 B. Vanessa Díaz-González1,2†
B. Vanessa Díaz-González1,2† Álvaro Ramos-Luzardo3†
Álvaro Ramos-Luzardo3† Luis Alberto Henríquez-Hernández2,4,5*Lluis Serra-Majem2,5,6Inmaculada Bautista-Castaño1,5Andrea Acosta-Dacal2,4Octavio P. Luzardo2,4,5Elisabeth Hernández-García2Judith Cornejo-Torre2Juan Ramón Hernández-Hernández2,6Pilar Fernández-Valerón3
Luis Alberto Henríquez-Hernández2,4,5*Lluis Serra-Majem2,5,6Inmaculada Bautista-Castaño1,5Andrea Acosta-Dacal2,4Octavio P. Luzardo2,4,5Elisabeth Hernández-García2Judith Cornejo-Torre2Juan Ramón Hernández-Hernández2,6Pilar Fernández-Valerón3- 1Triana Primary Health Care Center, Servicio Canario de la Salud, Las Palmas de Gran Canaria, Spain
- 2Research Institute of Biomedical and Health Sciences (IUIBS), Universidad de Las Palmas de Gran Canaria, Las Palmas de Gran Canaria, Spain
- 3Department of Biochemistry and Molecular Biology, Physiology, Genetics, and Immunology, Universidad de Las Palmas de Gran Canaria, Las Palmas de Gran Canaria, Spain
- 4Toxicology Unit, Clinical Sciences Department, Universidad de Las Palmas de Gran Canaria, Las Palmas de Gran Canaria, Spain
- 5Centro de Investigación Biomédica en Red Fisiopatología de la Obesidad y la Nutrición (CIBEROBN), Instituto de Salud Carlos III, Madrid, Spain
- 6Centro Hospitalario Universitario Insular Materno Infantil (CHUIMI), Servicio Canario de la Salud, Las Palmas de Gran Canaria, Spain
Introduction: Obesity is a pathological state that involves the dysregulation of different metabolic pathways and adipose tissue cells, constituting a risk factor for the development of other diseases. Bariatric surgery is the most effective treatment. The study of the behavior of pollutants in situations of extreme weight loss can provide biomonitoring information and tools to manage diseases of environmental etiology.
Aim: To determine the prevalence of serum persistent and non-persistent pollutants in obese patients subjected to bariatric surgery and analyze the impact of sociodemographic variables on these changes.
Methods: GC-MS/MS and UHPLC-MS/MS were utilized to determine the detection rates and concentrations of 353 compounds, including persistent organic pollutants (POPs), pesticides, pharmaceuticals, and rodenticide, in serum samples of 59 obese patients before and after undergoing bariatric surgery.
Results: Detection rates of p,p’-DDE, HCB, β-HCH, naphthalene, phenanthrene and PCB congeners 138, 153 and 180 significantly increased due to surgery-induced weight loss. Serum levels of p,p’-DDE, PCB-138, PCB-153 and PCB-180 also increased after surgery. Correlations between naphthalene levels, weight loss, variation of total lipids and time after surgery were found. Additionally, correlations were observed between concentrations of PCB-138 and weight loss, and between phenanthrene levels and reduction of total lipids. No statistically significant differences were observed for other groups of contaminants, pharmaceuticals and other chemicals included in the quantification methods.
Conclusions: Increment of POPs was observed after bariatric surgery. Serum concentrations of POPs after surgery were influenced by adiposity-related variables. Although biomonitoring studies show a decreasing tendency of exposure, rapid weight loss leads to an increase of circulating POPs. Further research on the interplay between adipose tissue, POPs and peripheral organs is required.
1 Introduction
During the last three decades, the prevalence of obesity has doubled worldwide (1, 2). Due to this fact, it is now considered the pandemic of the modern era, which carries a huge socioeconomic impact (1, 3). According to the European Regional Report on Obesity, published by the WHO in May 2022, 60% of the European adult population are affected either by overweight or obesity (4). This chronic physical condition is characterized by an increased body mass index (BMI, expressed as kg/m2) that allows for its classification in different somatotypes, namely overweight (25 ≤ BMI <30), class I obesity (30 ≤BMI <35), class II (35 ≤ BMI <40) and class III or severe obesity (BMI ≥ 40) (5). It is a multifactorial disease that originates as a result of the combination of intrinsic, physiological and behavioral causes together with extrinsic, lifestyle, dietary and exposure factors (3). Although this disease was primarily related to excessive fat accumulation in the adipose tissue, growing evidence points to whole-body low-grade chronic inflammation, dysregulation of the gut microbiota, alterations of the cell cycle in adipocytes and elevated levels of reactive oxygen species as important hallmarks of obesity (6, 7). Thus, rather than an imbalance of calories in and out, the underlying causes of obesity might involve the destabilization of energy homeostasis mechanisms themselves (3). Beyond the physical limitations that increased body mass involves, obesity has been associated with a set of comorbidities and complications, such as dyslipidemia, depression, cancer, type II diabetes, cardiovascular diseases and susceptibility to severe infections, i.e. SARS-CoV-2 (8–11).
Substantial progress has been made in the treatment of obesity over the last decades. This includes lifestyle interventions by restructuring eating and physical activity habits; pharmacological therapies targeting either digestive lipases or the central nervous system (CNS); administration of oral hydrogel capsules that induce the feeling of satiety; slightly invasive endoscopic bariatric therapies, such as intragastric balloons and endoscopic gastroplasty; and bariatric surgery, which shows the strongest evidence of sustained weight loss (12, 13). In spite of the promising results of pharmacotherapeutic strategies in clinical trials, bariatric surgery is still the most effective approach to achieve long-term body fat reduction, reducing the incidence of type 2 diabetes mellitus and obesity-associated cancer (12, 14). In general terms, bariatric surgery is indicated when there has been a poor response to other treatments, in patients with class 2 obesity with complications, or patients with class 3 obesity.
Recent advances in the research of obesity and the adipose tissue has reassessed it from being merely an storage tissue to a complex, metabolically active organ with different endocrine functions (15). Hence, the adipose tissue plays an important toxicological role with regard to xenobiotic lipophilic molecules. Firstly, it exerts a protective effect by sequestering hydrophobic chemicals from the bloodstream. Secondly, the adipose tissue is considered an internal source of low-concentration chronic exposure to stored xenochemicals, which may be released during lipolysis. Thirdly, adipocytes exhibit several receptors that can be either activated or inhibited by the interaction with these compounds, thereby constituting a key target for their activity (16) and reinforcing the obesogen theory (17). Interestingly, the association between adiposity and the presence of persistent organic pollutants (POPs) have been reported in previous studies, in which plasma levels of these contaminants were not only related to BMI and gender, but also appeared to increase in response to rapid weight loss (18), suggesting a transference between the adipose tissue and the circulatory system.
POPs are toxic organic molecules with some physicochemical properties that make them especially resistant to degradation and very susceptible to bioaccumulation and biomagnification (19). Therefore, their release into circulation could lead to undesired consequences. Even though most POPs are listed in the Stockholm Convention (20) and they are banned or under strict regulation in many countries, they are currently detected in the individuals due to their ubiquitous nature, their persistence in the environment and, in some cases, their transgenerational inheritance (19, 21). According to data, exposure to POPs is a contributing factor to different pathological conditions including obstetric defects, cardiovascular disease, metabolic syndrome, neurological and immunological disorders and cancer (8, 22–28). In the Spanish population, the levels of some POPs have decreased since their prohibition in the late 20th century (29–31). However, exposure to these chemicals in the Canary Islands –a Spanish archipelago located near the west African coast– was proven to be higher than in the continental Europe (26). Despite the wide knowledge about the prevalence of these contaminants in this North Atlantic region, little is known about the situation in the obese non-elderly inhabitants. Moreover, the role of the bariatric surgery-induced weight loss in relation to these substances is unexplored.
This study aims to determine the serum levels of 353 compounds, including POPs, pesticides, pharmaceuticals, and rodenticides, in a cohort of obese patients from Gran Canaria Island (Spain), and stablish a comparison within samples from the same patients, collected one year after undergoing bariatric surgery. Additionally, the association between the resulting concentrations and sociodemographic factors were analyzed.
2 Materials and methods
2.1 Study population and sample collection
A total of 59 adult patients were included in this study, composed of 43 women and 16 men aged from 20 to 69 years old whose BMI ranged from 35 to 60 kg/m2. The patients underwent a bariatric surgery, preceded by a clinical evaluation, from March, 30th to July, 7th, 2015, after which they followed a strict dietary control for one year and submitted to a second evaluation from March, 15th to December, 23rd, 2016. Weight, height, and body composition were recorded using the Tanita BC-420MA III (Girod Medical, Madrid, Spain) before the intervention and during the follow-up visits. At the time of the initial visit and the final assessment, whole blood was collected in 4 mL tubes with EDTA and centrifuged at 3000g for 5 min. The serum was separated within a maximum of 2 h after collection. The obtained serum was kept at −20 °C until chemical analysis. We reported weight loss outcomes as total body weight loss (TBWL, expressed in kilograms), percentage of total body weight loss (%TBWL) and percentage of excess body weight loss (%EWL). Clinically relevant parameters, such as lipidemia, smoking habit, presence of comorbidities and depressive state, were measured both before and after the follow-up (Table 1).
