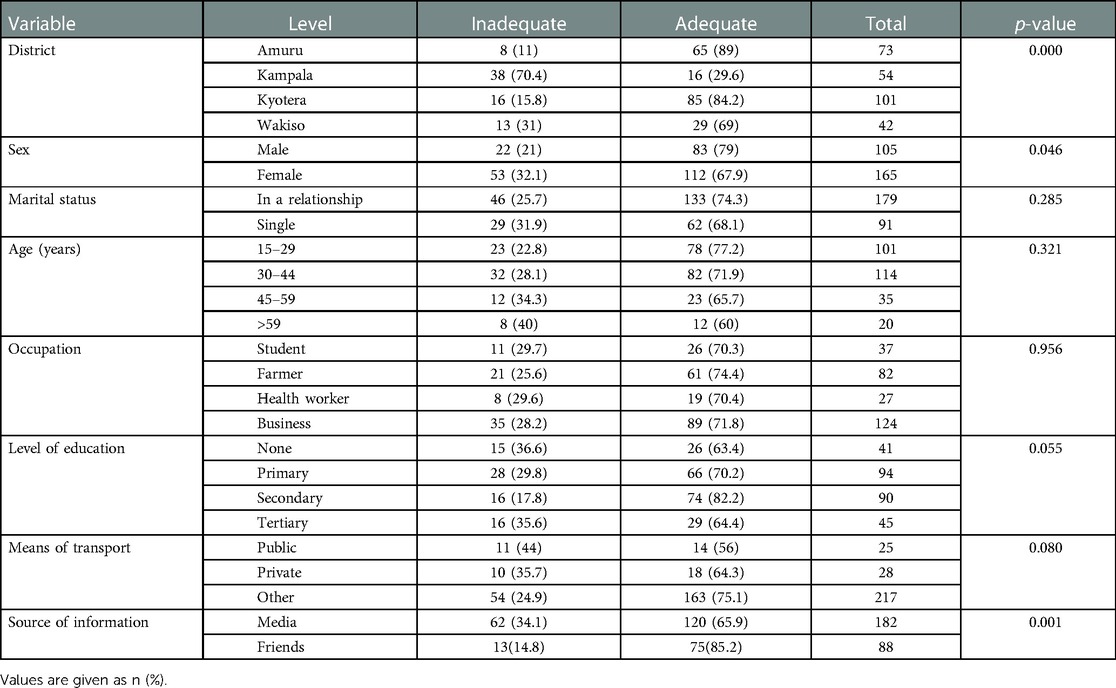
Table 2. Distribution of knowledge of COVID-19 prevention measures according to demographic characteristics.
The majority (72.2%) of the respondents had an adequate knowledge of COVID-19 control measures. The knowledge was associated significantly with district (p = 0.00), sex (p = 0.046), and source of information (p = 0.001) (Table 2). It is worth observing that people from Kyotera, Amuru, and Wakiso had a higher knowledge of COVID-19 control measures than those from Amuru and Kyotera. In fact, no respondents were found to have inadequate knowledge in Wakiso and Kampala. It was also discovered that the means of transport commonly used by a person was significantly associated with his/her knowledge. The majority of the men (69.5%) and women (71.5%) had an above-average knowledge of COVID-19 prevention measures.
The dependent variable was the level of knowledge, whereas the independent variables were those that were significantly associated with the level of knowledge in a chi-square test (district of residence, sex, and source of information). The factors were considered as significantly related to knowledge if the corresponding p-value was <0.05 (critical). People in the Kampala district were associated with increased odds [adjusted odds ratio (AOR) = 4.668, p = 0.003] of having adequate knowledge compared to those from the Amuru district as presented in Table 4.
Men were twice as likely to have adequate knowledge compared to women, although this relationship was not significant.
