 Jingfeng Chen
Jingfeng Chen Lina Wen2†
Lina Wen2†- 1Department of Geriatric Endocrinology and Metabolism, Guangxi Academy of Medical Sciences and the People's Hospital of Guangxi Zhuang Autonomous Region, Nanning, China
- 2Cardiovascular Medicine Cadre Ward and Geriatric Cardiovascular Medicine Department, Guangxi Academy of Medical Sciences and the People's Hospital of Guangxi Zhuang Autonomous Region, Nanning, China
- 3Department of Nursing, Guangxi Academy of Medical Sciences and the People's Hospital of Guangxi Zhuang Autonomous Region, Nanning, China
Background: Although the relationship between health literacy and glycemic control has been explored in patients with diabetes, little is known about the relationship between different categories of diabetes health literacy and glycemic control in rural areas. Therefore, this study focused on the relationship between different categories of health literacy and glycemic control among diabetic patients in rural areas of Guangxi, China
Objective: To explore the potential profiles of health literacy among rural diabetes patients in Guangxi and investigate their relationship with blood sugar control.
Methods: A health literacy questionnaire was administered to 2280 rural diabetes patients in five cities in the Guangxi Zhuang Autonomous Region. Latent profile analysis was conducted to identify potential health literacy profiles.
Results: Health literacy among rural diabetes patients in Guangxi could be categorized into high literacy-high functionality and low literacy-low criticality groups. The latent categories of health literacy were associated with blood sugar control, with diabetes patients in the high literacy-high functionality group demonstrating better blood sugar control than those in the low literacy-low criticality group (P < 0.05).
Conclusion: Health literacy among rural diabetes patients in Guangxi exhibits heterogeneity. Healthcare professionals should pay attention to patients with low literacy and low criticality in rural areas and develop interventions to enhance their health literacy, thereby improving their blood sugar control.
1 Introduction
Diabetes is one of the most globally significant chronic diseases, with complex pathophysiology and unclear etiology. According to a report from the International Diabetes Federation (IDF), China has the highest number of diabetes patients in the world, with nearly 114 million adult cases, accounting for 24% of the total global diabetes population (1). Furthermore, the growth of diabetes patients in rural areas has outpaced urban areas (2). This increase in prevalence has placed a considerable burden on healthcare systems and management costs (3). Surveys indicate that the prevalence of diabetes in adults in Guangxi’s rural areas is 5.9%, with only 22.2% achieving adequate blood sugar control (4). Diabetes primarily results from insufficient insulin secretion or resistance, and poor long-term blood sugar control can lead to various complications. Therefore, maintaining good blood sugar control is essential for preventing and delaying complications (5).
Currently, diabetes cannot be cured, and patients require lifelong oral antidiabetic medication or subcutaneous insulin injections to effectively control blood sugar, slow disease progression, reduce complication rates, and improve prognosis (6).Health literacy refers to an individual’s ability to obtain health information through various channels, correctly understand and apply this information to actively maintain and promote their own health (7). The American Diabetes Association includes improving health literacy among diabetes patients as an essential component of overall diabetes management in its “Standards of Medical Care in Diabetes” (8). Diabetes patients with lower health literacy, due to limited reading and mathematical abilities, are more likely to have suboptimal blood sugar control and an increased risk of diabetes complications (9). Conversely, a higher level of health literacy can effectively control blood sugar levels, manage complications, and enhance quality of life for diabetes patients (10). The level of health literacy may vary among different diabetes patients based on factors such as cognitive level and treatment stage (11). Analyzing health literacy levels and capturing individual characteristics are prerequisites for implementing personalized and precise interventions.
Latent profile analysis is a “person-centered” statistical method that classifies heterogeneous populations into different homogeneous subgroups based on health literacy levels. This approach offers new insights for individualized and precise interventions. Currently, research on the health literacy of diabetes patients, both domestically and internationally, tends to focus on variable-centered research methods, with limited studies on category divisions and the relationship between different categories and blood sugar control. This study utilizes latent profile analysis to categorize the health literacy of diabetes patients in rural areas and analyze the relationship between different categories and blood sugar control. This research aims to provide a basis for diabetes health management in rural areas in the future.
2 Materials and methods
2.1 Sample
Between January 2022 and July 2022, a multi-stage stratified sampling method was employed to select the study subjects. In the first stage, five cities, namely Nanning, Guilin, Hechi, Chongzuo, and Yulin, were randomly selected based on the geographical regions of the Guangxi Zhuang Autonomous Region (central, eastern, southern, western, and northern). In the second stage, three counties were randomly chosen within each of the selected cities, resulting in a total of 15 counties for the survey. In each county, one internal medicine department from a local hospital was selected for the investigation. A total of 152 individuals were surveyed in each hospital, resulting in 2280 patients being surveyed in total.Inclusion criteria were as follows: (1) Conforming to the diagnostic criteria for diabetes established by the Chinese Diabetes Society in 2020 (8); (2) Age ≥ 18 years; (3) Registered and currently residing in the surveyed area. Exclusion criteria were as follows: (1) Patients with gestational diabetes; (2) Patients with a known history of dementia or other mental disorders based on medical records or information obtained from family members; (3) Patients in the acute phase of their illness, unable to cooperate with the investigation. Written informed consent was obtained from all participants, and informed consent was provided by the administrators of all hospitals participating in this study.
