 Izadora Sthephanie da Silva Assis1,2†
Izadora Sthephanie da Silva Assis1,2† Kaio Cezar Rodrigues Salum1,2,3†
Kaio Cezar Rodrigues Salum1,2,3† Rafaela de Freitas Martins Felício4
Rafaela de Freitas Martins Felício4 Lohanna Palhinha1
Lohanna Palhinha1 Gabriella de Medeiros Abreu2,5Tamara Silva6
Gabriella de Medeiros Abreu2,5Tamara Silva6 Fernanda Cristina Carvalho Mattos5Eliane Lopes Rosado5
Fernanda Cristina Carvalho Mattos5Eliane Lopes Rosado5 Verônica Marques Zembrzuski2
Verônica Marques Zembrzuski2 Mario Campos Junior2
Mario Campos Junior2 Clarissa Menezes Maya-Monteiro1
Clarissa Menezes Maya-Monteiro1 Pedro Hernán Cabello2
Pedro Hernán Cabello2 João Regis Ivar Carneiro3
João Regis Ivar Carneiro3 Patrícia Torres Bozza1‡
Patrícia Torres Bozza1‡ Ana Carolina Proença da Fonseca1,2,6,7*‡
Ana Carolina Proença da Fonseca1,2,6,7*‡- 1Laboratory of Immunopharmacology, Oswaldo Cruz Institute, Oswaldo Cruz Foundation, Rio de Janeiro, Brazil
- 2Human Genetics Laboratory, Oswaldo Cruz Institute, Oswaldo Cruz Foundation, Rio de Janeiro, Brazil
- 3Clementino Fraga Filho University Hospital, Federal University of Rio de Janeiro, Rio de Janeiro, Brazil
- 4Birth Defects Epidemiology Laboratory, Oswaldo Cruz Institute, Oswaldo Cruz Foundation, Rio de Janeiro, Brazil
- 5Josué de Castro Nutrition Institute, Federal University of Rio de Janeiro, Rio de Janeiro, Brazil
- 6Genetics Laboratory, Grande Rio University/AFYA, Rio de Janeiro, Brazil
- 7Postgraduate Program in Translational Biomedicine, Grande Rio University/AFYA, Rio de Janeiro, Brazil
Introduction: Genetic obesity is considered a rare disease, affecting up to 10% of patients with severe early-onset obesity. Over the past years, significant advances have been made; however, the majority of patients are misdiagnosed with polygenic obesity. Thus, this study aimed to identify deleterious copy number variations (CNVs) linked to obesity and explore the clinical phenotypes.
Method: The sample comprised 195 adults with severe obesity (BMI≥35kg/m2) who developed this phenotype during childhood or adolescence. We investigated the CNV using Multiplex Ligation-dependent Probe Amplification [MLPA] and real-time PCR. Chromosomal microarray analysis was used to assess the extent of genomic alterations.
Results: One patient showed a ~206 kb deletion in the distal of the 16p11.2 region, encompassing twelve genes. The gene linked to the development of severe obesity was SH2B1. This alteration was found in a male patient with metabolic syndrome (MS), and hypertension. Two patients exhibited a large deletion in the proximal of the 16p11.2 region. One patient showed a ~534 kb deletion without twenty-nine genes. This female patient had hypertension and bronchitis. The other patient presented a ~598 kb deletion of the proximal 16p11.2 region, including thirty-two genes. This female patient exhibited MS, and moderate binge-eating disorder.
Conclusion: Our study showed three genomic deletions at the 16p11.2 region in patients with severe obesity from Brazil. These results support the clinical utility of genetic testing to identify patients with the genetic form of obesity who may benefit from specific medical treatment, family genetic counseling, and targeted therapeutic intervention.
Introduction
Obesity is defined as excessive fat accumulation, which may impair health (1). The common form of obesity has a multifactorial etiology; however, monogenic forms were identified in human (2). Genetic obesity is a rare disease, affecting up to 10% of patients with extreme and early-onset obesity (3). It occurs due to single-gene alterations or genomic copy number variants (CNVs), leading to both syndromic and non-syndromic forms of obesity. The main difference is the presence of development delay and intellectual deficit in syndromic obesity (4, 5). Several genes were identified as potential causes of non-syndromic monogenic obesity (NSMO), most of which are involved in hypothalamus development and/or the leptin-melanocortin pathway. These patients exhibit severe obesity with early onset and hyperphagia, caused by disruption of the satiety systems (2, 5, 6). In Brazil, previous results of our group identified 7 potential pathogenic variants in adult patients with severe obesity (5.7%), who developed this phenotype during childhood (7–11).
In recent years, new technological developments have allowed the characterization of new genetic forms of monogenic obesity due to CNVs. These genomic variations in several chromosomal regions were described in patients with genetic forms of severe obesity. Examples include deletions of chromosome band 6q16 including the SIM1 gene, 11p13 which includes the BDNF gene, the recurrent 220-kb deletion of distal 16p11.2 including the SH2B1 gene (OMIM #613444), and the recurrent 600-kb 16p11.2 proximal deletion (OMIM #611913, unknown gene) (4, 12–14). Molecular diagnosis is crucial to detect patients who might benefit from specific medical management, target therapeutic intervention, and genetic counseling to the patient and family. Despite this importance, the majority of individuals with genetic obesity are underdiagnosed (15).
To our knowledge, no reports of CNVs in Brazilian patients with NSMO were found in the literature. Thus, this study aimed to investigate potential CNVs linked to obesity and explore the clinical phenotype of the patients.
Material and methods
Patients
This cross-sectional observational study included 195 adult subjects with severe obesity and early onset from Rio de Janeiro, Brazil. Inclusion criteria were: severe obesity phenotype (BMI ≥ 35 kg/m2), developed during childhood (0-11 years, n=128 individuals) or adolescence (12-21 years, n=67 individuals), and also a candidate for bariatric surgery in our country. The period of obesity onset was self-reported. Exclusion criteria were: (1) pregnancy, (2) lactation, and (3) the presence of symptoms suggestive of syndromic obesity (cognitive delay, dysmorphic characteristics, and organ-specific developmental abnormalities). All patients were volunteers of a non-governmental organization, Rescue Group to Self-Esteem and Citizenship of the Obese (in Portuguese, “Grupo de Resgate à Autoestima e Cidadania do Obeso”). This study was approved by the Ethics Committee of the Oswaldo Cruz Foundation (CAAE:09225113.0.0000/Protocol N°: 346.634) and informed written consent was obtained from all participants before inclusion in this study.
