 Henrique Fernandes Magalhães1,2
Henrique Fernandes Magalhães1,2 Ivanilda Soares Feitosa1,2Elcida de Lima Araújo1,2
Ivanilda Soares Feitosa1,2Elcida de Lima Araújo1,2 Ulysses Paulino Albuquerque1,2*
Ulysses Paulino Albuquerque1,2*- 1Programa de Pós-Graduação em Etnobiologia e Conservação da Natureza, Departamento de Biologia, Universidade Federal Rural de Pernambuco, Recife, Brazil
- 2Laboratório de Ecologia e Evolução de Sistemas Socioecológicos, Departamento de Botânica, Centro de Biociências, Universidade Federal de Pernambuco, Recife, Brazil
People living in areas vulnerable to diseases caused by extreme climate change events, such as semiarid regions, tend to recognize them quickly and, consequently, develop strategies to cope with their effects. Our study investigated the perception of diseases by farmers living in the semiarid region of Northeastern Brazil and the adaptive strategies locally developed and used. To this end, the effect of the incidence and severity of locally perceived diseases on the frequency of adaptive responses adopted by the farmers was tested. The research was conducted in rural communities in the Pernambuco State, Northeastern Region of Brazil. Semi-structured interviews with 143 farmers were conducted to collect information about major drought and rainfall events, the perceived diseases related to these events, and the adaptive strategies developed to mitigate them. The incidence and severity of diseases perceived by farmers were calculated using the Participatory Risk Mapping method and the frequency of adaptive strategies. Our findings demonstrated that few climate change-related diseases were frequently mentioned by farmers, indicating low incidence rates. Among them, direct transmission diseases were the most frequently mentioned. Adaptive strategies to deal with the mentioned diseases related to prophylactic behavior were less mentioned, except if already utilized. Our model demonstrated that incidence was the only explanatory variable with a significant impact on the adaptive strategies used to deal with the effects of these risks on health. Our findings suggest that the estimated incidence of diseases should be considered in the development of predictive climate change models for government policy measures for the public health security of populations in areas of greater socio-environmental vulnerability.
Introduction
There is extensive evidence that the global climate is changing rapidly. A recent survey by the World Meteorological Organization (WMO, 2020) demonstrated that 2015 to 2019 were the five warmest years on record compared to any other equivalent period in history. Such changes drive the incidence of heatwaves, floods, and storms and affect the dynamics of air, water, and food supply, which are key drivers of human health (WHO, 2009).
Human health problems caused by extreme climate change events (e.g., prolonged droughts and rainfall) are diverse, ranging from heatwave related diseases and mortalities to infections transmitted by different vectors, causing respiratory problems and mental illness (McMichael et al., 2006; Younger et al., 2008; McMichael, 2013). According to data from the World Health Organization (WHO), an increase of up to 250,000 deaths is expected between 2030 and 2050 due to climate change impacts on human health (Watts et al., 2015). Climate change impacts pose significant global threats to human health, and the projections are staggering (e.g., McMichael et al., 2006; Costello et al., 2009; Hayes et al., 2018; Watts et al., 2018; Austin et al., 2020).
Diseases arising from climate change risks are diverse and transmitted directly and indirectly (Smith et al., 2014; Watts et al., 2018). Direct transmission occurs primarily with changes in the frequency of non-seasonal weather conditions, such as droughts and intense, prolonged rainfall. Indirect transmission occurs through natural systems, such as disease vectors and infections transmitted through water and air pollution, or by human systems, such as occupational factors, malnutrition, and mental stress (Smith et al., 2014). Some authors also prefer to categorize the impacts of climate change on human health into primary, secondary, and tertiary risks (Butler and Harley, 2010; McMichael, 2013). The primary, secondary, and tertiary risks correspond to direct transmission; indirect transmission mediated by biophysical and ecological processes and systems (such as variation in water flow) and by vectors of infectious diseases; and indirect transmission that arises, for example, as consequences of tensions and conflicts arising from factors related to climate change, such as migration and shortage of basic resources (these risks include mental health problems; McMichael, 2013) respectively. This study uses both classification criteria, considering secondary and tertiary risks as subcategories of indirect risks.
The health of vulnerable human populations tends to be more impacted by extreme climate change events, largely due to reduced access to health services and the barriers in seeking these services (Handley et al., 2014; Hayes et al., 2018). This includes rural populations living in semiarid regions, which, in addition to low rainfall totals and annual and inter-annual irregularities in rainfall patterns, have poor infrastructure for coping with the adversities of climate change (Banerjee, 2014; Dhanya and Ramachandran, 2016). In the semiarid region of Northeastern Brazil, for example, the dependence on forest resources and the low income of rural populations have already been documented, factors that make rural populations more vulnerable to climate change (de Albuquerque et al., 2012; dos Santos et al., 2013; Silva et al., 2017; Gonçalves et al., 2021).
Vulnerability, according to the Intergovernmental Panel on Climate Change (IPCC), corresponds to the predisposition of a given population and/or locality to be impacted by changes in climate and occurs as a function of three main factors: sensitivity, adaptive capacity, and exposure (IPCC, 2007). Sensitivity corresponds to the way a system can be affected (negatively or not); adaptive capacity corresponds to the ability to cope (minimizing or avoiding) with damage; and exposure corresponds to the presence of people, systems, and their relationships, which can be potentially impacted by the effects of climate change (IPCC, 2007). Thus, it is acknowledged that semiarid regions are more vulnerable because local human populations depend more on the natural resources provided locally for their subsistence and because they are more sensitive and exposed to the adverse effects of climate change. Based on this premise, these populations tend to recognize incident diseases associated with climate change more quickly (McMichael et al., 2006; Lafferty, 2009; Bhatta et al., 2020). Thus, in addition to the search for understanding how climate change interferes with people’s way of life, it is essential to evaluate the perception of human populations in this context because people tend to develop knowledge and practices related to health to prevent the spread of diseases, modifying local medical systems (Ferreira et al., 2015). Therefore, local medical systems may offer clues about recent changes in disease incidences on a time scale (Estomba et al., 2006; Ferreira et al., 2015; Santoro et al., 2015; Santoro and Albuquerque, 2020).
Considering diseases as risks to human health, which can be caused or enhanced by extreme climate events, this study defines risks as potentially unfavorable or harmful circumstances arising from the effects generated by environmental changes in people’s daily lives (Smith et al., 2000). According to the United Nations Office for Disaster Risk Reduction (UNDRR), risk can also correspond to the probability of the occurrence of an adverse effect arising from an environmental phenomenon (UNDRR, 2009). Thus, the risk perception can be used to anticipate change and enable the development of adaptive strategies to deal with potential negative effects. These adaptive strategies can be characterized as reactions or adjustments to situations perceived as risky at the collective or individual level (Smith et al., 2000; Smit and Wandel, 2006; Boillat and Berkes, 2013; Oliveira et al., 2017). This study considered both long-term (prophylactic) and short-term (therapeutic/treatment) adaptive strategies.
In relation to risk perceptions arising from climate change, whether on a local or regional scale, there is evidence that disease incidence may be related to the adoption of adaptive mitigation strategies (e.g., Lafferty, 2009; Oloukoi et al., 2014; de Perez et al., 2015; Bhatta et al., 2020). Although the severity assigned to diseases has received little attention in the literature, it is believed that adaptive strategies may be adopted based on the classification of diseases according to their severity, as has been recorded in studies on environmental risk perception (e.g., Smith et al., 2000; Quinn et al., 2003; Baird et al., 2009). Identifying popular strategies to adjust to climate change and avoid health risks is a gap to be filled in scientific knowledge, potentially contributing to collective public health management.
Thus, understanding how residents of semiarid regions—areas having a high probability of extreme climate change events and their direct implications, such as water scarcity (Martins et al., 2015)—perceive health risks and manage them amidst increasingly accelerated climate change is essential for the development and implementation of more effective adaptive responses (Austin et al., 2020). Thus, our study aimed to investigate the perception of farmers living in the northeastern semiarid region about local diseases, highlighting the adaptive strategies developed locally and used to mitigate health problems. For this, we tested the hypothesis that the incidence and severity of diseases related to climate change drive the adopted adaptive responses. It is expected that there is a higher frequency of adaptive strategies developed for more incidents and more severe diseases.
Materials and Methods
Study Area
The study was conducted in two semiarid areas in the Pernambuco State, Northeastern Brazil (Figure 1). The first select area was the Catimbau National Park (Catimbau NAPAR), a Conservation Unit that covers 62,294.14 hectares, located between the “agreste” and “sertão” of the Pernambuco State in the domain of three municipalities in the São Francisco River Basin: Buíque, Tupanatinga, and Ibimirim (ICMBio, 2002) (Figure 2). In the Catimbau NAPAR, six rural communities were selected: Muquem (8.49414° S; 37.2999° W), Breus (8.49076° S; 37.29059° W), Açude Velho (8.4592° S; 37.30289° W), Tunel (8.46208° S; 37.31967° W), Dor de Dente (8.51355° S; 37.31413° W) and Igrejinha (8.49966° S; 37.25743° W). The total number of local adult residents in each of these communities, according to data obtained through the Family Health Program (FHP) of the Buíque Municipality, were: Muquem (n = 38), Breus (n = 32), Açude Velho (n = 17), Tunel (n = 6), Dor de Dente (n = 13), and Igrejinha (n = 112), totaling 218 people.