Most (57.8%) of the respondents had a good attitude toward COVID-19 and its prevention measures. The majority (75.9%) of the people strongly agreed that COVID-19 was a dangerous infectious disease. Most (72.2%) of the people strongly agreed that COVID-19 was a dangerous infectious disease. The good attitudes toward COVID-19 and its prevention may also be explained by the fact that most of the respondents strongly agreed that they were at risk of contracting the disease (53.7%) and that the transmission can be prevented (54.1%) (Table 3).
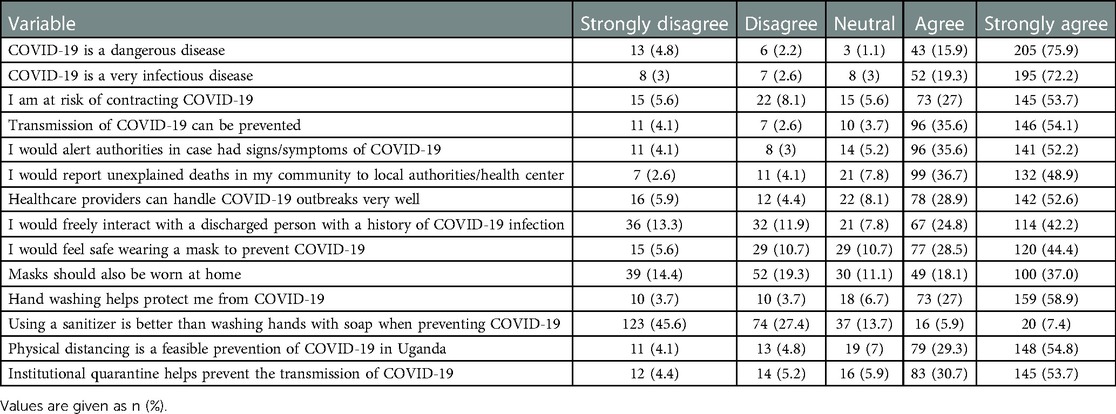
Table 3. Attitudes of respondents toward COVID-19 prevention and control measures.
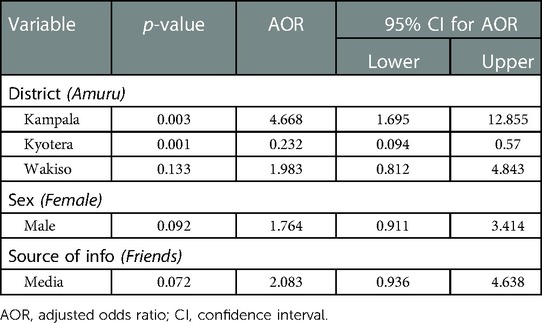
Table 4. Logistic regression for analysis of factors relating to knowledge of the respondents about COVID-19 and the prevention measures.
The majority of the respondents from Kyotera, Kampala, and Amuru had a good attitude toward COVID-19 prevention measures, whereas most of the respondents from Wakiso (28/42, 66.7%) had a poor attitude. The association between district and attitude levels was significant (p = 0.006). There was also a significant association between the knowledge of COVID-19 prevention measures and the practice of these measures (p = 0.005), as presented in Table 5.
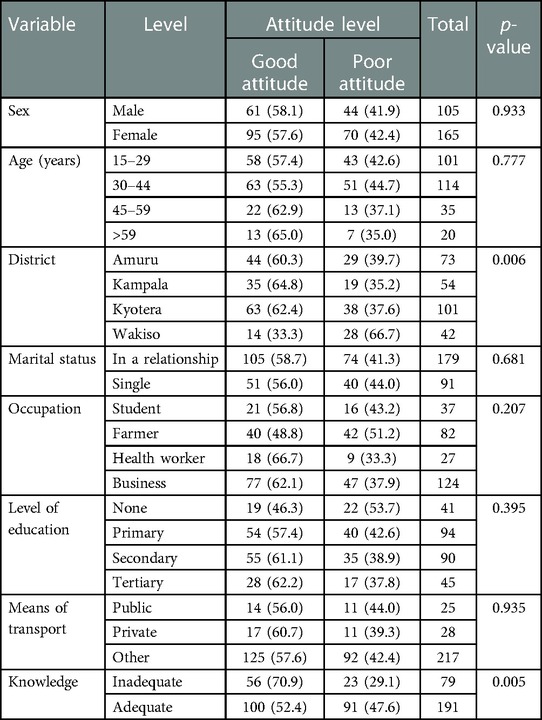
Table 5. The association between attitudes and demographic characteristics of the respondents.
