 Natalia Carasek1,2
Natalia Carasek1,2 Pauliana Lamounier1,2
Pauliana Lamounier1,2 Isabela Gomes Maldi1Marina Nahas Dafico Bernardes1
Isabela Gomes Maldi1Marina Nahas Dafico Bernardes1 Hugo Valter Lisboa Ramos1
Hugo Valter Lisboa Ramos1 Claudiney Cândido Costa1
Claudiney Cândido Costa1 Fayez Bahmad Jr.2*
Fayez Bahmad Jr.2*- 1Center for Rehabilitation and Readaptation Dr. Henrique Santillo (CRER), Goiânia, GO, Brazil
- 2Post Graduate Program of the Faculty of Health Sciences of the University of Brasília, Brasília, DF, Brazil
Objectives: The aim of the study was to assess whether hearing aids (HA) and cochlear implants (CI) bring benefits to cognition or mitigate cognitive decline in older adults.
Methods: This is a systematic literature review registered on the International Prospective Register of Systematic Reviews (PROSPERO) and based on the criteria recommended by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). The Population, Intervention, Comparison, Outcome, and Study type (PICOS) strategy was used to define eligibility. Studies that met the criteria were included in the qualitative synthesis. We assessed the risk of bias through the Joanna Briggs Institute Critical Appraisal Checklists.
Results: A total of 3,239 articles, found in eight databases, addressed the relationship between HA, CI, and cognition. We selected 30 experimental articles reporting measures of cognitive outcomes for older adults to include in the qualitative analysis. Of those, 23 studies reported a significant improvement in outcome and seven reported no significant change.
Conclusions: This systematic review indicates that CI and HA can bring benefits to cognition in older adults.
Systematic review registration: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42021273690
Introduction
Over 1.5 billion people are estimated to experience some decline in hearing capacity during their lifetime, of which at least 430 million will need care (1). Hearing impairment is the third most common chronic disease that affects older adults and is present in about 30% of individuals aged 65 years or more and up to 90% of those are older than 85 years (2). When a person has dementia associated with hearing loss, the communication difficulties generated by both conditions are intensified. This can lead to consequences such as increased self-perception of advanced age, social isolation, reduced participation in daily life activities, and lower quality of life (3). Another important domain of mental health is reported to be affected by hearing loss is cognitive functioning itself (4), establishing a possible cause–effect nexus between the two conditions.
Dementia affects around 46.8 million people worldwide, resulting in a very high estimated financial cost (5). Current drug treatments targeting neuropathological processes such as Alzheimer's disease offer limited benefit. Studies indicate that presbycusis precedes the onset of clinical dementia by 5 to 10 years, being a possible non-invasive biomarker that may offer an alternative way to modify the management of these patients (5, 6).
The pathological mechanisms for hearing loss leading to cognitive decline remain unclear, although several hypotheses have been proposed. One of the main potential explanations is based on the “deprivation hypothesis,” according to which hearing loss affects the anatomic and functional integrity of the brain, as suggested by several magnetic resonance imaging (MRI) studies (7). Patients with untreated hearing loss often develop atrophy of the temporal lobe (auditory cortex), whereas patients with dementia have diffuse brain atrophy. In addition, cerebral gliosis has been demonstrated in both diseases, which may contribute to their symptoms (8).
Other mechanisms for this relationship include the “cognitive load hypothesis,” in which cognitive impairment could be the result of devoting more resources to effortful sensory perception, to the detriment of other cognitive processes; the “information degradation hypothesis,” that is when impoverished perceptual input causes cognitive decline; and the “common cause hypothesis,” which assumes that both hearing loss and cognitive impairment are caused by common underlying processes (e.g., generalized effects of the aging brain or age-related cerebrovascular disease). Although presented as alternatives, the different hypotheses proposed may not be mutually exclusive and are likely to act in conjunction (7).
Accordingly, if hearing loss does contribute to cognitive impairment, it could be expected that auditory rehabilitation, through HA or CI, should mitigate cognitive decline (2). However, there are no consistent answers to this question in the scientific literature thus far. Thus, this review aimed to assess whether HA or CI benefits cognition or mitigates cognitive decline in older adults with hearing loss.
Methods
Design and registration
This study is a systematic review, conceived according to the Cochrane Handbook for Systematic Reviews of Interventions (9) and registered in PROSPERO (International Prospective Register of Systematic Reviews) under the ID number CRD42021273690 (10). We conducted the research following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) methodology (11).
Eligibility criteria
Inclusion criteria
We included studies following the PICOS strategy (anagram in which P denoted population; I, intervention (or exposure); C, comparison; O, outcome; and S, study type) (11). Our population of interest was “older adults with hearing loss,” the intervention “hearing rehabilitation through CI or HA,” and the comparison between “non-rehabilitated and rehabilitated patients;” the outcome was “improvement in cognition status,” and the study designs included randomized clinical trials, quasi-experimental studies, cohort studies, and systematic reviews with or without meta-analysis.
Exclusion criteria
(1) Age <50 years;
(2) Hearing rehabilitation through mechanisms other than CI or HA (e.g., stapedotomy, osteoanchored prosthesis, and ventilation tube);
(3) Studies in languages other than English, Portuguese, Spanish, or French.
Search strategy
The search used Medical Subject Headings (MeSH) vocabulary in English and its alternative descriptors. After three pilot trials in the PubMed database to assess the feasibility of the proposal, the keywords and the search strategy were defined using Boolean operators in the following search string: “(Cochlear Implantation OR Cochlear Implants OR Cochlear Implant OR Hearing Aids OR Correction of Hearing Impairment OR Audiologic Rehabilitation OR Correction of Hearing Loss OR Rehabilitation of Hearing Impaired) AND (Cognitive Impairment OR dementia OR Cognitive Dysfunction OR Cognitive Decline OR Cognitive Dysfunctions OR Cognitive Impairment OR Neurocognitive Disorders OR Neurocognitive Dysfunction OR Cognitive Dysfunctions OR Mental Deterioration OR Alzheimer's disease)”.
The ultimate search swept eight electronic databases: PubMed (MEDLINE), SciELO, Scopus, Lilacs, Embase, Epistemonikos, ClinicalTrials.gov, and Cochrane Library, from September to October 2021. A subsequent update was performed in March 2022 to ensure up-to-date information.
Data extraction
The initial search found 3,239 references, exported to EndNote Web (Clarivate Analytics) for reference management and deletion of duplicates. We excluded 772 duplicated articles, and the 2,467 unique references remaining were exported to the software Rayyan—Intelligent Systematic Review (https://www.rayyan.ai/) (12), allowing the selection process by two blinded reviewers (two different members of the research team, which gave their evaluations without knowledge of the other one's assessment). Initial evaluation of relevance was through the titles, then abstracts, and in the third stage, full-text analysis. In case of conflict, a third examiner decided whether or not to include the study.
We extracted data from the selected studies including authors, title, city/country of origin, year of publication, study design, number of participants, age, assessment method for hearing loss, cognitive domains evaluated, rehabilitation strategy, the time between assessments, and clinical outcomes.
