 Bibi Uhre Nielsen1*†
Bibi Uhre Nielsen1*† Christine Råberg Mikkelsen1†Peter Sandor Oturai2
Christine Råberg Mikkelsen1†Peter Sandor Oturai2 Rikke Krogh-Madsen3,4
Rikke Krogh-Madsen3,4 Terese Lea Katzenstein1
Terese Lea Katzenstein1 Christian Ritz5
Christian Ritz5 Tacjana Pressler1Thomas Peter Almdal6Inger Hee Mabuza Mathiesen1
Tacjana Pressler1Thomas Peter Almdal6Inger Hee Mabuza Mathiesen1 Daniel Faurholt-Jepsen1
Daniel Faurholt-Jepsen1- 1Cystic Fibrosis Center Copenhagen, Department of Infectious Diseases, Copenhagen University Hospital – Rigshospitalet, Copenhagen, Denmark
- 2Department of Clinical Physiology and Nuclear Medicine, Copenhagen University Hospital – Rigshospitalet, Copenhagen, Denmark
- 3Centre for Physical Activity Research, Copenhagen University Hospital – Rigshospitalet, Copenhagen, Denmark
- 4Department of Infectious Diseases, Copenhagen University Hospital – Hvidovre, Copenhagen, Denmark
- 5Department of Nutrition, Exercise and Sports, University of Copenhagen, Frederiksberg, Denmark
- 6Department of Endocrinology, Copenhagen University Hospital – Rigshospitalet, Copenhagen, Denmark
Objective: We hypothesized that the insulin-sensitizing adipokine adiponectin (ADP) is upregulated in cystic fibrosis (CF) related diabetes (CFRD) and underweight adults with CF. We aimed to assess correlations between glucose metabolism, body composition and ADP in CF.
Methods: We performed a cross-sectional study among adults with CF at the Copenhagen CF Center. The study included a fasting level of ADP, an oral glucose tolerance test (OGTT), and a dual energy-x-ray absorptiometry scan.
Results: In total, 115 patients were included of whom 104 had an OGTT performed. Glucose intolerance was not correlated with ADP in multivariable analysis, while increased hepatic insulin resistance (i.e., HOMA-IR) was correlated with reduced ADP levels. ADP declined by 4% (eβ 0.96, 95% CI: 0.94, 0.98), 5% (eβ 0.95, 95% CI: 0.93, 0.98), 9% (eβ 0.91, 95% CI: 0.87, 0.95), and 83% (eβ 0.17, 95% CI: 0.08, 0.37) for each one unit (kg/m2) increase in body mass index, fat mass index, muscle mass index, and bone mineral content index, respectively.
Conclusions: In CF, ADP was negatively correlated with hepatic insulin resistance as well as low fat, muscle, and bone mass, but not with glucose intolerance. This suggests that malnutrition leads to higher ADP levels in CF.
Introduction
The fat tissue hormone adiponectin (ADP) is predominantly produced by adipocytes and is considered an important link between fat metabolism and glucose regulation (1, 2). ADP regulates the energy homeostasis, through insulin-sensitizing effects (3), upregulation of the expenditure of stored energy and improvement of the lipid metabolism (4), and this seem to affect both the body composition and the glucose metabolism (5). Consistently, ADP was found to be negatively correlated with fat mass and fasting glucose in obese individuals and thus a higher level of ADP is thought to be related to improved glucose metabolism in healthy normal-weight adults (5).
ADP improves insulin secretion and insulin sensitivity (4, 6), meanwhile insulin is a negative regulator of ADP (7, 8). Accordingly, enhanced levels of ADP have been shown in several studies in type 1 diabetes (9, 10). This suggests that increased ADP levels seen in type 1 diabetes is a compensatory mechanism aiming at stimulating beta cell function (9), and a similar compensation may be observed in other types of pancreatogenic diabetes.
Cystic fibrosis (CF) related diabetes (CFRD) is a type of pancreatogenic diabetes characterized by decreased insulin secretion as well as low body mass index (BMI) explained by both low muscle and low fat mass (11). Hence, although type 1 diabetes and CFRD have very different pathophysiology, pancreatic insulin deficiency and hyperglycemia are present in both diseases. Therefore, ADP may also be increased in CFRD, and, in theory, elevated ADP could postpone onset of CFRD by improving both insulin secretion and insulin sensitivity. However, existing data do not fully support this theory. In two studies among adults with CF, Ziai et al. found no clear association between ADP and the total insulin secretion (12) and Hammana et al. reported no association between insulin resistance and ADP among individuals with CF (13). Thus, ADP levels might be influenced by other factors than glucose tolerance in individuals with CF.
We recently reported that individuals with CF and glucose intolerance had reduced BMI (14). Therefore, we hypothesized that the reduction in body mass can confound a potential correlation between ADP and glucose intolerance. This is further supported by Panagopoulou et al., who found that ADP was increased in individuals with a low fat free mass in a study including both individuals with and without CF (11). However, this finding might be biased, as individuals with CF seem to have higher ADP levels compared to non-CF controls (15, 16). Furthermore, no studies have shown that fat mass is negatively correlated with ADP levels in CF.