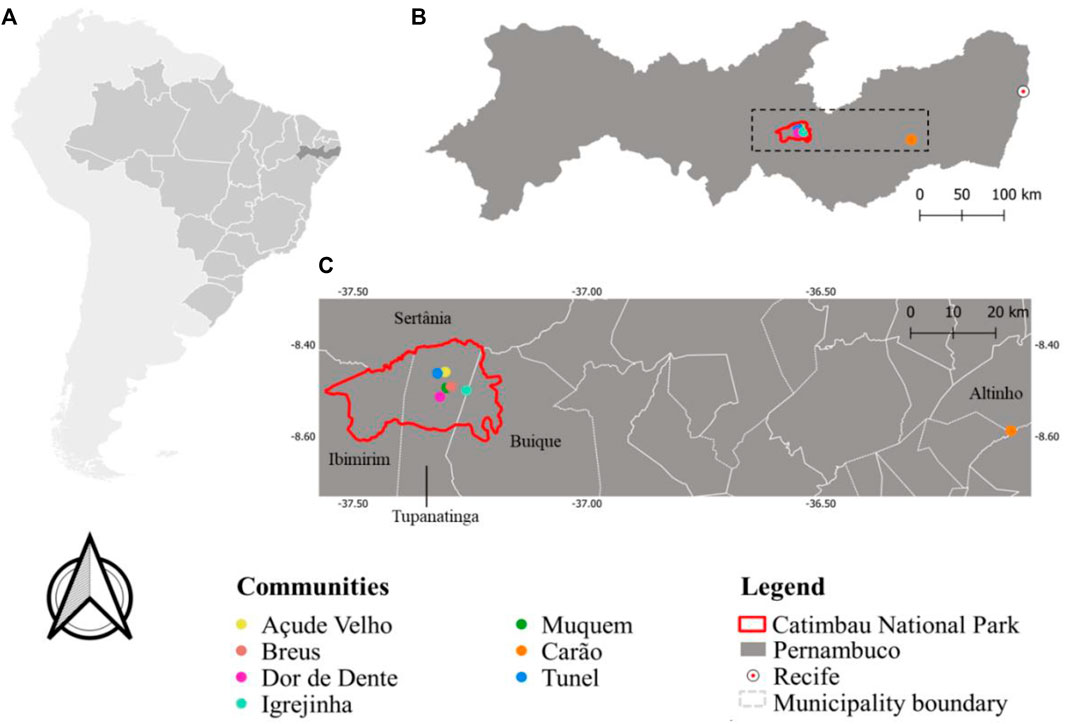
FIGURE 1. Map of the Catimbau National Park location, highlighting the rural communities of the research (Açude Velho, Breus, Dor de Dente, Igrejinha, Muquem, and Tunel) and Carão, Altinho Municipality (Pernambuco State, semiarid region of Northeastern Brazil). All elements highlighted on the map (study area locations) have been revised and are correctly flagged in the legend.

FIGURE 2. Landscape of Igrejinha, rural community located in the Catimbau National Park (Pernambuco State, semiarid region of Northeastern Brazil). Photo: Henrique F. Magalhães.
The second selected area was the Carão (08° 35′13.5″ S and 36° 05′ 34.6″ W), a rural community located in the Altinho Municipality, Pernambuco State, in the center of the “agreste,” 168 km from the state capital. According to information obtained through the Carão health center, the local population currently consists of 140 people (27 were under 18 years old) in 55 family units (households; Figure 3).

FIGURE 3. Landscape of the Carão rural community, located in the Altinho Municipality (Pernambuco State, semiarid region of Northeastern Brazil). Photo: Regina C. S. Oliveira.
The semiarid tropical climate (BSh), according to the Köppen-Geiger Scale, typical of the semiarid region of Northeastern Brazil (Alvares et al., 2013), is predominant in both the Catimbau NAPAR (ME, 2015) and Carão (Cruz et al., 2014). In the Catimbau NAPAR, the mean annual temperature is 23°C, with great interannual irregularity in rainfall, varying from 650 to 1,100 mm annually (ME, 2015). All rural communities selected for the study in the Catimbau NAPAR are located in the driest strip of the park (PELD Catimbau, 2016). The annual temperature in Carão is around 25°C, with an average rainfall of around 622 mm between March and July (BDE, 2017).
Droughts are recurrent climatic events in Northeastern Brazil and are generally associated with the El Niño phenomenon, which results in lower rainfall than the historical average in this semiarid region, which is about 800 mm per year (Magalhães, 2016; Marengo et al., 2018). Additionally, the precipitation is concentrated in a few months and evapotranspiration levels exceed 2,000 mm per year. As the semiarid region is a climatic Frontier area, any decrease in relation to the average may have a large impact (Magalhães, 2016). Based on historical records, as illustrated in Table 1, in the last 50 years, there were at least nine periods of prolonged drought in the semiarid region of the Brazilian Northeast, which brought intensive losses to both the ecosystem and people’s livelihoods: 1979–1983, 1986–1987, 1992–1993, 1997–1999, 2002–2003, 2005, 2007–2008, 2010, and 2012–2017 (Marengo et al., 2017; Lima and Magalhães, 2018; Marengo et al., 2018; Cunha et al., 2019). Since 2010, the region has experienced the longest and most severe drought periods in its history, especially since 2015, due to the El Niño phenomenon (Marengo et al., 2018). According to data from the Instituto Nacional de Meteorologia (INMET, 2021), the Pernambuco State had lower precipitation and higher temperature averages in some months of an otherwise average year (Figures 4, 5).
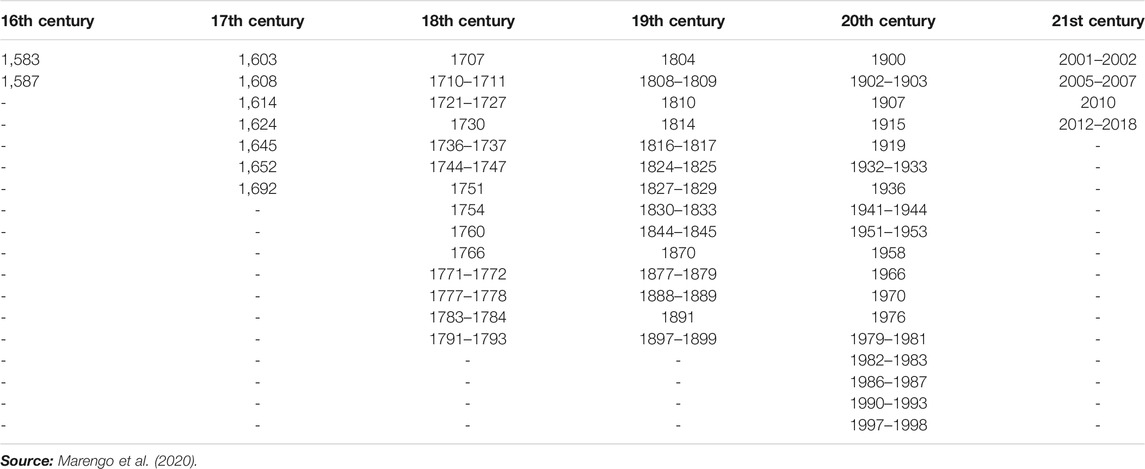
TABLE 1. History of drought periods in the Northeastern Region of Brazil.
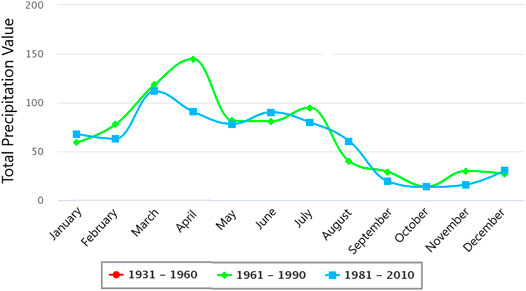
FIGURE 4. Comparative graph of historical variations in accumulated precipitation (mm) in the Pernambuco State in three annual intervals of 30 years. Source: Adapted from INMET (2021).
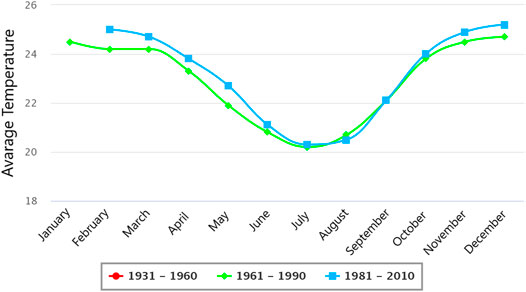
FIGURE 5. Comparative graph of historical variations in average temperature (oC) in the Pernambuco State in three annual intervals of 30 years. Source: Adapted from INMET (2021).
In the Catimbau NAPAR and Carão, this research was carried out with small farmers whose main source of local income is derived from subsistence agriculture and livestock, with emphasis on the planting of corn and beans and the operation of small goat, cattle, pig, and poultry farms. However, both areas have suffered agricultural losses and water resource shortages, characterizing them as risk areas for extreme drought events (Martins et al., 2015; Marengo et al., 2018), which may imply the proliferation of diseases related to extreme events of climate change (WHO, 2009). In the Catimbau NAPAR, this situation is aggravated by socio-environmental conflicts that have distinguished the area since it was founded (in 2002), involving the park management body—the Chico Mendes Institute for Biodiversity Conservation (ICMBio) —and residents, who had never been compensated since the park’s foundation and continue to live within the area, which is not legally permitted, according to the National System of Conservation Units (Brasil, 2000). Such a scenario made it very difficult for us to access some people living in the region because our presence was interpreted as an intervention by the environmental agency responsible for the park’s administration. To alleviate this situation, we adopted a cautious approach to residents, based on informal conversations and by explaining our project. For this reason, we also started our data collection in Carão, as we wanted to obtain a larger sample and, for the reasons mentioned above, Catimbau NAPAR was no longer a viable alternative. We chose Carão because our team has been conducting research in the region for 13 years and, therefore, has extensive knowledge about the site and a good relationship with residents.