2.2 Survey tools
2.2.1 General information questionnaire
This questionnaire was developed by the researchers and includes demographic information such as age, gender, marital status, educational level, and per capita annual disposable income (9). It also covers disease-related data, including disease duration, glycated hemoglobin levels, whether the participant is using antidiabetic medication, and whether they are undergoing insulin treatment.
2.2.3 Health literacy scale
The Health Literacy Scale (HLS) is an assessment tool developed by Ishikawa et al. in 2008 for evaluating the health literacy of diabetes patients. In 2021, Zhao Xiaoyan et al. (12) translated and validated the scale into Chinese. The scale consists of three dimensions: functional health literacy, communicative health literacy, and critical health literacy, encompassing a total of 14 items. Respondents use a 4-point Likert scale, with scores ranging from 1 to 4, corresponding to “completely absent” to “most of the time.” Notably, the functional health literacy dimension is reverse-scored. The total score on the scale ranges from 14 to 56, with higher scores indicating better health literacy. The Cronbach’s α coefficient for the Chinese version of HLS is 0.868.
2.3 Ethical considerations
The hospital where the authors are affiliated received approval from the Ethics Committee (Approval Number: KT-KJT-2021-26). The questionnaire outlined the voluntary and confidential nature of participation, and all hospital administrators and participants provided informed consent.
2.4 Data collection
This study involved questionnaire surveys, blood collection at local hospitals, and assisting patients in filling out standardized questionnaires. Researchers recorded general information and glycated hemoglobin values for diabetes patients in 15 hospitals and entered the results into Excel, which were then transmitted to us via the internet. Upon completion of the questionnaires, they were also sent to us electronically. We compiled data from the 15 hospitals and stored it in Excel spreadsheets. All data were independently verified and input into SPSS by two researchers. All information is stored on a secure computer to prevent data leakage.
2.5 Data analysis
This study employed SPSS 22.0 and Mplus 8.3 software for data statistical analysis and processing. (1) The health literacy scores of rural diabetes patients, treated as a continuous variable, were used as the manifest variable for latent profile data processing with Mplus 8.3 (13). The initial model started from “1” and gradually increased the number of latent categories until the best model fit was achieved. Fit indices included: (i) Akaike Information Criteria (AIC), Bayesian Information Criteria (BIC), and adjusted Bayesian Information Criteria (aBIC), with smaller values indicating better fit; (ii) Entropy, which represents classification accuracy, and when Entropy > 0.8, it indicates classification accuracy > 90%; (iii) Model comparisons were primarily based on the Bootstrap Likelihood Ratio Test (BLRT) and Likelihood Ratio Test (LMR). When the p-values corresponding to LMR and BLRT reached a significance level, it indicated that the model had a better fit than the previous one. This study comprehensively evaluated the fit of various category models and selected the best model.(2) Data were analyzed using SPSS 25.0 software. For quantitative data that followed a normal distribution, descriptive statistics were presented as x ± s (mean ± standard deviation). For data that did not follow a normal distribution, descriptive statistics were presented as M (Q1, Q3) (median with interquartile range). Qualitative data were described using frequency counts. Multivariate logistic regression analysis was used to determine whether statistically significant differences existed among different latent profile groups concerning their manifest characteristics. Based on these results and considering the normal distribution of the total health literacy scores, different latent profile groups’ health literacy levels were compared using t-tests, one-way analysis of variance, or non-parametric tests such as the Mann-Whitney U test and Kruskal-Wallis H test. All tests were two-tailed, and p<0.05 was considered statistically significant.
3 Results
3.1 Basic information of patients
A survey was conducted on 2,280 rural diabetic patients, of which a total of 2,178 rural diabetic patients were effectively surveyed. The basic profile of the patients surveyed is shown in Table 1. The surveyed rural diabetic patients had an average age of (63.25 ± 12.71) years and an average duration of illness of (7.96 ± 4.07) years. The male proportion was 55.28%, indicating a higher representation of males than females. In terms of educational background, the majority had completed junior high school education, accounting for 31.43%. The proportion of patients with per capita disposable annual family income ≥18931 yuan was 37.74%. The proportion of patients with a family history of diabetes was 14.55%, and the proportion of patients with HbA1c control <7.0% was 22.68%.
