 Sándor Halmi1,2
Sándor Halmi1,2 Eszter Berta1,3
Eszter Berta1,3 Ágnes Diószegi4Lívia Sira1Péter Fülöp4
Ágnes Diószegi4Lívia Sira1Péter Fülöp4 Endre V. Nagy1Ferenc Győry5Zsolt Kanyári5Judit Tóth6
Endre V. Nagy1Ferenc Győry5Zsolt Kanyári5Judit Tóth6 Harjit Pal Bhattoa7
Harjit Pal Bhattoa7 Miklós Bodor1,3*
Miklós Bodor1,3*- 1Division of Endocrinology, Department of Medicine, Faculty of Medicine, University of Debrecen, Debrecen, Hungary
- 2Doctoral School of Health Sciences, University of Debrecen, Debrecen, Hungary
- 3Department of Clinical Basics, Faculty of Pharmacy, University of Debrecen, Debrecen, Hungary
- 4Division of Metabolism, Department of Medicine, Faculty of Medicine, University of Debrecen, Debrecen, Hungary
- 5Department of Surgery, Faculty of Medicine, University of Debrecen, Debrecen, Hungary
- 6Division of Radiology and Imaging Science, Department of Medical Imaging, Faculty of Medicine, University of Debrecen, Debrecen, Hungary
- 7Department of Laboratory Medicine, Faculty of Medicine, University of Debrecen, Debrecen, Hungary
Background: Insulinomas are rare insulin-secreting neuroendocrine neoplasms of the pancreas. First-line treatment is the surgical removal of the tumor, however, the localization with standard imaging techniques is often challenging. With the help of selective intraarterial calcium stimulation the insulinoma’s localization can be narrowed down to one third of the pancreas which the selected artery supplies.
Objective: We aimed to prove the usefulness of the calcium stimulation test in case of 9 patients treated between 2006 and 2021 diagnosed with endogenous hyperinsulinemic hypoglycemia confirmed by fasting test, where conventional imaging methods, like transabdominal ultrasound, CT or MRI failed to detect the source of hyperinsulinemia.
Methods: We performed selective intraarterial calcium stimulation with angiography with calcium gluconate injected to the main supporting arteries of the pancreas (splenic, superior mesenteric and gastroduodenal arteries); blood samples were obtained from the right hepatic vein before, and 30, 60 and 120 seconds after calcium administration.
Results: With selective angiography we found a significant elevation of insulin levels taken from the right hepatic vein in five of the nine cases. On histopathology, the lesions were between 1-2 cm, in one case malignancy was also confirmed. In four patients we found a significant rise of insulin levels obtained from all catheterized sites, which confirmed the diagnosis of nesidioblastosis. In three cases no surgery was performed, and the symptoms relieved with medical treatment.
Conclusions: Selective intraarterial calcium stimulation remains an important tool in localization of the source of insulin excess, especially in cases where other diagnostic modalities fail.
1 Introduction
Insulinoma is a rare neoplasm of the pancreatic beta cells with an estimated incidence of 1-4/1 million (1, 2). Despite its rare occurrence, insulinoma is the most common functioning neuroendocrine tumor of the pancreas. Most insulinomas are sporadic, however, 5-10% of the cases can also present as part of multiple endocrine neoplasia type 1 and 4, or rarely neurofibromatosis type 1 or tuberous sclerosis (3). The cases with underlying endocrine tumor syndromes need even more stringent medical attention as 16-25% of the MEN-1 syndrome cases are malignant (4, 5).
Sporadic insulinomas develop mainly in middle-aged patients, but they can occur at any age with a female predominance (60%); 87-94% of insulinoma cases are benign and solitaire (2, 3, 6).
The appropriate diagnosis of insulinoma is often delayed and is established only years after the first appearance of the clinical symptoms (7, 8). The average time until biochemically verified diagnosis is at least 2 years, but can often take 5 or more years, or even longer, and repeated hypoglycemic episodes can lead to damage of autonomic nervous system (7, 9, 10). Weight gain is also a common finding occurring in 39-50% of patients (7, 8, 11).
The biochemical diagnosis of endogenous hyperinsulinemic hypoglycemia must be obtained. The primary suspicion for insulinoma should raise when Whipple’s triad is present (7, 12). The suspected diagnosis based on the presence of Whipple’s triad needs to be verified with a method successfully detecting 99% of the cases, namely the up to 72 hours long fasting test with concurrent measurements of beta-cell polypeptides (insulin >4 µU/mL, C-peptide >0.2 nmol/L and proinsulin >5 pmol/L) at the time of hypoglycemia (3, 7).
In most cases surgical removal of the tumor is curative. However, the localization of the tumor can be quite challenging with the widely accessible conventional imaging methods as insulinomas are usually smaller than 2 centimeters in diameter (13, 14). In patients with MEN-1 syndrome insulinomas are between 1-3 cm-s and can be multifocal (14).
According to the equal distribution of beta-cells in the pancreas, insulinomas can develop anywhere within the organ, while extrapancreatic tumors are very rare (<2%) (14–16).
