
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol., 08 January 2024
Sec. Clinical Diabetes
Volume 14 - 2023 | https://doi.org/10.3389/fendo.2023.1306134
This article is part of the Research TopicThe Underlying Mechanisms and Novel Approaches for Diabetes and its Related ComplicationsView all 36 articles
 Sejeong Lee1†
Sejeong Lee1† Jaehyun Bae2†
Jaehyun Bae2† Seung Up Kim3,4Minyoung Lee5
Seung Up Kim3,4Minyoung Lee5 Yong-ho Lee5Eun Seok Kang5Bong-Soo Cha5
Yong-ho Lee5Eun Seok Kang5Bong-Soo Cha5 Byung-Wan Lee5*‡
Byung-Wan Lee5*‡Aim: Hepatic ketogenesis is a key metabolic pathway that regulates energy homeostasis. Some related controversies exist regarding the pathogenesis of metabolic-associated fatty liver disease (MAFLD). We aimed to investigate whether intact ketogenic capacity could reduce the risk of MAFLD based on transient electrography (TE) in patients with newly diagnosed type 2 diabetes (T2D).
Methods: A total of 361 subjects with newly diagnosed T2D were recruited and classified into two groups based on the median serum β-hydroxybutyrate (βHB) level, referred to as the intact and impaired ketogenesis groups. The glucometabolic relevance of ketogenic capacity and associations of the baseline serum β-HB and MAFLD assessed with TE were investigated.
Results: Compared to the impaired ketogenesis group, the intact ketogenesis group showed better insulin sensitivity, lower serum triglyceride levels, and higher glycated hemoglobin levels. The controlled attenuation parameter (CAP) was lower in the intact ketogenesis group without statistical significance (289.7 ± 52.1 vs. 294.5 ± 43.6; p=0.342) but the prevalence of moderate–severe steatosis defined by CAP ≥260 dB/m was significantly lower in the intact group. Moreover, intact ketogenesis was significantly associated with a lower risk of moderate–severe MAFLD after adjusting for potential confounders (adjusted odds ratio 0.55, 95% confidence interval 0.30–0.98; p=0.044).
Conclusion: In drug-naïve, newly diagnosed T2D patients, intact ketogenesis predicted a lower risk of moderate–severe MAFLD assessed by TE.
With pathophysiologic homeostasis of fatty acids (FAs), nonalcoholic fatty liver disease (NAFLD) develops due to the accumulation of overwhelmingly delivered FAs from peripheral tissues or de novo lipogenesis and the limited capacity of FA disposal in a milieu of metabolic disorders with no evidence of secondary causes (1). With advances in the understating of disease unmet requirements (2–4), growing interests and studies have accumulated regarding the recently proposed definition of metabolic-associated fatty liver disease (MAFLD) to achieve a more accurate representation of the underlying pathophysiology of fatty liver disease as metabolically driven (5).
Unlike pathological ketogenesis that mainly arises from acute hyperglycemic complications of diabetes in the absence or absolute deficiency of insulin, physiologic ketone bodies are produced under a fasting state, are utilized as compensatory energy sources for extrahepatic tissues, especially for the brain, and are considered to be related to beneficial metabolic effects, according to recent studies (6–8). In stable homeostatic states, ketogenesis could serve as an optimal pathway for the clearance of excess lipids, but it is often impaired and underutilized in specific subgroups of individuals (9–11). In the healthy liver with normal glucose tolerance status, FAs delivered into the liver are disposed of through β-oxidation resulting in the generation of ketone bodies, including acetone, acetoacetate, and β-hydroxybutyrate (βHB), along with down-regulation of de novo lipogenesis (6). However, in the metabolic dysregulated liver, FAs driven from peripheral tissues might be oxidized to carbon dioxide via the tricarboxylic acid (TCA) cycle, which promotes gluconeogenesis and increases plasma glucose concentrations (12, 13). Based on previous studies that looked at suppressed ketogenesis in individuals with fatty liver disease (14, 15) and the correlation between ketone bodies and anti-hepatic steatotic effects (16, 17), we recently demonstrated that intact ketogenesis might be associated with decreased risk of hepatic steatosis using non-image based specific MAFLD indices, including NAFLD liver fat scores, Framingham steatosis indices, and other measurements, in patients with newly diagnosed type 2 diabetes (T2D) (18). In the present study, we aimed to define MAFLD more accurately using transient elastography (TE), which is a more reliable method for assessment of the liver steatosis stage to elucidate whether the presence of ketogenesis influences hepatic steatosis in newly diagnosed T2D patients.
From the prospective cohort diabetes registry at the Severance Diabetes Center, a tertiary care hospital in Seoul, which was conducted on newly diagnosed glucose intolerance or diabetic patients, we evaluated the association between ketogenesis and risk of hepatic steatosis in patients with newly diagnosed T2D using a cross-sectional design. The cohort comprised patients who underwent a standardized mixed-meal stimulation test on their first visit to the diabetes center in 2009. The registry protocol required routine collection of blood samples at 0 and 90 minutes (basal and stimulated, respectively) to analyze glucose, insulin, and C-peptide levels.