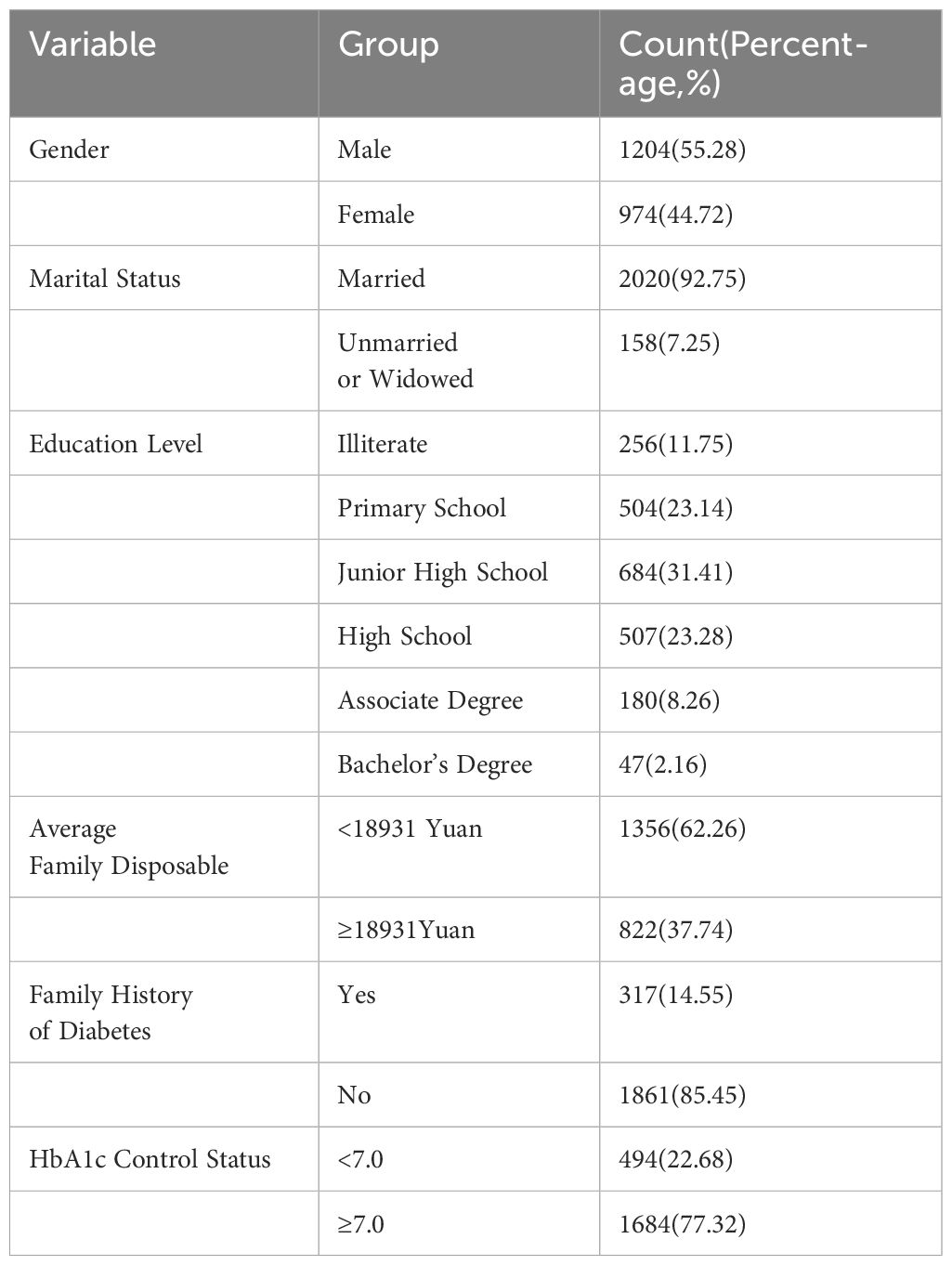
Table 1 General information of surveyed rural diabetic patients (n=2178).
3.2 Latent profile analysis of health literacy in rural diabetes patients
The fitting statistics for the profile models are shown in Table 2. According to the entropy, the class 2 model fits the best. And the P-values of both LMR and BLRT were statistically significant, so the class 2 model was chosen as the final model.
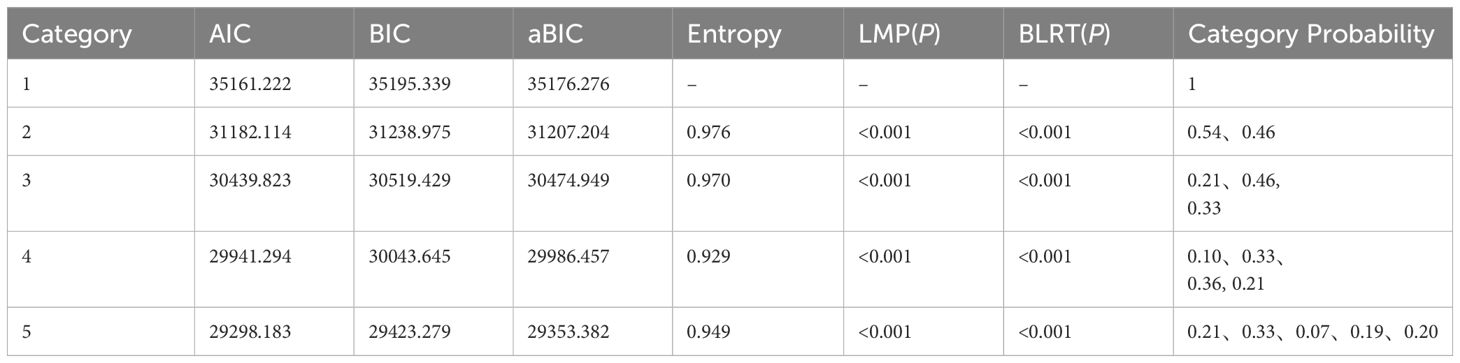
Table 2 Model fit indices of latent profile models for health literacy in rural diabetes patients (n=2178).
3.3 Characteristics and naming of latent casses for health literacy in rural diabetes patients
The health literacy of diabetic patients in rural areas is categorized into two potential groups, showing distinct characteristics across three dimensions. Category 1, with a total health literacy score of (39.53 ± 4.795), exhibits relatively higher levels of health literacy across all dimensions. Among these, the functional health literacy dimension scored the highest at (14.72 ± 1.366), thus labeled as the high literacy-high functionality group. Category 2, with a total health literacy score of (22.82 ± 3.768), demonstrated lower scores across various dimensions of health literacy. Particularly, the critical dimension scored the lowest at (6.24 ± 1.280), hence named the low literacy-low criticality group. The scores for each dimension of health literacy for the two categories of rural diabetic patients are detailed in Table 3.
