 Jessica Sheringham
Jessica Sheringham Joanna Klaptocz1
Joanna Klaptocz1 Marcella Ucci
Marcella Ucci
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Environ. Health, 15 August 2024
Sec. Housing Conditions and Public Health
Volume 3 - 2024 | https://doi.org/10.3389/fenvh.2024.1358484
This article is part of the Research TopicWomen In Environmental Health: Housing Conditions and Public HealthView all 4 articles
Background: Housing is a well-recognised determinant of health. It is not known, however, how local decision makers conceptualise the links between housing and health and, in turn, what opportunities they recognise to intervene to address health inequalities.
Materials and methods: A qualitative interview study was undertaken in two areas of London with a range of staff working for public services or local voluntary groups who had professional or lived experience of local housing problems. Data were analysed using a conceptual model that articulated how housing may lead to health inequalities.
Results: Twenty individuals were interviewed, comprising fifteen staff employed by two London Councils and five individuals working in the voluntary sector helping people with housing problems. All participants recognised the importance of structural inequalities in determining access to appropriate quality housing and in influencing the health effects of housing. Overcrowding emerged as a prominent theme, exemplifying the interrelated nature of housing problems. Participants actively considered how the role of public services could alleviate or exacerbate health inequalities. Interventions were often focused specifically on housing and were limited by participants' partial views of the housing-health landscape.
Discussion: A comprehensive framing of housing as a determinant of health inequities was a relevant lens to conceptualise the relationship between housing and health in London. Integration of policies, services and information is needed to design and implement holistic interventions to address inequalities associated with housing. Future conceptual models to understand the interrelationship between place, housing and health may benefit from explicit consideration of the role of public services.
The importance of housing as an environmental determinant of health has been widely recognised. Serious hazards in the home for example are estimated to cost the NHS £1.4bn/year (1). Housing is also widely recognised as a social determinant of health (2), with scholars emphasising how structural inequalities impact access to decent housing across aspects such as gender or race (2, 3). It is argued that structural differences in policies, power and resources lead to inequalities in intermediary determinants, such as housing. Indeed, there is ample evidence that exposures to substandard housing are not equally distributed across populations (4), For example, in England, household overcrowding is more than four times more prevalent in ethnic minority populations other than White British (5), and families living on low income are more than five times more likely to be living in poor quality housing than those on high incomes (6). In England, some groups are also more likely than others to live in homes with damp and mould, including those on low income, with disabilities, from ethnic minority backgrounds, and those with long-term illness (7).
In England, local and regional public services (local authorities) have various responsibilities for housing in their areas, typically for approximately 200,000 residents. These responsibilities include the management of council housing (public housing rented to households) but they also have duties for assessing and planning housing needs across all housing tenures (8, 9). Since 2013, local authorities have also been responsible for the public health of their residents (10). Responsibility for health services resides with the National Health Service (NHS), which holds administrative data on health.
It is not well understood how local authorities can (or should) intervene to address health inequalities linked to housing. There are two main reasons for this lack of understanding. Firstly, there is a lack of clear evidence on the health benefits of housing interventions (11, 12). The lack of evidence on how housing interventions can benefit health has led to calls for more research to understand the pathways by which housing interventions can influence health (13). The understanding of such pathways in a local and national context is important because they could inform prospective development or implementation of policy and/or interventions or they could help us understand why or how variable or unintended consequences of housing interventions arise. Secondly, there is evidence that health is not routinely considered in building policies at a national level (14). While local policies are affected by national policies, it is still not clear how local policies can or do consider health inequalities related to housing.
In this qualitative study, we set out to address two related objectives. Firstly, we sought to understand how local policy makers and resident representatives in two areas of London conceptualised local pathways linking housing and health inequalities. Secondly, we sought to understand the opportunities considered at a local level to address health inequalities from a policy perspective in an urban English setting.
An exploratory interview study was conducted in two areas of London with responsibility for a range of public services. Ethical approval was obtained from UCL Ethical Review Committee (2037/006). The study initially had a focus on understanding the availability and role of administrative data in evaluating and addressing health inequalities associated with housing. As part of the process we also needed to understand local priorities and opportunities for which data would be relevant. We therefore carried out interviews and workshops to explore local understandings of the pathways by which housing influences health inequalities. In this paper, we describe a secondary analysis of the interview data to explore participants' understandings of the pathways by which housing influences health inequalities and the opportunities they identified to address such inequalities.
