 Adela Socol
Adela Socol Horia Iuga2
Horia Iuga2
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Environ. Sci., 11 December 2023
Sec. Environmental Economics and Management
Volume 11 - 2023 | https://doi.org/10.3389/fenvs.2023.1286099
This article is part of the Research TopicExploring New Development Patterns for Climate Change Resilience and MitigationView all 5 articles
The continuous growth in average temperature around the world, caused especially by CO2 emissions, generates climate changes significantly impacts not only economic or social domains, but also human health. The previous literature provides evidence of degradation of human health due to climate change and emphasizes pressure on governments to increase government spending on health. The aim of this study is to analyze the impact of climate change, expressed by temperature and CO2 emissions, on healthcare spending in the European Union member states using available data from 2000 to 2020. In addition to prior research, this paper incorporates supplementary control variables such as governance, macroeconomic factors (GDP and inflation) and human development index. To capture the dynamic impact of climate change on healthcare expenditure, we use the Generalized Method of Moments (GMM) technique and the panel VAR Granger causality method. Empirical findings suggest that an increase in temperature and CO2 emissions levels, along with improvements in governance, economic growth, inflation, and human development, contribute to higher healthcare expenditures. Rising temperature and CO2 emissions are directly increasing the health burden on individuals’ health and force governments to enhance health spending. The paper is notable for its comprehensive approach, filling a significant gap in existing literature by combining climate change variables with governance, economic and human development indicators. The study provides policymakers with valuable insights into how climate change and other governance, economic and human factors impact healthcare spending. Global warming appears as a topic directly correlated with the governmental health spending burden and highlights the need for government involvement in mitigating global warming, reducing pollution and gas emissions.
Environmental degradation is a pressing global issue today, negatively influencing the economy, human health, and environmental aspects such as air quality and ozone levels. A primary contributor to this degradation is the escalating trend of carbon dioxide emissions (Weimin et al., 2022). The release of greenhouse gases due to human activities has led to a discernible surge in global temperatures, and this has been linked to an escalation in the occurrence and intensity of heatwaves and hot summers (IPCC, 2021). Recent years are the hottest on record (European Commission, 2022). Europe faces irreversible climate effects, including biodiversity loss and more forest fires. Concurrently, heatwaves significantly impact human health, causing illnesses and deaths (European Parliament, 2018). Between 2030 and 2050, an additional 250.000 deaths per year could result from malnutrition, malaria, diarrhea, and heat stress, attributable to climate change (WHO, 2021).
Climate change contributes to the decline in human health, with most studies primarily emphasizing the negative physical health effects (Rocque et al., 2021). Upon entering the European Union, many nations, notably former communist states, underwent significant industrialization (Wawrzyniak, 2020). This surge in industry escalated carbon emissions until 2010, elevating temperatures. Anticipating this, the EU initiated climate strategies by 2008, introducing the Climate and Energy package. A key 2020 target was reducing emissions by 20% from 1990 benchmarks (European Parliament, 2023b). While emissions dipped post-2010, environmental and health impacts lingered. Spending on healthcare is pivotal for individual health and a country’s economic progress (Lopreite and Zhu, 2020; Lopreite et al., 2023). The industrial boom and rising CO2 levels aggravated health issues, especially respiratory and heart conditions (Beatty and Shimshack, 2014). Medical expenses for treatment and preventive measures have surged, driving up healthcare costs and putting a strain on healthcare systems. Concurrently, the rise in average temperatures, resulting from higher emissions, affects human health in different ways. It leads to heat-related illnesses and tropical diseases in areas previously unaffected. Healthcare spending in this area has risen sharply. For example, heat-related hospital admissions have increased by 15% in the past decade in some EU countries, according to certain statistics (European Environment Agency, 2022). In 2022 alone, over 60.000 individuals in Europe died because of extreme heat, a figure three times higher than previous estimates. With the ongoing warming of the planet, this number is anticipated to increase annually (WHO, 2023). In 2019, the European Parliament declared a climate emergency, leading to the Commission’s European Green Deal for a climate-neutral 2050. On 24 June 2021, the European Parliament adopted the climate law, mandating a 55% emissions reduction by 2030 and climate neutrality by 2050. This strengthens the EU’s global leadership in combating climate change and led to a 2021 legislative package called “Fit for 55"(European Parliament, 2023c).
The environmental changes described earlier led to specific health issues that, in turn, increased healthcare costs. This chain of events paints a tangible picture of how industrialization and climate change have had economic impacts on public health. Europe stands out as a significant climatic focal point (van Daalen, et al., 2022), experiencing a warming rate almost 1°C above the global increase, and surpassing any other continent (European Commission, 2022). In 2019 the EU was the fourth largest greenhouse gas emitter after China, the United States and India (European Parliament, 2023a). Furthermore, projections regarding Europe’s climate warn that unless robust measures are taken to mitigate and adapt, temperatures and their subsequent effects on health will escalate at an expedited pace (Ballester et al., 2023). In future projections (period 2021–2050 vs 1981–2010), around 0.4% of the yearly number of respiratory hospital admissions (RHAs) in Europe are estimated to result from heat, based on the average predictions across climate change forecasts. In absolute numbers, represents approximately 26,000 cases annually in Europe (Åström et al., 2013).
The research question is positioned at the critical intersection between environmental conditions and healthcare economics and is based on the findings of previous literature in the actual context of climate change affecting human health: Does climate change impact government healthcare spending in the European Union countries?
This paper tackles a relatively novel subject, extending existing academic discourse on health and medical spending by analyzing various factors that influence healthcare expenditures. However, there are relatively few empirical studies on the impact of climate change on health spending, especially for EU member countries, but no study combines these factors with governance variables, human development variables and macroeconomic variables, simultaneously.
The aim of the study is to explore the relationship between healthcare expenditure (dependent variable) and specific climate change factors such as temperature and CO2. We add several control variables: governance, macroeconomic and human development variables. The study includes all 27 European Union member countries during the period 2000–2020. The main findings of this work can be summarized as follows: Increases in temperature and CO2 levels lead to higher healthcare spending. Enhancements in governance, increased GDP growth, inflation, and a rise in the human development index all contribute to growth in governmental healthcare expenditure. These findings weave together the themes and evidence presented, offering a comprehensive view of the subject matter.
The central objective of this study is to explore the impact of climate change using two specific climate change variables (temperature and CO2 emissions) on government health spending for all EU member states, based on data from 2000 to 2020. We also introduced several control variables, namely, governance, two macroeconomic variables (GDP and inflation) and a human development variable (Human development index). Human development index (HDI) is considered suitable for our analysis because represents essential aspects of human capabilities, while we use the life expectancy indicator (LIFE) instead of the human development index only for robustness tests, evaluating the stability of their main outcomes. The rationale for this decision arises from HDI’s structure and their study’s emphasis: HDI combines three facets - health (quantified by life expectancy at birth), education (quantified by average adult schooling years and projected schooling for new students) and living standards (represented by Gross National Income per head). By using life expectancy as an alternative for HDI, we are isolating the health dimension (life expectancy) from the overall human development measure. In essence, they are aiming to assess how the results might differ when focusing solely on the health dimension rather than a more comprehensive development index that also encompasses education and income levels. The study primarily examines climate change’s impact on health spending. Life expectancy is a pertinent gauge of health outcomes in a population and using LIFE allows us to delve deeper into how climate variations potentially affect health results and, in turn, health expenditures.
To the best of the authors’ knowledge, this is a pioneering study on the subject, considering all relevant variables. The results will help decision makers gauge how climate change affects healthcare spending and how GDP, governance, inflation and the human development index affect government healthcare spending in selected countries. Moreover, to ensure the robustness of the model, we additionally used other indicators from the above-mentioned groups (e.g., GDP per capita growth, used interchangeably with GDP per capita, life expectancy used instead of Human Development or individual variables from Worldwide Governance Indicators studied alternately instead of the Governance variable, determined by the method of Principal Component Analysis from Worldwide Governance Indicators).
The innovation of this paper lies in its comprehensive, pioneering approach to examining the effects of climate change variables (specifically temperature and CO2 emissions) on governmental health expenditures in all EU member states from 2000 to 2020, while also incorporating additional control variables like governance, macroeconomic factors, and human development indices.
While there is vast literature exploring the climate change or healthcare government challenges, there remains a scarcity of research specifically examining the interplay between the specific two dimensions–climate change expressed by average temperature and CO2 emissions on the one hand and government spending on health on the other - especially within the unique context of the European Union. This gap in understanding becomes particularly significant given the current manifestations of global warming and requires an integrative analysis that holistically examines how climate change might affect government spending on health and how these dynamics manifest themselves in the EU’s interconnected landscape and how the relationship between climate change and health spending is affected by governance variables, macroeconomic or human development. This study endeavors to bridge this gap, offering insights that can inform both policy-making and future academic pursuits.
This study enhances the current literature in four significant ways. Firstly, it contemporaneously addresses both temperature and CO2 emissions concerning climate. Secondly, it incorporates control variables such as governance, macroeconomic elements, and human development indicators. Thirdly, all empirical models are validated by robust tests that show strong evidence of long-term relationships between variables and produce effective empirical results that are indeed plausible for policy engagement. Fourthly, the paper presents a set of political implications that state governments can consider.
Political Implications: Healthcare spending should consider the increased burden on health units during periods of extreme temperatures. The findings of this research underline a crucial connection between climate change and a rise in healthcare spending within the European Union, holding substantial implications for policymakers. The data emphasizes an immediate need to focus on both environmental conservation and public health. By showcasing the financial consequences of health problems associated with climate change, the results advocate for the incorporation of climate change prevention methods and adaptation into healthcare strategies. Using improved governance, economic growth, and an emphasis on human development, a comprehensive strategy can be developed to lessen healthcare expenditure and enhance the overall wellbeing of society.
The remainder of this paper is organized as follows. Section 2 presents the actual stage of the knowledge in the field and the research hypotheses; Section 3 describes the data and method; Section 4 refers to results and discussions. At the end, the authors present the conclusions of the paper.
The nexus between climate change and healthcare expenditure is becoming increasingly visible. Stern (2007) notes a 0.7°C rise in global average temperature over the past century, raising global concerns. The World Health Organization confirms this, stating that heatwave exposure impacted 125 million people from 2000 to 2016, increasing health risks (WHO, 2018). Complementing this, Zammit et al. (2021) argue that even a single-degree uptick in temperature due to global warming activates an acclimatization process that, if sustained, triggers pathways leading to neurodegeneration, like oxidative stress and excitotoxicity. Meanwhile, Tong et al. (2021) caution that such heatwaves lead to a surge in heat-related ailments - heat exhaustion, heatstroke, dehydration - requiring medical intervention and straining healthcare budgets. These interconnected findings heighten the urgency for addressing climate change’s multifaceted impact on health. Such conditions often necessitate urgent medical care and hospital admissions, resulting in elevated healthcare costs. For example, during extreme heat events, hospitals may see a surge in admissions, putting strain on healthcare systems and requiring additional resources to treat affected individuals (Boz and Ozsari, 2020).
Increasing temperatures can change the habitats of disease-bearing vectors such as mosquitoes, facilitating the spread of illnesses like malaria and dengue fever into previously unaffected regions (Chowdhury et al., 2018). The public health measures required to address this expansion, including prevention, diagnosis, treatment, and containment, collectively contribute to increased healthcare costs and implicitly on government health expenditures. Increased temperatures can raise ground-level ozone levels, leading to respiratory issues (WHO, 2018), particularly in urban locations. Addressing and treating these health concerns necessitates financial investments in healthcare services as well as measures to control environmental conditions.
Climate change and the associated increase in extreme weather events can impact healthcare infrastructure. For example, heatwaves may require hospitals to upgrade cooling systems, while rising sea levels and storms can damage healthcare facilities, necessitating repairs and improvements (Sasmaz et al., 2021).
Governments must anticipate these climate-related health risks and integrate them into healthcare planning. This involves investing in preventive measures such as early warning systems for heatwaves, improving healthcare infrastructure to withstand extreme weather events, and developing public health campaigns to educate the population about the risks associated with temperature extremes (Schneider, and Breitner, 2016).
The link between temperature and health spending is not isolated from broader economic factors. For example, the increased need for healthcare services during extreme temperature events may strain existing healthcare resources (Wondmagegn et al., 2019), leading to potential cost increases across the system (Fotourehchi and Çalışkan, 2018).
The impact of temperature on health spending also has social dimensions. Vulnerable populations may be disproportionately affected by temperature-related health issues, requiring targeted interventions. Addressing these disparities may necessitate additional spending on social support programs and tailored healthcare services.
Considering these, we can formulate the research hypothesis of this study:
Hypothesis 1. (H1): Rising temperatures lead to increased government health spending.