One goal during surgery is to reduce the exocrine and endocrine functional loss of the pancreas; parenchyma-sparing partial pancreatectomy or tumor enucleation can only be performed after proper localization of the insulinoma. Conventional non-invasive imaging techniques like transabdominal ultrasound, contrast-enhanced CT and MRI can localize the tumor properly with detection rates of 9-63%, 63-94% and 60-90%, respectively (3). In some cases, none of the above-mentioned procedures can localize the tumor and there is need for additional diagnostic procedures. Somatostatin receptor scintigraphy has a 47-60% sensitivity (3, 17). Endoscopic ultrasound sensitivity can reach 92.6%, meanwhile the most reliable method of identifying insulinomas up to date is 68Ga-Exendin-4 PET/CT with an accuracy of 97.7% (18, 19).
With invasive techniques, like endoscopic ultrasound or selective intraarterial calcium stimulation with venous sampling (ASVS) the detection rate increases, although the usefulness of these examinations is highly dependent on the centers’ facilities and the examiners’ experience. Pre-operative localization is essential, as 9-23% of insulinomas cannot be found by intraoperative inspection and palpation (14).
The currently used ASVS procedure is based on the observation that intravenous calcium stimulates the production and release of native insulin from the hyperfunctioning pancreatic β cells, an effect not seen in case of normal β cells (3). During the test calcium stimulation is performed through the catheterized major pancreatic arteries and blood samples are collected from the right hepatic vein (20).
The advantage of the ASVS is that besides establishing the localization of the insulinoma, it complements the morphological picture with functional information, thus the sensitivity of the procedure is reported 62.5-100% with a specificity of 89.2% (14).
In our retrospective study we examined the usefulness of ASVS in patients with hyperinsulinemic hypoglycemia, where the standard imaging methods could not find the exact localization of the tumor within the pancreas.
2 Patients and methods
2.1 Patients
Nine patients treated between 2006 and 2021 at the Division of Endocrinology, University of Debrecen were retrospectively analyzed. Each patient presented the clinical symptoms characteristic for insulinoma, and the diagnosis was supported by standard biochemical tests.
The diagnosis of the endogenous hyperinsulinemic hypoglycemia was confirmed by the detection of symptomatic hypoglycemia accompanied by documented biochemical hypoglycemia (blood glucose level below 2.5 mmol/l) and elevated insulin and C peptide levels (above 4 µU/mL and 0.2 nmol/L, respectively) during 72 hours fasting.
We included only patients in whom conventional imaging methods, like transabdominal ultrasound, CT or MRI failed to detect the source of hyperinsulinemia. Patients with proven factitious hypoglycemia caused by glucose-lowering drugs or with a history of diabetes mellitus were excluded.
2.2 Methods
The aim of the study was to evaluate the use of ASVS in case of nine patients previously diagnosed with insulinoma by clinical symptoms and confirmed by fasting test. With an aim to achieve information about the proper localization of the insulinoma we performed selective angiography with calcium stimulation. During selective angiography, after the punction of the right femoral artery, the gastroduodenal, superior mesenteric and splenic arteries were, one after the other, catheterized. Four ml of 10% calcium gluconate was administered to each artery. The sampling catheter was guided through the right femoral vein and placed into the right hepatic vein. Samples were obtained after selective stimulations of the arteries supplying the respective pancreatic regions before calcium administration, and 30, 60 and 120 seconds after injection. The highest insulin level of these set of samples was used for comparison. A more than 1.5 times increase of the baseline insulin level was considered significant and confirmed tumor localization within the pancreas. Insulin levels were measured from serum samples at the Department of Laboratory Medicine, University of Debrecen by chemiluminescence immunoassay (CLIA) on a Liaison XL analyzer (Diasorin Inc, Stillwater, MN, USA).
3 Results
In this retrospective study ASVS was performed in nine patients with endogenous hyperinsulinemic hypoglycemia. The mean patients’ age was 45 ± 25 years with a 7:2 male predominance. In case of all patients, transabdominal ultrasound, CT scan and MRI failed to localize the pancreatic neuroendocrine tumor. In case of two cases (patients 1 and 2) octreotide scintigraphy was also performed and found to be negative. Since our case series encompasses a long period in which this procedure was just getting available, endoscopic ultrasound (EUS) was not performed due to lack of equipment and diagnostic expertise in our center.
We did precisely localize the insulin overproduction source in five cases comparing the insulin content of the samples obtained from the hepatic vein (Figure 1). In most of our cases the patients’ serum insulin levels peaked early, as soon as 30 seconds after calcium administration with a slight decrease in the samples obtained later. These findings correlate with literature data (21).