To our knowledge, existing data in CF populations have related ADP to glucose metabolism and body composition in separate studies. Hence, this supports studying ADP in relation to both glucose metabolism and body composition in the same CF population to expand the current insight in the ADP metabolism in CF. We therefore aimed to assess the association between glucose intolerance, insulin resistance and ADP as well as the associations between measures of body composition (i.e., fat mass, muscle mass, bone mass) and ADP among adults with CF in the Copenhagen CF cohort.
Methods
This study on ADP was nested in a cross-sectional study including 134 adults (≥18 years) with CF conducted at the Copenhagen CF center in 2017 prior to the new CF modulator treatment [for details (14)]. The study was approved by the Danish Ethical Committee (H-16022305) and all participants signed the consent after receiving oral and written information about the study. Demographic data, spirometry, and exocrine pancreas function data were obtained from the Danish CF database.
ADP and glucose tolerance were obtained during a standard 2-hour oral glucose tolerance test (OGTT) done during routine visits with clinically stable participants. The participants were fasted for 8 hours before the OGTT. The OGTT included venous blood (i.e., EDTA) samples collected prior, and 1 and 2 hours after intake of 75 g anhydrous glucose. The samples were centrifuged and frozen (-80°C) within 1 hour for the purpose of analyzing all samples in one batch. Fasting plasma (p) was used to assess total ADP levels quantified by duplicate enzyme linked immunosorbent assay analyses (Biovendor, Karasek, Czech Republic). P-insulin (e801 module) and p-glucose (c702 module) were analyzed using a Cobas 8000. Normal glucose tolerance status (NGT), indeterminate glucose tolerance, impaired glucose tolerance (IGT), and CFRD were classified according to the American Diabetes Association CFRD Consensus Statement (17). Homeostatic model assessment for insulin resistance (HOMA-IR) was used as a marker for hepatic insulin resistance (18, 19). Matsuda index equation was used to calculate peripheral insulin sensitivity from the three time points of the OGTT (20, 21), and the 1-hour insulin secretion rate (ISR1hour) was used as a marker of beta cell function (22). At the day of the OGTT, the C-reactive protein (CRP) (normal range: <10 mg/L) were measured (Cobas 8000, c702 module) as a marker of systemic inflammation.
Body composition was assessed by a dual energy X‐ray absorptiometry (DXA) scanner (Lunar Prodigy Pro, GE Healthcare, Madison, WI, USA). The estimates included total fat mass, muscle mass, and bone mass (bone mineral content). Equivalent to body mass index (BMI, kg/m2), all measurements (mass in kilo) were divided with squared height (m2) to obtain fat-, muscle-, and bone mineral content indices. Weight and height were measured on the day of the DXA scan.
Statistical analyses
Data were summarized as either medians (interquartile range, IQR) or counts (percentage). To assess the correlations between the measurements of glucose metabolism (glucose tolerance and insulin resistance) and ADP, linear regression models adjusted for age and sex (minimal adjusted models) and additionally adjusted for exocrine pancreas function (sufficient/insufficient), CRP, and fat mass index (multivariable models) were fitted. We used linear regression models adjusted for age and sex (minimal adjusted models) as well as linear regression models additionally adjusted for exocrine pancreas function (sufficient/insufficient) and CRP (multivariable models) to assess the correlations between measurements of body mass compartments and ADP levels. In all analyses, ADP was logarithmic transformed, and β-coefficients from the linear models were subsequently back transformed to derive the correlations as ratios. To convert the correlations to percentage reduction or increase per one unit increase of the independent variable, 1 was subtracted from the ratios and multiplied by 100. Sensitivity analyses including both fat mass index and muscle mass index or bone mineral content index were also carried out to adjust for potential confounding. Data were analyzed with R x64.
Results
The study included 115 participants, among whom all had fasted blood sampling and a DXA scan conducted and 104 (90%) also consented to an OGTT. Table 1 presents the clinical characteristics with an almost equal number of study participants in each of the four glucose tolerance groups (i.e., NGT, indeterminate glucose tolerance, IGT, and CFRD). The median [IQR] ADP level was 10.0 μg/mL [6.3-12.0 μg/mL].