Blood samples were collected after a 12-hour overnight fasting period. A metabolic workup was obtained, including a lipid profile, fasting glucose, glycated hemoglobin, reactive C PCR, blood pressure, and anthropometric parameters (weight, height, waist, hip, and neck circumference). We also measured serum concentration of leptin, resistin, monocyte chemoattractant protein-1/CCL2 (MCP1), and plasminogen activator inhibitor-1 (PAI-1) by Human Adipocyte Magnetic Bead (Millipore-Merck [cat# HADCYMAG-61 k]) on Bio-Plex 200 Multiplexing Analyzer System, according to the manufacturer’s protocol.
Copy number variation analyses
Genomic DNA was isolated from peripheral blood using the QIAamp Blood Kit (Qiagen, Valencia, CA, USA). The DNA concentration was measured using the Nanodrop spectrophotometer (Thermo Fisher Scientific, Waltham, MA, United States).
CNV of the BDNF gene was investigated by real-time PCR assay using SYBR Green I chemistry and StepOne® Plus Real-Time PCR System. ALB gene, located in 4q11, was used as a reference gene of invariable copy number variation to calculate the relative BDNF gene copy number. Two sets of primers were designed using Primer3Plus software, and are available upon request. All reactions were carried out in triplicate and a melting curve analysis was done to certify the specificity of each primer product.
CNV of the LEPR, POMC, SIM1, LEP, MC4R, MC2R, and MC3R genes and the 16p11.2 region were determined by multiplex ligation-dependent probe amplification (SALSA MLPA Kit P220-B3 Obesity; MRC Holland, Amsterdam, Netherlands). Labeled MLPA products were detected by ABI Prism 3130xl Genetic Analyzer (Applied Biosystems) with GeneScan500 LIZ size standard (Life Technologies). Data were analyzed with GeneMarker® v.2.2.0 (Soft Genetics). The gene deletion or duplication was confirmed using quantitative real-time PCR (primers are available upon request). Then, chromosomal microarray analysis (CGH-array) was carried out to validate and identify the genomic breakpoints based on the human genome build GRCh38 (hg38).
American College of Medical Genetics and Genomics guidelines were used to classify the identified CNVs into 4 categories: pathogenic, likely pathogenic, variants of uncertain significance (VUS), and likely benign (16).
Functional enrichment analysis of deleted genes in the CNV
The enrichment analysis of the list of genes affected by the deleted region in three obese patients was submitted to ToppGene (17). To facilitate a more comprehensive visualization of the results, a bar plot was constructed using the ggplot2 package (18) to display top 20 biological processes associated with these genes. The Venn diagram was constructed using the ggVennDiagram package. Additionally, the Venn diagram was generated using the ggVennDiagram package (19) in R version 4.4.1 (20) to illustrate the intersections of deleted genes across the three patients.
The targets of deleted microRNAs were found using miRWalk (21). The genes were considered targets of miRNAs, based on energy < -20 and the duplicated gene symbol was removed for each analysis (22). The Venn diagram was also constructed using the target intersection of both miRNA (https://bioinformatics.psb.ugent.be/webtools/Venn/). The enrichment analysis from genes target of miRNAs was released using web approach Metascape which aggregates 40 different databases to investigate function enrichment (23).
Results
Basic and genomic characteristics of the study population
This study included 195 unrelated Brazilian patients with severe obesity and early-onset. The basic clinical characteristics of the cohort are presented in Table 1.
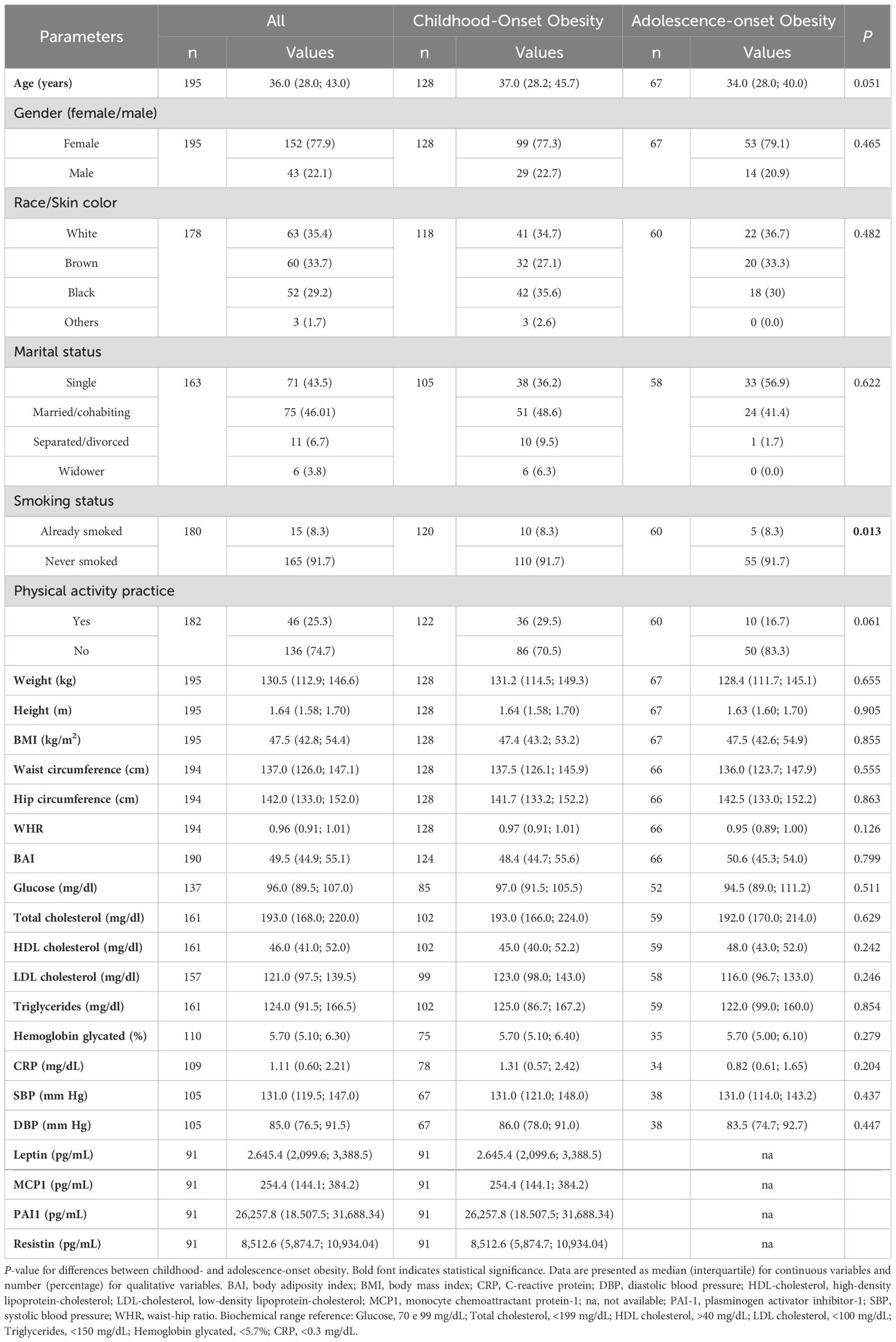
Table 1. Basic characteristics of the study population.