At the multivariate level, logistic regression was conducted. Respondents with adequate knowledge were significantly associated with increased odds of having good attitudes compared to those with limited knowledge [p = 0.016, 95% confidence interval (CI) = 1.161–4.256] as presented in Table 7. People from Wakiso had increased odds of having a good attitude toward COVID-19 prevention measures compared to people from the Amuru district.
Most (63.7%) of the people adhered to the practices recommended by the Ministry of Health to prevent the spread of COVID-19. However, some guidelines were not followed, for example most of the people never washed their hands routinely (73.7%) as recommended by the Ministry of Health (Table 8). The majority of the people also never avoided masses of people (63.0%) as well as the cleaning of surfaces (45.2%). Similarly, most of the people avoided sharing masks (74.8%), given that most of them did not even wear masks (59.6%).
The adherence to COVID-19 prevention measures was associated with knowledge about these measures, the attitude of the people toward these measures, and the district (location). The associations were determined using chi-square tests, and the associations were rendered significant if the p-value was <0.05 (the critical value). There was a significant association between the district of the respondents and adherence to COVID-19 prevention measures.
High levels of adherence were observed among people aged 45–59 years compared to those who were aged 60 years or above. The majority of married people (65.4%) had a high level of adherence to the measures compared to unmarried people (60.4%) as presented in Table 9.
The determination of the factors influencing the practice of respondents about COVID-19 prevention measures involved logistic regression. The dependent variable was the practice level, whereas the independent variables were those that were significantly associated with the practice level in a chi-square test (district of residence, level of knowledge, and attitude). The factors were considered to be significantly related to knowledge if the corresponding p-value was <0.05 (critical value). The results were presented in Table 10. People in Wakiso were significantly associated with reduced odds of thoroughly practicing the prevention measures compared to those in the Amuru district (p < 0.01, AOR = 0.255, 95% CI = 0.085–0.762).
People with a good attitude were 2.5 times as likely to adhere to the COVID-19 prevention measures compared to those with a poor attitude. People with adequate knowledge were 28 times as likely to adhere to the COVID-19 prevention measures compared to those with poor attitudes.
During the year 2020, the world was hit by continuous strong waves of the COVID-19 pandemic (14). Uganda, like other low-income countries that are characterized by a weak and less financed health sector, was faced with difficulties in the prevention and containment of the disease. Many government agencies and ministries, such as the Ministry of Health, and stakeholders carried out campaigns to sensitize the public about SOPs aimed at increasing knowledge of the pandemic, as well as adherence to the procedures to reduce the spread and contain the pandemic. Therefore, the present study aimed to assess the knowledge, attitude, and adherence of people relating to these prevention measures, given the government of Uganda's and stakeholders’ sensitization. The results of this study could be used to evaluate the impact of government and stakeholder sensitization, and the methods used on people's knowledge and attitudes as well as their practice/adherence. This evaluation can also be used to identify the gaps and strengths in these campaigns for future improvement in case of similar outbreaks.