Risk of bias
Studies that met all of the inclusion criteria and were ultimately selected by our peer review were then evaluated by a third party through the Joanna Briggs Institute (JBI) Critical Appraisal Checklists (13) for systematic reviews, randomized clinical trials, and quasi-experimental studies (non-randomized), to assess the risk of bias. In our search, most of the studies that evaluated patients exposed to HA or CI did not classify themselves methodologically into either “cohort studies” or “quasi-experimental studies.” On the contrary, they mostly only mentioned that they were longitudinal studies that evaluated patients with and without auditory rehabilitation through HA or CI. Because our study searched for rehabilitation and both HA and CI are types of interventions, the follow-up after intervening in a non-randomized way would be considered a quasi-experimental study. Therefore, those studies were all evaluated using the JBI Critical Appraisal Checklist for quasi-experimental studies. The details of the items present in the checklists can be found in Tables 5, 6, 7.
Ethical aspects
The methodological design in this study used secondary data analysis and was conducted by using a thorough process reinforcing research ethics in all of its stages and was approved by the Research Ethics Committee, in a national and unified database of research involving human beings CEP/CONEP, through the protocol number CAAE 36929420.1.0000.5082.
Results
Study selection
We selected 33 references, three of which corresponded to systematic review studies. No extra articles were found by searching the reference lists of included articles. The PRISMA flow diagram (Figure 1) details the article selection process.
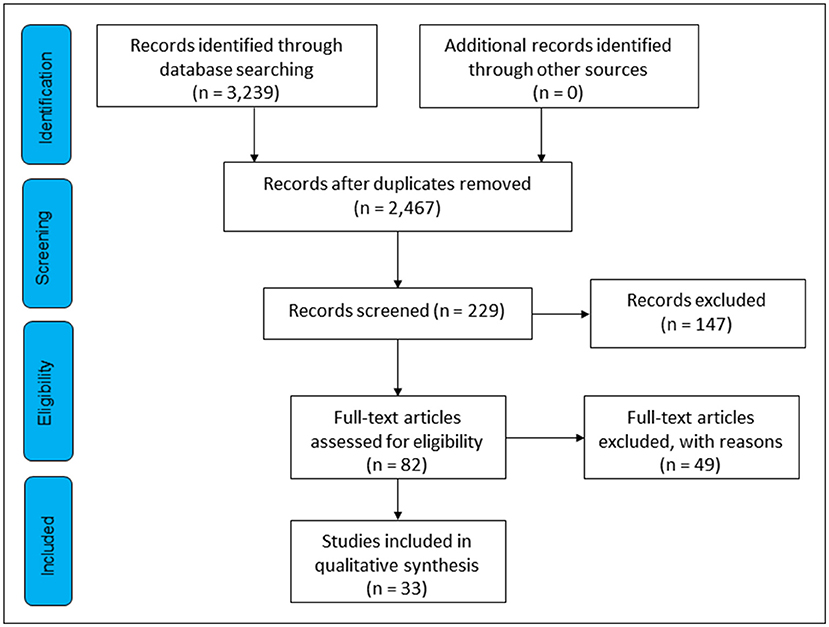
Figure 1. PRISMA flow diagram representing the selection process.
Characteristics and quality of the studies
The descriptive analysis of the studies was divided according to the type of study: “randomized clinical trials” (Table 1), “quasi-experimental and cohort” (Table 2), and “systematic reviews” (Table 3). The highlights of the cognitive outcome by intervention subgroup and study type are available in Table 4.
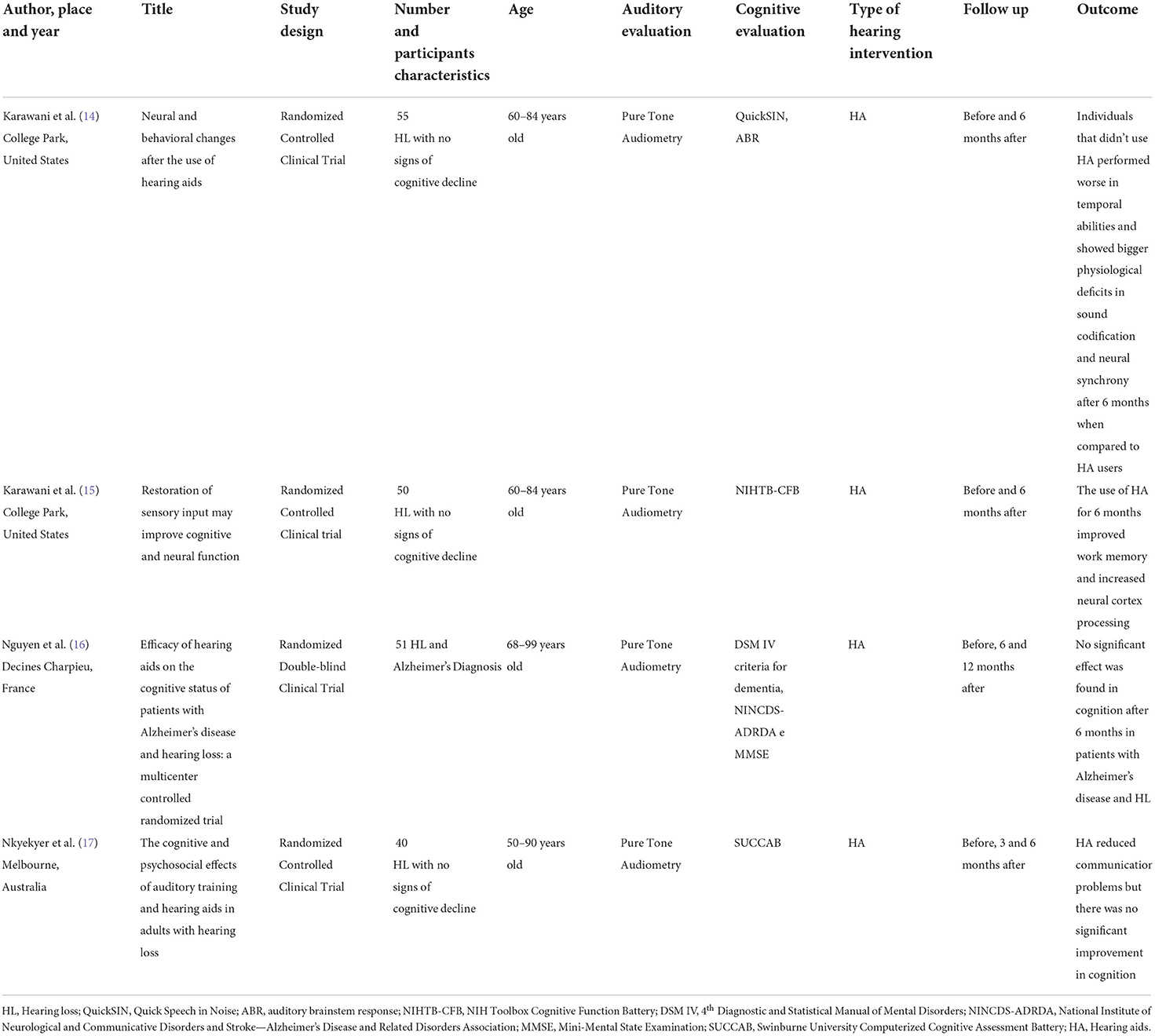
Table 1. Descriptive synthesis of the randomized clinical trials.