Copy number imbalances were found in three individuals (diagnostic yield of 1.5%). The genomic alterations were confirmed by real-time PCR and CGH-array. All three patients were found with pathogenic CNVs at the 16p11.2 locus, of which one was restricted to the distal region flanked by segmental duplications (SD) blocks breakpoint (BP)2 and BP3, and two to the proximal region flanked by SD blocks BP4 and BP5 (Supplementary Figure S1). All CNVs were in heterozygosity.
Clinical features of the patients with CNVs
Patient 1 had deletion for three probes from 16p11.2 in MLPA, showing a complete deletion of the SH2B1 gene. The deletion was shown to have a size of ~206 kb in the distal of the 16p11.2 region, encompassing twelve genes (ATXN2L, TUFM, MIR4721, SH2B1, ATP2A1, AS1, RABEP2, CD19, NFATC2IP, MIR4517, SPNS1 and LAT) (Figure 1). The patient was a 19-year-old male individual, which reported severe early-onset obesity (childhood). His body weight was 127.5 kg for 1.62 m of height with a BMI of 48.6 kg/m2. The waist circumference was 138 cm; hip circumference was 134 cm; WHR, 1.03; neck circumference, was 44 cm. We measured biochemical parameters, in which fasting plasma glucose was 112 mg/dl, total cholesterol, 281 mg/dl; HDL-c, 53 mg/dl; LDL-c, 175 mg/dl; TG, 263 mg/dl; glycated hemoglobin, 5,2%; and reactive C protein, 0.76 mg/l. The patient had hypertension and metabolic syndrome.
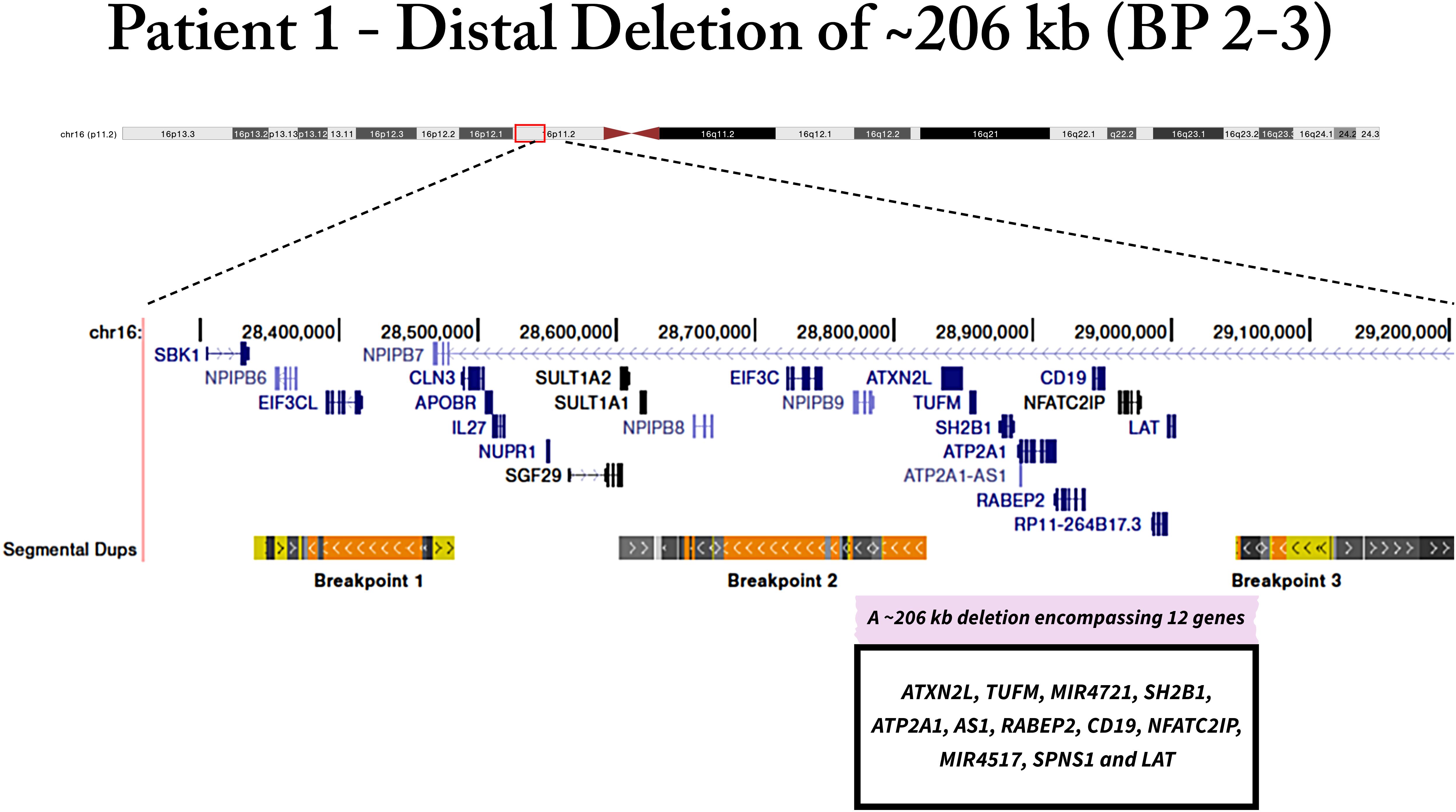
Figure 1. Genomic deletion of patient 1 in 16p11.2 region, which includes SH2B1 gene. The deletion encompasses twelve genes.