Mitigation strategies, including PHSM, have been employed in various countries to limit the transmission of COVID-19 and contain it. As highlighted by Wilder-Smith et al., the containment of the pandemic depends on the success of preventive measures that have been instituted (15). This has been evident in many countries, including Uganda, Tanzania, as well as China and Germany (16–18). In this study, most respondents had a good attitude toward COVID-19 prevention and control measures instituted by the government of Uganda. For instance, the majority of respondents reported having avoided crowded places, practiced social distancing, avoided sharing masks, and washed their hands with soap regularly; however, these may be subjective given the fact that they were individual reports. These findings were in agreement with those of Amodan et al. (19), who reported that people in Uganda observed physical distancing, as well as avoided touching their faces. Other studies also registered similar findings (20, 21). In this study, a significant number of respondents were aware that they were at risk of contracting COVID-19. Similarly, Kasozi et al. (22) and Okaka and Omondi (23) reported that respondents were aware of the risk of contracting COVID-19 but the implementation of practices such as hand washing was problematic and challenging in Uganda and Kenya, respectively. This could be combated by investing heavily in the sensitization of the public to induce behavior change in communities, especially in future pandemics and epidemic outbreaks, such as the common Ebola and Marburg outbreaks, since adequate knowledge is often associated with good attitudes and practices (24).
In this study, most of the respondents had adequate knowledge of COVID-19 and its prevention measures. This could be explained by the fact that most of the respondents were aware of the transmission routes as well as the signs and symptoms of COVID-19 (Table 6), given the government of Uganda's sensitization programs. Similar findings have been reported in Tanzania as well as Kenya in 2020, where more than 80% of the respondents had good knowledge of COVID-19 (25). The findings were also similar to those from a study conducted in Kenya in 2020 in which the authors revealed that most of the people had adequate knowledge of COVID-19 (26).
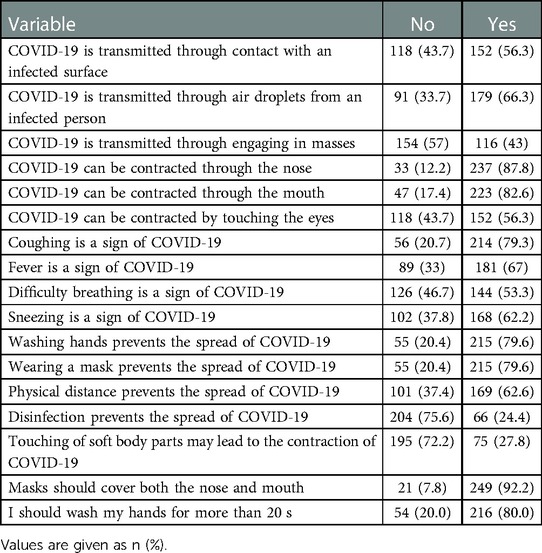
Table 6. Knowledge assessment of COVID-19 and prevention measures.
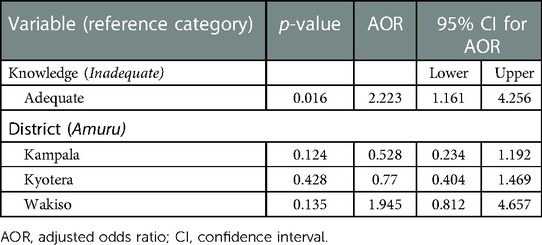
Table 7. Logistic regression results factors relating to attitude levels.

Table 8. Adherence to the recommended guidelines for the prevention and control of COVID-19.

Table 9. The association between demographic characteristics and adherence to COVID-19 prevention measures.
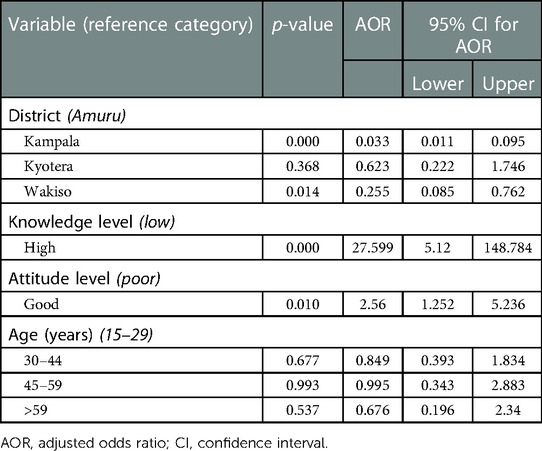
Table 10. Logistic regression for the relationship between adherence levels and demographic characteristics.