Several theories in the literature elucidate the relationship between CO2 emissions and government health expenditure (Sohail et al., 2023): 1. Nightingale’s Environmental Theory: Florence Nightingale emphasized the significance of a pristine environment, including clean air, for optimal health. CO2 emissions, a contributor to air pollution, when unchecked, can escalate healthcare expenses due to pollution-induced ailments. 2. Life Course Health Development (LCHD) Framework: This framework accentuates health as an evolving process influenced by various determinants like biology, environment, and social context. Within this, CO2 emissions, an environmental determinant, can profoundly influence health. Resultantly, governments might escalate health budgets to tackle and preempt related health issues. 3. Carbon Dioxide Theory: This theory posits that surging CO2 levels elevate global temperatures, leading to heat-driven health issues and the spread of diseases. These health challenges can amplify governmental health costs. 4. Systematic Linkage Model: The Systematic Linkage Model connects health spending and carbon emissions, advocating for energy-efficient medical gear. This approach mutually benefits environmental sustainability and reduces operational costs. 5. Environmental Kuznets Curve (EKC): This theory suggests an inverse U-shaped connection between per capita income and environmental degradation. Initially, economic growth intensifies pollution, but after reaching a specific income threshold, the environment starts benefiting from continued economic progress. Wang et al. (2023) found that in the long term, social globalization, energy, and economic growth influence CO2 emissions. Sohail et al. (2023) indicate that specific economic stages may necessitate more healthcare investment to address health issues caused by CO2 emissions.
Global greenhouse emission concerns urge decision-makers worldwide to prioritize the environment, assess their ecological footprint, and find methods to enhance environmental quality (Nuţă et al., 2015). The desired climate neutrality that has been on the agenda of governments in recent years is, however, profoundly influenced after 2022 by manifestations of the energy crisis, against the background of the geo-political conflict of Ukraine, which negatively influences energy markets, studied between February and October 2022 (Chishti et al., 2023c).
Researchers globally, using varied methods, concur that rising CO2 emissions adversely impact public health and consequently inflate healthcare spending. The consensus underscores the urgency to address CO2 emissions for both health and economic reasons. They have concentrated their research on different regions and countries: Malaysia (Samah et al., 2020), USA (Gündüz, 2020), West Africa (Oyelade et al., 2020), Southeast Asia (Taghizadeh-Hesary and Taghizadeh-Hesary, 2020), 33 OECD countries (Akbar et al., 2021), BRICS countries (Li et al., 2022), Brazil (Travassos et al., 2020), Canada (Jerrett et al., 2003), China (Jia et al., 2021), Iran (Raeissi et al., 2018), Latin America (Koengkan et al., 2021), MENA countries (Khoshnevis and Khanalizadeh, 2017).
Kim T. J. et al. (2017) discovered that the 1997 wildfires’ effects on individuals persisted for over a decade. Isen et al. (2017) demonstrated the impact of clean air legislation on increased earnings in adulthood due to reduced exposure to pollutants in childhood. Chaabouni et al. (2016) found unidirectional causality between CO2 emissions and health spending in 51 countries between 1995 and 2013. Usman et al. (2019) observed that climate change factors, i.e., air pollution, had two indicators; namely, CO2 and temperature, and showed a significantly positive relationship with government spending on health in 13 emerging economies from 1994 to 2017.
Developing on a highlighted literature gap, Zhang et al. (2023) innovatively construct a health quality index, which is used as a dependent variable for China’s case from 1980 to 2020 and demonstrates by applying the VECM method that CO2 emissions negatively impact health quality.
This circumscribes the second hypothesis of the research:
Hypothesis 2. (H2): Increasing CO2 emissions lead to increased government health spending.
Rising neglect and unawareness in areas like CO2 emissions and healthcare spending jeopardize global health (Sohail et al., 2023). There are numerous studies that argue that GDP influences health spending (Samudram et al., 2009; Zaidi and Saidi, 2018; Wang et al., 2019; Azam and Awan, 2022). They all claim that GDP positively and strongly influences health spending. In their 2019 study, Wang and others utilized yearly time series data spanning from 1975 to 2017 to investigate the long-term interconnection between health spending, CO2 emissions, and GDP per capita. They employed the bootstrap ARDL cointegration model for this analysis, focusing on 18 countries listed by the World Health Organization and the Organization for Economic Cooperation and Development (OECD). Their primary findings indicate a positive correlation among the three studied variables. Kutlu and Örün’s (2022) study reveals that in 21 OECD countries from 1992 to 2018, CO2 emissions and GDP per capita have a positive impact on health spending. The results of their study conclude that the effect of carbon dioxide (CO2) emissions, urban population and GDP per capita are significant and positive on health expenditure. OECD countries’ recent rapid economic growth and environmental pollution have increased long-term health spending. Other researchers, for example, Javaid et al. (2023) found through regression analysis that GDP significantly impacts CO2 emissions both in the short and long term, indicating that GDP compromises environmental sustainability by elevating CO2 emissions. Environmental performance proves to be essential in establishing integrated sustainable development profiles of companies (Ma et al., 2022). Precursors of economic growth, foreign direct investment is a catalyst for pollution and significantly potentiates the export of highly polluting goods, as resulted from the study developed for five ASEAN countries between 1990 and 2019 (Salam and Chishti, 2022). Environmental policies simultaneously with circular economy and energy transitions contribute to global sustainable electricity generation and implicitly to sustainable development (Chishti et al., 2023b).
GDP, a crucial economic indicator, significantly influences healthcare expenditure (Efthalitsidou et al., 2021). A robust GDP often leads to higher public and private healthcare allocations, enabling more advanced treatments and facilities (Onisanwa, 2014). Affluent countries typically invest a larger portion of their budget in healthcare, improving its quality and availability (Barati and Hadiseh, 2020). Furthermore, GDP growth enhances individual purchasing power, rendering healthcare services more accessible. Higher incomes also encourage investment in preventative care and expensive treatments, thus elevating health expenditure (Chaabouni and Saidi, 2017). A strong GDP creates a stable economic environment, attracting investment in healthcare infrastructure such as hospitals and research centers (Rodríguez and Nieves Valdés, 2019). These developments necessitate sustained spending for upkeep and staffing. Additionally, a high GDP often leads to increased government revenue through taxation (Ullah et al., 2023), which may be channeled into public health initiatives, vaccination programs, and subsidized healthcare, thereby boosting overall healthcare spending. Moreover, a high GDP can lead to the implementation of various solutions, for example, artificial intelligence, to combat climate change by analyzing data and predicting the results. Artificial intelligence helps develop sustainable solutions, optimize resources and minimize carbon emissions for a sustainable future (Firdaus et al., 2022). The ideal of future development of economies is mandatorily linked to green innovations, which contribute decisively to green economic growth, as recent study has shown based on innovative econometric methods (Wavelet Quantile Correlation and Wavelet Transform Causality), for the case of G-7 economies (Zaman et al., 2023). Climate mitigation technologies is impacted by GDP, as well as natural resources, monetary policy, environmental taxes and economic globalization, as evidenced by a study developed for G-7 economies (Chishti and Patel, 2023).
Economic studies highlight multiple factors elevating health spending, with economic growth being the most scrutinized demand driver. To a lesser extent, another macroeconomic factor, inflation, was also investigated. The existing studies find that the relationship between health expenditure and inflation to be positive: inflation significantly increases health spending (De la Maisonneuve et al., 2017; Jakovljevic et al., 2017; Yip et al., 2017; Dunn et al., 2018; Siami-Namini, 2018; Cheng and Nopphol, 2019). For example, the results of the study by Azam and Awan (2022) conclude that inflation significantly increases health spending in sample economies (15 Asian countries from 2000Q1-2017Q4). Siami-Namini (2018), in his study found that inflation rate positively and significantly affected health expenditure in G7 countries during 1995–2015.
Inflation, the overall increase in prices and decrease in the purchasing value of money, can substantially influence health spending. When inflation rates rise, the cost of goods and services typically follows suit. Inflation can increase healthcare costs, including medical supplies, medications, and labor. This rise in operational expenses often results in increased out-of-pocket costs for patients, reducing healthcare affordability (Dunn et al., 2018). Additionally, public healthcare funding can also be affected. If a government’s budget allocation for healthcare remains static while inflation is increasing, the real value of that funding diminishes. This reduction can lead to a lower quality of healthcare services, as resources become scarcer. It may necessitate cutbacks in services, a decline in staff-to-patient ratios, or limits on the availability of new, potentially more effective, but more expensive treatments (Yip et al., 2017). Moreover, inflation affects income levels. Nominal wage increases may not keep pace with inflation, impacting real income and healthcare affordability. This is especially tough for fixed-income groups, such as retirees, as rising healthcare costs consume a greater share of their unchanging income (Cheng and Nopphol, 2019). Lastly, high inflation rates can deter investment in healthcare infrastructure. Uncertain economic conditions make it risky for both public and private sectors (Koijen et al., 2016) to invest in long-term projects like hospitals or medical research facilities, thereby affecting the quality and accessibility of healthcare in the long run (De la Maisonneuve et al., 2017; Jakovljevic et al., 2017).
Little is known about the link between governance and health expenditures. Rahman et al., 2018 argue in their paper that spending should be managed through proper governance. It is acknowledged that research reveals positive outcomes between governmental health expenditures and governance (Jakovljevic et al., 2016; Kaur, 2020; Ray and Linden, 2020). Effective governance is crucial for directing health spending and ensuring quality healthcare. Strong governance structures aid in the strategic allocation of resources and the formulation of well-funded, comprehensive healthcare policies in both developed and developing countries (Nakatani et al., 2023). Such policies not only aim to improve the infrastructure but also address systemic issues like healthcare inequality. Conversely, poor governance often results in ineffective policies, plagued by corruption or bureaucracy, that may lead to misallocation of funds (Kim Y. et al., 2017). On the other hand, governance is key in revenue collection and allocation. A transparent and efficient tax system can generate more public revenue, a portion of which can be allocated to healthcare. In countries where governance is poor, revenue often leaks through corruption, reducing the funds available for public health (Maugeri et al., 2023). Governance impacts the regulatory environment and effective governance can ensure the regulation of healthcare prices, quality of medical services, and even the conduct of healthcare professionals. This, in turn, can help in controlling expenditures and increasing the efficacy of healthcare services. Poor regulatory frameworks can result in inefficiencies that balloon healthcare costs (Raeesi et al., 2018). Governance can also influence healthcare spending through international partnerships. A government with strong international relations can secure funding or expertise from international organizations or more developed nations. Such partnerships can lead to an increase in healthcare spending that is both efficient and effective (Kochuvilayil et al., 2023). The role of governance extends to crisis management, which was particularly evident during the COVID-19 pandemic. Well-governed countries have been more effective in securing necessary funding for healthcare services in times of crisis, ensuring the continuity and quality of care (Makin and Layton, 2021).
The rise in health expenditures is intricately linked to improvements in the Human Development Index, yet it is also influenced by the escalating challenges posed by climate change on public health. In fact, in an extended approach, human capital has favorable effects on the efficiency of sustainable development, as evidenced by the instrumented study of the provinces of China between 1998 and 2017 (Chishti et al., 2023a). Human development, measured through indicators like education, income, and life expectancy, significantly influences health spending. For example, a more educated population tends to be more aware of the importance of healthcare and preventive measures, leading to higher healthcare consumption (Biadgilign et al., 2019). Human development influences health spending in interconnected ways. Longer life expectancy results in an older population requiring more healthcare, thereby increasing expenditure (Brooks et al., 2005). Simultaneously, societal progress brings advanced, albeit expensive, medical technologies into common use. Higher incomes and increased awareness further fuel this demand. As social infrastructure improves, governments in developed nations expand public healthcare benefits, raising national health budgets (Miranda-Lescano et al., 2023). Urbanization, another byproduct of development, brings unique healthcare needs (Lin and Guo, 2023) like stress management and pollution control, necessitating specialized services and escalating costs (Shao et al., 2022). Development also means greater integration into the global economy, leading to increased risks like pandemics that require substantial health expenditure to manage (Pervaiz et al., 2021). These factors create a cycle where development and health spending are intrinsically linked, each reinforcing the other.
To analyse the influence of climate change on health expenditure, we use data from 27 European Union (EU) countries over the period 2000–2020, considering the average temperature and CO2 emissions as proxies for climate change. The motivation for choosing these countries and the analysis interval is based on the common post-2000 history of most EU countries, given that 13 of the 27 component countries joined after 2000 (10 in 2004, 2 in 2007 and one in 2013). Thus, the analysis interval captures new EU states at about a decade of experimentation with free democratic regimes, after about 4 decades of totalitarian regimes.
To determine the impact of climate change on health expenditure, this study performs the dynamic panel system GMM method (Generalized Method of Moments) and the panel VAR Granger causality method technique. Compared to previous literature explaining the impact of climate change on health spending by exploring its direct effects, our study also looked at the moderating effects of various factors, such as economic, governance or human development.
