
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Environ. Sci. , 18 October 2024
Sec. Environmental Systems Engineering
Volume 12 - 2024 | https://doi.org/10.3389/fenvs.2024.1415604
This article is part of the Research Topic Environmental Impacts of Materials and their Life Cycle View all 9 articles
 Constantin Keul1
Constantin Keul1 Sebastian Spierling1
Sebastian Spierling1 Venkateshwaran Venkatachalam1*
Venkateshwaran Venkatachalam1* Hans-Josef Endres1
Hans-Josef Endres1 Leonie Barner2Kerstin Wyssusek3,4
Leonie Barner2Kerstin Wyssusek3,4Plastics are a versatile material group with many applications in the healthcare sector. Clinicians, particularly in the operating rooms, have become increasingly dependent on single-use instruments and consumables typically packaged in Polyethylene Terephthalate (PET) resulting in significant amounts of PET waste. In this study, a life cycle assessment (LCA) methodology based on ISO 14040/44 is conducted to assess the environmental impacts of existing and potential future end-of-life options for PET anaesthesia and surgical instrument packaging waste in an Australian hospital context. The results show the reduction potential of environmental impacts by recycling of PET waste via direct collection or in Materials Recovery Facility (MRF) in Australia, Indonesia and New Zealand. When replacing end-of-life options such as landfill or incineration with recycling, a reduction of 88% of total Climate Change (CC) impact can be seen. Furthermore, there is a reduction in environmental impacts across other impact categories through this change. Even if the recyclate quality (up to 30%) was reduced, there is a significant reduction in the environmental impacts. The transition of end-of-life options to recycling offers the potential for reduction of emissions and enables a circular economy for plastics. Furthermore, based on the results of LCA, opportunities and challenges of circular economy pathways in health industry are identified and discussed in this study.
Increase in population and extended life expectancy, the quantity and size of healthcare facilities, and the use of disposable medical products have all contributed to a global increase in the amount of healthcare waste (HCW) that is generated annually (Kwakye et al., 2011). The health sector is responsible for 4.6% of global greenhouse gas (GHG) emissions while healthcare facilities are the second leading contributor of waste in the United States of America (USA) (MacNeill et al., 2020).
Of all healthcare waste in the USA, 20%–33% is generated in the operating rooms (OR) (Kwakye et al., 2011; Kagoma et al., 2012). Waste management in healthcare is complex, dependent on local and state regulations and frequently faces many obstacles. A review of operating room waste management initiatives highlighted the challenges and misconceptions of introducing recycling strategies in hospitals in general and ORs in particular (Wyssusek et al., 2019; Wyssusek et al., 2020). Clinicians, particularly in ORs have become increasingly dependent on single-use instruments and consumables typically packaged in Polyethylene Terephthalate (PET). PET is a transparent, durable, and lightweight plastic, impermeable to microorganisms and therefore used for the storage of medical equipment in ORs to ensure sterility (Wyssusek et al., 2020).
Previous analyses in this field have mainly focused on the distinction between the sterilization (i.e., reuse) of materials in the operating room or the assessment of various surgical procedures in general. However, these analyses primarily focus on different anaesthesia practices used and the current waste disposal practices (Thiel et al., 2015; Wu and Cerceo, 2021; Friedericy et al., 2022). A study by Ivanović et al. analyzed the material flow of single-use medical products and packaging in a German hospital, revealing that 619 g of consumables were used per patient daily, 86% of which were plastics (Ivanović et al., 2022). Personal protective equipment and incontinence products accounted for the majority of plastic usage, particularly polypropylene and latex. The results aim to identify ways to reduce plastic use in hospitals. Another study by Liu et al. developed a model to assess the economic and environmental benefits of recycling medical plastic waste in China (Liu et al., 2022). The findings show that each ton of recycled medical plastic waste generates 2,708.6 yuan in economic benefits, while reducing dioxin and carbon dioxide emissions during the recycling process (Liu et al., 2022). Scenario simulations suggest that recycling benefits and emission reduction potential increase annually, while CO₂ emissions follow an inverted “U” pattern (Liu et al., 2022). A study by Mushtaq et al. evaluates the environmental impacts of hospital waste management in urban areas of Pakistan using a life cycle assessment (Mushtaq et al., 2022). Two scenarios were compared: the current management and an integrated approach with waste segregation and recycling. Scenario B showed lower greenhouse gas emissions and could save 37,756.44 kg of CO2-equivalents annually, making waste management more sustainable. Since such a comparison of different end-of-life options for PET waste has not yet been identified in any of the studies, this approach has been adopted for the analysis conducted here.
An Australian OR recycling case study estimated that 40% of the operating room plastic is PET (McGain et al., 2015). Data from our own tertiary hospital PET waste audit at the Royal Brisbane and Women’s Hospital revealed that over 12 months the total volume of PET waste recovered from our ORs to be approximately 1,700 kg (Wyssusek et al., 2020). PET was previously not recycled at our facility and was discarded to landfill. Degradation rates for PET are estimated to be up to 500 years depending on environmental circumstances (Chamas et al., 2020).