This study revealed that people who received COVID-19 news mainly from the media, such as the radio and television, were twice as likely to have adequate knowledge compared to those who relied on their friends for information. This might have been due to the fact that the trusted and reliable sources of information, i.e., the Ministry of Health and COVID-19 stakeholders, disseminated appropriate information mainly through media houses (27). Similarly, a study conducted in 2020 in Uganda reported a high knowledge score among people with phones connected to the Internet (28). In addition, this study revealed that the proportion of respondents with a high level of knowledge was higher among people with a formal education (who had attained at least a primary level), compared to those without a formal education. This was in agreement with the findings of Isah et al. in Nigeria, who reported that higher levels of education are associated with high knowledge of COVID-19 and its prevention guidelines (29).
The present study reported that most of the respondents strongly agreed that masks can help prevent COVID-19. This agreement with COVID-19 prevention measures, however, did not mean adherence to these measures as this study found that the level of adherence was low. These study findings were in agreement with the findings by Mboya et al., which revealed that public mask-wearing was regarded as an effective measure of stopping the spread of the virus when public compliance is high (25). Furthermore, a systematic review in Kenya found that the use of facemasks was very pertinent in preventing the spread of COVID-19 (30). That study also reported that the majority of people strongly agreed that they were at risk of getting COVID-19, and they were aware that the disease could be avoided mainly through hand washing, physical social distancing, as well as institutional quarantine.
The community had already been in lockdown for months due to COVID-19 and hence was fragile. This resulted in low counts of respondents in some districts. Due to this situation, we also only considered the questions the respondents were comfortable responding to, causing fluctuations in the totals.
The findings revealed multiple facilitators and barriers to adherence to PHSM. Factors such as good attitude and following media reports were considered to be promoters, while sufficient knowledge of COVID-19 among respondents facilitated adherence to PHSM. Respondents with low levels of knowledge of COVID-19 need to be targeted, to improve their attitude and adherence to safe practices. The platform to be used for communication on COVID-19 to the public should be radios, given that most respondents reported using them as their source of information.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
This activity was in response to a public health emergency and was therefore determined to be non-research. AFROHUN’s Uganda office determined this to be non-research and its primary intent was public health practice or a disease control activity (specifically, epidemic or endemic disease control activity). We sought permission from District Health Officers before district entry. We sought verbal informed consent in the local language from respondents.
BBM was responsible for conceptualization and data curation. DB, WB, AM, and JDK were responsible for conceptualization and funding acquisition. MT and BBM were responsible for data analysis and writing the final draft. IN and ST conducted the fieldwork coordination. All authors contributed to the article and approved the submitted version.
This study was made possible by the generous support of the American people through the U.S. Agency for International Development (USAID) One Health Workforce—Next Generation (OHW-NG) Award 7200AA19CA00018. The contents and associated materials are the responsibility of the authors and do not necessarily reflect the views of USAID or the U.S. Government.
We acknowledge the contributions of the District Health Offices of Kampala, Wakiso, Amuru, and Kyotera for supporting the teams that conducted this study. We also thank the communities from these high-risk districts and staff at all health facilities visited during this study. We thank the Ugandan Ministry of Health for the technical guidance and One Health Workforce—Next Generation (OHW-NG) project through Africa One Health University Network (AFROHUN) for the support rendered during the study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. CDC. COVID-19 (2020). Available at: https://www.cdc.gov/coronavirus/2019-ncov/index.html (Accessed September 1, 2022).
2. World Health Organization. Coronavirus disease (COVID-19) pandemic (2020). Available at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019. (Accessed August 31, 2022).
3. Morens DM, Breman JG, Calisher CH, Doherty PC, Hahn BH, Keusch GT, et al. The origin of COVID-19 and why it matters. Am J Trop Med Hyg. (2020) 103(3):955. doi: 10.4269/ajtmh.20-0849
4. World Health Organization. WHO coronavirus (COVID-19) dashboard (2023). Available at: https://covid19.who.int/ (Accessed February 14, 2023).
