
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Environ. Health , 21 September 2023
Sec. Housing Conditions and Public Health
Volume 2 - 2023 | https://doi.org/10.3389/fenvh.2023.1202149
This article is part of the Research Topic Insights in Environmental Health: 2023 View all 5 articles
 Patricia González-Marín1,2
Patricia González-Marín1,2 Hugo Vásquez-Vera1*Antonio López-Gay3,4Andrés Peralta5,6
Hugo Vásquez-Vera1*Antonio López-Gay3,4Andrés Peralta5,6 Miguel Solana-Solana3
Miguel Solana-Solana3 Ana Fernández1,7
Ana Fernández1,7
Background: Prior studies have reported conflicting findings on the impact of gentrification of neighborhood residents. While some suggest it could worsen mental health, others indicate improved self-perceived health, although this effect may vary among social groups. This study aimed to determine health inequities, according to socioeconomic position, among residents of different neighborhoods of Barcelona between 2011 and 2017, considering the intensity of the gentrification process.
Methods: Observational study with two transversal cuts (2011 and 2017). Neighborhoods were categorized into three groups based on the intensity of gentrification: intensive, moderate-mild, and no gentrification processes. We fitted Poisson robust models to estimate the prevalence ratio (PR) of poor self-reported and poor mental health according to socioeconomic position (social class III vs. I). We then calculated relative differences between 2011 and 2017 through the interaction between the year and socioeconomic position (PRi). The calculations were adjusted for age and household disposable income in the neighborhood and were stratified by sex.
Results: In neighborhoods undergoing moderate or mild gentrification during the study period, we found widening inequities in mental health between the most disadvantaged social class and the most privileged social class. Between 2011 and 2017, relative differences in poor mental health increased in moderate-low gentrification neighborhoods [women: PRi: 2.51 (1.52–4.17); men: PRi: 1.99 (1.09–3.61)], equivalent to an increase of 12.9 and 11.5 percentage points, respectively. No statistically significant differences were found in the other neighborhoods.
Discussion: The increase in mental health inequalities observed among residents of transitional neighborhoods could be explained by factors such as residential insecurity, eviction from the neighborhood, and rising housing prices.
Neighborhoods of major cities are experiencing dramatic and rapid demographic and socioeconomic changes. Neighborhoods are known to be core social determinants of health and consequently it is crucial to understand how these changes impact the quality of life, wellbeing and health of their residents. One of these changes is gentrification, which can be defined as “a process in which neighborhoods with low SES [socioeconomic status] experience increased investment and an influx of new residents of higher SES” (1). Gentrification has several consequences, including the physical displacement of vulnerable residents and symbolic displacement, which can be defined as a process whereby residents do not recognize the “new” neighborhood and feel disconnected (2).
The drivers of gentrification can vary depending on the context, making it crucial to understand the urban renewal story of each city and its specific factors (3). In the case of Barcelona, Spain, the city has undergone significant transformations that have altered its urban landscape and social and demographic composition (4). One notable change is the considerable increase in tourists visiting the city, especially since the 1992 Olympic Games, which has led to the conversion of long-term housing into tourist accommodation, mainly in the city center. This transformation has significantly affected the daily lives of the city's residents (5, 6).
Additionally, young migrant adults with higher incomes and university education have been drawn to Barcelona's urban core due to the city's dynamism and lifestyle possibilities. These dynamics have stimulated housing rehabilitation and appreciation, but have also resulted in the displacement of long-standing residents, particularly older adults (7). Moreover, these dynamics have also altered the commercial network in the city centre (8).
The appeal of visiting and living in Barcelona, along with political factors such as insufficient public housing and significant liberalization of the real estate market, have contributed to a surge in housing prices (9). Consequently, there is a heightened risk of housing insecurity and accelerated displacement of residents to other neighborhoods or peripheral municipalities (10, 11).
The literature on the health effects of gentrification is gaining increasing attention but is inconclusive. Some studies have shown a relationship between gentrification and psychosocial stress (12) and poor mental health (13). These effects are often attributed to the breakdown of social networks, housing insecurity, the loss of attachment to a place, and displacement of long-term residents. A recent study reported a range of potential poor health outcomes and pathways associated with gentrification. At the individual level, these include individual-level physical and mental health issues, such as obesity, asthma, chronic stress, and depression. At the neighborhood level, gentrification may affect health determinants such as safety and the emergence of new drug-dealing/use. At the institutional level, gentrification may also influence health determinants, such as healthcare precariousness and worsened school conditions (14).
However, two recent systematic reviews (1, 15) have concluded that the impact of gentrification on health is not homogeneous across social groups, with variations along different axes of inequality, such as age, race, gender, and social class. For example, research indicates that older adults living in gentrified neighborhoods have a higher risk of anxiety and depression than people living in non-gentrified neighborhoods, regardless of the economic resources available in the area (16).