The inclusion criteria of this study were as follows: aged 19 years or older, newly diagnosed with T2D according to the 2019 guidelines of the Korean Diabetes Association, serum βHB levels measured at the center since its availability in 2017, TE results measured within six months before or after the baseline measurement of βHB. Patients who had received organ transplantation or chemotherapy, as well as those who used steroids or had previously taken antidiabetic medications before the initial blood sampling or visited the emergency room due to hyperglycemia, were excluded. Additionally, we excluded those who were extreme outliers [i.e., alanine aminotransferase (ALT) ≥1,000 IU/L, triglycerides (TGs) ≥1,000 mg/dL], aged ≥80 years, and with glycated hemoglobin (HbA1c) ≥11% from the study. Finally, 361 newly diagnosed T2D patients were included as study participants. The study protocol was approved by the institutional review board of Severance Hospital (4–2022–1101). Informed consent was waived because of the retrospective nature of the study.
Patient data, such as age, sex, weight, height, and use of antidiabetic drugs or antihypertensive drugs at baseline, were collected by reviewing electronic medical records. The following laboratory variables were measured at baseline: serum HbA1c, creatinine, aspartate aminotransferase (AST), ALT, total cholesterol, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), TGs, urine albumin, urine creatinine, and serum βHB. Body mass index (BMI) was calculated as body weight divided by height squared (kg/m2) and the estimated glomerular filtration rate (eGFR) was assessed based on the four-variable modification of diet in the renal disease study formula. Glucometabolic parameters, including serum glucose, C-peptide, and insulin, were measured after overnight fasting and postprandial. The postprandial level was obtained 90 minutes after the mixed-meal test (Mediwell Diabetic Meal; Meail Dairies Co., Yeongdong-gun, Chungbuk, Korea) was given. The homeostasis model assessments of insulin resistance (HOMA-IR) index and HOMA-β were calculated to assess insulin resistance and pancreatic β-cell function.
The ketogenic capacity of the subject was assessed prior to the administration of diabetes medication by measuring the concentration of serum βHB, which is the most prevalent form of ketone bodies. The concentration of serum βHB in a fasting state was quantified with a commercial enzymatic assay from Landox Laboratories Ltd. (County Antrim, UK) and an Atellical CH 930 analyzer (Siemens Healthcare Diagnostics, Marburg, Germany). In cases where the concentration of βHB was below the lower limit of detection for the assay, a value of zero was recorded.
TE was performed by an experienced specialist without knowing the subject’s clinical details using a Fibroscan 501® (Echosens, Paris, France). The procedure was conducted with a standard probe and the final value was obtained using a standard procedure. The principles of controlled attenuation parameter (CAP) measurement for TE have been described previously (19, 20). Hepatic steatosis was categorized into four grades based on the CAP value [decibels per meter (dB/m)]: less than 238 dB/m for steatosis stage 0 (S0), 238 dB/m to 259 dB/m for steatosis stage 1 (S1, mild), 260 dB/m to 292 dB/m for steatosis stage 2 (S2, moderate), and greater than 293 dB/m for steatosis stage 3 (S3, severe) (21, 22).
The characteristics of the study participants were analyzed according to the status of ketogenesis using Student’s t-test for continuous variables and Pearson’s χ2 test for categorical variables. All continuous variables were presented as the mean ± standard deviation, and categorical variables were presented as a number with percentage (%). The correlations between serum βHB levels and steatosis stages and CAP scores were assessed with Pearson’s correlation analysis. Multivariable logistic regression analysis was applied to determine the independent association between ketogenesis and hepatic steatosis. The ketogenic capacity defined as intact or impaired ketogenesis based on the median serum βHB level was used as a variable in the logistic regression. Age, sex, BMI, HbA1c, LDL-C, HOMA-IR, and HOMA-β were adjusted in the multivariable regression analysis. Statistical analyses were performed using R software version 3.6.3 (R Project for Statistical Computing, Vienna, Austria). The adjusted odds ratio (OR) and 95% confidence interval (CI) were determined. P-values <0.05 were considered statistically significant.
A total of 361 newly diagnosed T2D patients who satisfied both inclusion and exclusion criteria were included as study participants. Subjects were divided into intact (βHB>0, n=163) and impaired ketogenesis (βHB=0, n=198) groups according to the baseline level of βHB. Baseline characteristics stratified by the level of βHB are presented in Table 1. The mean age and BMI of the study subjects were 54.3 ± 12.5 years and 27.4 ± 4.2 kg/m2, respectively. A total of 60.9% of the patients were men. Both groups had similar characteristics in terms of age, sex, BMI, and liver enzyme levels. However, the group with intact ketogenesis had notably higher levels of HbA1c, indicating poorer glycemic control, compared to the group with impaired ketogenesis. In the context of insulin secretory function, the intact ketogenesis group also demonstrated markedly lower levels of fasting and postprandial C-peptide and insulin levels compared to patients with impaired ketogenesis. Additionally, subjects in the intact ketogenesis group had decreased HOMA-β and lower HOMA-IR without significance compared to the impaired group. Meanwhile, TG levels were lower and LDL-C levels were higher, without statistical significance, but TG/LCL-C was significantly lower in the intact group. Collectively, the subjects with intact ketogenesis capacity at the time of first diagnosis of T2D showed higher serum glucose levels with more prominent insulin deficiency and potentially lower insulin resistance.