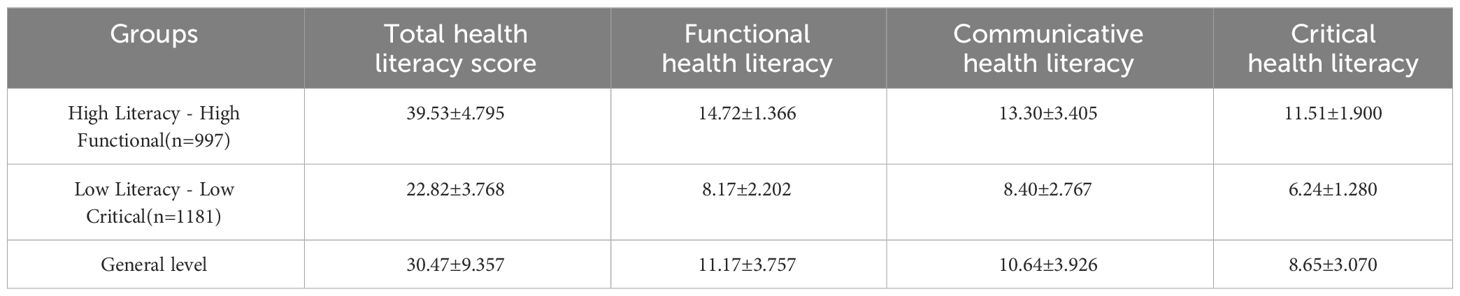
Table 3 Health literacy scores for different categories of rural diabetes patients (n=2178).
3.4 Comparison of socio-demographic characteristics of different latent classes of health literacy in rural diabetes patients
Comparison of socio-demographic characteristics of different potential categories of health literacy among diabetic patients in rural areas is shown in Table 4, which shows that the differences between the two groups were statistically significant (p < 0. 05) in terms of educational level (χ2 = 83.169, p < 0. 001), per capita annual disposable income of the family (χ2 = 64.792, p < 0. 001), the duration of the disease with or without complications (χ2 = 10.106, p<0.001), family history of diabetes (χ2 = 27.362, p<0.001) the difference was statistically significant (p<0. 05).
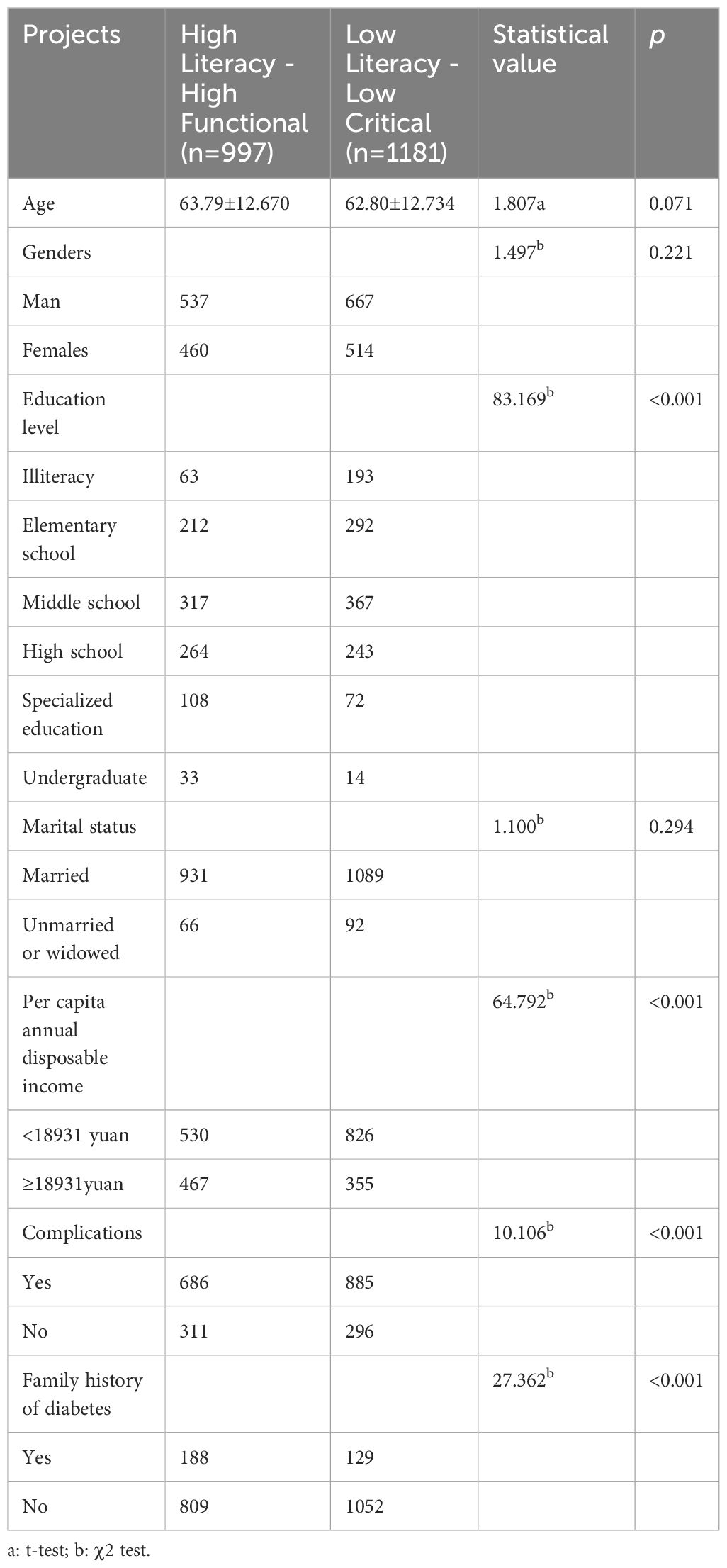
Table 4 Comparison of socio-demographic characteristics of different latent classes.
