 Shufan Li
Shufan Li Peng Wang
Peng Wang Jing Wang
Jing Wang Jinlei Zhao2
Jinlei Zhao2 Xing Wang
Xing Wang
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Endocrinol., 26 January 2024
Sec. Diabetes: Molecular Mechanisms
Volume 15 - 2024 | https://doi.org/10.3389/fendo.2024.1289254
This article is part of the Research TopicMechanistic and Physiological Implications of Insulin Resistance in Metabolic DiseasesView all 9 articles
Objective: To systematically evaluate the effects of mind-body exercise on risk factors of metabolic syndrome such as insulin resistance.
Methods: Web of Science, PubMed, The Cochrane Library, EBSCO host, Embase, China Knowledge Network, China Biomedical Literature Database, Wanfang, and VIP were searched for the period from the establishment of the database to 1 July 2023, and randomized controlled trials of mind-body exercise interventions in patients with metabolic syndrome were collected. We applied the Cochrane Risk of Bias tool RoB2 to evaluate the methodological quality of the included literature and used RevMan5.4 software and Stata15.1 for statistical analysis.
Results: A total of 14 randomized controlled trials with 1148 patients were included in this study. Meta-analysis showed that mind-body exercise significantly improved insulin resistance [SMD=-0.78, 95% CI: (-1.13, -0.43), P<0.0001], waist circumference [SMD=-2.20, 95% CI: (-3.34, -1.06), P=0.0001], body mass index (SMD=-1.50, 95% CI: [-2.03, -0.97), P<0.00001], systolic blood pressure [SMD=-3.65, 95% CI: 9-5.56, -1.74), P=0.0002], diastolic blood pressure [SMD=-3.32, 95% CI: (- 3.77, -2.87), P<0.00001], fasting blood glucose [SMD=-0.57, 95% CI: (-0.99, -0.15), P=0.008], triglycerides [SMD=-0.27, 95% CI: (-0.46, -0.08), P=0.004], high-density lipoprotein cholesterol [SMD=0.58, the 95% CI: (0.28, 0.87), P=0.0001]. Subgroup analysis showed that the intervention program with exercise form of fitness qigong, exercise cycle of 24-48 weeks, and exercise frequency of 6-7 times/week could significantly improve each risk factor.
Conclusion: Mind-body exercise is effective in improving risk factors in patients with metabolic syndrome. Current evidence recommends an intervention program of low to moderate intensity fitness qigong, with 6-7 sessions per week for 24-48 weeks in patients with metabolic syndrome.
Systematic review registration: https://www.crd.york.ac.uk/prospero/, identifier CRD42023454135.
Metabolic syndrome (MetS) refers to a pathological condition in which various metabolic components in the body are abnormally aggregated, including central obesity, hypertension, glucose or insulin metabolism disorders, and lipid abnormalities. The pathological mechanisms involve insulin resistance and obesity (1, 2). MetS is a significant risk factor for cardiovascular diseases, type 2 diabetes, stroke, and other conditions (3, 4). It is also an important clinical indicator for predicting overall mortality and cardiovascular mortality (5). The prevalence of MetS is on the rise globally, with the prevalence in Chinese adults increasing from 8.8% in 1991 to 29.3% in 2015 (6). In the United States, the prevalence among adults is 35%, reaching close to 50% in the population aged 60 and above (7).
Currently, preventive and therapeutic measures for MetS primarily involve non-pharmacological and pharmacological interventions. Non-pharmacological treatments mainly focus on dietary control and exercise intervention, while pharmacological treatments target blood sugar, blood lipids, blood pressure, and other related aspects. Exercise is a crucial component of health management for individuals with MetS, offering the advantages of simplicity, feasibility, and minimal side effects (8). Moderate-intensity exercise has been shown to effectively reduce the occurrence of MetS (9–11). Mind-body exercise refers to activities that simultaneously engage both the body and consciousness. The core of this exercise involves training individuals to consciously control the activities of various parts of their bodies, achieving a harmonious unity of body and mind (12). Mind-body exercises are characterized by gentle and slow movements (moderate to low-intensity exercise), coordinated body movements with breathing, and common examples include yoga, Tai Chi, and fitness qigong (12, 13). Existing research has found that mind-body exercise can improve specific risk factors for MetS, such as obesity, hypertension, hyperglycemia, and dyslipidemia (14–17). Regular mind-body exercise can reduce body fat, enhance insulin sensitivity and reactivity in peripheral target tissues through skeletal muscle exercise, increase the utilization of glucose, alleviate insulin resistance, and improve skeletal muscle blood flow, promoting glucose uptake and metabolism in skeletal muscles, thereby ameliorating metabolic syndrome (18).
Different mind-body exercises have varying intervention effects. Yoga has a significant impact on waist circumference (WC) and systolic blood pressure (SBP) in individuals with MetS (19). Tai Chi can improve obesity, blood pressure, blood sugar, and blood lipids in community-dwelling adults at risk for MetS (15). Fitness qigong can improve WC, blood pressure, and lipid abnormalities in MetS patients (17). By reviewing previous research, it is noted that the forms of mind-body exercises included in previous meta-analyses were limited, outcome indicators were restricted, insulin resistance was not analyzed, and the impact of various elements of exercise on outcome indicators was not investigated. To address these gaps, this study aims to answer the following questions: Can mind-body exercise effectively improve insulin resistance and obesity in MetS patients? Can it effectively regulate blood pressure, blood sugar, and blood lipids in MetS patients? Which type of mind-body exercise intervention is more suitable for MetS patients? This study will comprehensively collect published randomized controlled trials, systematically evaluate the intervention effects of mind-body exercise on insulin resistance and other risk factors for metabolic syndrome, and provide scientific exercise programs for the prevention and improvement of metabolic syndrome, offering reliable evidence for clinical practice.
This study followed the international guidelines for writing Meta-analyses (20) for the selection and use of research methods, PROSPERO registration number: CRD42023454135.
Two researchers conducted searches across nine databases, including Web of Science, PubMed, The Cochrane Library, EBSCO host, Embase, China Knowledge Network, China Biomedical Literature Database, Wanfang, and VIP. and supplemented with literature retrospectives, all of which were searched for the period of construction through July 1, 2023. The English search utilized the following subject terms and their free word combinations: Exercise, physical activity, movement, Mind-Body Exercise, Yoga, Traditional sports, Tai chi, Baduanjin, Wuqinxi, Yijinjing, Liuzijue, Qigong, Metabolic Syndrome, Insulin Resistance Syndrome X, randomized controlled trial.
(1) The study subjects were patients diagnosed with metabolic syndrome by authoritative criteria. (2) The interventions were mind-body exercises, including yoga, tai chi, and fitness qigong (Baduanjin, Wuqinxi, and Yijinjing); and the control group could be treated with usual care, health promotion, etc. (3) The main outcome indicators were insulin resistance and obesity. Insulin resistance was selected as insulin resistance index (HoMA-IR), and waist circumference (WC) and body mass index (BMI) were selected for obesity. Secondary outcome indicators were blood pressure, blood glucose, and blood lipids. Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were selected for blood pressure, fasting blood glucose (FBG) for blood glucose, and triglycerides (TG) and high-density lipoprotein cholesterol (HDL-C) for blood lipids. (4) The type of literature included was randomized controlled trial (RCT).
(1) Animal experiments. (2) Review and conference literature. (3) Combined intervention studies with interventions other than exercise. (4) Literature data could not be extracted.
Literature inclusion and exclusion were strictly based on predefined criteria. Two individuals independently screened the literature, cross-checked the screened literature, and any discrepancies were resolved through discussion and evaluation by a third person. The screened literature was subjected to data extraction, cross-checking and if there were discrepancies in the data, the data was verified by a third person. Data extracted included: type of study, age, diagnostic criteria, sample size, intervention method and type of study. Data extracted included:(1) basic information (first author, year of publication, country, age, diagnostic criteria); (2) experimental information (sample size, intervention, exercise variables); (3) outcome indicators.
Adopting the Cochrane Handbook of Systematic Evaluation 6.3 criteria for evaluating risk of bias, the Revised Cochrane risk-of-bias tool for randomized trials (RoB2) was used to assess the risk of bias in 5 areas. The methodological quality of the inclusion literature was evaluated independently by 2 researchers, and if there were disagreements, they were resolved by a third person in a joint discussion.
Data extracted from the literature were subjected to systematic Meta-analysis in Review Manager 5.4 software. Measures with the same measurement tool were expressed as weighted mean difference (MD) and its 95% confidence interval (CI), while measures with different measurement tools were expressed as standardized mean difference (SMD) and its 95% CI. The supplement and clarification have been added to the data processing. In this study, Cochran’s Q test was employed, along with the I2 statistic, to assess the magnitude of heterogeneity. When P > 0.1 and I2 < 50%, it was considered that there was small heterogeneity among the studies, and a fixed-effects model was used to combine the effect size (the fixed-effects model assumes that all included studies share a common true effect size, or that, apart from random error, the observed effect sizes are all true effect sizes). When P < 0.1 or I2 > 50%, it was considered that there was significant heterogeneity among the studies, and a random-effects model was used to combine the effect size (the random-effects model assumes that the true effect size varies with the inclusion of different studies). Publication bias test was performed using the Begg test of Stata15.1 software.