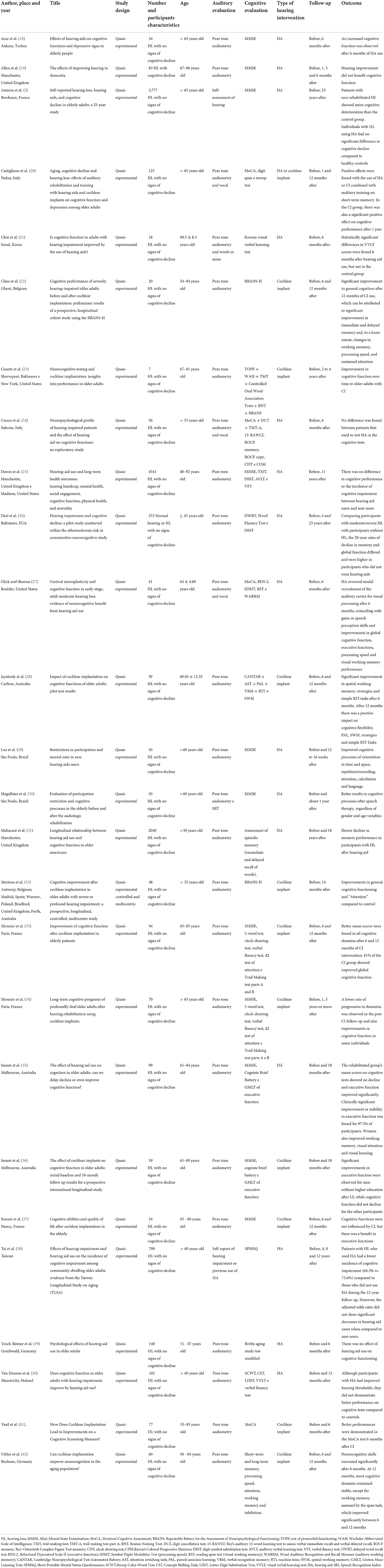
Table 2. Descriptive synthesis of the quasi-experimental studies.
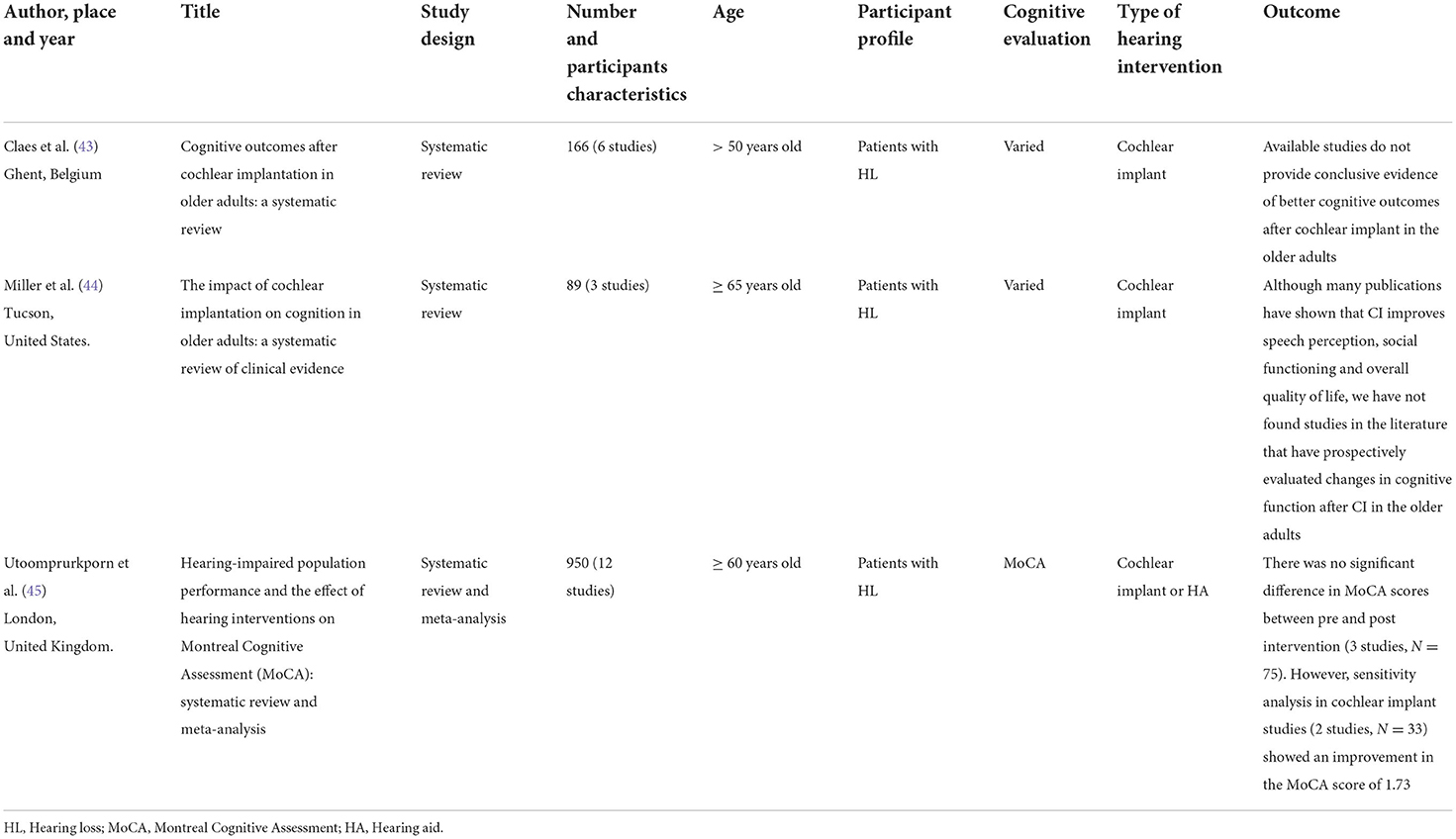
Table 3. Descriptive synthesis of the systematic review studies.
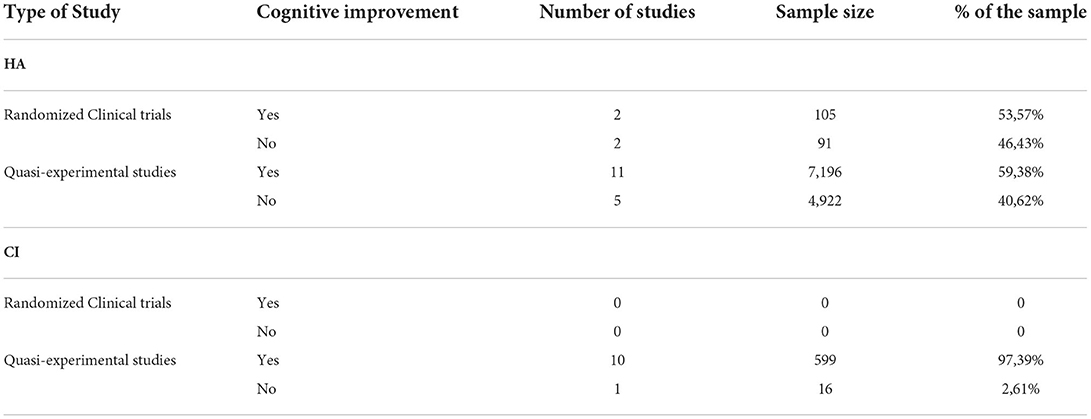
Table 4. Cognitive improvement.
A summary of the articles' quality regarding the JBI risk of bias assessment is given in Figures 2, 3. The majority of the included experimental studies obtained a percentage of adequacy to the criteria close to or above 70% and therefore considered, respectively, of high and moderate methodological quality. The mean score was 69.23% for randomized clinical trials and 77.88% for quasi-experimental studies. The complete measurement questions and answers in each kind of study are given in Tables 5, 6, 7.