Legal Procedures and Informant Selection
To meet the legal aspects of research involving humans, this study was submitted and approved by the Research Ethics Committee of the University of Pernambuco, according to the Certificate of Submission for Ethics Appreciation (CSEA) number 89890617.1.0000.5207. All residents who agreed to participate in the research were asked to sign a free and informed consent form, as governed by the current legislation of the National Health Council (Resolution No. 466/2012).
The initial contact with both rural communities was made through a previous survey on the number of households in each of the seven communities in the study (in the case of Carão, this step was not necessary due to long-term studies conducted by our team in the region for at least 10 years). Data regarding the number of people living in each rural community were obtained through the Family Health Program (FHP) of Catimbau Village, Buíque Municipality (PE), and the health center of Carão, Altinho Municipality (PE). Adults and older people (above 18 years old) living in rural communities were chosen.
Data Collection and Processing
Data collection for the study occurred between July 2018 and September 2019. Of the 358 residents in the two study areas (218 in the Catimbau NAPAR and 140 in Carão, as mentioned above), it is important to note that some of these residents are above 60 years old and have health problems. Additionally, some residents were not available at the time of the survey and refused to participate in the research (especially in the Catimbau NAPAR, a scenario of numerous socio-environmental conflicts, as previously mentioned). Thus, our sample was ultimately composed of 143 people who agreed to participate in the study, comprising 94 people living in the Catimbau NAPAR in the six selected rural communities: Muquem (n = 30), Breus (n = 20), Açude Velho (n = 9), Tunel (n = 6), Dor de Dente (n = 4), and Igrejinha (n = 25); and 49 people living in Carão.
Before our fieldwork, the study’s aims and methods were explained to informants to clarify doubts. After this step, people would be free to voluntarily accept (or refuse) to participate in the research. We also conducted a pilot study to ensure that the interviewers understood the questions.
The selection of the sample of the population that accepted to participate in the research was made from a census (Espinosa et al., 2014), as well as the collection of socioeconomic data from the selected informants (see Supplementary Table S1). Thus, residents who had relevant information for our study were interviewed, including people who lived in the same household. The information collected was carefully evaluated by removing inconsistencies or biases that compromised the validity of the information. Based on our observations and information from the scientific literature, people from the same family or who live in the same household do not necessarily have the same experiences or develop the same adaptive climate change strategies. This depends on other correlated factors, such as agriculture and risk experience (e.g., Weber, 2010; Bryan et al., 2013; Rodriguez et al., 2017).
To analyze perceptions on climate change-related diseases, semi-structured interviews were conducted with the participants due to the flexibility of the previously elaborated questions (Albuquerque et al., 2014; Magalhães et al., 2019). The field interviews were organized in two stages, which are described below. In the first stage, each participant was identified and asked about the years in which major extreme weather events (non-seasonal) occurred, such as droughts and rainfall. Without this design, the participants could have cited diseases related to environmental change in general and not those specifically related to climate change. Extreme droughts were the most characteristic climate change events faced in semiarid regions, with the period between 2012 and 2015 being pointed out as the most critical in the last 50 years (Martins et al., 2015). By comparing historical data on drought events in Northeastern Brazil (Table 1), the historical data cited by our informants were validated because they corresponded with the scientific data (such as the year 1993 and the period 2012–2014, the most mentioned by farmers in both study areas). Thereafter, using the free list technique (da Silva et al., 2014), the participants were asked to name or list diseases perceived as a result of the extreme drought and rainfall events in the region. We emphasize here that because the focus of the proposal of our experimental design was diseases “perceived by people” and not “scientifically designated” diseases, we do not use previously cataloged information regarding the incident diseases in the regions.
In the second stage, based on the list of mentioned diseases, each participant was asked to classify and organize them according to their severity i.e., the degree of impact on their lives (Smith et al., 2000). The severity of the diseases was represented by numbers following a decreasing ordinal classification (for example, number 1 represented the disease considered the most severe; number 2, the disease considered the second most severe; and so on). Additionally, based on each disease mentioned, the participants were asked about adaptive strategies used (if any) to mitigate them. In this study, the adaptive strategies, to paraphrase Smit and Wandel (2006), were considered responses developed by the participants to mitigate the potentially harmful effects arising from the diseases they perceived.
Although age was one of the main differences between our two areas of study, as Carão has a higher proportion of older people (80.7%), we chose not to categorize the sample sizes according to the age for each place of study due to the diverse evidence from scientific literature demonstrating that age is not a good predictor of the number of extreme weather events or perceived risks related to these weather phenomena. In this sense, a person’s experience in agriculture explains much more than age (Slegers, 2008; Gbetibouo, 2009; Fosu-Mensah et al., 2012). For example, a 60-year-old person may have lived for 40 years outside the community and participated in activities unrelated to agriculture; and a 35-year-old person could have worked in agriculture for 30 years. In this case, the younger person has more experience in agriculture than the older person and, therefore, would tend to perceive a greater number of extreme weather events and risks related to these phenomena. We believe that studies that consider categorizing sampling units according to the length of experience in agriculture (which was not our study proposal), can provide interesting insights.
Data Analysis
The incidence index (Ii) and the severity index (Sj) attributed to each perceived illness were initially calculated to test our hypothesis using the method suggested by Baird et al. (2009), adapted from Smith et al. (2000) (see Supplementary Table S2), and the objective was to understand and describe the local risk perception (in this case, diseases and risks to human health). Originally, this method—Participatory Risk Mapping (PRM)—was developed to access and quantitatively evaluate perceived environmental risks (see Smith et al., 2000; Baird et al., 2009). Compared to other methods used for this same purpose, the PRM stands out for being an extremely accurate and easily applicable method, which enables the researcher to assess the potential that a particular risk has of affecting people’s lives (da Silva et al., 2014; Magalhães et al., 2019). To the best of our knowledge, this is the first time the PRM has been applied to the perception of specific risks to human health (diseases).
The incidence index (Ii) corresponds to the ratio between the number of people who mentioned a certain disease (nr) and the total number of people in the sample (nj), represented by the equation:
The values assumed by Ii can vary between 0 and 1, which corresponds to the lowest and 1 corresponds to the highest incidence respectively.
Following the method proposed by Baird et al. (2009), the disease severity indexes (Sj) were calculated in two steps. Initially, the individual value of the risk severity index (Rij) was obtained by the equation:
where ni represents the total number of risks mentioned by each informant (i), and rij represents the classification of each risk individually. Next, all the results found for Rij were summed and divided by the number of times the risk was mentioned as the most severe (Nj). Next, the severity index (Sj) was obtained, with values ranging between 0 (risks that are not considered severe) and 1 (risks considered extremely severe), using the following equation:
Some of the obtained Ij and Sj results were represented using risk maps, graphical representations that allow the analysis of the space and distribution of incidence and severity of the mentioned diseases. As observed in the risk maps (Figures 6, 7), the upper part of the graph illustrates the first quadrant (where it is possible to observe the diseases classified as low incidence and very severe) and the second quadrant (where the diseases locally considered as high incidence and very severe appear); and the lower part displays the third quadrant (where the diseases perceived as low incidence with low severity are illustrated) and the fourth quadrant (where flu, a disease classified as not very severe, although with high local incidence is illustrated). Here, influenza is highlighted because it was the only disease mentioned in the fourth quadrant whose incidence was high. For this purpose, the PRM proposed by Baird et al. (2009) is the most recommended because the type of severity index (Sj) classification used facilitates both the elaboration and interpretation of risk maps (Baird et al., 2009) due to the similarity of the type of values presented by the incidence indices (Ii) and severity (Sj). For that reason, we opted for this model.
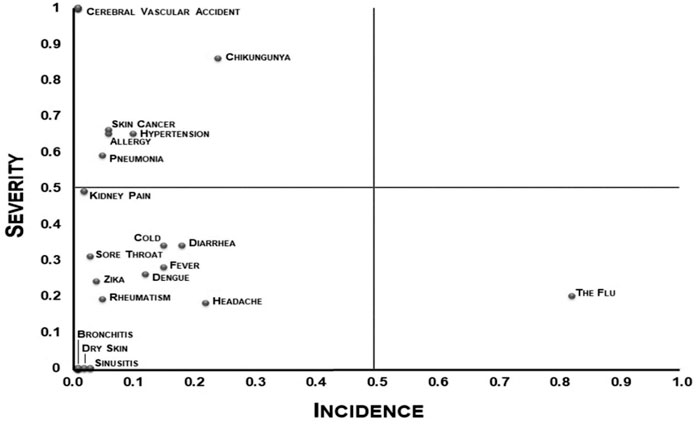
FIGURE 6. Map of disease incidence and severity perceived by farmers in the Catimbau NAPAR.
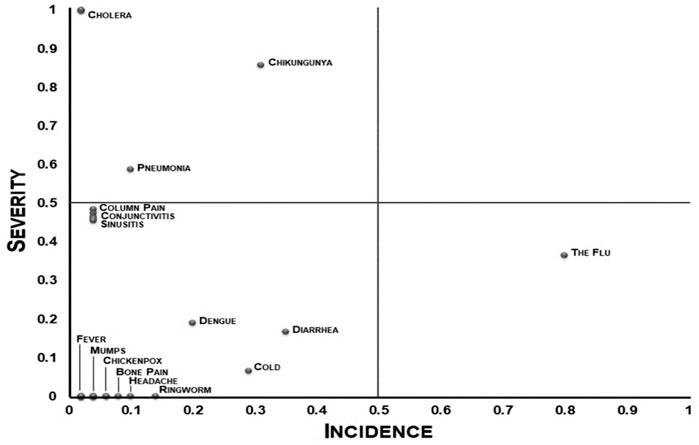
FIGURE 7. Map of disease incidence and severity perceived by farmers in Carão.