Swope and Hernandez (2019) developed a conceptual model that provides a comprehensive view of how housing may lead to inequalities in health (15). This model was used as an underpinning theoretical framework for the study. The model proposes that structural inequalities lead to unequal distribution across four pillars of housing factors associated with health: cost (housing affordability), conditions (housing quality), consistency (residential stability) and context (neighbourhood opportunity). The mechanisms by which housing pillars are affected comprise availability of housing stock, distribution of resources and ability to develop financial resources through housing equity. These pillars may interact with each other and other structural inequalities to intensify and embed health inequalities.
We selected the Swope and Hernandez model firstly because it was built from a synthesis of multidisciplinary literature sources to provide a comprehensive framing of the relationship between housing and health, which aligned with our first objective of seeking to understand how participants conceptualised housing and health inequalities. Secondly, we selected this model because the authors have used it as the basis of recommendations for promoting health and equity (16), which aligned with our second objective, to understand participants' views on the opportunities available to them to intervene to reduce health inequalities associated with housing.
We used the conceptual model to inform data collection materials and analysis (described later). We did not seek to produce an exhaustive account of each element of the model, but used it to help us understand how actors conceptualised the pathways.
Informed by our data, we also drew on WHO's conceptual framework for social determinants of health. In this framework, structural mechanisms generate stratified and divided societies leading to “hierarchies of power, prestige and access to resources” (2). They arise from the broader socioeconomic and political context. We used Assari's conceptualization of structural inequalities (i.e., the effects policies and practices on a societal level, independent of individual actions, efforts, talent or needs), to distinguish structural inequalities in our data from the many reported variations in experiences or outcomes that may be due to more proximal determinants, such as (17).
The study was located in two London local authority areas, both with multicultural populations and where housing and use of data were priorities. LA1 was in inner London, and characterised by stark inequalities within very small areas. This borough had very limited green space, and had few opportunities to build more housing. LA2 was in outer London, characterised by high overall levels of socioeconomic disadvantage. It had set up an initiative to build and buy homes in its area to increase the supply of affordable housing to its residents.
Council staff and volunteers working with people experiencing housing problems were recruited from the two London boroughs. Staff in each of the two councils plus two key community organisations were approached to identify participants working in or with housing teams, public health and health intelligence and to broker introductions to the research team. Further participants were identified by snowball sampling, through asking participants to recommend others with relevant experience or roles. We sought similar numbers of participants in each geographical area, and at least 25% of the sample from voluntary or community sector perspectives.
Semi-structured interviews were conducted in January–June 2022 to explore participants' perceptions of how housing affects health and practical levers that could be targeted to achieve better health through housing interventions. A topic guide was developed using the Swope and Hernandez model (15), as a basis.
Initial descriptive analysis was conducted by EI with MU and JS and was shared with participants to check validity of our interpretation and discussed with staff to explore priorities for intervention. [ref webpage]
A secondary thematic analysis of these data was conducted by JK, which combined a deductive approach based on the Swope and Hernandez model with inductive coding to capture insights falling outside of the conceptual model.
An initial coding framework was iterated following independent double coding of two interviews by JS and frequent discussions between JS and JK to build a deeper common understanding of the conceptual model and how it applied to the dataset. Instances were discussed where data did not fit the conceptual model or where there was discrepancy in authors' interpretation of the data or coding framework, to identify new codes and thus possible adaptations/modifications of the model and ensuing recommendations. Due to the small number of subgroups in our data, we didn't seek to draw out comparisons between different types of participants to staff vs. community/voluntary sector and between boroughs.
Twenty interviews were conducted in total in 2022, comprising fifteen council staff in housing, environmental health, strategy, and public health departments, and five community and voluntary sector representatives who handle problems on behalf of minority ethnic groups, asylum seekers and social housing tenants (Table 1).
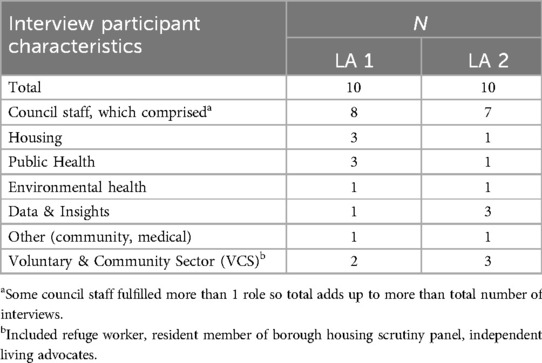
Table 1. Characteristics of interview participants (n = 20).
We address the first objective of participants' conceptualisations of housing and health pathways leading to health inequalities by describing below two interrelated themes. The first was structural inequalities, which emerged as an overarching driver of inequalities across the entire pathway from access to housing, to health outcomes. The second was household overcrowding, which exemplified the interacting mechanisms by which inequalities developed across all the pillars of housing in the Swope and Hernandez model (i.e., cost, conditions, consistency and context) (15). We selected these themes because they emerged as prominent across all the data and because they illustrate—in different ways—the relevance of the conceptual model to how pathways to inequalities may arise in an urban UK context.