The computer searched yielded 4247 documents, and 3499 documents were obtained after removing duplicates; 3359 documents were excluded after initial screening by reading the titles and abstracts, and 140 documents were left; after further full-text re-screening, 126 documents that did not meet the inclusion criteria were excluded, and finally 14 documents were included in the meta-analysis. see Figure 1 for details.
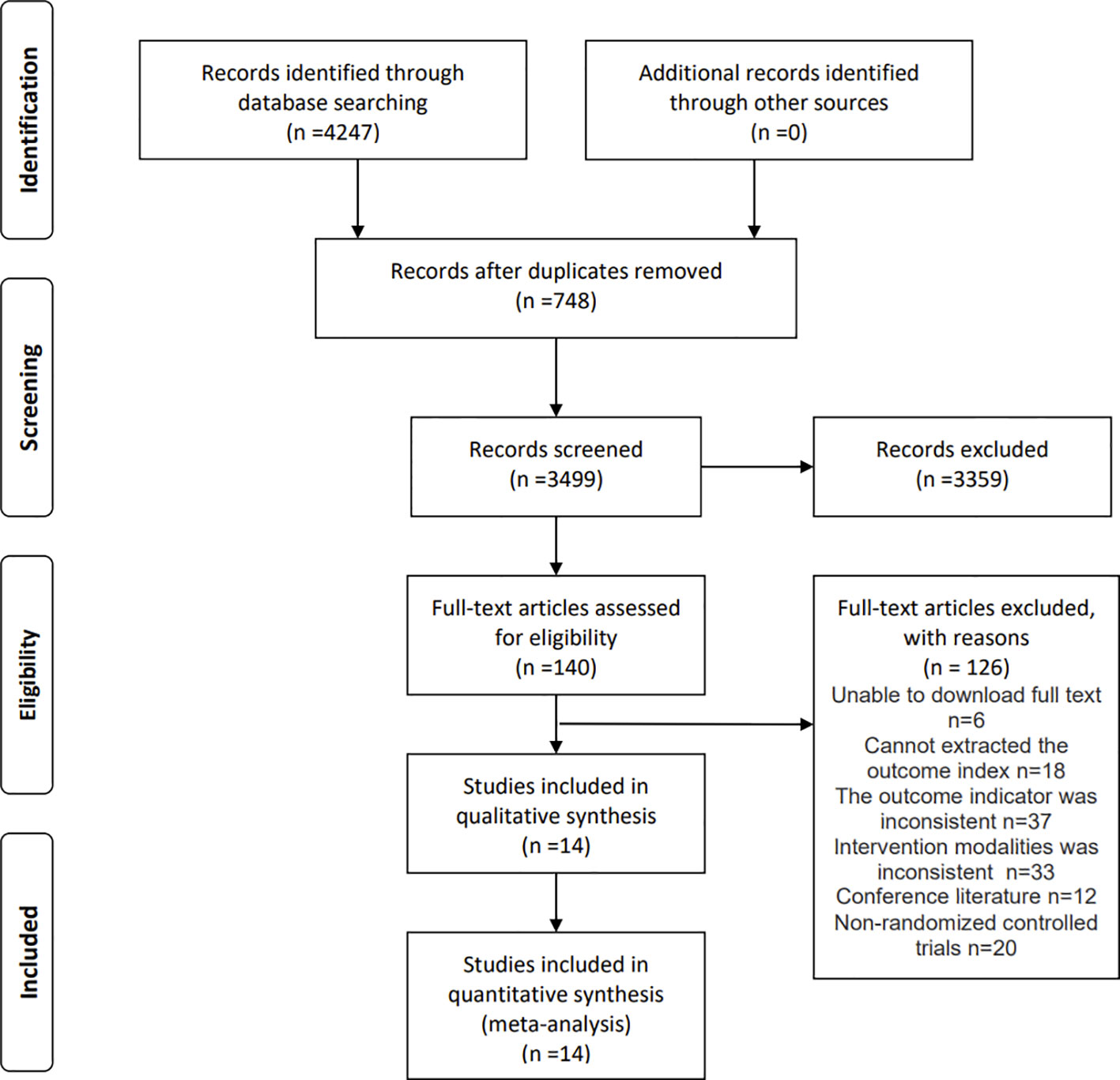
Figure 1 Flow Diagram of Literature Search.
Table 1 presents the basic information of the 14 included RCTs, involving a total of 1,148 participants aged between 40 and 73. Interventions included yoga, tai chi, baduanjin, wuqinxi, and yijinjing, conducted over periods ranging from 10 to 48 weeks, with 2 to 7 sessions per week and durations between 30 and 90 minutes.
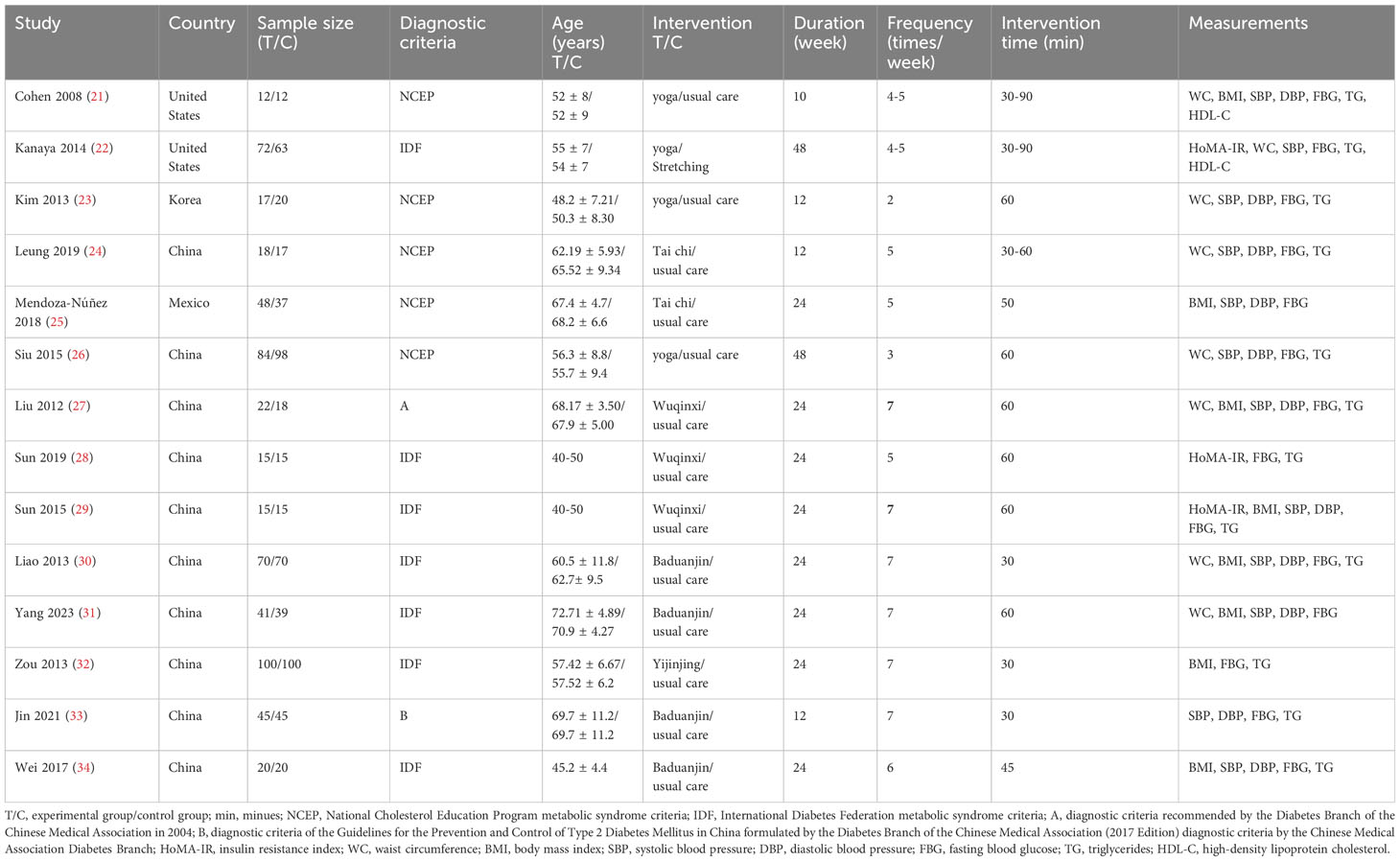
Table 1 Basic Characteristics of the Literature.