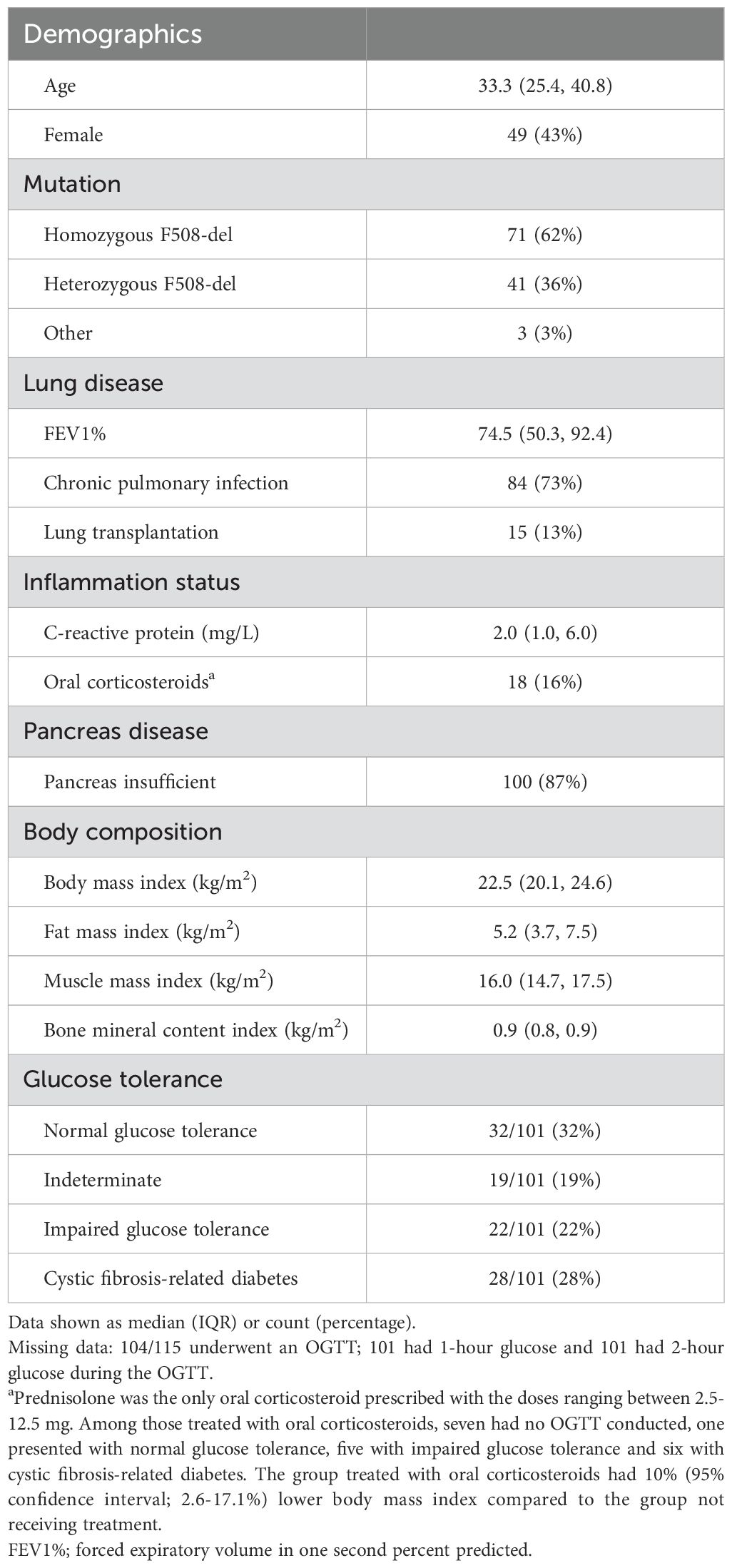
Table 1. Background characteristics of 115 adults with cystic fibrosis.
In models adjusted for age and sex, those with IGT had borderline higher ADP levels compared to NGT (eβ 1.21, 95% CI: 0.98; 1.59, p=0.078) and those with CFRD had higher ADP levels compared to NGT (eβ 1.25, 95% CI: 1.03; 1.53, p=0.026). However, in the fully adjusted models including exocrine pancreas insufficiency, CRP and fat mass index as covariates the estimates for IGT vs NGT (eβ 1.09, 95% CI: 0.85; 1.41) and CFRD vs NGT (eβ 1.14, 95% CI: 0.91; 1.44) were lower. In multivariable analyses, we found no correlation between glucose tolerance groups and ADP (Figure 1). We found no correlation between p-glucose and ADP, while higher levels of p-insulin were correlated with lower levels of ADP, with the strongest correlation seen between fasting p-insulin and ADP (Table 2). Further, insulin sensitivity (inverse HOMA-IR and Matsuda index) was correlated with higher levels of ADP, while we found no correlation between insulin secretion (ISR1hour) and ADP levels (Table 2).