3.5 Comparison of HbA1c control rate in rural diabetes patients with different latent profiles of health literacy
The standardized HbA1c rate for all study subjects was 22.68%. The high literacy-high functionality group demonstrated a blood sugar control rate of 39.12% (390/997), while the low literacy-low criticality group exhibited a blood sugar control rate of 9.66% (104/1077). The blood sugar control rate in the high literacy-high functionality group was significantly higher than that in the low literacy-low criticality group (P < 0.001). The results are presented in Table 5.
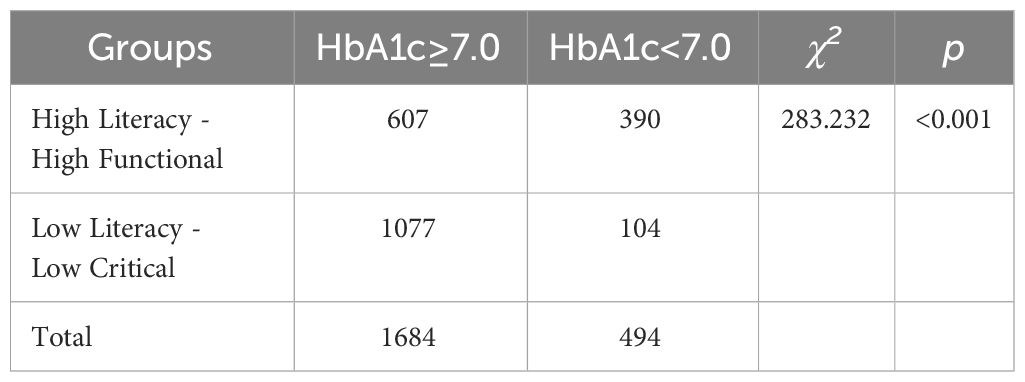
Table 5 Comparison of HbA1c control rate in DM patients with different health literacy levels.
3.6 Impact of health literacy level in diabetes patients on blood sugar control
The HbA1c standardization rate was considered as the dependent variable, while health literacy served as the independent variable. After controlling for variables such as age, gender, educational level, family per capita disposable income, family history of diabetes, medication usage, insulin use, and presence of comorbidities, a variable screening using the entry method (α = 0.05) was conducted for logistic regression analysis. The results showed that age, gender, presence of medication, insulin use, education level, per capita disposable household income, and health literacy category were the influencing factors of HbA1c attainment rate, (p<0.05),The attainment rate of HbA1c control was higher in males as compared to females (OR:0.764,CI:0.606-0.964). Patients in the high-literacy-high-functionality group may have a higher rate of achieving HbA1c control compared to patients in the low-literacy-low-criticism group (OR: 5.295, CI 4.103-6.827). Patients taking oral hypoglycaemic agents had a higher rate of achieving HbA1c control compared to patients not taking oral hypoglycaemic agents (OR: 2.270, CI: 1.750-2.943). Patients using insulin had a higher rate of achieving HbA1c control compared to patients not using insulin (OR: 2.957, CI:2.338-3.740). Compared with patients with per capita disposable annual household income <18931 yuan, patients with per capita disposable annual household income ≥18931 yuan had a higher rate of achieving HbA1c control (OR: 1.682, CI: 1.331-2.125). The results are presented in Table 6.