Anesthesia and surgical procedures significantly contribute to PET waste accumulated in healthcare - A problem that will most likely increase over the next decades as concerns about infectious diseases, aging and growing population will increase demand. Common items from anesthesia practice packaged in PET are, central venous line kits, arterial line kits, rapid infusion devices, cell salvage equipment, laryngeal masks, epidural and spinal packs. A variety of single use surgical instruments such as staplers, cutters, trocars, and closure devices are typically packaged in PET. These items are predominantly prepared for clinical use before any patient contact which makes them an ideal target for separation from other recyclable OR waste. With a steadily increasing demand of plastic products (Plastics Europe, 2023) and the current linearity of the plastic economy (take-make-use and dispose without recovering the materials after use) (Geyer et al., 2017) the development of a circular economy for plastics becomes more and more important (Ellen Macarthur Foundation, 2024). McGain et al. highlighted how different clinical choices for anesthesia practice may impact GHG emissions in their recent life cycle assessment (McGain et al., 2021). With an increase in the use of such single-use plastic products in the healthcare sector and a significant amount of them disposed in landfills and not recycled, it is important to highlight and quantify the negative environmental impacts of not recovering these plastic wastes after use. This will help policymakers and other stakeholders across the plastic value chain to consider these impacts when designing such products and develop adequate recycling and incineration infrastructure to recover them after use.
An LCA is an internationally standardized method to quantify the potential environmental impacts of a product system. Therefore, the goal of this study is to conduct an LCA based on ISO 14040/44 (DIN EN ISO 14040:2021-02, 2021; DIN EN ISO 14044:2021-02, 2021) for the current end-of-life options of single-use anaesthetic and surgical instrument PET packaging waste from Royal Brisbane Women’s Hospital. There have been several LCA studies that have been conducted in the past that compare the environmental performance between single-use (disposable) and reusable instruments on a product level in the health sector like dental burs (Unger and Landis, 2014), laryngoscopes (Sherman et al., 2018), instruments used in delivery rooms (van Zanten et al., 2024) and spinal fusion surgeries (Leiden et al., 2020). However, this study focusses not on the product and its reusability unlike previous studies, but on the different end of life pathways of such products after use in an Australian context. The standard scenarios of incineration and landfill are examined, and they are compared to various recycling pathways. Mechanical recycling in Brisbane, Jakarta, and Wellington is also compared. The recycling process is carried out using both single-grade PET waste and mixed PET waste, which is initially sorted in the Material Recovery Facility (MRF). Subsequently, the results of this comprehensive analysis are presented in impact categories such as Acidification, Climate Change, Eutrophication, and Resource Use, Fossils. Additional impact categories are also presented in the Supplementary Information (SI). To show the impacts on Australian level, the results are upscaled. Furthermore, based on the results of LCA, opportunities and challenges of circular economy pathways are identified. Transformation of the healthcare industry to a circular economy will assist in the provision of high value healthcare in a low emissions future (Australian Government Department of Health and Aged Care, 2023).
The recycling of hospital PET waste appears to be a promising alternative to conventional disposal methods. The scenarios considered in this study primarily differ in the pathways - at source collection or MRF - and the location where the recycling takes place, i.e., Australia, New Zealand, and Indonesia. The recycling processes themselves differ in certain aspects such as transport distance and use of energy mix. The recycling scenarios are modeled using both single-grade PET waste and mixed PET waste, which is first sorted in the MRF. The end product of these processes is recycled PET granules. Additionally, a comparison is made with landfill and incineration, both of which take place in Australia. An overview of the different scenarios is shown below in Figure 1. A detailed description is also provided in the SI (A1).
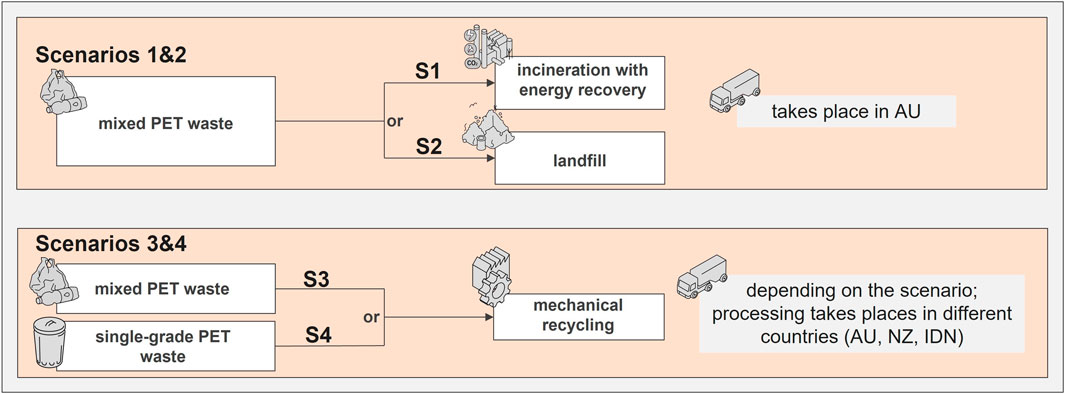
Figure 1. Different waste stream scenarios for the disposal of mixed or single-grade plastic waste.
To assess the environmental impacts of different end-of-life scenarios for PET waste from operating rooms the life cycle assessment methodology based on ISO 14040 and ISO 14044 is applied to quantify the potential environmental impacts of the end-of-life scenarios (DIN EN ISO 14040:2021-02, 2021; DIN EN ISO 14044:2021-02, 2021).
The main goal of the study is to compare the potential environmental impacts of different end-of-life scenarios for the treatment of hospital PET waste. The resulting PET granules can subsequently be used for further processing. Therefore, it serves as an intermediate product. The LCA is conducted on a gate to grave (collection of the wastes till the processing of polymer granulates or energy recovery in the case of incineration) basis. Various sorting and material qualities are assessed and the uncertainties in these process parameters are addressed in a sensitivity analysis and an additional uncertainty analysis for transport distances. The declared unit (DU) for assessment is defined as the treatment of 1 kg of PET waste (at source collection and MRF) by different EoL options (mechanical recycling, landfill and incineration) in Australia, New Zealand, or Indonesia.