We address our second objective, participants' views of the opportunities for intervening with the aim of reducing inequalities, through three key themes: the role of local public services, to capture the activities or agency of local policy making to effect change; integration of information across sectors concerned with housing and health; and joint working, to capture the ways in which local actors worked together i.e., within local authorities between directorates, between health and local authorities, or collaborations with voluntary, private sector or national partners.
All participants considered that in-built structural inequalities drove inequalities in health.
Participants gave multiple examples of barriers due to poverty, ethnicity, migration status, existing health needs or disability that manifested in creating unequal access to decent housing and inequitable services for those living in poor housing.
In both participating boroughs, high population density has led to low availability of adequately sized, affordable homes. Council staff commented on the disproportionate effects of this situation on those on low incomes.
“The poor are just pushed out and continue to be pushed out because it's too expensive to live.” (ID003, LA1, Staff)
Council staff also recognised how the application of the UK welfare system, which includes benefits such as a housing allowance for those unable to work or on low incomes, led to structural inequalities in access to decent housing. Some of these inequities related to income:
“The local housing allowance … which is the maximum that you can get with benefits covers nowhere near the level that is required to meet the rent in the private rented sector so people are forced to move out.” (ID006, LA1, Staff)
Other inequities related to ethnicity, for example where residents cared for family members in their own homes:
When we make payments to the individuals that require support so they could buy their own care one of the regulations is, if you live with the person that you are caring for you are not entitled to what is called direct payments. Now we found out very quickly that the community of Pakistani heritage in XXX tend to have their parents moving in with them, which effectively meant …they're not entitled to those direct payments. It's a bit of an unfair system, they are taking the burden from society, from the local authorities, to look after their parents but we are not supporting them. (ID016, LA2, Staff)
Several community and voluntary sector representatives described difficulties for renters in accessing repairs to housing, both within the private rental sector and social housing properties. Some residents simply did not report problems:
“[we surveyed] all the homes to see that they were in the right condition to return to us and there were quite a few where we picked up damp and mould issues that the resident hadn't self-reported …there are also residents who kind of live with those issues.” (ID013, LA1, Staff)
Where residents tried to report problems, there were many examples of difficulties in navigating systems to report housing problems and access help, particularly experienced by those new to the UK or with language barriers.
“Often they don't know how to work the services in terms of getting in contact with the council and how to do that here so often they call their GP as they are often told to, any problems call your GP.” (ID006, LA1, Staff)
In some cases, inequities occurred where council housing repairs systems were not set up adequately for disabled people. This resulted in multiple, avoidable problems in communication and instances where repair responses were unsatisfactory because disability had not been considered. In other cases, however, inequalities related specifically to asylum seekers appeared to result from more overt discrimination.
“A guy who's wheelchair-bound and some tradesmen came to do work on the property, and his flooring, it's like the wood flooring that kind of clips together to make it smooth, and they hadn't put it back properly so there was a lip in it, which meant he couldn't get past it in his wheelchair. So little things that anyone else, you would just step over it really, barely notice it, but he couldn't get through his living room because of it.” (ID013, LA2, Staff)
“…she's been asking for weeks, possibly months and bearing in mind that the agency supposedly has this property check every month, nothing had happened. Within four days of me sending photos and an email to the property people, they'd done it. And I find it really shocking … Is it because I'm a white middle-class nosy woman? And is it because she's an asylum seeker and her voice hasn't been heard?” (ID010, LA2, VCS)
Inequities in the response to housing problems impacted on both the severity of housing issues (worsening the longer they were unaddressed) and the extent to which housing issues affected individuals. Delays often led to more severe housing problems. It also affected residents’ mental wellbeing who reported feeling powerless to mediate change and/or frustration when issues weren't dealt with appropriately.
We focus on household overcrowding because it emerged as a major issue in almost all of the interviews we conducted. We also focus on it because, tudy participants' descriptions of overcrowding exemplify how multiple and interacting pathways connect housing with health and wellbeing, and associated inequalities.
While affordability was identified as a very strong driver of overcrowding, participants also noted how limited neighbourhood opportunity—the dense population of the areas—was a cause of overcrowding, at both neighbourhood and household level.
