 Okti Sri Purwanti
Okti Sri Purwanti Nursalam Nursalam
Nursalam Nursalam Moses Glorino Rumambo Pandin
Moses Glorino Rumambo Pandin- 1Department of Advanced Nursing, Faculty of Nursing, Universitas Airlangga, Surabaya, Indonesia
- 2Department of Nursing, Faculty of Health Science, Universitas Muhammadiyah Surakarta, Surakarta, Indonesia
- 3English Department, Faculty of Humanities, Universitas Airlangga, Surabaya, Indonesia
Introduction: Uncontrolled blood sugar levels may result in complications, namely diabetic neuropathy. Diabetic neuropathy is a nerve disorder that causes symptoms of numbness, foot deformity, dry skin, and thickening of the feet. The severity of diabetic neuropathy carries the risk of developing diabetic ulcers and amputation. Early detection of diabetic neuropathy can prevent the risk of diabetic ulcers. The purpose: to identify early detection of diabetic neuropathy based on the health belief model.
Method: This research searched for articles in 6 databases via Scopus, Ebsco, Pubmed, Sage journal, Science Direct, and SpringerLink with the keywords “screening Neuropathy” AND “Detection Neuropathy” AND “Scoring Neuropathy” AND “Diabetic” published in 2019-2023. In this study, articles were identified based on PICO analysis. Researchers used rayyan.AI in the literature selection process and PRISMA Flow-Chart 2020 to record the article filtering process. To identify the risk of bias, researchers used the JBI checklist for diagnostic test accuracy.
Results: This research identified articles through PRISMA Flow-Chart 2020, obtaining 20 articles that discussed early detection of diabetic neuropathy.
Conclusion: This review reports on the importance of early detection of neuropathy for diagnosing neuropathy and determining appropriate management. Neuropathy patients who receive appropriate treatment can prevent the occurrence of diabetic ulcers. The most frequently used neuropathy instruments are the vibration perception threshold (VPT) and questionnaire Michigan Neuropathy Screening Instrument (MNSI). Health workers can combine neuropathy instruments to accurately diagnose neuropathy.
Introduction
Diabetes mellitus may cause neuropathy, retinopathy, and nephrotic complications. The increase in the number of diabetes mellitus cases that occur if not managed properly can cause complications, some complications that occur in diabetes mellitus sufferers that occur can significantly affect the decline in the quality of life of diabetes patients so that low quality of life can affect the physical and mental well-being of diabetes patients (1). On the other hand, diabetes mellitus over a long period may be a factor that worsens the condition of heart failure patients (2). For diabetes mellitus patients, diabetic neuropathy is the most common complication in type 2 diabetes mellitus patients. Diabetic neuropathy results in decreased function of the sensory (decreased sensitivity), motor (deformity), and autonomic (callus) nerves (3). The majority of diabetics experience small wounds on the feet that lose sensitivity and develop into diabetic ulcers. Diabetic ulcers can cause infection and foot amputation (4). The health belief model estimates patient attitudes in preventing diabetic neuropathy. The health belief model includes vulnerability, benefits, obstacles, the seriousness of illness, and support received (5).
The incidence of neuropathy in the world reaches 2.4% of the human population, and the prevalence of neuropathy cases increases in old age by 8.0%. Globally, the highest prevalence of neuropathy occurs in the Asian continent. A higher incidence of neuropathy can be found in countries on the Southeast Asian continent, namely Malaysia (54.3%), the Philippines (58.0%) and Indonesia (58.0%) (6). A study showed that 50% of patients aged > 60 years experience neuropathy in the early stages of type 2 diabetes (7). Diabetic who experience complications from diabetic neuropathy in Indonesia reach 54% (8).
Early detection of neuropathy is to establish an early diagnosis of neuropathy and determine patient care. Proper treatment for neuropathy patients can prevent diabetic ulcers (9). Nurses can carry out early detection of neuropathy using neuropathy instruments before the emergence of neuropathy symptoms. Patients who are aware of the signs of neuropathy and carry out appropriate foot care can prevent diabetic ulcers (10). In fact, patients are willing to undergo a neuropathy examination if the patient feels the severity of neuropathy symptoms. Health workers make a diagnosis of neuropathy after clinical signs of neuropathy appear (11).
Based on the explanation above, early detection of neuropathy is carried out to confirm the diagnosis and prevent diabetic ulcers. This research aimed to determine early detection of diabetic neuropathy based on the health belief model.