On the other hand, other studies have found that self-rated health was better among people living in gentrified environments than among those living in a non-gentrified neighborhood, although the stratification of results showed that racial minorities living in newly-gentrified areas may experience a negative effect on their self-rated health (17, 18). This suggests that gentrification may improve overall self-rated health in the neighborhood but conceal negative consequences on the health of vulnerable groups, thus widening health inequalities across social axes.
Another axis of inequality is gender. Historically, women have been assigned different responsibilities to men, mainly focused on reproductive tasks, while men have been assigned responsibilities the productive sphere (19). These distinct social constructs influence how people interact with the city. Typically, men perceive the neighborhood as a place of leisure and rest (20), while women use it to create support networks (21) and often make use of existing resources and facilities close to the family home (20). Thus, due to the social and emotional links established by women with their residential environment, the urban, economic, and social transformations of the neighborhood brought about by gentrification may have a greater impact on women than on men (19, 22).
Gentrification is a dynamic and progressive phenomenon, characterized by various processes unfolding over time. Moreover, there is already broad evidence of health inequalities in Barcelona, which are found in all neighborhoods in the city (23–25).
In this study, we hypothesized that in highly gentrified or gentrifying neighborhoods, inequalities related to health, especially mental health, would be exacerbated, particularly in women. This hypothesis was based on the observations mentioned above, showing that processes of gentrification disrupt community cohesion, leading to the breakdown of social support systems and weakening protective factors for mental health, especially for long-term residents as they witness the transformation of their neighborhood. Rising house prices in the area can create additional stress for people if they cannot afford the cost of housing. In addition, as the cost of housing rises, residents may be less able to afford other necessities, which can impact their health.
This study aimed to investigate whether health inequalities changed in neighborhoods that were gentrified between 2011 and 2017 in Barcelona, the aftermath of the economic crisis of 2008.
We conducted a cross-sectional study with two cut-off points. Our study universe consisted of non-institutionalized individuals aged more than 15 years residing in Barcelona (26, 27). The main data sources were the Barcelona Health Survey for the years 2011 and 2016/2017. This survey is conducted every 5 years by the Barcelona Public Health Agency in a representative sample of the population of the city to obtain data on their health, disabilities, health-related behaviors, and their physical and socioeconomic context. Participants are selected in advance and are contacted at home by professional interviewers. The survey is administered through personal, home-based interviews conducted by the professional interviewers.
Dependent variables consisted of self-rated health and the risk of poor mental health. To assess self-rated health, participants were asked “How is your health in general?” Response options were “excellent”, “very good”, “good”, “fair”, and “poor”. We created a dichotomous outcome variable, with the responses “fair” or “poor” coded as “poor self-rated health” (28). Mental health was evaluated using the 12-item version of the General Health Questionnaire (12-GHQ). Participants with a score of ≥3 were classified as having a high probability of poor mental health (29–31).
Explanatory variables consisted of individual socioeconomic position, the level of gentrification, and the year.
To assess socioeconomic position, we used the social class classification of the Spanish Society of Epidemiology, which comprises five categories, based on the individual's current or last occupation (32). These five categories were recoded as follows: (a) social class I (I + II), the highest social class; (b) social class II (III), and (c) social class III (IV + V), the lowest social class.
To evaluate the neighborhoods’ gentrification process, we used the Gentrification Index (GI) (33). The GI is a composite index comprising seven theoretical dimensions associated with various axes of neighborhood socioeconomic transformation: (a) population rejuvenation; (b) changes in the origin of the population, understood as the growth of the population born in countries with a high Human Development Index; (c) changes in family arrangements/values, associated with the growth of single-person adult households; (d) attraction to the population with a university degree; (e) population substitution, understood as a loss of the population without a university degree due to the effect of migration and changes of residence; (f) speed of change, which introduces the transformative capacity of migratory and residential flows to modify the composition of the population; (g) transformations in the housing market, measured through price increases.
The GI yields a final score ranging from 0 to 1, where 0 indicates the lowest degree of gentrification between 2011 and 2017 and 1 indicates the highest degree. We categorized the neighborhoods in three groups based on quartiles (Figure 1): C1 (GI => 0.51), neighborhoods that underwent intense gentrification processes between 2011 and 2017; C2-C3 (GI > 0.30 and GI < 0.51), neighborhoods with moderate or mild processes associated with gentrification; and C4 (GI <= 0.31), neighborhoods not undergoing any significant gentrification processes between 2011 and 2017 (33).
