
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol. , 16 January 2024
Sec. Thyroid Endocrinology
Volume 14 - 2023 | https://doi.org/10.3389/fendo.2023.1305629
This article is part of the Research Topic Advances in Thyroid Surgery and Ablation Therapy - Treatment Considerations in the Era of Quality of Life View all 12 articles
 Feng-Yu Chiang1,2Yu-Chen Shih3
Feng-Yu Chiang1,2Yu-Chen Shih3 Ching-Feng Lien1,2Chih-Chun Wang1,2
Ching-Feng Lien1,2Chih-Chun Wang1,2 Chien-Chung Wang1Tzer-Zen Hwang1,2Yaw-Chang Huang1
Chien-Chung Wang1Tzer-Zen Hwang1,2Yaw-Chang Huang1 Che-Wei Wu4Tai-Hung Yeh1*
Che-Wei Wu4Tai-Hung Yeh1* Tzu-Yen Huang4,5*
Tzu-Yen Huang4,5*Objectives: The feasibility and reliability of trans-thyroid cartilage EMG recording method (TCERM) during intraoperative monitoring (IONM) of the recurrent laryngeal nerve (RLN) in thyroid surgery have been established. This study compared two different recording electrode placements on the ipsi-lateral and contra-lateral lamina of the thyroid cartilage (TC).
Methods: Fifty consecutive patients undergoing total thyroidectomy with 100 RLNs at risk were enrolled. Two paired subdermal needle electrodes were inserted into the subperichondrium of the bilateral TC lamina to record electromyography (EMG) signals. The channel leads from the TC electrodes were connected to the patient interface with two different modes. In A-mode, the electrode leads were placed ipsi-laterally, and channel 1 monitored the left RLN and channel 2 monitored the right RLN respectively. In B-mode, the electrode leads were placed contra-laterally, and channels 1 and 2 simultaneously monitored the same side of the RLN. The amplitudes of four EMG signals (V1-R1-R2-V2) recorded by A-mode and B-mode were compared.
Results: All EMG amplitudes of V1-R1-R2-V2 signals recorded with B-mode were all above 500μV and significantly higher than those with A-mode (p<0.001). No false loss of signal, electrode dislodgement, or needle-related complications were noted during IONM. Postoperatively, all patients had symmetrical vocal cord movement. Lower EMG amplitudes were observed in older and male patients. Histopathology and laterality showed no significant differences in EMG amplitude.
Conclusion: During using TCERM in thyroid surgery, the recording electrodes should be placed contra-laterally on the TC lamina. This approach ensures high and stable EMG signals, which are important for high-quality IONM of the RLN.
During the application of intraoperative neuromonitoring (IONM) in thyroid surgery, at least one pair of electrodes is required to record the electromyography (EMG) signal or potential difference from the intrinsic laryngeal muscle, a diagnostic procedure used to assess recurrent laryngeal nerve (RLN) function.
Surface electrode placement is preferred over intramuscular placement because of its non-invasive nature to the vocal cords (1, 2). Therefore, surface electrodes placed on the endotracheal tube (ETT electrodes) have been commonly used to monitor RLN function for decades. However, ETT electrodes often experience changes in electrode-vocal cord contact quality due to laryngeal edema or electrode displacement during surgical manipulation of the trachea. The inconsistent electrodes-vocal cord contact quality can lead to significant changes in the EMG amplitudes during surgery, making quantitative amplitude analysis and actual RLN function evaluation difficult (3–9).
In recent years, the trans-thyroid cartilage EMG recording method (TCERM) has been reported to provide higher quality and more stable EMG signals than the trans-ETT recording method (10–20). The one-channel recording method, in which two independent recording electrodes are placed on the contra-lateral TC lamina, was utilized in the studies by Chiang (10), Liddy (11), Van Slycke (12), Türk (13), and Jung (14). With this electrode placement, both sides of the RLN can be successfully monitored with the same channel electrodes, but it does not provide the lateral discrimination of nerve stimulation. Using the one-channel recording method, Lee et al. (15) placed the recording electrodes on the ipsilateral TC lamina during unilateral hemithyroidectomy. This approach successfully obtained EMG signals, but only one side of the RLN could be monitored.
During using TCERM, the EMG signals can be recorded by one- or two-channel methods, and the recording electrodes can be ipsi-laterally or contra-laterally placed on the TC lamina. When performing a two-channel recording method for TCERM, two pairs of recording electrodes are required to be placed on the bilateral TC lamina. The method is similar to the use of Medtronic standard EMG ETT (3), where the paired electrodes are placed on both sides of the ETT. With this type of electrode placement, the left paired electrodes monitor the left RLN and the right paired electrodes monitor the right RLN separately. However, in the reports of Chiang (16), Huang (17) and Chiu (18), the channel leads of the TC electrodes were inserted into the patient interface with a cross-connection. With this connection, the placement of the recording electrodes on the TC lamina changes from ipsi-lateral to contra-lateral position, and both channels will monitor the same RLN simultaneously. In order to understand the differences between the two EMG recording methods in which the electrodes are placed on the TC lamina ipsi-laterally and contra-laterally, further investigation is necessary.
From August 2022 to November 2022, 50 consecutive patients undergoing nerve-monitored total thyroidectomy for various thyroid diseases were enrolled in this study. All surgical procedures were performed by the same surgeon (F.-Y.C.). This study was approved by the E-Da Hospital Institutional Review Board (EMRP-112-015/ed112358).
General anesthesia was induced with 2% lidocaine (1 mg/kg), propofol (2-3 mg/kg), a single dose of rocuronium (0.6 mg/kg), and a bolus of fentanyl (2 μg/kg) as necessary. Regular oral endotracheal tubes were intubated and anesthesia was maintained with sevoflurane and propofol target-controlled infusion. Sugammadex (1 mg/kg) was administrated to reverse rocuronium-induced neuromuscular blockade at the time point of skin incision.