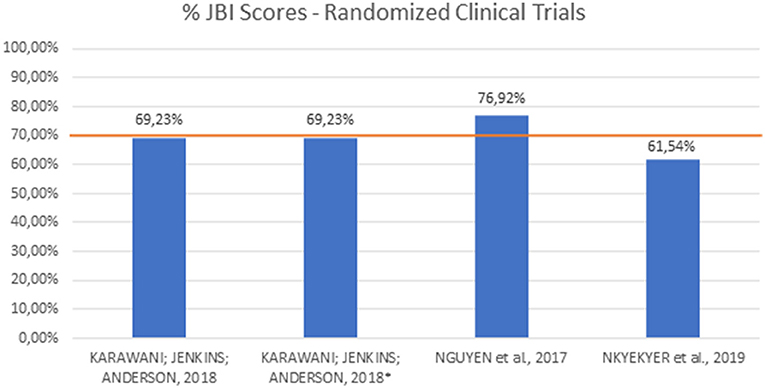
Figure 2. JBI scores for randomized clinical trials.
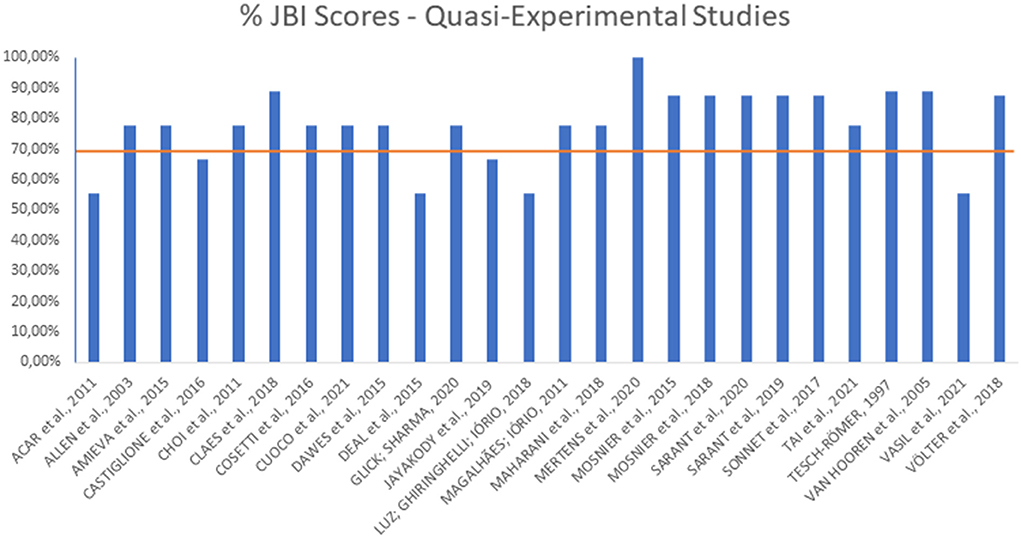
Figure 3. JBI scores for quasi-experimental studies.
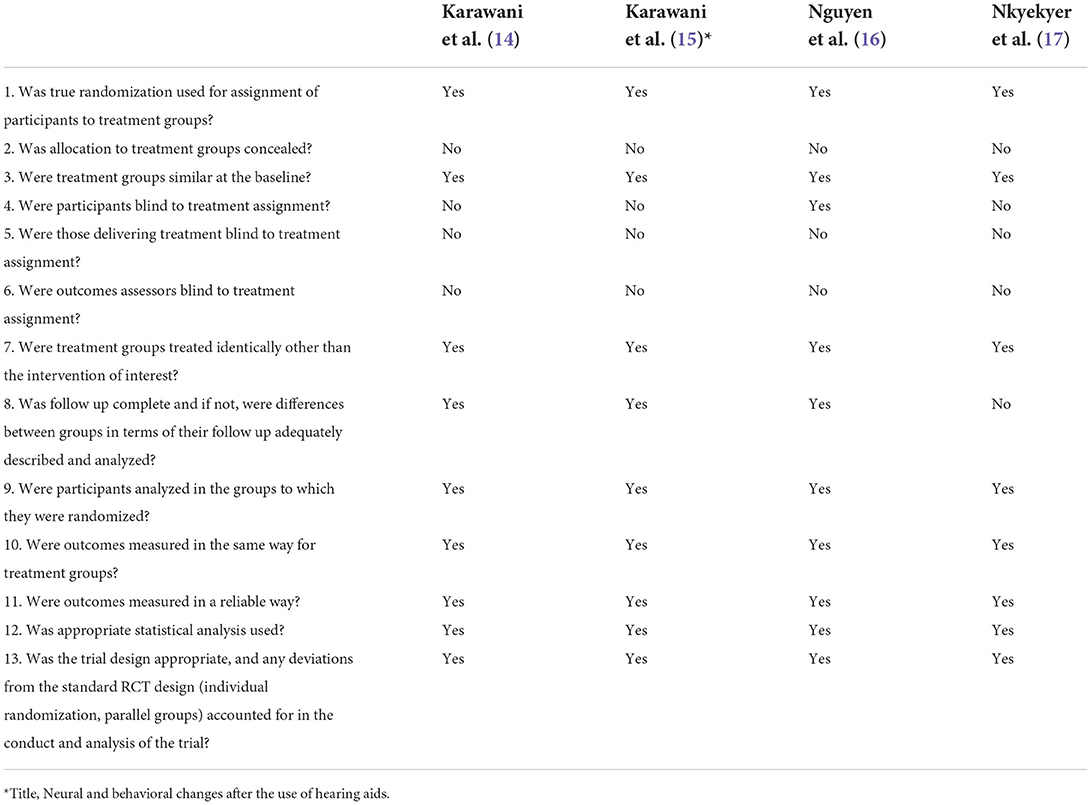
Table 5. JBI Checklist for randomized clinical trials.