Methodology
This research used a scoping review approach. The initial stage of this research was identifying problems based on existing phenomena. Next, the researcher determined inclusion and exclusion criteria in literature screening. The researcher compiled the final results based on the literature included in the screening process. Researchers used the PRISMA Flow chart 2020 diagram to document the literature selection process. Researchers conducted literature searches based on 6 databases, namely PubMed, Scopus, Science Direct, Sage Journal, Ebsco and SpringerLink. At the literature search stage, researchers used a combination of the keywords “Screening Neuropathy” AND “Detection Neuropathy” AND “Scoring Neuropathy” AND “Diabetic” in literature published in the last 5 years (2019-2023). Based on the results of the literature search, the researcher downloaded the articles and carried out filtering. Researchers excluded review articles, letters to the editor, subchapters from books, and articles that were incomplete. Researchers carried out literature screening analysis that was explained in the inclusion and exclusion criteria. The literature selection process used Rayyan. AI by inputting literature search results on the website. In the initial stage of literature selection, researchers remove duplicate literature that was detected. Next, select articles based on title, abstract, full text. Documentation of the literature selection process using the PRISMA Flow chart 2020 diagram in Figure 1. Data extraction based on the results of the literature selection, the researcher carried out data extraction including the following: 1. Author and year, 2. Study design, 3. Sample, 4. Variables, 5. Instrument, 6. Intervention, 7. Analysis, 8. Results. Researchers recorded all instruments used in early examination of diabetic neuropathy. The risk of bias assessment in this review uses a critical appraisal checklist that is available from the Joanna Brings Institute (JBI). Researchers used the JBI diagnostic test accuracy checklist to assess the risk of bias across the literature. The JBI diagnostic test accuracy checklist can be used in literature assessments with cross-sectional and case study research designs. Risk bias if an assessment of ≥50% is considered to meet critical assessment criteria (12). The risk of bias results can be seen in Table 1.
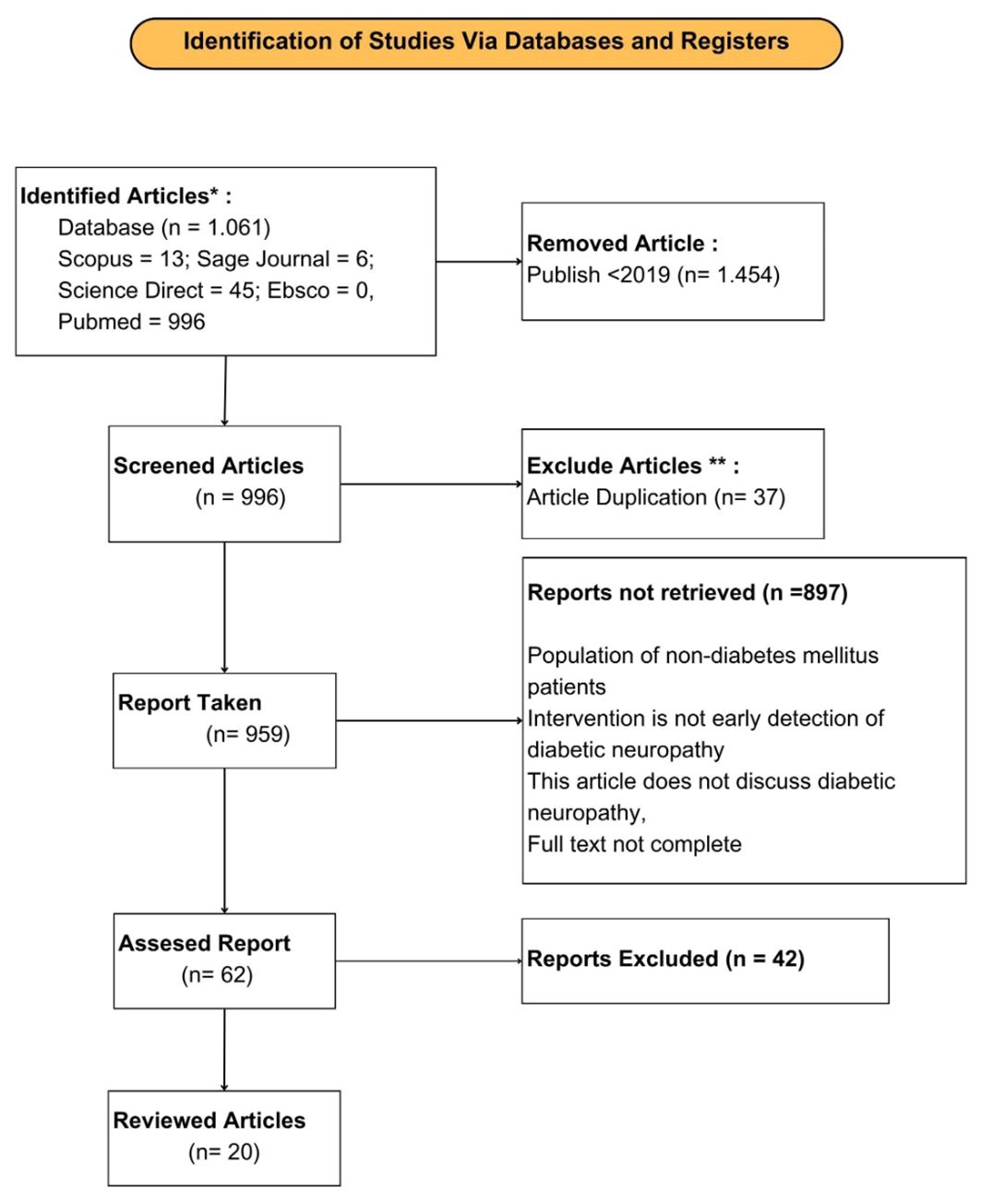
Figure 1 PRISMA flow chart 2020 diagram.