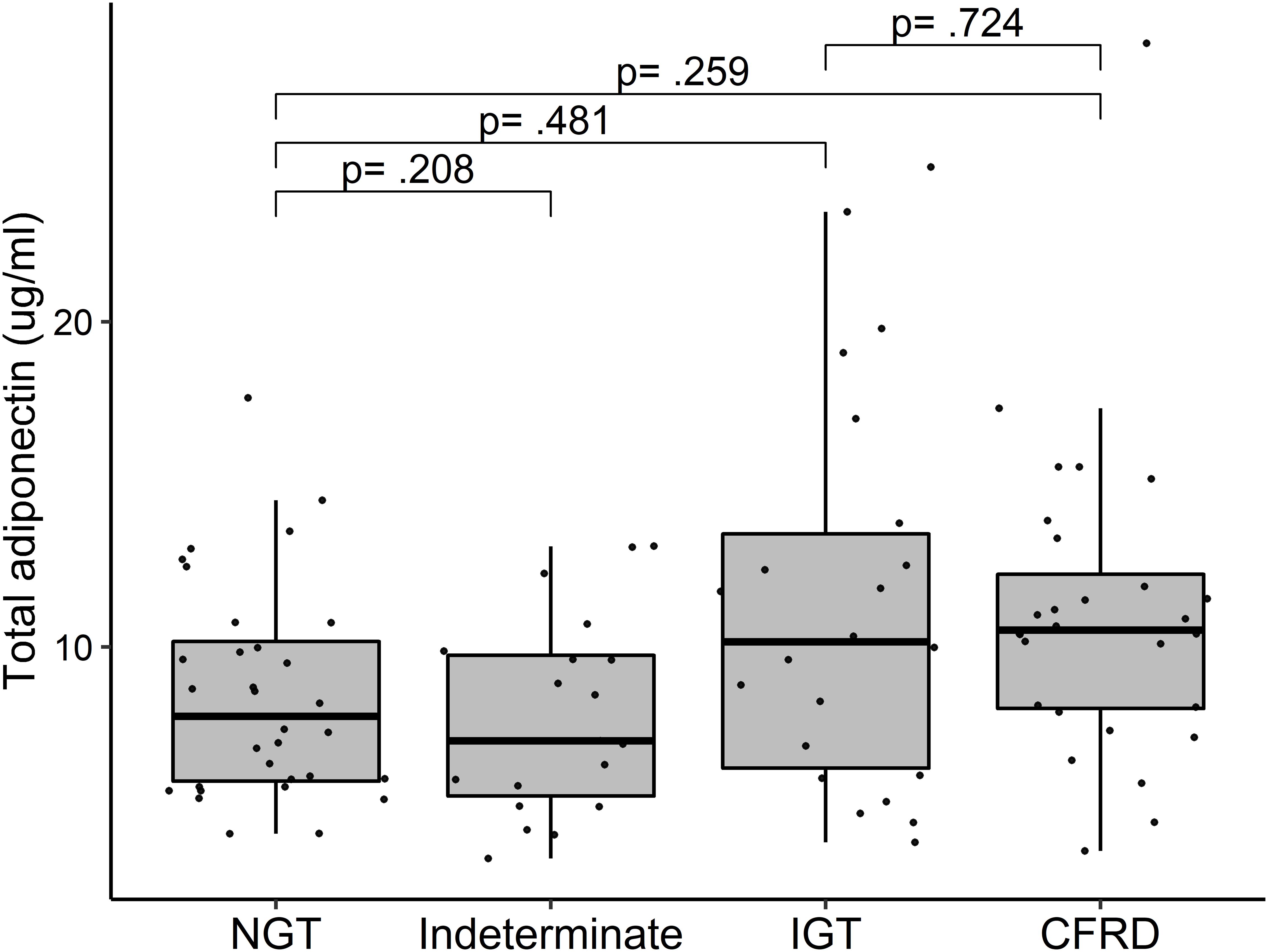
Figure 1. Adiponectin levels among 101 adults with cystic fibrosis stratified by glucose tolerance. P-values were calculated in a linear regression model with logarithmic transformed adiponectin and adjusted for age, sex, exocrine pancreas function (sufficient/insufficient), C-reactive protein and fat mass index. Missing data: Among 104 with an OGTT, glucose tolerance was assessed in 101. NGT, normal glucose tolerance; IGT, impaired glucose tolerance; CFRD, cystic fibrosis related diabetes.

Table 2. Linear regression models between measurements of glucose metabolism and adiponectin in 115 individuals with cystic fibrosis.
BMI, fat mass index, muscle mass index, and bone mineral content index were all negatively correlated with ADP in both minimal adjusted analyses and multivariable analyses indicating that for each one kg/m2 increase in BMI, fat mass index, and muscle mass index the levels of ADP decreased by 4-9% (p<0.05, Table 3). In multivariable sensitivity analyses including both fat mass index and muscle mass index, the negative correlation between fat mass index and ADP persisted although it was no longer statistically significant; ADP was 3% lower (eβ 0.97/kg/m2, 95% CI: 0.94; 1.00, p=0.078) for each one unit (kg/m2) increase in fat mass index. The correlations between muscle mass index and ADP (eβ 0.93/kg/m2, 95% CI: 0.88; 0.97, p<0.001) and between bone mineral content index and ADP (eβ 0.23/kg/m2, 95% CI: 0.10; 0.53, p<0.001) were not affected by adjustment with fat mass index.