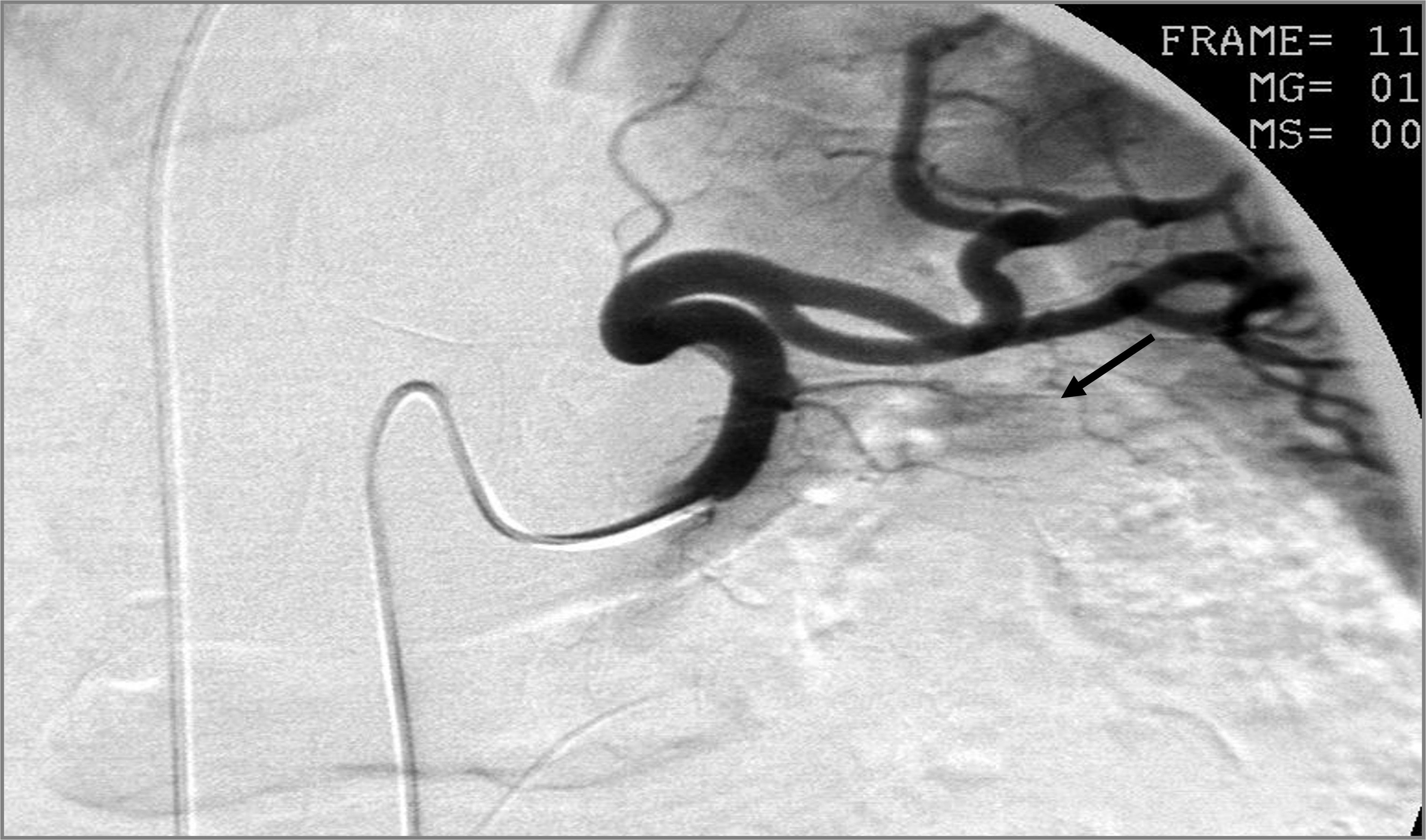
Figure 1. Angiography during ASVS in patient 1. After surgery, the insulinoma could be retrospectively identified on the angiography recording in the tail of the pancreas (arrow), where it was predicted by the ASVS insulin samples.
Clinical symptoms ceased and biochemical remission was achieved after surgery in 4 patients (Table 1). One patient, who had several comorbidities, has been lost due to postoperative complications, the histology of the pancreatic tumor and local metastases confirmed malignant insulinoma.
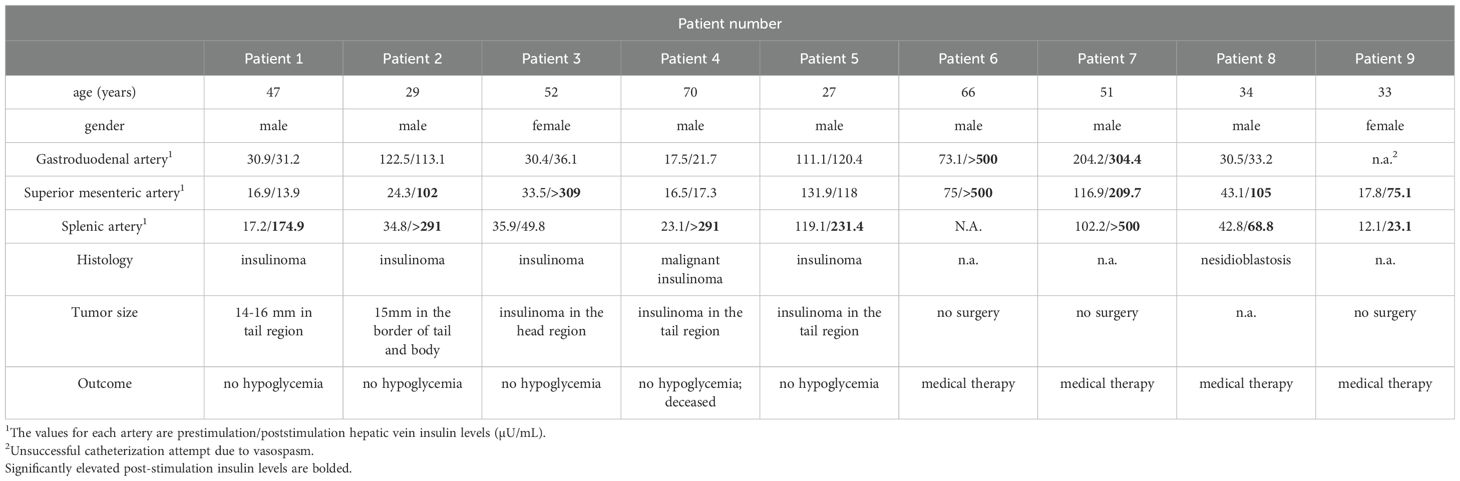
Table 1. Results of selective intraarterial calcium stimulation and patient outcome.