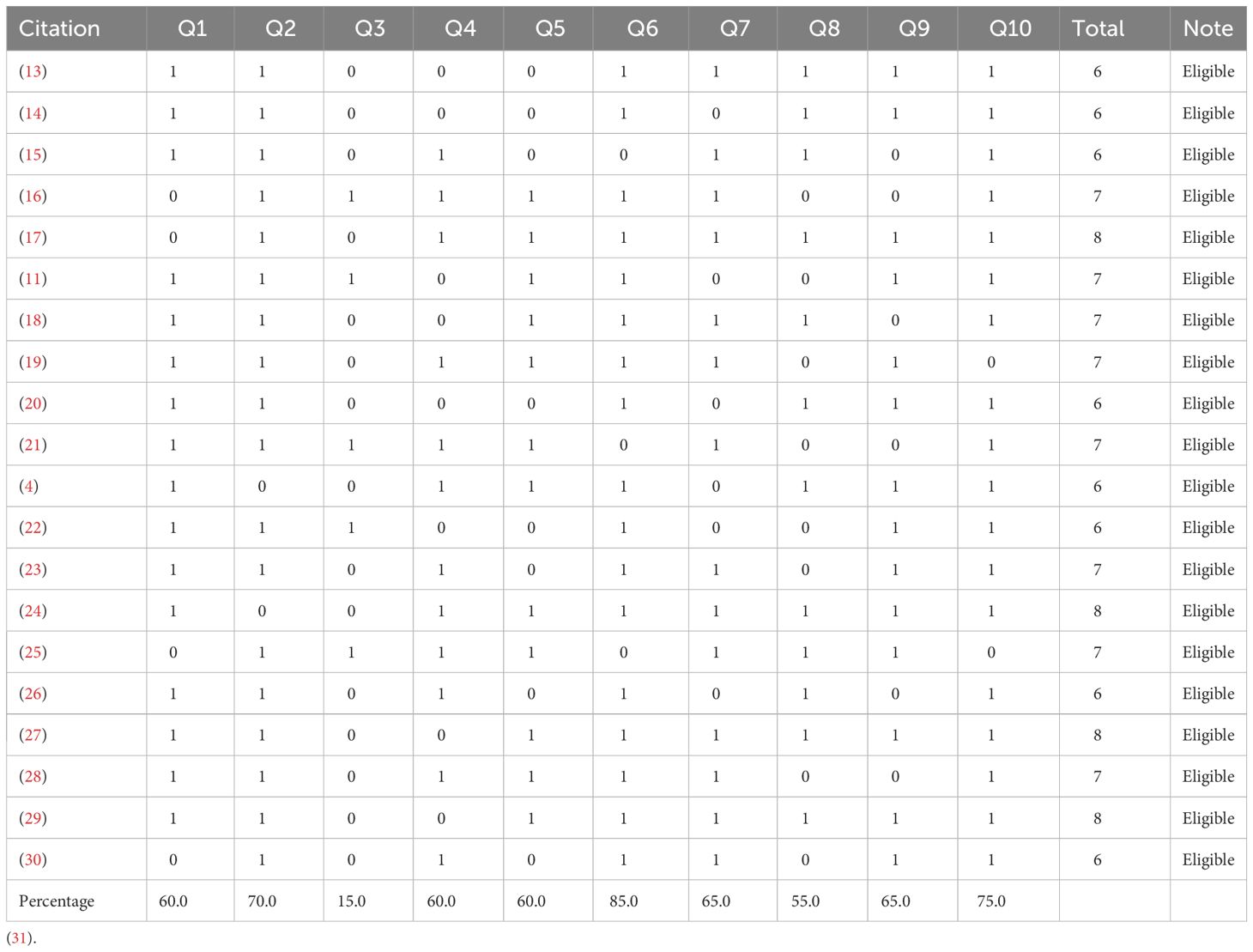
Table 1 Critical appraisal of eligible diagnostic test accuracy.