After resection of the pyramidal lobe and exposure of the TC, two paired subdermal needle electrodes (length, 12.0 mm; diameter, 0.4 mm; needle spacing, 2.5 mm, Medtronic, Jacksonville, FL) (Figure 1) were bilaterally inserted into the subperichondrium of the middle TC lamina from the anterior edge of the thyrohyoid muscle with a slope of 10° to 15° on each side (blue color electrodes on the left; red color electrodes on the right) (Figure 2). After the needle electrode was placed, it was confirmed that it was stable and not prone to dislodge. The electrode wires were then sutured to the anterior laryngeal soft tissue and the surgical sheet.
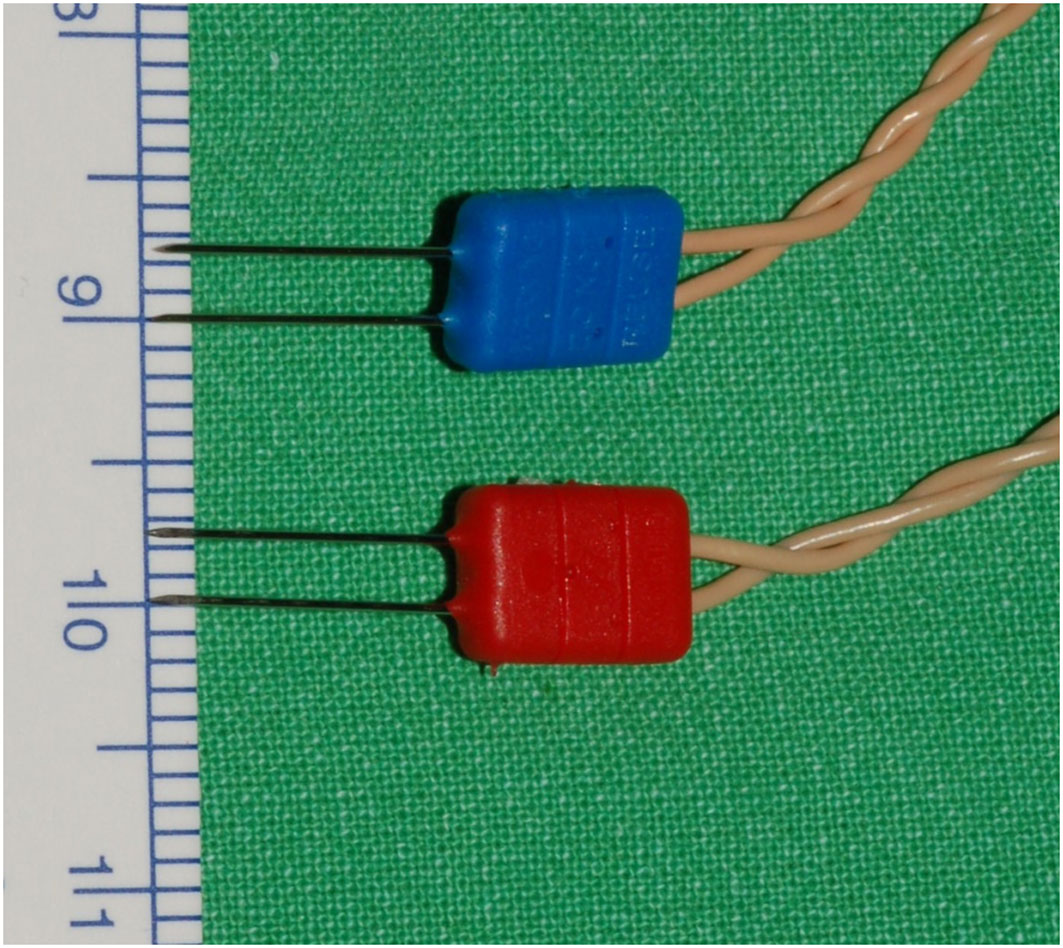
Figure 1 Medtronic paired subdermal needle electrodes: 12.0 mm length, 0.4 mm diameter, and 2.5 mm needle spacing.
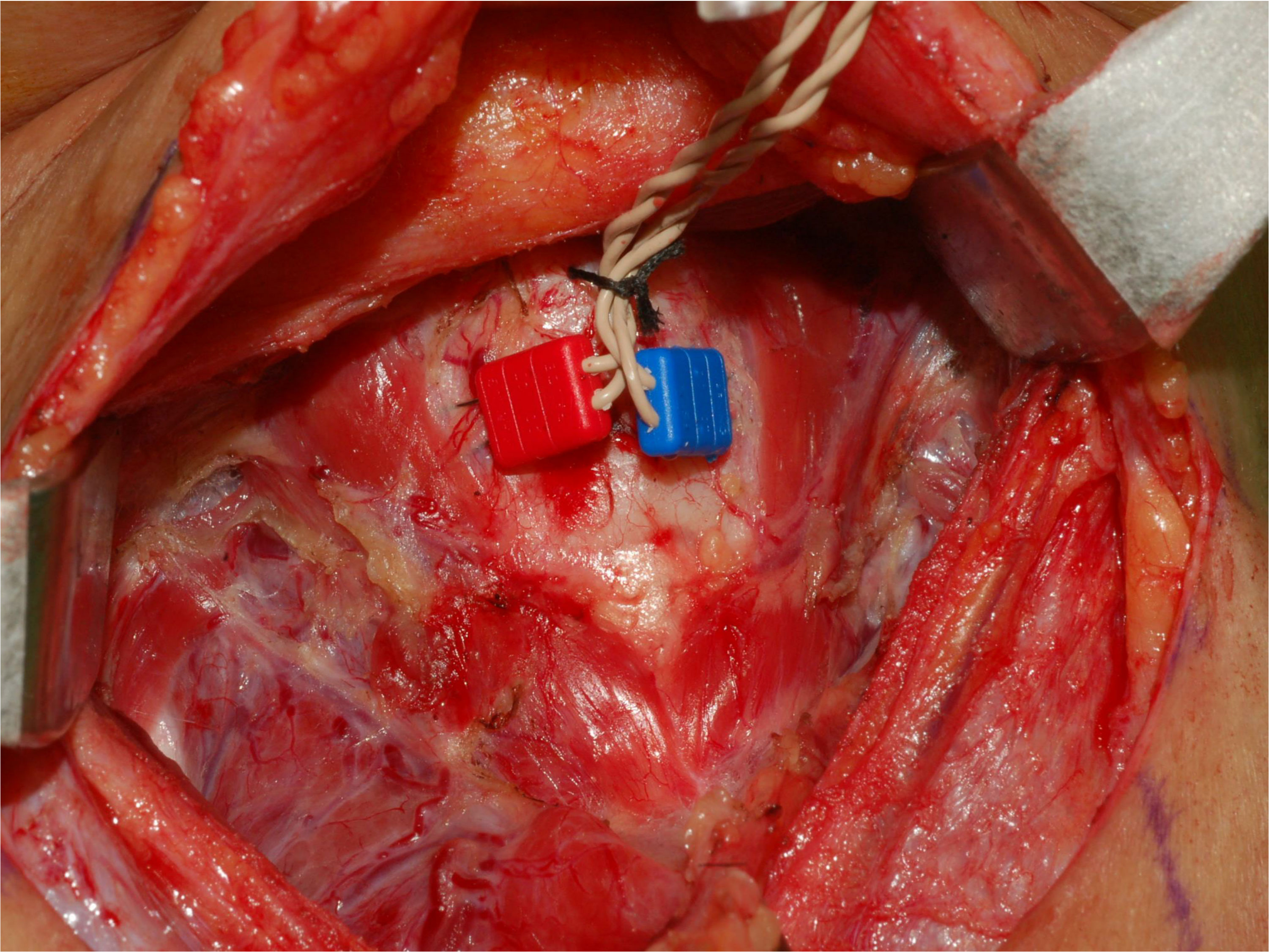
Figure 2 Insertion of paired needles into the subperichondrium of the middle TC lamina with a 10° to 15° angle on each side.