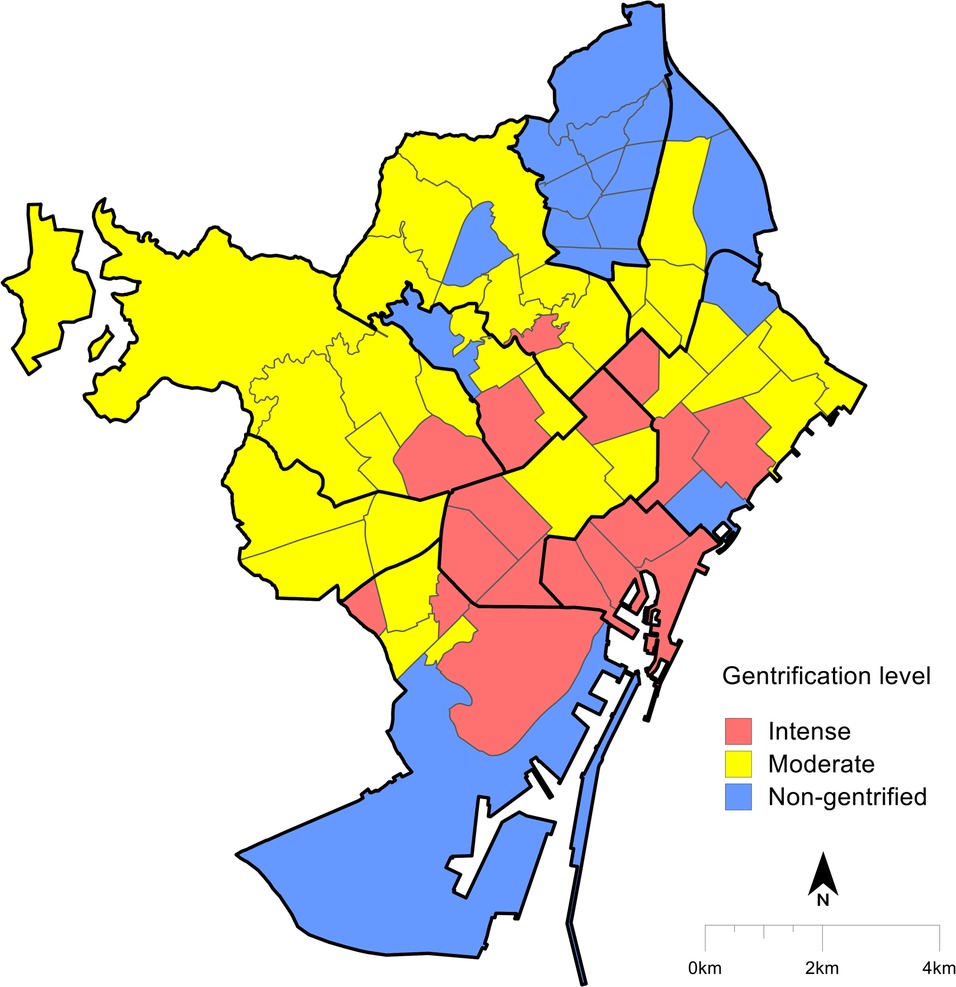
Figure 1. Neighborhood typology according to the gentrification index (2011–2017) (33).
Level of gentrification and sex (i.e., women/men) were used as stratifying variables. We made this decision, based on two hypotheses. Firstly, we hypothesized that health inequalities would increase in neighborhoods with high or moderate-low gentrification processes, while these inequalities would remain stable in non-gentrified neighborhoods. Secondly, we chose to stratify by sex (as a proxy of gender), because we hypothesized that inequalities would be more pronounced among women, as they are more affected by changes related to gentrification, such as changes in businesses, housing prices, and the breakdown of social networks).
Age and the average household disposable income index were included as adjusting variables, to avoid potential confounding factors. The household disposable income index was obtained from data provided by the Barcelona City Council Department of Statistics (34). This index is a theoretical indicator that is constructed from gross household disposable income and gross household disposable income per capita, while also including variables related to the level of education of the resident population, employment status, the characteristics of the motor fleet, and housing prices. The indicator reveals the relative position of each territorial unit in relation to the average of the city, set at a value equal to one hundred.
Firstly, we performed a descriptive analysis of the dependent and sociodemographic variables, by the level of gentrification (i.e., intense, moderate/mild or none) of the neighborhood, sex, and year.
Then, we combined the databases of 2011 and 2017 to estimate if there were any differences in the magnitude of health-related inequalities between 2011 and 2017. We stratified the analysis by sex and level of gentrification.
We estimated the prevalence ratios (PR) and their 95% confidence intervals (95% CI) for poor self-rated health and poor mental health when comparing class III with class I. We fitted three Poisson regression models with robust variance, introducing the interaction between year and social class. The inclusion of this interaction allowed us to identify whether variations in health inequalities during the period were statistically significant. The result of the interaction can be interpreted as a relative difference between the PR of each year (i.e., as a ratio of prevalence ratios) or,
The three models were:
(1) Model 1: crude model including only the interaction between year and social class.
(2) Model 2: Model 1 adjusted by age.