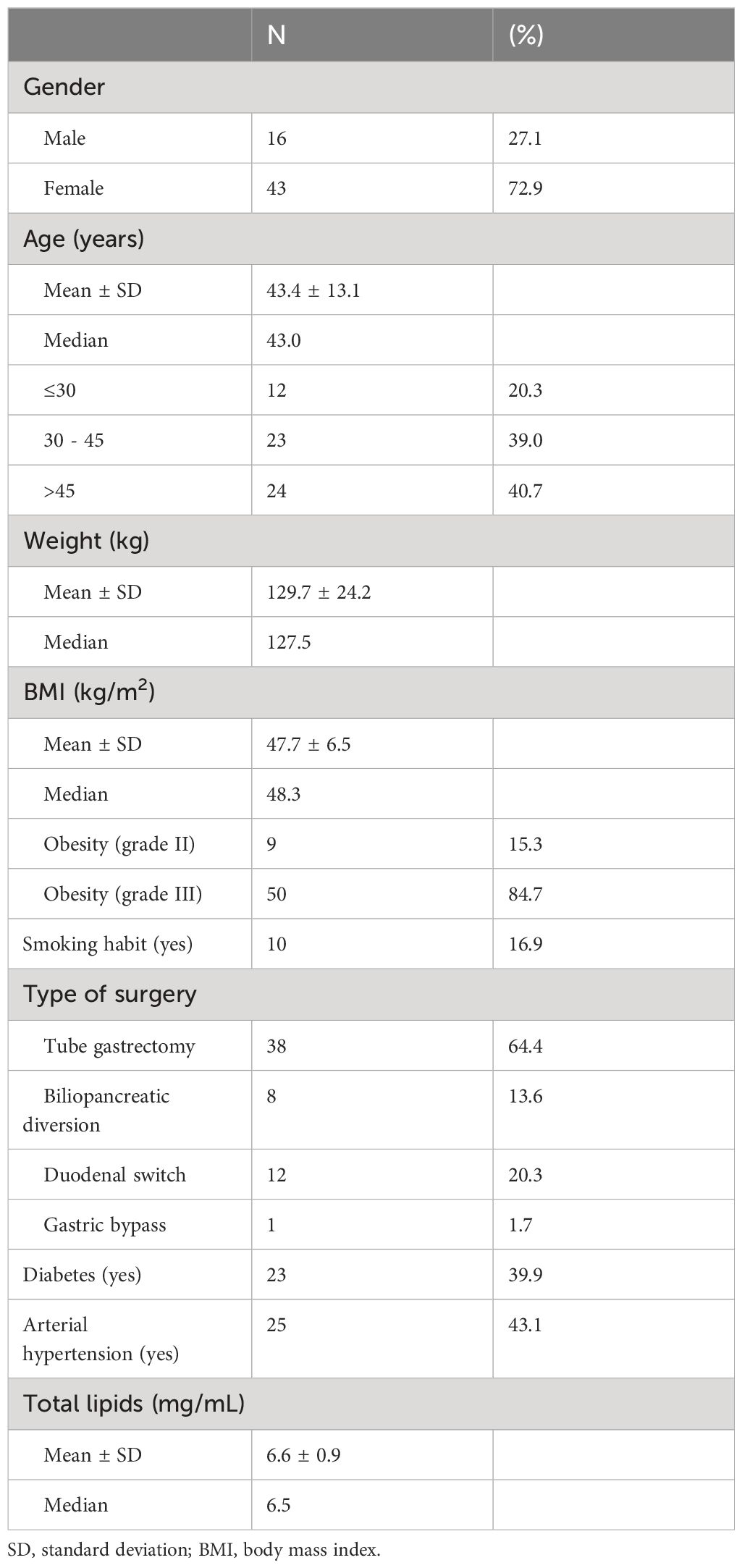
Table 1 Characteristics of patients before surgery (n = 59).
The study was approved by the Clinical Research Ethics Committee of the CHUIMI (Complejo Hospitalario Universitario Insular Materno Infantil): ethical approval code 2024-093-728, on June 26th, 2014.
2.2 Sample preparation
Samples underwent a QuEChERS-based protocol for the extraction of analytes of interest (32), which have been modified and validated for the analysis of analytes in serum (33). Briefly, 250 μL of serum samples were introduced in 2 mL Eppendorf tubes and 10 μL of a mixture of procedural internal standards (P-ISs) were then added to reach a final concentration of 4 ng/μL of acenaphthene-d10, chlorpyrifos-d10, chrysene-d12, diazinon-d10, PCB-200, and phenanthrene-d10 for Gas Chromatography (GC); and atrazine-d5, carbendazim-d3, cyromazine-d4, diazinon-d10, linuron-d3 and pirimicarb-d6 for Liquid Chromatography (LC). After a 10-minute incubation at room temperature, 500 μL of acidified acetonitrile (1% formic acid (FA)) were added and properly mixed by vortexing. The serum-acetonitrile mixture underwent an ultrasonic bath (Selecta, Barcelona, Spain) for 20 minutes at room temperature, after which 150 mg of anhydrous magnesium sulfate and 37.5 mg of sodium acetate were added. Samples were vortexed and vigorously shaken for one minute and centrifuged at 4200 rpm and 4°C for 10 minutes in a centrifuge 5804/R with a rotor FA-45-48-11 (Eppendorf, Hamburg, Germany). The resulting supernatant was collected with a 1-mL syringe and introduced in an inserted chromatography amber vial using a polyester, HPLC-certified, 0.2μm Chromafil PET-20/15 MS syringe filter (Macherey-Nagel, Düren, Germany).
Applying this method, clean-up, evaporation and solvent change steps are avoided and 353 analytes can be detected and quantified through gas chromatography coupled to triple quadrupole mass spectrometry (GC-MS/MS) and liquid chromatography coupled to triple quadrupole mass spectrometry (LC-MS/MS) in a complementary manner (33, 34).
2.3 Instrumental analysis
2.3.1 CG-MS/MS
A total of 129 out of 353 compounds were analyzed by GC-MS/MS. To that end, an Agilent 7890B gas chromatographer was used, along with an Agilent 7693 automatic sampler and a tandem-coupled Agilent 7010 mass spectrometer (Agilent Technologies, Santa Clara, California, USA). The injection volume was 1.5μL and two fused (5%-phenyl)-methylpolysiloxane silica ultra-inert capillary columns (Agilent J&W HP-5MS, Agilent Technologies) were used for chromatographic separation. Both columns were 15 m long, had an internal diameter of 0.25 mm and a film thickness of 0.25 μm. The selected carrier gas was helium (99.9999% purity), which was pumped in constant flow. Nitrogen (99.9999% purity, Linde, Dublin, Ireland) was used as a collision gas. With regards to the oven temperature, the program was as follows: 1.8 min at 80°C; increase of 40°C/min until reaching 170°C; increase of 10°C/min until 310°C; and hold at 310°C for 3 min. The multiple reaction monitoring (MRM) mode was used in runs of 21.05 min, divided in 24-time segments.
2.3.2 LC-MS/MS
A total of 224 out of 353 analytes were quantified using an Agilent 1290 ultrahigh-performance liquid chromatographer (UHPLC), coupled in tandem with an Agilent 6460 mass spectrometer (Agilent Technologies, Palo Alto, USA). An InfinityLab Poroshell 120 (100mm of length, 2.1 mm of thickness and a particle diameter of 2.7 μm) was the column of choice for chromatographic separation. The mobile phases A and B were composed of ultrapure water (2 mM ammonium acetate; 0.1% FA) and MeOH (2 mM ammonium acetate), respectively. A volume of 8 μL was injected at a flow rate of 0.4 mL/min, with an oven temperature of 50°C. Each run lasted for 18 min. The dynamic MRM (dMRM) mode was selected to operate the mass spectrometer. A nitrogen generator NGMs-1 (Atlas Copco, Stockholm, Sweden) was used to produce nitrogen as a drying and desolvation gas. As a collision gas, Nitrogen 6.0 (99.9999% purity, Linde, Dublin, Ireland) was used.
The optimal operating conditions of the mass spectrometer analyses for both GC-MS/MS and LC-MS/MS have been described in previous work and can be found in Supplementary Table S1 in the Supplementary Material (33).
2.4 Quality of analysis and quality control
The limits of quantification (LOQs) for the analysis of these analytes have been previously established (33). Briefly, LOQs were determined by performing recovery assays, being the lowest concentrations, whose accuracy ranged from 70% to 120% and the standard deviation was lower than 20% and can be referenced in Supplementary Table S1. These criteria were stablished in the SANTE/12682/2019 guidance definition (35). Every 25 vials, an internal QC sample was included, which was obtained by spiking fetal bovine serum (FBS; Lonza, Basel, Switzerland) at 5 ng/mL with all analytes and subsequently processing as the rest of serum samples. QCs were accepted when the percentages of recovery ranged between 70% and 120% and the standard deviation was lower than 20%, according to the SANTE 12682/2019 recommendations (35).