Results
In this study, there were 1,061 pieces of literature that were included in the screening process. The researcher identified duplicate literature and removed them. Next, the literature was selected based analysis to obtain the final results of the literature to be reviewed. Based on the results of the selection of literature included in this review, there were 20 pieces of literature. The literature research design was divided into 2 types, namely 18 literatures with a cross sectional study design and 2 literatures with a case control study design. The results of the selection of literature to be reviewed can be seen in the PRISMA Flow Chart 2020 diagram at Figure 1 (32).
Based on the final results of the literature screening, showed that early detection of neuropathy can be done using several methods that will be described as follows Tables 2, 3.
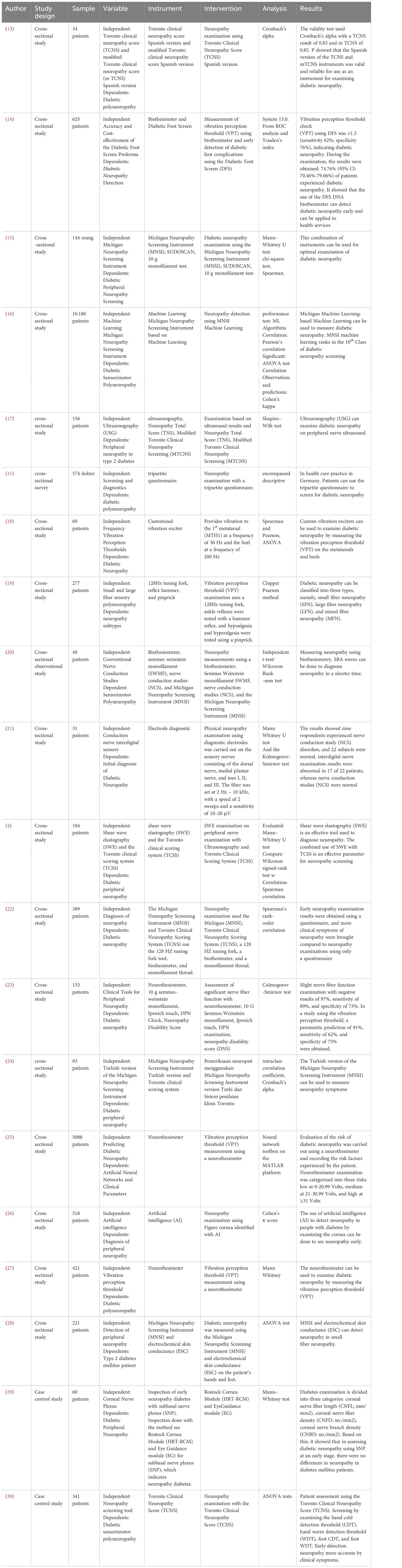
Table 2 Journal review.

Table 3 Neuropathy detection based on review.
Discussion
The final results of this review were 20 pieces of literature that discussed early detection of neuropathy in diabetes patients. Researchers used diabetic neuropathy instruments to carry out early detection of neuropathy. Of the 20 literatures, there were 20 literatures that showed good results in diabetic neuropathy examination. The results of JBI’s critical appraisal risk of bias, show that the journals included in this research meet the critical appraisal requirements with an assessment reaching ≥50%. However, in question 3, the assessment was <50%, 3 studies did not include exclusions for samples included in the study, and 3 articles excluded samples because the sample data was empty.
Diabetes Mellitus is a very important health problem in society, the incidence and number of cases of Diabetes Mellitus sufferers has always increased over the past few years (34, 35). Diabetes Mellitus (DM) or diabetes is a heterogeneous group of disorders with typical signs of increased blood glucose levels or hyperglycemia (36). Diabetic patients experience blood glucose resistance for a long time resulting in neuropathy complications. Prolonged high blood glucose levels will result in damage to the blood vessels walls (37). In this condition, the patient’s body cannot use the glucose in the blood to convert it into energy due to the accumulation of glucose in the blood (38). Neuropathy may cause damage to sensory, motor, and autonomic nerves. The clinical symptoms felt by diabetes patients are based on the damaged nerves, for example motor neuropathy (deformity), sensory neuropathy (decreased sensitivity), and autonomic neuropathy (callus). To confirm the diagnosis of neuropathy, health workers can carry out early detection of neuropathy (3).
Delay in early diagnosis of neuropathy may cause the severity of neuropathy and development of diabetic ulcers. The length of time a person living with diabetes can provide an idea of the course of the disease and also the person’s severity (37). Examination results showed severe neuropathy identify the risk of diabetic ulcers (39). Patients suffering from neuropathy will experience decrease in quality of life because they experience symptoms of neuropathy such as pain, deformity and callus (3).
Diabetic neuropathy examination can be carried out using instruments that are available in health services. However, most neuropathy instruments can only detect after the patient has symptoms of neuropathy. For instance, monofilament instruments can detect neuropathy that has decreased sensitivity in the feet (40), the MNSI questionnaire can identify neuropathy based on signs of neuropathy symptoms felt by diabetics (41).