The comparative LCA is constructed with a combination of secondary data from the scientific literature and inventory datasets from commercial life cycle inventory (LCI) databases. The transport distance for the collection and recovery of the single-grade and mixed plastic waste in different countries are calculated using the “EcoTransIT” tool (EcoTransIT World, 2020). A detailed breakdown of the different datasets used in the study is shown in the SI (A3).
A list of the used data sets can be found in the SI. The evaluation of the individual scenarios is conducted by modeling the product system and End-of-Life scenarios with the help of the LCA software. A detailed depiction of the system boundaries can be derived from the comprehensive process flow diagrams in the SI. For both recycling pathways, the production steps during recycling are identical, except for the preceding sorting process. In scenarios 1-3, a mixed plastic stream is considered, which is sorted first. The waste stream from scenarios 1 and 2 is sent to incineration and landfill respectively. The non-usable waste from scenario 3 is sent to landfill. In the scenario 4, a pure PET waste stream is assumed, with only a 5.9% misplacement rate. The misplacements are subsequently sorted and divided into usable PET or waste, which also goes to landfill. The modeling of the product system and the calculation of potential environmental impacts are conducted using the LCA for Experts (formerly known as GaBi) software by Sphera Solutions GmbH (version 10.7.0.183) (Sphera, 2023a). The used LCI datasets were taken from the Sphera Managed LCA Content database (Sphera, 2023b).
The impact assessment methodology chosen for this study is the Environmental Footprint 3.0 (Zampori and Pant, 2019). All impact category indicators within this method are analyzed in the study. The following impact categories have been analyzed in detail: Acidification Potential (AP), Climate Change (CC), Eutrophication Potential (EP), and Resource use, fossils (RU). Results for the additional impact categories are provided in the SI (A4).
For a better understanding, the individual scenarios and their abbreviations are described below. The baseline scenarios are scenarios S1 and S2. In scenario S1, the waste is incinerated in Brisbane, Australia and in scenario S2 it is landfilled in Brisbane, Australia. Scenario S3 describes a possible recycling route for the surgical waste. Here, the mechanical recycling of a mixed waste stream is considered, which has to be sorted first. This scenario is examined in the geographical regions of Brisbane, Australia (S3a), Jakarta, Indonesia (S3b) and Wellington, New Zealand (S3b). Scenario 4 also depicts a mechanical recycling option in which, in contrast to scenario 3, single-grade PET waste is recycled. Here, too, the geographical regions Brisbane, Australia (S4a), Jakarta, Indonesia (S4b) and Wellington, New Zealand (S4c) are examined.
Figure 2 presents the percentage share of each scenario in the overall impact of all scenarios. The sum of all impacts from individual scenarios is assumed as the totality. The negative percentages are derived from the assigned credits for respective treatment processes. To enable a direct comparison of different EoL-options, it is important to consider potential products of the different options. To do so, a credit for avoided primary material production is considered for resulting recyclates. The recyclate qualities are 90% for scenario 3% and 100% for scenario 4. Credits are also considered due to the incineration of waste for resulting energy. Particularly noticeable is also that recycling processes in scenarios S3a-c and S4 a-c have a negative impact in almost all impact categories.
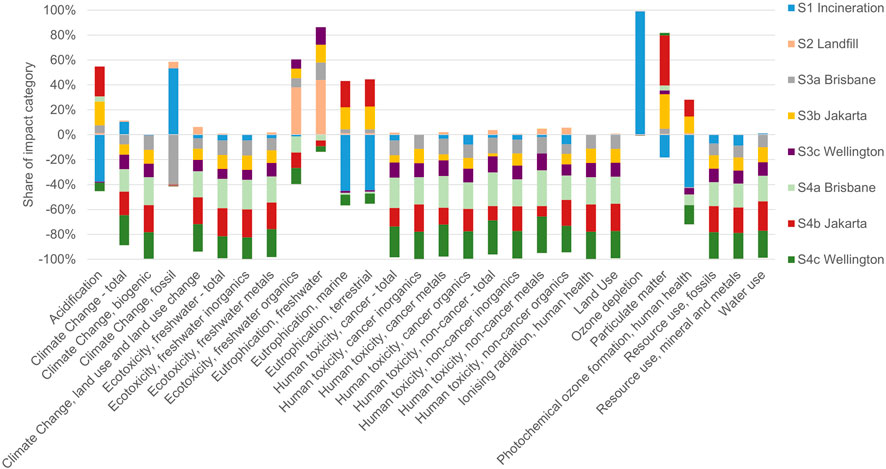
Figure 2. Impact overview for all Impact Categories.
The categories “Acidification Potential,” “Climate Change,” “Eutrophication, freshwater,” and “Resource use, fossils” are examined and described in more detail below. The results of these impact categories per kg of PET waste are shown in Table 1. All other results for the remaining impact categories of the EF 3.0 methodology can be found in the SI.