The channel leads from the TC electrodes were connected to the NIM 3.0 patient interface with A- and B-mode (Figures 3A, B). In A-mode, the two blue electrode leads were inserted into channel 1, and the two red electrode leads were inserted into channel 2. With A-mode TCERM, the recording electrodes are placed ipsi-laterally on the TC lamina, where the left paired electrodes monitor the left side nerves and the right paired electrodes monitor the right side nerves, respectively (Figures 4A, B). In B-mode, one of the blue electrode leads was inserted into channel 2 and one of the red electrode leads was inserted into channel 1. With B-mode TCERM, the recording electrodes were placed contra-laterally on each side of the TC lamina. The evoked EMG signals were recorded simultaneously by channels 1 and 2, and the signal with higher amplitude between the two channels was selected and registered (Figures 5A, B).

Figure 3 The channel leads from the TC electrodes are connected to the patient interface: ipsi-laterally in A-mode (A) and contra-laterally in B-mode (B).
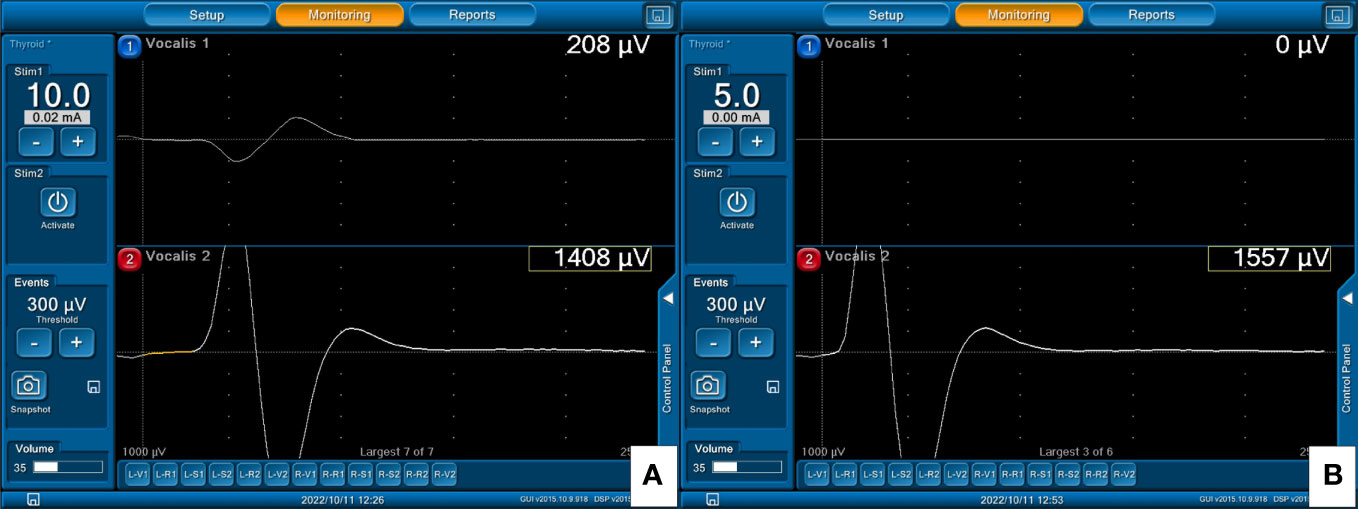
Figure 4 With A-mode TCERM, the left paired TC electrodes monitor the left side nerves and the right TC electrodes monitor the right side nerves, respectively. The EMG signals elicited by stimulation of the right VN (A) and right RLN (B) are shown on channel 2.