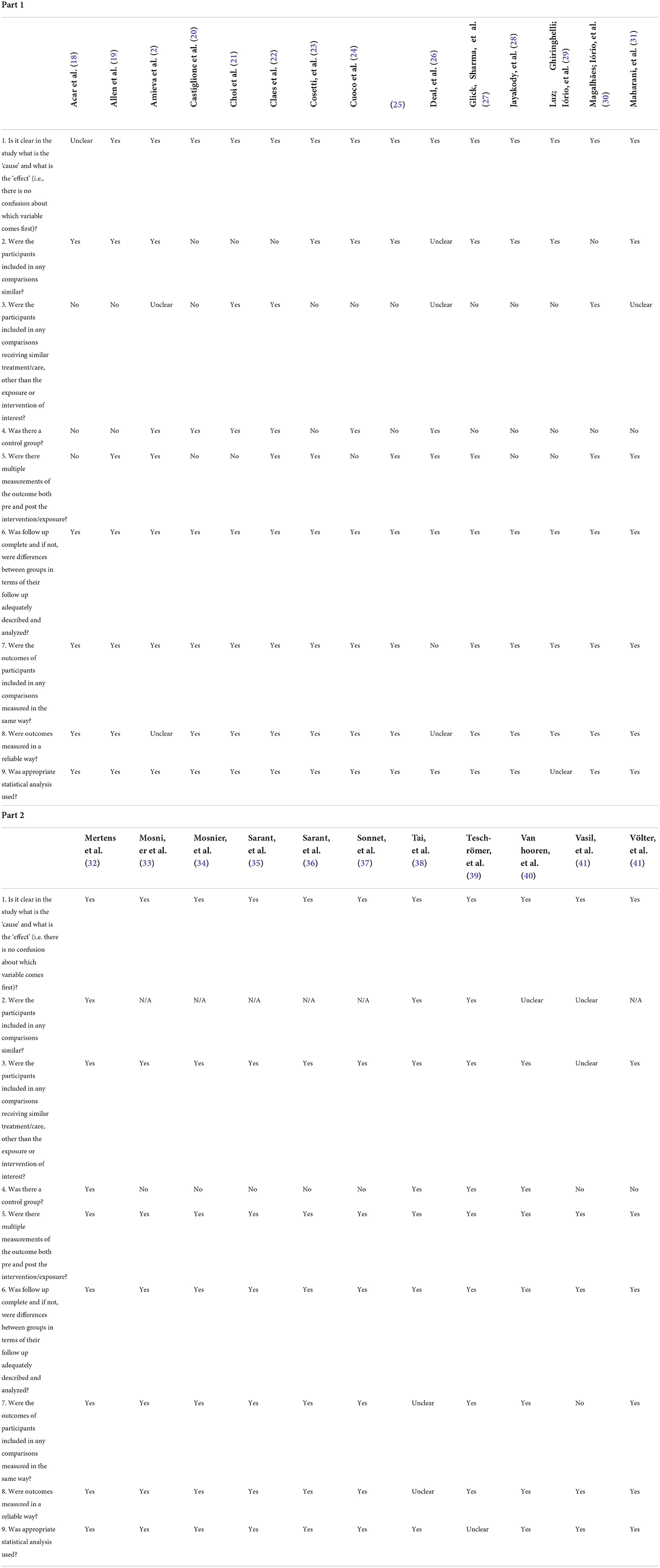
Table 6. JBI Checklist for quasi-experimental studies.
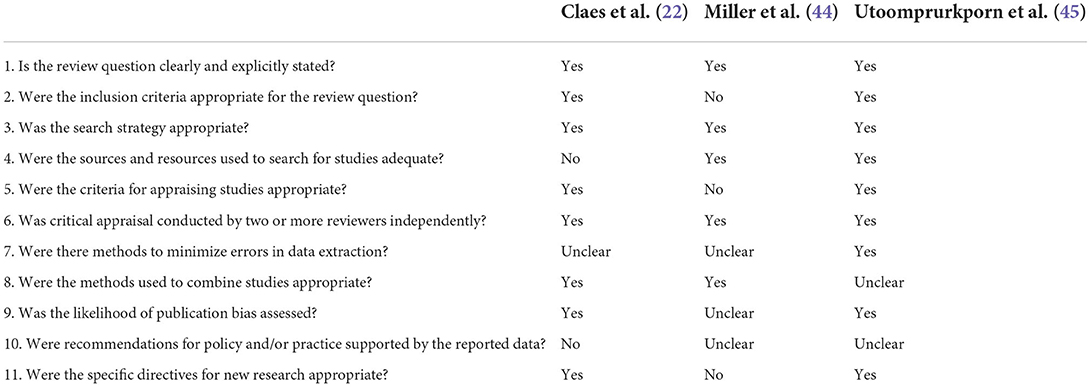
Table 7. JBI Checklist for systematic literature reviews.
Discussion
The global increase in life expectancy is one of the greatest health achievements in the last 150 years. However, age-related chronic conditions have also increased substantially, negatively affecting the independence and quality of life of older adults, contributing to a pessimistic picture of aging, in which presbycusis plays a leading role (4). Associated with the aging of the population, there is also a progressive increase in dementia and neurocognitive disorders (46). This research sought to systematically analyze the literature on the cognitive benefits of treating hearing loss, to determine the best management practices in this vulnerable and growing population.
Patient profile
Only two studies (16, 19) searched a population with hearing loss associated with signs of cognitive decline and/or diagnosis of Alzheimer's disease; two other studies (33, 34) included hearing loss patients with or without cognitive alterations. The remaining studies selected patients with hearing loss without signs of cognitive disease.
As for the age of the patients, most studies evaluated individuals over 60 years. In total, three studies (24, 32, 41) included participants aged 55 and older, and another three studies (17, 31, 39) included 50 or older patients. Because age acts as a risk factor for both presbycusis and dementia, a clear definition of age groups was fundamental to this review.
Main outcome
Type of intervention: Cochlear implant
In 10 of the articles, the intervention was based on cochlear implants, including a total of 615 CI recipients. Of these, only one study (37) found no difference in the cognitive functions after CI, although there was a benefit on executive functions (responsible for coordination and integration of the neurofunctional triad of learning: working memory, inhibitory control, and cognitive flexibility). This study evaluated patients prospectively, through the Mini-Mental State Examination (MMSE), before surgery, 6 months after, and 12 months after the CI, with a sample of 16 patients. All the other studies reported improvements in cognitive domains after CI.
Castiglione et al. (20) found that among patients undergoing CI, there was a statistically significant positive effect on cognitive performance after 1 year. The analysis of the Montreal Cognitive Assessment (MoCA) subtasks showed that the greatest increment after treatment and auditory training was in long-term memory, followed by tasks that assess visual–spatial and logical executive skills. We must point out that MoCA needs to be adapted with a visual on-screen presentation for patients with hearing loss, to avoid bias related to their hearing impairment. In this study, the authors reported that the test materials were adapted for individuals according to their hearing loss and hearing treatment program.
Claes et al. (22) conducted a quasi-experimental study in which they evaluated older patients with severe post-lingual hearing loss preoperatively, and 6 and 12 months after rehabilitation with CI, using the Repeatable Battery for the Assessment of Neuropsychological Functioning for Hearing impaired individuals (RBANS-H). This battery of cognitive tests is specific for the hearing impaired, a strength of this study. The authors found a significant improvement in general cognition after 12 months, which could be attributed to the increase in immediate and delayed memory and, to a lesser extent, also to changes in working memory, processing speed, and sustained attention. Even though the study reported preliminary results, with a sample of only 20 patients, it showed promising outcomes.
Mertens et al. (32) conducted a prospective, quasi-experimental controlled, and multicenter study with a similar approach, using the RBANS-H, with a larger sample, of 48 patients. The patients were evaluated before and 14 months after CI, with improvements in general cognitive functioning and in the “attention” subdomain, compared to the control group.
Similar results were found in two other studies (28, 29) that used two different complex batteries of neurocognitive assessments. Cosetti et al. (23) had a slightly longer follow-up than all other studies in this group, ranging from 2 to 4 years (mean 3.7 years). Jayakody et al. (28) described that the cognitive tests used were adapted for patients with hearing loss.
Overall, two publications from the same research group (33, 34) had the same design but changed in the sample size (94 and 70 participants, respectively) and in the follow-up time (12 months and 5 years, respectively). A multi-domain cognitive assessment showed that 6 months after CI, there were better mean scores in all cognitive domains, and after 12 months, 81% of the intervention group showed improvement in global cognitive function. After 5 years, a possible beneficial effect on cognition was also demonstrated. Of the patients with prior mild cognitive decline, 6% developed dementia, 61% remained stable, and 32% returned to normal cognition. Among patients with normal cognition, 32% developed mild cognitive decline and none developed dementia.
The study conducted by Sarant et al. (36) had a follow-up time of 18 months and a sample size of 59 patients. The authors observed relative stability and statistically significant clinical improvement in cognition after the intervention. Völter et al. (42) found that 6 months after CI, neurocognitive skills increased significantly and between 6 and 12 months, and most cognitive domains remained stable, except for working memory (assessed by the span task), which improved.