2.5 Statistical analysis
PASW Statistics v19.0 (SPSS Inc., Chicago, Illinois, USA) was used to perform statistical analyses. Chi-squared tests, Wilcoxon test and Mann-Whitney U tests were conducted for comparisons before and after surgery of sociodemographic variables, for detection rates, and concentrations, respectively. The Kolmogorov–Smirnov test for normality was used to check the distributions of sociodemographic variables and POPs. A Student’s t test was used to analyze the variation of total lipids. Bivariate correlation Kendall’s τ test was performed to study the influence of sociodemographic characteristics on the differences in serum levels of POPs. The results were reported as medians and interquartile ranges. Concentration values below the LOD were not included in the statistical analysis. Those values between the LOD and the LOQ were only taken into account to determine the detection rates. To study concentration changes before and after surgery, half of the LOQ was taken if the compound had not been quantified at that time point.
Serum total cholesterol and triglyceride concentrations were determined enzymatically and used for the lipid adjustment of results (36, 37). POP concentrations were individually corrected for total lipids (TL) by dividing the raw POP concentration by TL and are expressed in nanograms of analyte per gram of lipid weight (ng/g lw).
The level of statistical significance was set at 0.05 and all tests were two tailed.
3 Results
Before surgery, mean weight was 129.7 kg which translates into a mean BMI of 47.7 kg/m2. After surgery (mean follow-up of 534 ± 24.1), Mann-Whitney U tests revealed that these parameters were significantly reduced and reached 83.6 kg (ρ < 0.001) and 31.0 kg/m2 (ρ < 0.001), respectively (Table 2). Thus, a mean weight loss of 45.28 kg was observed. According to the BMI, all patients had at least class II obesity and 84.7% had class III obesity at the beginning of the study. Bariatric surgery resulted in an important decrease in the frequency of class III obesity and 21.4% of the patients achieved normal weight (Table 2). Remarkably, only one patient failed to lose weight during this period, showing an increase of 0.6 kg. Since body weight was affected by the intervention, Mann-Whitney U tests also showed a significant reduction in total lipids in blood from 6.6 mg/mL to 5.9 mg/mL (ρ < 0.001), which involves a mean reduction of 0.668 mg/mL.
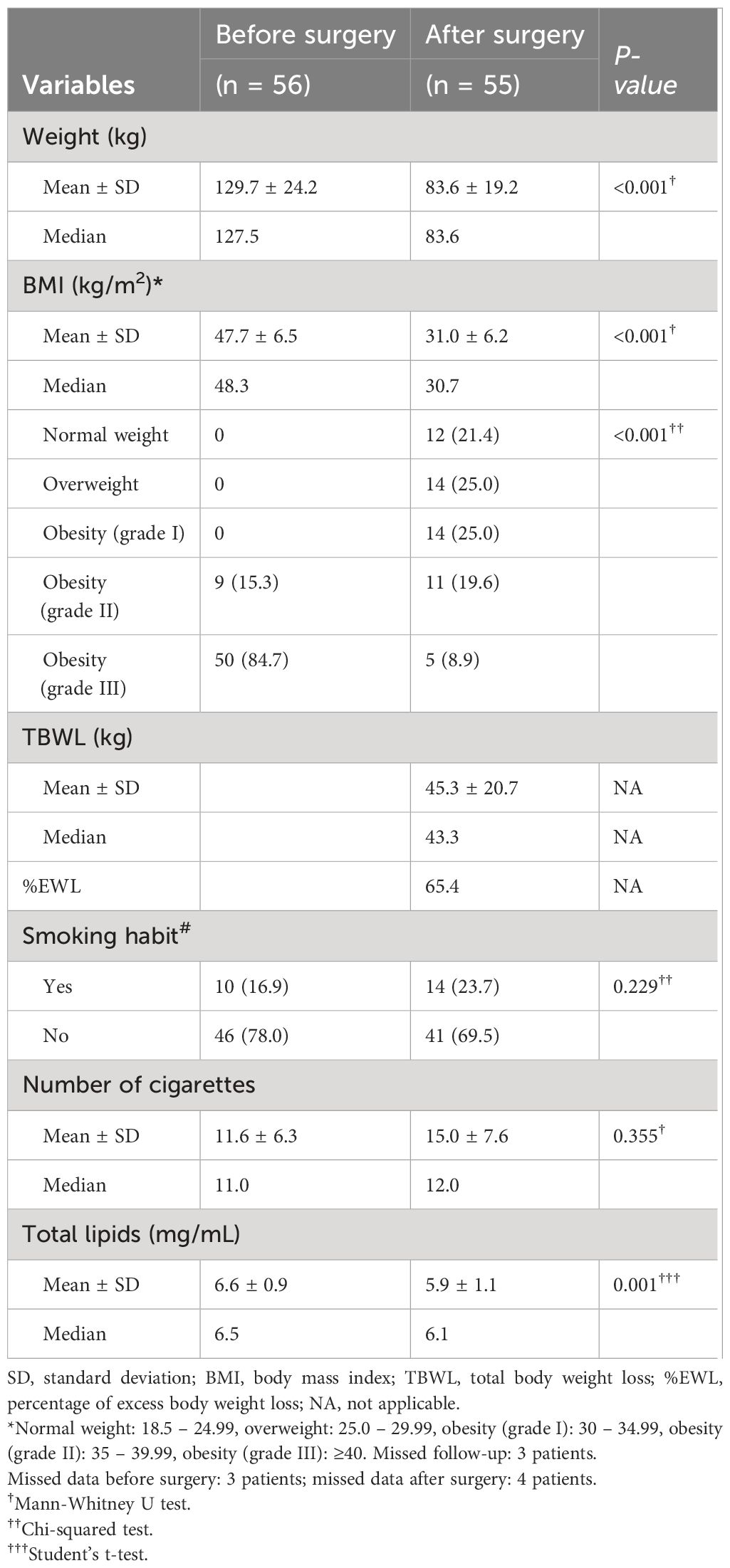
Table 2 Changes observed after surgery in the patients included in the study (mean follow-up (days): 534 ± 24.1).
A total of 353 compounds, including POPs, pesticides, pharmaceuticals, and rodenticides, were analyzed. Among them, 55 POPs –including 16 polycyclic aromatic hydrocarbons (PAH), 8 polybrominated diphenyl ethers (PBDE), 18 polychlorinated biphenyls (PCB) congeners and 13 organochlorine pesticides (OCP)- were included (Supplementary Table S1). The results shown below refer solely and exclusively to the compounds detected and quantified in the series.
Among the 55 POPs analyzed, dichlorodiphenyldichloroethilene (p,p’-DDE), hexachlorobenzene (HCB), β-hexachlorocyclohexane (β-HCH), PCB-138, PCB-153, PCB-180 and phenanthrene were identified in serum both before and after surgery (Table 3). Of note, p,p’-DDE displayed the highest frequency of detection before and after surgery, being detected in 69.6% and 96.2% of the patients, respectively. Changes were also observed in the detection rates of HCB (from 5.4% to 44.2%), β-HCH (from 8.9% to 59.9%), PCB-138 (from 16.1% to 75.0%), PCB-153 (from 10.7% to 61.5%), PCB-180 (from 10.7% to 73.1%) and phenanthrene (from 3.6% to 67.3%), with ρ<0.001 in all cases (Table 3). Certain OCPs, such as dichlorodiphenyldichloroethane (p,p’-DDD) and dichlorodiphenyltrichloroethane (p,p’-DDT), were detected in less than 5% of the series prior the surgery and were not present afterwards. Interestingly, naphthalene was only detected after the intervention, being observed in 71.2% of the patients. Other non-POP compounds were detected either before or after surgery. For instance, both frequency of detection and concentration of 2-phenylphenol changed during the follow-up, from 14.3% to 57.7% (ρ < 0.001) and from 1.2 ppb to 0.36 ppb (ρ = 0.029). This was not the case for acetaminophen, whose frequency of detection remained the same, even though mean concentration increased from 3.9 ppb to 9.9 ppb after surgery (Table 3). Lastly, fenitrothion and flucythrinate II were only detected after surgery, being present in 42.3% and 11.5% of the cohort, respectively.