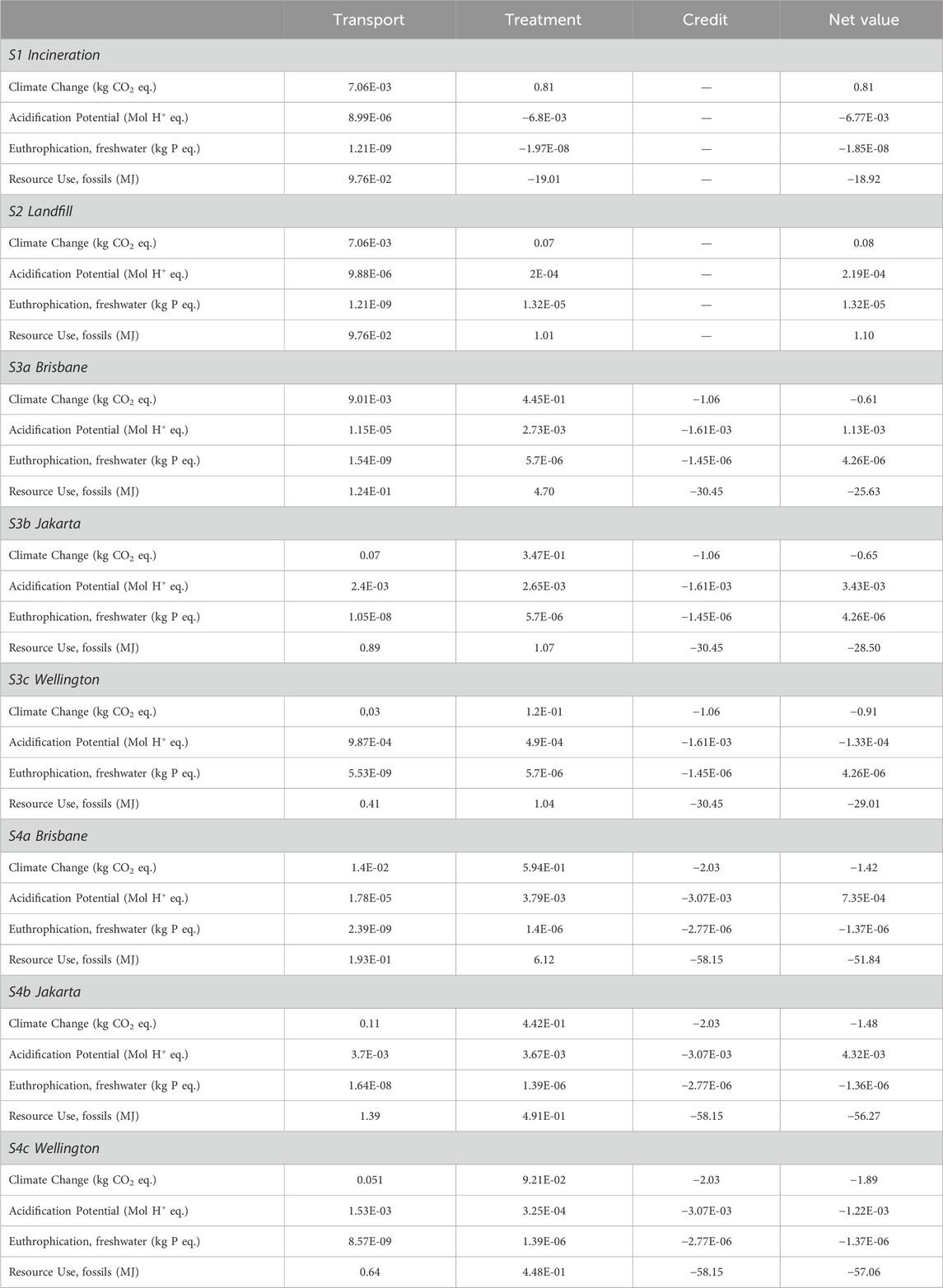
Table 1. Life Cycle Impact Assessment (LCIA) results of the study per kg of PET waste.
In the category of “Climate Change”, scenario S1 (incineration) with 0.81 kg CO2 eq./kg PET exhibits the highest CC in comparison to other scenarios. For scenario S2 the CC is 0.08 kg CO2 eq/kg PET. In both scenarios, no significant contribution from transportation can be identified, but rather the impacts of PET treatment dominate. Subsequently, scenarios S3a, S3b, and S3c follow. With a total value of −0.61 kg CO2 eq./kg PET in scenario S3a, −0.65 kg CO2 eq./kg PET in scenario S3b, and −0.91 kg CO2 eq./kg PET in scenario S3c, these values are notably lower than S1 and S2. The negative values in the LCA results occur when environmental credits are given to the product system i.e., after the recycling of plastic wastes, these recyclates are assumed to be used for the same applications and this means that the use of these recyclates substitute the need for primary production of virgin polymers and the associated environmental impacts. Therefore, this part of the avoided environmental impacts is given to the product system in the form of credits and when the credits are more than the environmental impacts, the net value becomes negative. Transportation also does not exert a significant influence in these scenarios. The total value is comprised of the recycling treatment and, most importantly, the provided credit for recovery. The scenarios S4a-S4c have an even lower overall impact in this impact category. In these scenarios, the credit surpasses all other components of the total value significantly. These values are −1.42 kg CO2 eq./kg PET for scenario S4a, −1.48 kg CO2 eq./kg PET for scenario S4b, and −1.89 kg CO2 eq./kg PET for scenario S4c. Again, transportation contributes less to the overall impacts. The highest contribution comes from the allocated credit due to the higher recyclate quality.
The results of the “Acidification Potential” particularly indicate that transportation causes the most significant differences in this category. This is especially evident in scenarios S3b and S4b, which include transportation to Jakarta. In these scenarios, transportation contributes equally to the overall impact as the end-of-life treatment of PET. Overall, the total value is highest in scenario S3b with 3.43E-03 Mol H+-eq./kg PET and 4.32E-03 Mol H+-eq./kg PET in scenario S4b. At the second recycling location in Wellington, which involves a longer transportation distance, the total values are lower. The total values are −1.33E-04 Mol H+-eq./kg PET for scenario S3c and −1.22E-03 Mol H+-eq./kg PET for scenario S4c. In this case, the recycling process has significantly less influence. Additionally, the impact of transportation is less than half of what is observed in the scenarios in Jakarta. In the scenarios in Brisbane, no significant transportation influences can be observed. The recycling process alone accounts for the total value of 1.13E-03 Mol H+-eq./kg PET in scenario S3a and 7.34E-04 Mol H+-eq./kg PET in scenario S4a. The scenarios for landfill and incineration do not show any transportation influence due to the low transport distances. The total values for scenario S1 are −6.77E-03 Mol H+-eq./kg PET, and 2.19E-04 Mol H+-eq./kg PET for scenario S2. Scenario 2 does not involve any credit participation in the overall result as no materials/energy are recovered during the landfill process.