Patients 2 and 3 presented a deletion in the SEZ6L2 gene probe, localized in the 16p11.2 region. Further analyzes showed that patient 2 exhibited a ~534 kb deletion of proximal 16p11.2 locus, encompassing twenty-nine genes (SPN, QPRT, C16orf54, ZG16, KIF22, MAZ, PRRT2, PAGR1, MVP, CDIPT, CDIPTOSP, SEZ6L2, ASPHD1, KCTD13, TMEM219, TAOK2, HIRIP3, INO80E, DOC2A, C16orf92, TLCD3B, LOC112694756, ALDOA, PPP4C, TBX6, YPEL3, LOC101928595, GDPD3, MAPK3) (Figure 2). The deletion was detected in a 45-year-old female patient, who developed obesity during adolescence. Her body weight was 112.9 kg for 1.51 m with a BMI of 49.5 kg/m2. Her waist circumference was 144 cm; hip circumference was 147 cm; WHR, 0.98; neck circumference, was 47 cm. The blood pressure was 142/71 mmHg. Biochemical parameters were obtained, in which fasting plasma glucose was 86 mg/dl; total cholesterol, 235 mg/dl; HDL-c, 57 mg/dl; LDL- c, 151 mg/dl; TG, 134 mg/dl. The patient exhibited hypertension and bronchitis.
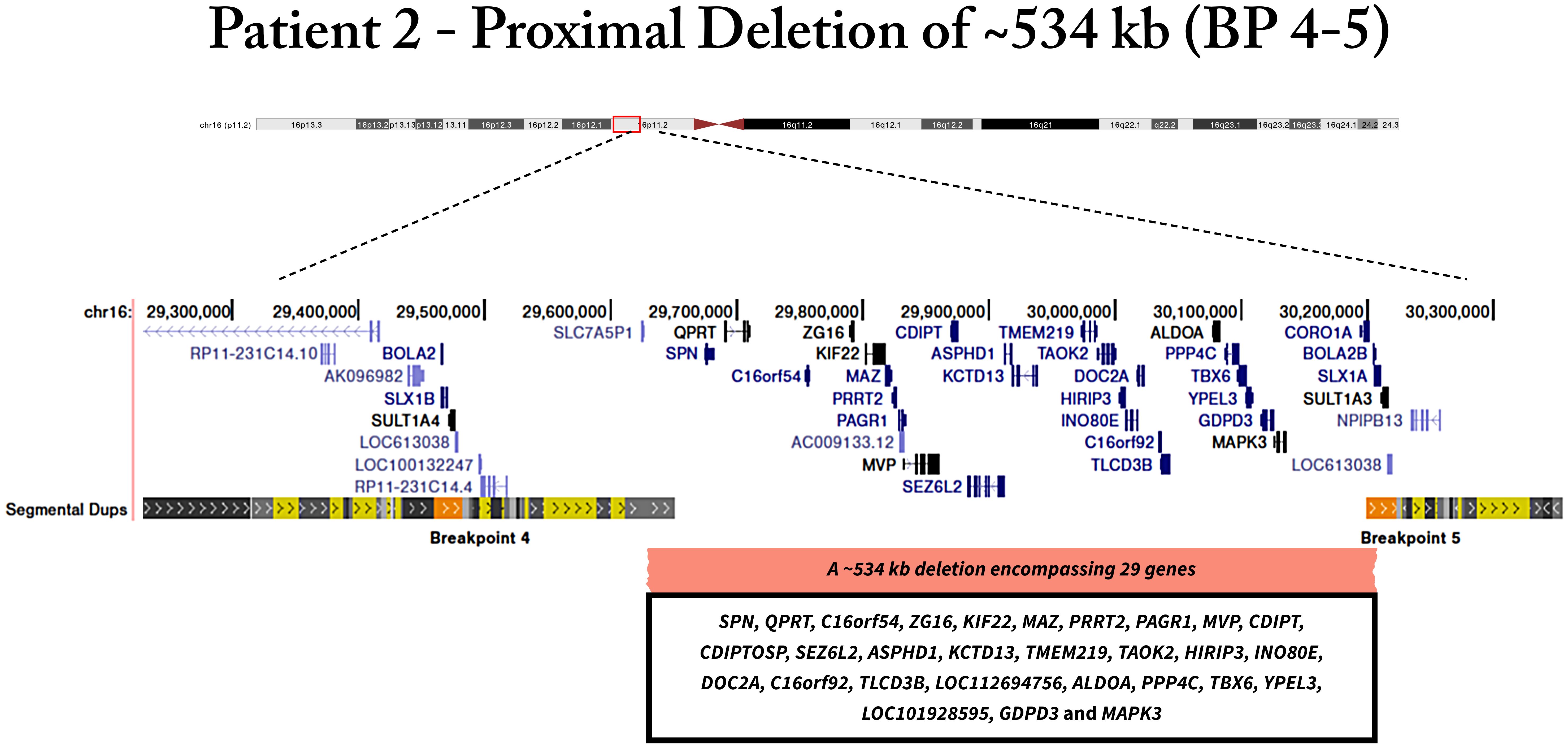
Figure 2. Genomic deletion of patient 2 located in proximal region of 16p11.2, encompassing twenty-nine genes.