Table 1 presents the variables and data sources. The dependent variable refers to health expenditure and the core explanatory variables that reflect climate change are average temperature and CO2 emissions. Climate change is a major concern for public health, and experts consider temperature increase the biggest threat to climate change, which makes the target of limiting the increase in global average temperature to a maximum of 1.5°C by the end of the twenty-first century to be set by the Intergovernmental Panel on Climate Change (Hayashi et al., 2022). In line with previous literature (Karahasan and Pinar, 2023), this study considers the average temperature as a proxy for climate change, especially due to the direct mechanisms by which the Earth’s surface temperature reflects its specific energy balance (atmospheric air temperature rises or falls, under the influence of a combination of factors - solar radiation, heat inside the Earth, greenhouse gases, etc.). CO2 emissions is considered indicator of climate change in our study, as similar research considered them (Cengiz and Manga, 2022), starting from their significant percentage in greenhouse gas emissions and their defining role in heat capture and global warming. The climate future of the planet depends on the effectiveness of CO2 mitigation policies, which makes the main drivers of CO2 emissions - human activity, economic development or carbon intensity - the subject of national and inter-state analyses, in the fight against global warming.
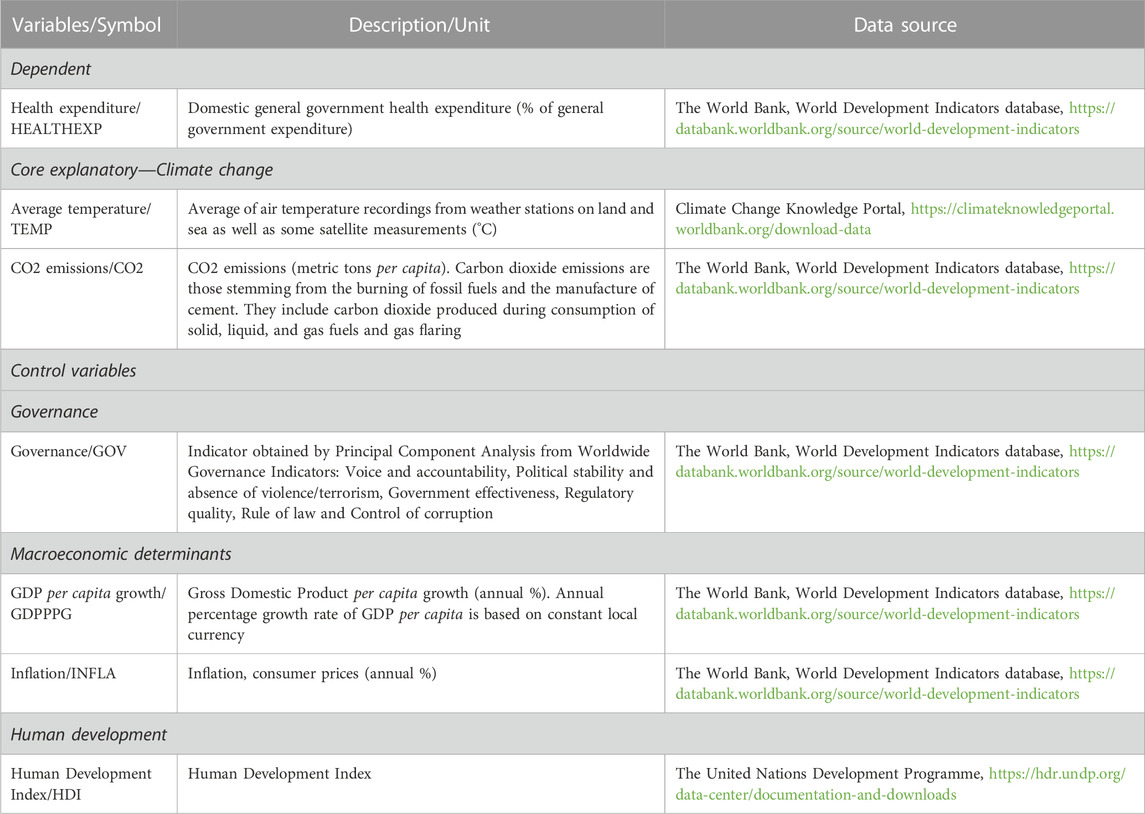
TABLE 1. Variables and data sources.
To control the macroeconomic level, this study uses Gross Domestic Product per capita growth rates and annual inflation rates, while to control the institutional country’s factors, the Worldwide Governance Indicators are employed. These Worldwide Governance Indicators capture six dimensions of governance: Voice and accountability, Political stability and absence of violence/terrorism, Government effectiveness, Regulatory quality, Rule of law and Control of corruption. We use Principal Component Analysis to create a single comprehensive variable of governance, based on the mentioned Worldwide Governance Indicators. To estimate the effects of human development, we utilize Human Development Index, that measures the main dimensions of a long and healthy life, education and decent standard of living.
To study the influence of climate change impact on health expenditure in the European Union (2000–2020), we use the following dynamic panel data model:
where i represents the country, t is the period (years), HEALTHEXPi,t-1 represents 1-year lag of HEALTHEXP, Control denotes control variables, TEMP is average temperature, CO2 represents CO2 emissions, GOV is governance, GPPPPG is GDP per capita growth, INFLA reflects inflation, HDI is Human Development Index (as they are set in Table 1), α0 is constant (intercept), α1,2,3,4,5,6,7 are the coefficients of the estimated parameters and ui,t is the error term. The variables TEMP and CO2 are considered in modelling in their form of first difference, temperature variation and CO2 emissions variation respectively.
System GMM (Arellano and Bond, 1991; Blundell and Bond, 1998; Roodman, 2009) was selected as the appropriate dynamic panel technique method for this study because it has the ability to address types of data such as those collected by us, in terms of panel size (21 years and 27 states) and adequately manages heteroscedasticity, serial correlation, cross-sectional dependence and endogeneity, respectively reverse causality problems between variables (Sarafidis and Wansbeek, 2012; Kumar et al., 2022; Asteriou et al., 2023; Gerged et al., 2023). We opted for the Generalized Method of Moments (GMM) over other methods for several key reasons:
1. GMM is well-suited to handle potential endogeneity issues, which arise when one or more explanatory variables are correlated with the error term. This is particularly relevant when studying dynamic relationships over time, as with the impact of climate change on healthcare expenditure. The VAR Granger panel analysis proven that there is causality between the analyzed variables, so the endogeneity is present, because the simultaneity is considered a marker of endogeneity (when two variables simultaneously influence each other) (Wintoki et al., 2012; Labras and Torrecillas, 2018; Chatterjee and Nag, 2023).
2. The study spans 2 decades (2000–2020), making the data both cross-sectional (across the European Union member states) and time-series. GMM is designed for such dynamic panel data, efficiently accounting for both within (across time for the same country) and between (across different countries) variations.
3. GMM can effectively use lagged values of variables as instruments, allowing the model to account for previous periods’ influence on current outcomes. This is especially valuable when studying cumulative effects, such as the long-term impact of CO2 emissions on healthcare spending.
The choice of GMM and panel VAR Granger causality methods for this study is motivated by the need to provide reliable and efficient estimates that consider potential endogeneity, capture the dynamic interrelations between variables, and ascertain the direction of causality, all while addressing the specific challenges and complexities posed by the study’s focus on the EU countries’ diverse landscape. One of the main advantages of the GMM method is its ability to manage endogeneity concerns. Given the potential for certain factors, like health expenditure, to be influenced by past values or other endogenous variables in the model, GMM is apt for such estimations. Moreover, the GMM estimator uses lagged values of the variables as instruments, which helps in achieving consistent and efficient estimates, especially when the panel has a short time dimension and a larger cross-sectional dimension, as in the case of 27 EU countries over 20 years. For heterogeneity point of view, GMM considers unobserved country-specific effects, which are crucial when analyzing diverse EU countries with varying histories, economies, and health systems. Regarding the Granger causality technique, it allows to establish the direction of causality between variables. In the context of climate change and health expenditure, it is imperative to discover if changes in climate indicators lead to variations in health spending, or vice versa. Also, panel VAR model is suitable to examine the dynamic interdependencies between multiple variables over time. Given that the study is not just about the direct impact of climate change but also about the moderating effects of economic, governance, or human development factors, a panel VAR can capture these complex interrelations.
To check the robustness and sensitivity of our findings, we have alternatively used instead of explanatory variables other indicators that capture similar facets of the same types of phenomena (e.g., GDP per capita growth, used interchangeably with GDP per capita, life expectancy used instead of Human Development or individual variables from Worldwide Governance Indicators studied alternately instead of the Governance variable, determined by the method of Principal Component Analysis from Worldwide Governance Indicators).
The data were preliminarily tested by analyzing the classical assumptions of regression models studied for the chosen variables: multicollinearity, stationarity, cross-sectional dependence, heteroskedasticity, cointegration, serial correlation and normality (Maladjian and Khoury, 2014). Attention has been paid to the phenomenon of endogeneity, which is not as often analyzed as would be required in econometric analyzes, because ignoring it can lead to inconsistent results (Ullah et al., 2018; Ibrahim and Arundina, 2022). Three major sources of endogeneity are presented in the literature: unobserved heterogeneity (when the relationship between two or more variables is influenced by an unobservable factor), simultaneity (when two variables simultaneously influence each other), and dynamic endogeneity (when the present value of a variable is influenced by itself, or other variables’ past values) (Wintoki et al., 2012; Labras and Torrecillas, 2018; Chatterjee and Nag, 2023). We applied PVAR Granger causation tests (Granger, 1969; Lopez and Weber, 2017), to study whether there is reverse causality between variables and we used the system GMM method, which takes into account the effect of lag of the dependent variable on it and has the potential to effectively manage endogeneity.
Econometric data were processed using STATA.
The descriptive statistics of the variables are presented in Table 2, which provides an overview of inhomogeneous developments between states and the period under review. The average HEALTHEXP value is 12.816%, ranges from 5.741% to 20.578%, with a standard deviation of 2.730, which denotes a medium dispersion from the mean. The analysis of the evolution of government health expenditures shows an increasing trend of their level in the analyzed period from year to year, less in 2020 compared to the previous year, behavior that proves to be atypical in this general pattern of growth of about 20 years and which must be understood amid the manifestations of the COVID-19 pandemic and related population mobility restrictions and which led to fewer cases of presentation of those who needed medical care in the medical system and thus generated lower costs. The year 2020 is also atypical in terms of average temperature values, which decreased compared to the previous year, amid the reduction of pollution attributable to mobility restrictions. As for climate change variables, they show significant differences between states. In the case of the annual average temperature, it presents a minimum value of 0.910°C and a maximum value of 20.350°C, explained by the geographical extent of the analyzed states and the existing climate types. CO2 emissions record values within a wide range, between 2.972 mt per capita and 25.610 mt per capita, significant differences between states and the analyzed period, with an average of 7.512 and a standard deviation of 3.509. The GOV variable, obtained through the Principal Component Analysis process (out of the six dimensions of Worldwide Governance Indicators), is between the minimum of −5.509 and the maximum of 4.157, with a standard deviation of 2.259, compared to the average of 0.000 and characterizes a group of nations differently governed and institutionally developed during the analyzed period. The macroeconomic variables, GDPPPG and INFLA, also characterize a conglomerate of heterogeneous states that have gone through different periods of developments. GDP per capita growth varies between negative values of −14,464% and maximum positive values of 23.201%, which illustrate a high degree of inequality in the evolution of the economies. Regarding the levels of economic development of the analyzed states, the chosen analysis horizon captures the 27 EU states in different stages of economic growth or recession, different levels of economic evolution, as well as recovery rates from various difficult situations. Inflation is between a minimum value of −4.478% and a maximum of 45.667% and given an average of 2.477. HDI presents smaller fluctuations in relation to the rest of the indicators, has an average of 0.866 and a standard deviation of 0.048.
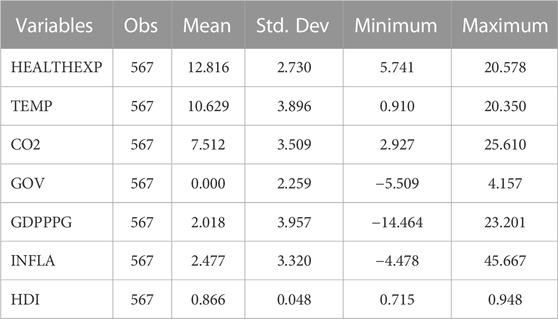
TABLE 2. Descriptive statistics.
The preliminary investigation of the variables starts with the analysis of multicollinearity between variables (Table 3), whose results denote that the variables are not correlated, the value of the correlation coefficients obtained being below the critical threshold (considered to be approximately 0.8) (Vatcheva et al., 2016). VIF (Variance Inflation Factor) was also studied, whose average value for the entire panel is 1.68 and with unit values of maximum 2.9, which indicates the absence of multicollinearity (Koengkan et al., 2019).