For “Eutrophication, freshwater”, no noticeable influence of transportation can be observed in any scenario. The overall value of each scenario consistently comprises the impact of the PET treatment and the allocated credit. The lowest overall values are achieved in scenarios S4a to c, which are closely clustered together at −1.37E-06 kg P eq./kg PET for scenario S4a, −1.36E-06 kg P eq./kg PET for scenario S4b, and −1.37E-06 kg P eq./ kg PET for scenario S4c. Following these scenarios is scenario S1 with an overall value of −1.85E-08 kg P eq./kg PET. Scenarios S3a to c all have a similar overall value, amounting to 4.26E-06 kg P eq./kg PET for all scenarios. The highest overall value among all considered scenarios is achieved by scenario S2 at 1.32E-05 kg P eq./kg PET and this is due to the fact that landfilling of plastic wastes can result in a possible generation of leachates which can affect water resources.
The results in the impact category “Resource use, fossils” also show a very low influence of transportation on the overall impact in each scenario. Only scenarios S3b to c and S4b to c exhibit a minimal contribution. The remaining overall values primarily result from the treatment of PET and the allocated credits. The best values are provided by scenarios S4a-c at −51.84 MJ/kg PET, −56.27 MJ/kg PET, and −57.06 MJ/kg PET. They are followed by scenarios S3a-c at −25.63 MJ/kg PET, −28.50 MJ/kg PET, and −29.01 MJ/kg PET. In scenarios S4a and S3a, the influence of PET waste treatment is the highest, due to the use of different energy mixes (for example different share of renewable energies). After the six scenarios described above, scenario S1 follows with −18.91 MJ/kg PET, and scenario S2 with 1.10 MJ/kg PET. In general, credit allocation contributes significantly to the overall results, particularly in scenarios S3a to c and S4a to c.
To further examine the influence of different recycled material qualities on the potential overall impact in the “Climate Change” category, a sensitivity analysis was conducted. In this analysis, the quality was varied between 0% and 100%, allowing the determination of the break-even point. The results of the sensitivity analysis are presented in Figure 3. More information on the sensitivity analysis is shown in detail in the SI (A2).
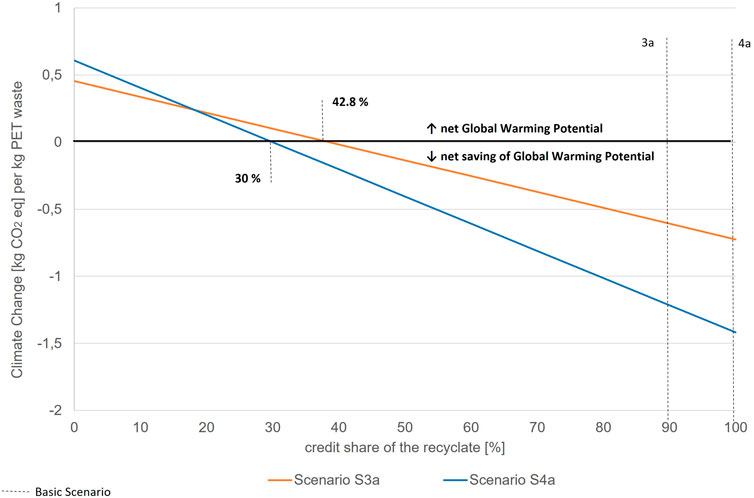
Figure 3. Sensitivity analysis.
When considering the sensitivity analysis, it is noticeable that scenarios S3a and S4a have different “break-even points.” For scenario S3a, a reduction of CC is observed once the substitution potential reaches 42.8%. In contrast, for scenario S4a, this occurs already at a share of 30%. Additionally, the linear slope of this scenario is much steeper compared to scenario S3a. The two percentage rates assumed for the scenarios are also evident, with 90% for scenario S3a (Nessi et al., 2021) and 100% for scenario S4a.
In order to evaluate further uncertainties regarding the estimated transport distances, an uncertainty analysis was carried out in which the total transport distance was varied by ± 50 km for each scenario. This only led to a small visible change for the scenarios in Brisbane, where a variation of around 0.5%–0.7% more or less was recognizable. For these scenarios, the 50 km is relatively more significant than for the much greater transportation distances to Jakarta or Wellington. For the scenarios in Jakarta or Wellington, the total value only changes by 0.2% due to the variation and is even lower. In general, a possible uncertainty in the transportation distances has very little influence on the overall values. The detailed illustration can be found in the Supplementary Information in Figure A4ac.
This study assesses the environmental impacts of existing and potential future end-of-life options for PET anaesthesia and surgical instrument packaging waste in an Australian hospital context. We highlight the need for clinicians and the healthcare industry to engage in and promote circular economy practice to reduce the environmental burden generated from healthcare.