Patient 3 presented a ~598 kb deletion of proximal 16p11.2 region that includes thirty-two genes (SMG1P2, MIR3680-2, MIR3680-1, SPN, QPRT, C16orf54, ZG16, KIF22, MAZ, PRRT2, PAGR1, MVP, CDIPT, CDIPTOSP, SEZ6L2, ASPHD1, KCTD13, TMEM219, TAOK2, HIRIP3, INO80E, DOC2A, C16orf92, TLCD3B, LOC112694756, ALDOA, PPP4C, TBX6, YPEL3, LOC101928595, GDPD3, MAPK3) (Figure 3). The patient 3 was a 31-year-old female with severe early-onset obesity (during childhood). Her body weight was 96.3kg in 1.55 m with a BMI of 40.1 kg/m2. The waist circumference was 115 cm; hip circumference was 130 cm; WHR was 0.88, and neck circumference, was 39.5 cm. Regarding biochemical parameters, fasting glucose was 62 mg/dl; total cholesterol, 206 mg/dl; HDL-c, 43 mg/dl; LDL- c, 143 mg/dl; TG, 100 mg/dl. We also measured the concentration of serum hormones and cytokines, leptin, 2,656.19 pg/m; MCP1, 133.07 pg/ml; PAI-1, 37,486.56 pg/ml; and resistin, 9,411.69 pg/ml. She presented metabolic syndrome and moderate binge-eating disorder (BED), consuming a median of 3,578.42 kcal per day.
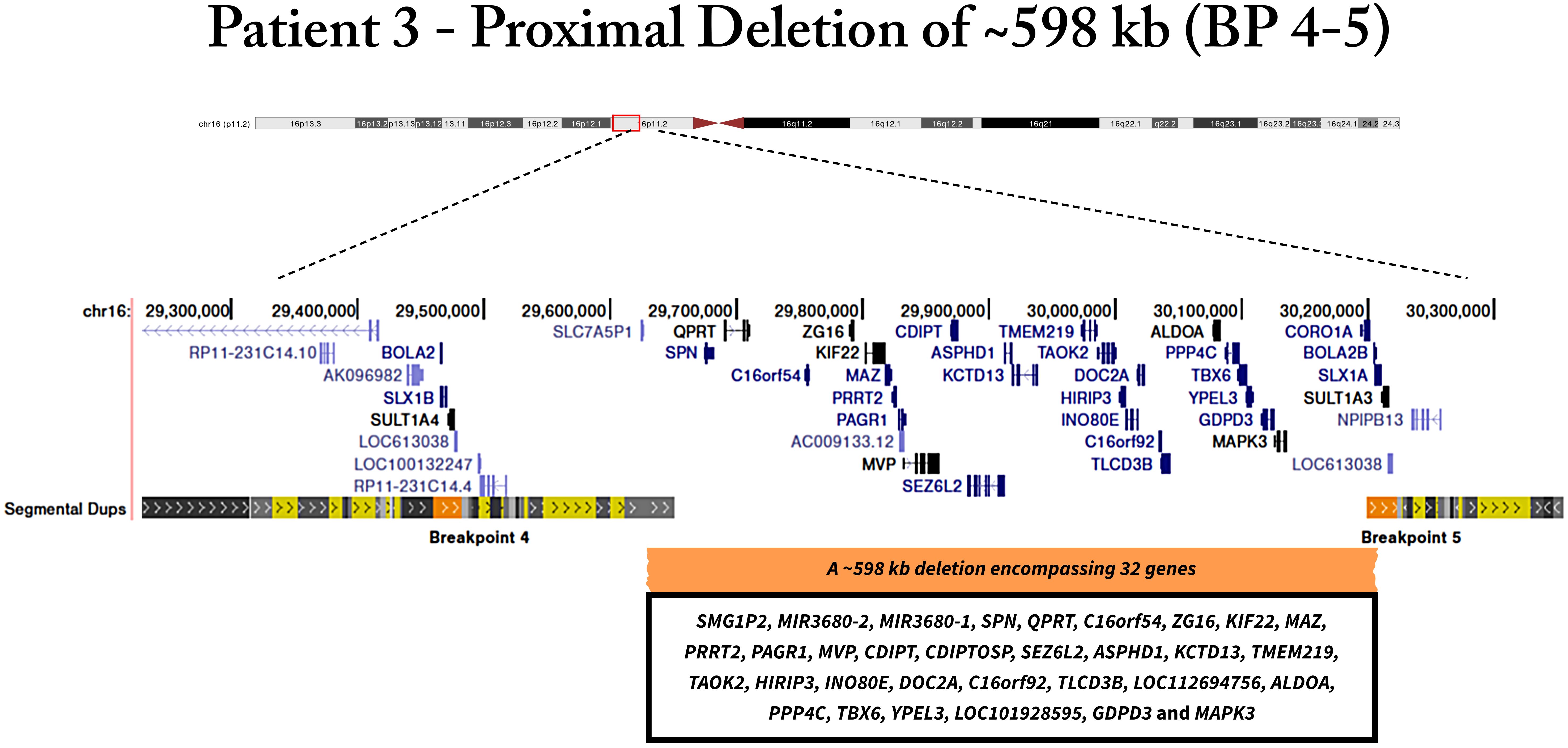
Figure 3. Genomic deletion of patient 3 located in 16p11.2 locus, encompassing thirty-two genes.
Functional enrichment analysis of deleted genes in the patients
Firstly, each patient’s signatures of common and specific genes deleted in the 16p11.2 region were analyzed (Supplementary Figure S2). Patient 1 has twelve specific deleted genes, which were presented in the other patients. Among these deleted genes, they act in different pathways related to the concentration and transport of micro and macromolecules; proliferation and differentiation of specific immune cells; and cytoskeleton regulation (Supplementary Figure S3).
Patients 2 and 3 had the same twenty-nine deleted genes; however, patient 3 had three more deleted genes. These common genes act in different biological processes, among them the main pathways are related to the development, differentiation, and communication of the central nervous system. For example, these genes are involved in the development of the brain and head; axonogenesis; and the development and differentiation central nervous system (Supplementary Figure S4).