To calculate the incidence of adaptive strategies used to mitigate the diseases perceived by farmers, a similar logic to that used to calculate the incidence of risk (Ij), mentioned earlier, was adopted. The difference was to divide the number of adaptive strategies mentioned for each disease by the participants’ total number of adaptive strategies (see Supplementary Table S2). The indexes obtained in relation to the incidence of adaptive strategies (whose values could also vary from 0 to 1) were used in our analysis as dependent variables. The values of Ij and Sj were used as independent variables.
Subsequently, the data regarding perceived diseases were categorized (into direct and indirect diseases), and the mentioned adaptive strategies were classified (into therapeutic and prophylactic behavioral strategies) by the resident farmers of the Catimbau NAPAR (see Tables 1, 3) and Carão (see Tables 2, 4) regions to facilitate the explanation and discussion of our results. Finally, our hypothesis was tested for both areas using generalized linear models (GLM) with Gaussian distribution, in which the data were processed by calculating the logarithm (base 10) of n + 1 value to reduce the possible effects of large variation amplitudes. The statistical test was performed using the software R, version 3.6.3 (R Development Core Team 2019).
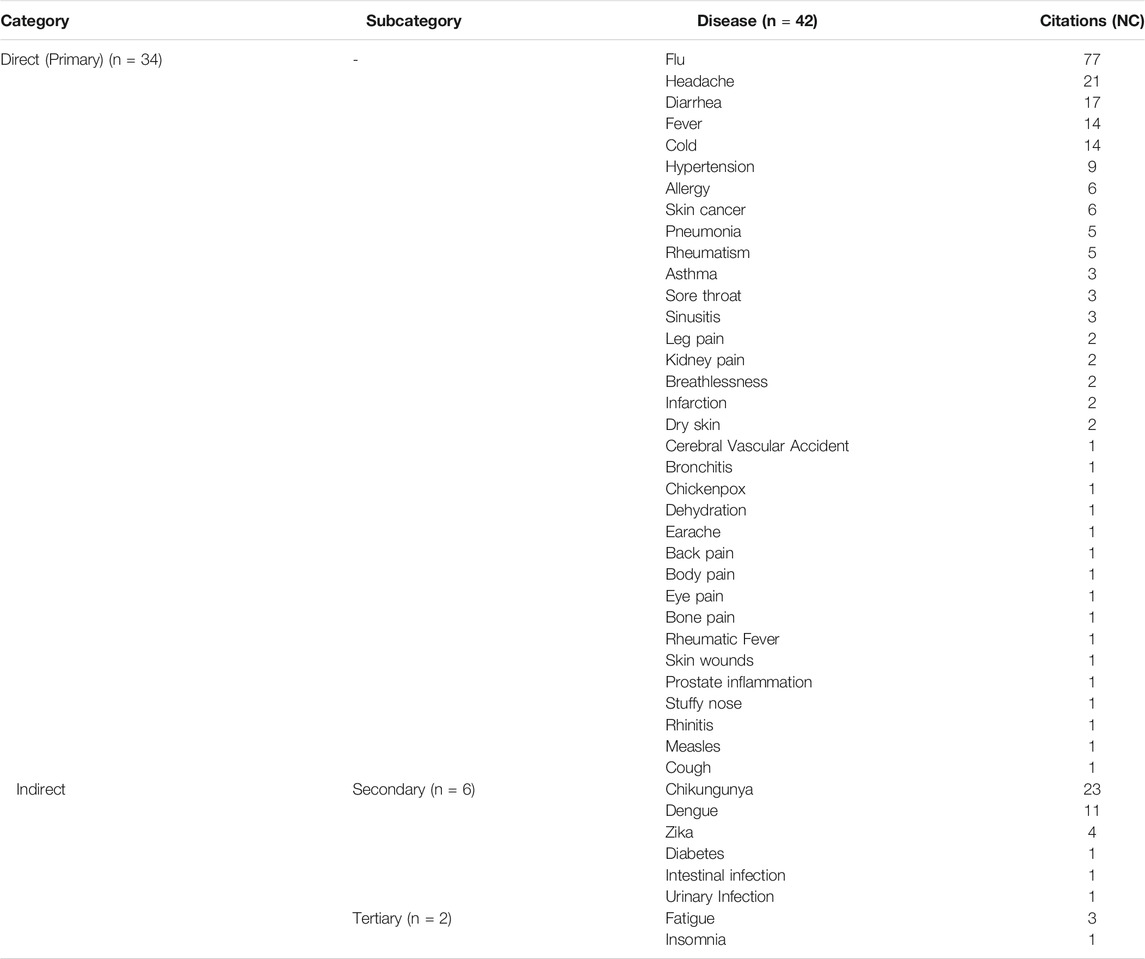
TABLE 2. Climate change-related diseases perceived by small-scale farmers living in the Catimbau NAPAR, Pernambuco State, Northeastern Brazil.
Results
Perceived Diseases Related to Climate Change and Adopted Adaptive Strategies
A total of 42 diseases related to drought and prolonged rainfall events were mentioned by farmers living in the Catimbau NAPAR. The farmers in Carão mentioned 31 diseases related to extreme climate change events. These diseases were listed in two categories based on their sources of transmission: direct (or primary) and indirect (subcategorized into secondary and tertiary), when transmission occurs through climatic phenomena, such as rain and heatwaves, and mediation of natural processes or systems (such as contaminated water or vectors) or human systems (fatigue caused by the need to walk long distances in the intense heat to work) respectively.
In both Catimbau NAPAR and Carão, most of the diseases mentioned were from direct transmission (n = 34, 26), followed by secondary indirect transmission (n = 6,4) and tertiary indirect transmission (n = 2, 1). Influenza stands out in the first category as the most frequently mentioned disease among residents of the rural communities of the Catimbau NAPAR (NC (number of citations) = 77) and Carão (NC = 39). The most mentioned diseases in the second category in both areas were chikungunya (NC = 23,15) and dengue (NC = 11, 10) (Table 3).
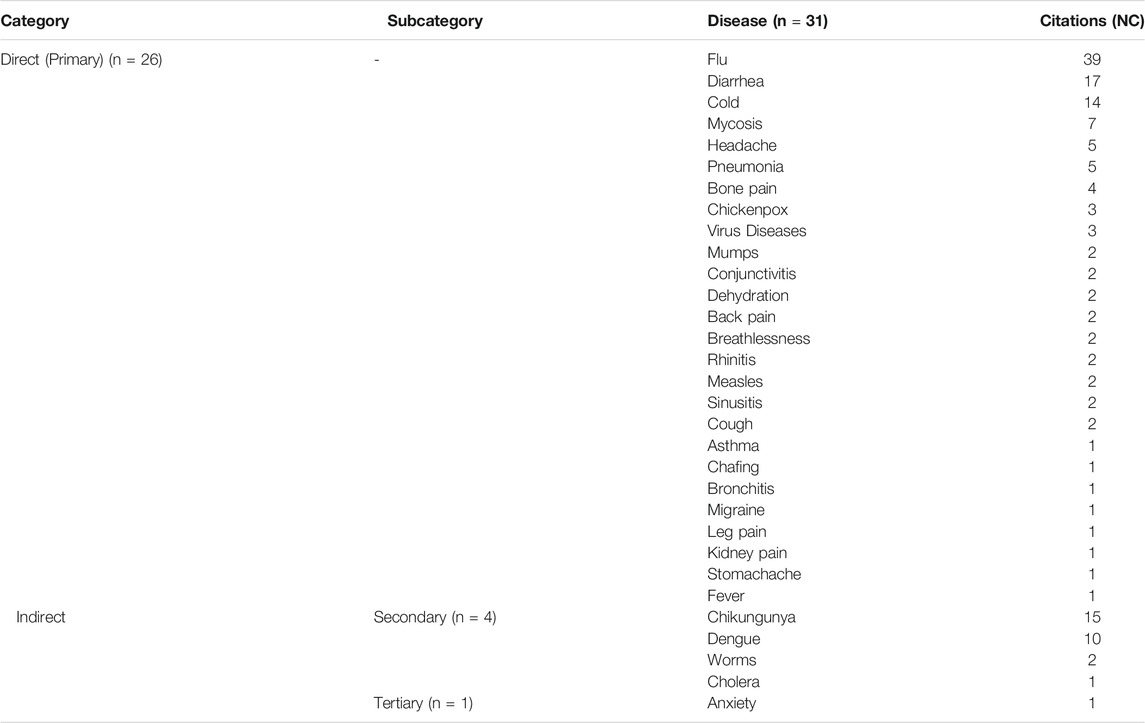
TABLE 3. Climate change-related diseases perceived by smallholder farmers living in Carão, Pernambuco State, Northeastern Brazil.
It is evident that all diseases perceived by farmers living in the two study areas are considered to have a low local incidence (except for influenza, whose incidence is very high, although with low severity; Figures 6, 7). Among these, diseases of low severity, such as dengue and cold predominated. Diseases perceived as having high severity were also mentioned, such as pneumonia and chikungunya, a disease of indirect transmission perceived as more severe.