(3) Model 3: Model 2 adjusted by the household disposable income index. Only results from model 3 are presented in this article. Using the results of model 3, we calculated absolute differences by using the margins command in STATA, which allowed us to predict PRs and their 95% CI. Finally, to ease interpretation, we generated graphs that illustrated the difference between individuals in class III and class I who reported poor self-rated health and risk of poor mental health in 2011 and 2017 with 95% CI. Once this was done, we estimated the absolute difference, i.e., the difference of the differences:
Databases were anonymized and all analyses were weighted according to the Barcelona Health Survey's weights. The statistical software used for the analysis was STATA 15.
The sample included 1,645 women and 1,600 men in 2011 and 1,780 women and 1,606 men in 2017. The sociodemographic and health characteristics of the sample are shown in Table 1. Analysis of social class revealed that neighborhoods without gentrification processes had a higher percentage of women and men in social class III, which increased sharply from 2011 to 2017. In neighborhoods with mild-moderate gentrification, the distribution of social class was fairly homogeneous, except for men in the year 2011. Neighborhoods experiencing intense gentrification processes had slightly more women and men in class III, and no significant changes were observed between 2011 and 2017.
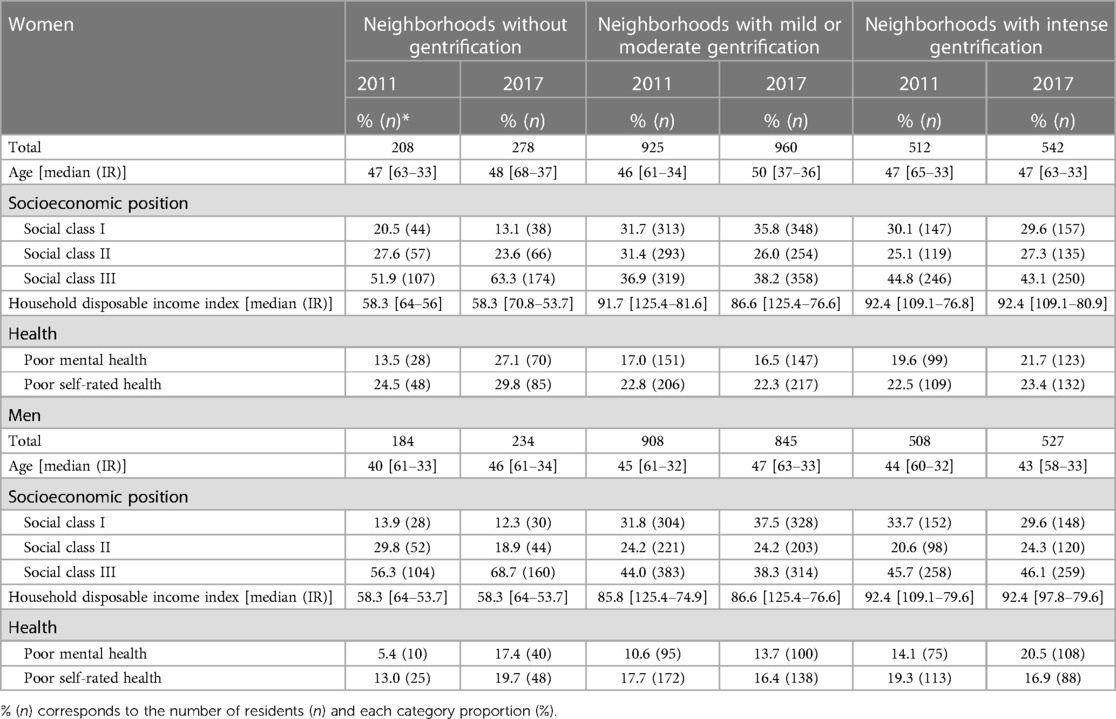
Table 1. Socioeconomic and health characteristics of Barcelona residents, stratified by the gentrification process of the neighborhood, sex, and year.
The prevalence of poor mental health in women increased between 2011 and 2017, regardless of social class and the gentrification process experienced by the neighborhood, with the exception of women in class I living in neighborhoods undergoing mild-moderate gentrification processes, where the prevalence decreased. The pattern in men was similar.
In contrast, the prevalence of poor self-rated heath in women in class I decreased or remained stable between 2011 and 2017, but generally increased among women in class III, regardless of the gentrification-related process of the neighborhood. In men, the prevalence of poor self-rated health increased or remained stable, regardless of social class, except among those in class I living in neighborhoods undergoing mild or moderate processes, where it decreased (for more details see Supplementary Material Appendix 1).
In neighborhoods with moderate or mild gentrification processes, the absolute difference in the percentage of women with poor mental health between class III and class I was 1.3 percentage points (Figure 2A). In 2017 this difference was 14.2 percentage points. Thus, inequalities increased during the period by 19.9 points, which was statistically significant. The increase in inequalities was also reflected in the relative difference in PRs (PRi) between 2011 and 2017, which more than doubled in all models [e.g., PRi = 2.51 (95% CI = 1.53–4.17)] (for more details see Supplementary Material Appendix 2). The same pattern was observed in neighborhoods without gentrification processes, but the results were not statistically significant. In neighborhoods with intense gentrification processes, the absolute difference between 2011 and 2017 decreased by 0.8 percentage points, but this decrease was not statistically significant.