As shown in Figure 2, a total of 14 randomized controlled trials were included. One study (25) had unclear bias in the randomization process, and all studies were rated as “Some concerns” for bias in the implementation of the predefined interventions. No studies showed bias related to outcome data missing, outcome measurement bias, or selective reporting bias.
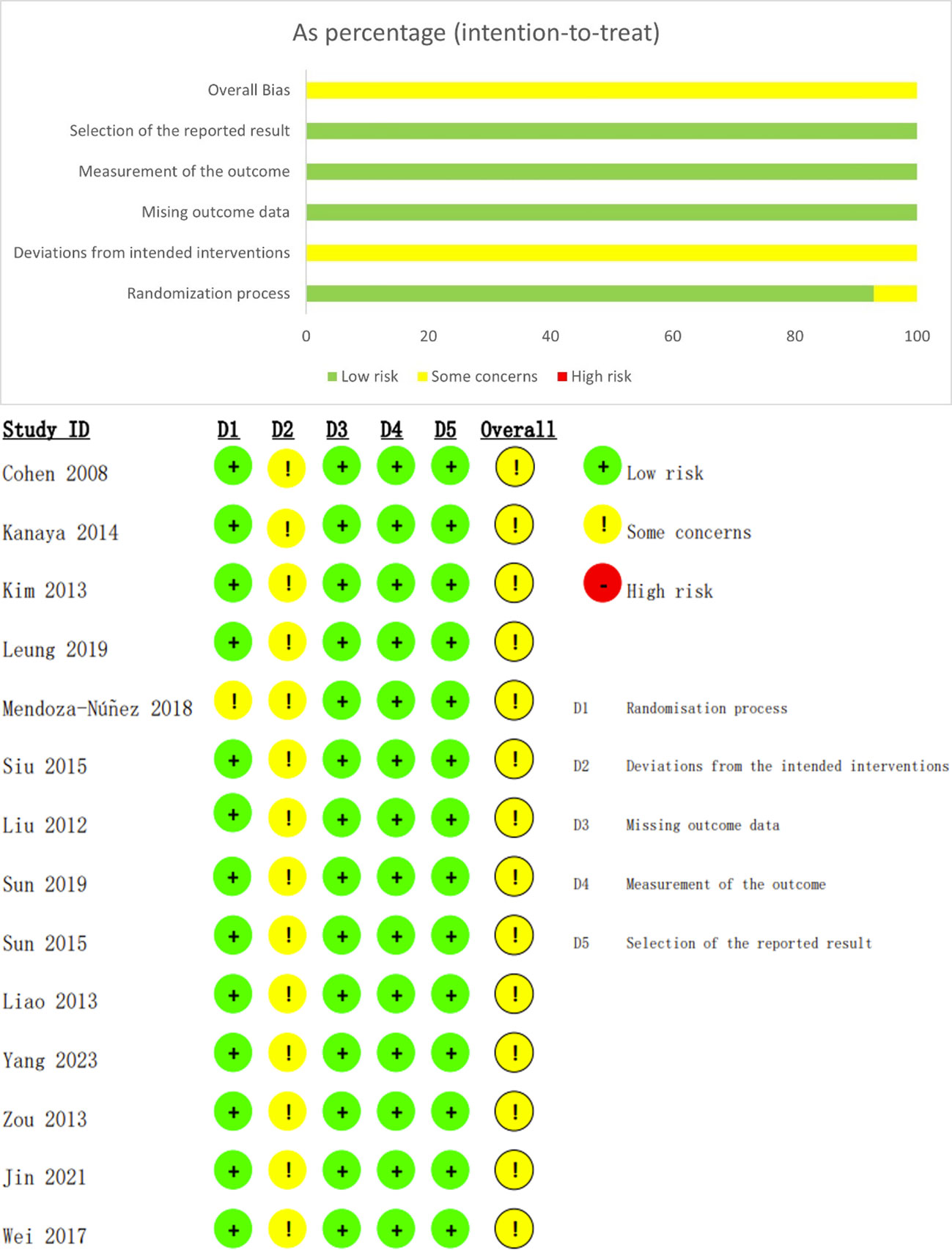
Figure 2 Risk of bias assessment of included studies.
The three included papers (comprising 8 studies) reported the results of the Insulin Resistance Index (Figure 3), with low heterogeneity between studies (I²=41%, P=0.11), and they were analyzed using a fixed-effects model. Mind-body exercise reduced insulin resistance in patients with metabolic syndrome [SMD=-0.78, 95% CI: (-1.13, -0.43), P<0.0001], and the difference was statistically significant compared to the control group.
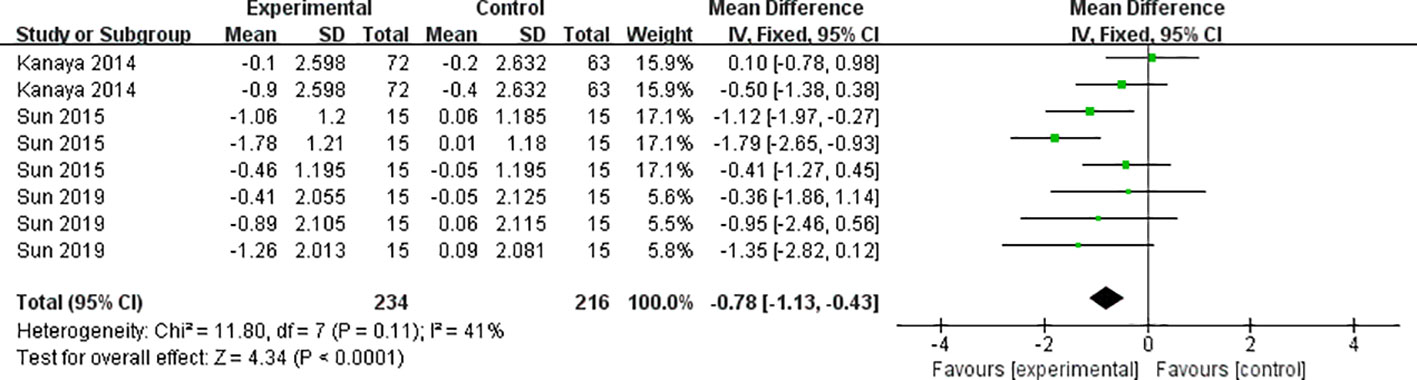
Figure 3 Meta-analysis of insulin resistance.
The eight included papers (comprising 12 studies) reported the results of waist circumference (Figure 4), with high heterogeneity between studies (I²=60%, P=0.004), and they were analyzed using a random-effects model. Mind-body exercise reduced waist circumference in patients with metabolic syndrome [SMD=-2.20, 95% CI: (-3.34, -1.06), P=0.0001], and the difference was statistically significant compared to the control group.
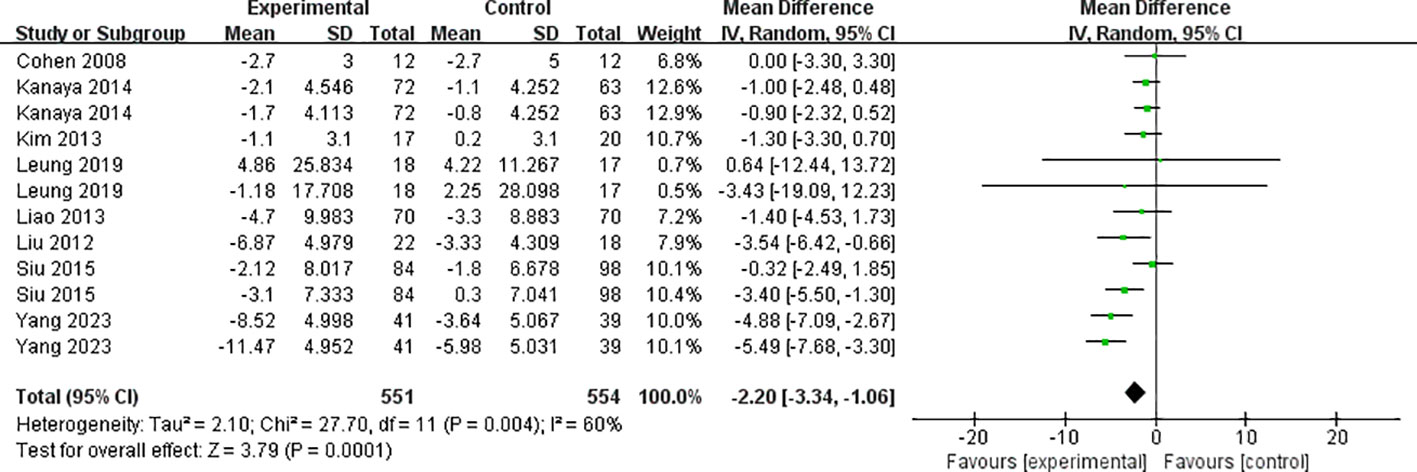
Figure 4 Meta-analysis of waist circumference.