Vibration perception threshold (VPT): there are 7 studies using different instruments in the vibration perception threshold measurement method, namely biotesimeter (14, 20), neurotesimeter (23) (25) (27), (18) vibratip, 128 Hz tuning fork (19). During the VPT examination, researchers provided vibrations at certain points to detect vibration sensations in the feet of diabetic patients. The vibration range given during the VPT examination was from 1-50V with the result categories being mild neuropathy, moderate neuropathy and severe neuropathy.
Michigan neuropathy screening instrument (MNSI): there are 7 studies using the MNSI in early screening for diabetic neuropathy. The MNSI questionnaire consists of 11 questions regarding signs and symptoms of neuropathy in diabetes mellitus patients. Researchers have developed the MNSI questionnaire, there is a research that has developed the MNSI in the form of machine learning, the MNSI is available in various versions such as the Turkish version of the MNSI (33).
Toronto clinical neuropathy score (TCNS): there are 7 studies that use TCNS in the examination of diabetic neuropathy. Researchers translated the TCNS into Spanish (13). In another study, TCNS was modified into the modified Toronto clinical neuropathy score (m-TCNS) instrument (m-TCNS) (17).
Other examinations: Diabetic neuropathy examination, apart from using the above instruments, can also use ultrasonography (USG), tripartite questionnaire, electrode diagnostic, shear wave elastography artificial neural network and artificial intelligence, cornea module. The results based on neuropathy examination using this instrument were normal and neuropathic. However, this instrument is rarely used in health services.
The research used a combination of early detection methods for neuropathy: other research used a combination of the early detection instruments mentioned above and combined using other instruments such as monofilament, sudoscan, electrochemical skin conductance, Ipswich touch, neuropathy disability score and Hammer reflex. Instruments for early detection of neuropathy in each study can also be seen in detail in Table 2.
Over time, many researchers have developed instruments for early detection of diabetic neuropathy. The development of this instrument can make it easier for health workers to detect neuropathy early and determine appropriate treatment so as to prevent the occurrence of diabetic ulcers. For example, researchers translated the Turkish version of the MNSI questionnaire so that it can be used by Turkish health workers in detecting neuropathy (24). Based on existing research, examination of diabetic neuropathy can use artificial intelligence instruments by looking at images of the cornea in diabetes mellitus patients (26).
The results of the diabetic neuropathy examination are stated to be in accordance with the instrument used. There is an instrument that describes the results of neuropathy with 3 classifications, namely mild neuropathy, moderate neuropathy and severe neuropathy (41). Furthermore, there are instruments that identify neuropathy with normal results and neuropathy. Health workers can combine instruments for early detection of neuropathy so that examination results are more accurate (42).
A study using the Toronto Clinical Neuropathy Score (TCNS), hand cold Detection Threshold (CDT), Hand Warm Detection Threshold (WDT), Foot CDT, and Foot WDT instruments in diagnosing neuropathy did not show accurate results. Early diagnosis of neuropathy is more accurate through the patient’s clinical symptoms. Based on this, the doctor confirms the diagnosis of neuropathy after the patient feels clinical symptoms (30).
Neuropathy examination in diabetes patients using an early neuropathy detection tool. Various neuropathy screening tools are available with different assessment methods. The neuropathy questionnaire instrument detects neuropathy through clinical symptoms. Questionnaire questions cover patient symptoms such as pain, deformity, and decreased sensitivity. Physical examination of neuropathy using a monofilament instrument and a tuning fork.
Based on the articles included in this study, it discusses the sensitivity and specificity of neuropathy instruments. The sensitivity and specificity of the instrument show the accuracy of the instrument in diagnosing neuropathy. Validity measurements in articles use different methods including validity tests using Cronbach’s alpha and ROC/AUC assessments. We found vibration perception threshold examination (biothesimener/neurothesimeter/vibratip) is the most frequently used physical examination instrument for neuropathy detection with a sensitivity value of 62%; and specificity of 76%). Vibrations of 1-50V are given to the patient’s feet at several examination points, indicating neuropathy if they feel vibrations ≥25V and no neuropathy if they feel <25V. The vibration perception threshold instrument has become the gold standard for detecting neuropathy and ulcer risk (14).
Apart from physical examination instruments using the vibration perception threshold, the MNSI questionnaire is also the most frequently used in the early detection of neuropathy. This questionnaire consists of 15 questions regarding neuropathy symptoms with the results identifying neuropathy into 3 categories, namely low, moderate, and severe (15). Several studies combine the MNSI questionnaire with physical examination tools such as monofilaments and tuning forks. The MNSI questionnaire has been adapted and translated into various languages including Indonesian, Arabic, and Thai.