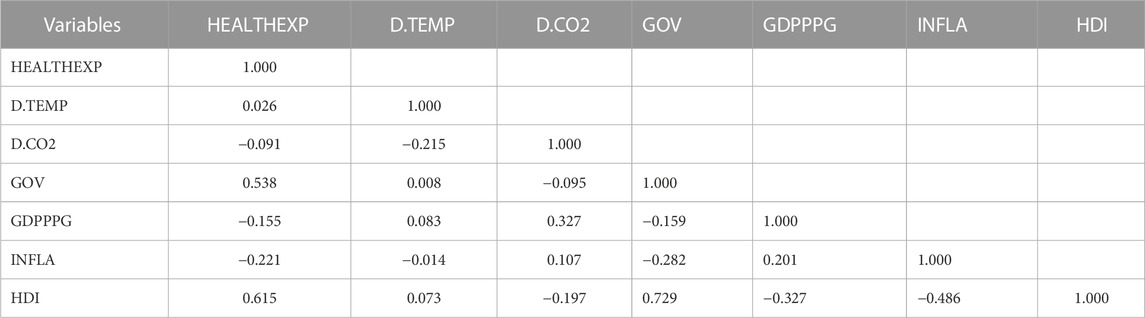
TABLE 3. Correlation matrix of the variables (multicollinearity).
The study of the stationarity of data (Table 4) was performed through the Levin-Lin-Chu (LLC) and the Phillips-Perron (PP) tests (with demean option for managing cross-sectional dependence) (Perron and Vogelsang, 1992; Levin et al., 2002). The null hypothesis that all panels contain unit roots is rejected for all variables and the stationarity is demonstrated. Cross-sectional dependence analysis (Table 4) was obtained with the Pesaran test (Pesaran, 2004), whose results indicate that the null hypothesis of cross-section independence is rejected, so the data are cross-sectionally dependent.
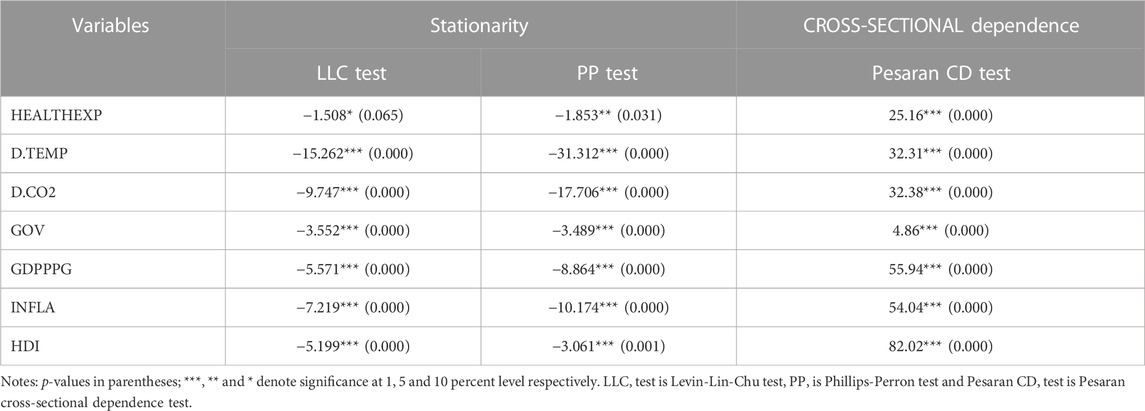
TABLE 4. Results of stationarity and cross-sectional dependence.
To test the heteroskedasticity, we used the White, Cameron & Trivedi (Cameron and Trivedi, 1990) and the Breusch-Pagan (Breusch and Pagan, 1979) tests, whose outcomes reveal that no heteroscedasticity in the residuals (Table 5). To study the premise of existence of a long-term equilibrium among variables, we performed the co-integration Pedroni (Pedroni, 2004) and Westerlund (Westerlund, 2005) tests, whose results (Table 6) prove the presence of a long-term co-integration relationship between variables. The serial correlation is studied through the Wooldridge test (Wooldridge, 2002; Drukker, 2003), which proves that the null hypothesis of no serial correlation is rejected and that there is serial correlation in our data (Table 7). The normality based on skewness and kurtosis was performed and denotes that all variables are normally distributed, except for HEALTHEXP is not normally distributed (Table 8).
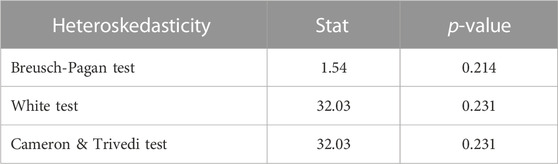
TABLE 5. Results of heteroskedasticity.

TABLE 6. Results of cointegration tests.

TABLE 7. Results of serial correlation test.

TABLE 8. Results of normality test.
Reverse causality between variables (Table 9), based on Granger PVAR tests (Lopez and Weber, 2017), illustrates important two-way causality between TEMP and GDPPPG, which are mutually affected. Also, bidirectional causalities were obtained for variables CO2—INFLA and INFLA-HDI. The outputs reveal that HEALTHEXP is influenced by GDPPPG, while HEALTHEXP influences HDI, which in turn causes CO2. An important relationship was obtained for CO2 influencing TEMP. The results also show that INFLA and HDI cause GDPPG.
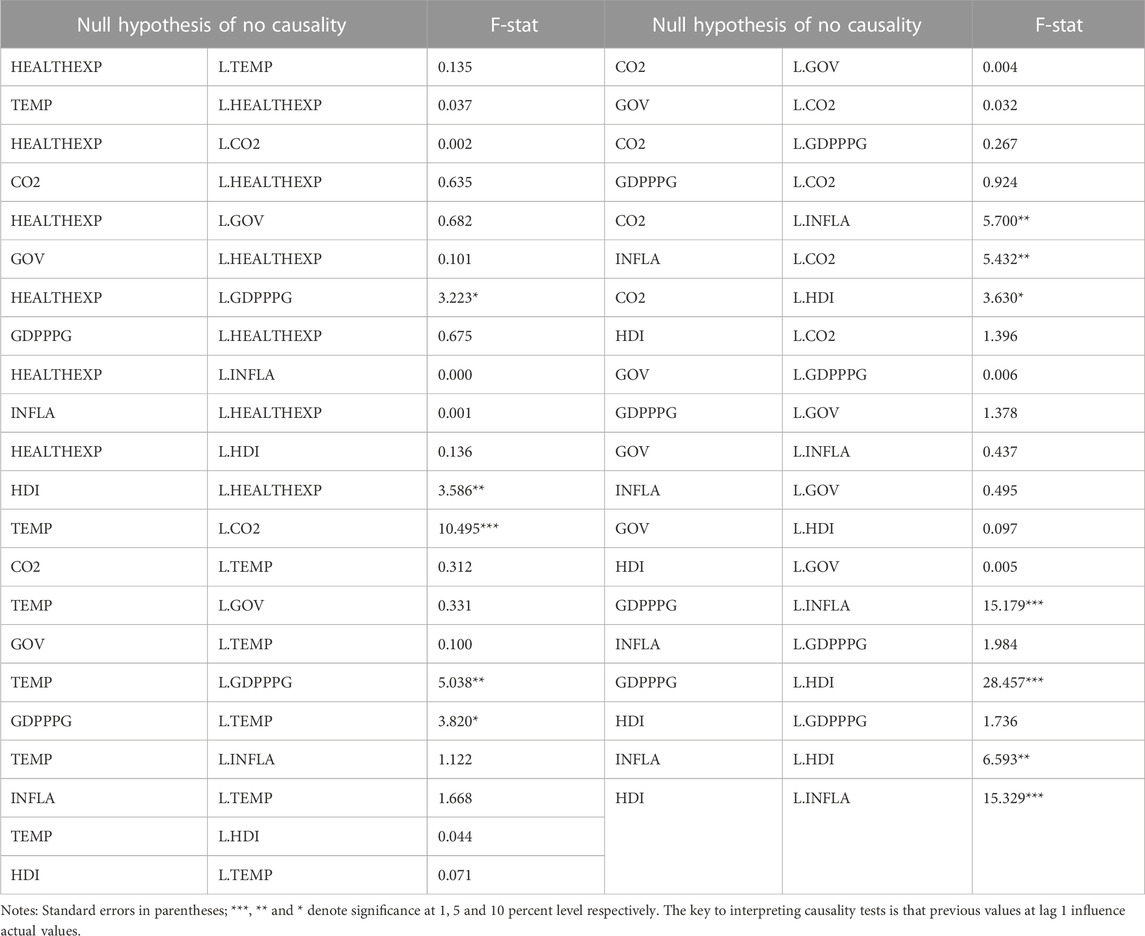
TABLE 9. PVAR Granger causality between variables.
Several important findings arise from our reverse causality analysis. First, it follows that CO2 emissions influence temperature. Global warming is an essential topic of current environmental policies and underlines the importance of shaping economic and sustainable development policies that contribute to lowering CO2 emissions. Such a demonstrated link between CO2 and temperature proves the importance of studying climate change variables as comprehensively as possible. The analysis also found that GDP per capita growth and temperature influence each other, confirming the results of previous climate-change economic literature and showing the interdependencies between economic growth and temperature. Human development influences CO2 emissions, but also GDP per capita growth. In turn, GDP per capita growth influences health expenditure, which causes human development. The interdependencies between the analyzed variables are numerous and represent arguments of the combined analysis of climate change, economic, governance and human development variables.
Once the causality between the mentioned variables was established, the two-step system GMM analysis was put into practice by successively testing several models that analyze the impact of climate change on health expenditure, based on dynamic panel models (Table 10). The post-estimation analysis of the two-step system GMM models proves that the p-values of the Hansen tests accept the null hypothesis of overidentifying restrictions (Labras and Torrecillas, 2018). The value of the Wald tests sustains the goodness of fit models, and the second-order no-autocorrelation hypothesis is not rejected by the Arellano and Bond tests for autocorrelation AR (2), whereas AR (1) is significant, confirming the serial autocorrelation in the errors.
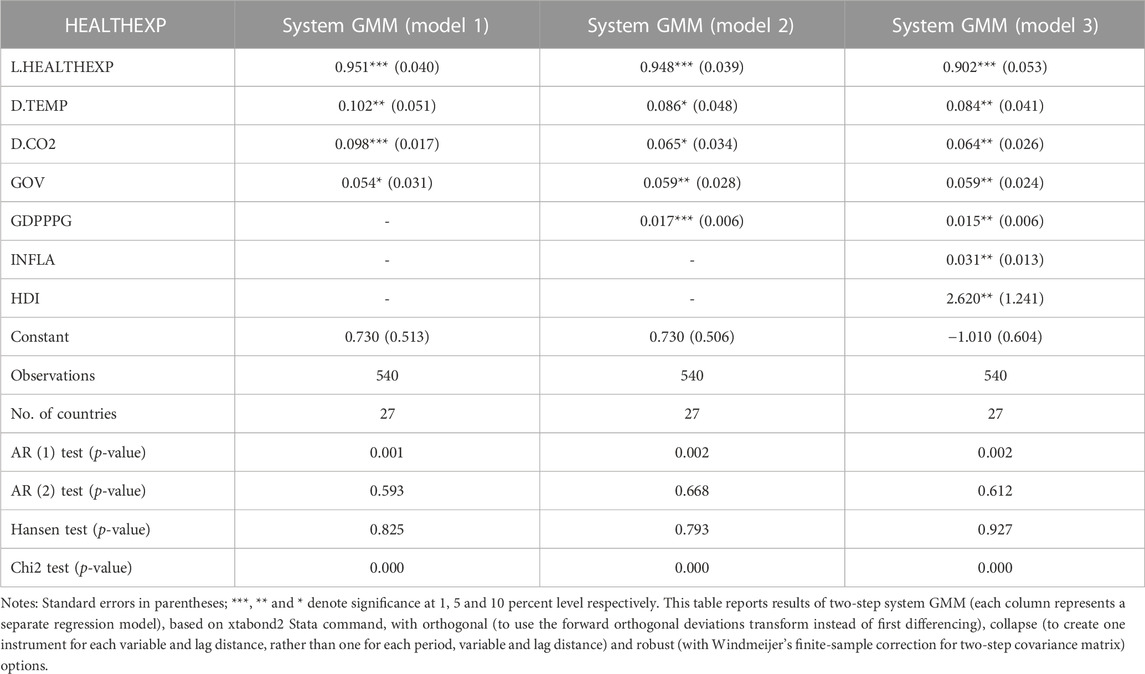
TABLE 10. The effect of climate change on health expenditure (system GMM models).
The importance and influence of climate change on health expenditures are significant in all estimated models. The results obtained for each of the analyzed independent variables are detailed below. We obtain the dynamic persistence of health expenditure and confirm the dynamic specification of the models with statistically significant lag1 for health expenditure, which provides a positive correlation between HEALTHEXPit-1 and HEALTHEXP itself.