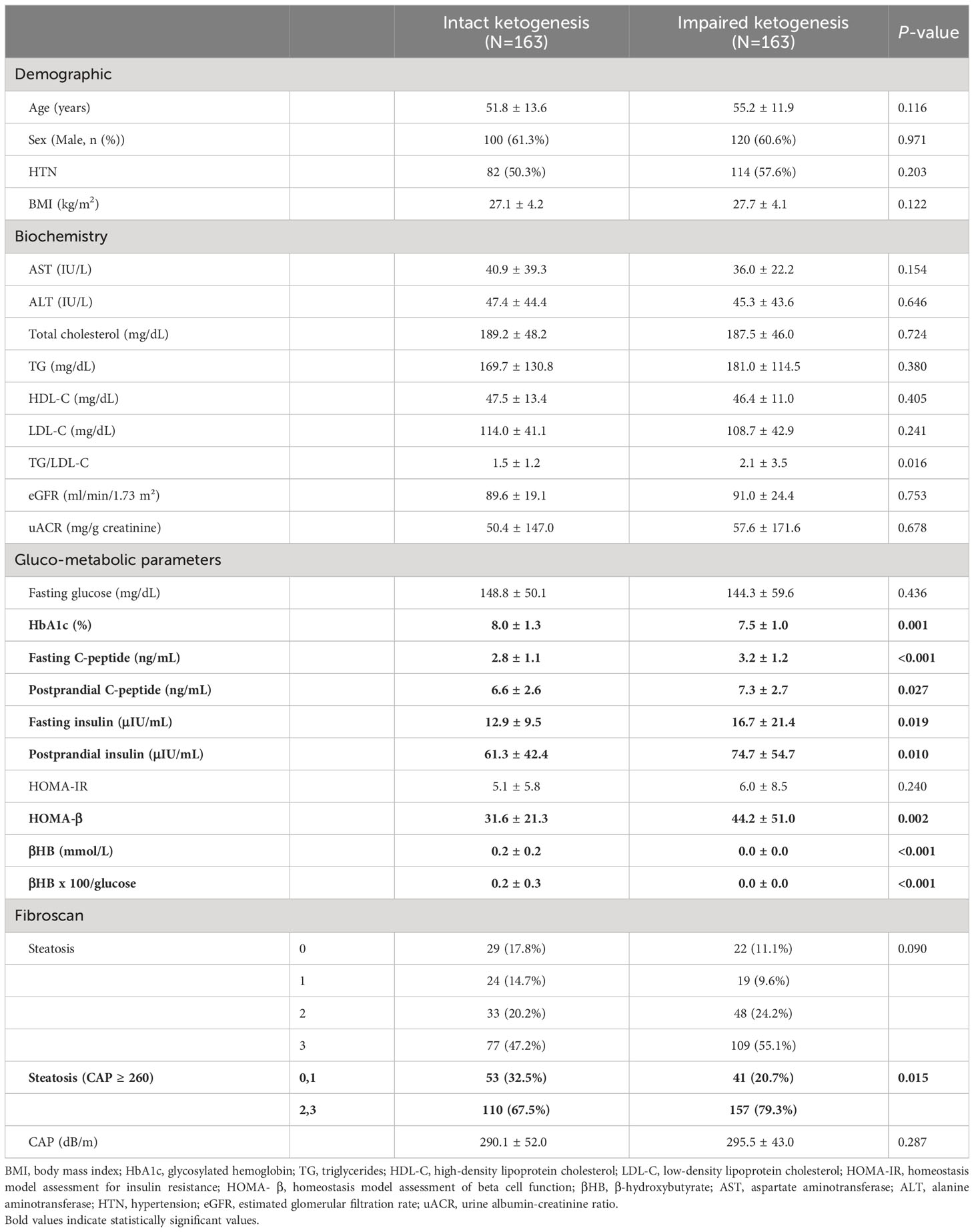
Table 1 Characteristics of the study population according to baseline βHB.
In this study, the presence of significant MAFLD was defined as steatosis stage ≥S2 (moderate–severe) (21, 22). The intact ketogenesis group showed a tendency to lower levels of steatosis stage and CAP values (290.1 ± 52.0 vs. 295.5 ± 43.0) compared with the impaired ketogenesis group, but this difference was not statistically significant. However, moderate–severe hepatic steatosis was less common in the intact group (67.5% vs. 79.3%) with statistical significance (p=0.015).
Collinearity among ketogenic capacities based on serum βHB levels and hepatic steatosis was calculated using Pearson’s correlation analysis (Table 2). Liver steatosis stages stratified from stage S0 to S4 showed a significant negative correlation with βHB and moderate–severe hepatic steatosis showed a negative correlation. Additionally, a negative correlation was observed between CAP scores and βHB levels (r=-0.094, p=0.009).