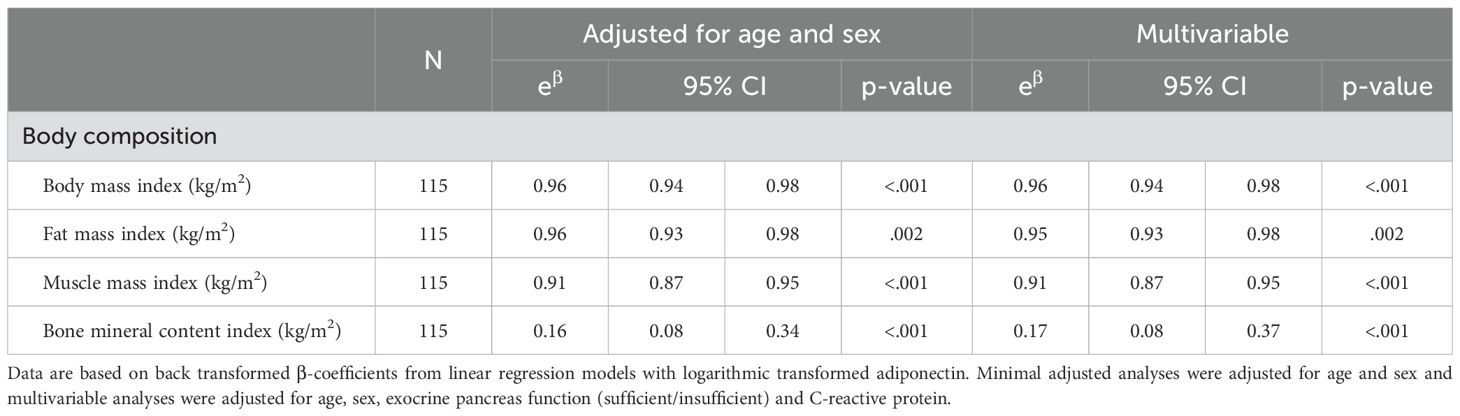
Table 3. Linear regression models between measurements of body composition and adiponectin in 115 adults with cystic fibrosis.
Discussion
In this study among adults with CF, we found that ADP levels were unrelated to p-glucose and insulin secretion rate, while ADP was inversely correlated with p-insulin levels and positively correlated with insulin sensitivity. Moreover, ADP was negatively correlated with BMI, fat mass, muscle mass, and bone mass.
Overall, severe glucose intolerance was associated with higher ADP levels, although this was partially confounded by pancreas insufficiency, inflammation, and fat mass index. Hence, the association was likely explained by fat mass rather than glucose intolerance. This is similar to previous studies in CF showing that ADP did not change with glucose tolerance status (12, 13). Likewise, we did not find any correlation between insulin secretion rate and ADP, which is also comparable to a former study in individuals with CF (12). However, we did see that the measured p-insulin levels and markers of insulin sensitivity were correlated with ADP and not affected by adjustment with fat mass. HOMA-IR, usually considered a marker of hepatic insulin resistance (23), seemed to be stronger linked to levels of ADP compared to the Matsuda index, which is a better marker of peripheral insulin sensitivity (24). Yet, CF liver disease does not seem to explain the inverse correlation between hepatic insulin resistance and ADP, as CF liver disease has been linked to elevated levels of ADP in CF (11). In other words, ADP is unlikely to explain the link between CF liver disease and glucose intolerance (25) as well as the relationship between reduced insulin sensitivity and CFRD (26). This indicates that CFRD should be differentiated from non-alcoholic fatty liver disease and type 2 diabetes and treatments targeting these diseases should therefore not be used as CFRD management in lean individuals without thorough evaluation.
We also found that all measures and compartments of body mass were negatively correlated with ADP, which is in line with a recent CF study from Qatar (27), but in contrast with a previous CF study from Canada, which reported no correlation between BMI and ADP (13). However, it is not clear from the previous study whether the model was adjusted for sex and age, which is important, since cofactors such as female sex (13) and increasing age (28) are correlated with increased levels of ADP. Further, we showed that fat mass index was negatively correlated with ADP, which seems to be in contrast to a study by Panagopoulou et al., who found a positive association between body fat percentage and ADP (11). However, their study included non-CF controls, thus our study design is not comparable to their study design and differences should be interpreted with caution. Although our findings deviated from previous studies in CF, we found similar trends as is known from several non-CF studies reporting negative associations between fat mass and ADP (29–31). Furthermore, we found increased muscle mass to be correlated with low ADP, unrelated to the fat mass. This is in line with data from Polito et al., who demonstrated that frequent physical exercise lead to lower levels of ADP (15). Similarly, in a non-CF study among individuals with a high prevalence of sarcopenia, both muscle mass index and muscle strength were negatively correlated with ADP (32). This highlights that though ADP levels are strongly connected to body composition and most likely plays important regulatory roles in CF metabolism, ADP appears to be less valuable for evaluating nutritional status in clinical settings.
Following the introduction of new highly effective modulator therapy in the CF population, real-life studies have found significant increases in body mass (33). This change is likely to lead to a reduction in ADP, potentially worsening hepatic insulin sensitivity. Although, hepatic insulin sensitivity does not appear to be the cause of CFRD, it could further complicate disease severity and management. This suggests that incretin-based therapies may play a role in CFRD treatment in near future, as this class of drug seems to enhance ADP levels during treatment (34). However, such interventions should be watchfully introduced, as the current literature provides little knowledge about what role adiponectin plays in pulmonary inflammation and lung function deterioration, and increasing ADP may therefore have both protective (35) or harmful effects on lung function (27).