Temperature and health expenditure. The results based on system GMM models reveal that increasing the average temperature has a positive and significant impact on health expenditure in the sample countries. These results confirm that H1 hypothesis can be accepted. Hypothesis H1 implied that rising temperatures lead to increased government health spending.
The surge in global temperatures activates biological mechanisms like oxidative stress, contributing to neurodegenerative conditions (Zammit et al., 2021). Concurrently, heatwaves increase the incidence of heat-related ailments, such as heat exhaustion, requiring urgent medical care and straining healthcare finances (Tong et al., 2021). Hospitals often see a spike in admissions during such events, adding financial burden to healthcare systems (Boz and Ozsari, 2020). Warmer climates also expand the habitats of disease vectors like mosquitoes, facilitating the spread of maladies like malaria into new areas (Chowdhury et al., 2018). This necessitates additional public health measures, thereby escalating healthcare costs. Furthermore, climate change poses infrastructural challenges; hospitals may need to enhance cooling systems for heatwaves, and storms can cause facility damage, necessitating costly repairs (Sasmaz et al., 2021). Therefore, it is crucial for governments to integrate these climate-related health risks into healthcare planning, including preventive measures and infrastructure upgrades, to manage the increasing financial strain on healthcare systems (Schneider and Breitner, 2016).
CO2 and health expenditure. In the GMM models, we find that the growth of CO2 emissions contribute to higher health spending, thus validating the H2 hypothesis. Hypothesis H2 referred to the fact that increasing CO2 emissions lead to increased government health spending.
Our study reveals a direct correlation between the growth in CO2 emissions and a subsequent escalation in healthcare expenditures incurred by the government. This relationship underscores the economic implications of environmental factors on public health budgets. This result is consistent with previous studies: (Samah et al., 2020), Gündüz (2020), Oyelade et al. (2020), Taghizadeh-Hesary and Taghizadeh-Hesary (2020), Akbar et al. (2021), Li et al. (2022), Travassos et al. (2020), Jerrett et al. (2003), Jia et al. (2021), Khoshnevis and Khanalizadeh (2017).
Rising CO2 emissions boost healthcare costs by aggravating air quality, increasing respiratory issues, and causing more extreme weather events that result in injuries and worsen chronic conditions. These factors together amplify the financial burden on healthcare systems. These elements collectively burden healthcare systems and escalate spending (González et al., 2014). Moreover, climate change-driven migration can lead to population surges in less-affected regions, adding further strain on healthcare infrastructure and increasing expenditures (Li et al., 2022). Climate change worsens air quality and elevates ground-level ozone, intensifying urban respiratory issues. Addressing these health challenges requires both medical treatments and environmental control measures, leading to increased healthcare costs (Ballester et al., 2023).
Governance and health expenditure. The results of our study reveal positive results between government spending on health and governance, results that coincide with previous studies (Jakovljevic et al., 2016; Kaur, 2020; Ray and Linden, 2020).
Strong governance plays a pivotal role in healthcare, influencing everything from resource allocation to policy formulation in both developed and developing countries (Nakatani et al., 2023). Effective governance structures contribute to creating comprehensive, well-financed healthcare policies that aim to improve not just infrastructure but also address systemic issues like health inequality. A transparent and efficient tax system under good governance can generate increased public revenue, a portion of which can be channeled into healthcare. Moreover, governance significantly impacts the regulatory landscape, setting the stage for effective control of healthcare prices, service quality, and professional conduct (Raeesi et al., 2018). This regulatory oversight helps manage costs while enhancing the effectiveness of healthcare services. In the international arena, good governance can facilitate partnerships with other nations or global organizations, securing additional funding or expertise that leads to more effective and efficient healthcare spending (Kochuvilayil et al., 2023). Lastly, the role of governance becomes particularly critical during crises, as evidenced during the COVID-19 pandemic. Well-governed countries were more effective in securing necessary healthcare funding in times of crisis, ensuring the continuity and quality of care (Makin and Layton, 2021).
GDP and health expenditure. A robust GDP often serves as a catalyst for enhanced healthcare spending in multiple ways. First, it allows for greater allocations in both public and private healthcare sectors, enabling the adoption of more advanced treatments and facilities (Onisanwa, 2014). This is especially true in wealthier countries, which typically dedicate a larger portion of their budget to improve the quality and availability of healthcare (Barati and Hadiseh, 2020). As GDP growth enhances individual purchasing power, it renders healthcare services more accessible to the general population. This increased financial capability not only allows people to seek medical care more readily but also encourages investment in preventative care (Chaabouni and Saidi, 2017) and more expensive treatment options. In a stable economic environment fostered by a strong GDP, there’s an attraction for investment in healthcare infrastructure such as hospitals and research centers (Rodríguez and Nieves Valdés, 2019). These facilities require sustained spending for their upkeep and staffing. Additionally, a high GDP typically boosts government revenue through taxation. This additional revenue can be channeled into public health initiatives, vaccination programs, and subsidized healthcare, thereby elevating overall healthcare expenditure across the board.
Inflation and health expenditure. Existing studies find that the relationship between health spending and inflation is positive: inflation significantly increases health spending. The results of our study are identical to Azam and Awan. (2022); Siami-Namini (2018); Dunn et al. (2018); Yip et al. (2017); Cheng and Nopphol (2019); Koijen et al. (2016); De la Maisonneuve et al. (2017) and Jakovljevic et al. (2017).
Rising inflation boosts costs in goods, services, and healthcare alike. This rise inflates the operational costs for healthcare providers, impacting everything from medical supplies to medications and labor costs. Consequently, patients often face higher out-of-pocket expenses, making healthcare less affordable (Dunn et al., 2018). On the public funding side, if governmental healthcare budgets remain stagnant amid rising inflation, the real value of that funding diminishes, potentially leading to a decline in the quality of healthcare services due to resource scarcity (Yip et al., 2017). Such a scenario could necessitate cuts in services, reduced staffing levels, or limitations on the availability of new, more effective but costlier treatments (Cheng and Nopphol, 2019).
Inflation also has an impact on income levels, as nominal wage growth may not keep up, affecting the affordability of healthcare, especially for fixed-income groups like retirees. The rising costs of healthcare can consume an increasingly large portion of their limited incomes (De la Maisonneuve et al., 2017; Jakovljevic et al., 2017).
Human development and health expenditure. The progression of human development significantly impacts healthcare expenditures in various ways. An aging population due to increased life expectancy necessitates more medical care, thereby elevating costs (Brooks et al., 2005). With societal advancement, the adoption of costly medical technologies becomes more widespread. Government initiatives to expand public healthcare in developed countries also contribute to rising health budgets (Miranda-Lescano et al., 2023). Urbanization, a development byproduct, poses unique health challenges like stress and pollution, requiring specialized and often expensive services (Shao et al., 2022; Lin and Guo, 2023). Furthermore, increased global interconnectedness exposes countries to risks like pandemics, requiring substantial healthcare spending (Pervaiz et al., 2021).
To check the robustness and sensitivity of our baseline results, we use several alternative explanatory variables and perform two-step system GMM models (Table 11). Three of the Worldwide Governance Indicators variables (Voice and accountability VOICE, Political stability and absence of violence/terrorism POLSTAB, Government effectiveness GOVEF) were used separately instead of the GOV variable (obtained by the Principal Component Analysis method from the six Worldwide Governance Indicators). For macroeconomic factors, Gross Domestic Product growth (GDPG, annual%) was used as a substitute of Gross Domestic Product per capita growth. For the HDI variable, robustness tests were performed using the Life expectancy indicator (lnLIFE, its logarithm form). The results obtained through robustness tests and based on alternative variables indicate the same meanings of climate change impact on health expenditure, but also of control variables on the dependent variable that render health spending.
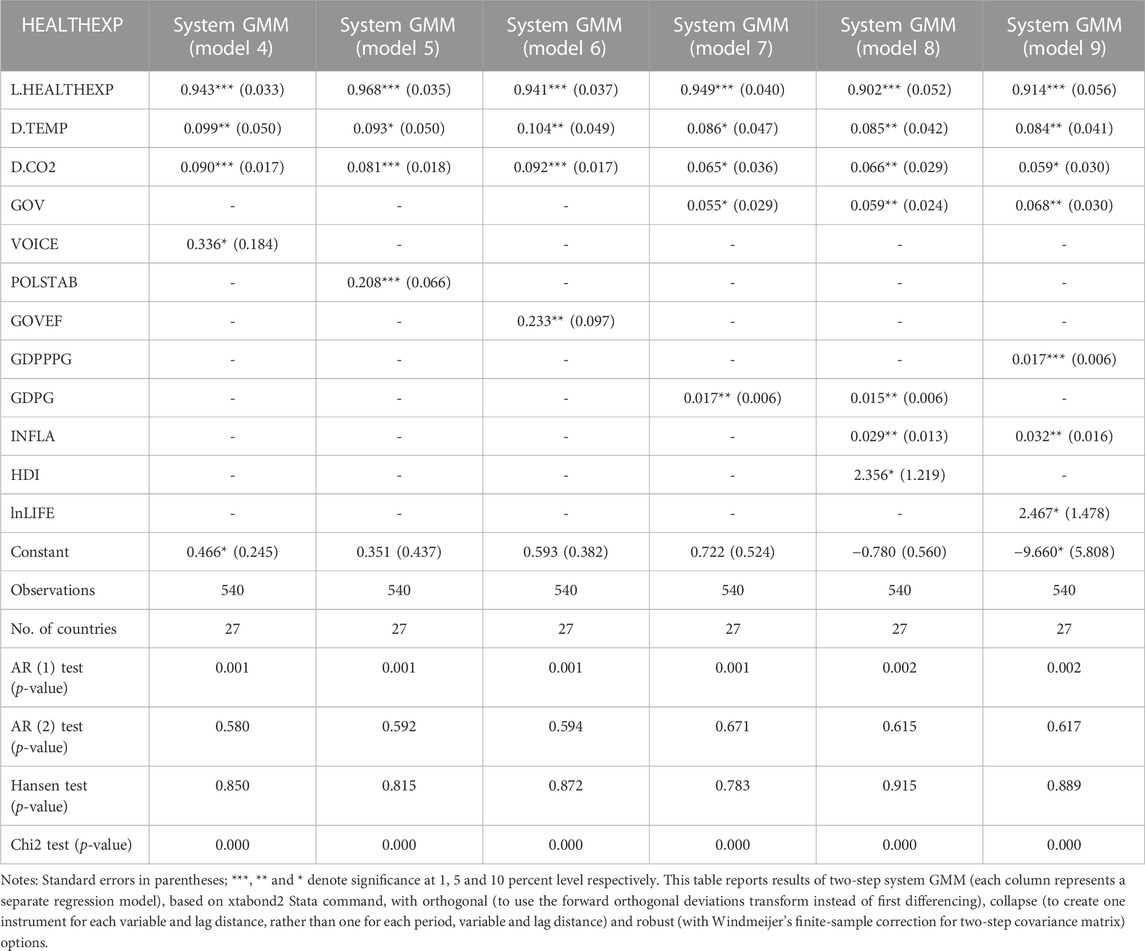
TABLE 11. The results of robustness tests (system GMM models).
The connection between temperature fluctuations and government health spending is multifaceted and shaped by a mix of direct and indirect elements. The effects stretch beyond immediate health consequences, encompassing wider environmental, social, and economic considerations. Recognizing this link is vital for policymakers since it emphasizes the urgent need to intertwine climate-related issues within healthcare strategies and policies. By comprehending the diverse impacts of temperature on health, governments can devise comprehensive solutions that simultaneously tend to urgent health requirements and contribute to overall societal prosperity. The escalation in both the frequency and severity of temperature extremes requires a prompt, all-encompassing response. Necessary measures include significant investment in healthcare facilities, the execution of public health drives, the creation of early warning systems, and dedicated strategies for at-risk groups. These initiatives form a vital part of a strategy to alleviate the health effects of temperature variations and the ensuing costs. With growing evidence of the ties between temperature changes and healthcare expenditure, this subject is set to remain a paramount concern for governments, healthcare entities, and policymakers alike. It illustrates compellingly how climatic shifts can create tangible fiscal impacts on public health and serves as a clarion call for a unified, forward-thinking approach.