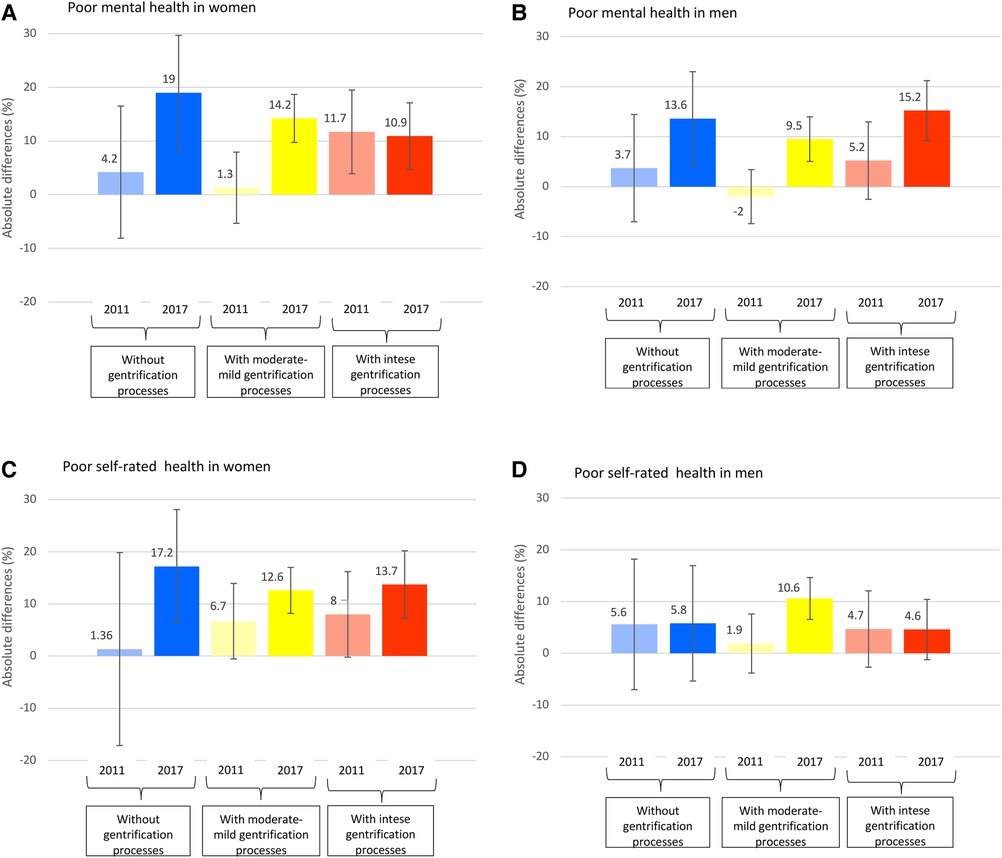
Figure 2. (A–D) Absolute differences in poor mental health and poor self-rated health by socioeconomic position, stratified by the gentrification processes of the neighbourhood, sex, and year.
Among men (Figure 2B), in neighborhoods with moderate or mild gentrification processes, the absolute difference between class III and class I was −2 in 2011, increasing to 9.5 points in 2017 (11.5 percentage points), which was statistically significant. As among women, this was also reflected in the relative difference of PRs (PRi) between 2011 and 2017, which nearly doubled in all models [e.g., PRi = 1.99 (95% CI = 1.09–3.61)] (Supplementary Material Appendix 2). In neighborhoods with and without intense gentrification processes, we observed no significant differences between 2011 and 2017.
Inequalities in self-rated health among women (Figure 2C) showed the same pattern as in mental health for neighborhoods without gentrification and moderate or mild gentrification processes, although the results were not statistically significant. Among neighborhoods with intense gentrification processes, poor self-rated health increased between 2011 and 2017, but this increase was not statistically significant. In men (Figure 2D), the increase in inequalities between 2011 and 2017 was smaller than that in women, and was not statistically significant.
This study shows that inequities in mental health between the most disadvantaged social class and the most privileged social class widened between 2011 and 2017 in neighborhoods with a moderate or mild gentrification level during the study period. However, in neighborhoods not undergoing gentrification and those undergoing intense gentrification, health inequalities remained unchanged between 2011 and 2017. We observed no changes in self-rated health inequalities between 2011 and 2017 in any of the neighborhoods.