In the other four patients the insulin levels of the right hepatic vein increased to a near similar extent after calcium stimulation of each of the three arteries. This was considered compatible with hyperplasia of the pancreatic beta-cells indicating nesidioblastosis. In case of these patients, surgery was not performed except for one case; partial pancreatectomy was followed by medical treatment. Symptoms were prevented by Ca antagonist-diazoxide combination therapy (Table 1).
In all our insulinoma cases the ASVS procedure was diagnostic and helped in designing and performing the surgery and also confirmed the hormonal activity of the neuroendocrine tumors.
4 Discussion
Insulinoma is the most common functional neuroendocrine tumor of the pancreas and is the most common cause of endogenous hyperinsulinemic hypoglycemia (7). Prevention of neurological damage may be facilitated by early localization of the autonomic focus. In most cases surgical removal is curative, although the precise localization of the tumor is often challenging, as most tumors are below 2 centimeters in diameter. On the contrary, non-functioning pancreatic neuroendocrine tumors tend to be larger, therefore are more easily detectable with conventional imaging, still being recognized later due to the lack of symptoms. Insulinomas have an outstanding surgical curability with a reported 5-year disease-free survival rate of 100% due to the relatively low percentage of malignancies (3, 22).
Nesidioblastosis was first described in children and neonates, characterized by beta-cell hyperplasia and hypertrophy. The extremely rare focal cases might be treated surgically, but in the majority of the cases pharmaceutical approach needs to be implemented (23, 24). Diffuse hyperplasia of the pancreatic islet cells is often difficult to identify with routine imaging techniques, therefore in cases of nesidioblastosis ASVS is a particularly useful diagnostic tool. During ASVS insulin level elevation was found to be significantly higher in insulinomas than in nesidioblastosis (25). We found comparably marked insulin elevation in two of the nesidioblastosis cases. EUS is a relatively new technique. It is minimally invasive, can identify neoplasms smaller than 2 cm with a high sensitivity and specificity. It also allows tissue sampling for further histological evaluation. However, the sensitivity of EUS can vary from 40% to 92.6% depending on the tumor’s location. Its accuracy is also highly dependent on the examiner’s expertise and cannot be used to assess distant metastases (18, 26, 27). Furthermore, in the absence of hyperechogenic lesions it has also limited use in the diagnosis of nesidioblastosis (23, 28, 29).
ASVS provides information about hormonal activity of the lesion as well, and thus helps localize the tumor and might help in a more precise surgical approach with a significant decrease of reoperations (30). Another study published by Morera et al. found a 90.9% sensitivity for ASVS in localizing the tumor, which is higher than the one obtained by several studies with EUS. Moreover, its sensitivity was comparable to that of intraoperative ultrasound (IOUS) performed together with palpation (31). Although it has a 47-60% sensitivity, the locally attainable octreotide scintigraphy performed in two of our cases failed to detect and localize the insulinoma (3, 17). According to several studies involving 10-20 patients, the ASVS method’s overall accuracy is around 90%. In a meta-analysis involving 339 patients a sensitivity of 93% and specificity of 86% was found (3, 32, 33). Those cases where standard imaging techniques could not detect a solitary lesion and during ASVS equally increased insulin concentrations were obtained by calcium stimulation on more than one supplying artery, were considered nesidioblastosis (24). In these patients, no tumors were found during laparotomy either. Moreover, after conservative therapy the hypoglycemic symptoms relieved, which also supports our theory.
Of course there are limitations of this technique as well. Hatoko et al. tried lower doses of calcium administration because of adverse reactions, such as nausea, hypoglycemia, hypercalcemia (34). Due to the invasive nature of the examination complication of vessel punctuation, such as bleeding or hematoma can also occur. In addition, false negative and positive results can also be found, caused by technical flaws or anatomical variants, although these are rare in case of investigations performed in skilled and well-equipped centers (35). Complications of ASVS are very rare; according to Perkov et al., complication rate is negligible, but certain precautions are needed (36). In a study of seventeen patients no complications occurred after performing ASVS, data which correlates well with our findings (37).