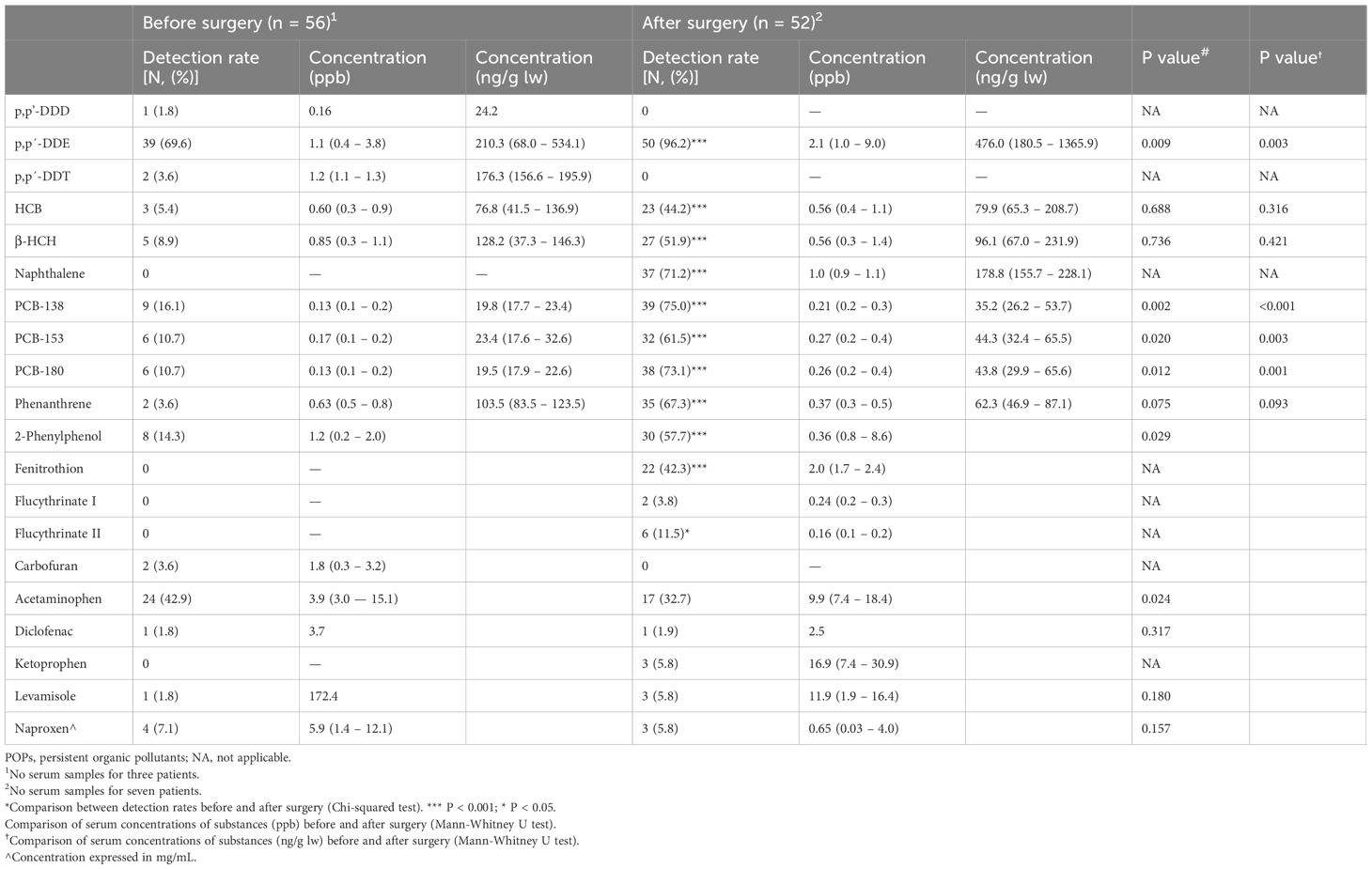
Table 3 Serum concentrations of detected substances before and after surgery. Detection rates and concentrations [expressed in median (percentile 25th—percentile 75th)] are included, in parts per billion (ng/mL) and, in the case of POPs, in ng/g lw.
After surgery, serum levels of p,p’-DDE increased from 210.3 ng/g lw to 476.0 ng/g lw (ρ = 0.003). PCB-138 increased from 19.8 ng/g lw to 35.2 ng/g lw (ρ < 0.001). Concentrations also increased from 23.4 ng/g lw to 44.3 ng/g lw in the case of PCB-153 (ρ = 0.003) and from 19.5 ng/g lw to 43.8 ng/g lw in the case of PCB-180 (ρ = 0.001) (Table 3, Figure 1). As for naphthalene, serum levels after surgery were 178.8 ng/g lw. With regards to phenanthrene, no significant changes in concentration were observed. We replicated the analyses using the Wilcoxon test, observing the same trend: ρ < 0.001, ρ = 0.028, ρ = 0.043 and ρ = 0.043 for p,p’-DDE and the PCB congeners -138, -153, and -180, respectively (Data not shown). No other significant differences were observed (Table 3). We wanted to explore which serum lipid parameters might be related to the observed changes in POPs levels. Before surgery, we did not observe any significant correlation between POPs concentrations and serum cholesterol, HDL, LDL or triglyceride levels (Data not shown). After surgery we observed a negative correlation between the concentration of HCB and HDL, so that the higher the HCB concentration, the lower the HDL concentration (τ = -0.576; ρ = 0.009). The same trend was observed between naphthalene and cholesterol (τ = -0.529; ρ = 0.001), HDL (τ = -0.438; ρ = 0.005), LDL (τ = -0.467; ρ = 0.003), and triglycerides (τ = -0.382; ρ = 0.013). Finally, a similar negative correlation was observed between phenanthrene and triglycerides (τ = -0.469; ρ = 0.005). No other significant correlations were detected.
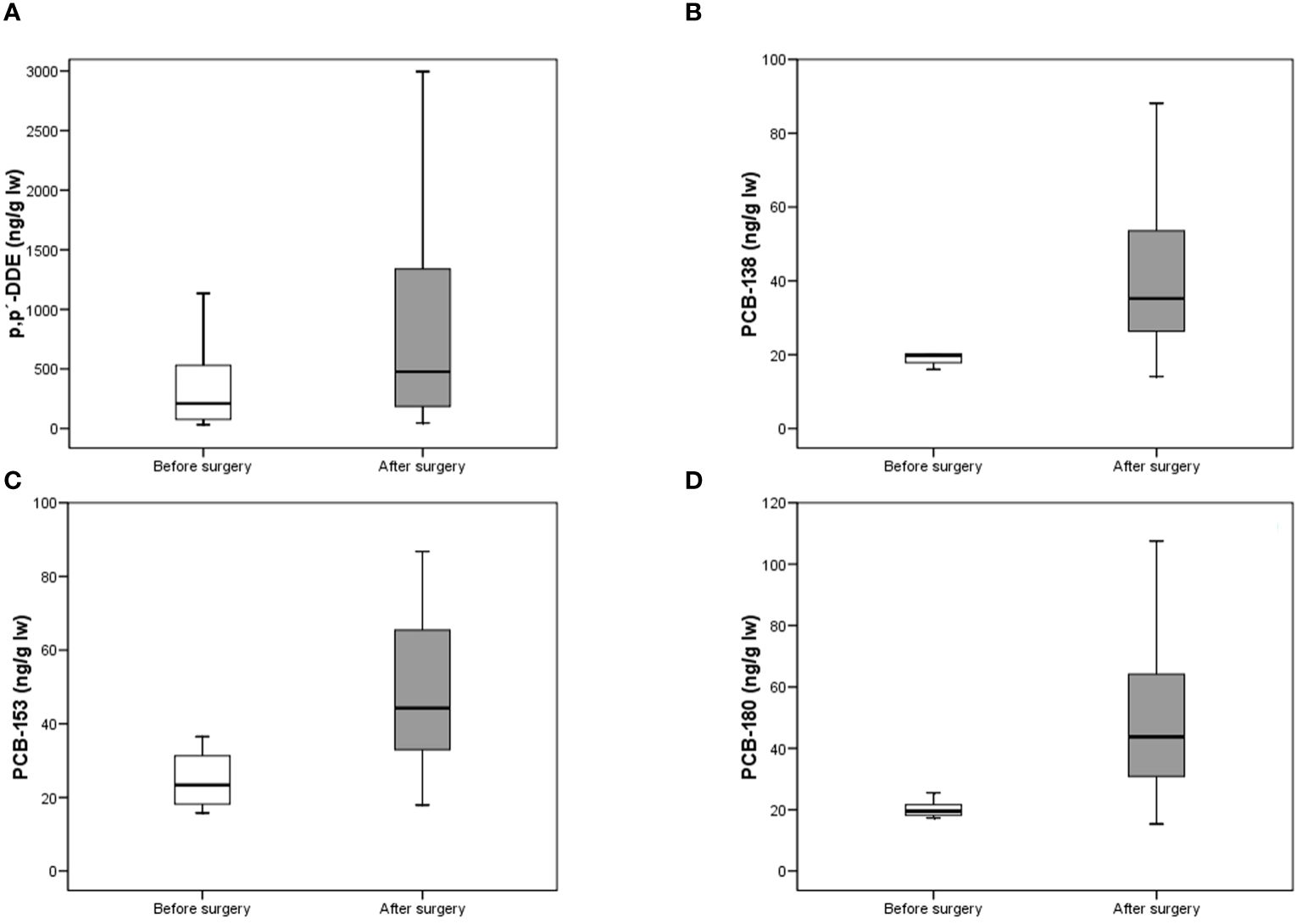
Figure 1 Concentrations (ng/g lw) of p,p’-DDE (A), PCB-138 (B), PCB-153 (C) and PCB-180 (D) before and after surgery (Mann-Whitney U test). The lines connect the medians, the boxes cover the 25th to 75th percentiles, and the minimal and maximal values are shown by the ends of the bars.