Meanwhile, neuropathy instruments such as the Toronto Clinical Neuropathy Score (TCNS, ultrasonography (USG), tripartite questionnaire, diagnostic electrodes, artificial neural network shear wave elastography, and artificial intelligence, cornea modules are still rarely used in diabetic neuropathy examination. Research also combines instruments of Early detection to get accurate results.
Conclusion
This review reports on the importance of early detection of neuropathy for diagnosing neuropathy and determining appropriate management. Neuropathy patients who receive appropriate treatment can prevent the occurrence of diabetic ulcers. The most frequently used neuropathy instruments are the vibration perception threshold (VPT) and questionnaire Michigan Neuropathy Screening Instrument (MNSI). Health workers can combine neuropathy instruments to accurately diagnose neuropathy.
Author contributions
OP: Conceptualization, Investigation, Methodology, Resources, Software, Visualization, Writing – original draft, Writing – review & editing. N: Supervision, Validation, Writing – original draft, Writing – review & editing, Methodology. MP: Supervision, Validation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
I would like to thank the parties involved in completing this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Ayu G, Krisna P, Faozi E. An overview : quality of life of diabetes mellitus type 2 patients who participate in the prolanis program in sukoharjo regency. Jurnal berita Ilmu keperawatan. (2023) 16:29–38. doi: 10.23917/bik.v16i1.762
2. Hudiyawati D, Rosyid FN, Pratiwi A, Sulastri S, Kartinah K. The effect of structured education and telemonitoring on self-care, self-efficacy and quality of life in heart failure patients: A randomized controlled trial. Evid. Based Care J. (2023) 13:7–16. doi: 10.22038/EBCJ.2023.69805.2819
3. Saranya S, Banupriya N, Sivaharni S, Suvalakshmi E, Suganthi B. Early detection of chronicity foot lesion in diabetic neuropathy patients. IOP Conf Series: Materials Sci Eng. (2019) 590:1–7. doi: 10.1088/1757-899X/590/1/012065
4. Wang F, Zheng M, Hu J, Fang C, Chen T, Wang M, et al. Value of shear wave elastography combined with the Toronto clinical scoring system in diagnosis of diabetic peripheral neuropathy. Med (United States). (2021) 100:E27104. doi: 10.1097/MD.0000000000027104
5. Orbell S. Encyclopedia of behavioral medicine, encyclopedia of behavioral medicine. New York, Springer New York (2020). doi: 10.1007/978-1-4419-1005-9.
6. Malik RA, Andag-Silva A, Dejthevaporn C, Hakim M, Koh JS, Pinzon R, et al. Diagnosing peripheral neuropathy in South-East Asia: A focus on diabetic neuropathy. J Diabetes Investig. (2020) 11:1097–103. doi: 10.1111/jdi.13269
7. Chevtchouk L, Da Silva MHS, Do Nascimento OJM. Ankle-brachial index and diabetic neuropathy: Study of 225 patients. Arq Neuropsiquiatr (2017) 75:533–8. doi: 10.1590/0004-282x20170084
8. Kementerian Kesehatan RI. Profil kesehatan Indonesia tahun 2019’. In: Short textbook of preventive and social medicine. Indonesia, Ministry of Health Indonesia (2020). p. 28–8. doi: 10.5005/jp/books/11257_5
9. Basir IS, Syam Y, Yusuf S, Sandi S. Accuracy of Ipswich Touch Test (IpTT) to detect small fiber neuropathy and large fiber neuropathy as a risk factor of diabetic foot ulcers in public health centers. Enfermeria Clinica. (2020) 30:308–12. doi: 10.1016/j.enfcli.2019.07.108
10. Jones K, Backhouse MR, Bruce J. Rehabilitation for people wearing offloading devices for diabetes-related foot ulcers: a systematic review and meta-analyses. J Foot Ankle Res. (2023) 16:1–14. doi: 10.1186/s13047-023-00614-2
11. Ziegler D, Landgraf R, Lobmann R, Reiners K, Rett K, Schnell O, et al. Screening and diagnosis of diabetic polyneuropathy in clinical practice: A survey among German physicians (PROTECT Study Survey). Primary Care Diabetes. (2022) 16:804–9. doi: 10.1016/j.pcd.2022.09.009
12. Sucheston-Campbell LE, Clay-Gilmour AI, Barlow WE, Budd GT, Stram DO, Haiman CA, et al. Genome-wide meta-analyses identifies novel taxane-induced peripheral neuropathy-associated loci. Pharmacogenet Genomics. (2018) 28:49–55. doi: 10.1097/FPC.0000000000000318