The eight included papers (consisting of 11 studies) reported the results of body mass index (Figure 5), with high heterogeneity between studies (I² = 71%, P = 0.0002), and they were analyzed using a random-effects model. Mind-body exercise reduced body mass index in patients with metabolic syndrome [SMD = -1.50, 95% CI: (-2.03, -0.97), P < 0.00001], and the difference was statistically significant compared to the control group.
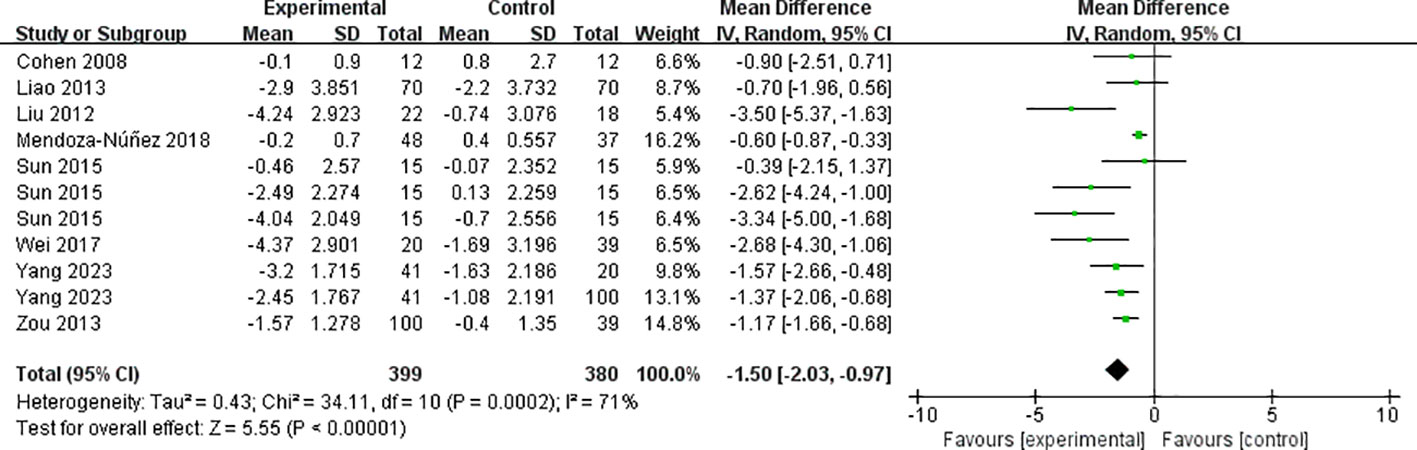
Figure 5 Meta-analysis of body mass index.
The twelve included papers (comprising 17 studies) reported the results of systolic blood pressure (Figure 6), with high heterogeneity between studies (I² = 75%, P < 0.00001), and they were analyzed using a random-effects model. Mind-body exercise reduced systolic blood pressure in patients with metabolic syndrome [SMD = -3.65, 95% CI: (-5.56, -1.74), P = 0.0002], and the difference was statistically significant compared to the control group.
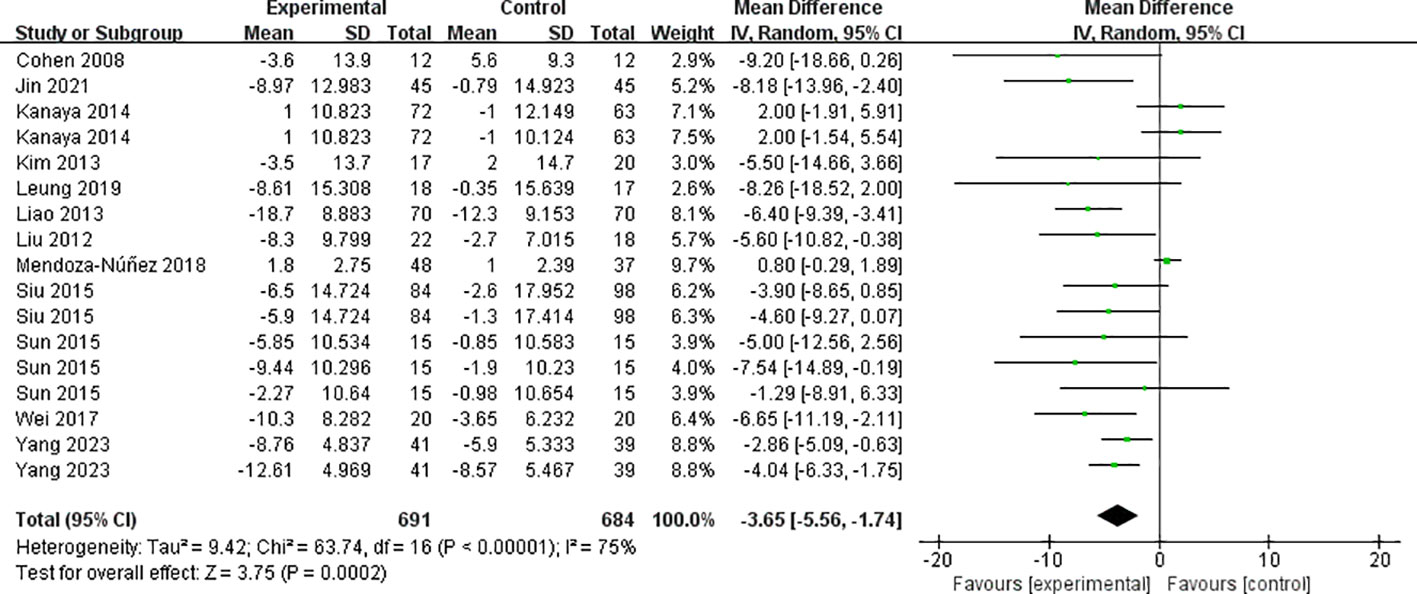
Figure 6 Meta-analysis of systolic blood pressure.
The eleven included papers (comprising 15 studies) reported the results of diastolic blood pressure (Figure 7), with low heterogeneity between studies (I² = 28%, P = 0.15), and they were analyzed using a fixed-effects model. Mind-body exercise reduced diastolic blood pressure in patients with metabolic syndrome SMD = -3.32, 95% CI: (-3.77, -2.87), P < 0.00001], and the difference was statistically significant compared to the control group.
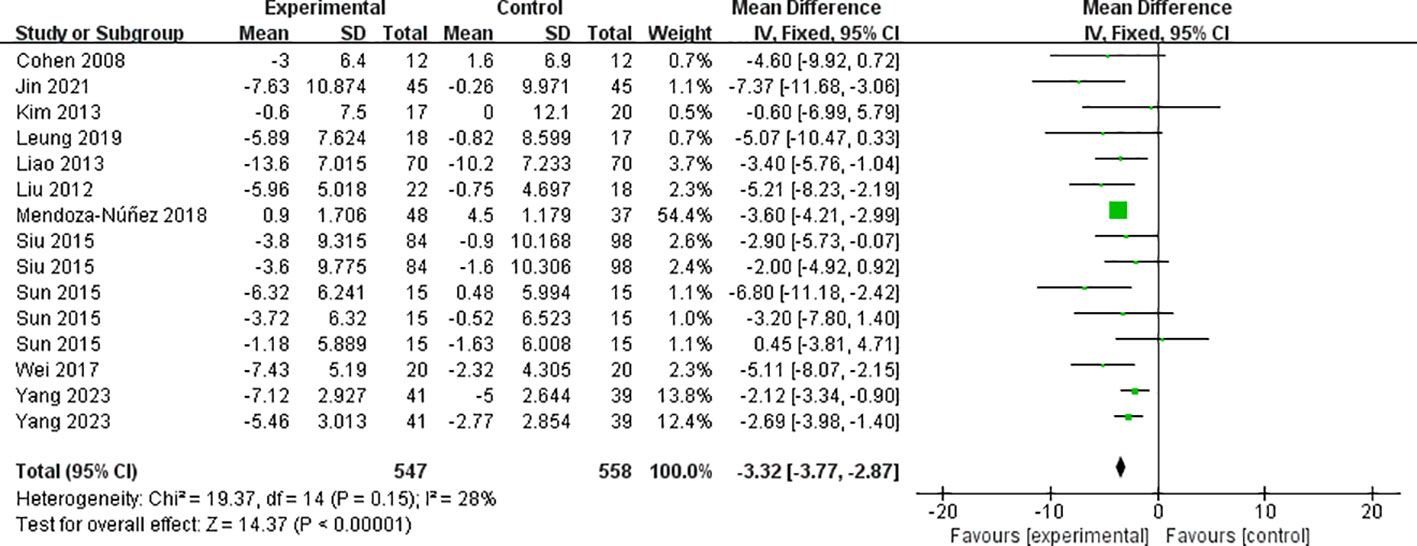
Figure 7 Meta-analysis of diastolic blood pressure.