Gentrification processes lead to several changes in neighborhoods that may affect residents’ health, but their impact differs depending on the social group to which residents belong (35). For example, one of the processes occurring in gentrifying neighborhoods is the influx of private capital for reinvestment in the area, which can modify the neighborhoods’ housing market (36). Thus, the owners of both land and properties may view the urban transformation of neighborhoods as a business opportunity to attract individuals with greater purchasing power or tourists, driving up the prices of housing and commercial premises. Consequently, there may be instances of real estate mobbing, with forced displacement of the most disadvantaged residents to make room for more lucrative real estate opportunities (7).
This type of residential insecurity and fear of being driven out of the neighborhood can cause psychosocial stress (12), negatively affecting mental health (13, 14). In addition, the replacement of traditional stores by tourist-oriented or trendy shops that do not cater to the daily needs of long-term residents from lower social classes directly affects their quality of life and health (6).
These mechanisms, among others, contribute to increasing health inequalities among disadvantaged groups. However, the extent of these phenomena varies, depending on the stage of gentrification. They may be more pronounced in neighborhoods that are recently undergoing changes (mild or moderate gentrification), where most disadvantaged people from lower social classes have not yet been displaced. In contrast, in neighborhoods with intense gentrification (advanced stages of sociodemographic replacement), most residents would tend to have higher purchasing power and, in general, better health status. Even individuals from lower social classes (as measured by occupational classification) who manage to remain in intensely gentrified areas are likely to possess characteristics related to other axes of inequality, such as gender, immigration status, or income, which enable them to adapt to the changes in their neighborhood or even benefit from them. Consequently, health inequalities in intensely gentrified areas may persist or even decrease. Indeed, our findings show that health inequalities were maintained in neighborhoods with intense gentrification between 2011 and 2017, although there was a slight tendency for them to decrease in women.
Finally, in non-gentrified neighborhoods, we observed a non-significant increase in health inequalities between 2011 and 2017. Most of these neighborhoods are inhabited by people from disadvantaged social classes, who may have been particularly affected by the consequences of the economic crisis. Since 2011, Spain implemented austerity policies that affected the viability of the welfare state. These policies included labor market reforms, such as making dismissal cheaper and reducing unemployment benefits, as well as increasing value added tax from 18% to 21% and from 8% to 10%, and implementing health co-payment (37), among other measures. These changes in the economic landscape increased job instability and the cost of living, which had direct repercussions on the finances of the most disadvantaged people, affecting their health.
Although inequalities in mental health were similar in women and men, gentrification could have a more negative effect on women due to the different ways in which they use city spaces, which are often linked to their assigned social roles (19). Even in contemporary times, women still bear a disproportionate burden as caregivers, particularly those in the most disadvantaged social classes, as women in more privileged backgrounds are more likely to hire individuals to perform caregiving tasks. To fulfill these caregiving responsibilities, basic services and facilities must be available in the neighborhood. However, gentrification leads to the loss of local businesses, nearby leisure and care spaces, and neighborhood support networks, making it challenging to carry out daily activities and caregiving and resulting in longer and more time-consuming journeys (19). Gentrification tends to reinforce a city model that prioritizes economic performance and caters to the productive sphere, often neglecting the public reproductive sphere where women, especially those from the most disadvantaged social classes, engage in their daily activities (19).
This study has several limitations. The main limitation is that the sample is not representative at the neighborhood level because the information source (the Barcelona Health Survey) is only representative at the district level. However, this issue may be minimized to some extent by the grouping of neighborhoods. Another limitation is the small sample size of some groups of neighborhoods, which became more pronounced on stratification by different variables. Moreover, the generalisability of the results is limited because the processes related to gentrification are highly influenced by the unique social and political context of each city or territory. Therefore, our results can only be applied to similar contexts. Finally, the GI may not fully capture the gentrification process of the city's neighborhoods due to the complexity of the phenomenon.
Despite these limitations, to our knowledge, this is the first study on health inequalities due to gentrification in Spain and it was carried out by a multidisciplinary public health team and experts in neighborhood change and gentrification. In addition, this study may be useful for local policy makers- or those in similar contexts -to design and implement public policies aiming to reduce social and health inequalities. For future research, it would be interesting to study gentrification with mixed methodologies to further deepen understanding of the relationship between gentrification and health. Similarly, the gender and intercultural perspective should be incorporated, in addition to other axes of inequality such as age.
The results of this study show that gentrification may increase mental health inequalities, especially at the start of the gentrification process. This impact is observed both in men and women, but more research is needed to validate these results and to understand the mechanisms that may underpin them.
The datasets presented in this article are not readily available because the datasets are the property of the Public Health Agency of Barcelona. Any request has to be done through official channels. Requests to access the datasets should be directed todmFzcXVlemh1Z0BwYWhvLm9yZw==.
Ethical review and approval was not required for this study in accordance with the national legislation and the institutional requirements. Written informed consent was not required for this study in accordance with the national legislation and the institutional requirements.