Finally, we did see that lower bone mass was correlated with higher ADP levels. Although CF bone disease and osteoporosis are common and the results mimic data from individuals with anorexia nervosa, where osteoporosis was linked to higher ADP levels (36), these data should be interpreted with caution. If any true association do exist between bone mass and ADP, we speculate that ADP could stimulate osteoclast formation and thus reduce bone mass, as has been seen in in vitro studies (37). Even so, as individuals with CF are often malnourished, reduced fat and muscle mass might lead to increased ADP as well as a subsequent loss of bone mass and thus correlations between bone and ADP might be a chance finding due to the impact from other body compartments, which strongly correlate with bone mass.
As ADP may have a role as an anti-inflammatory agent (3), chronic inflammation could have been correlated with lower levels of ADP in CF (16). However, we found no impact from inflammation in our study as adjusting for CRP did not affect the correlations between body mass and ADP, and the CRP was generally low, and participants were clinically stable without signs of pulmonary exacerbations. At the same time, a limitation in this study is that we only measured total ADP without assessing the high molecular weight isoform, a sub-component of ADP suggested to be a superior marker of insulin sensitivity (38). Moreover, despite the adjustment for fat mass, the results could still be partly confounded by the effect of fat mass, as fasting insulin, HOMA-IR, muscle, and bone mass are all positively correlated with fat mass and difficult to separate completely. Lastly, as this was a cross-sectional study, all mentioning of causal relations are speculative.
Conclusions
Among adults with CF, we found no correlation between glucose tolerance and ADP, although insulin sensitivity was correlated with higher levels of ADP. Moreover, we found that all measures of body composition were negatively correlated with ADP similar to non-CF populations. This suggests that malnutrition irrespective of CF is associated with higher ADP levels and with increasing body weight after the new highly effective modulator therapy, factors such as fat mass, ADP levels and hepatic insulin sensitivity may become more important in the development of glucose intolerance in CF.
Data availability statement
Qualified researchers can request access to patient-level data after publication, including analytic code. Patient-level data will be anonymized to protect the privacy of the participants. Proposals should be directed to the corresponding author to gain access. Requests can be made after publication and until 5 years following article publication. Requests to access the datasets should be directed to Bibi Uhre Nielsen,YmliaS51aHJlLm5pZWxzZW4uMDFAcmVnaW9uaC5kaw==.
Ethics statement
The studies involving humans were approved by The Danish Ethical Committee, Capital Region (H-16022305). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
BN: Conceptualization, Formal Analysis, Visualization, Writing – original draft, Writing – review & editing. CM: Conceptualization, Writing – original draft, Writing – review & editing, Data curation. PO: Methodology, Writing – original draft, Writing – review & editing. RK-M: Writing – original draft, Writing – review & editing. TK: Writing – original draft, Writing – review & editing. CR: Formal Analysis, Writing – original draft, Writing – review & editing. TP: Writing – original draft, Writing – review & editing. TA: Conceptualization, Writing – original draft, Writing – review & editing. IM: Conceptualization, Writing – original draft, Writing – review & editing. DF-J: Conceptualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was supported by the Danish Cystic Fibrosis Foundation (CRM) (www.cystiskfibrose.dk); and Torkild Steenbecks Legat. The funders had no role in study design, data collection, data analysis, interpretation of data, writing the manuscript or decision to publish.
Conflict of interest
TA holds stocks in Novo-Nordisk A/S.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
CF, Cystic fibrosis; ADP, adiponectin; CFRD, cystic fibrosis related diabetes;OGTT, oral glucose tolerance test; NGT, normal glucose tolerance; IGT, impaired glucose tolerance; HOMA-IR, Homeostatic model assessment for insulin resistance;ISR1hour, 1-hour insulin secretion rate; CRP, C-reactive protein; DXA, dual energy X‐ray absorptiometry; BMI, body mass index.
References