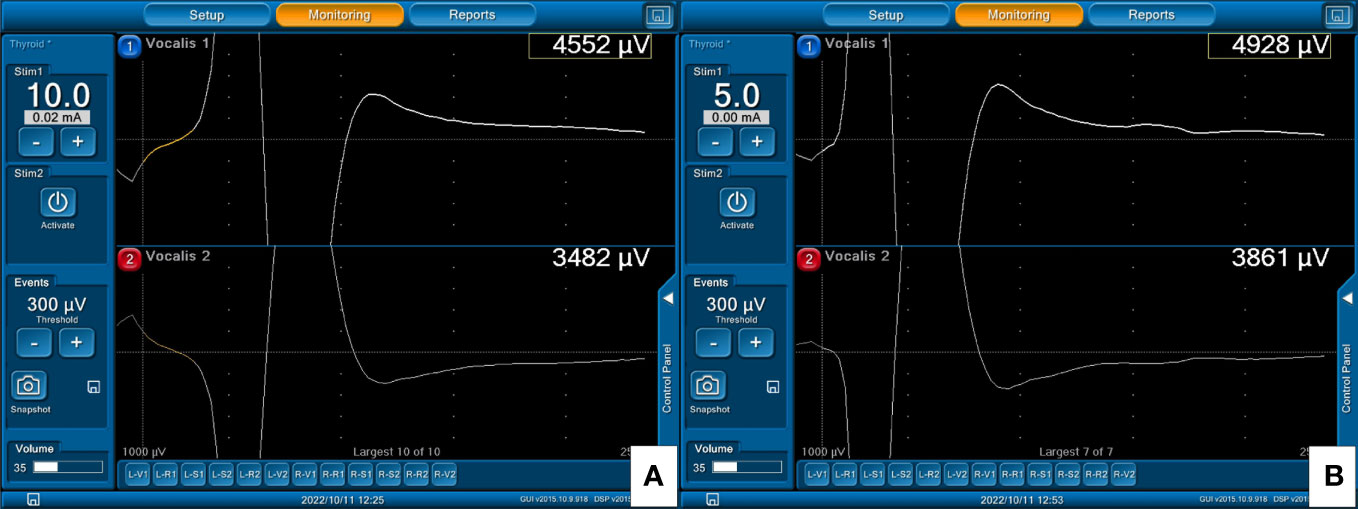
Figure 5 With B-mode TCERM, the EMG signal is recorded simultaneously by channels 1 and 2, and the higher amplitude is selected on channel 1 after stimulation of the right VN (A) and right RLN (B).
The monitoring system generated stimuli with a time window set to 50 ms and an amplitude scale set to 0.2 mV/division. The pulsed stimuli were 100 μs in duration and 4 Hz in frequency. The event threshold was initially set at 300 μV and was reduced to 100 μV or even 50 μV if no EMG signal could be elicited from electrical stimulation of the RLN or vagus nerve (VN).
Standardized IONM procedures were followed routinely in all patients and V1-R1-R2-V2 signals were obtained from VN and RLN stimulation. At each step, EMG signals were first recorded by B-mode and then by A-mode. We used 5-10 mA of stimulus current for VN stimulation without VN exposure and 3-5 mA for RLN stimulation. The EMG amplitudes of V1-R1-R2-V2 signals recorded by A-mode and B-mode were compared, and the EMG amplitudes in the patients with different age, sex, and histopathology were also compared.
All patients underwent pre- and post-operative examination of vocal cord mobility using a flexible laryngofiberscope. All data are presented as mean and standard deviation. To analyze the variables, the paired t-test, independent t-test, and Mann-Whitney U test were performed using SPSS (Version 18.0 for Windows; SPSS Inc., Chicago, IL, USA). A two-tailed p value of less than 0.05 was considered statistically significant.
A total of 50 consecutive patients with 100 RLNs at risk were evaluated in this study. The cohort consisted of 42 females and 8 males. The age of the patients ranged from 23 to 78 years with a mean age of 55.3 years. In the diagnosis, 23 patients were benign disease and 27 patients were malignant disease.
The results for the EMG amplitudes of V1-R1-R2-V2 signals recorded by A-mode and B-mode are presented in Table 1. Using A-mode, the mean amplitudes showed consistently lower values compared to B-mode across all signals. Statistically, there was a significant difference in the mean amplitudes between the two recording methods for all signals, with p-values less than 0.001. Lower amplitudes were also found with A-mode TCERM, in which 50%, 19%, and 3% of V1 signals were less than 500μV, 300μV, and 100μV, respectively. In contrast, no (0%) B-mode V1-R1-R2-V2 signals were less than 500μV.
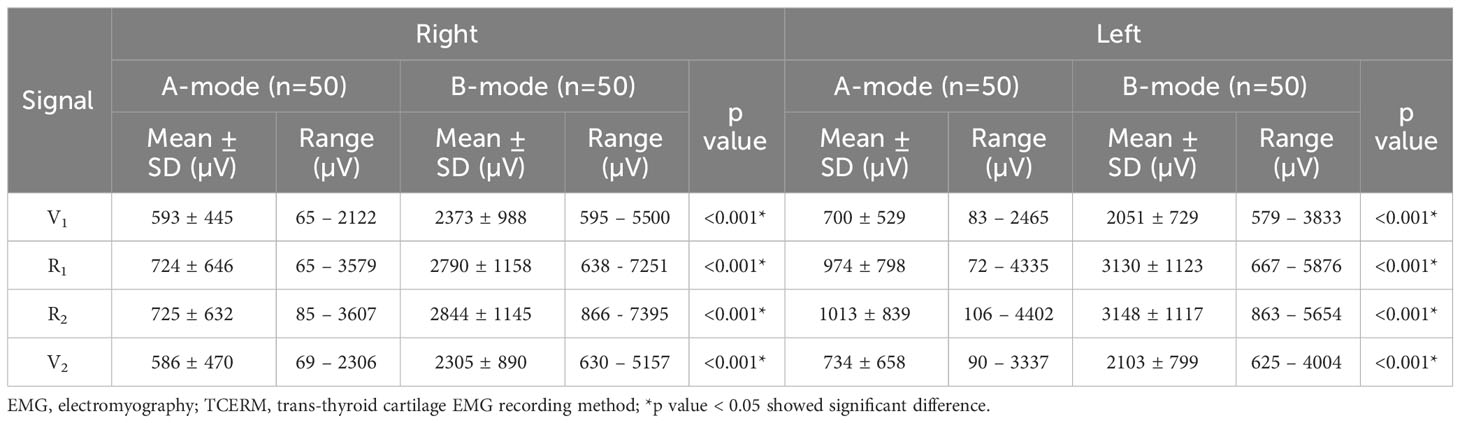
Table 1 The EMG amplitudes of V1-R1-R2-V2 signals recorded by A-mode and B-mode TCERM.
Table 2 compares the EMG amplitudes based on age, sex, and histopathology. In the age-based comparisons, patients aged ≥ 60 years had lower bilateral EMG amplitudes than those younger than 60 years. In sex-based comparisons, male patients had lower bilateral EMG amplitudes than female patients. This difference was significant (p<0.05) for all signals on the right side as well as for the left B-mode signals. In comparisons based on histopathology between patients with benign and malignant disease, the difference was not statistically significant.