Novel imaging techniques using somatostatin-receptors, like octreotide-scan; 68Ga-DOTATATE positron emission tomography (PET) or 68Ga-DOTATOC PET are recently used for the detection and follow-up of neuroendocrine tumors. According to a study, Exendin-4 PET/CT was superior to 68Ga-DOTATATE PET/CT and 18F-FDG PET/CT for the localization of the insulinoma, particularly in case of small and G2 tumors (38). Exendin-4 is a molecular tracer which targets glucagon-like peptide-1 receptor (GLP-1R), which has the highest expression on insulinoma beta islet cells and consequently has a very high sensitivity and specificity in localizing pancreatic insulinomas. Sensitivity can be as high as 97.7%, which exceeds any other imaging method. 68Ga-NOTA-exendin-4 PET/CT is currently the most sensitive imaging method for preoperative localization of insulinomas with a sensitivity of 97.7%. However, the availability of these techniques for detecting insulinomas is limited (39, 40). The expression of GLP-1R is higher in nesidioblastosis than in normal pancreatic tissue, but lower than in insulinoma cases, which can be also a drawback of this imaging method (41).
Molecular imaging is an emerging and promising tool in the detection of insulinomas; however, a significant percentage of insulinomas do not express somatostatin receptors (41). GLP-1R is overexpressed in 93% of the cases, consequently GLP-1 PET/CT improves insulinoma detectability vastly; however, overexpression is only present in 36% of patients with metastases and/or malignant lesions, making the method less informative in the rare but more malevolent malignant cases (41–43). Moreover, metastatic insulinomas often lack GLP-1 receptors, and often SST2 receptor overexpression can be found (positive SRS scan in 73%) (44).
Albeit in almost every case the combination of different imaging techniques is required, in the preoperative phase the precise localization of the insulinomas is unachievable in 10-27% of the cases (14). In a systematic review of 6222 cases evaluated between 1960 and 2011, ASVS localized correctly 84.7% of insulinomas, when applied, with a mean sensitivity of 89.2% (14). ASVS might provide additional functional information in MEN-1 cases when multiple neuroendocrine neoplasms are present in the pancreas and distinction is needed between potential functioning and non-functioning tumors (3).
There are different viewpoints about the best methods to localize the tumor; the available diagnostic procedures are different in every center, and the success rate can be highly dependent on the centers’ preparedness and experience (3, 22, 45). In the presented case series, our institution has served as referral center for neuroendocrine tumors, which explains the high success rate in localizing insulinomas and recognizing nesidioblastosis cases, which underscores the importance of the centralized management of rare endocrine tumors like insulinoma.
To avoid the late exocrine and endocrine pancreas function insufficiency and to facilitate postoperative healing, the best curing procedure is the pancreas saving surgical intervention, for which the exact localization of the tumor is indispensable. In the most recent European Neuroendocrine Tumor Society (ENETS) guidance paper, as first-line treatment modality for patients with preoperatively localized insulinomas a minimally invasive surgical approach is strongly suggested; laparoscopic procedures are reported to be safe and effective treatment options (7, 13, 14, 46).
The prevalence of nesidioblastosis is growing; the incidence increases after bariatric surgery (23, 47). In our institution we found a relatively high number of nesidioblastosis cases among the investigated hyperinsulinemic patients. In nesidioblastosis surgical intervention does not lead to complete healing (48). Preoperative screening is fundamental to avoid unnecessary surgery. Diazoxide reduces insulin secretion by indirect action on beta-cells and enhances glycolysis. Long-acting somatostatin analogues (SSAs) (octreotide, lanreotide and pasireotide) may prevent hypoglycemia when the insulinoma tumor cells express somatostatin receptors subtype 2 (14, 17). For metastatic insulinoma cases peptide receptor radionuclide therapy (PRRT) with 177Lu-DOTATATE and everolimus can be considered in advanced, progressive insulinoma cases when hypoglycemia is refractory to SSAs (7).
In a recent study of Andreassen et al., the tumors of 80 patients showed less staining for insulin and proinsulin in malignant insulinoma cases vs. benign lesions, possibly due to a diminished insulin storage capacity; to the contrary, glucagon staining was present only in malignant tumors. Malignancy is also associated with a lack of staining for CgA and higher Ki-67 staining as a result of poor differentiation (15). These findings also underscore the usefulness and importance of the ASVS technique.
In our series of patients ASVS provided important functional information and could successfully localize the origin of the elevated insulin levels, which were usually higher in localized insulinomas, then in nesidioblastosis. No complications occurred during ASVS. Although the number of patients studied is relatively small, according to our results ASVS is still an effective tool when the source of insulin over-secretion cannot be localized with non-invasive imaging. This is in line with the most recent ENETS recommendation (7).
One limitation of our case series investigation is that several, recently available imaging methods were not, or just partially performed (EUS, IOUS, radionucleotide-labeled techniques), so true comparison of these methods cannot be estimated. The limited number of cases is also a handicap of our study.
5 Conclusions
The localization of insulinoma is fundamental, as the treatment of choice is the surgical removal of the tumor. ASVS remains a reliable tool in localization and possesses important additional functional information that are not achievable with the use of other, novel and more expensive imaging techniques.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author/s.