The patient 3 has three specific genes deleted in the proximal 16p11.2 region. Two genes encode microRNA (miRNA) (MIR3680-1 and MIR3680-2) and one is a pseudogene (SMG1P2). The target genes of MIR3680-1 and MIR3680-2 were found using miRWalk. Our data showed that miRNA-3860-5p regulates 1330 genes, while miRNA-3860-5p modulates 2630 genes (Supplementary Tables S1, S2, respectively). The target genes of miRNA3860, 5p and 3p, were compared to identify common genes regulated by this miRNA, indicating that both modulate 354 genes (Supplementary Figure S5). These common genes are involved in different biological processes, including axonogenesis and the regulation of the development of neuron projection and the nervous system (Supplementary Figure S6).
Discussion
In the present study, we aimed to characterize the CNVs in genes related to NSMO by MLPA in patients with severe obesity and candidates for bariatric surgery in Brazil. In our cohort of 195 patients, 1.53% (3 individuals) had pathogenic deletions at the 16p11.2 region. In the short arm of chromosome 16, there are several flanking segmental duplications with a high degree of sequence identity, which could result in a recurrent rearrangement commonly caused by non-allelic homologous recombination events during meiosis. In this context, these genomic deletions are frequently not inherited from either parent but arise de novo (24).
The 16p11.2 distal deletion was found in one patient. This deletion has a size of ~206 kb, encompassing twelve genes. This locus includes the SH2B adaptor protein 1 (SH2B1) gene, linked to the development of obesity phenotype. Recently, Hanssen et al. (25) have investigated the clinical spectrum associated with 16p11.2 distal deletion in adults from the United Kingdom (UK) and Estonian biobanks. They reported that heterozygous carriers of this deletion have obesity with early onset, and accelerated metabolic disease, especially early and difficult-to-treat type 2 diabetes. This deletion was shown to account for 0.016% of the UK and 0.021% of Estonian biobanks (25).
We also found two patients with the proximal 16p11.2 deletion. This deletion represents the second most frequent genetic cause after MC4R point variants (26). Interestingly, a reciprocal duplication can influence BMI in a converse manner, resulting in underweight. It indicates that 16p11.2 CNVs have mirror etiologies, probably due to contrasting effects on energy homeostasis (27). In this line, an earlier study reported an abnormal satiety response in proximal 16p11.2 deletion carriers. However, the mechanism underlying this energy imbalance is still unknown (28). Controversially, murine models carrying paralogous 16p11.2 deletions and duplications showed an inverse phenotype found in humans, in which deletion and duplication mice resulted in under- and overweight, respectively (29, 30).
The functional enrichment analysis of deleted genes in our patients was performed to investigate the biological processes that are affected by the deletions. Interestingly, our data indicated that the deleted genes in the proximal 16p11.2 region are involved in brain development, as well as central nervous system development, differentiation, and communication. This result suggests that this deletion may impair the brain region’s development and/or function related to energy homeostasis, especially the hypothalamus development and/or the leptin-melanocortin pathway. It important to highlight that patient 2 and 3 have twenty-nine common genes deleted; however, patient 3 has more three specific genes deleted. Two of them are miRNAs that act mainly in axonogenesis and nervous system development. Previous studies showed that obesity is associated with miRNA deregulation (31). Further studies are necessary to elucidate the relation of miRNA deletion effects in the patients with NSMO.
A previous study observed that the proximal 16p11.2 deletion results in a highly penetrant form of obesity in adults; however, childhood presented a more variable phenotype. In addition, they also observed a low penetrance and variable phenotype in neurodevelopment disorders, including developmental delay and cognitive deficit. It is estimated that this deletion is found in 0.4% of patients with severe obesity – in line with our results (1%) (26).
Windholz et al. (32) investigated CNVs in classical obesity candidate genes in 194 children with severe early-onset obesity from Germany. By MLPA, they have analyzed POMC, LEP, LEPR, SIM1, MC4R, MC3R and MC2R genes. Similar to our results, they did not find CNVs in these candidate genes (32). In Brazil, D’Angelo et al. (4) performed a chromosomal microarray analysis on 279 patients with syndromic obesity. They identified a de novo recurrent 220-kb deletion of distal 16p11.2 in a 7-year female patient with overweight (BMI 20.5 kg/m2; 96.6th). This patient showed a deletion of 7 genes, including SH2B1. In addition, they found the recurrent 600-kb 16p11.2 proximal deletion in a 12-year male patient with obesity (BMI 30.4 kg/m2; 98.8th). Interestingly, a duplication of this same genomic rearrangement was observed in an 8-year-old female, which was reported to present obesity. This CNV was paternally inherited (4).
It is important to note that in this previous study, all the patients presented syndromic obesity, while our study included only individuals with non-syndromic obesity. It suggested that these rare forms of obesity may be associated with syndromic phenotypes or not. Thus, there is significant phenotypic variability among carriers of 16p11.2 deletions, and the etiology remains unclear. One possible explanation is other rare and common genetic variants contributing to clinical and neurobehavioral phenotypes. In addition, penetrance is age-dependent and each individual should be considered for your specific features (12).
Conclusion
Understanding the rare genetic forms of obesity etiology has proven difficult. Unfortunately, the majority of patients with NSMO are underdiagnosed, and the genetic diagnosis is crucial to adequate clinical management, family genetic counseling, or even in some cases, targeted therapeutic intervention (33). Here, we diagnosed three patients with NSMO caused by deletions in the 16p11.2 locus at both proximal and distal intervals. From a perspective, these results allow us to implement a quick and efficient diagnostic method for patients with these rare genetic forms in the future.