“There's that link of just not being able to afford somewhere big enough to give everyone their personal space.” (ID013, LA2, Staff)
“On the overcrowding side… really practical issues about where is the space to continue to build….” (ID0014, LA1, Staff)
Even those with the financial resources to move sometimes had to remain in overcrowded housing because of limited availability of adequately sized homes. Moreover, densely populated neighbourhoods and associated lack of outdoor space intensified the experience of lack of space in the home.
There was also recognition across participants that residents traded residential stability for overcrowding, particularly, though not exclusively amongst community and voluntary staff. They reported that residents sometimes chose to stay in a smaller home that becomes overcrowded as their family expands in order to access the community networks that enable them to work and care for their children.
“[this borough is] their home…their support network's here, their work's here, school's here….they could move out to somewhere that's perhaps going to be a bit better for their needs in terms of space and affordability but then they’d be isolated, so they’ve got that difficult choice to make.” (ID0011, LA1, Staff)
“They both felt that they was moved out and they felt very unhappy because all their family and all their connections [were in this borough]. They both worked and you know, family done child care and if the child wasn't well nan would look after them while they carried on working and they lost that.” (ID020, LA2, CVS)
In addition, some chose to become overcrowded in a single home because it enabled them to care for extended families:
“In some communities… it's not necessarily the lack of income of funding to move out it's the desire to look after ageing parents.” (ID001, LA2, Staff)
Participants described three major pathways through which they perceived overcrowding affected health inequalities: through increasing the likelihood and severity of damp and mould, and via the constraints it placed on opportunities for privacy and through the impacts on residents' capacity to carry out normal activities in the home. Specific health impacts were mentioned, particularly mental health issues, infections (increased risk of COVID-19) and chronic respiratory disease. However, rather than focusing on specific diseases, most participants referred to the impacts on general well-being and to function in the home. Participants also recognised the effects of overcrowding go beyond health and affect wider determinants of health, such as education and community safety.
“Mental health is a huge one. Then other things that come through, the second biggest one is I would say is respiratory problems. So you will frequently get patients calling about coughs, about chest infections, about difficulty breathing that they’ve attributed to the air quality in their home.” (ID009, LA1, Staff)
“I’ve also had quite a few examples of there being quite a few people in a property so then you’re very much on top of each other, going back to my Covid role obviously you can't then, if one of you gets Covid, can't isolate away from the rest of the family, so everyone would get it… I suppose just the mental health impact and everything of being so enclosed with everyone. And with working from home not having that space if you’ve got to work from home but everyone's sharing a two-bed and there's six of you in there and you’ve got kids running about it, it's difficult to be consumed by that as your daily life.” (ID013, LA2, Staff)
“It causes problems within the family, because if little kids need to go to bed and the adults or the teenagers are sharing the same room, that causes problems and tensions, and how do people do their homework? You know, where do you eat? All those sorts of things. Can even cause youngsters to go off the rails because they feel they can't stay at home, they have to be out, and when you're out, what do you do?” (ID019, LA1, VCS)
Staff in both councils were committed to the needs of their residents and sought to use public services to achieve equity for their residents. They described initiatives to directly address structural inequalities, for example, ensuring local policy prioritised people with specific needs, for example:
“..more recently we’ve… pulled out more bespoke housing offer for what we call more vulnerable groups. We mean by that, we mean care leavers, people who need adapted housing, older people increasingly, people with various disabilities, learning, mental health… the groups who their housing needs might not be met through normal stuff happening in the market or through standard council interventions… just making sure policies reflect their needs.” (ID014, LA1, Staff)
In one borough, one participant described aspirations to “municipalise the private rental sector” through exploiting the distinct levers they had as a council to take a role in building housing that was affordable for local people to rent. This would both increase the availability of housing stock to residents, and for those able to buy their homes, would enable them to build housing equity and financial resources.
Several council staff emphasized that their motivations were different from private sector builders, they had some financial capacity to buy land and build immediately in ways that could benefit residents:
“Private developers will wait for things, basically values go up a bit. That's what they would do. A few of them have done this actually. They bought a site in the borough, they will sit on it for a while, wait for values to go up and then they will build it. We're doing it now…building out schemes that no one else would build out, because we want to do it for the population, not because we want to make profit off it.” (ID005, LA2, Staff)
The barriers to reducing inequalities through building and financial levers were also recognised, however, both in terms of the scale they could feasibly impact (vs. the degree of housing need) and the financial constraints they were working under:
“We own the land, we’ve got the people now. We can access cheap funding. I think probably one challenge is kind of around scale. So we're currently building around 3,000 homes. Can we keep doing that? … there's a lack of support from government to buy and build properties, … that means that the finances are really, really tight.” (ID005, LA2, Staff)
Several participants within councils reflected on the difficulty of addressing housing problems without the support of wider public policy:
“…this isn't just a housing issue, this is a Housing, Health, Ministry of Justice and Department of Work and Pensions issue and it all has to be joined together…. if you invest in housing you then save the health budget and that's the bit that they don't get.” (ID006, LA1, Staff)
When all participants' views were interpreted together, they reflected a joined-up model of housing and health. Each participant's data, however, displayed disjointed and partial views. Most participants recognised that their lack of information across the pathway resulted in housing issues being addressed in a fragmented way.