Following the surgical intervention, 12 patients reduced their weight to achieve normal values, while 16 remained with obesity type II-III (Table 2). We did not observe concentration differences of any of the analyzed substances between both groups (Mann-Whitney U test, ρ > 0.05 in all cases). In order to determine whether the increase observed in serum concentrations of POPs was associated with other variables included in the study, a bivariate correlation test was performed (Table 4). By analyzing the whole series, the elevation of naphthalene levels positively correlated with weight loss (τ = 0.317; ρ = 0.006), while a negative association with the increment of total lipids was observed (τ = -0.395; ρ = 0.001). However, segregation by sex revealed a different trend in women than in men. On one hand, the increase of naphthalene in females followed the pattern of the cohort when treated as a whole (for weight loss, τ = 0.351 and ρ = 0.012; for total lipids, τ = -0.439 and ρ = 0.002). In males, on the other, this increase was not associated with weight loss or increase of total lipids, but with time after surgery (τ = 0.661; ρ = 0.005). In the case of phenanthrene, a negative association with the increment of total lipids was observed both in the whole series (τ = -0.458; ρ < 0.001) and in women (τ = 0.529; ρ < 0.001), but not in men (Table 4). Finally, a positive association between the increasing levels of PCB-138 and weight loss was shown (τ = 0.223; ρ = 0.036). Nonetheless, such association was not observed when the series was segregated by sex (Table 4). The analyses regarding %EWL only showed a significant correlation with PCB-138 in the complete series (τ = 0.250; ρ = 0.025), with no significant differences observed when segmented by gender (Data not shown). No other correlations between POP concentrations and other sociodemographic variables were found.

Table 4 Bivariate correlations between serum POPs concentration in relation to time after surgery, weight loss and total lipid increase.
4 Discussion
The present study has demonstrated a significant increase in serum POPs levels associated with a substantial decrease in body weight following bariatric surgery. While age is indeed the primary demographic factor associated with increased levels of these substances, with a median of 532 days between both determinations, it is unlikely to be the underlying reason for the observed changes. Firstly, the levels of these substances have been decreasing over the decades (38, 39). Secondly, it has been observed that a decrease of 5 kilograms or more within a short period (1 year) is associated with an increase in POPs concentrations (38, 39). Lastly, recent studies have observed that patients undergoing bariatric surgery experience a significant increase in the concentrations of these substances in their bodies (40). In this regard, it is important to highlight that we did not observe significant changes in POPs levels due to the time elapsed between both measurements (Kendall’s τ test, ρ > 0.05 in all cases; Data not shown). However, to ascertain that any observed increases are attributable to rapid weight loss rather than solely accumulation over time, it would be interesting to compare the present findings with those of an intervention-free control group. Multiple control groups should be studied, comprising a lean group without intervention, an obese group without intervention, an obese group with gradual weight loss through lifestyle modifications, and an obese group with rapid weight loss through alternative methods such as lipectomy or pharmaceuticals. This approach would contribute to understanding the role of rapid weight loss in relation to the presence of these substances, especially when we do not observe significant differences between those patients who, after the surgical intervention, reduced their weight to normal values compared to those who remained with obesity type II-III. This suggests that the initial burden of pollutants, together with other demographic variables such as age and sex, significantly contribute to modulating the levels of these substances in the body.
To date, bariatric surgery is still the most effective intervention to treat obesity. In this study, we observed a mean weight loss of 45.28 kg, accounting for a 63.9% of excess weight loss (EWL), which allowed 21.4% of the patients to reach normal weight. This is in line with previous publications, in which patients managed to lose over 30 kg in one year (41, 42). It has been reported that maximum weight loss is achieved two years after surgery (43). Thus, differences in weight loss might be explained by the fact that patients were followed up for a longer period, namely 534 ± 24 days.
It was previously reported that p,p’-DDE, HCB, β-HCH, PCB-138 and PCB-180 were detected in more than half of the obese, elderly Canarian population (PREDIMED-plus) (18). In the present cohort, detection rates displayed by all POPs before surgery were lower detection rates than those observed in previous studies. However, they increased after surgery, being similar to those observed in the PREDIMED-plus for p,p’-DDE and even higher for PCB-138. Increases in the detection rates of circulating POPs after rapid weight loss have already been described (18, 41, 44) and it highlights the toxicological role of the adipose tissue, which is thought to sequester lipophilic xenobiotic molecules, thereby preventing other cell types from their deleterious effect (45).
Dichlorodiphenyldichloroethilene is a metabolite that results from the dehydrohalogenation of the organochlorine pesticide p,p’-DDT. Even though it was banned in most countries in the last decades of the 20th century, p,p’-DDT, p,p’-DDE and p,p’-DDD are still present in the population worldwide (18, 41). In this cohort, p,p’-DDE was the most frequently detected POP and showed the highest serum levels both before and after surgery, with detection rates of 69.6% and 96.2% and concentrations of 210.3 ng/g lw and 476.0 ng/g lw, respectively. This contrasts with results from the PREDIMED-plus, in which a detection rate of 95.4% and a mean concentration of 697.4 ng/g lw were determined. BMI was stated as a predictor of p,p’-DDE concentration (18). Nonetheless, levels of p,p’-DDE observed in this study are generally lower, despite the fact that mean BMI was much higher before surgery. This results might be explained by differences in age between these two cohorts (66.4 vs 43.4 years), given that a positive correlation between age and serum levels of POPs has been demonstrated by our group (18). Considering that DDT was banned in Spain in the 1970s (46), older individuals were probably subject to direct exposure during pregnancy and early life, which might have led to higher serum levels of DDT metabolites in the adulthood. Yet, p,p’-DDE is still the most prevalent POP in the Canary islands regardless the mean age of the participants, probably due to intensive use, transplacental transfer during pregnancy (21) and bioaccumulation through the trophic chain (19).
A completely different scenario was observed in the case of HCB and β-HCH, whose detection rates increased after surgery but no concentration increment was observed. Conversely, previous studies on the relation between bariatric surgery and serum POPs showed an increase in levels of both OCPs (41). Increase in HCB and β-HCH levels after weight loss has been also reported in obese non-operated individuals (18, 47, 48). HCB and β-HCH are highly persistent (49), being the β-HCH the most resistant to degradation and the most prevalent in the environment (Srivastava, 50). Due to the mean age of the patients, direct exposure to these toxicants is not expected. Thus, dietary intake might have played an important role in their accumulation in the body due to biomagnification, given that they are especially susceptible to atmospheric deposition on the soil (51). More profound knowledge on diet and lifestyle may be necessary to fully comprehend the different routes of exposure.
With regards to the PCBs, they are industrial halogenated chemicals that were widely used as lubricants and coolants in electronic devices until their application was banned in the last decades of the 20th century. More than 20 years later, numerous PCB congeners are still present in most populations and have been detected in blood and breast milk (52, 53), being the congeners 138, 153 and 180 the most frequently detected in the Canary islands (18, 39). In this study, these congeners were detected before and after surgery and displayed an increase in both detection rate and concentration. It has been stablished that PCB exposure takes place mainly via dietary intake and indoor air inhalation (54). However, differences in pharmacokinetics and degradation patterns hamper the determination of the primary composition of manufacture mixtures and, consequently, their origin (55). Remarkably, bivariate correlation tests revealed a significant positive association between PCB-138 serum levels and weight loss. This suggests a possible contribution of the adipose tissue by acting as an endogenous source of exposure in conditions of enhanced lypolysis (45). However, other variables must be considered when interpreting the present results. It is important to highlight the close relationship between serum levels of certain POPs (such as PCBs) and body composition. In this regard, it has been observed that visceral fat releases a greater amount of PCBs than subcutaneous fat in individuals subjected to strict weight loss diets, a finding that could not be replicated in patients undergoing bariatric surgery (56). Moreover, a significant negative correlation has been observed between BMI, waist circumference, fat mass percentage, total and subcutaneous abdominal adipose tissue, and serum PCB levels (57). Although our results support previous observations by other authors, it is necessary to understand the pharmacokinetics of these compounds to comprehend the consequences of fat tissue mobilization, especially when it occurs rapidly.
Polycyclic aromatic hydrocarbons are not POPs per se. Although they are semipersistent, their constant, massive release into the atmosphere has led them to be included in this category. Here, we report a substantial increase in the detection rate of both naphthalene and phenanthrene after surgery. To our knowledge, this is the first time that increases in detection rates and serum levels of PAHs after weight loss are described. Naphthalene and phenanthrene are petrogenic-origin volatile compounds that can be suspended in both indoor and outdoor air (58, 59), which suggests that transport from industrialized north African regions may contribute to exposure. Dietary intake via plant products and processed food is also considered an important source of exposure to PAHs (60, 61). Nonetheless, these factors might not fully explain such changes in the prevalence of these contaminants. We hypothesize that sequestration in scarcely metabolically active white adipose tissue, which constitutes a hallmark of obesity pathophysiology, could protect PAHs from degradation, thereby allowing them to accumulate. The observed concentration increase in women positively correlates with weight loss for naphthalene, and negatively correlates with variation in total lipids for both naphthalene and phenanthrene, thereby supporting this hypothesis. In that sense, further research in the mechanisms of interplay between blood and adipose tissue is required.