Adaptive strategies were listed in two categories referring to the behavior adopted for developing the strategy: therapeutic behavior, subcategorized according to the origin of the behavior; and prophylactic behavior (Tables 4, 5). In the Catimbau NAPAR, 19 adaptive strategies were mentioned, including therapeutic (n = 10) and prophylactic behavior strategies (n = 9). In Carão, 14 adaptive strategies were mentioned by local farmers, including therapeutic (n = 8) and prophylactic behavioral strategies (n = 6).
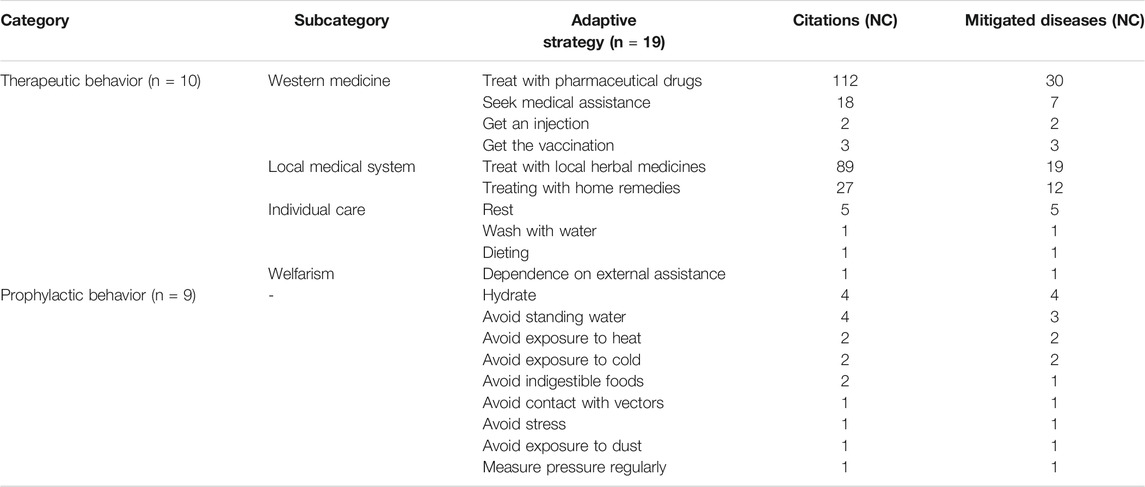
TABLE 4. Adaptive strategies used to mitigate diseases perceived by farmers living in the Catimbau NAPAR, Pernambuco State, Northeastern Brazil.
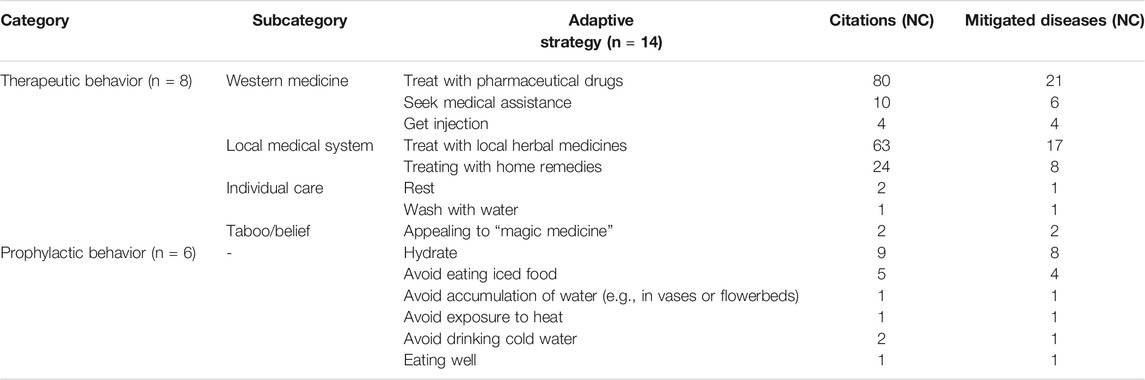
TABLE 5. Adaptive strategies used to mitigate diseases perceived by farmers living in Carão, Pernambuco State, Northeastern Brazil.
Among the therapeutic strategies, the subcategory that obtained the highest number of mentions, both in the Catimbau NAPAR (n = 4) and Carão (n = 3), is related to the use of pharmaceutical drugs: NC = 112 in the Catimbau NAPAR used for the treatment of 30 locally perceived diseases; and NC = 80 in Carão, used for the treatment of 21 locally perceived diseases. Among the adaptive therapeutic strategies related to the local medical system, the number of citations referring to treatment with local herbal medicines is noteworthy: NC = 89, 63 in the Catimbau NAPAR and Carão, used for the treatment of 19 and 17 locally perceived diseases respectively. It is also worth noting that adaptive strategies were also cited related to individual care, such as resting (NC = 5, two in the Catimbau NAPAR, and Carão); and taboo/beliefs in Carão such as using “magic” medicine (NC = 2).
Among the adaptive strategies of prophylactic behavior (n = 9 in the Catimbau NAPAR and n = 6 in Carão), the most frequently mentioned was hydration (NC = 4 in the Catimbau NAPAR and NC = 9 in Carão). This category demonstrates the significance of strategies related to escape/evasion behaviors to avoid sources or vectors that transmit diseases.
Relationship Between the Incidence and Severity of Perceived Illnesses and the Frequency of Used Adaptive Strategies
The incidence and severity attributed to perceived diseases related to climate change explained the frequency of adaptive strategies used among farmers in both the Catimbau NAPAR (z = 5.221; p = 6.22e - 06) and Carão (z = 5.617; p = 5.15e—06; Tables 6, 7). Among the independent variables tested in our models, the incidence of perceived diseases had great predictive power in both the Catimbau NAPAR (z = 5.151; p = 7.77e - 06) and Carão (z = 5.288; p = 1.26e - 05). Severity did not demonstrate predictive power in the models, suggesting that severity may not influence people’s perception of diseases related to extreme rainfall and drought events that affect them the most, rather than potentiating them, as expected.

TABLE 6. Generalized Linear Model used to test the effect of incidence and severity of diseases perceived by farmers in the Catimbau NAPAR on the frequency of used adaptive strategies. The p-values for the significant predictors are highlighted in bold. Significance code p-value: *** [0, 0.001]; ** (0.001, 0.01]; * (0.01, 0.05]; (0.05, 0.1]; (0.1, 1].

TABLE 7. Generalized Linear Model used to test the effect of disease incidence and severity perceived by Carão farmers on the frequency of used adaptive strategies. The p-values for significant predictors are highlighted in bold. Significance code p-value: *** [0, 0.001]; ** (0.001, 0.01]; * (0.01, 0.05]; (0.05, 0.1]; (0.1, 1].
Discussion
The results obtained demonstrate that diseases with the highest incidents tend to be prioritized in relation to the adoption of adaptive strategies to deal with their effects, both in the Catimbau NAPAR and Carão. This information is extremely relevant for understanding the importance of local therapeutic and prophylactic behaviors. Few diseases were mentioned very often by farmers, and most diseases had a low incidence. A possible explanation is that the diseases experienced by the population and the resources used for their treatment vary within time scales, which points to the existence of dynamic medical systems that can influence the perception of local populations (Santoro and Albuquerque, 2020). A diachronic study (with data collected over an 8-year time interval) also conducted in Carão, Santoro and Albuquerque (2020) observed that although incidence has a positive effect on the number of adaptive strategies, both allopathic and traditional medicines, it does not explain the variation in knowledge associated with these treatments, nor their efficacy. Thus, we believe that diachronic variations should not be disregarded in the analysis of disease perception or the related factors because disease incidence can drive the evolution of medical systems at different time scales (Santoro and Albuquerque, 2020).
Another possible explanation is that the diseases identified in this study with low incidence (almost all of them) may correspond to diseases perceived as common locally. People’s perception of these diseases is a complex phenomenon related to cognitive factors, such as judgment of environmental events and their local consequences on their way of life (Nyantakyi-Frimpong and Bezner-Kerr, 2015). Although common illnesses are considered to have less severity, data from the United Nations Children’s Emergency Fund (UNICEF) and the World Health Organization (WHO) demonstrate that common conditions, such as diarrhea, are among the leading contributors to child mortality worldwide (WHO and UNICEF, 2004; Young et al., 2012). Therefore, this category of perceived diseases should not be neglected in the development of prophylactic and emergency adaptive measures by civil society or public authorities.
In this study, although disease incidence and severity explained the frequency of adaptive strategies used to cope with their effects, the evidence also demonstrated that the predictive power of incidence is greater. This indicates that severity may not exert any influence on people’s perception of the diseases that affect them the most in their social-ecological systems, instead of potentiating it, as expected. One possible explanation may be related to the vulnerability of the socio-ecological systems: recent and regular experiences of prolonged drought in the regions (Martins et al., 2015) and their harmful consequences on agroecosystems and farmers. Among these implications, the scarcity of water is highlighted, with implications for people’s health; poor infrastructure, which does not meet local needs (the poor condition of local roads, for example); remoteness from the nearest urban centers; and the low purchasing power of farmers. Given this completely unfavorable scenario, it was observed that, as the farmers attested, they find themselves unmotivated or unable to seek adaptive strategies and treatments to deal with diseases perceived as more severe.