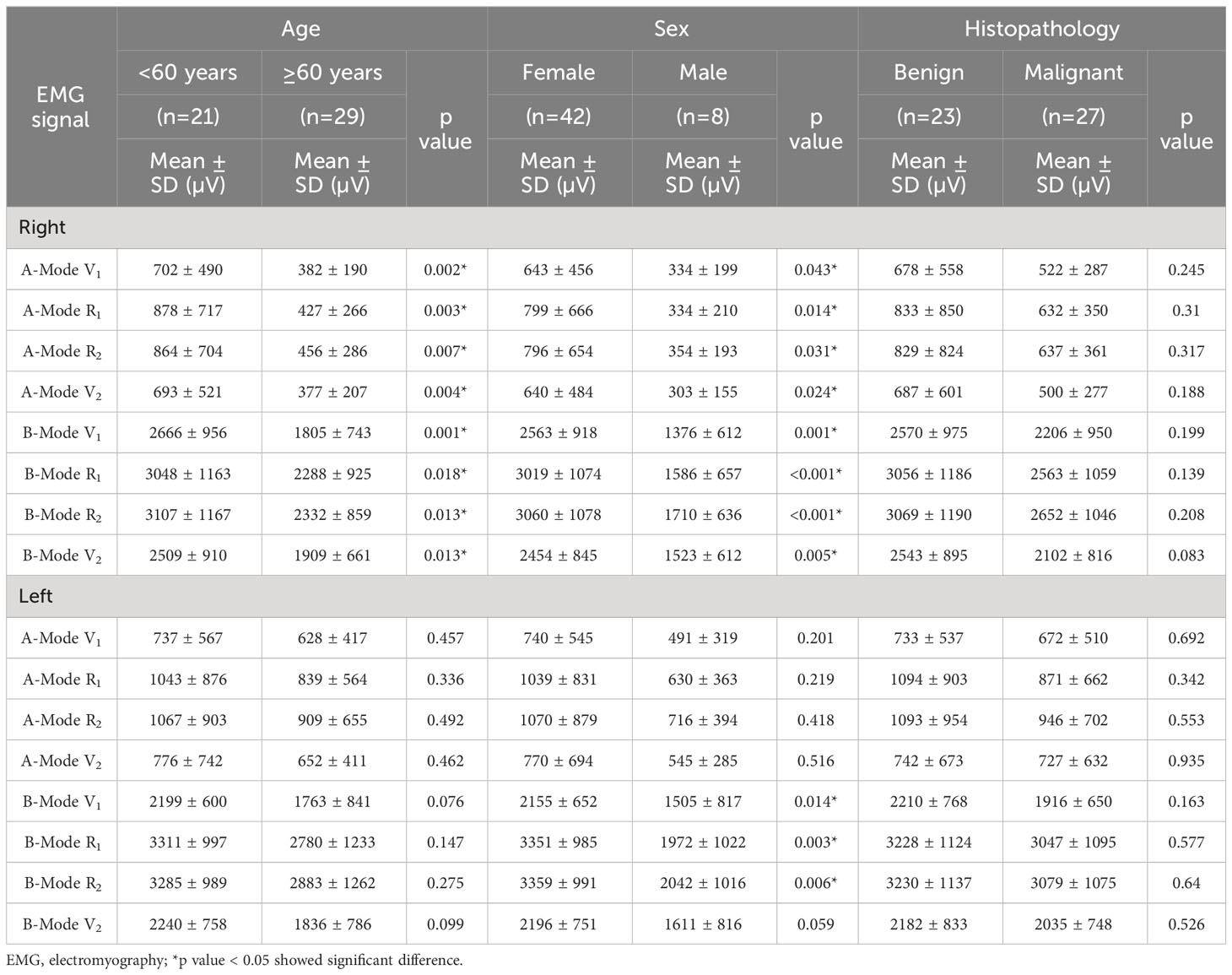
Table 2 Comparison of EMG amplitudes in patients of different age, sex, and histopathology.
When comparing the effect of laterality on EMG amplitude, there was no specific side that showed notably higher EMG amplitude in this comparison (Table 3).
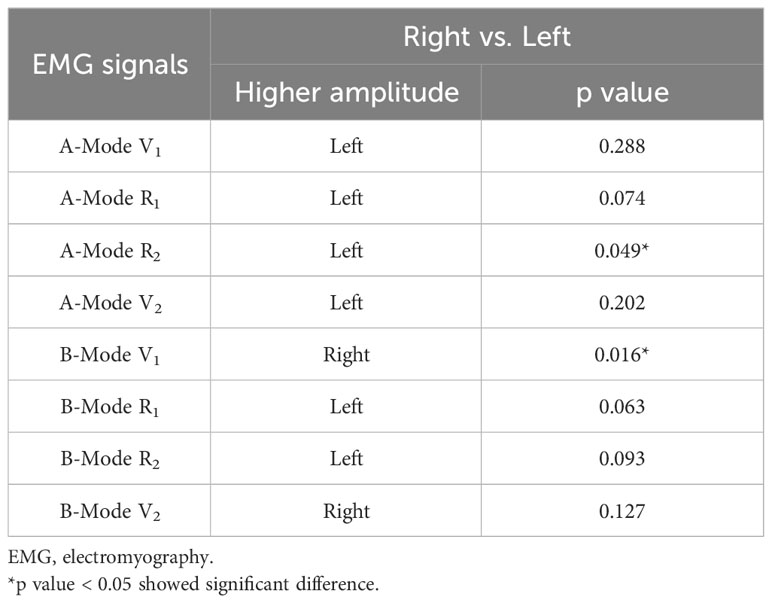
Table 3 Comparison of laterality and EMG amplitudes.
Five RLNs experienced a significant decrease in amplitude intraoperatively due to traction distress. The amplitude recovered completely in 3 nerves and recovered more than 70% in another 2 nerves, and all 5 cases showed symmetric vocal cord movement postoperatively. In addition, no occurrence of false loss of signal (LOS), electrode dislodgement, or needle-related complications were observed.