Patz et al. (2014) noted that by 2050 the Earth’s temperature will increase to an average of 32C°. The human population will face more health problems, the health sector will be severely affected by the temperature. Regarding the relationship between CO2 and health expenditure, if CO2 emissions are not effectively reduced, increased medical spending can improve people’s health. Thus, we can suggest that the governments of EU Member States increase health spending because only in this way can citizens’ health improve and increase the stock of healthy human capital. While economic growth is crucial for EU countries, it should not compromise environmental integrity or the wellbeing of future generations. Improved public health is integral to this equation, as it correlates with economic efficiency and growth. Policymakers are increasingly recognizing the need for robust public health strategies. Evidence shows that nations with better economic and environmental conditions also enjoy superior health outcomes (Rodríguez and Nieves Valdés, 2019; Barati and Hadiseh, 2020). Additionally, cutting greenhouse gas emissions yields significant health benefits, including lower costs for environmental mitigation, thereby offering a compelling reason for immediate action. The overarching implication is that sustainable development should be the focal point for policymakers, ensuring a balanced approach that does not jeopardize future generations. Governments should avoid supporting economic activities that pollute the environment, as this not only negatively impacts human health but also leads to increased expenditures on both pollution control and healthcare.
Policy recommendations. By implementing some recommendations, policymakers can better prepare for and mitigate the impacts of climate change on health expenditures, ultimately leading to more sustainable and resilient healthcare systems and societies.
The policy recommendations derived from the findings of this study can be summarized into several key areas, each addressing the interplay between climate change, economic factors, and health expenditures. The focus of these recommendations is to guide policymakers in mitigating the impacts of climate change on healthcare systems and economies:
1. Strengthen Environmental Regulations: Given the direct correlation between CO2 emissions and rising health costs, policies should target reducing emissions through stricter environmental regulations (Ballester et al., 2023). This includes promoting renewable energy sources, enhancing energy efficiency, and encouraging sustainable practices across industries.
2. Healthcare System Resilience and Adaptation: Governments need to invest in making healthcare systems more resilient to climate change impacts. The governments must upgrade infrastructure for extreme weather (Sasmaz et al., 2021), expand capacity for higher patient numbers during heatwaves or pollution crises, and ensure sufficient medical supplies.
3. Public Health Initiatives: Launching public health initiatives aimed at prevention and education to lessen climate change’s health effects, including heatwave warnings, campaigns on risks of extreme temperatures, and efforts to curb vector-borne diseases.
4. Climate-Integrated Healthcare Planning: The governments should integrate climate change considerations into healthcare planning and policy formulation, assessing its potential health impacts and incorporating these into national and local healthcare strategies.
5. Economic Policies for Sustainable Growth: Formulating and enacting economic policies for sustainable growth, mindful of climate impact, by investing in green technology, backing sustainable agriculture, and favoring low-footprint industries.
6. Governance and Policy Enforcement: Strengthen governance structures to ensure effective implementation and enforcement of policies related to climate change and healthcare. This also involves ensuring transparency and accountability in the use of funds allocated for climate change adaptation and health expenditure.
7Addressing Inflation and Healthcare Costs: Creating strategies to handle inflation’s effect on healthcare costs (Azam and Awan, 2022), including price regulation for medical essentials and boosting public healthcare funding to counteract escalating expenses.
8. Focus on Human Development: Focusing on policies enhancing human development like education, healthcare access, and poverty alleviation, directly improving health outcomes and reducing climate change-related healthcare costs.
Our study provides important insights in line with previous literature and contribute in several ways to the actual stage of knowledge by examining the critical relationship between climate change, specifically temperature and CO2 levels, and governmental healthcare spending across EU countries. First, we use an empirical framework that simultaneously examines the effects of climate change, economic, governance and human proxies on health governmental spending. These problems have sometimes been analyzed individually and at other times in different combinations; however, to our knowledge, no study has included these variables as factors of influence. Moreover, it is essential to simultaneously analyze the impact of these factors on health expenditure to avoid identifying false associations. Second, by focusing on the time frame of 2000–2020, the study uncovers new insights and sheds light on how environmental factors directly influence healthcare economics. Third, the study considers relevant control variables like governance, macroeconomic factors, and human development, that adds further depth to the understanding of the dynamics between climate change and health governmental spending. This study contributes to a better understanding of the role of climate change, macroeconomic, governance institutional and human factors in health spending and it can be valuable for policymakers in shaping legislative frameworks and public policies that compete with both increasing the quality of healthcare, mitigating environmental issues, economic growth, strengthening institutional governance of states, and increasing human development.
This study investigates the impact of climate change on health expenditure in the European Union countries, between 2000 and 2020, and examines the moderating roles of several control variables, respectively countries’ governance indicators, macroeconomic determinants (GDP per capita growth and inflation) and human development. To capture the climate change, two indicators were used, which are intensely considered as markers of global warming and whose valences are recognized in the previous literature: temperature and CO2 emissions. The results were obtained through dynamic system GMM and PVAR Granger causality methods.
We find that climate change, quantified by the increase in average temperature and CO2 emissions, burdens the health systems of the European Union countries. The results that prove the positive correlation between climate change and health spending are in line with the previous literature which emphasized the importance of climate change mitigation. Elevated global temperatures and CO2 levels not only exacerbate existing health issues but also create new challenges, such as heat-related illnesses and the spread of diseases like malaria. These lead to additional healthcare costs. There is a direct correlation between rising levels of CO2 emissions and increased governmental healthcare spending. This emphasizes the need for environmental considerations in public health budget planning.
Our comprehensive approach addresses the multifaceted relationship between various factors and healthcare expenditures, through the estimating impact of several variables (governance, macroeconomic indicators and human development) on health expenditure. Effective governance contributes to efficient healthcare spending and is crucial for the formulation of policies that address not just immediate healthcare needs but also systemic issues like health inequality. A robust GDP generally leads to increased healthcare spending, while rising inflation makes healthcare less affordable for the general population and may lead to reduced quality in healthcare services if public funding does not keep pace. With societal progress, healthcare expenditures often increase, driven by factors like an older population, advancements in medical technology, and health issues related to urban living.
This study has theoretical and practical implications. Each government is responsible for ensuring healthy air quality for its population. Viewing climate change solely as an environmental or developmental issue overlooks its considerable impact on both public health and national healthcare budgets, impacts that are expected to increase in the near term. A deeper grasp of how climate change influences healthcare costs can improve both policy direction and decision-making. We consider that holistic planning needed, given the complexity and interconnectedness of these factors, there is an urgent need for integrated, multi-dimensional planning that considers all these variables in healthcare budgeting and policy formulation.
This study’s findings are instrumental for policymakers, providing a nuanced understanding of the various factors that contribute to rising healthcare expenditures. Understanding the relationship between healthcare spending and climate change is crucial for policymakers and regulators to create a legislative environment that helps reduce global warming and does not put pressure on government health spending. Against the background of global warming and results demonstrating the increasing pressure on health systems, generated by climate change and pollution, the role of regulators is to urgently configure, implement and monitor a regulatory framework that contributes both to environmental conservation and increasing the capacity of health systems to manage patients’ problems. Other extensive categories directly interested in the studied issues are citizens of the entire planet, whose interests converge health preservation and favorable environmental conditions, that do not contribute to diseases or medical problems.
A first limit of research refers to the study of a single conglomerate of countries (the European Union) and expanding the research area could contribute to obtaining relevant results for other groupings of states. The availability of data on health expenditure in the European Union has not allowed the research period to be extended. Future research directions involve both the extension of the researched area, the analysis period, as well as the study of other typologies of relationships between health variables and those that characterize climate change. The range of both categories of indicators mentioned is wide and refers to: medical infrastructure, health policies, seasonal temperature, high and low temperatures, greenhouse gases, ocean heat, sea level, glaciers, etc.
Publicly available datasets were analyzed in this study. This data can be found here: https://databank.worldbank.org/source/world-development-indicators, https://climateknowledgeportal. worldbank.org/download-data and https://hdr.undp.org/data-center/documentation-and-downloads.
AS: Conceptualization, Formal Analysis, Investigation, Methodology, Supervision, Validation, Visualization, Writing–original draft, Writing–review and editing. HI: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Supervision, Validation, Visualization, Writing–original draft, Writing–review and editing. DS: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Supervision, Validation, Visualization, Writing–original draft, Writing–review and editing. ICI: Conceptualization, Formal Analysis, Investigation, Methodology, Supervision, Validation, Visualization, Writing–original draft, Writing–review and editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. Publication fee is covered by “1 Decembrie 1918” University of Alba Iulia.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Akbar, M., Hussain, A., Akbar, A., and Ullah, I. (2021). The dynamic association between healthcare spending, CO2 emissions, and human development index in OECD countries: evidence from panel VAR model. Environ. Dev. Sustain. A Multidiscip. Approach Theory Pract. Sustain. Dev. 23 (7), 10470–10489. doi:10.1007/s10668-020-01066-5
Arellano, M., and Bond, S. (1991). Some tests of specification for panel data: Monte Carlo evidence and an application to employment equations. Rev. Econ. Stud. 58 (2), 277–297. doi:10.2307/2297968
Asteriou, D., Spanos, K., and Trachanas, E. (2023). Financial development, economic growth and the role of fiscal policy during normal and stress times: evidence for 26 EU countries. Int. J. Finance Econ. 1–20. doi:10.1002/ijfe.2793
Åström, C., Orru, H., Rocklöv, J., Strandberg, G., Ebi, K. L., and Bertil, F. (2013). Heat-related respiratory hospital admissions in Europe in a changing climate: a health impact assessment. BMJ Open 3 (1), e001842. doi:10.1136/bmjopen-2012-001842
Azam, M., and Awan, A. M. (2022). Health is wealth: a dynamic sur approach of examining a link between climate changes and human health expenditures. Soc. Indic. Res. 163, 505–528. doi:10.1007/s11205-022-02904-x
Ballester, J., Quijal-Zamorano, M., Méndez Turrubiates, R. F., Pegenaute, F., Herrmann, F. R., Robine, J. M., et al. (2023). Heat-related mortality in Europe during the summer of 2022. Nat. Med. 29, 1857–1866. doi:10.1038/s41591-023-02419-z
Barati, M., and Hadiseh, F. (2020). Asymmetric effect of income on the US healthcare expenditure: evidence from the nonlinear autoregressive distributed lag (ARDL) approach. Empir. Econ. 58 (4), 1979–2008. doi:10.1007/s00181-018-1604-7
Beatty, T. K., and Shimshack, J. P. (2014). Air pollution and children's respiratory health: a cohort analysis. J. Environ. Econ. Manag. 67, 39–57. doi:10.1016/j.jeem.2013.10.002
Biadgilign, S., Ayenew, H. Y., Shumetie, A., Chitekwe, S., Tolla, A., Haile, D., et al. (2019). Good governance, public health expenditures, urbanization and child undernutrition nexus in Ethiopia: an ecological analysis. Bmc Health Serv. Res. 19, 40–10. doi:10.1186/s12913-018-3822-2
Blundell, R., and Bond, S. (1998). Initial conditions and moment restrictions in dynamic panel data models. J. Econ. 87 (1), 115–143. doi:10.1016/S0304-4076(98)00009-8
Boz, C., and Ozsari, S. H. (2020). The causes of aging and relationship between aging and health expenditure: an econometric causality analysis for Turkey. Int. J. Health Plan. Manag. 35 (1), 162–170. doi:10.1002/hpm.2845
Breusch, T. S., and Pagan, A. R. (1979). A simple test for heteroscedasticity and random coefficient variation. Econometrica 47, 1287–1294. doi:10.2307/1911963
Brooks, N., Adger, W. N., and Kelly, P. M. (2005). The determinants of vulnerability and adaptive capacity at the national level and the implications for adaptation. Glob. Environ. Chang. 15 (2), 151–163. doi:10.1016/j.gloenvcha.2004.12.006
Cameron, A. C., and Trivedi, P. K. (1990). The information matrix test and its applied alternative hypotheses. University of California–Davis, Institute of Governmental Affairs. Working paper 372.