Data availability statement
The original contributions presented in the study are included in the Supplementary Datasheet 1. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by the Ethics Committee of the Oswaldo Cruz Foundation (CAAE:09225113.0.0000/ Protocol Nº: 346.634). The studies were conducted in accordance with the local legislation and institutional requirements. The patients/participants provided written informed consent prior to enrollment (resolution nº466/2012 of Ministry of Health, Brazil
Author contributions
Id: Writing – original draft, Methodology, Formal analysis. KS: Writing – original draft, Methodology, Formal analysis. RF: Formal analysis, Investigation, Methodology, Validation, Writing – review & editing. LP: Writing – review & editing, Methodology. Gd: Writing – review & editing, Validation, Methodology. TS: Writing – review & editing, Validation. FM: Writing – review & editing, Methodology, Data curation. ER: Writing – review & editing, Resources, Funding acquisition. VZ: Writing – review & editing, Visualization, Data curation. MC: Writing – review & editing, Conceptualization. CM: Writing – review & editing, Visualization, Resources. PC: Writing – review & editing, Visualization, Funding acquisition. JC: Writing – review & editing, Visualization, Resources, Funding acquisition. PB: Writing – review & editing, Supervision, Conceptualization. Ad: Writing – review & editing, Writing – original draft, Supervision, Conceptualization.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the Oswaldo Cruz Foundation (Fiocruz, Brazil) and Carlos Chagas Filho Foundation for Research Support in the State of Rio de Janeiro (FAPERJ) (GRANT: E-26/210.663/2021 and E-26/202.291/2019).
Acknowledgments
The authors would like to thank the Edson Fernandes and Nereida Proença da Fonseca for their great technical assistance and the “Programa de Desenvolvimento Tecnologico em Insumos para Saude” (PDTIS) platform for multiplex analysis. We are grateful to patients who kindly agreed to participate in this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2024.1495534/full#supplementary-material
References
1. World Health Organization. Obesity and overweight. (2024). Available online at: https://www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweight (accessed June 30, 2024).
2. Loos RJF, Yeo GSH. The genetics of obesity: from discovery to biology. Nat Rev Genet. (2022) 23:120–33. doi: 10.1038/s41576-021-00414-z
3. Dosda S, Renard E, Meyre D. Sequencing methods, functional characterization, prevalence, and penetrance of rare coding mutations in panels of monogenic obesity genes from the leptin-melanocortin pathway: A systematic review.Obes Rev., vol. 95. (2024). 25(8):e13754. doi: 10.1111/obr.13754
4. D’Angelo CS, Varela MC, de Castro CIE, Otto PA, Perez ABA, Lourenço CM, et al. Chromosomal microarray analysis in the genetic evaluation of 279 patients with syndromic obesity. Mol Cytogenetics. (2018) 11:1–18. doi: 10.1186/s13039-018-0363-7
5. Styne DM, Arslanian SA, Connor EL, Farooqi IS, Murad MH, Silverstein JH, et al. Pediatric obesity—Assessment, treatment, and prevention: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. (2017) 102:709–57. doi: 10.1210/jc.2016-2573
6. da Fonseca ACP, Mastronardi C, Johar A, Arcos-Burgos M, Paz-Filho G. Genetics of non-syndromic childhood obesity and the use of high-throughput DNA sequencing technologies. J Diabetes Its Complications. (2017) 31(10):1549–1561. doi: 10.1016/j.jdiacomp.2017.04.026
7. da Fonseca ACP, Abreu GM, Zembrzuski VM, Junior MC, Carneiro JRI, Neto JFN, et al. Study of LEP, MRAP2 and POMC genes as potential causes of severe obesity in Brazilian patients. Eating Weight Disorders-Studies Anorexia Bulimia Obes. (2021) 26:1399–408. doi: 10.1007/s40519-020-00946-z
8. da Fonseca ACP, de Medeiros Abreu G, Palhinha L, Zembrzuski VM, Junior MC, Carneiro JRI, et al. A rare potential pathogenic variant in the BDNF gene is found in a Brazilian patient with severe childhood-onset obesity. Diabetes Metab Syndrome Obesity: Targets Ther. (2021) 14:11. doi: 10.2147/DMSO.S267202
9. da Fonseca ACP, De Medeiros Abreu G, Zembrzuski VM, Campos Junior M, Carneiro JRI, Magno FCCM, et al. Identification of the MC4R start lost mutation in a morbidly obese Brazilian patient. Diabetes Metab Syndrome Obesity: Targets Ther. (2019) 12:257–266. doi: 10.2147/DMSO.S189455
10. da Fonseca ACP, Assis ISS, Salum KCR, Palhinha L, Abreu GM, Zembrzuski VM, et al. SH2B1 variants as potential causes of non-syndromic monogenic obesity in a Brazilian cohort. Eating Weight Disorders-Studies Anorexia Bulimia Obes. (2022) 27:3665–74. doi: 10.1007/s40519-022-01506-3
11. Salum KCR, de Souza GO, Abreu G, de M, Campos Junior M, Kohlrausch FB, et al. Identification of a rare and potential pathogenic MC4R variant in a Brazilian patient with adulthood-onset severe obesity. Front Genet. (2020) 11:1589. doi: 10.3389/fgene.2020.608840
12. Chung WK, Roberts TPL, Sherr EH, Snyder LG, Spiro JE. 16p11. 2 deletion syndrome. Curr Opin Genet Dev. (2021) 68:49–56. doi: 10.1016/j.gde.2021.01.011
13. Faivre L, Cormier-Daire V, Lapierre JM, Colleaux L, Jacquemont S, Genevieve D, et al. Deletion of the SIM1 gene (6q16. 2) in a patient with a Prader-Willi-like phenotype. J Med Genet. (2002) 39:594–6. doi: 10.1136/jmg.39.8.594
14. Han JC, Liu Q-R, Jones M, Levinn RL, Menzie CM, Jefferson-George KS, et al. Brain-derived neurotrophic factor and obesity in the WAGR syndrome. New Engl J Med. (2008) 359:918–27. doi: 10.1056/NEJMoa0801119
15. da Fonseca ACP, Bozza PT, Cabello PH. Genetic profiles in the obese population. Obes Diabetes. (2020), 107–25.
16. Kearney HM, Thorland EC, Brown KK, Quintero-Rivera F, South ST. American College of Medical Genetics standards and guidelines for interpretation and reporting of postnatal constitutional copy number variants. Genet Med. (2011) 13:680–5. doi: 10.1097/GIM.0b013e3182217a3a
17. Chen J, Bardes EE, Aronow BJ, Jegga AG. ToppGene Suite for gene list enrichment analysis and candidate gene prioritization. Nucleic Acids Res. (2009) 37:305–11. doi: 10.1093/nar/gkp427
18. Wickham H. ggplot2 - elegant graphics for data analysis | Hadley wickham. In: Springer Science & Business Media. Springer (2017). Available at: https://ggplot2-book.org/.