Ethics statement
The studies involving humans were approved by Institutional Review Board of the University of Debrecen. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
SH: Writing – original draft. EB: Writing – review & editing. ÁD: Methodology, Writing – review & editing. LS: Methodology, Writing – review & editing. PF: Methodology, Writing – review & editing. EN: Conceptualization, Writing – review & editing. FG: Investigation, Writing – review & editing. ZK: Investigation, Writing – review & editing. JT: Investigation, Writing – review & editing. HB: Investigation, Writing – review & editing. MB: Conceptualization, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Service FJ, McMahon MM, O’Brien PC, Ballard DJ. Functioning insulinoma—Incidence, recurrence, and long-term survival of patients: A 60-year study. Mayo Clin Proc. (1991) 66:711–9. doi: 10.1016/s0025-6196(12)62083-7
2. Chen LJ, Han YD, Zhang M. Diagnosis value preoperative localization of insulinoma by diffusion-weighted imaging: A pilot study. Med (United States). (2020) 99:E23048. doi: 10.1097/MD.0000000000023048
3. Zhao K, Patel N, Kulkarni K, Gross JS, Taslakian B. Essentials of insulinoma localization with selective arterial calcium stimulation and hepatic venous sampling. J Clin Med. (2020) 9:3091. doi: 10.3390/jcm9103091
4. Niederle B, Selberherr A, Bartsch DK, Brandi ML, Doherty GM, Falconi M, et al. Multiple endocrine neoplasia type 1 and the pancreas: diagnosis and treatment of functioning and non-functioning pancreatic and duodenal neuroendocrine neoplasia within the MEN1 syndrome - an international consensus statement. Neuroendocrinology. (2021) 111:609–30. doi: 10.1159/000511791
5. Sada A, Habermann EB, Szabo Yamashita T, Thompson GB, Lyden ML, Foster TR, et al. Comparison between sporadic and multiple endocrine neoplasia type 1–associated insulinoma. J Am Coll Surg. (2022) 235:756–63. doi: 10.1097/XCS.0000000000000307
6. Sada A, Glasgow AE, Vella A, Thompson GB, McKenzie TJ, Habermann EB. Malignant insulinoma: A rare form of neuroendocrine tumor. World J Surg. (2020) 44:2288–94. doi: 10.1007/s00268-020-05445-x
7. Hofland J, Falconi M, Christ E, Castaño JP, Faggiano A, Lamarca A, et al. European neuroendocrine tumor society (ENETS) 2023 guidance paper for functioning pancreatic neuroendocrine tumour syndromes. J Neuroendocrinol. (2023) 35(8):e13318. doi: 10.1111/jne.13318
8. Dizon AM, Kowalyk S, Hoogwerf BJ. Neuroglycopenic and other symptoms in patients with insulinomas. Am J Med. (1999) 106:307–10. doi: 10.1016/s0002-9343(99)00021-2
9. Hirshberg B, Livi A, Bartlett DL, Libutti SK, Alexander HR, Doppman JL, et al. Forty-eight-hour fast: The diagnostic test for insulinoma. J Clin Endocrinol Metab. (2000) 85:3222–6. doi: 10.1210/jcem.85.9.6807
10. Bakatselos SO. Hypoglycemia unawareness. Diabetes Res Clin Pract. (2011) 93:S92–96. doi: 10.1016/S0168-8227(11)70020-1
11. Luca VG, Kwadwo A, Guillaume NP, Damian W, Emanuel C. Clinical presentation of 54 patients with endogenous hyperinsulinaemic hypoglycaemia: A neurological chameleon (observational study). Swiss Med Wkly. (2018) 148:w14682. doi: 10.4414/smw.2018.14682
12. Cryer PE, Axelrod L, Grossman AB, Heller SR, Montori VM, Seaquist ER, et al. Evaluation and management of adult hypoglycemic disorders: An endocrine society clinical practice guideline. J Clin Endocrinol Metab. (2009) 94:709–28. doi: 10.1210/jc.2008-1410
13. de Carbonnières A, Challine A, Cottereau AS, Coriat R, Soyer P, Abou Ali E, et al. Surgical management of insulinoma over three decades. Hpb. (2021) 23:1799–806. doi: 10.1016/j.hpb.2021.04.013
14. Mehrabi A, Fischer L, Hafezi M, Dirlewanger A, Grenacher L, Diener MK, et al. A systematic review of localization, surgical treatment options, and outcome of insulinoma. Pancreas. (2014) 43:675–86. doi: 10.1097/MPA.0000000000000110
15. Andreassen M, Ilett E, Wiese D, Slater EP, Klose M, Hansen CP, et al. Surgical management, preoperative tumor localization, and histopathology of 80 patients operated on for insulinoma. J Clin Endocrinol Metab. (2019) 104:6129–38. doi: 10.1210/jc.2019-01204
16. Walker MP, Shenoy V, Metz DC, Stanley CA, Fraker D, Chandrasekhara V, et al. Case presentation of 8-year follow up of recurrent Malignant duodenal Insulinoma and lymph node metastases and literature review of Malignant Insulinoma management. BMC Endocr Disord. (2022) 22:310. doi: 10.1186/s12902-022-01219-9