PG designed the research protocol, conducted the analysis and wrote the first draft of the article. HV designed the research protocol, supported the analysis and interpretation of findings, reviewed the first draft of the manuscript and prepared the final version of the article. AL supported methodology and instruments related to gentrification measures, reviewed the first draft of the manuscript. AP supported methodology and instruments related to gentrification measures, reviewed the first draft of the manuscript. MS-S supported methodology and instruments related to gentrification measures, reviewed the first draft of the manuscript. AF designed the research protocol, supported the analysis and interpretation of findings, reviewed the first draft of the manuscript and coordinated the study. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors HV and AF declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fenvh.2023.1202149/full#supplementary-material.
1. Smith GS, Breakstone H, Dean LT, Thorpe RJ Jr. Impacts of gentrification on health in the US: a systematic review of the literature. J Urban Health. (2020) 97:845–56. doi: 10.1007/s11524-020-00448-4
2. Elliott-Cooper A, Hubbard P, Lees L. Moving beyond Marcuse: gentrification, displacement and the violence of un-homing. Prog Hum Geogr. (2019) 44(3):492–509. doi: 10.1177/0309132519830511
3. Hyra D. Commentary: Causes and Consequences of Gentrification and the Future of Equitable Development Policy. Cityscape. (2016) 18(3):169–77. https://www.american.edu/spa/metro-policy/upload/hyra-2016-cityscape-proofs.pdf
4. Degen M, García M. The transformation of the “Barcelona model”: an analysis of culture, urban regeneration and governance. Int J Urban Reg Res. (2012) 36.5:1022–38. doi: 10.1111/j.1468-2427.2012.01152.x
6. Sánchez-Ledesma E, Vásquez-Vera H, Sagarra N, Peralta A, Porthé V, Díez È; Photovoice Working Group of Public Health Agency of Barcelona. Perceived pathways between tourism gentrification and health: a participatory photovoice study in the Gòtic neighborhood in Barcelona. Soc Sci Med. (2020) 258:113095. doi: 10.1016/j.socscimed.2020.113095
7. Cocola-Gant A, Lopez-Gay A. Transnational gentrification, tourism and the formation of “foreign only” enclaves in Barcelona. Urban Stud. (2020) 57(15):3025–43. doi: 10.1177/0042098020916111
8. Fresnillo I. Los mercados renovados, ¿motor de gentrificación? Barcelona Metròpolis Número. (2018) 107:79–81.
10. Alemany A, Colau A, Escorhuela I, Odonia A, Pidemont M, Pisarello G, et al. Emergencia habitacional en el estado español. (2013).
11. Observatori DESC—Plataforma de Afectados por la Hipoteca. Emergència habitacional a Catalunya. (2015).
12. Mehdipanah R, Marra G, Melis G, Gelormino E. Urban renewal, gentrification and health equity: a realist perspective. Eur J Public Health. (2017) 28(2):243–8. doi: 10.1093/eurpub/ckx202
13. Wilder V, Mirto AL, Makoba E, Arniella G. The health impact of gentrification. J Gen Emerg Med. (2017) 2(5). Available at: https://scientonline.org/JGEM-5-030.pdf (Accessed November 11, 2019).
14. Anguelovski I, Triguero-Mas M, Connolly JJT, Kotsila P, Shokry G, Perez Del Pulgar C, et al. Gentrification and health in two global cities: a call to identify impacts for socially-vulnerable residents. Cities Heal. (2019) 4:40–9. doi: 10.1080/23748834.2019.1636507
15. Bhavsar NA, Kumar M, Richman L. Defining gentrification for epidemiologic research: a systematic review. PLoS One. (2020) 15(5):e0233361. doi: 10.1371/journal.pone.0233361
16. Smith RJ, Lehning AJ, Kim K. Aging in place in gentrifying neighborhoods: implications for physical and mental health. Gerontologist. (2018) 58(1):26–35. doi: 10.1093/geront/gnx105
17. Gibbons J, Barton MS. The association of minority self-rated health with black versus white gentrification. J Urban Heal. (2016) 93(6):909–22. doi: 10.1007/s11524-016-0087-0
18. Izenberg JM, Mujahid MS, Yen IH. Health in changing neighborhoods: a study of the relationship between gentrification and self-rated health in the state of California. Health Place. (2018) 52:188–95. doi: 10.1016/j.healthplace.2018.06.002
19. Col·lectiu Punt 6. Urbanismo feminista. Por una transformación radical de los espacios de vida. Barcelona: Virus Editorial (2019). 221.