Type of intervention: AASI
Overall, 20 articles had HA as an intervention, including a total of 12,149 fitted patients. Of these, seven studies found no benefit for cognition in the use of hearing aids. (16, 17, 19, 24, 25, 39, 40). The remaining 13 studies (2, 14, 15, 18, 20, 21, 26, 27, 29–31, 35, 38), which accounted for approximately 60% of the patient sample, obtained positive responses after HA intervention.
For the definition of HL in the target population, the studies considered audiometric parameters, necessarily including pure-tone audiometry (PTA) thresholds, with the exception of two studies. Amieva et al. (2) and Tai et al. (38) defined hearing loss through patients' self-report, without presenting objective criteria, which could have generated an information bias of the instrument kind (in which the measurement instrument provides inadequate results).
One study (20) assessed simultaneously HA and CI. The data reported indicate a positive effect of hearing aids or CI combined with auditory training on short-term memory in both groups. Among patients who underwent CI surgery, auditory rehabilitation also resulted in a positive effect on cognitive performance after 1 year.
The only two groups that studied the outcome in populations of patients with signs of cognitive illness or a diagnosis of dementia (16, 19) found no significant effect of hearing aid use on cognition after 6 months of treatment, suggesting that hearing improvement did not benefit cognitive function in this specific profile of patients.
Follow-up time
A total of four studies maintained longer patient follow-ups (2, 25, 26, 31), all in the HA group; three of them (2, 26, 31) also had the largest sample sizes, adding up to 10,358 patients together. Amieva et al. (2) had the longest follow-up of 25 years; followed by Deal et al. (26), with 23 years; Maharani et al. (31), with 18 years; and Dawes et al. (25), with 11 years.
Some studies, notably those in which cognitive tests were repeated three times in 1 year (22, 28, 33, 34, 37, 42), could have been susceptible to “practice effect” bias, in which the performance improvement may be also due to a learning process of the patients.
Furthermore, in general, studies with CI had shorter follow-ups, which could be explained by the fact that this technology was not so available in the past and has achieved a greater reach in the last few years. However, as cognitive decline and dementia are both slowly progressive phenomena,4 we believe that there is still a lack of studies with longer follow-ups (of several years or decades), especially in the CI group.
Additional findings
Sensory deprivation in older adults has been associated with decreased daily life activity and social participation, quality of life losses, and depressive symptoms. There is also a negative impact on individuals' autonomy due to a greater dependence on the caregivers (47). In addition to cognition impacts, some of the studies in this systematic review assessed additional outcomes. There was a general trend of positive correlations, indicating improvements to these outcomes after hearing rehabilitation. However, one study (19) did not observe improvement in daily life activities, psychiatric symptoms, or caregiver burden after the intervention.
Acar et al. (18), Castiglione et al. (20), Jayakody et al. (28), Mosnier et al. (34) and Nkyekyer et al. (17) found a positive correlation between auditory intervention and the reduction of depression levels, using the Geriatric Depression Scale (GDS). These results agreed with other studies in the scientific literature (48–50).
It is argued that there is also an indirect link mediated by social isolation, reduced physical activity, and depressive symptoms, which would also act as risk factors for dementia (4). These additional outcomes become even more relevant in this discussion when the “cognitive load hypothesis” is introduced as an alternative explanation for the cognitive decline in older adults with HL. This hypothesis is based on the principle that cognitive impairment could also result from the dedication of large brain resources to sensory perception to the detriment of other cognitive processes. Although presented as alternatives, the different hypotheses may not be mutually exclusive and probably work together in etiopathogenesis (4).
The assessment of the quality of life (QoL) has gained ground in the latest research. A total of six CI studies also evaluated the QoL as an outcome, through questionnaires such as “World Health Organization–Quality of Life” (WHOQOL). Only one research found stable QoL scores from 1 to 7 years after CI (34). All the others encountered a positive and significant QoL effect (22, 35–37, 42).
In addition, four studies found improvements in the self-perception of HL and participation restriction after auditory rehabilitation (29, 30, 32, 39). Among the questionnaires for this assessment, the Hearing Handicap Inventory for the Elderly (HHIE) and its shortest version, the Hearing Handicap Inventory for the Elderly–Screening Version (HHIE-S), stand out. These forms are composed of two scales: social, assessing the impact of hearing loss on the activities performed by the individual, and emotional, measuring the emotional response to hearing loss (51).
Study designs
Of the 30 studies included in the descriptive synthesis of this systematic review, only four were randomized clinical trials (14–17), as shown in Table 1. Many of the authors (2, 20–22, 24, 26, 32, 38, 39), despite conducting prospective and controlled studies, opted not to randomize them, pledging the existence of ethical barriers preventing their course. Therefore, their studies were categorized as quasi-experimental. According to these authors, although a randomized clinical trial is always the preferred option in terms of study design, it would be unethical to deny treatment to a population with significant hearing loss, especially when the intervention in the discussion was HA, as they are considered to be innocuous. Thus, the control groups of these studies were formed by patients who did not want the intervention.
Comparison with other systematic reviews
A total of three systematic reviews (43–45) presented themes and methodology comparable to this study and were therefore included and critically assessed. Claes et al. (43) conducted a study that evaluated patients whose rehabilitation was performed with CI. As for the databases used, there was a limited search, which included only two databases: MEDLINE (PubMed) and Cochrane Library. They included six studies, with a sample size of 166 patients. Although five of the six studies reported improvement in cognition after CI, in a variety of cognitive domains, the results were exposed to various risks of bias and were therefore considered to be inconclusive by the authors themselves.
Miller et al. (44) selected only three studies that met the inclusion criteria for the review, according to the authors. However, the age range of the three studies also included younger patients, 14, 19, and 23 years, respectively. In addition, one of the three studies described neither the measurements used for cognitive outcome results nor the number of participants in the sample, according to the table described in the authors' results, which could impair the reliability of the study.
Utoomprurkporn et al. (45) conducted a systematic review with meta-analysis including studies that reported MoCA score results for individuals with HL before and after CI intervention. A total of three studies met the criteria, with a sample of 75 patients. No significant difference in MoCA scores between pre- and post-rehabilitation was found. However, sensitivity analysis of two studies (with a sample of 33 individuals) showed an improvement in the MoCA score of 1.73. Despite achieving greater heterogeneity by selecting a single cognitive evaluation test (MoCA), this study reduced the sample size and, consequently, its length. Currently, a large number of different cognitive assessment tests were used, and their inclusion may help the extrapolation of the results data.
Our systematic review included 30 articles, whose methodological quality was considered high and moderate, with a total sample size of 12,804 patients, enabling the conclusion that auditory rehabilitation with CI or HA has a positive impact on cognition, leading to improvements in cognitive parameters.
Conclusion
The results of this systematic review indicate that in older adults with hearing loss, the use of CI or HA can bring benefits to cognition and are therefore a promising strategy in the rehabilitation field, not only for hearing abilities but also for cognitive status improvement.
Data availability statement
The original contributions presented in the study are included in the article/supplementary materials, further inquiries can be directed to the corresponding author.