Cengiz, O., and Manga, M. (2022). Is there any relationshiop between geopolitical risk and climate change? Ekon. Vjesn. 35 (1), 99–112. doi:10.51680/ev.35.1.8
Chaabouni, S., and Saidi, K. (2017). The dynamic links between carbon dioxide (CO2) emissions, health spending and GDP growth: a case study for 51 countries. Environ. Res. 158, 137–144. doi:10.1016/j.envres.2017.05.041
Chaabouni, S., Zghidi, N., and Mbarek, M. B. (2016). On the causal dynamics between CO2 emissions, health expenditures and economic growth. Sustain. Cities Soc. 22, 184–191. doi:10.1016/j.scs.2016.02.001
Chatterjee, C., and Nag, T. (2023). Do women boards enhance firm performance? Evidence from top Indian companies. Int. J. Discl. Gov. 20, 155–167. doi:10.1057/s41310-022-00153-5
Cheng, C. H. J., and Nopphol, W. (2019). Health care policy uncertainty, real health expenditures and health care inflation in the USA. Empir. Econ. 60 (4), 1–21. doi:10.1007/s00181-019-01818-x
Chishti, M. Z., Arfaoui, N., and Cheong, C. (2023a). Exploring the time-varying asymmetric effects of environmental regulation policies and human capital on sustainable development efficiency: a province level evidence from China. Energy Econ. 126, 106922. doi:10.1016/j.eneco.2023.106922
Chishti, M. Z., Dogan, E., and Zaman, U. (2023b). Effects of the circular economy, environmental policy, energy transition, and geopolitical risk on sustainable electricity generation. Util. Policy 82, 101585. doi:10.1016/j.jup.2023.101585
Chishti, M. Z., Khalid, A. K., and Sana, M. (2023c). Conflict vs sustainability of global energy, agricultural and metal markets: a lesson from Ukraine-Russia war. Resour. Policy 84, 103775. doi:10.1016/j.resourpol.2023.103775
Chishti, M. Z., and Patel, R. (2023). Breaking the climate deadlock: leveraging the effects of natural resources on climate technologies to achieve COP26 targets. Resour. Policy 82, 103576. doi:10.1016/j.resourpol.2023.103576
Chowdhury, F. R., Ibrahim, Q. S. U., Bari, M. S., Alam, M. J., Dunachie, S. J., Rodriguez-Morales, A. J., et al. (2018). The association between temperature, rainfall and humidity with common climate-sensitive infectious diseases in Bangladesh. PLoS ONE 13, e0199579. doi:10.1371/journal.pone.0199579
De la Maisonneuve, C., Moreno-Serra, R., Murtin, F., and Martins, J. O. (2017). The role of policy and institutions on health spending. Health Econ. 26 (7), 834–843. doi:10.1002/hec.3410
Drukker, D. M. (2003). Testing for serial correlation in linear panel-data models. Stata J. 3 (2), 168–177. doi:10.1177/1536867X0300300206
Dunn, A., Grosse, S. D., and Zuvekas, S. H. (2018). Adjusting health expenditures for inflation: a review of measures for health services research in the United States. Health Serv. Res. 53 (1), 175–196. doi:10.1111/1475-6773.12612
Efthalitsidou, K., Zafeiriou, E., Spinthiropoulos, K., Betsas, I., and Sariannidis, N. (2021). GDP and public expenditure in education, health, and defense. Empirical research for Greece. Empir. Res. Greece Math. 9 (18), 2319. doi:10.3390/math9182319
European Comission (2022). European state of the climate 2022. Copernicus. https://climate.copernicus.eu/esotc/2022.
European Commission (2022). Climate indicators: temperature. Copernicus. https://climate.copernicus.eu/climate-indicators/temperature.
European Environment Agency (2022). Premature deaths due to exposure to fine particulate matter in Europe. https://www.eea.europa.eu/ims/health-impacts-of-exposure-to.
European Parliament (2018). Climate change in Europe. https://www.europarl.europa.eu/news/en/headlines/society/20180703STO07123/climate-change-in-europe-facts-and- figures.
European Parliament (2023a). Climate change in Europe: facts and figures. https://www.europarl.europa.eu/news/en/headlines/society/20180703STO07123/climate-change-in-europe-facts-and-figures.
European Parliament (2023b). EU progress towards its 2020. https://www.europarl.europa.eu/news/en/headlines/priorities/climate-change/20180706STO07407/eu-progress-towards-2020-climate-change-goals-infographic.
European Parliament (2023c). Green Deal: key to a climate-neutral and sustainable EU. https://www.europarl.europa.eu/news/en/headlines/society/20200618STO81513/green-deal-key-to-a-climate-neutral-and-sustainable-eu.
Firdaus, R., Xue, Y., Gang, L., and Sibt e Ali, M. (2022). Artificial intelligence and human psychology in online transaction fraud. Front. Psychol. 13, 947234. doi:10.3389/fpsyg.2022.947234
Fotourehchi, Z., and Çalışkan, Z. (2018). Is it possible to describe a Kuznets curve for health outcomes? An empirical investigation. Panoeconomicus 65 (2), 227–238. doi:10.2298/PAN150814011F
Gerged, A. M., Beddewela, E. S., and Cowton, C. J. (2023). Does the quality of country-level governance have an impact on corporate environmental disclosure? Evidence from Gulf Cooperation Council countries. Int. J. Finance Econ. 28, 1179–1200. doi:10.1002/ijfe.2469
González, P. F., Landajo, M., and Presno, M. J. (2014). The driving forces behind changes in CO2 emission levels in EU-27. Differences between member states. Environ. Sci. Policy 38, 11–16. doi:10.1016/j.envsci.2013.10.007
Granger, C. W. J. (1969). Investigating causal relations by econometric models and cross-spectral methods. Econometrica 37, 424–438. doi:10.2307/1912791
Gündüz, M. (2020). Healthcare expenditure and carbon footprint in the USA: evidence from hidden cointegration approach. Eur. J. Health Econ. 21 (5), 801–811. doi:10.1007/s10198-020-01174-z
Hayashi, K., Fujimoto, M., and Nishiura, H. (2022). Quantifying the future risk of dengue under climate change in Japan. Front. Public Health 10, 959312. doi:10.3389/fpubh.2022.959312
Ibrahim, M., and Arundina, T. (2022). Practical panel modelling. Gedung Permata Kuningan, PH Level: Publisher National Committee of Islamic Economy and Finance (KNEKS) KNEKS Headquarter Office. Available at: https://kneks.go.id/storage/upload/1675248927-[FINAL]%20Practional%20Panel%20Modeling%20-%20Applications%20in%20Islamic%20Banking%20and%20Finance_PDF.pdf.
IPCC (2021). “Working group 1: the physical science basis,” in Climate change 2021: the physical science basis. Editor V. Masson-Delmotte (Cambridge University Press).
Isen, A., Rossin-Slater, M., and Walker, W. R. (2017). Every breath you take—every dollar you’ll make: the long-term consequences of the clean air act of 1970. J. Political Econ. 125 (3), 848–902. doi:10.1086/691465
Jakovljevic, M., Potapchik, E., Popovich, L., Barik, D., and Getzen, T. E. (2017). Evolving health expenditure landscape of the BRICS nations and projections to 2025. Health Econ. 26 (7), 844–852. doi:10.1002/hec.3406
Jakovljevic, M. B., Vukovic, M., and Fontanesi, J. (2016). Life expectancy and health expenditure evolution in Eastern Europe—DiD and DEA analysis. Expert Rev. Pharm. Outcomes Res. 16 (4), 537–546. doi:10.1586/14737167.2016.1125293
Javaid, M. Q., Ximei, K., Irfan, M., Sibt-e-Ali, M., and Shams, T. (2023). Exploring the nonlinear relationship among financial development, human capital and CO2 emissions: a comparative study of South and East Asian emerging economies. Environ. Sci. Pollut. Res. 30, 87274–87285. doi:10.1007/s11356-023-28512-x
Jerrett, M., Eyles, J., Dufournaud, C., and Birch, S. (2003). Environmental influences on healthcare expenditures: an exploratory analysis from Ontario, Canada. J. Epidemiol. Community Health 57 (5), 334–338. doi:10.1136/jech.57.5.334
Jia, H., Jiang, H., Yu, J., Zhang, J., Cao, P., and Yu, X. (2021). Total health expenditure and its driving factors in China: a gray theory analysis. Healthcare 9 (2), 207. doi:10.3390/healthcare9020207
Karahasan, B. C., and Pinar, M. (2023). Climate change and spatial agricultural development in Turkey. Rev. Dev. Econ. 27 (3), 1699–1720. doi:10.1111/rode.12986
Kaur, A. (2020). Health status, government health expenditure and economic growth nexus in India: a toda–yamamoto causality approach. Arthaniti J. Econ. Theory Pract. 22 (1), 34–46. doi:10.1177/0976747920963401
Khoshnevis, Y. S., and Khanalizadeh, B. (2017). Air pollution, economic growth and health care expenditure. Econ. Research-Ekonomska Istraživanja 30 (1), 1181–1190. doi:10.1080/1331677X.2017.1314823
Kim, T. J., Vonneilich, N., Lüdecke, D., and Knesebeck, O. (2017a). Income, financial barriers to health care and public health expenditure: a multilevel analysis of 28 countries. Soc. Sci. Med. 176, 158–165. doi:10.1016/j.socscimed.2017.01.044
Kim, Y., Knowles, S., Manley, J., and Radoias, V. (2017b). Long-run health consequences of air pollution: evidence from Indonesia’s forest fires of 1997. Econ. Hum. Biol. 26, 186–198. doi:10.1016/j.ehb.2017.03.006
Kochuvilayil, A., Rajalakshmi, S., Krishnan, A., Vijayanand, S. M., Kutty, V. R., Iype, T., et al. (2023). Palliative care management committees: a model of collaborative governance for primary health care. Public Health Action 13 (1), 12–18. doi:10.5588/pha.22.0028
Koengkan, M., Fuinhas, J. A., and Marques, A. C. (2019). “The relationship between financial openness, renewable and nonrenewable energy consumption, CO2 emissions, and economic growth in the Latin American countries: an approach with a panel vector auto regression model,” in In the extended energy-growth nexus: theory and empirical applications (Academic Press), 199–229. doi:10.1016/B978-0-12-815719-0.00007-3
Koengkan, M., Fuinhas, J. A., and Silva, N. (2021). Exploring the capacity of renewable energy consumption to reduce outdoor air pollution death rate in Latin America and the Caribbean region. Environ. Sci. Pollut. Res. 28 (2), 1656–1674. doi:10.1007/s11356-020-10503-x
Koijen, R. S., Philipson, T. J., and Uhlig, H. (2016). Financial health economics. Econometrica 84 (1), 195–242. doi:10.3982/ECTA11182
Kumar, A., Ahmed, K., Bhayo, M. R., and Kalhoro, M. R. (2022). Banking performance and institutional quality: evidence from dynamic panel data analysis. Int. J. Finance Econ. 28, 4717–4737. doi:10.1002/ijfe.2673
Kutlu, G., and Örün, E. (2022). The effect of carbon dioxide emission, GDP per capita and urban population on health expenditure in OECD countries: a panel ARDL approach. Int. J. Environ. Health Res., 1–10. doi:10.1080/09603123.2022.2083088
Labras, R., and Torrecillas, C. (2018). Estimating dynamic Panel data. A practical approach to perform long panels. Rev. Colomb. Estad. 41 (1), 31–52. doi:10.15446/rce.v41n1.61885
Levin, A., Lin, C.-F., and Chu, C.-S. J. (2002). Unit root tests in panel data: asymptotic and finite-sample properties. J. Econ. 108, 1–24. doi:10.1016/S0304-4076(01)00098-7
Li, F., Chang, T., Wang, M. C., and Zhou, J. (2022). The relationship between health expenditure, CO2 emissions, and economic growth in the BRICS countries-based on the Fourier ARDL model. Environ. Sci. Pollut. Res. Int. 29 (8), 10908–10927. doi:10.1007/s11356-021-17900-w
Lin, L., and Guo, M. (2023). Effects of urbanization on multiple human perceived temperatures in South China. Front. Environ. Sci. 11. doi:10.3389/fenvs.2023.1117443
Lopez, L., and Weber, S. (2017). Testing for granger causality in panel data. Stata J. 17 (4), 972–984. doi:10.1177/1536867X1801700412
Lopreite, M., Misuraca, M., and Puliga, M. (2023). An analysis of the thematic evolution of ageing and healthcare expenditure using word embedding: a scoping review of policy implications. Socio-Economic Plan. Sci. 87 (B), 101600. doi:10.1016/j.seps.2023.101600
Lopreite, M., and Zhu, Z. (2020). The effects of ageing population on health expenditure and economic growth in China: a Bayesian-VAR approach. Soc. Sci. Med. 265, 113513. doi:10.1016/j.socscimed.2020.113513
Ma, X., Akhtar, R., Akhtar, A., Hashim, R. A., and Sibt-e-Ali, M. (2022). Mediation effect of environmental performance in the relationship between green supply chain management practices, institutional pressures, and financial performance. Front. Environ. Sci. 10, 972555. doi:10.3389/fenvs.2022.972555
Makin, A. J., and Layton, A. (2021). The global fiscal response to COVID-19: risks and repercussions. Econ. Anal. Policy 69, 340–349. doi:10.1016/j.eap.2020.12.016
Maladjian, C., and Khoury, R. E. (2014). Determinants of the dividend policy: an empirical study on the Lebanese listed banks. Int. J. Econ. Finance 6 (4), 240–256. doi:10.5539/ijef.v6n4p240
Maugeri, A., Barchitta, M., Puglisi, F., and Agodi, A. (2023). Socio-economic, governance and health indicators shaping antimicrobial resistance: an ecological analysis of 30 european countries. Glob. Health 19 (12), 12. doi:10.1186/s12992-023-00913-0
Miranda-Lescano, R., Leonel, M., and Oriol, R. (2023). Human development and decentralization: the importance of public health expenditure. Ann. Public Coop. Econ. 94 (1), 191–219. doi:10.1111/apce.12373
Nakatani, R., Zhang, Q., and Valdes, I. (2023). Health expenditure decentralization and health outcomes: the importance of governance. Publius J. Fed. doi:10.1093/publius/pjad031
Nuţă, F. M., Tabără, N., Nuţă, A. C., and Creţu, C. (2015). An assessment upon the environmental policy in Romania. Econ. Research-Ekonomska Istraživanja 28 (1), 641–649. doi:10.1080/1331677X.2015.1083874
Onisanwa, I. D. (2014). The impact of health on economic growth in Nigeria. J. Econ. Sustain. Dev. 5 (19), 159–166. Available at: https://www.iiste.org/Journals/index.php/JEDS/article/viewFile/16114/16445.