Given the health risks that obesity poses for the individuals, it is undeniable that bariatric surgery is the most effective treatment to prevent complications associated with this disease, thus constituting a potent tool to alleviate the healthcare system (13). This fact is particularly important in the Canarian archipelago, where obesity, diabetes and metabolic syndrome are highly prevalent (62). Nevertheless, such increase of serum levels of POPs after bariatric surgery-induced rapid weight loss should not be ignored, especially considering that physical exercise, as a weight control strategy, has been proposed as an effective approach to reduce the adverse effects of POPs in situations of rapid weight loss (63). In this regard, the benefits of physical exercise — healthier lifestyle, better vascular health, or better intestinal microecological balance— should be complemented by its ability to reduce the burden of POPs and their adverse effects (64). Therefore, beyond the outcome of bariatric surgery, physical exercise should complement obesity treatment, not only in mitigating the action of contaminants but also due to its enormous health benefits.
These contaminants have the capability to alter molecular, metabolic and endocrine pathways, leading to the development of diverse pathologies (65). For instance, PCBs and OCPs are molecules with endocrine-disrupting and neurotoxic potential whose exposure is associated with elevation of inflammatory markers, cardiovascular disorders, breast and prostate cancer and endometriosis (27, 49, 55, 66). Strong associations between carcinogenesis and PAH exposure have also been demonstrated and additive effects in mixtures of PAHs have been suggested (67, 68). Particularly, naphthalene and phenanthrene, which were highly prevalent in this series after surgery, are correlated with erythrocyte disruption and cardiovascular disease, respectively (69). Furthermore, synergistic effects have been described in certain POPs (70), although the role of exposure-related pathogenesis remains unclear. Based on our results, it would be expected that the literature would report associations between bariatric surgery and pathologies related to POPs, such as neurotoxicity or cancer. While it is true that an association between bariatric surgery and certain neurological pathologies has been observed (71), some authors attribute it to nutritional deficiencies (72, 73) while others do not (74). Therefore, it cannot be ruled out that certain toxins mobilized as a result of weight loss may play a role. Regarding cancer, the literature shows that bariatric surgery reduces the incidence of both hormone-dependent and non-hormone-dependent cancers (75–77). Overall, even though the risk-benefit ratio of bariatric surgery is positive, and policies have proven effective on lowering the environmental burden of POPs, we believe that strong follow-up, legislative and biomonitoring measures are required to prevent the development of exposure-associated pathologies.
5 Conclusion
Bariatric surgery-induced weight loss led to a significant increase of detection rates and serum levels of p,p’-DDE, HCB, β-HCH and PCB congeners 138, 153 and 180. Detection rates of PAHs, namely naphthalene and phenanthrene, also increased after surgery. Sex differences were found with respect to the correlation between concentration of naphthalene, phenanthrene and PCB-138 and weight loss, total lipids and time after surgery. To our knowledge, the effect of bariatric surgery on the concentration of POPs had not previously been assessed in Spain. Moreover, this is the first time that presence of circulating PAHs after surgery is recorded. The role of adipose tissue as a source of POP exposure and the potential effects of the release of these compounds into the circulatory system are not clear. Thus, toxicokinetics of POPs, as their effects on peripheral tissues, and the mechanisms underlying adipocyte-blood transfer, require further investigation.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Clinical Research Ethics Committee of the CHUIMI (Complejo Hospitalario Universitario Insular Materno Infantil): ethical approval code 2024-093-728, on June 26th, 2014. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
BVD-G: Data curation, Writing – review & editing, Methodology. ÁR-L: Writing – review & editing. LAH-H: Data curation, Formal analysis, Supervision, Writing – review & editing. LS-M: Conceptualization, Writing – review & editing. IB-C: Data curation, Methodology, Writing – review & editing. AA-D: Methodology, Writing – review & editing. OPL: Funding acquisition, Supervision, Writing – review & editing. EH-G: Data curation, Writing – review & editing. JC-T: Data curation, Writing – review & editing. JRH-H: Data curation, Writing – review & editing. PF-V: Methodology, Supervision, Writing – original draft.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was partially funded by a predoctoral grant to ÁR-L from the University of Las Palmas de Gran Canaria (ULPGC-2021-2022) and by a post-doctoral grant to the author AA-D (APCR2022010003) from the Catalina Ruiz research staff training aid program of the Regional Ministry of Economy, Knowledge and Employment of the Canary Islands Government.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2024.1412261/full#supplementary-material
References
1. Ng M, Fleming T, Robinson M, Thomson B, Graetz N, Margono C, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. (2014) 384:766–81. doi: 10.1016/S0140-6736(14)60460-8
2. WHO. Obesity and overweight (2021). Available online at: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
3. Dhurandhar NV, Petersen KS, Webster C. Key causes and contributors of obesity: A perspective. Nurs Clin North Am. (2021) 56:449–64. doi: 10.1016/j.cnur.2021.07.007
4. Boutari C, Mantzoros CS. A 2022 update on the epidemiology of obesity and a call to action: as its twin COVID-19 pandemic appears to be receding, the obesity and dysmetabolism pandemic continues to rage on. Metabolism. (2022) 133:155217. doi: 10.1016/j.metabol.2022.155217
5. Smith KB, Smith MS. Obesity statistics. Prim Care. (2016) 43:121–135, ix. doi: 10.1016/j.pop.2015.10.001
6. Salvestrini V, Sell C, Lorenzini A. Obesity may accelerate the aging process. Front Endocrinol (Lausanne). (2019) 10:266. doi: 10.3389/fendo.2019.00266
7. Green M, Arora K, Prakash S. Microbial medicine: prebiotic and probiotic functional foods to target obesity and metabolic syndrome. Int J Mol Sci. (2020) 21:2890. doi: 10.3390/ijms21082890
8. Henriquez-Hernandez LA, Luzardo OP, Zumbado M, Camacho M, Serra-Majem L, Alvarez-Leon EE, et al. Blood pressure in relation to contamination by polychlorobiphenyls and organochlorine pesticides: Results from a population-based study in the Canary Islands (Spain). Environ Res. (2014) 135:48–54. doi: 10.1016/j.envres.2014.05.036
9. Vekic J, Zeljkovic A, Stefanovic A, Jelic-Ivanovic Z, Spasojevic-Kalimanovska V. Obesity and dyslipidemia. Metabolism. (2019) 92:71–81. doi: 10.1016/j.metabol.2018.11.005
10. Santos AL, Sinha S. Obesity and aging: Molecular mechanisms and therapeutic approaches. Ageing Res Rev. (2021) 67:101268. doi: 10.1016/j.arr.2021.101268
11. Muscogiuri G, Bettini S, Boschetti M, Barrea L, Savastano S, Colao AER, et al. Low-grade inflammation, CoVID-19, and obesity: clinical aspect and molecular insights in childhood and adulthood. Int J Obes (Lond). (2022) 46:1254–61. doi: 10.1038/s41366-022-01111-5
12. Ruban A, Stoenchev K, Ashrafian H, Teare J. Current treatments for obesity. Clin Med (Lond). (2019) 19:205–12. doi: 10.7861/clinmedicine.19-3-205
13. Perdomo CM, Cohen RV, Sumithran P, Clement K, Fruhbeck G. Contemporary medical, device, and surgical therapies for obesity in adults. Lancet. (2023) 401:1116–30. doi: 10.1016/S0140-6736(22)02403-5
14. Colquitt JL, Pickett K, Loveman E, Frampton GK. Surgery for weight loss in adults. Cochrane Database Syst Rev. (2014) 2014:CD003641. doi: 10.1002/14651858.CD003641.pub4
15. Lafontan M. Historical perspectives in fat cell biology: the fat cell as a model for the investigation of hormonal and metabolic pathways. Am J Physiol Cell Physiol. (2012) 302:C327–359. doi: 10.1152/ajpcell.00168.2011
16. Papalou O, Kandaraki EA, Papadakis G, Diamanti-Kandarakis E. Endocrine disrupting chemicals: an occult mediator of metabolic disease. Front Endocrinol (Lausanne). (2019) 10:112. doi: 10.3389/fendo.2019.00112
17. Aaseth J, Javorac D, Djordjevic AB, Bulat Z, Skalny AV, Zaitseva IP, et al. The role of persistent organic pollutants in obesity: A review of laboratory and epidemiological studies. Toxics. (2022) 10:65. doi: 10.3390/toxics10020065
18. Henriquez-Hernandez LA, Ortiz-Andrelluchi A, Alvarez-Perez J, Acosta-Dacal A, Zumbado M, Martinez-Gonzalez MA, et al. Human biomonitoring of persistent organic pollutants in elderly people from the Canary Islands (Spain): A temporal trend analysis from the PREDIMED and PREDIMED-Plus cohorts. Sci Total Environ. (2021) 758:143637. doi: 10.1016/j.scitotenv.2020.143637
19. Jones KC. Persistent organic pollutants (POPs) and related chemicals in the global environment: some personal reflections. Environ Sci Technol. (2021) 55:9400–12. doi: 10.1021/acs.est.0c08093
20. Convention S. All POPs listed in the Stockholm Convention. Geneve, Switzerland: Stockholm Conference, Stockholm, Stockholm Convention Web site (2019).