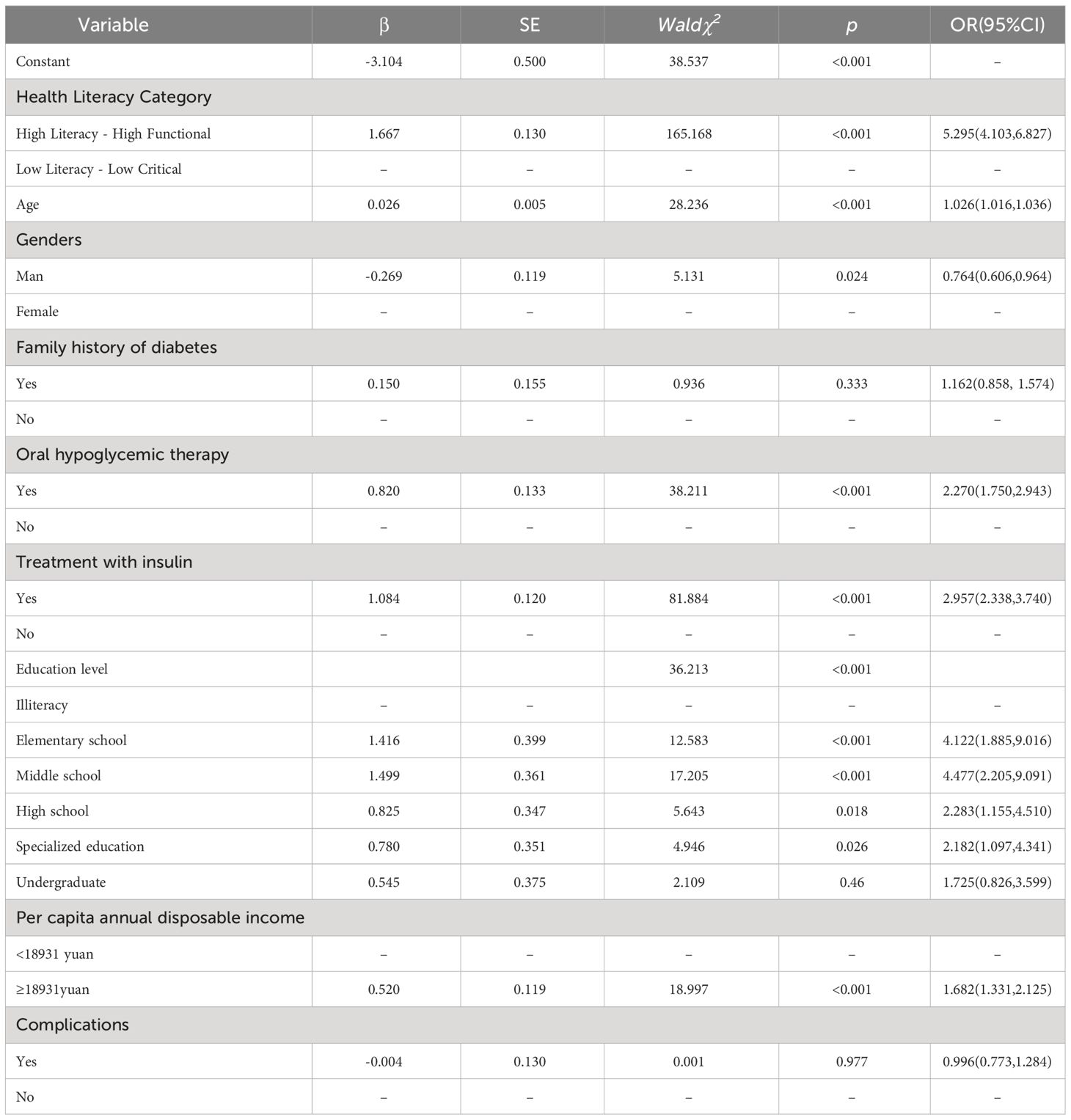
Table 6 Logistic regression analysis of HbA1c control rate in rural diabetes patients.
4 Discussion
4.1 Characteristics of different latent profiles of health literacy in rural diabetes patients
The use of latent profile analysis aids in identifying heterogeneity among rural diabetes patients, facilitating the identification of variations in health literacy levels among individuals. This approach helps pinpoint issues related to health literacy among patients and allows for targeted interventions aimed at improving their knowledge level, thereby serving as a reference for interventions in glycemic control. This study employed latent profile analysis to classify rural diabetes patients into two latent categories based on health literacy: the high literacy-high functionality group and the low literacy-low criticality group. The latter, constituting 54.22% (1181/2178) of the total, exhibits relatively lower scores across health literacy dimensions compared to the overall level. This suggests difficulties in accessing and utilizing health information and inaccurate judgment of health information among these patients. Probable causes include the relatively underdeveloped economic status of Guangxi, situated in the western region of China (12), with rural diabetes patients having lower educational levels and relatively lower incomes (14, 15). Consequently, these patients have limited disease-related knowledge and information acquisition abilities, compounded by long disease durations leading to decreased disease awareness (16). Healthcare providers should encourage these patients to acquire knowledge through various channels and offer personalized or group health education to enhance their understanding and acquisition of health information, especially for those with lower literacy and limited learning abilities. The high literacy-high functionality group comprises 45.78% (997/2178) of the patients, displaying higher scores in all dimensions of health literacy compared to the overall level. Notably, this group excels particularly in the functional aspect of health literacy, indicating their willingness to invest time and effort in understanding diabetes-related health knowledge. This may be attributed to their relatively higher cultural and knowledge levels, enhancing their reading and information utilization abilities. Healthcare providers should encourage patients in this group to foster a strong desire to improve health and enhance their awareness of health.
4.2 Factors affecting health literacy in rural diabetes patients
By exploring the differences in disease-related information and demographic characteristics among different health literacy categories, it was found that patients in the high literacy-high functionality group have higher educational levels and relatively younger ages compared to those in the low literacy-low criticality group, which is consistent with other studies (17–19). Additionally, the low literacy-low criticality group of diabetes patients showed a higher prevalence of comorbid complications, suggesting an inverse relationship between the occurrence of diabetes complications and the level of health literacy. Ajuwon’s findings show that lower health literacy among African Americans is associated with lower self-management behaviours that can lead to complications of type 2 diabetes (20). This is similar to our findings. The results of this study also indicate that patients in the high literacy-high functionality group have higher average monthly family incomes compared to those in the low literacy-low criticality group, consistent with other research (21, 22). This could be attributed to an increased awareness of disease treatment in situations where material needs are met, prompting patients to actively invest in their health, thereby enhancing their health literacy regarding chronic diseases.