Oyelade, A. O., Tijani, O. D., Wakile, M. O., and Kanimodo, A. L. (2020). Environmental quality and its attendant effect on human health: new evidence from panel quantile regression for Anglophone countries in West Africa. Int. Immunol. 8 (4), 89–95. doi:10.11648/j.iji.20200804.14
Patz, J. A., Frumkin, H., Holloway, T., Vimont, D. J., and Haines, A. (2014). Climate change: challenges and opportunities for global health. JAMA 312 (15), 1565–1580. doi:10.1001/jama.2014.13186
Pedroni, P. (2004). Panel cointegration: asymptotic and finite sample properties of pooled time series tests with an application to the PPP hypothesis. Econ. Theory 20, 597–625. doi:10.1017/S0266466604203073
Perron, P., and Vogelsang, T. J. (1992). Nonstationarity and level shifts with an application to purchasing power parity. J. Bus. Econ. Statistics 10 (3), 301–320. doi:10.2307/1391544
Pervaiz, R., Faisal, F., Rahman, S. U., Chander, R., and Ali, A. (2021). Do health expenditure and human development index matter in the carbon emission function for ensuring sustainable development? Evidence from the heterogeneous panel. Air Qual. Atmos. Health 14, 1773–1784. doi:10.1007/s11869-021-01052-4
Pesaran, M. H. (2004). General diagnostic tests for cross section dependence in panels. IZA Discussion Paper No. 1240. Available at: https://docs.iza.org/dp1240.pdf.
Raeesi, P., Harati-Khalilabad, T., Rezapour, A., Azari, S., and Javan-Noughabi, J. (2018). Effects of private and public health expenditure on health outcomes among countries with different health care systems: 2000 and 2014. Med. J. Islam. Repub. Iran. 32, 205–209. doi:10.14196/mjiri.32.35
Raeissi, P., Harati-Khalilabad, T., Rezapour, A., Hashemi, S. Y., Mousavi, A., and Khodabakhshzadeh, S. (2018). Effects of air pollution on public and private health expenditures in Iran: a time series study (1972-2014). J. Prev. Med. Public Health 51 (3), 140–147. doi:10.3961/jpmph.17.153
Rahman, M. M., Khanam, R., and Rahman, M. (2018). Health care expenditure and health outcome nexus: new evidence from the SAARC-ASEAN region. Glob. Health 14 (113), 113. doi:10.1186/s12992-018-0430-1
Ray, D., and Linden, M. (2020). Health expenditure, longevity, and child mortality: dynamic panel data approach with global data. Int. J. Health Econ. Manag. 20 (1), 99–119. doi:10.1007/s10754-019-09272-z
Rocque, R. J., Beaudoin, C., Ndjaboue, R., Cameron, L., Poirier-Bergeron, L., Poulin-Rheault, R.-A., et al. (2021). Health effects of climate change: an overview of systematic reviews. BMJ Open 11 (6), e046333. doi:10.1136/bmjopen-2020-046333
Rodríguez, A. F., and Nieves Valdés, M. (2019). Health care expenditures and GDP in Latin American and OECD countries: a comparison using a panel cointegration approach. Int. J. Health Econ. Manag. 19, 115–153. doi:10.1007/s10754-018-9250-3
Roodman, D. (2009). How to do Xtabond2: an introduction to difference and system GMM in Stata. Stata J. Promot. Commun. Statistics Stata 9 (1), 86–136. doi:10.1177/1536867X0900900106
Salam, M., and Chishti, M. Z. (2022). Will ASEAN countries be a potential choice for the export of pollution intensive goods? Environ. Sci. Pollut. Res. 29, 81308–81320. doi:10.1007/s11356-022-21427-z
Samah, I. H. A., Maizura, I., Husain, W. A. F. W., and Amlus, H. (2020). The impact of healthcare expenditure and healthcare sector growth on CO2 emission using dynamic panel data system GMM estimation model during COVID 19 crisis. Int. J. Energy Econ. Policy 10 (6), 235–241. doi:10.32479/ijeep.9769
Samudram, M., Sanggaran, M. N., and Vaithilingam, S. (2009). Keynes and Wagner on government expenditures and economic development: the case of a developing economy. Empir. Econ. 36 (3), 697–712. doi:10.1007/s00181-008-0214-1
Sarafidis, V., and Wansbeek, T. (2012). Cross- sectional dependence in panel data analysis. Econ. Rev. 31 (5), 483–531. doi:10.1080/07474938.2011.611458
Sasmaz, M. U., Karamıklı, A., and Akkucuk, U. (2021). The relationship between renewable energy use and health expenditures in EU countries. Eur. J. Health Econ. 22, 1129–1139. doi:10.1007/s10198-021-01312-1
Schneider, A., and Breitner, S. (2016). Temperature effects on health - current findings and future implications. eBioMedicine 6, 29–30. doi:10.1016/j.ebiom.2016.04.003
Shao, Q., Ran, T., and Luca, M. (2022). The effect of urbanization on health care expenditure: evidence from China. Front. Public Health 10, 850872. doi:10.3389/fpubh.2022.850872
Siami-Namini, S. (2018). Healthcare expenditure, economic growth, and inflation in the G7 countries: a panel co-integration approach. Res. J. Econ. 2 (2), 1–8. Available at: https://www.researchgate.net/publication/351234139_Healthcare_Expenditure_Economic_Growth_and_Inflation_in_the_G7_Countries_A_Panel_Cointegration_Approach.
Sohail, A., Du, J., and Abbasi, B. N. (2023). Exploring the interrelationship among health status, CO2 emissions, and energy use in the top 20 highest emitting economies: based on the CS-DL and CS-ARDL approaches. Air Qual. Atmos. Health 16, 1419–1442. doi:10.1007/s11869-023-01350-z
Stern, N. (2007). Stern review- the economics of climate change. Cambridge, UK: Cambridge University Press. doi:10.1017/CBO9780511817434
Taghizadeh-Hesary, F., and Taghizadeh-Hesary, F. (2020). The impacts of air pollution on health and economy in Southeast Asia. Energies 13 (7), 1812. doi:10.3390/en13071812
Tong, M. X., Wondmagegn, B. Y., Williams, S., Hansen, A., Dear, K., Pisaniello, D., et al. (2021). Hospital healthcare costs attributable to heat and future estimations in the context of climate change in Perth, Western Australia. Adv. Clim. Change Res. 12 (5), 638–648. doi:10.1016/j.accre.2021.07.008
Travassos, G. F., Antônio da Cunha, D., and Coelho, A. B. (2020). The environmental impact of Brazilian adults’ diet. J. Clean. Prod. 272 (122622), 122622. doi:10.1016/j.jclepro.2020.122622
Ullah, S., Akhtar, P., and Zaefarian, G. (2018). Dealing with endogeneity bias: the generalized method of moments (GMM) for panel data. Ind. Mark. Manag. 71, 69–78. doi:10.1016/j.indmarman.2017.11.010
Ullah, S., Luo, R., Adebayo, T. S., and Kartal, M. T. (2023). Dynamics between environmental taxes and ecological sustainability: evidence from top-seven green economies by novel quantile approaches. Sustain. Dev. 31 (2), 825–839. doi:10.1002/sd.2423
Usman, M., Ma, Z., Wasif Zafar, M., Haseeb, A., and Ashraf, R. U. (2019). Are air pollution, economic and non-economic factors associated with per capita health expenditures? Evidence from emerging economies. Int. J. Environ. Res. Public Health 16 (11), 1967. doi:10.3390/ijerph16111967
van Daalen, K. R., Romanello, M., Rocklöv, J., Semenza, J., Tonne, C., Markandya, A., et al. (2022). The 2022 Europe report of the Lancet Countdown on health and climate change: towards a climate resilient future. Lancet Public Health 7, 942–965. doi:10.1016/S2468-2667(22)00197-9
Vatcheva, K. P., Lee, M., McCormick, J. B., and Rahbar, M. H. (2016). Multicollinearity in regression analyses conducted in epidemiologic studies. Epidemiol 6, 227. doi:10.4172/2161-1165.1000227
Wang, C. M., Hsueh, H. P., Li, F., and Wu, C. F. (2019). Bootstrap ARDL on health expenditure, CO2 emissions, and GDP growth relationship for 18 OECD countries. Front. Public Health 7, 324. doi:10.3389/fpubh.2019.00324
Wang, Z., Chen, X., Ullah, S., and Abbas, S. (2023). Resource curse or blessing? Evaluating the role of natural resource, social globalization, and environmental sustainability in China. Resour. Policy 85 (A), 103749. doi:10.1016/j.resourpol.2023.103749
Wawrzyniak, D. (2020). CO2 emissions inthe visegrad group countries and the European union climate policy. Comp. Econ. Res. Central East. Eur. 23 (1). doi:10.18778/1508-2008.23.05
Weimin, Z., Sibt-e-Ali, M., Tariq, M., Dagar, V., and Khan, M. K. (2022). Globalization toward environmental sustainability and electricity consumption to environmental degradation: does EKC inverted U-shaped hypothesis exist between squared economic growth and CO2 emissions in top globalized economies. Environ. Sci. Pollut. Res. 29, 59974–59984. doi:10.1007/s11356-022-20192-3
Westerlund, J. (2005). New simple tests for panel cointegration. Econ. Rev. 24, 297–316. doi:10.1080/07474930500243019
Who, (2018). Heat and health. Available at: https://www.who.int/news-room/fact-sheets/detail/climate-change-heat-and-health.
Who, (2021). Climate change and health. Available at: https://www.who.int/news-room/fact-sheets/detail/climate-change-and-health.
Who, (2023). Statement – without preparation the heat can be deadly. Available at: https://www.who.int/europe/news/item/18-07-2023-statement---without-preparation-the-heat-can-be-deadly.
Wintoki, M. B., Linck, J. S., and Netter, J. M. (2012). Endogeneity and the dynamics of internal corporate governance. J. Financial Econ. 105 (3), 581–606. doi:10.1016/j.jfineco.2012.03.005
Wondmagegn, B. Y., Xiang, J., Williams, S., Pisaniello, D., and Bi, P. (2019). What do we know about the healthcare costs of extreme heat exposure? A comprehensive literature review. Sci. Total Environ. 657, 608–618. doi:10.1016/j.scitotenv.2018.11.479
Wooldridge, J. M. (2002). Econometric analysis of cross section and panel data. Cambridge, MA: MIT Press. Available at: https://www.jstor.org/stable/j.ctt5hhcfr.
Yip, W., Lee, Y.-C., Tsai, S., and Chen, B. (2017). Managing health expenditure inflation under a single-payer system: taiwan's National Health Insurance. Soc. Sci. Med. 233, 272–280. doi:10.1016/j.socscimed.2017.11.020
Zaidi, S., and Saidi, K. (2018). Environmental pollution, health expenditure and economic growth in the Sub-Saharan Africa countries: panel ARDL approach. Sustain. Cities Soc. 41, 833–840. doi:10.1016/j.scs.2018.04.034
Zaman, U., Chishti, M. Z., Hameed, T., and Akhtar, M. S. (2023). Exploring the nexus between green innovations and green growth in G-7 economies: evidence from wavelet quantile correlation and continuous wavelet transform causality methods. Environ. Sci. Pollut. Res. doi:10.1007/s11356-023-28982-z
Zammit, C., Torzhenskaya, N., Ozarkar, P. D., and Calleja, A. J. (2021). Neurological disorders vis-à-vis climate change. Early Hum. Dev. 155, 105217. doi:10.1016/j.earlhumdev.2020.105217
Keywords: temperature, CO2 emissions, healthcare risks, health expenditure, governance, human development
Citation: Socol A, Iuga H, Socol D and Iuga IC (2023) Does climate change drive up government healthcare costs in the European Union?. Front. Environ. Sci. 11:1286099. doi: 10.3389/fenvs.2023.1286099
Received: 30 August 2023; Accepted: 27 November 2023;
Published: 11 December 2023.
Edited by:
Alina Cristina Nuta, Danubius University of Galaţi, RomaniaReviewed by:
Milena Lopreite, University of Calabria, ItalyCopyright © 2023 Socol, Iuga, Socol and Iuga. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Adela Socol, YWRlbGEuc29jb2xAdWFiLnJv
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.