13. Idiáquez Rios JF, Acosta I, Prat A, Gattini F, Pino F, Barnett-Tapia C. Assessing diabetic polyneuropathy in Spanish-speaking patients: Translation and validation of the Toronto Clinical Neuropathy Score, New Jersey, United States. J Peripher Nerv Syst. (2023) 28:471–5. doi: 10.1111/jns.12577
14. Hnit MW, Han TM, Nicodemus L. Accuracy and cost-effectiveness of the diabetic foot screen proforma in detection of diabetic peripheral neuropathy in Myanmar’. J ASEAN Fed Endocrine Societies. (2022) 37:31–7. doi: 10.15605/jafes.037.01.06
15. Oh TJ, Song Y, Jang HC, Choi SH. SUDOSCAN in combination with the michigan neuropathy screening instrument is an effective tool for screening diabetic peripheral neuropathy. Diabetes Metab J. (2022) 46:319–26. doi: 10.4093/dmj.2021.0014
16. Haque F, Reaz MBI, Chowdhury MEH, Shapiai MI, Malik RA, Alhatou M, et al. A machine learning-based severity prediction tool for the michigan neuropathy screening instrument A machine learning-based severity prediction tool for the michigan neuropathy screening instrument. Diagnostics (2023) 13. doi: 10.3390/diagnostics13020264
17. Dhanapalaratnam R, Issar T, Poynten AM, Milner KL, Kwai NCG, Krishnan A V. Diagnostic accuracy of nerve ultrasonography for the detection of peripheral neuropathy in type 2 diabetes. Eur J Neurol. (2022) 29:3571–9. doi: 10.1111/ene.15534
18. Drechsel TJ, Monteiro RL, Zippenfennig C, Ferreira JSSP, Milani TL, Sacco ICN. Low and high frequency vibration perception thresholds can improve the diagnosis of diabetic neuropathy. J Clin Med. (2021) 10:1–13. doi: 10.3390/jcm10143073
19. Itani M, Gylfadottir SS, Krøigård T, Kristensen AG, Christensen DH, Karlsson P, et al. Small and large fiber sensory polyneuropathy in type 2 diabetes: Influence of diagnostic criteria on neuropathy subtypes. J Peripheral Nervous System. (2021) 26:55–65. doi: 10.1111/jns.12424
20. Ramanathan S, Thomas R, Chanu AR, Naik D, Jebasingh F, Sivadasan A, et al. Standard clinical screening tests, sural radial amplitude ratio and f wave latency compared to conventional nerve conduction studies in the assessment of sensorimotor polyneuropathy in patients with type 2 diabetes mellitus. Indian J Endocrinol Metab. (2021) 25:509–15. doi: 10.4103/ijem.ijem_426_21
21. Fateh HR, Madani SP. Role of interdigital sensory nerve conduction study as a noninvasive approach for early diagnosis of diabetic peripheral neuropathy. J Diabetes Metab Disord. (2021) 20:71–5. doi: 10.1007/s40200-020-00710-1
22. Gylfadottir SS, Itani M, Krøigård T, Kristensen AG, Christensen DH, Nicolaisen SK, et al. Diagnosis and prevalence of diabetic polyneuropathy: a cross-sectional study of Danish patients with type 2 diabetes. Eur J Neurol. (2020) 27:2575–85. doi: 10.1111/ene.14469
23. Pafili K, Trypsianis G, Papazoglou D. Clinical tools for peripheral neuropathy to exclude cardiovascular autonomic neuropathy in type 2 diabetes mellitus. Diabetes Ther. (2020) 11:979–86. doi: 10.1007/s13300-020-00795-0
24. Kaymaz S, Alkan H, Karasu U, Çobankara V. Turkish version of the Michigan Neuropathy Screening Instrument in the assessment of diabetic peripheral neuropathy: a validity and reliability study. Diabetol Int. (2020) 11:283–92. doi: 10.1007/s13340-020-00427-9
25. Dubey VN, Dave JM, Beavis J, Coppini DV. Predicting diabetic neuropathy risk level using artificial neural network and clinical parameters of subjects with diabetes. J Diabetes Sci Technol. (2022) 16:275–81. doi: 10.1177/1932296820965583
26. Preston FG, Meng Y, Burgess J, Ferdousi M, Azmi S, Petropoulos IN, et al. Artificial intelligence utilising corneal confocal microscopy for the diagnosis of peripheral neuropathy in diabetes mellitus and prediabetes. Diabetologia. (2022) 65:457–66. doi: 10.1007/s00125-021-05617-x
27. Liu M, Gao Y, Chen DW, Lin S, Wang C, Chen LH, et al. Quantitative vibration perception threshold in assessing diabetic polyneuropathy: Should the cut-off value be adjusted for Chinese individuals with type 2 diabetes? J Diabetes Invest. (2021) 12:1663–70. doi: 10.1111/jdi.13515