4.3 Relationship between latent profiles of health literacy and blood sugar control in rural diabetes patients
Studies (23–25) have indicated a significant negative correlation between health literacy among diabetes patients and glycemic control. In this study, the high literacy-high functionality group exhibited the highest number of patients meeting blood sugar control standards, while the low literacy-low criticality group showed fewer patients meeting these standards, highlighting differences in glycemic control between the two categories of patients. Logistic regression analysis revealed that the diverse latent profiles of health literacy among rural diabetes patients are influencing factors in glycemic control. Patients in the high literacy-high functionality group exhibited significantly better glycemic control compared to those in the low literacy-low criticality group. Achieving glycemic control reflects an individual’s spontaneous and multi-dimensional health-promoting behavior aimed at maintaining or improving their own health status (26). A higher level of health literacy in diabetes patients is associated with a better understanding of disease-related knowledge, improved treatment adherence, and a higher level of glycemic control (27). Therefore, healthcare professionals can encourage patients to learn and acquire knowledge related to diabetes. For diabetes patients in remote rural areas of Guangxi, interventions such as establishing platforms for diabetes knowledge acquisition and exchange could be implemented to enhance patient health literacy, consequently elevating their level of glycemic control.
5 Limitations
This was a multicenter cross-sectional study, and we conducted questionnaire surveys in 15 county-level hospitals. While we selected rural diabetes patients according to national diagnostic criteria, the models of the hemoglobin A1c measurement devices in these 15 county hospitals were not identical, resulting in slight variations in test results between hospitals. We were unable to transport these devices to rural areas for the study, so we chose to survey rural diabetes patients who sought treatment at the hospitals. Therefore, caution should be exercised when applying these findings for broader use. Second, we assessed patient literacy using the Health Literacy Scale, a tool that can be time-consuming in clinical use.
6 Conclusion
There are variations in health literacy levels among rural diabetes patients, categorizing them into two groups: high literacy with high functionality and low literacy with low criticality. The proportion of individuals with high literacy is relatively small, indicating significant room for improvement. Moreover, the group with low literacy and low criticality has a lower rate of blood glucose control. Healthcare professionals can enhance the health literacy of rural diabetes patients to improve their blood glucose control outcomes.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Ethics Committee of the People’s Hospital of Guangxi Zhuang Autonomous Region. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
JC: Writing – original draft, Data curation. LW: Writing – review & editing. GF: Writing – review & editing, Data curation. CB: Writing – original draft, Investigation, Data curation. XL: Writing – original draft, Investigation, Data curation. YZ: Writing – review & editing, Project administration.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. Technology, Guangxi Zhuang Autonomous Region.
Acknowledgments
We are very grateful to all the patients who actively cooperated with the investigation, and sincerely thank the medical staff of the 15 hospitals participating in the investigation for their help, and thank every member of the diabetes health management team of Guangxi Academy of Medical Sciences and Guangxi Zhuang Autonomous Region People’s Hospital for their joint efforts.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Sun H, Saeedi P, Karuranga S, Pinkepank M, Ogurtsova K, Duncan BB, et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. (2022) 183:109119. doi: 10.1016/j.diabres.2021.109119
2. Wang L, Gao P, Zhang M, Huang Z, Zhang D, Deng Q, et al. Prevalence and ethnic pattern of diabetes and prediabetes in China in 2013. JAMA. (2017) 317:2515–23. doi: 10.1001/jama.2017.7596
3. Lin X, Xu Y, Pan X, Xu J, Ding Y, Sun X, et al. Global, regional, and national burden and trend of diabetes in 195 countries and territories: an analysis from 1990 to 2025. Sci Rep. (2020) 10:14790. doi: 10.1038/s41598-020-71908-9
4. Lu W, Yang H, Meng X, Luo S, Xu J, Huang T, et al. Survey on the prevalence and knowledge, treatment and control of diabetes mellitus among adult residents in Guangxi. China Chronic Dis Prev Control. (2018) 26:250–3. doi: 10.16386/j.cjpccd.issn.1004-6194.2018.04.003
5. Laiteerapong N, Ham SA, Gao Y, Moffet HH, Liu JY, Huang ES, et al. The legacy effect in type 2 diabetes: impact of early glycemic control on future complications (The diabetes & Aging study). Diabetes Care. (2019) 42:416–26. doi: 10.2337/dc17-1144
6. Nauck MA, Wefers J, Meier JJ. Treatment of type 2 diabetes: challenges, hopes, and anticipated successes. Lancet Diabetes Endocrinol. (2021) 9:525–44. doi: 10.1016/S2213-8587(21)00113-3
7. Nutbeam D, Lloyd JE. Understanding and responding to health literacy as a social determinant of health. Annu Rev Public Health. (2021) 42:159–73. doi: 10.1146/annurev-publhealth-090419-102529
8. American Diabetes Association. Standards of medical care in diabetes–2014. Diabetes Care. (2014) 37 Suppl 1:S14–80. doi: 10.2337/dc14-S014
9. Hashim SA, Barakatun-Nisak MY, Abu SH, Ismail S, Hamdy O, Mansour AA. Association of health literacy and nutritional status assessment with glycemic control in adults with type 2 diabetes mellitus. Nutrients. (2020) 12(10):3152. doi: 10.3390/nu12103152
10. Butayeva J, Ratan ZA, Downie S, Hosseinzadeh H. The impact of health literacy interventions on glycemic control and self-management outcomes among type 2 diabetes mellitus: A systematic review. J Diabetes. (2023) 15:724–35. doi: 10.1111/1753-0407.13436
11. Roshan AG, Hosseinkhani SN, Norouzadeh R. Health literacy and self-efficacy of the elderly with diabetes. J Diabetes Metab Disord. (2023) 22:611–7. doi: 10.1007/s40200-023-01181-w
12. Xu D, Yang Q, Lai X, Xiao Y, Dai X, Xie J, et al. Analysis of the current status and influencing factors of metabolic management of hospitalized Zhuang diabetic patients in Guangxi. J Guangxi Med Univ. (2022) 39:1655–60. doi: 10.16190/j.cnki.45-1211/r.2022.10.021