All 14 included papers (comprising 21 studies) reported the results of fasting blood glucose (Figure 8), with high heterogeneity between studies (I² = 94%, P < 0.00001), and they were analyzed using a random-effects model. Mind-body exercise reduced fasting blood glucose in patients with metabolic syndrome [SMD = -0.57, 95% CI: (-0.99, -0.15), P = 0.008], and the difference was statistically significant compared to the control group.
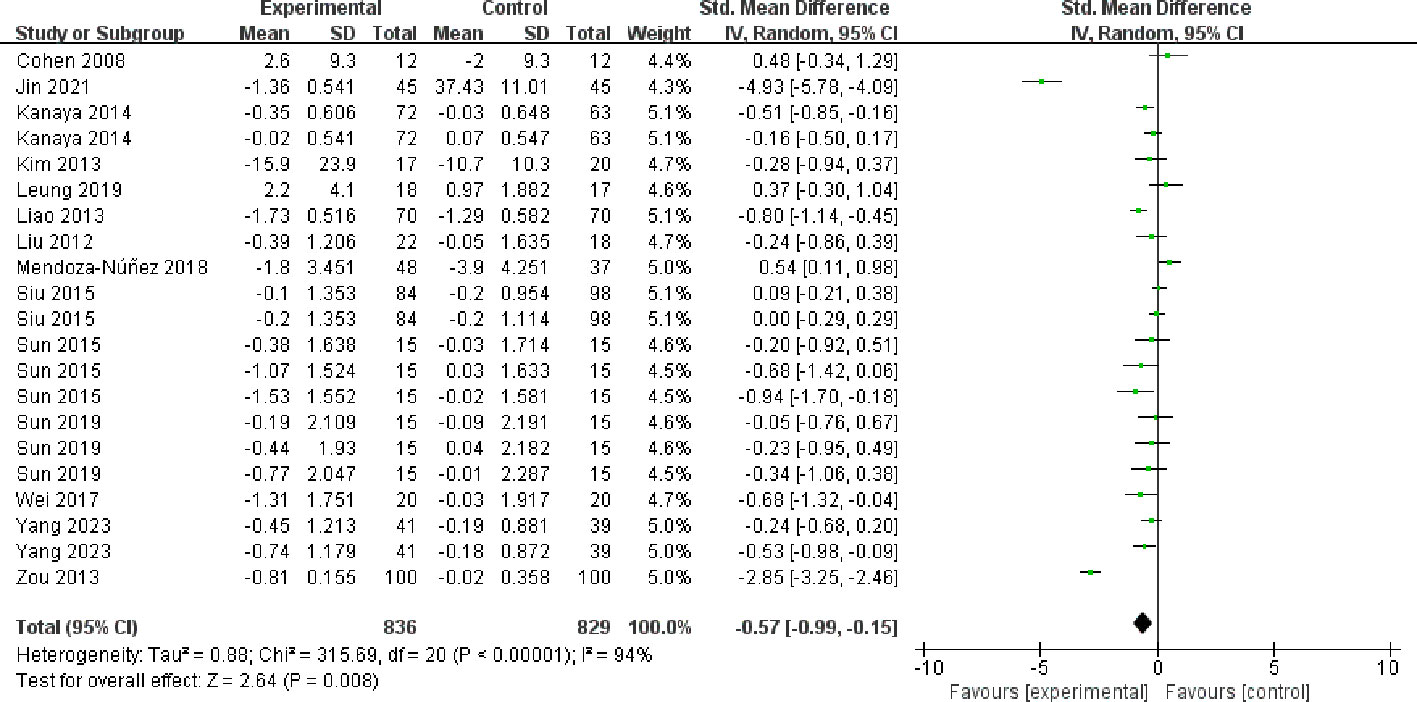
Figure 8 Meta-analysis of fasting blood glucose.
The twelve included papers (comprising 18 studies) reported the results of triglycerides (Figure 9), with high heterogeneity between studies (I² = 62%, P = 0.0003), and they were analyzed using a random-effects model. Mind-body exercise reduced triglycerides in patients with metabolic syndrome [SMD = -0.27, 95% CI: (-0.46, -0.08), P = 0.004], and the difference was statistically significant compared to the control group.
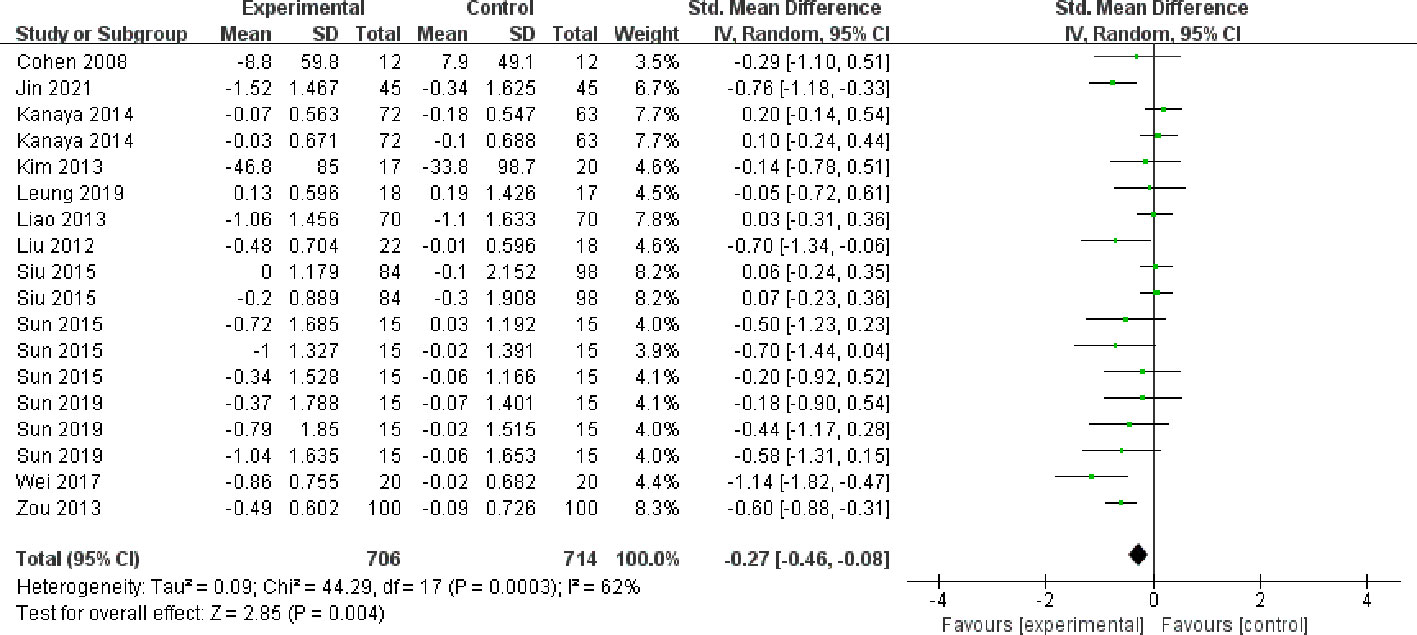
Figure 9 Meta-analysis of triglycerides.
The twelve included papers (comprising 19 studies) reported the results of High-density lipoprotein cholesterol (Figure 10), with high heterogeneity between studies (I² = 84%, P < 0.00001), and they were analyzed using a random-effects model. Mind-body exercise could improve High-density lipoprotein cholesterol in patients with metabolic syndrome [SMD = 0.58, 95% CI: (0.28, 0.87), P = 0.0001], and the difference was statistically significant compared to the control group.