With a total number of 2.7 million surgeries performed annually in Australia (Australian Institute of Health and Welfare, 2024), and more than 310 million surgeries globally, healthcare represents a significant potential for reductions in GHG emissions (Dobson, 2020). Approximately 1,700 kg of PET waste was generated from the operating room complex at an Australian tertiary hospital with around 27,000 surgeries performed per annum (Wyssusek et al., 2020). Extrapolating this to the global number of surgeries performed, the recovery potential for PET at source is significant.
The LCA results clearly indicate that scenarios, where PET waste is pre-sorted, yield significant potential for environmental savings. However, in the acidification category, the landfill and incineration scenarios perform slightly better, as the credits in recycling scenarios 3 and 4 account for a smaller share of the total than the impacts in the landfill and incineration scenarios. Incineration exhibits the least impact in the Acidification category. Landfill has the greatest impact in the Eutrophication category, while incineration stays in the middle range. However, positive environmental effects are only observed in scenarios involving single-grade PET waste. Recycling, as opposed to landfill and incineration, offers enormous potential for resource use savings. All recycling scenarios outperform landfill and incineration, resulting in significant savings of fossil resources. In terms of climate change, a clear comparison can be made. The landfill and incineration scenarios yield values of 0.08 and 0.81 kg CO2 eq. per kg of PET waste, respectively. Recycling scenario 3 achieves values ranging from −0.61 to −0.91 kg CO2 eq./kg PET, while recycling scenario 4 achieves values ranging from −1.42 to −1.89 kg CO2 eq./kg PET. When extrapolated to all surgeries performed annually in Australia, a substantial potential for savings for climate change emerges. Comparing incineration to the recycling scenario in Wellington, savings of 2.7 kg CO2 eq. per kg of PET waste are achieved. Extrapolating to all surgery wastes, (potential) incineration of the entire PET waste results in an impact of 3,717.9 tons of CO2 eq., while recycling of single-grade PET waste leads to savings of −8675.1 tons of CO2 eq. This amounts to potential savings of approximately 12 k tons, equivalent to 866 times the per capita carbon footprint of an Australian in 2021 (Knoema, 2022). However, it should be mentioned that most waste in Australia is landfilled and not incinerated. By comparing the scenarios with the lowest difference, landfill and recycling of unsorted PET waste in Brisbane, savings of 0.69 kg CO2 eq. per kg of PET waste is achieved. For all surgeries performed annually in Australia, this amounts to approximately 3 k tons of CO2-eq., which still corresponds to 221 times the per capita carbon footprint of an Australian in 2021. The per capita carbon footprint in 2021 was 14.31 tons CO2-eq. (Knoema, 2022). Thus, significant potential exists, particularly in this impact category, to reduce CO2 emissions. If this potential were to be considered on a global scale, through examining other continents, enormous savings could be achieved. Therefore, it is of great importance to highlight and raise awareness about hospital PET waste separation at source and subsequent recycling.
However, it is essential to critically evaluate the obtained LCA results. Due to insufficient primary data, aggregated background inventory datasets from Sphera database were used. These datasets do not precisely reflect the reality of recycling processes in Australia or other examined countries. Consequently, uncertainties may arise in the obtained data. Therefore, the data should be used with caution. Furthermore, a material quality of 90% in scenario 3 or 100% in scenario 4 was assumed. Whether these values can actually be achieved in reality depends heavily on local conditions and other parameters such as pre-sorting and the efficiency of recycling facilities (Nessi et al., 2021).
Overall, despite the limitations, this LCA analysis demonstrates enormous potential for environmental savings through alternative utilization of generated PET waste. Recycling and the reuse of high-quality PET significantly contribute to large-scale reduction of CO2 emissions. Therefore, the current waste management options should be reconsidered and revised. Compared to the studies analyzed in the introduction, a valuable contribution was made by providing not only a general overview of different waste types but also a more detailed and precise assessment of savings related to PET plastic packaging in the operating room. This has meaningfully supplemented the current scientific understanding and highlighted specific savings in this sector. This study also stands out in terms of life cycle assessment. The publication by Ivanović et al., only analyzed material flow and did not conduct a comprehensive life cycle assessment with various end-of-life options (Ivanović et al., 2022). While Liu et al. did perform an LCA, it was not specifically focused on PET plastics used for surgical single-use packaging (Liu et al., 2022). A similar situation is observed with Mushtaq et al.; although PET was specifically considered, the results do not provide specific insights into the potential of PET waste recycling (Mushtaq et al., 2022). Furthermore, this study can raise awareness among healthcare sector employees, emphasizing the importance of sorting PET products into single-grade waste to enable environmental savings. In future studies, it is crucial to establish solid inventory data for mechanical PET recycling, allowing for a reevaluation using these databases. This would provide a strong base for supporting the findings of this study. Additionally, the availability and infrastructure required for such a transition need to be researched and analyzed. Only through interdisciplinary collaboration across various sectors, including the healthcare sector and waste management organizations, can the shift from conventional end-of-life options to a recycling system and circular economy be achieved. Active participation in this topic is essential for both the healthcare sector and public areas and waste management facilities.
The healthcare sector has a professional obligation to address climate change and its effect on health attributed to by emissions from the very institutions tasked to protect life. Support from scientists, industry and governments are vital to tackle these challenges together. The recyclability and easy accessibility of OR PET waste in the form of clean, unsoiled packaging from anesthesia and surgical equipment mandates that PET packaging material should be segregated from other waste at source. Xiao et al. highlight in their roadmap for environmental sustainability of plastic use in anesthesia that moving forward the transition to environmental sustainability in healthcare will depend on new approaches such as rethink and research (Xiao et al., 2021).