To address this problem several council staff participants focused on the need for better sharing of routinely collected data on residents between teams and organisations. They commented on how this was needed to enable them to understand and respond to issues that residents faced.
“…[it relates to] public expectations, if they’ve given their data to the council they expect the council to know all of it, which they don't.” (ID007, LA1, Staff)
Some staff participants felt that increasing the granularity of these data could substantially change the learning and policy implications from it. For example, with respect to ethnicity, one participant gave an example of how combining micro-analysis of the subgroups of ethnicity with local knowledge of the cultural norms within communities:
“We have a lot of Asians of Bangladeshi heritage they are the most vulnerable, but when we dug even further … we found out that the Bangladeshi community in our borough are of the Sylheti heritage which makes a huge difference because suddenly your entire understanding of the culture changes.” (ID016, LA2, Staff)
Voluntary sector staff, in contrast, more commonly attributed the information gap to a lack of “joined up working”. They prioritised the need for clearer communication both across different branches of public services and with the public.
“A lot of it is about I think not communicating clearly, the staff it's their bread and butter, they do it every day. So they will use terminology that's familiar to them …it's a bit like you know going to see a doctor and they talk about it in some medical term. And you just need them to say, "You know, you have a cold or you have a whatever.” (ID010, LA2, VCS)
Generally, council staff gave examples of initiatives developed in one sector of the council, often quoting projects that sought primarily to increase and rebalance the availability of housing stock. Housing initiatives included renovating existing buildings to change the configuration of properties:
“In blocks like this they’re all one beds. You turn all 15 flats into two beds and as people move out or as they’re renovating or whatever, it's just a different way of thinking about the stock.” (ID004, LA1, Staff)
Councils were working on improving the conditions and quality of homes in council owned housing, through prioritising/preventing potentially harmful housing issues (e.g., damp) that that may develop as a result of overcrowding:
“We can carry out that, to some extent, quite peripheral work like repairs, and trying to make the home as liveable as possible.” (ID003, LA1, Staff)
However, councils observed they were constrained in the improvements they could make by national funding and planning regulations. For example:
“…[for] street properties Victorian and Georgian street properties. There's a lot of planning constraints about what you can do and how they have to look and all those kind of things that make it even more challenging to, kind of, change windows and things like that would make a real difference to the building.” (ID002 LA1 Staff)
Moreover, levers to improve housing conditions in the private rented sector were also acknowledged by many participants to be weak. Some participants referred to their use of selective licensing of private sector landlords (18), but resources to implement this effectively at a council level were limited, which meant they were unable to identify all unlicensed privately rented properties or in those they had identified, to follow up on problems within them:
“Trying to find the unlicensed premises, the amount of work it generates is just beyond what you could imagine, … being able to follow-up on these issues… in a timely manner.” (ID013, LA2, Staff)
However, both council staff and voluntary sector participants recognised some initiatives outside of housing that sought to address wellbeing associated with housing circumstances. For example, in relation to the neighbourhood and the role of community assets, there were examples of cross-sector working to improve wellbeing within the home.
“We’re looking at things like you know organising plays to get the kids out of the overcrowded accommodation for a period of time.” (ID006, LA1, Staff)
“I’ve brought in the parks people and transport planners and ourselves along with the newbuild people, the people that are leading on the development to say, right, when we do this can we have a safe route between the park and the canal through the estate. So, that we can encourage people, primarily out the estate into the park.” (ID007, LA1, Staff)
Moreover, representatives from the voluntary sector also reported how they were working with the council to improve the consideration of health considerations in design in council housing, recognising people's needs (and health circumstances) are likely to change over time:
“We've worked with the council to futureproof future housing by building it with widened doors, so if people are in a wheelchair as they get later on in life, they can still stay in the same premises or not have it adapted, and that lights and switches are at a position that if you're in a wheelchair, you can reach them.” (ID019, LA1, VCS).
This qualitative study of place-based relationships between housing and health found a consistent perception that structural barriers are a major cause of inequitable access to decent, affordable housing and may exacerbate the effects on health of exposure to poor housing. The study also indicated that participants recognise the multifaceted and interrelated nature of pathways between housing and health but often only have a partial view of such pathways, and limited agency to effect change outside of their own sector. Greater integration across sectors, within and beyond housing, may enable design and implementation of more holistic interventions that could tackle the drivers of health inequalities.