Observations about the lack of significance of severity in relation to people’s perception of diseases arising from climate change in the Catimbau NAPAR and Carão demonstrate that local conceptions of severity may be related to people’s previous experiences with certain diseases. This possible explanation finds support in evidence from the scientific literature (Miceli et al., 2008; Sachs et al., 2017; Scheideler et al., 2017; de Silva et al., 2019). For example, Sachs et al. (2017) demonstrated that diabetic patients’ concerns about adverse health events that they consider severe are systematically related to their past personal experiences with the diseases. da Silva et al. (2019) observed that university students from Northeastern Brazil tend to store adaptive information regarding diseases considered common and have low severity, which might be related to their experience with the diseases in question. Haque et al. (2012) found that farmers in Bangladesh perceive of greater concern diseases whose incidence is correlated with local extreme climate change events that they have had past personal experiences, such as drought and floods. This correlates with our field observations. Thus, this study supports the authors’ argument that these risks related to people’s past experiences should receive greater attention when designing and implementing adaptive coping strategies (Haque et al., 2012).
Finally, it was observed that farmers use more adaptive prophylactic behavior strategies. This might be because they are well supported by health information and services, either through a non-governmental organization (in the case of the Catimbau NAPAR communities) or a community health post (in the case of Carão). Research has highlighted that the adoption of personal prophylactic measures is influenced by factors such as knowledge, experience with the disease, and beliefs about health (Weinstein, 1993; Beaujean et al., 2013). Kisomi et al. (2016) found that the low index and inefficiency of prophylactic practices adopted among Malaysian farm workers regarding tick bites, which are transmitters of diseases in humans and animals, are related to low levels of knowledge and health beliefs, although they have extensive experience with the disease. Jin et al. (2020) highlighted the role of emotional factors, negatively correlated with risk communication, in the adoption of prophylactic behaviors related to the COVID-19 contagion. In this case, people’s experience with the disease and the amount of information about the risk of contamination is low because it is an emerging disease. Our study concluded that adequate prophylactic planning should be based on an open, honest, and updated flow of information, which can positively direct the adoption of adaptive measures, both prophylactic and therapeutic.
Conclusion
Our findings can provide useful information regarding the proposal and development of projects aimed at controlling and mitigating the diseases that most affect local populations in a scenario of increasingly extreme climate change in terms of speed and intensity. Hence, the growing importance of the dialogue between local ecological knowledge and scientific knowledge. The absence of this information can hinder understanding how people behave in these risk contexts and, consequently, the proposition of government policy measures favorable to social development in affected regions.
Our results suggest that some people’s understanding of incidence and severity may differ from the scientific community’s consensus. In this sense, it is advisable to conduct studies at local and global levels to identify the criteria people residing in different sociocultural contexts use to understand the concepts of incidence and severity. We also believe that diachronic studies that consider the influence of disease perception on the number of adaptive measures to treat them and the variation of knowledge associated with these treatments and their efficacy can help unravel the different factors that direct the evolution of medical systems. This can help fill gaps in the health literature.
Methodologically, our research introduced the PRM as a new approach for specific studies on the perception of human health risks. However, although it is a method that has a simple application and great practicality allowing researchers to analyze and evaluate results easily, these results may offer a limited and biased scope if not applied optimally or not considering an ideal scenario. In this sense, some considerations must be acknowledged. Although the low population density of the investigated communities, in addition to the low heterogeneity and the context of socio-environmental conflict evidenced in some communities of the Catimbau NAPAR, did not invalidate our results and conclusions, they may have limited its scope. Thus, further studies are recommended to compare more heterogeneous scenarios with more robust population densities. If the studies occur in conflict areas, we suggest that this factor must be considered in the experimental design of the research (which was not the case in our study).
Finally, it is recommended that this study is replicated, considering all the previously mentioned considerations, in different scenarios of prolonged climate change events (with high rainfall variation, for example) and, consequently, new diseases. Although our study focused only on diseases “perceived by people” and not “scientifically designated” diseases, we believe that further studies that compare these two types of information can provide broader insights. These additional studies may provide a more accurate understanding of the effect of the perception of diseases (especially those with the highest incidents) on the development of adaptive measures adopted to deal with their adverse effects and evaluate which strategies are more efficient. This information is essential for the proposition, elaboration, and application of predictive models based on people’s experiences in socio-environmental vulnerable contexts enhanced by extreme environmental changes and more efficient and favorable governmental policy measures for social development in affected regions.
Data Availability Statement
The raw data supporting the conclusion of this article will be made available by the authors, without undue reservation.
Ethics Statement
This study was submitted and approved by the Research Ethics Committee of the University of Pernambuco, according to the Certificate of Submission for Ethics Appreciation (CSEA) number 89890617.1.0000.5207, in order to meet the legal aspects of research involving human beings. All residents who agreed to participate in the research were asked to sign a free and informed consent form, as governed by the current legislation of the National Health Council (Resolution No. 466/2012). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
HM, IF, EdL, and UA designed and conceived the experimental design of the study. HM collected the data, performed the analyses, and wrote the initial manuscript. All authors contributed significantly to improving the manuscript and gave their final approval for publication.
Funding
This research was made possible by the National Institute of Science and Technology—Ethnobiology, Bioprospecting and Nature Conservation (INCT), which is certified by CNPq and financially supported by the Foundation for the Support of Science and Technology of the State of Pernambuco (FACEPE, grant no.: APQ-0562-2.01/17), for partial funding of the study; CAPES granted the doctoral scholarship to HFM; CAPES/FACEPE (PNPD Program), granted a post-doctoral scholarship to IF (CAPES/FACEPE: APQ-0700-2.05/16 and BCT-0259.2-05/17); and CNPq granted research productivity scholarships to ELA and UPA.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
This article is dedicated to the memory of our esteemed colleague and friend Ivanilda Soares Feitosa: mother, woman, and scientist. We are grateful for her dedication to this work as co-author and for establishing the necessary partnerships: her enthusiasm and dedication will be greatly missed. We are especially grateful to all the residents of the rural communities of the Catimbau NAPAR and the rural community of Carão who contributed to this study; to colleagues from the Laboratory of Ecology and Evolution of Socioecological Systems (LEA) who contributed to data collection; and to the Federal Rural University of Pernambuco (UFRPE) for providing transportation to the study area.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fenvs.2021.735595/full#supplementary-material
References
Albuquerque, U. P., Ramos, M. A., de Lucena, R. F. P., and Alencar, N. L. (2014). “Methods and Techniques Used to Collect Ethnobiological Data,” in Methods and Techniques in Ethnobiology and Ethnoecology. Editors U. P. Albuquerque, L. V. F. Cruz da Cunha, R. F. P. Lucena, and R. R. N. Alves (New York: Springer Protocols Handbooks), 15–37. doi:10.1007/978-1-4614-8636-7_2
Alvares, C. A., Stape, J. L., Sentelhas, P. C., de Moraes Gonçalves, J. L., and Sparovek, G. (2013). Köppen's Climate Classification Map for Brazil. Metz 22, 711–728. doi:10.1127/0941-2948/2013/0507
Austin, E. K., Rich, J. L., Kiem, A. S., Handley, T., Perkins, D., and Kelly, B. J. (2020). Concerns about Climate Change Among Rural Residents in Australia. J. Rural Stud. 75, 98–109. doi:10.1016/j.jrurstud.2020.01.010
Baird, T. D., Leslie, P. W., and McCabe, J. T. (2009). The Effect of Wildlife Conservation on Local Perceptions of Risk and Behavioral Response. Hum. Ecol. 37, 463–474. doi:10.1007/s10745-009-9264-z
Banerjee, R. R. (2014). Farmers' Perception of Climate Change, Impact and Adaptation Strategies: a Case Study of Four Villages in the Semi-arid Regions of India. Nat. Hazards 75, 2829–2845. doi:10.1007/s11069-014-1466-z
BDE (2017). Perfil Municipal. Altinho. Base de Dados Do Estado, Governo Do Estado de Pernambuco. Available at: http://www.bde.pe.gov.br/estruturacaogeral/PerfilMunicipios.aspx (Accessed November 9, 2020).
Beaujean, D. J. M. A., Bults, M., Van Steenbergen, J. E., and Voeten, H. A. C. M. (2013). Study on Public Perceptions and Protective Behaviors Regarding Lyme Disease Among the General Public in the Netherlands: Implications for Prevention Programs. BMC Public Health 13, 225. doi:10.1186/1471-2458-13-225
Bhatta, L. D., Udas, E., Khan, B., Ajmal, A., Amir, R., and Ranabhat, S. (2019). Local Knowledge Based Perceptions on Climate Change and its Impacts in the Rakaposhi valley of Gilgit-Baltistan, Pakistan. Ijccsm 12, 222–237. doi:10.1108/IJCCSM-05-2019-0024
Boillat, S., and Berkes, F. (2013). Perception and Interpretation of Climate Change Among Quechua Farmers of Bolivia: Indigenous Knowledge as a Resource for Adaptive Capacity. E and S 18, 21. doi:10.5751/ES-05894-180421
Brasil (2000). Lei n. 9.985, de 18 de julho de 2000. Regulamenta o art. 225, § 1o, incisos I, II, III e VII da Constituição Federal, institui o Sistema Nacional de Unidades de Conservação da Natureza e dá outras providências. Brasília: Presidência da República, Casa Civil, Subchefia para Assuntos Jurídicos.