17. McAuley G, Delaney H, Colville J, Lyburn I, Worsley D, Govender P, et al. Multimodality preoperative imaging of pancreatic insulinomas. Clin Radiol. (2005) 60:1039–50. doi: 10.1016/j.crad.2005.06.005
18. Sotoudehmanesh R, Hedayat A, Shirazian N, Shahraeeni S, Ainechi S, Zeinali F, et al. Endoscopic ultrasonography (EUS) in the localization of insulinoma. Endocrine. (2007) 31:238–41. doi: 10.1007/s12020-007-0045-4
19. Luo Y, Pan Q, Yao S, Yu M, Wu W, Xue H, et al. Glucagon-like peptide-1 receptor PET/CT with 68 ga-NOTA-exendin-4 for detecting localized insulinoma: A prospective cohort study. J Nucl Med. (2016) 57:715–20. doi: 10.2967/jnumed.115.167445
20. Doppman JL, Chang R, Fraker DL, Norton JA, Alexander HR, Miller DL, et al. Localization of insulinomas to regions of the pancreas by intra-arterial stimulation with calcium. Ann Intern Med. (1995) 123:269–73. doi: 10.7326/0003-4819-123-4-199508150-00004
21. Sung YM, Do YS, Lee MK, Shin SW, Liu WC, Choo SW, et al. Selective intra-arterial calcium stimulation with hepatic venous sampling for preoperative localization of insulinomas. Korean J Radiol. (2003) 4:101–8. doi: 10.3348/kjr.2003.4.2.101
22. Crippa S, Zerbi A, Boninsegna L, Capitanio V, Partelli S, Balzano G, et al. Surgical management of insulinomas: Short- and long-term outcomes after enucleations and pancreatic resections. Arch Surg. (2012) 147:261–6. doi: 10.1001/archsurg.2011.1843
23. Dravecka I, Lazurova I. Nesidioblastosis in adults. In: Neoplasma, vol. 61. SAP - Slovak Academic Press (2014). p. 252–6. doi: 10.4149/neo_2014_047
24. Dieterle MP, Husari A, Prozmann SN, Wiethoff H, Stenzinger A, Röhrich M, et al. Diffuse, adult-onset nesidioblastosis/non-insulinoma pancreatogenous hypoglycemia syndrome (NIPHS): review of the literature of a rare cause of hyperinsulinemic hypoglycemia. Biomedicines. (2023) 11:1732. doi: 10.3390/biomedicines11061732
25. Thompson SM, Vella A, Thompson GB, Rumilla KM, Service FJ, Grant CS, et al. Selective arterial calcium stimulation with hepatic venous sampling differentiates insulinoma from nesidioblastosis. J Clin Endocrinol Metab. (2015) 100:4189–97. doi: 10.1210/jc.2015-2404
26. Rösch T, Lightdale CJ, Botet JF, Boyce GA, Sivak MV, Yasuda K, et al. Localization of pancreatic endocrine tumors by endoscopic ultrasonography. N Engl J Med. (1992) 326:1721–6. doi: 10.1056/NEJM199206253262601
27. Téllez-Ávila F, Acosta-Villavicencio G, Chan C, Hernández-Calleros J, Uscanga L, Valdovinos-Andraca F, et al. Diagnostic yield of endoscopic ultrasound in patients with hypoglicemia and insulinoma suspected. Endosc Ultrasound. (2015) 4:52. doi: 10.4103/2303-9027.151349
28. Kann PH, Rothmund M, Zielke A. Endoscopic ultrasound imaging of insulinomas: Limitations and clinical relevance. Exp Clin Endocrinol Diabetes. (2005) 113:471–4. doi: 10.1055/s-2005-865752
29. McLean AM, Fairclough PD. Endoscopic ultrasound in the localisation of pancreatic islet cell tumours. Best Pract Research: Clin Endocrinol Metab. (2005) 19(2):177–93. doi: 10.1016/j.beem.2004.11.012
30. Morita S, Machida H, Kuwatsuru R, Saito N, Suzuki K, Iihara M, et al. Preoperative localization of pancreatic insulinoma by super selective arterial stimulation with venous sampling. Abdom Imaging. (2007) 32:126–8. doi: 10.1007/s00261-006-9040-0
31. Morera J, Guillaume A, Courtheoux P, Palazzo L, Rod A, Joubert M, et al. Preoperative localization of an insulinoma: Selective arterial calcium stimulation test performance. J Endocrinol Invest. (2016) 39:455–63. doi: 10.1007/s40618-015-0406-4
32. Kirchhoff TD, Merkesdal S, Frericks B, Brabant G, Scheumann G, Galanski M, et al. Der Kalziumstimulationstest (ASVS) bei Insulinomen des Pankreas: Vergleich mit der bildgebenden Lokalisationsdiagnostik. Radiologe. (2003) 43:301–5. doi: 10.1007/s00117-003-0881-z
33. Wiesli P, Brändle M, Schmid C, Krähenbühl L, Furrer J, Keller U, et al. Selective arterial calcium stimulation and hepatic venous sampling in the evaluation of hyperinsulinemic hypoglycemia: potential and limitations. J Vasc Intervent Radiol. (2004) 15:1251–6. doi: 10.1097/01.RVI.0000140638.55375.1E
34. Hatoko T, Murakami T, Sone M, Yabe D, Masui T, Nakamoto Y, et al. Low-dose selective arterial calcium stimulation test for localizing insulinoma: A single-center experience of five consecutive cases. Internal Med. (2020) 59:2397–403. doi: 10.2169/internalmedicine.4396-20