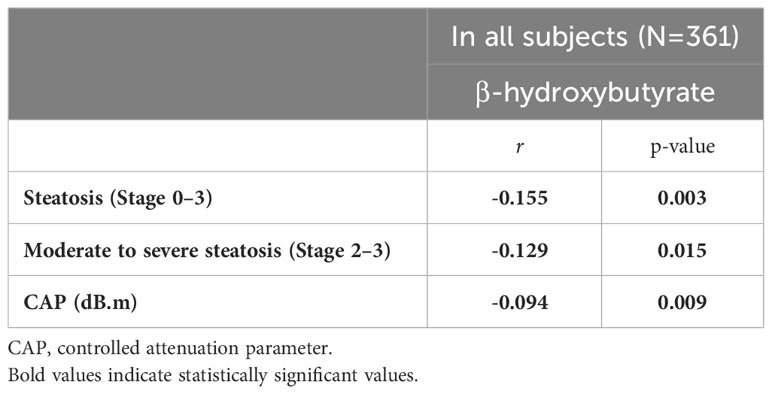
Table 2 Correlations between βHB and hepatic steatosis.
To evaluate whether intact ketogenesis was independently associated with hepatic steatosis, a multiple logistic regression analysis was performed adjusting for age, sex, BMI, HbA1c, LDL-C, HOMA-IR, and HOMA-β. When analyzing each steatosis stage separately, no significant association was found between the ketogenic capacity and all stages of hepatic steatosis. However, statistically significant results were obtained when comparing the stages of moderate–severe MAFLD with normal–mild MAFLD (Figure 1). Intact ketogenesis was associated with a lower OR for the risk of higher hepatic steatosis stage (adjusted OR, 0.55; 95% CI, 0.30–0.98). Adjusted ORs for each variable of hepatic steatosis are summarized in Table 3. BMI (adjusted OR, 1.43; 95% CI, 1.28–1.61; p<0.001) and HbA1c (adjusted OR, 1.37; 95% CI, 1.02–1.85; p=0.037) were associated with moderate–severe hepatic steatosis after adjusting for multiple risk factors. Intact ketogenesis was notably associated with a lower risk of moderate–severe hepatic steatosis compared with impaired ketogenesis.
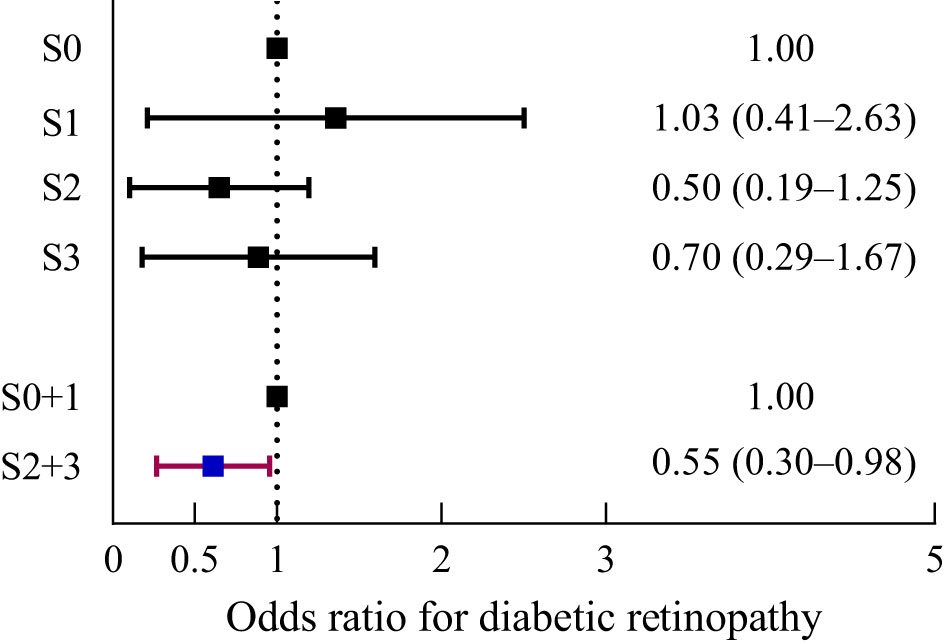
Figure 1 Risk of hepatic steatosis according to intact and impaired ketogenesis.