21. Zhang X, Cheng X, Lei B, Zhang G, Bi Y, Yu Y. A review of the transplacental transfer of persistent halogenated organic pollutants: Transfer characteristics, influential factors, and mechanisms. Environ Int. (2021) 146:106224. doi: 10.1016/j.envint.2020.106224
22. Kaiser J. Developmental biology. Endocrine disrupters trigger fertility problems in multiple generations. Science. (2005) 308:1391–2. doi: 10.1126/science.308.5727.1391a
23. Soto AM, Sonnenschein C. Environmental causes of cancer: endocrine disruptors as carcinogens. Nat Rev Endocrinol. (2010) 6:363–70. doi: 10.1038/nrendo.2010.87
24. Boada LD, Zumbado M, Henriquez-Hernandez LA, Almeida-Gonzalez M, Alvarez-Leon EE, Serra-Majem L, et al. Complex organochlorine pesticide mixtures as determinant factor for breast cancer risk: a population-based case-control study in the Canary Islands (Spain). Environ Health. (2012) 11:28. doi: 10.1186/1476-069X-11-28
25. Fenichel P, Chevalier N. Environmental endocrine disruptors: New diabetogens? C R Biol. (2017) 340:446–52. doi: 10.1016/j.crvi.2017.07.003
26. Henriquez-Hernandez LA, Luzardo OP, Valeron PF, Zumbado M, Serra-Majem L, Camacho M, et al. Persistent organic pollutants and risk of diabetes and obesity on healthy adults: Results from a cross-sectional study in Spain. Sci Total Environ. (2017) 607-608:1096–102. doi: 10.1016/j.scitotenv.2017.07.075
27. Pinson A, Franssen D, Gerard A, Parent AS, Bourguignon JP. Neuroendocrine disruption without direct endocrine mode of action: Polychloro-biphenyls (PCBs) and bisphenol A (BPA) as case studies. C R Biol. (2017) 340:432–8. doi: 10.1016/j.crvi.2017.07.006
28. Henriquez-Hernandez LA, Luzardo OP, Zumbado M, Serra-Majem L, Valeron PF, Camacho M, et al. Determinants of increasing serum POPs in a population at high risk for cardiovascular disease. Results from the PREDIMED-CANARIAS study. Environ Res. (2017) 156:477–84. doi: 10.1016/j.envres.2017.03.053
29. BOE. ORDEN de 1 de febrero de 1991 por la que se modifica el anexo de la de 7 de septiembre de 1989, sobre prohibición de comercialización y utilización de ciertos productos fitosanitarios en aplicación de las Directivas 90/335/CEE y 90/533/CEE (BOE n°37 del martes 12 de febrero de 1991) Vol. 37. Madrid, Spain: P. y. A. Ministerio de Agricultura. BOE (1991). p. 4777.
30. BOE. RD 1378/1999, de 27 de agosto, por el que se establecen medidas para la eliminación y gestión de los policlorobifenilos, policloroterfenilos y aparatos que los contengan. Madrid, Spain: M. d. l. Presidencia. BOE-A-1999-18193 (1999).
31. Porta M, Puigdomenech E, Ballester F, Selva J, Ribas-Fito N, Dominguez-Boada L, et al. [Studies conducted in Spain on concentrations in humans of persistent toxic compounds]. Gac Sanit. (2008) 22:248–66. doi: 10.1157/13123971
32. Anastassiades M, Lehotay SJ, Stajnbaher D, Schenck FJ. Fast and easy multiresidue method employing acetonitrile extraction/partitioning and “dispersive solid-phase extraction” for the determination of pesticide residues in produce. J AOAC Int. (2003) 86:412–31. doi: 10.1093/jaoac/86.2.412
33. Rial-Berriel C, Ramos-Luzardo Á, Acosta-Dacal A, Macías-Montes A, Fernández-Valerón P, Henríquez-Hernández LA, et al. Validation of a method scope extension for simple biomonitoring of 353 pollutants in serum samples. Toxins (2023) 11(6):498. doi: 10.3390/toxics11060498
34. Rial-Berriel C, Acosta-Dacal A, Gonzalez F, Pastor-Tiburon N, Zumbado M, Luzardo OP. Supporting dataset on the validation and verification of the analytical method for the biomonitoring of 360 toxicologically relevant pollutants in whole blood. Data Brief. (2020) 31:105878. doi: 10.1016/j.dib.2020.105878
35. EC. Analytical quality control and method validation procedures for pesticide residues in food and feed. E. Comission. SANTE/12682/2019. Brussels, Belgium (2019).
36. Phillips DL, Pirkle JL, Burse VW, Bernert JT Jr., Henderson LO, Needham LL. Chlorinated hydrocarbon levels in human serum: effects of fasting and feeding. Arch Environ Contam Toxicol. (1989) 18:495–500. doi: 10.1007/BF01055015
37. Bernert JT, Turner WE, Patterson DG Jr., Needham LL. Calculation of serum “total lipid” concentrations for the adjustment of persistent organohalogen toxicant measurements in human samples. Chemosphere. (2007) 68:824–31. doi: 10.1016/j.chemosphere.2007.02.043
38. Porta M, Lopez T, Gasull M, Rodriguez-Sanz M, Gari M, Pumarega J, et al. Distribution of blood concentrations of persistent organic pollutants in a representative sample of the population of Barcelona in 2006, and comparison with levels in 2002. Sci Total Environ. (2012) 423:151–61. doi: 10.1016/j.scitotenv.2012.02.001
39. Henriquez-Hernandez LA, Macias-Montes A, Acosta-Dacal A, Rial-Berriel C, Duarte-Lopes E, Lopes-Ribeiro AL, et al. Human biomonitoring of persistent and non-persistent pollutants in a representative sample of the general population from Cape Verde: Results from the PERVEMAC-II study. Environ Pollut. (2022) 306:119331. doi: 10.1016/j.envpol.2022.119331
40. Jansen A, Lyche JL, Polder A, Aaseth J, Skaug MA. Increased blood levels of persistent organic pollutants (POP) in obese individuals after weight loss-A review. J Toxicol Environ Health B Crit Rev. (2017) 20:22–37. doi: 10.1080/10937404.2016.1246391
41. Jansen A, Polder A, Muller MHB, Skjerve E, Aaseth J, Lyche JL. Increased levels of persistent organic pollutants in serum one year after a great weight loss in humans: Are the levels exceeding health based guideline values? Sci Total Environ. (2018) 622-623:1317–26. doi: 10.1016/j.scitotenv.2017.11.241
42. Sundgot-Borgen C, Bond DS, Sniehotta FF, Kvalem IL, Hansen BH, Bergh I, et al. Associations of changes in physical activity and sedentary time with weight recurrence after bariatric surgery: a 5-year prospective study. Int J Obes (Lond). (2023) 47:463–70. doi: 10.1038/s41366-023-01284-7
43. O’Brien PE, Hindle A, Brennan L, Skinner S, Burton P, Smith A, et al. Long-term outcomes after bariatric surgery: a systematic review and meta-analysis of weight loss at 10 or more years for all bariatric procedures and a single-centre review of 20-year outcomes after adjustable gastric banding. Obes Surg. (2019) 29:3–14. doi: 10.1007/s11695-018-3525-0
44. Brown RH, Ng DK, Steele K, Schweitzer M, Groopman JD. Mobilization of environmental toxicants following bariatric surgery. Obes (Silver Spring). (2019) 27:1865–73. doi: 10.1002/oby.22618
45. La Merrill M, Emond C, Kim MJ, Antignac JP, Le Bizec B, Clement K, et al. Toxicological function of adipose tissue: focus on persistent organic pollutants. Environ Health Perspect. (2013) 121:162–9. doi: 10.1289/ehp.1205485
46. BOE. Orden de 4 de diciembre de 1975 por la que se restringe el uso de ciertos plaguicidas de elevada persistencia Vol. 308. Madrid, Spain: M. d. Agricultura. BOE (1975). p. 26651.