Author contributions
NC planned the methodological design and performed the search in all databases, was one of the two reviewers blinded through inclusion steps, and wrote the Discussion section, and thus has the first authorship. PL oversaw the blinding process and the methodological progress and helped with the theoretical basis of the discussion, and has the second authorship. IM was the second blinded reviewer and helped construct the result tables, and thus has the third authorship, MB was the third part judge in the decisions on whether to include articles when a consensus could not be reached by the two blind reviewers and thus has the fourth authorship. HR and CC contributed equally to the discussions and suggested improvements throughout the manuscript, and FB was the senior advisor who supervised and oriented the entire production process of this systematic review and thus has senior and corresponding authorship. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
2. Amieva H, Ouvrard C, Giulioli C, Meillon C, Rullier L, Dartigues JF. Self-reported hearing loss, hearing AIDS, and cognitive decline in elderly adults: a 25-year study. J Am Geriatr Soc. (2015) 63:2099–104. doi: 10.1111/jgs.13649
3. Gopinath B, Schneider J, McMahon CM, Teber E, Leeder SR, Mitchell P. Severity of age-related hearing loss is associated with impaired activities of daily living. Age Ageing. (2012) 41:195–200. doi: 10.1093/ageing/afr155
4. Amieva H, Ouvrard C. Does treating hearing loss in older adults improve cognitive outcomes? A review J Clin Med. (2020) 9:805. doi: 10.3390/jcm9030805
5. Loughrey DG, Kelly ME, Kelley GA, Brennan S, Lawlor BA. Association of age-related hearing loss with cognitive function, cognitive impairment, and dementia a systematic review and meta-analysis. JAMA Otolaryngol Head Neck Surg. (2018) 144:115–26. doi: 10.1001/jamaoto.2017.2513
6. Albers MW, Gilmore GC, Kaye J, Murphy C, Wingfield A, Bennett DA, et al. At the interface of sensory and motor dysfunctions and Alzheimer's disease. Alzheimer's Dement. (2015) 11:70–98. doi: 10.1016/j.jalz.2014.04.514
7. Lin FR, Yaffe K, Xia J, Xue QL, Harris TB, Purchase-Helzner E, et al. Hearing loss and cognitive decline in older adults. JAMA Intern Med. (2013) 173:293–9. doi: 10.1001/jamainternmed.2013.1868
8. di Stadio A, Ralli M, Roccamatisi D, Scarpa A, della Volpe A, Cassandro C, et al. Hearing loss and dementia: radiologic and biomolecular basis of their shared characteristics A systematic review. Neurol Sci. (2021) 42:579–88. doi: 10.1007/s10072-020-04948-8
9. Higggins J, Green S. Cochrane Handbook for Systematic Reviews of Interventions. Version 62 Cochrane. Oxfordshire, UK: The Cochrane Collaboration (2021).
10. Cascudo NCM, Lamounier P, de Araújo PIMP, Maldi IG, Bernardes MND. Hearing Rehabilitation and Cognitive Decline: A Systematic Review. PROSPERO 2021 CRD42021273690 Available Online at: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42021273690 (accessed December 6, 2021).
11. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ (Online). (2009) 339:332–6. doi: 10.1136/bmj.b2535
12. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid AK, et al. Rayyan—a web and mobile app for systematic reviews. Syst Rev. (2016) 5:1–9. doi: 10.1186/s13643-016-0384-4
13. Tufanaru C, et al. Chapter 3: Systematic reviews of effectiveness. In: Aromataris E, Munn Z editors. JBI Manual for Evidence Synthesis. JBI. (2020) 2127–33. Available online at: https://synthesismanual.jbi.global
14. Karawani H, Jenkins K, Anderson S. Neural and behavioral changes after the use of hearing aids. Clin Neurophysiol. (2018) 129:1254–67. doi: 10.1016/j.clinph.2018.03.024
15. Karawani H, Jenkins K, Anderson S. Restoration of sensory input may improve cognitive and neural function. Neuropsychologia. (2018) 114:203–13. doi: 10.1016/j.neuropsychologia.2018.04.041
16. Nguyen MF, Bonnefoy M, Adrait A, Gueugnon M, Petitot C, Collet L, et al. Efficacy of hearing AIDS on the cognitive status of patients with alzheimer's disease and hearing loss: a multicenter controlled randomized trial. J Alzheimer's Dis. (2017) 58:123–37. doi: 10.3233/JAD-160793
17. Nkyekyer J, Meyer D, Pipingas A, Reed NS. The cognitive and psychosocial effects of auditory training and hearing aids in adults with hearing loss. Clin Interv Aging. (2019) 14:123–35. doi: 10.2147/CIA.S183905
18. Acar B, Yurekli MF, Babademez MA, Karabulut H, Karasen RM. Effects of hearing aids on cognitive functions and depressive signs in elderly people. Arch Gerontol Geriatr. (2011) 52:250–2. doi: 10.1016/j.archger.2010.04.013
19. Allen NH, Burns A, Newton V, Hickson F, Ramsden R, Rogers J, et al. The effects of improving hearing in dementia [Internet]. Available online at: https://academic.oup.com/ageing/article/32/2/189/29059 (accessed April 18, 2022).
20. Castiglione A, Benatti A, Velardita C, Favaro D, Padoan E, Severi D, et al. Aging, cognitive decline and hearing loss: effects of auditory rehabilitation and training with hearing aids and cochlear implants on cognitive function and depression among older adults. Audiol Neurootol. (2016) (21 Suppl. 1):21–8. doi: 10.1159/000448350
21. Choi AY, Shim HJ, Lee SH, Yoon SW, Joo EJ. Is cognitive function in adults with hearing impairment improved by the use of hearing aids? Clin Exp Otorhinolaryngol. (2011) 4:72–6. doi: 10.3342/ceo.2011.4.2.72
22. Claes AJ, van de Heyning P, Gilles A, van Rompaey V, Mertens G. Cognitive performance of severely hearing-impaired older adults before and after cochlear implantation: preliminary results of a prospective, longitudinal cohort study using the RBANS-H. Otol Neurotol. (2018) 39:E765–73. doi: 10.1097/MAO.0000000000001936
23. Cosetti MK, Pinkston JB, Flores JM, Friedmann DR, Jones CB, Roland JT, et al. Neurocognitive testing and cochlear implantation: insights into performance in older adults. Clin Interv Aging. (2016) 11:603–13. doi: 10.2147/CIA.S100255
24. Cuoco S, Cappiello A, Scarpa A, Troisi D, Autuori M, Ponticorvo S, et al. Neuropsychological profile of hearing-impaired patients and the effect of hearing aid on cognitive functions: an exploratory study. Sci Rep. (2021) 11:1–9. doi: 10.1038/s41598-021-88487-y
25. Dawes P, Cruickshanks KJ, Fischer ME, Klein BEK, Klein R, Nondahl DM. Hearing-aid use and long-term health outcomes: hearing handicap, mental health, social engagement, cognitive function, physical health, and mortality. Int J Audiol. (2015) 54:838–44. doi: 10.3109/14992027.2015.1059503
26. Deal JA, Sharrett AR, Albert MS, Coresh J, Mosley TH, Knopman D, et al. Hearing impairment and cognitive decline: a pilot study conducted within the atherosclerosis risk in communities Neurocognitive Study. Am J Epidemiol. (2015) 181:680–90. doi: 10.1093/aje/kwu333