35. Guettier JM, Kam A, Chang R, Skarulis MC, Cochran C, Alexander HR, et al. Localization of insulinomas to regions of the pancreas by intraarterial calcium stimulation: The NIH experience. J Clin Endocrinol Metab. (2009) 94:1074–80. doi: 10.1210/jc.2008-1986
36. Perkov D. Localization of pancreatic insulinomas with arterial stimulation by calcium and hepatic venous sampling - presentation of a single centre experience. Acta Endocrinol (Bucharest). (2016) 12:55–62. doi: 10.4183/aeb.2016.55
37. Tseng LM, Chen JY, Won JGS, Tseng HS, Yang AH, Wang SE, et al. The role of intra-arterial calcium stimulation test with hepatic venous sampling (IACS) in the management of occult insulinomas. Ann Surg Oncol. (2007) 14:2121–7. doi: 10.1245/s10434-007-9398-4
38. Chang L, Bi X, Li S, Tong Q, Gu Y, He Z, et al. The comparison of three different molecular imaging methods in localization and grading of insulinoma. Front Endocrinol (Lausanne). (2023) 14. doi: 10.3389/fendo.2023.1163176
39. Haug AR, Cindea-Drimus R, Auernhammer CJ, Reincke M, Wängler B, Uebleis C, et al. The Role of 68Ga-DOTATATE PET/CT in suspected neuroendocrine tumors. J Nucl Med. (2012) 53:1686–92. doi: 10.2967/jnumed.111.101675
40. Gabriel M, Decristoforo C, Kendler D, Dobrozemsky G, Heute D, Uprimny C, et al. 68Ga-DOTA-Tyr3-octreotide PET in neuroendocrine tumors: Comparison with somatostatin receptor scintigraphy and CT. J Nucl Med. (2007) 48:508–18. doi: 10.2967/jnumed.106.035667
41. Reubi JC, Perren A, Rehmann R, Waser B, Christ E, Callery M, et al. Glucagon-like peptide-1 (GLP-1) receptors are not overexpressed in pancreatic islets from patients with severe hyperinsulinaemic hypoglycaemia following gastric bypass. Diabetologia. (2010) 53:2641–5. doi: 10.1007/s00125-010-1901-y
42. Reubi JC, Waser B. Concomitant expression of several peptide receptors in neuroendocrine tumours: Molecular basis for in vivo multireceptor tumour targeting. Eur J Nucl Med Mol Imaging. (2003) 30:781–93. doi: 10.1007/s00259-003-1184-3
43. Antwi K, Fani M, Heye T, Nicolas G, Rottenburger C, Kaul F, et al. Comparison of glucagon-like peptide-1 receptor (GLP-1R) PET/CT, SPECT/CT and 3T MRI for the localisation of occult insulinomas: evaluation of diagnostic accuracy in a prospective crossover imaging study. Eur J Nucl Med Mol Imaging. (2018) 45:2318–27. doi: 10.1007/s00259-018-4101-5
44. Wild D, Christ E, Caplin ME, Kurzawinski TR, Forrer F, Brändle M, et al. Glucagon-like peptide-1 versus somatostatin receptor targeting reveals 2 distinct forms of Malignant insulinomas. J Nucl Med. (2011) 52:1073–8. doi: 10.2967/jnumed.110.085142
45. Ravi K, Britton BJ. Surgical approach to insulinomas: Are pre-operative localisation tests necessary? Ann R Coll Surg Engl. (2007) 89:212–7. doi: 10.1308/003588407X179008
46. Tamburrino D, Partelli S, Renzi C, Crippa S, Muffatti F, Perali C, et al. Systematic review and meta-analysis on laparoscopic pancreatic resections for neuroendocrine neoplasms (PNENs). Expert Rev Gastroenterol Hepatol. (2017) 11:65–73. doi: 10.1080/17474124.2017.1253473
47. Cao J, Kim C, Huynh T, Frugoli A, Henson H, Valdez V, et al. BYPASS-OMA: hypoglycemic hyperinsulinemic nesidioblastosis after gastric bypass surgery - A case report and review of the literature. Case Rep Endocrinol. (2022) 2022. doi: 10.1155/2022/5472304
Keywords: insulinoma, selective intraarterial calcium stimulation, ASVS, nesidioblastosis, hyperinsulinemic hypoglycemia, pancreas, functioning neuroendocrine tumor
Citation: Halmi S, Berta E, Diószegi Á, Sira L, Fülöp P, Nagy EV, Győry F, Kanyári Z, Tóth J, Bhattoa HP and Bodor M (2024) Single center experience in localization of insulinoma by selective intraarterial calcium stimulation angiography - a case series of 15 years. Front. Endocrinol. 15:1305958. doi: 10.3389/fendo.2024.1305958
Received: 02 October 2023; Accepted: 30 September 2024;
Published: 21 October 2024.
Edited by:
Bojana Popovic, University of Belgrade, SerbiaReviewed by:
Giulia Puliani, IRCCS Regina Elena National Cancer Institute, ItalyPeter Igaz, Semmelweis University, Hungary
Copyright © 2024 Halmi, Berta, Diószegi, Sira, Fülöp, Nagy, Győry, Kanyári, Tóth, Bhattoa and Bodor. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Miklós Bodor, bWJvZG9yQGdtYWlsLmNvbQ==