As a qualitative study, this research seeks to report on participants' views of the links between housing and health, and does not seek to provide any empirical data to quantitatively test such associations. This study had a small sample size and thus limited capacity to compare and contrast between subgroups within the data. It was focused on a narrow geographical area, with highly dense populations. This limits the study's transferability to other areas of the UK but was valuable in providing a highly localised perspective.
The Swope and Hernandez (2019) conceptual model takes a historical lens on how inequalities build over time from housing circumstances (15). It was beyond the scope of our study to explore in depth how inequalities originated or developed over time. However, its contemporary lens provides some insight into how housing can interact with major events. For example, interviews were taking place shortly after major lockdown due to COVID-19 whilst some restrictions to movement and requirements to isolate when infectious were still in place. Therefore, the experience of being confined to the home during COVID-19 was still ongoing for some individuals at this point. In addition, working from home remains a reality for many now and likely strengthens the relationships between which housing affects health.
There have been few studies of housing-health pathways, particularly in a UK context. One exception to this was Rolfe et al's (2000) realist evaluation of rehousing for social and private sector renters in west central Scotland (19). Our data were in line with their findings of the importance of tenants' experience of property quality and neighbourhood. In contrast, their data did not support the importance of housing affordability, whereas in our context, housing affordability emerged as a central determinant of wellbeing. This difference may be because at the time of Rolfe et al's study, housing benefit covered rents for many participants whereas several participants in our study observed that housing benefit did not adequately cover the cost of rent. One of the reasons for this difference could be the differences in the costs of housing between our study contexts. In London, rents are particularly high relative to wages and the opportunities for development, at least for one of the boroughs, impacted on the availability of housing locally. Also, at the time of the interviews, the cost-of-living crisis was felt deeply in the UK (20).
According to our literature search, there were no prior examples of the application of the Swope and Hernandez model to a UK context. Our findings, however, do concur with Ucci et al's study in another area of London which found the model captured well the complex web of interactions through which the housing and the neighbourhood impact family wellbeing (21). Additionally, we describe three ways in which this conceptual model can be adapted to be helpful in a UK context.
Firstly, the comprehensive conceptualisation of housing as a risk factor for inequalities helps to articulate the importance of structural inequalities in driving health inequalities associated with housing. Swope and Hernandez's framework proposes that, the effects of exposures are likely to be different depending on an individual's prior vulnerabilities and also the resources they have access to improve their health (see Figure 1, adapted from Swope and Hernandez). Therefore, the most disadvantaged groups (because they have less power and resources) are not just the ones most exposed to poor housing conditions, they are also more susceptible to its harmful effects on health (see Figure 1, mediators/moderators). These factors may also modifythe effectiveness of housing interventions and thus help to explain the evidence of uncertain, heterogeneous and sometimes counterintuitive effects of housing improvements on health (20). It could also help to further develop Thomson and Thomas's theory, which proposed that socioeconomic conditions may mediate the effects of housing improvements on health, by widening to broader structural inequalities and prompting consideration of residents' prior contextual circumstances in the design of future interventions (13).

Figure 1. Adaptation from Swope and Hernandez (15). Conceptual model of the impact of housing on health inequalities, for a UK urban context. The original model is in black font, with adaptations in red. Adapted from Housing as a determinant of health equity: A conceptual model, Carolyn B. Swope, Diana Hernández 243:112571 (2019), with permission from Elsevier.
Secondly, we suggest adapting the model to a UK context. This was because we found a consistent theme in our data on the role of public services in addressing health inequalities which did not fit the conceptual model so well. We speculate this misalignment might be because of contextual differences between the US and UK in the prominence of the public sector in housing, health and welfare, and also due to the differences in responsibilities for policies in these fields; in England for example, housing is predominantly the responsibility of local councils, but welfare policies are set at national level. In our study, local services emerged as important in several ways. Local policy makers—motivated by a vision to provide equitable housing for their local residents—recognised the distinct ways in which local public building programmes had the potential to address health inequalities in ways that the private sector couldn't. For example, public services were not driven by a profit motive and had the capacity to borrow more cheaply than the private sector. They faced barriers to realising their vision, however, which included a lack of national policy support. Local actors also recognised the unintended consequences of other public services on equitable housing provision and health, which—in common with Carmichael et al's finding at a national level—underlines the need to consider housing as part of a wider system (14). It has led us to make adaptations to the Swope and Hernandez framework for a UK setting. We have delineated both housing specific and wider public policies affecting health, informed by Mari'-Dell'Olmo et al, to signify that inequalities associated with housing are not only influenced by housing policy (22). We have also added a fifth pillar for intermediate determinants of health associated with housing—for public services and welfare at local and national levels—for the model for the UK context, to capture how the interrelationship between provision of health and social care services and housing and role of relevant welfare provision and entitlement (such as employment support, housing benefits) can mitigate or exacerbate inequalities. We add this pillar to emphasize that public services are not experienced as distal or unidirectional but closely linked to and influenced by resident experience and health. Furthermore, public services and welfare policies not only influence the other four pillars, but also are shaped by them, particularly at local level (Figure 1). This adaptation of the Swope and Hernandez model aligns it more closely with evidence generated from other studies conducted in a European context, which more explicitly explore—and describe—how public services can mitigate the health effects of poor or insecure housing (23).