When IONM is applied in thyroid surgery, the 4-step IONM procedure to obtain V1-R1-R2-V2 signals has been generally accepted as standard (21). The EMG amplitude measured at each step can reflect the functional status of the RLN. Theoretically, a decrease in EMG amplitude during surgery indicates a decreased number of muscle fibers participating in the polarization or a deficit of RLN function (22, 23). Therefore, maintaining high and stable EMG amplitudes throughout the entire surgical procedure is important to help not only for RLN identification, but also for early detection of adverse EMG changes to prevent impending traction injury, quantitative analysis of amplitude change after RLN dissection, accurate prediction of vocal cord function outcome, avoidance of the occurrence of false LOS, and elucidation of the mechanism and severity of nerve injury.
TCERM provides a novel surgical application for IONM technology. The recording electrodes placed on the outer surface of the TC lamina can well receive the evoked EMG signals from the thyroarytenoid or vocalis muscles, since the thyroarytenoid muscle runs through the entire length of the vocal cords from the angle of the inner TC lamina to the vocal processes of arytenoid cartilage. In addition, the TC electrodes can be placed and fixed directly on the TC lamina by the surgeon and the EMG signals will not be affected by electrodes position change during surgical maneuvers.
In clinical studies, several types of TC electrode placement for TCERM have been reported. Liddy (11), and Van Slycke (12) reported two independent surface electrodes sutured contra-laterally on the perichondrium of the TC lamina. Both studies concluded that TC surface electrodes provide similar and stable EMG responses with equal sensitivity for recording evoked EMG responses compared to ETT electrodes and appear to be a feasible and reliable alternative. Besides, several commercialized single or paired needle electrodes for TCERM have also been reported, where the recording electrode can be conveniently fixed on the TC by inserting them into the TC lamina. Chiang (10), Türk (13), and Jung (14) used two single-needle electrodes that were inserted into the TC lamina contra-laterally. The results of these studies showed that the mean EMG amplitude of all four EMG signals (V1-R1-R2-V2) recorded by the TC needle electrodes were significantly higher. In addition, no false LOS occurred, and the positive predictive value of LOS was 100%.
The Medtronic paired subdermal needle electrodes (12.0 mm in length, 0.4 mm in diameter and 2.5 mm in electrode spacing, Figure 1) are commonly applied in facial nerve monitoring and are also suitable for TCERM of the RLN in thyroid surgery. Lee et al. (15) used one paired needle electrode inserted into one side of the TC lamina during unilateral hemithyroidectomy, where the paired recording electrodes were placed ipsi-laterally on TC lamina. The results showed that EMG amplitude was significantly lower when needle insertion was superficial (< 5 mm) and the amplitude was less than 500 μV in 23.5% of cases for V1 signal. In this study, two-channel recording method was used and two paired needle electrodes were inserted into the subperichondrium of the bilateral TC lamina. Lower amplitudes were also found with A-mode TCERM, in which 50%, 19%, and 3% of V1 signals were less than 500μV, 300μV, and 100μV, respectively. Two possible reasons may explain why the A-mode TCERM has lower EMG amplitudes. One possibility is due to the increased impedance of calcified TC when the needles are inserted superficially. Another is that the spacing between the two recording needles is only 2.5 mm, so only a small part of the vacalis muscle can be monitored. However, with B-mode TCERM, where two pairs of recording electrodes are placed on the TC lamina contra-laterally, the two-channel recording needles allow monitoring of a larger area of the intrinsic laryngeal muscle. Figure 6 shows the significant difference between the right V1 signals recorded by A-mode and B-mode TCERM when needle electrodes were inserted into the TC lamina superficially (269μV vs. 2173μV).
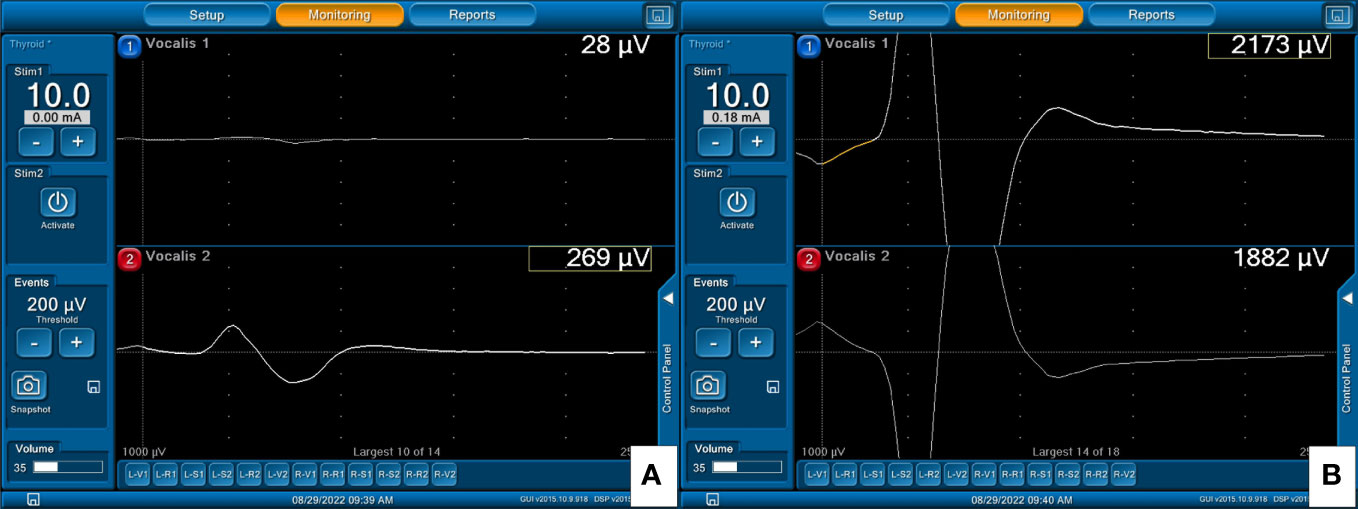
Figure 6 EMG signals from right VN stimulation: (A) 269μV with A-mode and (B) 2173μV with B-mode TCERM, in a patient in whom the needle electrodes were inserted superficially into the TC.