5. Ugandan Ministry of Health. COVID-19 response info hub (2023). Available at: https://covid19.gou.go.ug/statistics.html/ (Accessed February 14, 2023).
6. Olum R, Chekwech G, Wekha G, Nassozi DR, Bongomin F. Coronavirus disease-2019: knowledge, attitude, and practices of health care workers at Makerere University teaching hospitals, Uganda. Front Public Health. (2020) 8:181. doi: 10.3389/fpubh.2020.00181
7. Martinez-Alvarez M, Jarde A, Usuf E, Brotherton H, Bittaye M, Samateh AL, et al. COVID-19 pandemic in West Africa. Lancet Glob Heal. (2020) 8(5):e631–2. doi: 10.1016/S2214-109X(20)30123-6
8. World Health Organization. Cleaning and disinfection of environmental surfaces in the context of COVID-19 (2020). Available at: https://www.who.int/publications/i/item/cleaning-and-disinfection-of-environmental-surfaces-inthe-context-of-covid-19 (Accessed September 1, 2022).
9. Jones DL, Baluja MQ, Graham DW, Corbishley A, McDonald JE, Malham SK, et al. Shedding of SARS-CoV-2 in feces and urine and its potential role in person-to-person transmission and the environment-based spread of COVID-19. Sci Total Environ. (2020) 749:141364. doi: 10.1016/j.scitotenv.2020.141364
10. Ugandan Ministry of Health. Coronavirus (Pandemic). (2020). Available at: https://www.health.go.ug/covid/ (Accessed September 1, 2022).
11. Nabukeera M. Prevention and response to gender-based violence (GBV) during novel COVID-19 lock-down in Uganda. J Adult Prot. (2020) 23(2):116–33. doi: 10.1108/JAP-08-2020-0032
12. Sarki AM, Ezeh A, Stranges S. Uganda As a role model for pandemic containment in Africa. Am Public Health Assoc. (2020) 110:1800–2. doi: 10.2105/AJPH.2020.305948
13. CDC. How to protect yourself and others know how it spreads (2019). Available from: https://www.cdc.gov/coronavirus/2019-ncov/index.html (Accessed December 1, 2020).
14. Lone SA, Ahmad A. COVID-19 pandemic—an African perspective. Emerg Microbes Infect. (2020) 9(1):1300–8. doi: 10.1080/22221751.2020.1775132
15. Wilder-Smith A, Chiew CJ, Lee VJ. Can we contain the COVID-19 outbreak with the same measures as for SARS? Lancet Infect Dis. (2020) 20(5):e102–7. doi: 10.1016/S1473-3099(20)30129-8
16. Mfinanga SG, Mnyambwa NP, Minja DT, Ntinginya NE, Ngadaya E, Makani J, et al. Tanzania’s position on the COVID-19 pandemic. Lancet. (2021) 397(10284):1542–3. doi: 10.1016/S0140-6736(21)00678-4
17. Awobamise AO, Jarrar Y, Okiyi G. Evaluation of the Ugandan government’s communication strategies of the COVID-19 pandemic. Online J Commun Media Technol. (2021) 11(1):e202107. doi: 10.30935/ojcmt/10824
18. Lu G, Razum O, Jahn A, Zhang Y, Sutton B, Sridhar D, et al. COVID-19 in Germany and China: mitigation versus elimination strategy. Glob Health Action. (2021) 14(1):1875601. doi: 10.1080/16549716.2021.1875601
19. Amodan BO, Bulage L, Katana E, Ario AR, Fodjo JNS, Colebunders R, et al. Level and determinants of adherence to COVID-19 preventive measures in the first stage of the outbreak in Uganda. Int J Environ Res Public Health. (2020) 17(23):8810. doi: 10.3390/ijerph17238810
20. Ssebuufu R, Sikakulya FK, Mambo SB, Wasingya L, Nganza SK, Ibrahim B, et al. Knowledge, attitude, and self-reported practice toward measures for prevention of the spread of COVID-19 among Ugandans: a nationwide online cross-sectional survey. Front. Public Health (2020) 8:618731. doi: 10.3389/fpubh.2020.618731