28. Carbajal-Ramirez A, Hernández-Domínguez JA, Molina-Ayala MA, Rojas-Uribe MM, Chávez-Negrete A. Early identification of peripheral neuropathy based on sudomotor dysfunction in Mexican patients with type 2 diabetes. BMC Neurol. (2019) 19:1–6. doi: 10.1186/s12883-019-1332-4
29. Matuszewska-Iwanicka A, Stratmann B, Stachs O, Allgeier S, Bartschat A, Winter K, et al. Mosaic vs. Single image analysis with confocal microscopy of the corneal nerve plexus for diagnosis of early diabetic peripheral neuropathy. Ophthalmol Ther. (2022) 11:2211–23. doi: 10.1007/s40123-022-00574-z
30. Huang YC, Chuang YC, Chiu WC, Huang CC, Cheng BC, Kuo CEA, et al. Quantitative thermal testing as a screening and follow-up tool for diabetic sensorimotor polyneuropathy in patients with type 2 diabetes and prediabetes. Front Neurosci. (2023) 17:1115242. doi: 10.3389/fnins.2023.1115242
31. Whiting PF, Rutjes AWS, Westwood ME, Mallett S, Deeks JJ, Reitsma JB, et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. (2011) 155:529–36. doi: 10.7326/0003-4819-155-8-201110180-00009
32. Page MJ, Moher D, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ (Clinical Res ed.). (2021) 372:n160. doi: 10.1136/bmj.n160
33. Haque F, Reaz MBI, Chowdhury MEH, Kiranyaz S, Ali SHM, Alhatou M, et al. Performance analysis of conventional machine learning algorithms for diabetic sensorimotor polyneuropathy severity classification using nerve conduction studies. Comput Intell Neurosci. (2022) 2022:1–13. doi: 10.1155/2022/9690940
34. Sartika I, Azzam R. The relationship of self efficacy and family support with self care in elderly age diabetes mellitus type II. Jurnal Berita Ilmu Keperawatan. (2023) 16:89–98. doi: 10.23917/bik.v16i1.1161
35. Purwanti OS, Nurani P, Wulandari AU. Journal of medicinal and chemical sciences effect of video education about hypoglycemia on knowledge of diabetes mellitus patients and their families. J Med Chem Sci. (2021) 4:267–78. doi: 10.26655/JMCHEMSCI.2021.3.7
36. Nurlaela ES, Purwanti OS. Pengaruh strategi problem focused coping terhadap distress pada penyandang diabetes melitus. Jurnal Berita Ilmu Keperawatan. (2020) 13:31–9. doi: 10.23917/bik.v13i1.10401
37. Purwanti OS, Yetti K, Herawati T. ‘Relationship of visual impairment and peripheral artery disease with the occurrence of diabetic foot ulcers in Dr . Moewardi Hospital’. Frontiers of Nursing (2019) 6:157–60. doi: 10.2478/FON-2019-0023
38. Ismail MH, Yulian V. Pengaruh dukungan kelompok terhadap kualitas hidup penderita diabetes melitus. Jurnal Berita Ilmu Keperawatan. (2019) 12:51–8. doi: 10.23917/bik.v12i2.9806
39. Chuter V, Quigley F, Tosenovsky P, Ritter JC, Charles J, Cheney J, et al. Australian guideline on diagnosis and management of peripheral artery disease: part of the 2021 Australian evidence-based guidelines for diabetes-related foot disease. J foot ankle Res. (2022) 15:51. doi: 10.1186/s13047-022-00550-7
40. Olaiya MT, Hanson RL, Kavena KG, Sinha M, Clary D, Horton MB, et al. Use of graded Semmes Weinstein monofilament testing for ascertaining peripheral neuropathy in people with and without diabetes. Diabetes Res Clin Pract. (2019) 151:1–10. doi: 10.1016/j.diabres.2019.03.029
41. Pamungkas RA, Usman AM, Chamroonsawasdi K. View of clinical features of peripheral neurophaty among onset type 2 diabestes mellitus_ A michigan neuropathy screening instrument (MNSI) approach. Indonesian Contemp Nurs J. (2023) 7:46–52. doi: 10.20956/icon.v7i2.21689Ò9
Keywords: diabetes mellitus, neuropathy, early detection of neuropathy, neuropathy instrument, neuropathy examination
Citation: Purwanti OS, Nursalam N and Pandin MGR (2024) Early detection of diabetic neuropathy based on health belief model: a scoping review. Front. Endocrinol. 15:1369699. doi: 10.3389/fendo.2024.1369699
Received: 12 January 2024; Accepted: 19 March 2024;
Published: 24 April 2024.
Edited by:
Federico Biscetti, Agostino Gemelli University Polyclinic (IRCCS), ItalyReviewed by:
Sudhanshu Kumar Bharti, Patna University, IndiaCosmin Mihai Vesa, University of Oradea, Romania
Copyright © 2024 Purwanti, Nursalam and Pandin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nursalam Nursalam, bnVyc2FsYW1AZmtwLnVuYWlyLmFjLmlk