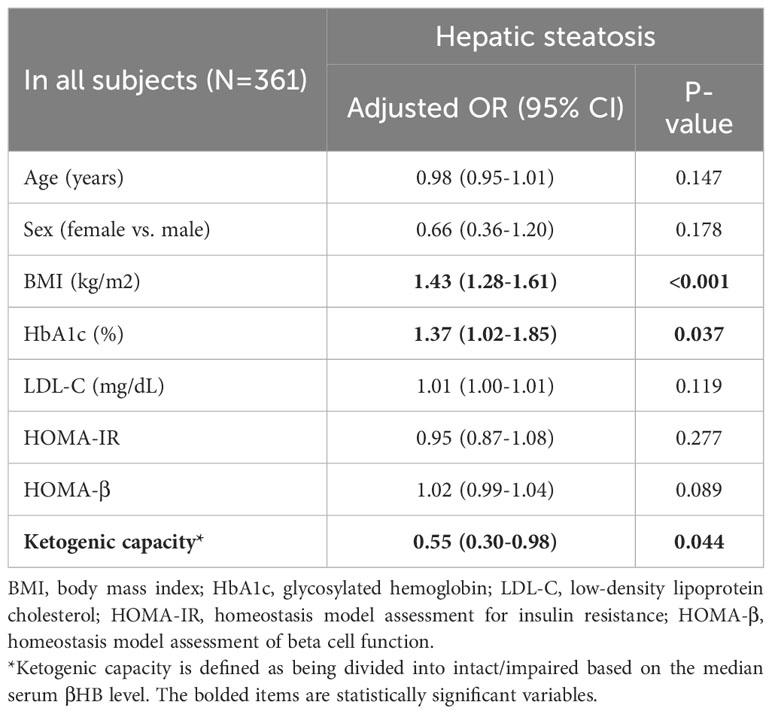
Table 3 Logistic regression analysis for MAFLD incidence based on TE.
Most studies have reported reduced risk for incident hepatic steatosis or advanced hepatic fibrosis in subjects with fasting ketonuria and intact ketonemia (23, 24); however, some studies reported higher ketone levels in subjects with suspected fatty liver disease, prediabetes, or diabetes (25–27). In this cross-sectional study, we investigated the relationship between ketogenic capacity and MAFLD in newly diagnosed T2D patients by measuring serum βHB and CAP levels using TE to assess the ketogenic capacity and MAFLD, respectively. We used the CAP score rather than liver stiffness measurements (LSMs) because we expected that metabolic properties, such as ketogenesis, would preferentially appear in the form of hepatic steatosis rather than fibrosis.
This study had three main findings. First, 42.7% of the T2D patients had serum βHB>0.1 mmol/L, and 3.3% of the patients had >0.57 mmol/L, which was the median serum βHB level of subjects with 2+ ketonuria in the previous study (28). Second, intact ketogenesis predicted a lower risk of moderate–severe MAFLD assessed by TE. Third, T2D patients with intact ketogenesis tended to be more insulin sensitive and had relatively lower insulin secretory function compared to those with impaired ketogenesis.
Either physiologic or pathologic ketogenesis in humans is an effective way to supply efficient energy because it has an adaptive mechanism that allows the liver to utilize deposited TGs to provide energy in the form of ketone bodies during periods of glucose deprivation as well as to dispose of the delivered FAs in the liver; delivered FAs are converted to acetyl-CoA through β-oxidation, thereby undergoing non-oxidative pathway processing to produce ketone bodies (6, 29). In the excess glucose status of T2D, activation of ketogenesis might not be a pathophysiologic mechanism for producing more metabolic fuel but may be an efficient pathway for the disposal of excess FAs. Impairment of the ketogenic pathway in T2D might be activation of gluconeogenesis rather than ketone body generation in the dysregulated liver. In a dysregulated situation, converted acetyl-CoA from FAs is oxidized to carbon dioxide via the TCA cycle, which increases hepatic oxygen consumption and promotes gluconeogenesis (30). As a result, both hepatic de novo lipogenesis and oxidative stress are increased, thereby inducing or aggravating MAFLD. In addition, intact or efficient ketogenesis might have other putative mechanisms that prevent the development of MAFLD; the ketogenic process is reported to induce the hepatic peroxisome proliferation-activated receptor α (PPARα)-fibroblast growth factor 21 (FGF21) axis, which plays a critical role in energy metabolism and whose dysregulation is associated with MAFLD (31, 32). In addition, the ketogenic pathway activates hepatic autophagy and suppresses inflammatory responses (33–35), which is also thought to be beneficial in improving MAFLD.
With respect to intact ketogenesis and MAFLD, our measurements in βHB are in line with a previous study that obtained serum βHB measurements in T2D patients using a nuclear magnetic resonance spectroscopy-based test (36) and found reduced risk for incident hepatic steatosis or advanced hepatic fibrosis in subjects with fasting ketonuria (18, 23, 24). In this study, T2D patients with intact ketogenesis showed a tendency towards lower steatosis stages and CAP values. In particular, the prevalence of moderate–severe hepatic steatosis was significantly lower in the intact ketogenesis group compared to the impaired group. In the logistic regression analysis, intact ketogenesis was significantly associated with lower risk of moderate–severe steatosis. These results are in line with our previous study that reported the relationship between ketogenic capacity and hepatic steatosis indices (18). Considering the ketogenic mechanisms that were described above, the results of our study, showing an association between intact ketogenesis and lower risk of moderate–severe MAFLD in subjects with T2D, are convincing.
Relatively severe insulin resistance in impaired ketogenic subjects is considered to have contributed to the development or aggravation of MAFLD. The greater difference in the plasma insulin levels between the two groups, compared to the difference in the HOMA-IR, might be due to lower hepatic insulin clearance in the impaired ketogenesis group, which has been reported to be associated with MAFLD (37).