21. Okello G, Izudi J, Teguzirigwa S, Kakinda A, Van Hal G. Findings of a cross-sectional survey on knowledge, attitudes, and practices about COVID-19 in Uganda: implications for public health prevention and control measures. Biomed Res Int. (2020) 2020:5917378. doi: 10.1155/2020/5917378
22. Kasozi KI, MacLeod E, Ssempijja F, Mahero MW, Matama K, Musoke GH, et al. Misconceptions on COVID-19 risk among Ugandan men: results from a rapid exploratory survey. Front Public Health. (2020) 8:416. doi: 10.3389/fpubh.2020.00416
23. Okaka FO, Omondi P. Knowledge, attitude, and practices (KAP) towards COVID-19 among older people living in informal settlements in Nairobi city, Kenya. Athens J Soc Sci. (2021) 9(4): doi: 10.30958/ajss.9-4-2
24. Li Z, Jin H, Chen W, Sun Z, Jing L, Zhao X, et al. Influencing factors of knowledge, attitude, and practice regarding medical nutrition therapy in patients with diabetes: a national cross-sectional study in urban China. J Diabetes Res. (2017) 2017:8948452. doi: 10.1155/2017/8948452
25. Mboya IB, Ngocho JS, Mgongo M, Samu LP, Pyuza JJ, Amour C, et al. Community engagement in COVID-19 prevention: experiences from Kilimanjaro region, northern Tanzania. Pan Afr Med J. (2020) 35(Suppl 2):146. doi: 10.11604/pamj.supp.2020.35.146.24473
26. Austrian K, Pinchoff J, Tidwell JB, White C, Abuya T, Kangwana B, et al. COVID-19 related knowledge, attitudes, practices and needs of households in informal settlements in Nairobi, Kenya (2020). SSRN [Preprint] (2020). Available at: http://dx.doi.org/10.2139/ssrn.3576785
27. Gender SS. Economic precarity and Uganda government’s COVID-19 response. African J Gov Dev. (2020) 9(1.1):287–308.
28. Usman IM, Ssempijja F, Ssebuufu R, Lemuel AM, Archibong VB, Ayikobua ET, et al. Community drivers affecting adherence to WHO guidelines against COVID-19 amongst rural Ugandan market vendors. Front Public Health. (2020) 8:340. doi: 10.3389/fpubh.2020.00340
29. Isah MB, Abdulsalam M, Bello A, Ibrahim MI, Usman A, Nasir A, et al. Coronavirus disease 2019 (COVID-19): A cross-sectional survey of the knowledge, attitudes, practices (KAP) and misconceptions in the general population of Katsina State, Nigeria. UJMR (2021) 6(1):24–37. doi: 10.47430/ujmr.2052.001
Keywords: attitude, adherence, COVID-19, prevention, measures, knowledge
Citation: Methodius T, Musewa A, Mirembe BB, Birungi D, Nitumusiima S, Naigaga I, Kabasa JD and Bazeyo W (2023) Knowledge, attitudes, and adherence relating to COVID-19 and its prevention measures in high-risk districts of Uganda in 2020. Front. Epidemiol. 3:1068097. doi: 10.3389/fepid.2023.1068097
Received: 12 October 2022; Accepted: 20 February 2023;
Published: 2 May 2023.
Edited by:
Ronald Olum, Makerere University, UgandaReviewed by:
Keneth Iceland Kasozi, University of Edinburgh, United Kingdom© 2023 Methodius, Musewa, Mirembe, Birungi, Nitumusiima, Naigaga, Kabasa and Bazeyo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Methodius Tubihemukama bWV0aG9kZGl1c0BnbWFpbC5jb20=
Specialty Section: This article was submitted to Infectious Disease Epidemiology, a section of the journal Frontiers in Epidemiology
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.