20. Santos G. L’urbanisme barceloní, una mirada a la vida quotidiana. Barcelona Metròpolis Número. (2017) 104:10–4.
21. Balagueró LG. L’impacte de la gentrificació en les dones. Barcelona Metròpolis Número. (2018) 107:24–5.
22. Ortiz-Guitart A, López-Gay A, Sales-Favá J, Solana-Solana M. La gentrificación desde una mirada de género: un ejemplo en Barcelona. Ciudad y Territ Estud Territ. (2021) 53(210):945–62. doi: 10.37230/CyTET.2021.210.03
23. Rodríguez-Fonseca M, Palència L, Marí-Dell'Olmo M, Gandarillas A, Domínguez-Berjón MF, et al. Evolution of socio-economic inequalities in mortality in small geographical areas of the two largest cities in Spain (Barcelona and Madrid), 1996–2007. Public Health. (2013) 127(10):916–21. doi: 10.1016/j.puhe.2013.07.001
24. Marí-Dell'Olmo M, Gotsens M, Pasarín MI, Rodríguez-Sanz M, Artazcoz L, Garcia de Olalla P, et al. Socioeconomic inequalities in COVID-19 in a European urban area: two waves, two patterns. Int J Environ Res Public Health. (2021) 18(3):1256. doi: 10.3390/ijerph18031256
25. López-Contreras N, Rodríguez-Sanz M, Novoa A, Borrell C, Medallo Muñiz J, Gotsens M. Socioeconomic inequalities in suicide mortality in Barcelona during the economic crisis (2006–2016): a time trend study. BMJ Open. (2019) 9(8):e028267. doi: 10.1136/bmjopen-2018-028267
26. Bartoll X, Rodríguez-Sanz M, Borrell C. Manual de l’Enquesta de salut de Barcelona 2011. Barcelona: Agència de Salut Pública de Barcelona (2012).
27. Bartoll X, Baranda L, González JM, Perez K, Pasarin M, Rodríguez-Sanz M, et al. Manual metodològic de l’Enquesta de salut de Barcelona de 2016/17. Barcelona: Agència de Salut Pública de Barcelona (2018).
28. Quesnel-Vallée A. Self-rated health: caught in the crossfire of the quest for “true” health? Int J Epidemiol. (2007) 36:1161–4. doi: 10.1093/ije/dym236
29. Goldberg D. Manual of the general health questionnaire. Windsor, England: NFER Publishing (1978).
30. Sánchez-López MDP, Dresch V. The 12-item general health questionnaire (GHQ-12): reliability, external validity and factor structure in the Spanish population. Psicothema. (2008) 20(4):839–43.
31. Bones Rocha K, Pérez K, Rodríguez Sanz M, Borrell C, Obiols Llandrich J. Propiedades psicométricas y valores normativos del general health questionnaire (GHQ-12) en población general española. Int J Clin Heal Psychol. (2011) 11(1):125–39.
32. Domingo-Salvany A, Bacigalupe A, Carrasco JM, Espelt A, Ferrando J, Borrell C. Propuestas de clase social neoweberiana y neomarxista a partir de la clasificación nacional de ocupaciones 2011. Gac Sanit. (2013) 27(3):263–72. doi: 10.1016/j.gaceta.2012.12.009
33. López-Gay A, Sales-Favà J, Solana M, Fernández A, Peralta A. Midiendo los procesos de gentrificación en Barcelona y Madrid: Una propuesta metodológica. XII CTV, XIII Int Conf Virtual City Territ (2019).
34. Departament d’Estadística i Difusió de Dades. Ajuntament de Barcelona. Estadística i Difusió de Dades. (2017).
35. Ministerio de Sanidad; Servicios Sociales e Igualdad. Comisión para reducir las desigualdades sociales en salud en España. Avanzando hacia la equidad. Propuestas de políticas e intervenciones para reducir las desigualdades sociales en salud en España. Madrid: Ministerio de Sanidad, Servicios Sociales e Igualdad. Gobierno de España (2015).
36. Smith N. La nueva frontera urbana. Ciudad revanchista y gentrificación. Traficantes de Sueños (2012). 380.
37. Mateos A, Penadés A. Spain: crisis and cutouts. Rev Cienc Polit. (2013) 33(1):161–83. Available at: https://www.cis.es/cis/opencms/ES/index.html (Accessed July 17, 2020).
Keywords: health inequalites, urban health, gentrification, housing, mental health, self-rated health
Citation: González-Marín P, Vásquez-Vera H, López-Gay A, Peralta A, Solana-Solana M and Fernández A (2023) Gentrification and its association with health inequalities in Barcelona (2011–2017). Front. Environ. Health 2:1202149. doi: 10.3389/fenvh.2023.1202149
Received: 7 April 2023; Accepted: 30 August 2023;
Published: 21 September 2023.
Edited by:
Ayodeji E. Iyanda, Prairie View A&M University, United StatesReviewed by:
Veronica Toffolutti, Queen Mary University of London, United Kingdom© 2023 González-Marín, Vásquez-Vera, López-Gay, Peralta, Solana-Solana and Fernández. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hugo Vásquez-Vera dmFzcXVlemh1Z0BwYWhvLm9yZw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.