Bryan, E., Ringler, C., Okoba, B., Roncoli, C., Silvestri, S., and Herrero, M. (2013). Adapting Agriculture to Climate Change in Kenya: Household Strategies and Determinants. J. Environ. Manage. 114, 26–35. doi:10.1016/j.jenvman.2012.10.036
Butler, C. D., and Harley, D. (2010). Primary, Secondary and Tertiary Effects of Eco-Climatic Change: The Medical Response. Postgrad. Med. J. 86, 230–234. doi:10.1136/pgmj.2009.082727
Costello, A., Abbas, M., Allen, A., Ball, S., Bell, S., Bellamy, R., et al. (2009). Managing the Health Effects of Climate Change. The Lancet 373, 1693–1733. doi:10.1016/s0140-6736(09)60935-1
Cruz, M. P., Medeiros, P. M., Sarmiento-Combariza, I., Peroni, N., and Albuquerque, U. P. (2014). "I Eat the Manofê So it Is Not Forgotten": Local Perceptions and Consumption of Native Wild Edible Plants from Seasonal Dry Forests in Brazil. J. Ethnobiol. Ethnomedicine 10, 45. doi:10.1186/1746-4269-10-45
Cunha, A. P. M. A., Zeri, M., Deusdará Leal, K., Costa, L., Cuartas, L. A., Marengo, J. A., et al. (2019). Extreme Drought Events over Brazil from 2011 to 2019. Atmosphere 10, 642. doi:10.3390/atmos10110642
da Silva, R. H., da Ferreira, W. S., Ferreira Júnior, W. S., Muniz de Medeiros, P., and Albuquerque, U. P. (2019). Adaptive Memory and Evolution of the Human Naturalistic Mind: Insights from the Use of Medicinal Plants. PLoS ONE 14, e0214300. doi:10.1371/journal.pone.0214300
da Silva, T. C., Cruz, M. P., de Sousa Araújo, T. A., Schwarz, M. L., and Albuquerque, U. P. (2014). “Methods in Research of Environmental Perception,” in Methods and Techniques in Ethnobiology and Ethnoecology. Editors U. P. Albuquerque, L. V. F. Cruz da Cunha, R. F. P. Lucena, and R. R. N. Alves (New York: Springer Protocols Handbooks), 99–109. doi:10.1007/978-1-4614-8636-7_7
de Albuquerque, U. P., de Lima Araújo, E., El-Deir, A. C. A., de Lima, A. L. A., Souto, A., Bezerra, B. M., et al. (2012). Caatinga Revisited: Ecology and Conservation of an Important Seasonal Dry Forest. Scientific World J. 2012, 1–18. doi:10.1100/2012/205182
de Perez, E, C., Nerlander, L., Monasso, F., van Aalst, M., Mantilla, G., Muli, E., et al. (2015). Managing Health Risks in a Changing Climate: Red Cross Operations in East Africa and Southeast Asia. Clim. Dev. 7, 197–207. doi:10.1080/17565529.2014.951012
Dhanya, P., and Ramachandran, A. (2016). Farmers' Perceptions of Climate Change and the Proposed Agriculture Adaptation Strategies in a Semi Arid Region of South India. J. Integr. Environ. Sci. 13, 1–18. doi:10.1080/1943815X.2015.1062031
dos Santos, D. M., da Silva, K. A., de Albuquerque, U. P., dos Santos, J. M. F. F., Lopes, C. G. R., and Araújo, E. d. L. (2013). Can Spatial Variation and Inter-annual Variation in Precipitation Explain the Seed Density and Species Richness of the Germinable Soil Seed Bank in a Tropical Dry forest in north-eastern Brazil? Flora - Morphol. Distribution, Funct. Ecol. Plants 208, 445–452. doi:10.1016/j.flora.2013.07.006
Espinosa, M. M., Bieski, I. G. C., and Martins, D. T. O. (2014). “Sampling in Ethnobotanical Studies of Medicinal Plants,” in Methods and Techniques in Ethnobiology and Ethnoecology. Editors U. P. Albuquerque, L. V. F. Cruz da Cunha, R. F. P. Lucena, and R. N. Alves (New York: Springer Protocols Handbooks), 197–212. doi:10.1007/978-1-4614-8636-7_13
Estomba, D., Ladio, A., and Lozada, M. (2006). Medicinal Wild Plant Knowledge and Gathering Patterns in a Mapuche Community from North-western Patagonia. J. Ethnopharmacology 103, 109–119. doi:10.1016/j.jep.2005.07.015
Ferreira, W. S., Nascimento, A. L. B., Ramos, M. A., Medeiros, P. M., Soldati, G. T., Santoro, F. R., et al. (2015). “Resilience and Adaptation in Social-Ecological Systems,” in Evolutionary Ethnobiology. Editors U. P. Albuquerque, P. M. Medeiros, and A. Casas (New York: Springer), 105–119. doi:10.1007/978-3-319-19917-7
Fosu-Mensah, B. Y., Vlek, P. L. G., and MacCarthy, D. S. (2012). Farmers' Perception and Adaptation to Climate Change: a Case Study of Sekyedumase District in Ghana. Environ. Dev. Sustain. 14, 495–505. doi:10.1007/s10668-012-9339-7
Gbetibouo, G. A. (2009). Understanding Farmers’ Perceptions and Adaptations to Climate Change and Variability: The Case of the Limpopo Basin, South Africa. Washington, D.C.: International Food Policy Research Institute Discussion.
Gonçalves, P. H. S., da Cunha Melo, C. V. S., de Assis Andrade, C., de Oliveira, D. V. B., de Moura Brito Junior, V., Rito, K. F., et al. (2021). Livelihood Strategies and Use of forest Resources in a Protected Area in the Brazilian Semiarid. Environ. Dev. Sustain. 24, 1–21. doi:10.1007/s10668-021-01529-3
Handley, T. E., Kay-Lambkin, F. J., Inder, K. J., Lewin, T. J., Attia, J. R., Fuller, J., et al. (2014). Self-reported Contacts for Mental Health Problems by Rural Residents: Predicted Service Needs, Facilitators and Barriers. BMC Psychiatry 14, 1–12. doi:10.1186/s12888-014-0249-0
Haque, M. A., Yamamoto, S. S., Malik, A. A., and Sauerborn, R. (2012). Households' Perception of Climate Change and Human Health Risks: A Community Perspective. Environ. Health 11, 1. doi:10.1186/1476-069X-11-1
Hayes, K., Blashki, G., Wiseman, J., Burke, S., and Reifels, L. (2018). Climate Change and Mental Health: Risks, Impacts and Priority Actions. Int. J. Ment. Health Syst. 12, 1–12. doi:10.1186/s13033-018-0210-6
ICMBio (2002). Decreto s/no de 13 de dezembro de 2002. Cria o Parque Nacional do Catimbau, nos Municípios de Ibirimirim, Tupanatinga e Buíque, no Estado de Pernambuco, e dá outras providências. Brasília: Instituto Chico Mendes de Conservção da Biodiversidade, Ministério do Meio Ambiente.
INMET (2021). Gráficos climatológicos: Pernambuco. Instituto Nacional de Meteorologia. Available at: https://clima.inmet.gov.br/GraficosClimatologicos/PE/82890 (Accessed August 28, 2021).
IPCC (2007). “Climate Change 2007: Synthesis Report,” in Contribution of Working Groups I, II and III to the Fourth Assessment Report of the Intergovernmental Panel on Climate Change. Editors C. W. Team, R. K. Pachauri, and A. Reisinger (Geneva: IPCC), 104. doi:10.1038/446727a
Jin, Z., Zhao, K.-b., Xia, Y.-y., Chen, R.-j., Yu, H., Tamunang Tamutana, T., et al. (2020). Relationship between Psychological Responses and the Appraisal of Risk Communication during the Early Phase of the COVID-19 Pandemic: a Two-Wave Study of Community Residents in China. Front. Public Health 8, 550220. doi:10.3389/fpubh.2020.550220
Kisomi, M. G., Wong, L. P., Tay, S. T., Bulgiba, A., Zandi, K., Kho, K. L., et al. (2016). Factors Associated with Tick Bite Preventive Practices Among Farmworkers in Malaysia. PLoS ONE 11, e0157987. doi:10.1371/journal.pone.0157987
Lafferty, K. D. (2009). The Ecology of Climate Change and Infectious Diseases. Ecology 90, 888–900. doi:10.1890/08-0079.1
Lima, J. R. d., and Magalhães, A. R. (2018). “Secas no Nordeste: registros históricos das catástrofes econômicas e humanas Do século 16 ao século 21,” in Parcerias Estratégicas. Editor CGEE (Brasília: Centro de Gestão e Estudos Estratégicos), 191–212.
Magalhães, A. R. (2016). “Vida e seca no Brasil,” in Secas no Brasil: política e gestão proativas. Editors E. De Nys, N. L. Engle, and A. R. Magalhães (Brasília: Centro de Gestão e Estudos Estratégicos; Banco Mundial), 19–35.