13. Bi X, Wang M. Latent variable modeling with Mplus application. Chongqing: Chongqing University Press (2018).
14. Zhou J, Yang S, Lu Y. Analysis of factors affecting glycemic control in urban and rural type 2 diabetes mellitus patients in Nanning City. Pract Prev Med. (2021) 28:785–91. doi: 10.3969/j.issn.1006-3110.2021.07.004
15. Zhao Y, Xu S, Wu Q, Xu Y, Wang Liu H, et al. Current situation and influencing factors of diabetes prevention and control literacy among some urban and rural residents in Zhejiang Province. China Chronic Dis Prev Control. (2015) 23:862–4. doi: 10.16386/j.cjpccd.issn.1004-6194.2015.11.018
16. Xu L, You S, Ning J, Huang Y, Lu G. Analysis of health literacy level and influencing factors in type 2 diabetes mellitus patients with poor glycaemic control. J Clin Military Med. (2022) 50:359–63. doi: 10.16680/j.1671-3826.2022.04.08
17. An Y, Zhang Y, Yu J. Factors influencing health literacy of type 2 diabetes mellitus patients and its role in glycaemic control. China Health Eng. (2022) 21:261–3. doi: 10.19937/j.issn.1671-4199.2022.02.028
18. Nie X, Li Y, Li L, Li HX. A study on the health information literacy level of urban and rural residents in six provinces of China. Chin J Prev Med. (2014) 48:566–70. doi: 10.3760/cma.j.issn.0253-9624.2014.07.007
19. Shi M, Wei W LIF, LI Y, Li L. Status of diabetes-related behaviours and influencing factors among urban and rural residents in six provinces of China. Chin J Prev Med. (2014) 48:571–5. doi: 10.3760/cma.j.issn.0253-9624.2014.07.008
20. Ajuwon AM, Insel K. Health literacy, illness perception, depression, and self-management among African Americans with type 2 diabetes. J Am Assoc Nurse Pract. (2022) 34:1066–74. doi: 10.1097/JXX.0000000000000763
21. Meherali S, Punjani NS, Mevawala A. Health literacy interventions to improve health outcomes in low- and middle-income countries. Health Lit Res Pract. (2020) 4:e251–66. doi: 10.3928/24748307-20201118-01
22. Mei X, Zhong Q, Chen G, Huang Y, Li J. Exploring health literacy in Wuhan, China: a cross-sectional analysis. BMC Public Health. (2020) 20:1417. doi: 10.1186/s12889-020-09520-9
23. Gomes MB, Muniz LH, Melo L, Pizarro MH, Barros BSV, Santos DC, et al. Health literacy and glycemic control in patients with diabetes: a tertiary care center study in Brazil. Diabetol Metab Syndr. (2020) 12:11. doi: 10.1186/s13098-020-0519-6
24. Zheng Z, Liu Y, Zhang W. Impact of disease-related health literacy on glycaemic control in community diabetic patients. Med Food Ther Health. (2020) 18:196–8. doi: 10.3761/j.issn.0254-1769.2012.01.027
25. Zhu X, Zhang X, Shen Y, Wang T, Wang F, Hu K, et al. Study on the relationship between glycaemic control and diabetes-related health literacy in patients with type 2 diabetes. China Health Educ. (2018) 34:873–8. doi: 10.16168/j.cnki.issn.1002-9982.2018.10.002
26. Luo H, Patil SP, Cummings DM, Bell RA, Wu Q, Adams AD, et al. Health literacy, self-management activities, and glycemic control among adults with type 2 diabetes: A path analysis. J Public Health Manag Pract. (2020) 26:280–6. doi: 10.1097/PHH.0000000000000984
Keywords: rural areas, diabetes, health literacy, blood sugar control, latent profile analysis
Citation: Chen J, Wen L, Fu G, Bai C, Lei X and Zhang Y (2024) The relationship between health literacy and blood sugar control in rural areas among diabetes patients. Front. Endocrinol. 15:1334100. doi: 10.3389/fendo.2024.1334100
Received: 06 November 2023; Accepted: 22 April 2024;
Published: 10 May 2024.
Edited by:
Åke Sjöholm, Gävle Hospital, SwedenReviewed by:
Sueziani Binte Zainudin, Sengkang General Hospital, SingaporeKrishnamurthy Nakuluri, The University of Iowa, United States
Justyna Grudziąż-Sękowska, Medical Centre for Postgraduate Education, Poland
José Pablo Miramontes González, Hospital Universitario Río Hortega, Spain
Copyright © 2024 Chen, Wen, Fu, Bai, Lei and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yanping Zhang, 2584026044@qq.com
†These authors share first authorship