Thirdly, we note that participants generally held only a partial view of housing and health pathways. Many recognised that an integrated understanding is needed to inform interventions to address inequalities. Our findings are in line with Hernandez and Swope's companion paper, which recommends taking a holistic perspective to intervention design and integration across different scientific disciplines (16). Strategies to adopt a more integrated approach include adopting governance arrangements in public services that bring together representatives of housing, public health and treatment services with representatives from other services such as education and social care, as advocated by Marmot et al. as a “whole systems approach” (24). Practical enactment of such strategies can include enabling sharing of residents' housing and health conditions data to facilitate referrals, and expedite repairs or rehousing when health is at risk. A clearer understanding can also be built through more frequent and clearer communication between individuals in different organisations and with residents.
This qualitative interview study underscores the relevance of a comprehensive framing of housing as a determinant of health, and of local interventions underpinned by system-wide approaches. This framing—alongside addressing barriers to integration—can help to promote consideration of the relationships between multiple exposures on health and to prompt holistic approaches to policy change and intervention design. Building a stronger shared understanding of the pathways by which inequitable access to decent housing conditions could strengthen capacity for local policies to reduce health inequalities.
The raw data that was used in this article are not readily available because participants did not consent to others outside of the research team having access to their interviews.
The studies involving humans were approved by University College London Ethical Review Committee (Ref: 2037/006). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
JS: Conceptualization, Formal Analysis, Funding acquisition, Methodology, Project administration, Supervision, Writing – original draft. JK: Formal Analysis, Writing – review & editing. EI: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Writing – review & editing. MU: Conceptualization, Funding acquisition, Methodology, Supervision, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
This report is independent research funded by the UCL Health of the Public Small Grants Scheme and supported by the National Institute for Health and Care Research ARC North Thames. The views expressed in this publication are those of the author(s) and not necessarily those of the National Institute for Health and Care Research or the Department of Health and Social Care.
This project was a collaboration between London Boroughs of Barking and Islington, Care City and HealthWatch Islington. We wish to thank all those that generously gave their time to be interviewed, source lived experiences or take part in discussions.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Wilson W, O'Donnell M, Bellis A, Barton C. The Cost of Unhealthy Housing to the National Health Service (2019). Available online at: https://commonslibrary.parliament.uk/research-briefings/cdp-2019-0046/ (Accessed December 14, 2023).
2. World Health Organisation. A Conceptual Framework for Action on the Social Determinants of Health. Geneva: WHO Press (2010). Available online at: https://www.who.int/publications/i/item/9789241500852 (Accessed June 24, 2024).
3. Hahn RA. What is a social determinant of health? Back to basics. J Public Health Res. (2021) 10(4). doi: 10.4081/jphr.2021.2324
4. Krieger J, Higgins DL. Housing and health: time again for public health action. Am J Public Health. (2002) 92(5):758–68. doi: 10.2105/AJPH.92.5.758
5. Ministry of Housing, Communities and Local Government. Overcrowded households (2020). Available online at: https://www.ethnicity-facts-figures.service.gov.uk/housing/housing-conditions/overcrowded-households/latest#by-ethnicity-and-area (Accessed December 14, 2023).
6. Try L. Trying Times: How People Living in Poor Quality Housing Have Fared During the Cost of Living Crisis. London: Resolution Foundation (2023). Available online at: www.resolutionfoundation.org/publications (Accessed June 26, 2023).
7. Department of Levelling Up, Housing and Communities, Department of Health and Social Care, UK Health Security Agency. Understanding and addressing the health risks of damp and mould in the home. Available online at: www.gov.uk (Accessed December 14, 2023).