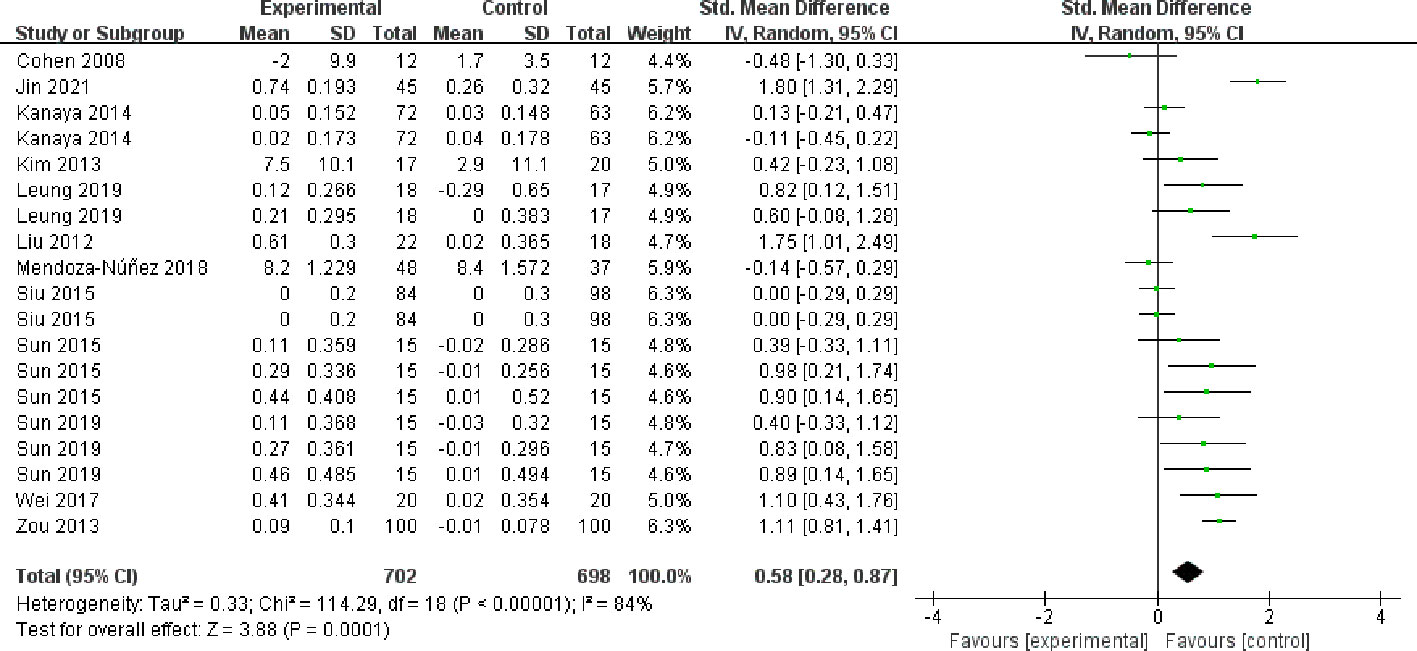
Figure 10 Meta-analysis of High-density lipoprotein cholesterol.
To explore possible reasons for heterogeneity, this paper presents subgroup analyses of highly heterogeneous outcome indicators. The intervention effect of mind-body exercise on patients with metabolic syndrome may be affected by different exercise forms, exercise intensity, exercise cycle, exercise frequency, exercise time, and other factors. However, these factors were not analyzed in subgroups because exercise intensity and exercise time were similar among the studies.
As shown in Table 2, exercise intervention programs may contribute to heterogeneity. Concerning exercise form, fitness qigong exhibited significant differences in all outcome indicators, yoga in waist circumference, and tai chi in fasting blood glucose, compared with controls. Regarding the exercise period, 10-12 weeks showed significant differences in systolic blood pressure, triglycerides, and HDL cholesterol, while 24-48 weeks exhibited significant differences in all outcome indicators compared with controls. In terms of exercise frequency, there was a significant difference in systolic blood pressure at 2-3 times/week, in BMI at 4-5 times/week, and in all outcome indicators at 6-7 times/week compared to the control group.
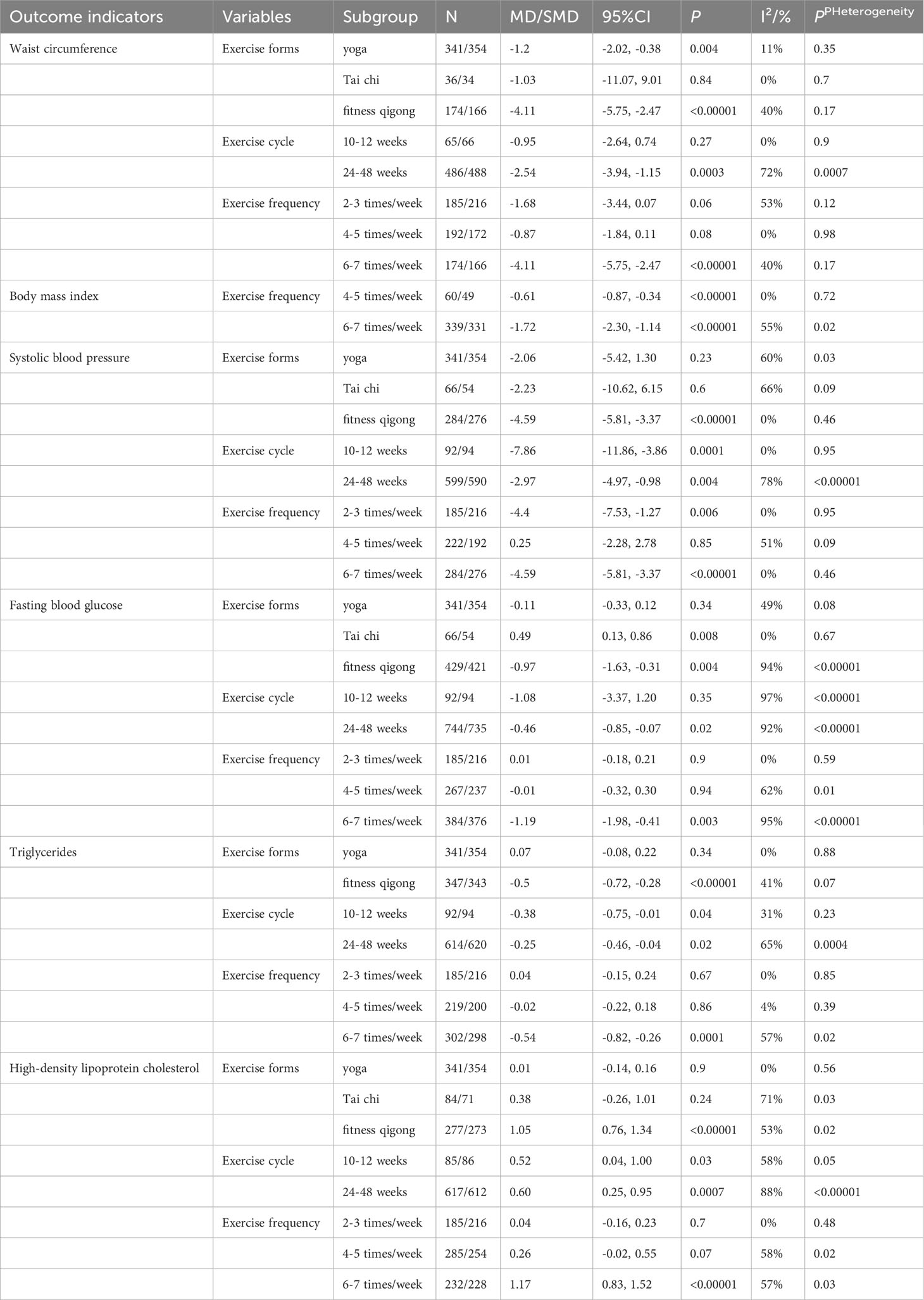
Table 2 Results of subgroup moderated effects.
To assess the stability of the meta-analysis results, sensitivity tests were conducted for all outcome indicators. The results showed that, by systematically excluding individual studies and reanalyzing, the point estimates of the combined effect size remained within the original effect size’s 95% confidence interval. Therefore, the results of the meta-analysis for each outcome indicator appear to be stable.
In this study, the insulin resistance index included fewer than 10 studies, and the test efficacy was insufficient for a publication bias test. Therefore, only the other outcome indexes were tested for publication bias. The results of the Begg test (Table 3) showed that P > 0.05, suggesting that there was no publication bias in the study.
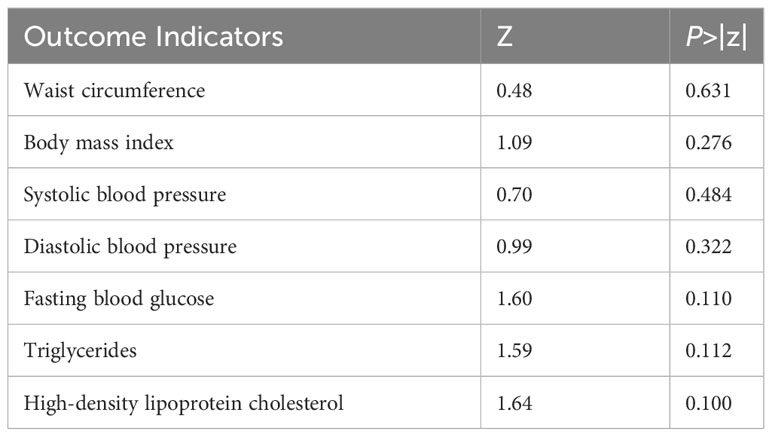
Table 3 Results of Begg’s test.
The results of this study demonstrate that mind-body exercise can reduce insulin resistance and obesity in patients with MetS and regulate blood pressure, fasting blood glucose, and lipid levels. These findings partially align with previous research (35). Existing studies have indicated the potential clinical effectiveness of mind-body exercise in improving MetS risk factors (35). Yoga has been shown to reduce waist circumference and systolic blood pressure in MetS patients (19). Tai Chi has antioxidative and blood glucose-lowering effects in older individuals with MetS (25). Additionally, fitness qigong effectively improves waist circumference, blood pressure, diastolic blood pressure, triglycerides, and HDL-C levels in MetS patients (17, 36). Furthermore, the impact of mind-body exercise on metabolic risk factors has been confirmed in other disease populations as well (37, 38).