1. Ghoshal K, Chatterjee T, Chowdhury S, Sengupta S, Bhattacharyya M. Adiponectin genetic variant and expression coupled with lipid peroxidation reveal new signatures in diabetic dyslipidemia. Biochem Genet. (2021) 59:781–98. doi: 10.1007/s10528-021-10030-5
2. Ghoshal K. Adiponectin: Probe of the molecular paradigm associating diabetes and obesity. World J Diabetes. (2015) 6:151. doi: 10.4239/wjd.v6.i1.151
3. Wang Y, Ma XL, Lau WB. Cardiovascular adiponectin resistance: the critical role of adiponectin receptor modification. Trends Endocrinol Metab NIH Public Access;. (2017) 28:519–30. doi: 10.1016/j.tem.2017.03.004
4. Achari AE, Jain SK. Adiponectin, a therapeutic target for obesity, diabetes, and endothelial dysfunction. Int J Mol Sci. (2017) 18:1321. doi: 10.3390/ijms18061321
5. Yang WS, Lee WJ, Funahashi T, Tanaka S, Matsuzawa Y, Chao CL, et al. Weight reduction increases plasma levels of an adipose-derived anti-inflammatory protein, adiponectin. J Clin Endocrinol Metab. (2001) 86:3815–9. doi: 10.1210/jcem.86.8.7741
6. Okamoto M, Ohara-Imaizumi M, Kubota N, Hashimoto S, Eto K, Kanno T, et al. Adiponectin induces insulin secretion in vitro and in vivo at a low glucose concentration. Diabetologia. (2008) 51:827–35. doi: 10.1007/s00125-008-0944-9
7. Fasshauer M, Neumann S, Eszlinger M, Paschke R, Klein J. Hormonal regulation of adiponectin gene expression in 3T3-L1 adipocytes. Biochem Biophys Res Commun. (2002) 290:1084–9. doi: 10.1006/bbrc.2001.6307
8. Blüher M, Michael MD, Peroni OD, Ueki K, Carter N, Kahn BB, et al. Adipose tissue selective insulin receptor knockout protects against obesity and obesity-related glucose intolerance. Dev Cell. (2002) 3:25–38. doi: 10.1016/S1534-5807(02)00199-5
9. Leth H, Andersen KK, Frystyk J, Tarnow L, Rossing P, Parving HH, et al. Elevated levels of high-molecular-weight adiponectin in type 1 diabetes. J Clin Endocrinol Metab. (2008) 93:3186–91. doi: 10.1210/jc.2008-0360
10. Pereira RI, Snell-Bergeon JK, Erickson C, Schauer IE, Bergman BC, Rewers M, et al. Adiponectin dysregulation and insulin resistance in type 1 diabetes. J Clin Endocrinol Metab. (2012) 97:E642. doi: 10.1210/jc.2011-2542
11. Panagopoulou P, Fotoulaki M, Manolitsas A, Pavlitou-Tsiontsi E, Tsitouridis I, Nousia-Arvanitakis S. Adiponectin and body composition in cystic fibrosis. J Cyst Fibros. (2008) 7:244–51. doi: 10.1016/j.jcf.2007.10.003
12. Ziai S, Elisha B, Hammana I, Tardif A, Berthiaume Y, Coderre L, et al. Normal total and high molecular weight adiponectin levels in adults with cystic fibrosis. J Cyst Fibros. (2011) 10:483–6. doi: 10.1016/j.jcf.2011.07.005
13. Hammana I, Malet A, Costa M, Brochiero E, Berthiaume Y, Potvin S, et al. Normal adiponectin levels despite abnormal glucose tolerance (or diabetes) and inflammation in adult patients with cystic fibrosis. Diabetes Metab. (2007) 33:213–9. doi: 10.1016/j.diabet.2007.01.004
14. Nielsen BU, Faurholt-Jepsen D, Oturai PS, Qvist T, Krogh-Madsen R, Katzenstein TL, et al. Associations between glucose tolerance, insulin secretion, muscle and fat mass in cystic fibrosis. Clin Med Insights Endocrinol Diabetes. (2021) 14:117955142110382. doi: 10.1177/11795514211038259
15. Polito R, Nigro E, Elce A, Monaco ML, Iacotucci P, Carnovale V, et al. Adiponectin expression is modulated by long-term physical activity in adult patients affected by cystic fibrosis. Mediators Inflammation. (2019) 2019:1–7. doi: 10.1155/2019/2153934
16. Moriconi N, Kraenzlin M, Müller B, Keller U, Nusbaumer CPG, Stöhr S, et al. Body composition and adiponectin serum concentrations in adult patients with cystic fibrosis. J Clin Endocrinol Metab. (2006) 91:1586–90. doi: 10.1210/jc.2005-2135
17. Moran A, Brunzell C, Cohen RC, Katz M, Marshall BC, Onady G, et al. Clinical care guidelines for cystic fibrosis-related diabetes: A position statement of the American Diabetes Association and a clinical practice guideline of the Cystic Fibrosis Foundation, endorsed by the Pediatric Endocrine Society. Diabetes Care. (2010) 33:2697–708. doi: 10.2337/dc10-1768
18. Matsuda M, DeFronzo RA. Insulin sensitivity indices obtained from oral glucose tolerance testing: Comparison with the euglycemic insulin clamp. Diabetes Care. (1999) 22:1462–70. doi: 10.2337/diacare.22.9.1462
19. Haffner SM, Kennedy E, Gonzalez C, Stern MP, Miettinen H. A prospective analysis of the HOMA model: The Mexico City Diabetes Study. Diabetes Care. (1996) 19:1138–41. doi: 10.2337/diacare.19.10.1138
20. Matsuda M, Defronzo RA. Study on Index for Insulin Sensitivity (2021). Available online at: http://mmatsuda.diabetes-smc.jp/english.html. (accessed February 09, 2021).