In this study, the B-mode TCERM provides high-quality IONM results: 1) the mean EMG amplitudes of V1-R1-R2-V2 signals showed significantly higher as compared with A-mode TCERM, 2) all V1 signals were higher than 500μV that was recommended by international IONM guidelines as a satisfactory initial EMG signal for proper interpretation, diagnosis, and verification of RLN function, 3) the amplitudes of V2 and R2 signal showed close to or higher than those of V1 and R1 signals in 95 nerves and all showed normal vocal cords movement, 4) the amplitude decreased significantly due to traction distress during surgery in 5 nerves, 3 nerves recovered completely, 2 nerves recovered more than 70%, and all cases showed normal vocal cord movement postoperatively and 5) no occurrence of false LOS.
This study has several limitations similar to other studies when using needle electrodes for TCERM, including:
1). Adequate flap elevation is required to expose TC and limits its use in small neck incision wounds. Pyramidal lobe resection and pre-laryngeal lymph node dissection are routine procedures for our thyroid surgery. TC exposure is not an issue in this study.
2). Patients with calcified TC may have difficulty inserting needle electrodes into the TC lamina. In this study, when the electrodes were placed superficially on the TC, the EMG amplitude showed significantly lower with A-mode TCERM, but a satisfactory EMG signal was obtained with B-mode TCERM.
3). Penetration of the needle electrodes into the larynx may cause laryngeal hematoma, laceration, infection, or rupture of the endotracheal cuff. Although the needle electrodes are inserted into the TC lamina, the needle-related complications can be avoided by proper setup maneuvers, where the needles are inserted into the subperichondrium of the middle thyroid lamina from the anterior margin of the thyrohyoid muscle with a slope of 10° to 15° on each side.
4). Whether the TC thickness is affected by thyroiditis and whether this subsequently affects nerve signaling remains unknown, necessitating future research to confirm.
The paired subdermal needle electrodes used in this study provide a two-channel recording method for IONM of the RLN. From the results of this study, the B-mode TCERM with the recording electrodes placed contra-laterally on the TC lamina meets the requirements for high-quality IONM in thyroid surgery as compared with A-mode TCERM. The novel application of B-mode TCERM provides high and stable EMG amplitudes throughout the entire surgical procedure, which is useful for 1) detection of adverse EMG changes early to prevent impending traction injury, 2) quantifying the amplitude change before and after RLN dissection to elucidate the mechanism and severity of nerve injury, 3) accurately predicting the outcome of vocal cord function, 4) obtaining satisfactory EMG signals, even the needle electrodes placed superficially on the calcified TC lamina, and 5) avoid unnecessary staged thyroidectomy due to false LOS.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding authors.
The studies involving humans were approved by E-Da Hospital Institutional Review Board (EMRP-112-015/ed112358). The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because Retrospective chart review, informed consent was waived.
F-YC: Conceptualization, Data curation, Formal analysis, Investigation, Resources, Supervision, Visualization, Writing – original draft, Writing – review & editing. Y-CS: Data curation, Investigation, Resources, Writing – original draft, Writing – review & editing. C-FL: Formal analysis, Investigation, Writing – review & editing. CChun-W: Data curation, Resources, Writing – review & editing. CChung-W: Data curation, Resources, Writing – review & editing. T-ZH: Project administration, Supervision, Writing – review & editing. Y-CH: Formal analysis, Writing – review & editing. C-WW: Funding acquisition, Project administration, Supervision, Writing – review & editing. T-HY: Data curation, Resources, Supervision, Validation, Writing – original draft, Writing – review & editing. T-YH: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Resources, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was supported by grants from Kaohsiung Medical University Hospital, Kaohsiung Medical University (KMUH111-1R48, KMUH111-1R49), and National Science and Technology Council (NSTC112-2314-B-037-033, NSTC 112-2314-B-037-034), Taiwan.
The authors would like to thank all the patients included in this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
EMG, Electromyography; ETT, Endotracheal tube; IONM, Intraoperative monitoring; LOS, Loss of signal; RLN, Recurrent laryngeal nerve; TC, Thyroid cartilage; TCERM, Trans-thyroid cartilage EMG recording method; VN, Vagus nerve.
1. Dralle H, Sekulla C, Lorenz K, Brauckhoff M, Machens A, Group GIS. Intraoperative monitoring of the recurrent laryngeal nerve in thyroid surgery. World J Surg (2008) 32:1358–66. doi: 10.1007/s00268-008-9483-2
2. Randolph GW, Dralle H, Group wtIIMS, Abdullah H, Barczynski M, Bellantone R, et al. Electrophysiologic recurrent laryngeal nerve monitoring during thyroid and parathyroid surgery: international standards guideline statement. Laryngoscope (2011) 121(S1):S1–S16. doi: 10.1002/lary.21119
3. Lu I-C, Chu K-S, Tsai C-J, Wu C-W, Kuo W-R, Chen H-Y, et al. Optimal depth of NIM EMG endotracheal tube for intraoperative neuromonitoring of the recurrent laryngeal nerve during thyroidectomy. World J Surg (2008) 32:1935–9. doi: 10.1007/s00268-008-9549-1