Magalhães, H. F., Oliveira, R. C. S., Feitosa, I. S., and Albuquerque, U. P. (2019). “Collection and Analysis of Environmental Risk Perception Data,” in Methods and Techniques in Ethnobiology and Ethnoecology. Editors U. P. Albuquerque, R. F. P. Lucena, L. V. F. Cruz da Cunha, and R. R. N. Alves (New York, NY: Springer Protocols Handbooks), 149–159. doi:10.1007/978-1-4614-8636-7
Marengo, J. A., Alves, L. M., Alvala, R. C. S., Cunha, A. P., Brito, S., and Moraes, O. L. L. (2018). Climatic Characteristics of the 2010-2016 Drought in the Semiarid Northeast Brazil Region. Acad. Bras. Ciênc. 90, 1973–1985. doi:10.1590/0001-3765201720170206
Marengo, J. A., Cunha, A. P. M. A., Nobre, C. A., Ribeiro Neto, G. G., Magalhaes, A. R., Torres, R. R., et al. (2020). Assessing Drought in the Drylands of Northeast Brazil under Regional Warming Exceeding 4 °C. Nat. Hazards 103, 2589–2611. doi:10.1007/s11069-020-04097-3
Marengo, J. A., Torres, R. R., and Alves, L. M. (2017). Drought in Northeast Brazil-past, Present, and Future. Theor. Appl. Climatol 129, 1189–1200. doi:10.1007/s00704-016-1840-8
Martins, E. S. P. R., De Nys, E., Molejón, C., Biazeto, B., Silva, R. F. V., and Engle, N. (2015). Monitor de Secas do Nordeste, em busca de um novo paradigma para a gestão de secas. 1st ed. Brasília: Banco Mundial. doi:10.13140/RG.2.1.4238.8886
McMichael, A. J. (2013). Globalization, Climate Change, and Human Health. N. Engl. J. Med. 368, 1335–1343. doi:10.1056/NEJMra1109341
McMichael, A. J., Woodruff, R. E., and Hales, S. (2006). Climate Change and Human Health: Present and Future Risks. The Lancet 367, 859–869. doi:10.1016/S0140-6736(06)68079-3
Miceli, R., Sotgiu, I., and Settanni, M. (2008). Disaster Preparedness and Perception of Flood Risk: a Study in an alpine valley in Italy. J. Environ. Psychol. 28, 164–173. doi:10.1016/j.jenvp.2007.10.006
ME (2015). Mapeamento e análise espectro-temporal das Unidades de Conservação de Proteção Integral da Administração Federal no Bioma Caatinga. Parque Nacional do Catimbau. Editor N. C. F. Freire Recife: Ministério da Educação, Fundação Joaquim Nabuco, Universidade Federal de Campina Grande).
Nyantakyi-Frimpong, H., and Bezner-Kerr, R. (2015). The Relative Importance of Climate Change in the Context of Multiple Stressors in Semi-arid Ghana. Glob. Environ. Change 32, 40–56. doi:10.1016/j.gloenvcha.2015.03.003
Oliveira, R. C. d. S., Albuquerque, U. P., da Silva, T. L. L., Ferreira Júnior, W. S., Chaves, L. d. S., and Araújo, E. d. L. (2017). Religiousness/spirituality Do Not Necessarily Matter: Effect on Risk Perception and Adaptive Strategies in the Semi-arid Region of NE Brazil. Glob. Ecol. Conservation 11, 125–133. doi:10.1016/j.gecco.2017.05.004
Oloukoi, G., Bob, U., and Jaggernath, J. (2014). Perception and Trends of Associated Health Risks with Seasonal Climate Variation in Oke-Ogun Region, Nigeria. Health & Place 25, 47–55. doi:10.1016/j.healthplace.2013.09.009
PELD Catimbau (2016). Projeto Ecológico de Longa Duração Sítio Parque Nacional Do Catimbau. Mapas temáticos. PELD-PRONEX Catimbau. Available at: https://www.peldcatimbau.org/mapas-tematicos (Accessed November 4, 2020).
Quinn, C. H., Huby, M., Kiwasila, H., and Lovett, J. C. (2003). Local Perceptions of Risk to Livelihood in Semi-arid Tanzania. J. Environ. Manage. 68, 111–119. doi:10.1016/S0301-4797(03)00013-6
R Development Core Team (2019). The R Project for Statistical Computing News via Twitter. Vienna: R Development Core Team.
Rodriguez, N., Eakin, H., and De Freitas Dewes, C. (2017). Perceptions of Climate Trends Among Mexican maize Farmers. Clim. Res. 72, 183–195. doi:10.3354/cr01466
Sachs, M. L., Sporrong, S. K., Colding-Jørgensen, M., Frokjaer, S., Helboe, P., Jelic, K., et al. (2017). Risk Perceptions in Diabetic Patients Who Have Experienced Adverse Events: Implications for Patient Involvement in Regulatory Decisions. Pharm. Med. 31, 245–255. doi:10.1007/s40290-017-0200-z
Santoro, F. R., and Albuquerque, U. P. (2020). What Factors Guide Healthcare Strategies over Time? A Diachronic Study Focused on the Role of Biomedicine and the Perception of Diseases in the Dynamics of a Local Medical System. Acta Bot. Bras. 34, 720–729. doi:10.1590/0102-33062020abb0002
Santoro, F. R., Ferreira Júnior, W. S., Araújo, T. A. d. S., Ladio, A. H., and Albuquerque, U. P. (2015). Does Plant Species Richness Guarantee the Resilience of Local Medical Systems? A Perspective from Utilitarian Redundancy. PLoS ONE 10, e0119826–18. doi:10.1371/journal.pone.0119826
Scheideler, J. K., Taber, J. M., Ferrer, R. A., Grenen, E. G., and Klein, W. M. P. (2017). Heart Disease versus Cancer: Understanding Perceptions of Population Prevalence and Personal Risk. J. Behav. Med. 40, 839–845. doi:10.1007/s10865-017-9860-0
Silva, J. M. C. d., Barbosa, L. C. F., Leal, I. R., and Tabarelli, M. (2017). “The Caatinga: Understanding the Challenges,” in Caatinga: The Largest Tropical Dry Forest Region in South America. Editors J. M. C. Silva, I. R. Leal, and M. Tabarelli (Berlin: Springer International Publishing), 3–19. doi:10.1007/978-3-319-68339-3_1
Slegers, M. F. W. (2008). "If Only it Would Rain": Farmers' Perceptions of Rainfall and Drought in Semi-arid central Tanzania. J. Arid Environments 72, 2106–2123. doi:10.1016/j.jaridenv.2008.06.011
Smit, B., and Wandel, J. (2006). Adaptation, Adaptive Capacity and Vulnerability. Glob. Environ. Change 16, 282–292. doi:10.1016/j.gloenvcha.2006.03.008
Smith, K., Barrett, C. B., and Box, P. W. (2000). Participatory Risk Mapping for Targeting Research and Assistance: With an Example from East African Pastoralists. World Dev. 28, 1945–1959. doi:10.1016/S0305-750X(00)00053-X
Smith, W. J., Liu, Z., Safi, A. S., and Chief, K. (2014). Climate Change Perception, Observation and Policy Support in Rural Nevada: A Comparative Analysis of Native Americans, Non-native Ranchers and Farmers and Mainstream America. Environ. Sci. Pol. 42, 101–122. doi:10.1016/j.envsci.2014.03.007
UNDRR (2009). “Summary and Recommendations: 2009 Global Assessment Report on Disaster Risk Reduction,” in Risk and Poverty in a Changing Climate: Invest Today for a Safer Tomorrow (Geneva, Switzerland: United Nations Office for Disaster Risk Reduction, International Strategy for Disaster Reduction), 24. doi:10.1037/e522342010-005
Watts, N., Adger, W. N., Agnolucci, P., Blackstock, J., Byass, P., Cai, W., et al. (2015). Health and Climate Change: Policy Responses to Protect Public Health. Lancet 386, 1861–1914. doi:10.1016/S0140-6736(15)60854-6
Watts, N., Amann, M., Ayeb-Karlsson, S., Belesova, K., Bouley, T., Boykoff, M., et al. (2018). The Lancet Countdown on Health and Climate Change: from 25 Years of Inaction to a Global Transformation for Public Health. The Lancet 391, 581–630. doi:10.1016/S0140-6736(17)32464-9
Weber, E. U. (2010). What Shapes Perceptions of Climate Change? Wires Clim. Change 1, 332–342. doi:10.1002/wcc.41
Weinstein, N. D. (1993). Testing Four Competing Theories of Health-Protective Behavior. Health Psychol. 12, 324–333. doi:10.1037/0278-6133.12.4.324
WHO (2009). Protecting Health from Climate Change: Global Research Priorities. Editor WHO (Geneva, Switzerland: World Health Organization, WHO Library Cataloguing-in-Publication Data).
WHOUNICEF (2004). Joint Statement: Clinical Management of Acute Diarrhoea (WHO/FCH/CAH/04.07). Geneva, Switzerland: World Health Organization, Department of Child and Adolescent Health and Development, and United Nations Children’s Fund, Programme Division.
WMO (2020). The Global Climate in 2015-2019. WMO Statements on Climate, 1249. Geneva, Switzerland: World Meteorological Organization.
Young, M., Wolfheim, C., Marsh, D. R., and Hammamy, D. (2012). World Health Organization/United Nations Children's Fund Joint Statement on Integrated Community Case Management: An Equity-Focused Strategy to Improve Access to Essential Treatment Services for Children. Am. J. Trop. Med. Hyg. 87, 6–10. doi:10.4269/ajtmh.2012.12-0221
Keywords: climate change, semi-arid, smallholder—farming sector, disease perception, adaptive strategies
Citation: Magalhães HF, Feitosa IS, Araújo EdL and Albuquerque UP (2022) Farmers’ Perceptions of the Effects of Extreme Environmental Changes on Their Health: A Study in the Semiarid Region of Northeastern Brazil. Front. Environ. Sci. 9:735595. doi: 10.3389/fenvs.2021.735595
Received: 02 July 2021; Accepted: 23 December 2021;
Published: 19 January 2022.
Edited by:
Orsolya Valkó, Hungarian Academy of Science, HungaryReviewed by:
Msafiri Mkonda, Sokoine University of Agriculture, TanzaniaChrispen Murungweni, Chinhoyi University of Technology, Zimbabwe
Copyright © 2022 Magalhães, Feitosa, Araújo and Albuquerque. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ulysses Paulino Albuquerque, dXBhNjc3QGhvdG1haWwuY29t