The strength of this study, to the best of our knowledge, is it is the first to show the association between ketogenic capacity and hepatic steatosis using TE imaging in subjects with drug-naïve, newly diagnosed T2D. The present study has some limitations to be considered. First, our study was a cross-sectional design, so we cannot offer a conclusive opinion on the association between ketogenic capacity and MAFLD. Second, we used TE to investigate the presence and extent of MAFLD. Although it is relatively less accurate than magnetic resonance imaging-based methods (38, 39), TE is well known for its good accessibility, reproducibility, and validation. Therefore, TE is recommended as an acceptable non-invasive method to assess MAFLD according to current guidelines (40, 41). Third, we only used blood βHB to assess ketogenic capacity. As mentioned in the introduction section, ketone bodies include βHB, acetoacetate, and acetone. Although βHB is the most abundant form of the blood ketone bodies, lack of data on acetoacetate and acetone might be a limitation. Especially, the βHB/acetoacetate ratio is known to reflect the hepatic redox state, which is a major phenotype of the genetic aspect of MAFLD pathogenesis (42). Therefore, if we had collected data on acetoacetate, the mechanistic explanation might be a little clearer. Finally, we do not have histological data based on liver biopsies, the gold standard for diagnosis of liver steatohepatitis and fibrosis.
In T2D patients, intact ketogenesis is related to the lower risk of moderate–severe MAFLD assessed by TE. This result is in line with a previous study that used MAFLD indices and is supported by putative pathophysiologic mechanisms, such as the favorable aspects of de novo lipogenesis and oxidative stress, induction of the PPARα-FGF21 axis, activation of hepatic autophagy, and suppression of inflammatory processes. Longitudinal studies including large populations, advanced imaging modalities, and/or histological data are needed to elucidate the relationship between ketogenesis and MAFLD.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by the Institutional review board of Severance Hospital. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
SL: Conceptualization, Data curation, Writing – original draft. JB: Conceptualization, Data curation, Formal Analysis, Writing – original draft. SK: Data curation, Writing – review & editing. ML: Conceptualization, Writing – review & editing. Y-HL: Conceptualization, Writing – review & editing. EK: Conceptualization, Writing – review & editing. B-SC: Conceptualization, Writing – review & editing. B-WL: Conceptualization, Data curation, Formal Analysis, Methodology, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Chalasani N, Younossi Z, Lavine JE, Charlton M, Cusi K, Rinella M, et al. The diagnosis and management of nonalcoholic fatty liver disease: practice guidance from the american association for the study of liver diseases. Hepatology (2018) 67(1):328–57. doi: 10.1002/hep.29367
2. Perumpail BJ, Khan MA, Yoo ER, Cholankeril G, Kim D, Ahmed A. Clinical epidemiology and disease burden of nonalcoholic fatty liver disease. World J Gastroenterol (2017) 23(47):8263–76. doi: 10.3748/wjg.v23.i47.8263
3. Bril F, Cusi K. Management of nonalcoholic fatty liver disease in patients with type 2 diabetes: A call to action. Diabetes Care (2017) 40(3):419–30. doi: 10.2337/dc16-1787
4. Ballestri S, Zona S, Targher G, Romagnoli D, Baldelli E, Nascimbeni F, et al. Nonalcoholic fatty liver disease is associated with an almost twofold increased risk of incident type 2 diabetes and metabolic syndrome. Evidence from a systematic review and meta-analysis. J Gastroenterol Hepatol (2016) 31(5):936–44. doi: 10.1111/jgh.13264
5. Eslam M, Newsome PN, Sarin SK, Anstee QM, Targher G, Romero-Gomez M, et al. A new definition for metabolic dysfunction-associated fatty liver disease: an international expert consensus statement. J Hepatol (2020) 73(1):202–9. doi: 10.1016/j.jhep.2020.03.039
6. Balasse EO. Kinetics of ketone body metabolism in fasting humans. Metabolism (1979) 28(1):41–50. doi: 10.1016/0026-0495(79)90166-5
7. Aubert G, Martin OJ, Horton JL, Lai L, Vega RB, Leone TC, et al. The failing heart relies on ketone bodies as a fuel. Circulation (2016) 133(8):698–705. doi: 10.1161/circulationaha.115.017355