4. Tsai C-J, Tseng K-Y, Wang F-Y, Lu I-C, Wang H-M, Wu C-W, et al. Electromyographic endotracheal tube placement during thyroid surgery in neuromonitoring of recurrent laryngeal nerve. Kaohsiung J Med Sci (2011) 27(3):96–101. doi: 10.1016/j.kjms.2010.08.002
5. Wu C-W, Wang M-H, Chen C-C, Chen H-C, Chen H-Y, Yu J-Y, et al. Loss of signal in recurrent nerve neuromonitoring: causes and management. Gland Surg (2015) 4(1):19. doi: 10.3978/j.issn.2227-684X.2014.12.03
6. Dionigi G, Bacuzzi A, Boni L, Rovera F, Dionigi R. What is the learning curve for intraoperative neuromonitoring in thyroid surgery? Int J Surg (2008) 6:S7–S12. doi: 10.1016/j.ijsu.2008.12.023
7. Kim HY, Tufano RP, Randolph G, Barczyński M, Wu CW, Chiang FY, et al. Impact of positional changes in neural monitoring endotracheal tube on amplitude and latency of electromyographic response in monitored thyroid surgery: results from the porcine experiment. Head Neck (2016) 38(S1):E1004–E8. doi: 10.1002/hed.24145
8. Snyder SK, Hendricks JC. Intraoperative neurophysiology testing of the recurrent laryngeal nerve: plaudits and pitfalls. Surgery (2005) 138(6):1183–92. doi: 10.1016/j.surg.2005.08.027
9. Chan W-F, Lo C-Y. Pitfalls of intraoperative neuromonitoring for predicting postoperative recurrent laryngeal nerve function during thyroidectomy. World J Surg (2006) 30:806–12. doi: 10.1007/s00268-005-0355-8
10. Chiang FY, Lu IC, Chang PY, Dionigi G, Randolph GW, Sun H, et al. Comparison of EMG signals recorded by surface electrodes on endotracheal tube and thyroid cartilage during monitored thyroidectomy. Kaohsiung J Med Sci (2017) 33(10):503–9. doi: 10.1016/j.kjms.2017.06.014
11. Liddy W, Lawson BR, Barber SR, Kamani D, Shama M, Soylu S, et al. Anterior laryngeal electrodes for recurrent laryngeal nerve monitoring during thyroid and parathyroid surgery: New expanded options for neural monitoring. Laryngoscope (2018) 128(12):2910–5. doi: 10.1002/lary.27362
12. Van Slycke S, Van Den Heede K, Magamadov K, Brusselaers N, Vermeersch H. New placement of recording electrodes on the thyroid cartilage in intra-operative neuromonitoring during thyroid surgery. Langenbeck’s Arch Surg (2019) 404:703–9. doi: 10.1007/s00423-019-01825-7
13. Türk Y, Kıvratma G, Özdemir M, İçöz G, Makay Ö. The use of thyroid cartilage needle electrodes in intraoperative neuromonitoring during thyroidectomy: C ase–control study. Head Neck (2021) 43(11):3287–93. doi: 10.1002/hed.26810
14. Jung SM, Tae K, Song CM, Lee SH, Jeong JH, Ji YB. Efficacy of transcartilaginous electrodes for intraoperative neural monitoring during thyroid surgery. Clin Exp Otorhinolaryngology (2020) 13(4):422–8. doi: 10.21053/ceo.2019.01529
15. Lee HS, Seo SG, Kim DY, Kim SW, Choi Y, Lee KD. Intraoperative neuromonitoring using a single transcartilage needle electrode during thyroidectomy. Laryngoscope (2021) 131(2):448–52. doi: 10.1002/lary.28835
16. Chiang F-Y, Wu C-W, Chang P-Y, Wu S-H, Chen H-Y, Lin Y-C, et al. Trans-thyroid cartilage recording for neural monitoring of the recurrent laryngeal nerve in thyroid surgery. Laryngoscope (2020) 130(4):E280–E3. doi: 10.1002/lary.28049
17. Huang T-Y, Kim H-Y, Dionigi G, Lu I-C, Chang P-Y, Chiang F-Y, et al. Laryngeal neural monitoring during pediatric thyroid cancer surgery—Is transcartilage recording a preferable method? Cancers (2021) 13(16):4051. doi: 10.3390/cancers13164051
18. Chiu K-L, Lien C-F, Wang C-C, Wang C-C, Hwang T-Z, Shih Y-C, et al. Intraoperative EMG recovery patterns and outcomes after RLN traction-related amplitude decrease during monitored thyroidectomy. Front Endocrinol (2022) 13:888381. doi: 10.3389/fendo.2022.888381
19. Wu C-W, Chiang F-Y, Randolph GW, Dionigi G, Kim HY, Lin Y-C, et al. Feasibility of intraoperative neuromonitoring during thyroid surgery using transcartilage surface recording electrodes. Thyroid (2018) 28(11):1508–16. doi: 10.1089/thy.2017.0680
20. Zhao Y, Li C, Zhang D, Zhou L, Liu X, Li S, et al. Experimental study of needle recording electrodes placed on the thyroid cartilage for neuromonitoring during thyroid surgery. J Br Surg (2019) 106(3):245–54. doi: 10.1002/bjs.10994
21. Chiang F-Y, Lee K-W, Chen H-C, Chen H-Y, Lu I-C, Kuo W-R, et al. Standardization of intraoperative neuromonitoring of recurrent laryngeal nerve in thyroid operation. World J Surg (2010) 34:223–9. doi: 10.1007/s00268-009-0316-8
22. Huang H-Y, Lien C-F, Wang C-C, Wang C-C, Hwang T-Z, Shih Y-C, et al. Necessity of routinely testing the proximal and distal ends of exposed recurrent laryngeal nerve during monitored thyroidectomy. Front Endocrinol (2022) 13:923804. doi: 10.3389/fendo.2022.923804
Keywords: recurrent laryngeal nerve (RLN), intraoperative neuromonitoring (IONM), thyroid surgery, electromyography (EMG), recording method
Citation: Chiang F-Y, Shih Y-C, Lien C-F, Wang C-C, Wang C-C, Hwang T-Z, Huang Y-C, Wu C-W, Yeh T-H and Huang T-Y (2024) Comparison of EMG amplitudes recorded by ipsilateral and contralateral electrodes placement during using trans-thyroid cartilage recording method in thyroid surgery. Front. Endocrinol. 14:1305629. doi: 10.3389/fendo.2023.1305629
Received: 02 October 2023; Accepted: 28 December 2023;
Published: 16 January 2024.
Edited by:
Joseph V. Martin, Rutgers University Camden, United StatesReviewed by:
Ilker Sengul, Giresun University, TürkiyeCopyright © 2024 Chiang, Shih, Lien, Wang, Wang, Hwang, Huang, Wu, Yeh and Huang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tai-Hung Yeh, UGV0ZXJ5ZWgzMTEyQGdtYWlsLmNvbQ==; Tzu-Yen Huang, dHlodWFuZy5lbnRAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.