27. Glick HA, Sharma A. Cortical neuroplasticity and cognitive function in early-stage, mild-moderate hearing loss: evidence of neurocognitive benefit from hearing aid use. Front Neurosci. (2020) 14:93. doi: 10.3389/fnins.2020.00093
28. Jayakody DMP, Friedland PL, Nel E, Martins RN, Atlas MD, Sohrabi HR. Impact of cochlear implantation on cognitive functions of older adults: pilot test results. Otol Neurotol. (2017) 38:e 289–95. doi: 10.1097/MAO.0000000000001502
29. Luz VB da, Ghiringhelli R, Iório MCM. Restrições de participação e estado mental: estudo em novos usuários de próteses auditivas. Audiol Commun Res. (2018) 23:e1884. doi: 10.1590/2317-6431-2017-1884
30. Magalhães R, Iório MCM. Avaliação da restrição de participação e de processos cognitivos em idosos antes e após intervenção fonoaudiológica. J Soc Bras Fonoaudiol. (2011) 23:51–5. doi: 10.1590/S2179-64912011000100012
31. Maharani A, Dawes P, Nazroo J, Tampubolon G, Pendleton N, Bertelsen G, et al. Longitudinal relationship between hearing aid use and cognitive function in older Americans. J Am Geriatr Soc. (2018) 66:1130–6. doi: 10.1111/jgs.15363
32. Mertens G, Andries E, Claes AJ, Topsakal V, van de Heyning P, van Rompaey V, et al. Cognitive improvement after cochlear implantation in older adults with severe or profound hearing impairment: a prospective, longitudinal, controlled, multicenter study. Ear Hear. (2020) 42:606–14. doi: 10.1097/AUD.0000000000000962
33. Mosnier I, Bebear JP, Marx M, Fraysse B, Truy E, Lina-Granade G, et al. Improvement of cognitive function after cochlear implantation in elderly patients. JAMA Otolaryngol Head Neck Surg. (2015) 141:442–50. doi: 10.1001/jamaoto.2015.129
34. Mosnier I, Vanier A, Bonnard D, Lina-Granade G, Truy E, Bordure P, et al. Long-term cognitive prognosis of profoundly deaf older adults after hearing rehabilitation using cochlear implants. J Am Geriatr Soc. (2018) 66:1553–61. doi: 10.1111/jgs.15445
35. Sarant J, Harris D, Busby P, Maruff P, Schembri A, Lemke U, et al. The effect of hearing aid use on cognition in older adults: can we delay decline or even improve cognitive function? J Clin Med. (2020) 9:254. doi: 10.3390/jcm9010254
36. Sarant J, Harris D, Busby P, Maruff P, Schembri A, Dowell R, et al. The effect of cochlear implants on cognitive function in older adults: Initial baseline and 18-month follow up results for a prospective international longitudinal study. Front Genet. (2019) 10:789. doi: 10.3389/fnins.2019.00789
37. Sonnet MH, Montaut-Verient B, Niemier JY, Hoen M, Ribeyre L, Parietti-Winkler C. Cognitive abilities and quality of life after cochlear implantation in the elderly. Otol Neurotol. (2017) 38:e296–301. doi: 10.1097/MAO.0000000000001503
38. Tai CJ, Tseng TG, Hsiao YH, Kuo TA, Huang CY, Yang YH, et al. Effects of hearing impairment and hearing aid use on the incidence of cognitive impairment among community-dwelling older adults: evidence from the Taiwan Longitudinal Study on Aging (TLSA). BMC Geriatr. (2021) 21. doi: 10.1186/s12877-021-02012-4
39. Tesch-Romer C. Psychological effects of hearing aid use in older adults. JGerontol B Psychol Sci Soc Sci. (1997).52:P127–38. doi: 10.1093/geronb/52b.3.p17
40. Van Hooren SAH, Anteunis LJC, Valentijn SAM, Bosma H, Ponds RWHM, Jolles J, et al. Does cognitive function in older adults with hearing impairment improve by hearing aid use? Int J Audiol. (2005) 44:265–71. doi: 10.1080/14992020500060370
41. Vasil KJ, Ray C, Lewis J, Stefancin E, et al. How does cochlear implantation lead to improvements on a cognitive screening measure? J Speech Lang Hear Res. (2021) 64:1053–5. doi: 10.1044/2020_JSLHR-20-00195
42. Völter C, Götze L, Dazert S, Falkenstein M, Thomas JP. Can cochlear implantation improve neurocognition in the aging population? Clin Interventions Aging. (2018) 13:701–12. doi: 10.2147/CIA.S160517
43. Claes AJ, van de Heyning P, Gilles A, van Rompaey V, Mertens G. Cognitive outcomes after cochlear implantation in older adults: a systematic review. Cochler Implants Int. (2018) 19:239–54. doi: 10.1080/14670100.2018.1484328
44. Miller G, Miller C, Marrone N, Howe C, Fain M, Jacob A. The impact of cochlear implantation on cognition in older adults: A systematic review of clinical evidence. BMC Geriatr. (2015) 15. doi: 10.1186/s12877-015-0014-3
45. Utoomprurkporn N, Woodall K, Stott J, Costafreda SG, Bamiou DE. Hearing-impaired population performance and the effect of hearing interventions on montreal cognitive assessment (MoCA): systematic review and meta-analysis. Int J Geriatr Psychiatr. (2020) 35:962–71. doi: 10.1002/gps.5354
46. Mamo SK, Reed NS, Price C, Occhipinti D, Pletnikova A, Lin FR, et al. Hearing loss treatment in older adults with cognitive impairment: a systematic review. J Spech Lang Heart Res. (2018) 61:2589–603. doi: 10.1044/2018_JSLHR-H-18-0077
47. Roets-Merken LM, Draskovic I, Zuidema SU, Van Erp WS, Graff MJL, Kempen GIJM, et al. Effectiveness of rehabilitation interventions in improving emotional and functional status in hearing or visually impaired older adults: A systematic review with meta-analyses. Clin Rehab. (2015) 29:107–19. doi: 10.1177/0269215514542639
48. Choi JS, Betz J, Li L, Blake CR, Sung YK, Contrera KJ, et al. Association of using hearing aids or cochlear implants with changes in depressive symptoms in older adults. JAMA Otol Head Neck Surg. (2016) 142:652–7. doi: 10.1001/jamaoto.2016.0700
49. Olze H, Gräbel S, Förster U, Zirke N, Huhnd LE, Haupt H, et al. Elderly patients benefit from cochlear implantation regarding auditory rehabilitation, quality of life, tinnitus, and stress. Laryngoscope. (2012) 122:196–203. doi: 10.1002/lary.22356
50. Contrera KJ, Sung YK, Betz J, Li L, Lin FR. Change in loneliness after intervention with cochlear implants or hearing aids. Laryngoscope. (2017) 127:1885–9. doi: 10.1002/lary.26424
Keywords: cochlear implants, hearing aids, correction of hearing impairment, cognition, cognition disorders
Citation: Carasek N, Lamounier P, Maldi IG, Bernardes MND, Ramos HVL, Costa CC and Bahmad F Jr (2022) Is there benefit from the use of cochlear implants and hearing aids in cognition for older adults? A systematic review. Front. Epidemiol. 2:934750. doi: 10.3389/fepid.2022.934750
Received: 03 May 2022; Accepted: 20 July 2022;
Published: 30 August 2022.
Edited by:
Norma De Oliveira Penido, Federal University of São Paulo, BrazilReviewed by:
Danielle Powell, Johns Hopkins University, United StatesMohammad Rezaei, Hamadan University of Medical Sciences, Iran
Copyright © 2022 Carasek, Lamounier, Maldi, Bernardes, Ramos, Costa and Bahmad. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fayez Bahmad Jr., ZmF5ZXpianImI3gwMDA0MDtnbWFpbC5jb20=