In this study, an LCA was conducted to compare different end-of-life options for hospital PET waste. Various geographical locations for mechanical recycling of single-grade and mixed PET waste were examined in multiple scenarios. The results demonstrate significant potential for environmental savings through recycling of this waste compared to conventional disposal methods. Particularly, alternative treatments offer substantial reductions in CC. The reduction in CC for each recycling scenario were multiple times higher than the annual CO2-footprint of an average Australian. Extrapolating these findings to a global scale could result in significant emission reductions. High-quality PET used in medical products can achieve favorable material properties after recycling, further contributing to potential savings. Consequently, hospital PET waste presents significant potential for a circular economy, necessitating awareness and engagement from the healthcare sector, PET producers, waste management facilities, and government agencies.
In addition, future studies could integrate additional sustainability aspects. Possible approaches could include incorporating socio-economic aspects, like Social Life Cycle Assessment or Life Cycle Costing (SLCA/LCC) to enable a holistic life cycle sustainability assessment.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
CK: Investigation, Software, Writing–original draft, Writing–review and editing, Data curation, Formal Analysis. SS: Formal Analysis, Investigation, Writing–original draft, Writing–review and editing, Methodology, Project administration, Supervision, Validation, Visualization. VV: Investigation, Methodology, Writing–original draft, Writing–review and editing, Conceptualization, Resources, Software. H-JE: Funding acquisition, Supervision, Writing–review and editing. LB: Conceptualization, Supervision, Validation, Writing–original draft, Writing–review and editing. KW: Conceptualization, Data curation, Project administration, Writing–original draft, Writing–review and editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. The publication of this article was funded by the Open Access Fund of Leibniz Universität Hannover.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fenvs.2024.1415604/full#supplementary-material
AP, Acidification Potential; CO2-eq., Carbon dioxide equivalents; CC, Climate Change; DU, Declared Unit; EF, Environmental Footprint; EP, Eutrophication Potential; GHG, Greenhouse Gases; HCW, Healthcare Waste; ISO, International Organization for Standardization; LCA, Life Cycle Assessment; LCC, Life Cycle Costing; LCIA, Life Cycle Impact Assessment; LCI, Life Cycle Inventory; MRF, Materials Recovery Facility; OR, Operating Rooms; PET, Polyethylene Terephthalate; RU, Resource Use, Fossils; SLCA, Social Life Cycle Assessment; SI, Supplementary Information.
Australian Government Department of Health and Aged Care (2023). Corporate plan 2023–24. Available at: https://www.health.gov.au/resources/publications/corporate-plan-2023-24 (Accessed April 09, 2024).
Australian Institute of Health and Welfare (2024). Hospitals at a glance 2017–18, Surgery in Australia's hospitals. Available at: https://www.aihw.gov.au/reports/hospitals/hospitals-at-a-glance-2017-18/contents/surgery-in-australia-s-hospitals (Accessed April 09, 2024).
Chamas, A., Moon, H., Zheng, J., Qiu, Y., Tabassum, T., Jang, J. H., et al. (2020). Degradation rates of plastics in the environment. ACS Sustain. Chem. Eng. 8, 3494–3511. doi:10.1021/acssuschemeng.9b06635
DIN EN ISO 14040:2021-02 (2021). Environmental management - life cycle assessment - principles and framework. Available at: https://www.beuth.de/de/norm/din-en-iso-14040/325953744 (Accessed March 15, 2024).
DIN EN ISO 14044:2021-02 (2021). Environmental management - life cycle assessment - requirements and guidelines. Available at: https://www.beuth.de/de/norm/din-en-iso-14044/325953813 (Accessed March 15, 2024).
Dobson, G. P. (2020). Trauma of major surgery: a global problem that is not going away. Int. J. Surg. 81, 47–54. doi:10.1016/j.ijsu.2020.07.017
EcoTransIT World (2020). Emission calculator. Available at: https://www.ecotransit.org/en/emissioncalculator/ (Accessed March 18, 2024).
Ellen Macarthur Foundation (2024). Circulytics: measuring circular economy performance. Available at: https://www.ellenmacarthurfoundation.org/resources/circulytics/resources (Accessed March 23, 2024).
Friedericy, H. J., van Egmond, C. W., Vogtländer, J. G., van der Eijk, A. C., and Jansen, F. W. (2022). Reducing the environmental impact of sterilization packaging for surgical instruments in the operating room: a comparative life cycle assessment of disposable versus reusable systems. Sustainability 14, 430. doi:10.3390/su14010430
Geyer, R., Jambeck, J. R., and Law, K. L. (2017). Production, use, and fate of all plastics ever made. Sci. Adv. 3, e1700782. doi:10.1126/sciadv.1700782
Ivanović, T., Meisel, H.-J., Som, C., and Nowack, B. (2022). Material flow analysis of single-use plastics in healthcare: a case study of a surgical hospital in Germany. Resour. Conservation Recycl. 185, 106425. doi:10.1016/j.resconrec.2022.106425
Kagoma, Y. K., Stall, N., Rubinstein, E., and Naudie, D. (2012). People, planet and profits: the case for greening operating rooms. CMAJ 184, 1905–1911. doi:10.1503/cmaj.112139
Knoema (2022). Australia CO2 Emissions (Tonnes per person), 1970-2023 - knoema.com. Available at: https://knoema.de/atlas/Australien/CO2-Emissionen-Tonnen-pro-Kopf (Accessed April 09, 2024).