19. Gao CH, Yu G, Cai P. ggVennDiagram: an intuitive, easy-to-use, and highly customizable R package to generate venn diagram. Front Genet. (2021) 12:706907/BIBTEX. doi: 10.3389/FGENE.2021.706907/BIBTEX
20. R Core Team. R: A Language and Environment for Statistical Computing (Vienna, Austria: R Foundation for Statistical Computing). (2021). Available online at: https://www.r-project.org/ (accessed November 20, 2024).
21. Sticht C, de la Torre C, Parveen A, Gretz N. miRWalk: an online resource for prediction of microRNA binding sites. PloS One. (2018) 13:e0206239. doi: 10.1371/journal.pone.0206239
22. Lewis BP, Burge CB, Bartel DP. Conserved seed pairing, often flanked by adenosines, indicates that thousands of human genes are microRNA targets. Cell. (2005) 120:15–20. doi: 10.1016/j.cell.2004.12.035
23. Zhou Y, Zhou B, Pache L, Chang M, Khodabakhshi AH, Tanaseichuk O, et al. Metascape provides a biologist-oriented resource for the analysis of systems-level datasets. Nat Commun. (2019) 10:1523. doi: 10.1038/s41467-019-09234-6
24. Shinawi M, Liu P, Kang S-HL, Shen J, Belmont JW, Scott DA, et al. Recurrent reciprocal 16p11. 2 rearrangements associated with global developmental delay, behavioural problems, dysmorphism, epilepsy, and abnormal head size. J Med Genet. (2010) 47:332–41. doi: 10.1136/jmg.2009.073015
25. Hanssen R, Auwerx C, Jõeloo M, Sadler MC, Henning E, Keogh J, et al. Chromosomal deletions on 16p11. 2 encompassing SH2B1 are associated with accelerated metabolic disease. Cell Rep Med. (2023) 4:101155. doi: 10.1016/j.xcrm.2023.101155
26. Walters RG, Jacquemont S, Valsesia A, De Smith AJ, Martinet D, Andersson J, et al. A new highly penetrant form of obesity due to deletions on chromosome 16p11.2. Nature. (2010) 463(7281):671–675. doi: 10.1038/nature08727
27. Jacquemont S, Reymond A, Zufferey F, Harewood L, Walters RG, Kutalik Z, et al. Mirror extreme BMI phenotypes associated with gene dosage at the chromosome 16p11.2 locus. Nature. (2011) 478(7367):97–102. doi: 10.1038/nature10406
28. Maillard AM, Hippolyte L, Rodriguez-Herreros B, Chawner SJRA, Dremmel D, Agüera Z, et al. 16p11.2 Locus modulates response to satiety before the onset of obesity. Int J Obes. (2016) 40(5):870–876. doi: 10.1038/ijo.2015.247
29. Horev G, Ellegood J, Lerch JP, Son YEE, Muthuswamy L, Vogel H, et al. Dosage-dependent phenotypes in models of 16p11.2 lesions found in autism. Proc Natl Acad Sci United States America. (2011) 108(41):17076–17081. doi: 10.1073/pnas.1114042108
30. Portmann T, Yang M, Mao R, Panagiotakos G, Ellegood J, Dolen G, et al. Behavioral abnormalities and circuit defects in the basal ganglia of a mouse model of 16p11.2 deletion syndrome. Cell Rep. (2014) 7(4):1077–1092. doi: 10.1016/j.celrep.2014.03.036
31. Mondal S, Rathor R, Singh SN, Suryakumar G. miRNA and leptin signaling in metabolic diseases and at extreme environments. Pharmacol Res Perspect. (2024) 12:e1248. doi: 10.1002/prp2.v12.4
32. Windholz J, Kovacs P, Schlicke M, Franke C, Mahajan A, Morris AP, et al. Copy number variations in “classical” obesity candidate genes are not frequently associated with severe early-onset obesity in children. J Pediatr Endocrinol Metab. (2017) 30(5):507–515. doi: 10.1515/jpem-2016-0435
33. Giannopoulou EZ, Zorn S, Schirmer M, Herrmann G, Heger S, Reinehr T, et al. Genetic obesity in children: overview of possible diagnoses with a focus on SH2B1 deletion. In: Hormone Research in Paediatrics, vol. 95. (2022). Available at: https://doi.org/10.1159/000520402 (accessed August 13, 2024).
Keywords: genetic obesity, copy number variations, SH2B1, bariatric surgery, MLPA, CGH-array, severe obesity
Citation: da Silva Assis IS, Salum KCR, Felício RdFM, Palhinha L, de Medeiros Abreu G, Silva T, Mattos FCC, Rosado EL, Zembrzuski VM, Campos Junior M, Maya-Monteiro CM, Cabello PH, Carneiro JRI, Bozza PT and da Fonseca ACP (2025) Genomic deletions on 16p11.2 associated with severe obesity in Brazil. Front. Endocrinol. 15:1495534. doi: 10.3389/fendo.2024.1495534
Received: 12 September 2024; Accepted: 25 November 2024;
Published: 17 January 2025.
Edited by:
Patricia De Gortari, National Institute of Psychiatry Ramon de la Fuente Muñiz (INPRFM), MexicoReviewed by:
Cecilia Contreras-Cubas, National Institute of Genomic Medicine (INMEGEN), MexicoViridiana Alcantara-Alonso, Imperial College London, United Kingdom
Copyright © 2025 da Silva Assis, Salum, Felício, Palhinha, de Medeiros Abreu, Silva, Mattos, Rosado, Zembrzuski, Campos Junior, Maya-Monteiro, Cabello, Carneiro, Bozza and da Fonseca. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ana Carolina Proença da Fonseca, YW5hX2Nhcm9sX3BmMkBob3RtYWlsLmNvbQ==; YW5hLnByb2VuY2FAaW9jLmZpb2NydXouYnI=
†These authors share first authorship
‡These authors share last authorship