21. DeFronzo RA, Matsuda M. Reduced time points to calculate the composite index. Diabetes Care. (2010) 33:2010. doi: 10.2337/dc10-0646
22. Hammana I, Potvin S, Tardif A, Berthiaume Y, Coderre L, Rabasa-Lhoret R. Validation of insulin secretion indices in cystic fibrosis patients. J Cyst Fibros. (2009) 8:378–81. doi: 10.1016/j.jcf.2009.08.007
23. Wallace TM, Levy JC, Matthews DR. Use and abuse of HOMA modeling. Diabetes Care. (2004) 27:1487–95. doi: 10.2337/diacare.27.6.1487
24. Gutch M, Kumar S, Razi SM, Gupta K, Gupta A. Assessment of insulin sensitivity/resistance. Indian J Endocrinol Metab. (2015) 19:160–4. doi: 10.4103/2230-8210.146874
25. Marshall BC, Butler SM, Stoddard M, Moran AM, Liou TG, Morgan WJ. Epidemiology of cystic fibrosis-related diabetes. J Pediatr. (2005) 146:681–7. doi: 10.1016/j.jpeds.2004.12.039
26. Colomba J, Boudreau V, Lehoux-Dubois C, Desjardins K, Coriati A, Tremblay F, et al. The main mechanism associated with progression of glucose intolerance in older patients with cystic fibrosis is insulin resistance and not reduced insulin secretion capacity. J Cyst Fibros. (2019) 18:551–6. doi: 10.1016/j.jcf.2019.01.009
27. AbdulWahab A, Allangawi M, Thomas M, Bettahi I, Sivaraman SK, Jerobin J, et al. Sputum and plasma adiponectin levels in clinically stable adult cystic fibrosis patients with CFTR I1234V mutation. Transl Med Commun. (2020) 5:1–7. doi: 10.1186/s41231-020-00053-2
28. Obata Y, Yamada Y, Takahi Y, Baden MY, Saisho K, Tamba S, et al. Relationship between serum adiponectin levels and age in healthy subjects and patients with type 2 diabetes. Clin Endocrinol (Oxf). (2013) 79:204–10. doi: 10.1111/cen.2013.79.issue-2
29. De Rosa A, Ludovica Monaco M, Capasso M, Forestieri P, Pilone V, Nardelli C, et al. Adiponectin oligomers as potential indicators of adipose tissue improvement in obese subjects. Eur J Endocrinol. (2013) 169:37–43. doi: 10.1530/EJE-12-1039
30. Meyer LK, Ciaraldi TP, Henry RR, Wittgrove AC, Phillips SA. Adipose tissue depot and cell size dependency of adiponectin synthesis and secretion in human obesity. Adipocyte. (2013) 2:217–26. doi: 10.4161/adip.24953
31. Kaser S, Tatarczyk T, Stadlmayr A, Ciardi C, Ress C, Tschoner A, et al. Effect of obesity and insulin sensitivity on adiponectin isoform distribution. Eur J Clin Invest. (2008) 38:827–34. doi: 10.1111/j.1365-2362.2008.02028.x
32. Harada H, Kai H, Shibata R, Niiyama H, Nishiyama Y, Murohara T, et al. New diagnostic index for sarcopenia in patients with cardiovascular diseases. PloS One. (2017) 12:e0178123. doi: 10.1371/journal.pone.0178123
33. Bower JK, Volkova N, Ahluwalia N, Sahota G, Xuan F, Chin A, et al. Real-world safety and effectiveness of elexacaftor/tezacaftor/ivacaftor in people with cystic fibrosis: Interim results of a long-term registry-based study. J Cyst Fibros. (2023) 22:730–7. doi: 10.1016/j.jcf.2023.03.002
34. Yaribeygi H, Maleki M, Atkin SL, Jamialahmadi T, Sahebkar A. Impact of incretin-based therapies on adipokines and adiponectin. J Diabetes Res. (2021) 2021:1–9. doi: 10.1155/2021/1815178
35. Garcia P, Sood A. Adiponectin in pulmonary disease and critically ill patients. Curr Med Chem. (2012) 19:5493–500. doi: 10.2174/092986712803833263
36. Legroux-Gérot I, Vignau J, Viltart O, Hardouin P, Chauveau C, Cortet B. Adipokines and bone status in a cohort of anorexic patients. Jt Bone Spine. (2019) 86:95–101. doi: 10.1016/j.jbspin.2018.03.014
37. Luo XH, Guo LJ, Xie H, Yuan LQ, Wu XP, Zhou H, et al. Adiponectin stimulates RANKL and inhibits OPG expression in human osteoblasts through the MAPK signaling pathway. J Bone Miner Res. (2006) 21:1648–56. doi: 10.1359/jbmr.060707
Keywords: cystic fibrosis, adiponectin, fat mass, muscle mass, bone mass
Citation: Nielsen BU, Mikkelsen CR, Oturai PS, Krogh-Madsen R, Katzenstein TL, Ritz C, Pressler T, Almdal TP, Mathiesen IHM and Faurholt-Jepsen D (2024) A cross-sectional study in adiponectin, glucose metabolism, and body composition in cystic fibrosis. Front. Endocrinol. 15:1382241. doi: 10.3389/fendo.2024.1382241
Received: 05 February 2024; Accepted: 07 October 2024;
Published: 28 October 2024.
Edited by:
Guy A. Rutter, Imperial College London, United KingdomReviewed by:
Valeria Grancini, Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico, ItalyKakali Ghoshal, Vanderbilt University Medical Center, United States
Copyright © 2024 Nielsen, Mikkelsen, Oturai, Krogh-Madsen, Katzenstein, Ritz, Pressler, Almdal, Mathiesen and Faurholt-Jepsen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bibi Uhre Nielsen, YmliaS51aHJlLm5pZWxzZW4uMDFAcmVnaW9uaC5kaw==
†These authors have contributed equally to this work