Kwakye, G., Brat, G. A., and Makary, M. A. (2011). Green surgical practices for health care. Arch. Surg. 146, 131–136. doi:10.1001/archsurg.2010.343
Leiden, A., Cerdas, F., Noriega, D., Beyerlein, J., and Herrmann, C. (2020). Life cycle assessment of a disposable and a reusable surgery instrument set for spinal fusion surgeries. Resour. Conservation Recycl. 156, 104704. doi:10.1016/j.resconrec.2020.104704
Liu, M., Wen, J., Feng, Y., Zhang, L., Wu, J., Wang, J., et al. (2022). A benefit evaluation for recycling medical plastic waste in China based on material flow analysis and life cycle assessment. J. Clean. Prod. 368, 133033. doi:10.1016/j.jclepro.2022.133033
MacNeill, A. J., Hopf, H., Khanuja, A., Alizamir, S., Bilec, M., Eckelman, M. J., et al. (2020). Transforming the medical device industry: road map to A circular economy. Health Aff. (Millwood) 39, 2088–2097. doi:10.1377/hlthaff.2020.01118
McGain, F., Jarosz, K. M., Nguyen, M. N. H. H., Bates, S., and O'Shea, C. J. (2015). Auditing operating room recycling: a management case report. A A Case Rep. 5, 47–50. doi:10.1213/XAA.0000000000000097
McGain, F., Sheridan, N., Wickramarachchi, K., Yates, S., Chan, B., and McAlister, S. (2021). Carbon footprint of general, regional, and combined anesthesia for total knee replacements. Anesthesiology 135, 976–991. doi:10.1097/ALN.0000000000003967
Mushtaq, M. H., Noor, F., Mujtaba, M. A., Asghar, S., Yusuf, A. A., Soudagar, M. E. M., et al. (2022). Environmental performance of alternative hospital waste management strategies using life cycle assessment (LCA) approach. Sustainability 14, 14942. doi:10.3390/su142214942
Nessi, S., Sinkko, T., Bulgheroni, C., Garcia-Gutierrez, P., Giuntoli, J., Konti, A., et al. (2021). Life Cycle Assessment (LCA) of alternative feedstocks for plastics production.Part 1, the Plastics LCA method: European Commission. Luxembourg: Joint Research Centre. Publications Office.
Plastics Europe (2023). Plastics - the facts 2021 ⋅ plastics Europe. Available at: https://plasticseurope.org/knowledge-hub/plastics-the-facts-2021/ (Accessed April 09, 2024).
Sherman, J. D., Raibley, L. A., and Eckelman, M. J. (2018). Life cycle assessment and costing methods for device procurement: comparing reusable and single-use disposable laryngoscopes. Anesth. Analg. 127, 434–443. doi:10.1213/ANE.0000000000002683
Sphera (2023a). Life cycle assessment software - Sphera LCA for Experts | Sphera (GaBi). Available at: https://sphera.com/life-cycle-assessment-lca-software/ (Accessed March 09, 2024).
Sphera (2023b). Sphera LCA data - most reliable LCA data | Sphera (GaBi). Available at: https://sphera.com/life-cycle-assessment-lca-database/ (Accessed April 09, 2024).
Thiel, C. L., Eckelman, M., Guido, R., Huddleston, M., Landis, A. E., Sherman, J., et al. (2015). Environmental impacts of surgical procedures: life cycle assessment of hysterectomy in the United States. Environ. Sci. Technol. 49, 1779–1786. doi:10.1021/es504719g
Unger, S. R., and Landis, A. E. (2014). Comparative life cycle assessment of reused versus disposable dental burs. Int. J. Life Cycle Assess. 19, 1623–1631. doi:10.1007/s11367-014-0769-3
van Zanten, F., Tensen, S., Snijder, L., Broeren, M., and Kwee, A. (2024). Impact of delivery instruments on the environment: a life cycle assessment. Repro Female Child. Health 3. doi:10.1002/rfc2.72
Wu, S., and Cerceo, E. (2021). Sustainability initiatives in the operating room. Jt. Comm. J. Qual. Patient Saf. 47, 663–672. doi:10.1016/j.jcjq.2021.06.010
Wyssusek, K., Keys, M., Laycock, B., Avudainayagam, A., Pun, K., Hansrajh, S., et al. (2020). The volume of recyclable polyethylene terephthalate plastic in operating rooms - a one-month prospective audit. Am. J. Surg. 220, 853–855. doi:10.1016/j.amjsurg.2020.05.011
Wyssusek, K. H., Keys, M. T., and van Zundert, A. A. J. (2019). Operating room greening initiatives - the old, the new, and the way forward: a narrative review. Waste Manag. Res. 37, 3–19. doi:10.1177/0734242X18793937
Xiao, M. Z. X., Abbass, S. A. A., Bahrey, L., Rubinstein, E., and Chan, V. W. S. (2021). A roadmap for environmental sustainability of plastic use in anesthesia and the perioperative arena. Anesthesiology 135, 729–737. doi:10.1097/ALN.0000000000003845
Keywords: plastic waste, recycling, circular economy, PET, medical waste, Australia
Citation: Keul C, Spierling S, Venkatachalam V, Endres H-J, Barner L and Wyssusek K (2024) Potential of polyethylene terephthalate (PET) in a circular economy from a life cycle assessment perspective - a case study for anaesthesia and surgical instrument packaging waste in Australia. Front. Environ. Sci. 12:1415604. doi: 10.3389/fenvs.2024.1415604
Received: 10 April 2024; Accepted: 04 October 2024;
Published: 18 October 2024.
Edited by:
Miguel Ángel Pardo Picazo, University of Alicante, SpainReviewed by:
Hasan Nikkhah, University of Connecticut, United StatesCopyright © 2024 Keul, Spierling, Venkatachalam, Endres, Barner and Wyssusek. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Venkateshwaran Venkatachalam, dmVua2F0YWNoYWxhbUBpa2sudW5pLWhhbm5vdmVyLmRl
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.