This study reveals that the intervention effects of mind-body exercise on MetS exhibit dose-dependent and selective influences. It is recommended to carefully select exercise intervention plans for different outcome indicators. For improving insulin resistance, waist circumference, BMI, fasting blood glucose, and HDL-C, the preferred intervention is fitness qigong, 6-7 times per week, for 24-48 weeks. For improving SBP and TG, the preferred intervention is fitness qigong, 6-7 times per week, for 10-12 weeks. Mind-body exercise emphasizes the combination of consciousness and spirit, focusing on conscious control of body activities, achieving mind-body unity (39). Research suggests that mind-body exercise can reduce inflammation, alleviate oxidative stress, lower circulating free fatty acids, thereby improving insulin resistance and obesity. Additionally, mind-body exercise enhances glucose utilization, lowers blood glucose levels (17, 29, 40, 41), induces the synthesis of APOA1-carrying lipoproteins, and increases HDL-C levels (17, 33). On the neurological level, mind-body exercise can alter markers of sympathetic and parasympathetic nervous system activity (42), increase sensitivity to stress reflexes, decrease arterial tension and peripheral resistance, thereby improving blood pressure levels (43). Numerous studies indicate that fitness qigong exercise can improve MetS risk factors and reduce the risk of cardiovascular disease in MetS patients (16, 17, 28, 34, 44–47). Long-term regular mind-body exercise can improve MetS risk factors, and meta-analysis (17, 36) also supports the results of this study. Fitness qigong interventions for longer durations (≥6 months) have a better effect on improving BMI, HDL-C, and cholesterol, and 12-24 weeks of wuqinxi intervention can significantly reduce blood pressure.
This study also found that yoga effectively reduces waist circumference, tai chi effectively lowers fasting blood glucose, and fitness qigong effectively improves various risk factors, which is inconsistent with previous results. Existing meta-analyses have found that in healthy populations and those with a history and risk of cardiovascular disease or MetS, yoga can improve obesity, blood pressure, lipid abnormalities, glycated hemoglobin, and insulin resistance, but not fasting blood glucose (14, 48). Tai Chi can improve obesity, blood pressure, blood glucose, and lipid abnormalities (15). In MetS populations, yoga can improve waist circumference and systolic blood pressure (19), and fitness qigong can improve waist circumference, blood pressure, and lipid abnormalities (17), with no significant impact on fasting blood glucose. The different effects of various mind-body exercises on MetS risk factors may be due to differences in the types of studies included. This study only included randomized controlled trials (RCTs), while studies by Cramer (2014, 2016) included RCTs, randomized crossover trials, and cluster randomized trials. Differences in the health status of the study participants may also directly influence the different results, as this study only included MetS patients, while some studies included healthy individuals, those at risk of MetS, and MetS patients. The variations in the health status of the study participants could lead to different outcomes.
In summary, mind-body exercise can effectively improve risk factors such as insulin resistance in patients with MetS. The current evidence recommends the adoption of moderate-intensity fitness qigong, with an intervention frequency of 6-7 times per week for 24-48 weeks for MetS patients. This study suggests that the above exercise regimen could be promoted in populations at risk of MetS to prevent the occurrence and progression of metabolic syndrome. It can also serve as a basis for clinical guidance on exercise for individuals with MetS, providing tailored exercise prescriptions for improving various symptoms in middle-aged and older individuals with MetS. However, this study has several limitations: the literature search was conducted in both Chinese and English, potentially leading to incomplete literature inclusion. Additionally, the age, condition, and duration of MetS in the patients were not specified, and the intervention effects of different mind-body exercises may be influenced by age, condition, and disease duration.
Mind-body exercise is effective in improving risk factors in patients with metabolic syndrome. Current evidence recommends an intervention program of low to moderate intensity fitness qigong, with 6-7 sessions per week for 24-48 weeks in patients with metabolic syndrome.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
SL: Conceptualization, Data curation, Writing – original draft, Methodology. PW: Data curation, Methodology, Writing – original draft. JW: Data curation, Writing – original draft. JZ: Data curation, Writing – original draft. XW: Data curation, Writing – original draft. TL: Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. Shanghai Key Lab of Human Performance (Shanghai University of Sport) (NO. 11DZ2261100).
We gratefully acknowledge the support of Shanghai Key Lab of Human Performance (Shanghai University of Sport).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Saklayen MG. The global epidemic of the metabolic syndrome. Curr hypertension Rep (2018) 20(2):12. doi: 10.1007/s11906-018-0812-z
2. Samson SL, Garber AJ. Metabolic syndrome. Endocrinol Metab Clinics North America (2014) 43(1):1–23. doi: 10.1016/j.ecl.2013.09.009
3. Zafar U, Khaliq S, Ahmad HU, Manzoor S, Lone KP. Metabolic syndrome: an update on diagnostic criteria, pathogenesis, and genetic links. Hormones (Athens Greece) (2018) 17(3):299–313. doi: 10.1007/s42000-018-0051-3
4. Xu H, Yin Y, Zhao Y. Meta-analysis of exercise effect on the cardiovascular risk factors in adults with metabolic syndrome. China Sport Sci Technol (2020) 56(5):59–70. doi: 10.16470/j.csst.2020065
5. Supriya R, Yu AP, Lee PH, Lai CW, Cheng KK, Yau SY, et al. Yoga training modulates adipokines in adults with high-normal blood pressure and metabolic syndrome. Scandinavian J Med Sci sports (2018) 28(3):1130–8. doi: 10.1111/sms.13029
6. Huang J, Huang JLW, Withers M, Chien K-L, Trihandini I, Elcarte E, et al. Prevalence of metabolic syndrome in Chinese women and men: a systematic review and meta-analysis of data from 734 511 individuals. Lancet (2018) 392:S14. doi: 10.1016/S0140-6736(18)32643-6
7. Ford ES, Giles WH, Dietz WH. Prevalence of the metabolic syndrome among US adults: findings from the third National Health and Nutrition Examination Survey. Jama (2002) 287(3):356–9. doi: 10.1001/jama.287.3.356
8. Sagawa N, Rockette-Wagner B, Azuma K, Ueshima H, Hisamatsu T, Takamiya T, et al. Physical activity levels in American and Japanese men from the ERA-JUMP Study and associations with metabolic syndrome. J Sport Health Sci (2020) 9(2):170–8. doi: 10.1016/j.jshs.2019.09.007
9. Miyatake N, Saito T, Wada J, Nishikawa H, Matsumoto S, Miyachi M, et al. Linkage between oxygen uptake at ventilatory threshold and muscle strength in subjects with and without metabolic syndrome. Acta Med Okayama (2007) 61(5):255–9. doi: 10.18926/AMO/32895
10. Zhang C, Wang H, Ding X, Shaosheng L, Shixiang W, Zhi X. Effects of exercise and high-fat dietary intervention on myocardial oxidative stress in male rats with metabolism syndrome. Chin J Rehabil Med (2022) 37(8):1039–45. doi: 10.3969/j.issn.1001-1242.2022.08.005
11. Chen D, Zhang H, Shao J, Tang L, Wu J, Ye Z. Summary of the best evidence of diet and physical activity management in patients with metabolic syndrome. Zhejiang Da Xue Xue Bao Yi Xue Ban (2022) 51(01):27–37. doi: 10.3724/zdxbyxb-2021-0378
12. Tanaka H, Suksom D. Mind-body exercises. Am J Lifestyle Med (2015) 9(6):459. doi: 10.1177/1559827615591153
13. Li JX, Hong Y, Chan KM. Tai chi: physiological characteristics and beneficial effects on health [J]. Br J sports Med (2001) 35(3):148–56. doi: 10.1136/bjsm.35.3.148
14. Chu P, Gotink RA, Yeh GY, Goldie SJ, Hunink MG. The effectiveness of yoga in modifying risk factors for cardiovascular disease and metabolic syndrome: A systematic review and meta-analysis of randomized controlled trials. Eur J Prev Cardiol (2016) 23(3):291–307. doi: 10.1177/2047487314562741