8. Mudaliar S, Alloju S, Henry RR. Can a shift in fuel energetics explain the beneficial cardiorenal outcomes in the empa-reg outcome study? A unifying hypothesis. Diabetes Care (2016) 39(7):1115–22. doi: 10.2337/dc16-0542
9. Sunny NE, Parks EJ, Browning JD, Burgess SC. Excessive hepatic mitochondrial tca cycle and gluconeogenesis in humans with nonalcoholic fatty liver disease. Cell Metab (2011) 14(6):804–10. doi: 10.1016/j.cmet.2011.11.004
10. Bergman BC, Cornier MA, Horton TJ, Bessesen DH. Effects of fasting on insulin action and glucose kinetics in lean and obese men and women. Am J Physiol Endocrinol Metab (2007) 293(4):E1103–11. doi: 10.1152/ajpendo.00613.2006
11. Fabbrini E, Sullivan S, Klein S. Obesity and nonalcoholic fatty liver disease: biochemical, metabolic, and clinical implications. Hepatology (2010) 51(2):679–89. doi: 10.1002/hep.23280
12. d'Avignon DA, Puchalska P, Ercal B, Chang Y, Martin SE, Graham MJ, et al. Hepatic ketogenic insufficiency reprograms hepatic glycogen metabolism and the lipidome. JCI Insight (2018) 3(12). doi: 10.1172/jci.insight.99762
13. Puchalska P, Crawford PA. Multi-dimensional roles of ketone bodies in fuel metabolism, signaling, and therapeutics. Cell Metab (2017) 25(2):262–84. doi: 10.1016/j.cmet.2016.12.022
14. Watanabe M, Tozzi R, Risi R, Tuccinardi D, Mariani S, Basciani S, et al. Beneficial effects of the ketogenic diet on nonalcoholic fatty liver disease: A comprehensive review of the literature. Obes Rev (2020) 21(8):e13024. doi: 10.1111/obr.13024
15. Cotter DG, Ercal B, Huang X, Leid JM, d'Avignon DA, Graham MJ, et al. Ketogenesis prevents diet-induced fatty liver injury and hyperglycemia. J Clin Invest (2014) 124(12):5175–90. doi: 10.1172/jci76388
16. Luukkonen PK, Dufour S, Lyu K, Zhang XM, Hakkarainen A, Lehtimäki TE, et al. Effect of a ketogenic diet on hepatic steatosis and hepatic mitochondrial metabolism in nonalcoholic fatty liver disease. Proc Natl Acad Sci U.S.A. (2020) 117(13):7347–54. doi: 10.1073/pnas.1922344117
17. Asif S, Kim RY, Fatica T, Sim J, Zhao X, Oh Y, et al. Hmgcs2-mediated ketogenesis modulates high-fat diet-induced hepatosteatosis. Mol Metab (2022) 61:101494. doi: 10.1016/j.molmet.2022.101494
18. Lee S, Bae J, Jo DR, Lee M, Lee Y-h, Kang ES, et al. Impaired ketogenesis is associated with metabolic-associated fatty liver disease in subjects with type 2 diabetes. Front Endocrinol (2023) 14:1124576. doi: 10.3389/fendo.2023.1124576
19. Sasso M, Beaugrand M, de Ledinghen V, Douvin C, Marcellin P, Poupon R, et al. Controlled attenuation parameter (Cap): A novel vcte™ Guided ultrasonic attenuation measurement for the evaluation of hepatic steatosis: preliminary study and validation in a cohort of patients with chronic liver disease from various causes. Ultrasound Med Biol (2010) 36(11):1825–35. doi: 10.1016/j.ultrasmedbio.2010.07.005
20. Chon YE, Jung KS, Kim SU, Park JY, Park YN, Kim DY, et al. Controlled attenuation parameter (Cap) for detection of hepatic steatosis in patients with chronic liver diseases: A prospective study of a native korean population. Liver Int (2014) 34(1):102–9. doi: 10.1111/liv.12282
21. Yen YH, Chen JB, Cheng BC, Chen JF, Chang KC, Tseng PL, et al. Using controlled attenuation parameter combined with ultrasound to survey non-alcoholic fatty liver disease in hemodialysis patients: A prospective cohort study. PloS One (2017) 12(4):e0176027. doi: 10.1371/journal.pone.0176027
22. Lupşor-Platon M, Feier D, Stefănescu H, Tamas A, Botan E, Sparchez Z, et al. Diagnostic accuracy of controlled attenuation parameter measured by transient elastography for the non-invasive assessment of liver steatosis: A prospective study. J Gastrointestin Liver Dis (2015) 24(1):35–42. doi: 10.15403/jgld.2014.1121.mlp
23. Kim Y, Chang Y, Kwon MJ, Hong YS, Kim MK, Sohn W, et al. Fasting ketonuria and the risk of incident nonalcoholic fatty liver disease with and without liver fibrosis in nondiabetic adults. Am J Gastroenterol (2021) 116(11):2270–8. doi: 10.14309/ajg.0000000000001344
24. Lim K, Kang M, Park J. Association between fasting ketonuria and advanced liver fibrosis in non-alcoholic fatty liver disease patients without prediabetes and diabetes mellitus. Nutrients (2021) 13(10). doi: 10.3390/nu13103400
25. Post A, Garcia E, van den Berg EH, Flores-Guerrero JL, Gruppen EG, Groothof D, et al. Nonalcoholic fatty liver disease, circulating ketone bodies and all-cause mortality in a general population-based cohort. Eur J Clin Invest (2021) 51(12):e13627. doi: 10.1111/eci.13627