8. The Housing Act 1985 (2018). Available online at: https://www.legislation.gov.uk/ukpga/1985/68/resources (Accessed December 14, 2023).
9. Department of Housing, Communities and Local Government. The Strategic Housing Role of Local Authorities: Powers and Duties. London: Department of Communities and Local Government (2008).
10. The Local Authorities (Public Health Functions and Entry to Premises by Local Healthwatch Representatives) Regulations 2013 (SI 2013/351), 351 (2013).
11. Ige J, Pilkington P, Orme J, Williams B, Prestwood E, Black D, et al. The relationship between buildings and health: a systematic review. J Public Health. (2018) 41(2):e121–e32. doi: 10.1093/pubmed/fdy138
12. Thomson H, Thomas S, Sellstrom E, Petticrew M. Housing improvements for health and associated socio-economic outcomes. Cochrane Database Syst Rev. (2013) 2:CD008657. doi: 10.1002/14651858.CD008657.pub2
13. Thomson H, Thomas S. Developing empirically supported theories of change for housing investment and health. Soc Sci Med. (2015) 124:205–14. doi: 10.1016/j.socscimed.2014.11.043
14. Carmichael L, Prestwood E, Marsh R, Ige J, Williams B, Pilkington P, et al. Healthy buildings for a healthy city: is the public health evidence base informing current building policies? Sci Total Environ. (2020) 719:137146. doi: 10.1016/j.scitotenv.2020.137146
15. Swope CB, Hernández D. Housing as a determinant of health equity: a conceptual model. Soc Sci Med. (2019) 243:112571. doi: 10.1016/j.socscimed.2019.112571
16. Hernández D, Swope CB. Housing as a platform for health and equity: evidence and future directions. Am J Public Health. (2019) 109(10):1363–6. doi: 10.2105/AJPH.2019.305210
17. Assari S. How unjust social structures help some but harm others 2019. Available online at: https://theconversation.com/how-unjust-social-structures-help-some-but-harm-others-113622 (Accessed December 14, 2023).
18. Department of Levelling Up, Housing and Communities. Selective Licensing in the Private Rented Sector: A Guide for Local Authorities. London: Department of Levelling Up, Housing and Communities (2023). Available online at: www.gov.uk (Accessed December 14, 2023).
19. Rolfe S, Garnham L, Godwin J, Anderson I, Seaman P, Donaldson C. Housing as a social determinant of health and wellbeing: developing an empirically-informed realist theoretical framework. BMC Public Health. (2020) 20(1):1138. doi: 10.1186/s12889-020-09224-0
20. Greater London Authority. The rising cost of living and its effects on Londoners (2022). Available online at: https://data.london.gov.uk/dataset/the-rising-cost-of-living-and-its-effects-on-londoners (Accessed December 14, 2023).
21. Ucci M, Ortegon-Sanchez A, Mead NE, Godward C, Rahman A, Islam S, et al. Exploring the interactions between housing and neighbourhood environments for enhanced child wellbeing: the lived experience of parents living in areas of high child poverty in England, UK. Int J Environ Res Public Health. (2022) 19(19):12563. doi: 10.3390/ijerph191912563
22. Marí-Dell’Olmo M, Novoa AM, Camprubí L, Peralta A, Vásquez-Vera H, Bosch J, et al. Housing policies and health inequalities. Int J Health Serv. (2017) 47(2):207–32. doi: 10.1177/0020731416684292
23. Vásquez-Vera H, Fernández A, Novoa AM, Delgado L, Barcala J, Macías C, et al. Our lives in boxes: perceived community mediators between housing insecurity and health using a PHOTOVOICE approach. Int J Equity Health. (2019) 18:52. doi: 10.1186/s12939-019-0943-0
24. The Marmot Review. Fair Society Healthy Lives (2010). Available online at: https://www.instituteofhealthequity.org/resources-reports/fair-society-healthy-lives-the-marmot-review (Accessed June 28, 2024).
Keywords: housing, health, inequalities, policy, public health, overcrowding
Citation: Sheringham J, Klaptocz J, Ingram E and Ucci M (2024) Understanding placed-based pathways by which housing is related to health inequalities: a qualitative interview study in London. Front. Environ. Health 3:1358484. doi: 10.3389/fenvh.2024.1358484
Received: 19 December 2023; Accepted: 22 July 2024;
Published: 15 August 2024.
Edited by:
Steven Schmidt, Lund University, SwedenReviewed by:
Hugo Vásquez-Vera, Pan American Health Organization, United States© 2024 Sheringham, Klaptocz, Ingram and Ucci. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jessica Sheringham, ai5zaGVyaW5naGFtQHVjbC5hYy51aw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.