15. Chau JPC, Leung LYL, Liu X, Lo SHS, Choi KC, Zhao J, et al. Effects of Tai Chi on health outcomes among community-dwelling adults with or at risk of metabolic syndrome: A systematic review. Complement Ther Clin Pract (2021) 44:101445. doi: 10.1016/j.ctcp.2021.101445
16. Lee SH, Jeon Y, Huang CW, Cheon C, Ko SG. Qigong and tai chi on human health: an overview of systematic reviews. Am J Chin Med (2022) 50(8):1995–2010. doi: 10.1142/S0192415X22500859
17. Tao S, Li Z. Effects of qigong exercise on cardiovascular risk factors in patients with metabolic syndrome: A systematic review and meta-analysis. Front Physiol (2023) 14:1092480. doi: 10.3389/fphys.2023.1092480
18. Roberts CK, Hevener AL, Barnard RJ. Metabolic syndrome and insulin resistance: underlying causes and modification by exercise training. Compr Physiol (2013) 3(1):1–58. doi: 10.1002/cphy.c110062
19. Cramer H, Langhorst J, Dobos G, Lauche R. Yoga for metabolic syndrome: A systematic review and meta-analysis. Eur J Prev Cardiol (2016) 23(18):1982–93. doi: 10.1177/2047487316665729
20. Page MJ, Mckenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ (2021) 372:n71. doi: 10.1136/bmj.n71
21. Cohen BE, Chang AA, Grady D, Kanaya AM. Restorative yoga in adults with metabolic syndrome: a randomized, controlled pilot trial. Metab Syndr Relat Disord (2008) 6(3):223–9. doi: 10.1089/met.2008.0016
22. Kanaya AM, Araneta MR, Pawlowsky SB, Barrett-Connor E, Grady D, Vittinghoff E, et al. Restorative yoga and metabolic risk factors: the Practicing Restorative Yoga vs. Stretching for the Metabolic Syndrome (PRYSMS) randomized trial. J Diabetes Complications (2014) 28(3):406–12. doi: 10.1016/j.jdiacomp.2013.12.001
23. Kim HN, Ryu J, Kim KS, Song SW. Effects of yoga on sexual function in women with metabolic syndrome: a randomized controlled trial. J Sex Med (2013) 10(11):2741–51. doi: 10.1111/jsm.12283
24. Leung LY, Chan AW, Sit JW, Liu T, Taylor-Piliae RE. Tai Chi in Chinese adults with metabolic syndrome: A pilot randomized controlled trial. Complement Ther Med (2019) 46:54–61. doi: 10.1016/j.ctim.2019.07.008
25. Mendoza-Núñez VM, Arista-Ugalde TL, Rosado-Pérez J, Ruiz-Ramos M, Santiago-Osorio E. Hypoglycemic and antioxidant effect of Tai chi exercise training in older adults with metabolic syndrome. Clin Interv Aging (2018) 13:523–31. doi: 10.2147/CIA.S157584
26. Siu PM, Yu AP, Benzie IF, Woo J. Effects of 1-year yoga on cardiovascular risk factors in middle-aged and older adults with metabolic syndrome: a randomized trial. Diabetol Metab Syndr (2015) 7:40. doi: 10.1186/s13098-015-0034-3
27. Liu H. Correlation research on effect of wuqinxi exercise on cognitive function in old people with metabolic syndrome. J Wuhan Institute Phys Educ (2012) 46(10):56–61. doi: 10.15930/j.cnki.wtxb.2012.10.010
28. Sun Q. Exploration of the mechanism of improving cardiovascular function by Five Animal Play intervention in the context of general health–a case study of middle-aged men with MS. J Qilu Normal Univ (2019) 34(04):108–14. doi: 10.3969/j.issn.1008-2816.2019.04.017
29. Sun H. The effect and biological mechanism of wuqinxi's intervention on middle-aged men's metabolic syndrome. China Sport Sci Technol (2015) 51(04):86–92. doi: 10.16470/j.csst.201504012
30. Liao S, Liang Y, Xia L, Tan Y. Effects of the traditional Chinese medicine fitness method of Baduanjin on patients with metabolic syndrome. Modern J Integrated Traditional Chin Western Med (2013) 22(23):2560–1. doi: 10.3969/j.issn.1008-8849.2013.23.022
31. Yang Y, Zhang X. Effect of elderly care-and -attention exercises improving metabolic syndrome index. Liaoning J Traditional Chin Med (2023) 50(01):83–6. doi: 10.13192/j.issn.1000-1719.2023.01.024
32. Zou Z, Shi X, Zhang H. Clinical study of 100 cases of metabolic syndrome intervened by Yi Jin Jing. J Changchun Univ Traditional Chin Med (2013) 29(03):398–9. doi: 10.13463/j.cnki.cczyy.2013.03.085
33. Jin J, Li Y, Cen L, Xiaoge D, Qiang J. Study on the effect of health-care qigong baduanjin exercises on metabolic syndrome. J Guangzhou Univ Traditional Chin Med (2021) 38(07):1426–31.
34. Wei W. A study of the effects of Baduanjin exercises on middle-aged men with metabolic syndrome. Contemp Sports Technol (2017) 7(28):192–3. doi: 10.16655/j.cnki.2095-2813.2017.28.192
35. Anderson JG, Taylor AG. The metabolic syndrome and mind-body therapies: a systematic review. J Nutr Metab (2011) 2011:276419. doi: 10.1155/2011/276419
36. Zou L, Zhang Y, Sasaki JE, Yeung AS, Yang L, Loprinzi PD, et al. Wuqinxi qigong as an alternative exercise for improving risk factors associated with metabolic syndrome: A meta-analysis of randomized controlled trials. . Int J Environ Res Public Health (2019) 16(8):1396. doi: 10.3390/ijerph16081396
37. Lee JA, Kim JW, Kim DY. Effects of yoga exercise on serum adiponectin and metabolic syndrome factors in obese postmenopausal women. Menopause (New York NY) (2012) 19(3):296–301. doi: 10.1097/gme.0b013e31822d59a2
38. Littman AJ, Bertram LC, Ceballos R, Ulrich CM, Ramaprasad J, McGregor B, et al. Randomized controlled pilot trial of yoga in overweight and obese breast cancer survivors: effects on quality of life and anthropometric measures. Support Care Cancer (2012) 20(2):267–77. doi: 10.1007/s00520-010-1066-8
39. Zhu Y, Guo H. The mechanism of the application of the BaDuanJin in the rehabilitation of slow disease. Chin Manipulation Rehabil Med (2019) 10(07):64–6. doi: 10.19787/j.issn.1008-1879.2019.07.033
40. Dela F, Prats C, Helge JW. Exercise interventions to prevent and manage type 2 diabetes: physiological mechanisms. Med sport Sci (2014) 60:36–47. doi: 10.1159/000357334
41. Kirwan JP, Sacks J, Nieuwoudt S. The essential role of exercise in the management of type 2 diabetes. Cleve Clin J Med (2017) 84(7 Suppl 1):S15–S21. doi: 10.3949/ccjm.84.s1.03
42. Pal R, Singh SN, Chatterjee A, Saha M. Age-related changes in cardiovascular system, autonomic functions, and levels of BDNF of healthy active males: role of yogic practice. Age (Dordr) (2014) 36(4):9683. doi: 10.1007/s11357-014-9683-7
43. Khatri D, Mathur KC, Gahlot S, Jain S, Agrawal RP. Effects of yoga and meditation on clinical and biochemical parameters of metabolic syndrome. Diabetes Res Clin Pract (2007) 78(3):e9–10. doi: 10.1016/j.diabres.2007.05.002
44. Yu DD, You LZ, Huang WQ, Cao H, Wang FJ, Tang XQ, et al. Effects of traditional Chinese exercises on blood glucose and hemoglobin A1c levels in patients with prediabetes: A systematic review and meta-analysis. J Integr Med (2020) 18(4):292–302. doi: 10.1016/j.joim.2020.04.003
45. Ching SM, Mokshashri NR, Kannan MM, Lee KW, Sallahuddin NA, Ng JX, et al. Effects of qigong on systolic and diastolic blood pressure lowering: a systematic review with meta-analysis and trial sequential analysis. BMC Complement Med Ther (2021) 21(1):8. doi: 10.1186/s12906-020-03172-3
46. Yang Z, Huang K, Yang Y, Xu Q, Guo Q, Wang X. Efficacy of traditional Chinese exercise for obesity: A systematic review and meta-analysis. Front Endocrinol (Lausanne) (2023) 14:1028708. doi: 10.3389/fendo.2023.1028708
47. Yu J, Chun B, Lee D, Rokni L. Effect of baduanjin exercise on metabolic syndrome risk: A systematic review and meta-analysis of randomized controlled trials. Iran J Public Health (2023) 52(5):880–91. doi: 10.18502/ijph.v52i5.12705
Keywords: mind-body exercise, metabolic syndrome, insulin resistance, meta-analysis, randomized controlled trials
Citation: Li S, Wang P, Wang J, Zhao J, Wang X and Liu T (2024) Effect of mind-body exercise on risk factors for metabolic syndrome including insulin resistance: a meta-analysis. Front. Endocrinol. 15:1289254. doi: 10.3389/fendo.2024.1289254
Received: 05 September 2023; Accepted: 08 January 2024;
Published: 26 January 2024.
Edited by:
Hilda Ghadieh, University of Balamand, LebanonReviewed by:
Frederic Harb, University of Balamand, LebanonCopyright © 2024 Li, Wang, Wang, Zhao, Wang and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tong Liu, bGl1dG9uZ0BzaWNmbC5lZHUuY24=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.