26. Mahendran Y, Vangipurapu J, Cederberg H, Stancáková A, Pihlajamäki J, Soininen P, et al. Association of ketone body levels with hyperglycemia and type 2 diabetes in 9,398 finnish men. Diabetes (2013) 62(10):3618–26. doi: 10.2337/db12-1363
27. Saasa V, Beukes M, Lemmer Y, Mwakikunga B. Blood ketone bodies and breath acetone analysis and their correlations in type 2 diabetes mellitus. Diagnostics (Basel) (2019) 9(4). doi: 10.3390/diagnostics9040224
28. Kim G, Lee SG, Lee BW, Kang ES, Cha BS, Ferrannini E, et al. Spontaneous ketonuria and risk of incident diabetes: A 12 year prospective study. Diabetologia (2019) 62(5):779–88. doi: 10.1007/s00125-019-4829-x
29. McGarry JD, Foster DW. Regulation of ketogenesis and clinical aspects of the ketotic state. Metabolism (1972) 21(5):471–89. doi: 10.1016/0026-0495(72)90059-5
30. Fletcher JA, Deja S, Satapati S, Fu X, Burgess SC, Browning JD. Impaired ketogenesis and increased acetyl-coa oxidation promote hyperglycemia in human fatty liver. JCI Insight (2019) 5(11). doi: 10.1172/jci.insight.127737
31. Badman MK, Pissios P, Kennedy AR, Koukos G, Flier JS, Maratos-Flier E. Hepatic fibroblast growth factor 21 is regulated by pparalpha and is a key mediator of hepatic lipid metabolism in ketotic states. Cell Metab (2007) 5(6):426–37. doi: 10.1016/j.cmet.2007.05.002
32. Piccinin E, Moschetta A. Hepatic-specific pparα-fgf21 action in nafld. Gut (2016) 65(7):1075–6. doi: 10.1136/gutjnl-2016-311408
33. Byun S, Seok S, Kim YC, Zhang Y, Yau P, Iwamori N, et al. Fasting-induced fgf21 signaling activates hepatic autophagy and lipid degradation via jmjd3 histone demethylase. Nat Commun (2020) 11(1):807. doi: 10.1038/s41467-020-14384-z
34. Youm YH, Nguyen KY, Grant RW, Goldberg EL, Bodogai M, Kim D, et al. The ketone metabolite β-hydroxybutyrate blocks nlrp3 inflammasome-mediated inflammatory disease. Nat Med (2015) 21(3):263–9. doi: 10.1038/nm.3804
35. Kim DH, Park MH, Ha S, Bang EJ, Lee Y, Lee AK, et al. Anti-inflammatory action of β-hydroxybutyrate via modulation of pgc-1α and foxo1, mimicking calorie restriction. Aging (Albany NY) (2019) 11(4):1283–304. doi: 10.18632/aging.101838
36. Garcia E, Shalaurova I, Matyus SP, Oskardmay DN, Otvos JD, Dullaart RPF, et al. Ketone bodies are mildly elevated in subjects with type 2 diabetes mellitus and are inversely associated with insulin resistance as measured by the lipoprotein insulin resistance index. J Clin Med (2020) 9(2). doi: 10.3390/jcm9020321
37. Najjar SM, Caprio S, Gastaldelli A. Insulin clearance in health and disease. Annu Rev Physiol (2023) 85:363–81. doi: 10.1146/annurev-physiol-031622-043133
38. Lee YH, Cho Y, Lee BW, Park CY, Lee DH, Cha BS, et al. Nonalcoholic fatty liver disease in diabetes. Part I: epidemiology and diagnosis. Diabetes Metab J (2019) 43(1):31–45. doi: 10.4093/dmj.2019.0011
39. Lee DH. Noninvasive evaluation of nonalcoholic fatty liver disease. Endocrinol Metab (Seoul) (2020) 35(2):243–59. doi: 10.3803/EnM.2020.35.2.243
40. Rinella ME, Neuschwander-Tetri BA, Siddiqui MS, Abdelmalek MF, Caldwell S, Barb D, et al. Aasld practice guidance on the clinical assessment and management of nonalcoholic fatty liver disease. Hepatology (2023) 77(5):1797–835. doi: 10.1097/hep.0000000000000323
41. Archer AJ, Belfield KJ, Orr JG, Gordon FH, Abeysekera KW. Easl clinical practice guidelines: non-invasive liver tests for evaluation of liver disease severity and prognosis. Frontline Gastroenterol (2022) 13(5):436–9. doi: 10.1136/flgastro-2021-102064
Keywords: ketogenesis, β-hydroxybutyrate, steatosis, MAFLD, diabetes
Citation: Lee S, Bae J, Kim SU, Lee M, Lee Y-h, Kang ES, Cha B-S and Lee B-W (2024) Intact ketogenesis predicted reduced risk of moderate-severe metabolic-associated fatty liver disease assessed by liver transient elastography in newly diagnosed type 2 diabetes. Front. Endocrinol. 14:1306134. doi: 10.3389/fendo.2023.1306134
Received: 03 October 2023; Accepted: 12 December 2023;
Published: 08 January 2024.
Edited by:
Qi Pan, Peking University, ChinaReviewed by:
Ildiko Szanto, Hôpitaux Universitaires de Genève (HUG), SwitzerlandCopyright © 2024 Lee, Bae, Kim, Lee, Lee, Kang, Cha and Lee. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Byung-Wan Lee, YndhbmxlZUB5dWhzLmFj
†These authors have contributed equally to this work and share first authorship
‡ORCID: Byung-Wan Lee, orcid.org/0000-0002-9899-4992
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.