47. Dirtu AC, Dirinck E, Malarvannan G, Neels H, Van Gaal L, Jorens PG, et al. Dynamics of organohalogenated contaminants in human serum from obese individuals during one year of weight loss treatment. Environ Sci Technol. (2013) 47:12441–9. doi: 10.1021/es400657t
48. Malarvannan G, Van Hoorenbeeck K, Deguchtenaere A, Verhulst SL, Dirinck E, Van Gaal L, et al. Dynamics of persistent organic pollutants in obese adolescents during weight loss. Environ Int. (2018) 110:80–7. doi: 10.1016/j.envint.2017.10.009
49. Jayaraj R, Megha P, Sreedev P. Organochlorine pesticides, their toxic effects on living organisms and their fate in the environment. Interdiscip Toxicol. (2016) 9:90–100. doi: 10.1515/intox-2016-0012
50. Srivastava V, Srivastava T, Kumar MS. Fate of the persistent organic pollutant (POP)Hexachlorocyclohexane (HCH) and remediation challenges. Int Biodeterioration Biodegradation. (2019) 140:43–56. doi: 10.1016/j.ibiod.2019.03.004
51. Femina Carolin C, Kamalesh T, Senthil Kumar P, Rangasamy G. An insights of organochlorine pesticides categories, properties, eco-toxicity and new developments in bioremediation process. Environ Pollut. (2023) 333:122114. doi: 10.1016/j.envpol.2023.122114
52. Kraft M, Rauchfuss K, Sievering S, Wockner M, Neugebauer F, Fromme H. Quantification of all 209 PCB congeners in blood-Can indicators be used to calculate the total PCB blood load? Int J Hyg Environ Health. (2017) 220:201–8. doi: 10.1016/j.ijheh.2016.09.006
53. Lehmann GM, LaKind JS, Davis MH, Hines EP, Marchitti SA, Alcala C, et al. Environmental chemicals in breast milk and formula: exposure and risk assessment implications. Environ Health Perspect. (2018) 126:96001. doi: 10.1289/EHP1953
54. Weitekamp CA, Phillips LJ, Carlson LM, DeLuca NM, Cohen Hubal EA, Lehmann GM. A state-of-the-science review of polychlorinated biphenyl exposures at background levels: relative contributions of exposure routes. Sci Total Environ. (2021) 776:145912. doi: 10.1016/j.scitotenv.2021.145912
55. Carlson LM, Christensen K, Sagiv SK, Rajan P, Klocke CR, Lein PJ, et al. A systematic evidence map for the evaluation of noncancer health effects and exposures to polychlorinated biphenyl mixtures. Environ Res. (2023) 220:115148. doi: 10.1016/j.envres.2022.115148
56. Dirinck E, Dirtu AC, Jorens PG, Malarvannan G, Covaci A, Van Gaal LF. Pivotal role for the visceral fat compartment in the release of persistent organic pollutants during weight loss. J Clin Endocrinol Metab. (2015) 100:4463–71. doi: 10.1210/jc.2015-2571
57. Dirinck E, Jorens PG, Covaci A, Geens T, Roosens L, Neels H, et al. Obesity and persistent organic pollutants: possible obesogenic effect of organochlorine pesticides and polychlorinated biphenyls. Obes (Silver Spring). (2011) 19:709–14. doi: 10.1038/oby.2010.133
58. Ifegwu OC, Anyakora C. Polycyclic aromatic hydrocarbons: part I. Exposure. Adv Clin Chem. (2015) 72:277–304. doi: 10.1016/bs.acc.2015.08.001
59. Ma Y, Harrad S. Spatiotemporal analysis and human exposure assessment on polycyclic aromatic hydrocarbons in indoor air, settled house dust, and diet: A review. Environ Int. (2015) 84:7–16. doi: 10.1016/j.envint.2015.07.006
60. Singh L, Varshney JG, Agarwal T. Polycyclic aromatic hydrocarbons’ formation and occurrence in processed food. Food Chem. (2016) 199:768–81. doi: 10.1016/j.foodchem.2015.12.074
61. Paris A, Ledauphin J, Poinot P, Gaillard JL. Polycyclic aromatic hydrocarbons in fruits and vegetables: Origin, analysis, and occurrence. Environ pollut. (2018) 234:96–106. doi: 10.1016/j.envpol.2017.11.028
62. Hernández-Yumar A, Abásolo Alessón I, González López-Valcárcel B. Economic crisis and obesity in the Canary Islands: an exploratory study through the relationship between body mass index and educational level. BMC Public Health. (2019) 19:1755. doi: 10.1186/s12889-019-8098-x
63. Serrano QA, Le Garf S, Martin V, Colson SS, Chevalier N. Is physical activity an efficient strategy to control the adverse effects of persistent organic pollutants in the context of obesity? A narrative review. Int J Mol Sci. (2024) 25:883. doi: 10.3390/ijms25020883
64. Liu C, Hou HS. Physical exercise and persistent organic pollutants. Heliyon. (2023) 9:e19661. doi: 10.1016/j.heliyon.2023.e19661
65. Alharbi OML, Basheer AA, Khattab RA, Ali I. Health and environmental effects of persistent organic pollutants. J Mol Liquids. (2018) 263:442–53. doi: 10.1016/j.molliq.2018.05.029
66. Peinado FM, Artacho-Cordon F, Barrios-Rodriguez R, Arrebola JP. Influence of polychlorinated biphenyls and organochlorine pesticides on the inflammatory milieu. A systematic review of in vitro, in vivo and epidemiological studies. Environ Res. (2020) 186:109561. doi: 10.1016/j.envres.2020.109561
67. Patel AB, Shaikh S, Jain KR, Desai C, Madamwar D. Polycyclic aromatic hydrocarbons: sources, toxicity, and remediation approaches. Front Microbiol. (2020) 11:562813. doi: 10.3389/fmicb.2020.562813
68. Barbosa F Jr., Rocha BA, Souza MCO, Bocato MZ, Azevedo LF, Adeyemi JA, et al. Polycyclic aromatic hydrocarbons (PAHs): Updated aspects of their determination, kinetics in the human body, and toxicity. J Toxicol Environ Health B Crit Rev. (2023) 26:28–65. doi: 10.1080/10937404.2022.2164390
69. Mallah MA, Changxing L, Mallah MA, Noreen S, Liu Y, Saeed M, et al. Polycyclic aromatic hydrocarbon and its effects on human health: An overeview. Chemosphere. (2022) 296:133948. doi: 10.1016/j.chemosphere.2022.133948
70. Rainey NE, Saric A, Leberre A, Dewailly E, Slomianny C, Vial G, et al. Synergistic cellular effects including mitochondrial destabilization, autophagy and apoptosis following low-level exposure to a mixture of lipophilic persistent organic pollutants. Sci Rep. (2017) 7:4728. doi: 10.1038/s41598-017-04654-0
71. Foster D, Falah M, Kadom N, Mandler R. Wernicke encephalopathy after bariatric surgery: losing more than just weight. Neurology. (2005) 65:1987; discussion 1847. doi: 10.1212/01.wnl.0000188822.86529.f0
72. Thaisetthawatkul P, Collazo-Clavell ML, Sarr MG, Norell JE, Dyck PJ. A controlled study of peripheral neuropathy after bariatric surgery. Neurology. (2004) 63:1462–70. doi: 10.1212/01.WNL.0000142038.43946.06
73. Alligier M, Borel AL, Savey V, Rives-Lange C, Brindisi MC, Piguel X, et al. A series of severe neurologic complications after bariatric surgery in France: the NEUROBAR Study. Surg Obes Relat Dis. (2020) 16:1429–35. doi: 10.1016/j.soard.2020.05.031
74. Clark N. Neuropathy following bariatric surgery. Semin Neurol. (2010) 30:433–5. doi: 10.1055/s-0030-1267287
75. Casagrande DS, Rosa DD, Umpierre D, Sarmento RA, Rodrigues CG, Schaan BD. Incidence of cancer following bariatric surgery: systematic review and meta-analysis. Obes Surg. (2014) 24:1499–509. doi: 10.1007/s11695-014-1276-0
76. Schauer DP, Feigelson HS, Koebnick C, Caan B, Weinmann S, Leonard AC, et al. Bariatric surgery and the risk of cancer in a large multisite cohort. Ann Surg. (2019) 269(1):95–101. doi: 10.1097/SLA.0000000000002525
Keywords: obesity, bariatric surgery, persistent organic pollutants, weight loss, obesogens
Citation: Díaz-González BV, Ramos-Luzardo Á, Henríquez-Hernández LA, Serra-Majem L, Bautista-Castaño I, Acosta-Dacal A, Luzardo OP, Hernández-García E, Cornejo-Torre J, Hernández-Hernández JR and Fernández-Valerón P (2024) Effect of bariatric surgery in the body burden of persistent and non-persistent pollutants: longitudinal study in a cohort of morbidly obese patients. Front. Endocrinol. 15:1412261. doi: 10.3389/fendo.2024.1412261
Received: 04 April 2024; Accepted: 09 July 2024;
Published: 22 July 2024.
Edited by:
Sjaak Pouwels, Elisabeth Tweesteden Hospital (ETZ), NetherlandsReviewed by:
Suba Gunawardana, Washington University in St. Louis, United StatesLuz-Ma.-Adriana Balderas-Peña, Instituto Mexicano del Seguro Social, Mexico
Copyright © 2024 Díaz-González, Ramos-Luzardo, Henríquez-Hernández, Serra-Majem, Bautista-Castaño, Acosta-Dacal, Luzardo, Hernández-García, Cornejo-Torre, Hernández-Hernández and Fernández-Valerón. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Luis Alberto Henríquez-Hernández, bHVpcy5oZW5yaXF1ZXpAdWxwZ2MuZXM=
†These authors have contributed equally to this work and share first authorship